
Eye Movement Alterations in Post-COVID-19 Condition: A Proof-of-Concept Study

 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
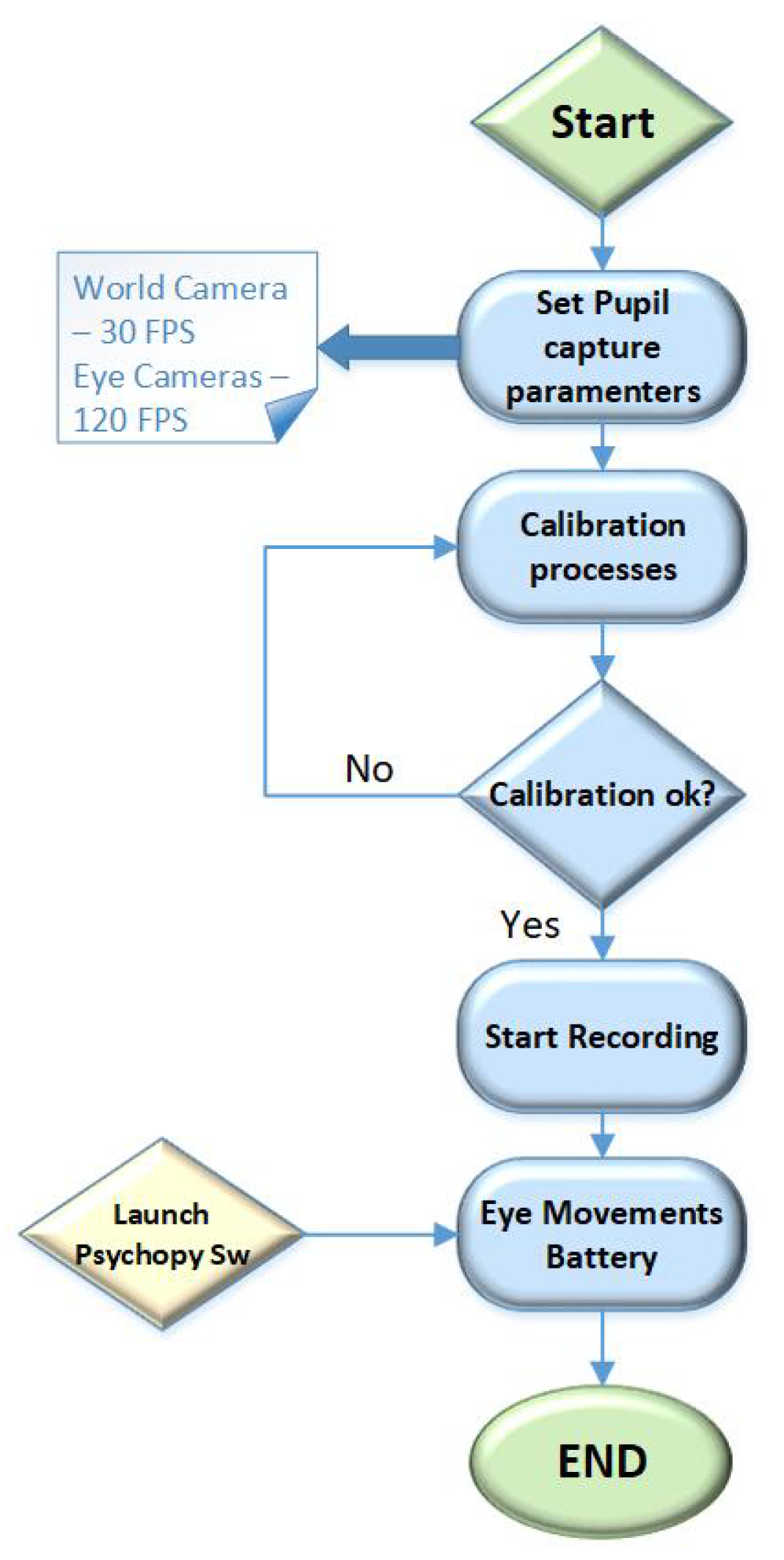
2.1. Hardware and Software Description
2.2. Description of the Eye Movement Battery
2.2.1. Horizontal Visually Guided Saccade Test
2.2.2. Horizontal Memory-Guided Saccade Test
2.2.3. Horizontal Visually Antisaccade Test
2.2.4. Eye Movement Features Characterization
2.3. Healthy Controls and Patients with the Post-COVID-19 Condition
3. Results
3.1. Validation of the Measurement of the Group of Healthy Volunteers
3.2. Post-COVID-19 Patients Measurement
3.3. Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vidal, M.; Turner, J.; Bulling, A.; Gellersen, H. Wearable eye tracking for mental health monitoring. Comput. Commun. 2012, 35, 1306–1311. [Google Scholar] [CrossRef]
- Larrazabal, A.J.; Garcia Cena, C.G.; Martínez, C.E. Video-oculography eye tracking towards clinical applications: A review. Comput. Biol. Med. 2019, 108, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Molitor, R.J.; Ko, P.C.; Ally, B.A. Eye movements in Alzheimer’s disease. J. Alzheimer’s Dis. 2015, 44, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noiret, N.; Carvalho, N.; Laurent, É.; Chopard, G.; Binetruy, M.; Nicolier, M.; Monnin, J.; Magnin, E.; Vandel, P. Saccadic eye movements and attentional control in Alzheimer’s disease. Arch. Clin. Neuropsychol. 2018, 33, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Wang, T.; Su, N.; Xiao, S.; Kapoula, Z. Specific saccade deficits in patients with Alzheimer’s disease at mild to moderate stage and in patients with amnestic mild cognitive impairment. Age 2013, 35, 1287–1298. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, L.D.; Pratt, J.; Levine, B.; Black, S.E. Antisaccades: A probe into the dorsolateral prefrontal cortex in Alzheimer’s disease. A critical review. J. Alzheimer’s Dis. 2010, 19, 781–793. [Google Scholar] [CrossRef] [Green Version]
- Crawford, T.J.; Higham, S.; Renvoize, T.; Patel, J.; Dale, M.; Suriya, A.; Tetley, S. Inhibitory control of saccadic eye movements and cognitive impairment in Alzheimer’s disease. Biol. Psychiatry 2005, 57, 1052–1060. [Google Scholar] [CrossRef]
- Pierrot-Deseilligny, C.; Milea, D.; Müri, R.M. Eye movement control by the cerebral cortex. Curr. Opin. Neurol. 2004, 17, 17–25. [Google Scholar] [CrossRef]
- Pretegiani, E.; Optican, L.M. Eye movements in Parkinson’s disease and inherited parkinsonian syndromes. Front. Neurol. 2017, 8, 592. [Google Scholar] [CrossRef]
- Fielding, J.; Kilpatrick, T.; Millist, L.; White, O. Antisaccade performance in patients with multiple sclerosis. Cortex 2009, 45, 900–903. [Google Scholar] [CrossRef]
- Fielding, J.; Kilpatrick, T.; Millist, L.; White, O. Multiple sclerosis: Cognition and saccadic eye movements. J. Neurol. Sci. 2009, 277, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Clough, M.; Millist, L.; Lizak, N.; Beh, S.; Frohman, T.C.; Frohman, E.M.; White, O.B.; Fielding, J. Ocular motor measures of cognitive dysfunction in multiple sclerosis I: Inhibitory control. J. Neurol. 2015, 262, 1130–1137. [Google Scholar] [CrossRef] [PubMed]
- Piccardi, L.; Noris, B.; Barbey, O.; Billard, A.; Schiavone, G.; Keller, F.; von Hofsten, C. Wearcam: A head mounted wireless camera for monitoring gaze attention and for the diagnosis of developmental disorders in young children. In Proceedings of the RO-MAN 2007-the 16th IEEE International Symposium on Robot and Human Interactive Communication, Jeju, Korea, 26–29 August 2007; pp. 594–598. [Google Scholar]
- Boraston, Z.; Blakemore, S.J. The application of eye-tracking technology in the study of autism. J. Physiol. 2007, 581, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Gorges, M.; Pinkhardt, E.H.; Kassubek, J. Alterations of eye movement control in neurodegenerative movement disorders. J. Ophthalmol. 2014, 2014, 658243. [Google Scholar] [CrossRef] [Green Version]
- Lage, C.; López-García, S.; Bejanin, A.; Kazimierczak, M.; Aracil-Bolaños, I.; Calvo-Córdoba, A.; Pozueta, A.; García-Martínez, M.; Fernández-Rodríguez, A.; Bravo-González, M.; et al. Distinctive Oculomotor Behaviors in Alzheimer’s Disease and Frontotemporal Dementia. Front. Aging Neurosci. 2021, 12, 525. [Google Scholar] [CrossRef]
- Shakespeare, T.J.; Kaski, D.; Yong, K.X.; Paterson, R.W.; Slattery, C.F.; Ryan, N.S.; Schott, J.M.; Crutch, S.J. Abnormalities of fixation, saccade and pursuit in posterior cortical atrophy. Brain 2015, 138, 1976–1991. [Google Scholar] [CrossRef]
- Ahmad, I.; Rathore, F.A. Neurological manifestations and complications of COVID-19: A literature review. J. Clin. Neurosci. 2020, 77, 8–12. [Google Scholar] [CrossRef]
- Alonso-Lana, S.; Marquié, M.; Ruiz, A.; Boada, M. Cognitive and neuropsychiatric manifestations of COVID-19 and effects on elderly individuals with dementia. Front. Aging Neurosci. 2020, 12, 369. [Google Scholar] [CrossRef]
- Li, Y.C.; Bai, W.Z.; Hashikawa, T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J. Med. Virol. 2020, 92, 552–555. [Google Scholar] [CrossRef]
- Roy, D.; Ghosh, R.; Dubey, S.; Dubey, M.J.; Benito-Leon, J.; Ray, B.K. Neurological and neuropsychiatric impacts of COVID-19 pandemic. Can. J. Neurol. Sci. 2021, 48, 9–24. [Google Scholar] [CrossRef]
- Ghosh, R.; Biswas, U.; Roy, D.; Pandit, A.; Lahiri, D.; Ray, B.K.; Benito-León, J. De novo movement disorders and COVID-19: Exploring the Interface. Mov. Disord. Clin. Pract. 2021, 8, 669–680. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Mahalakshmi, A.M.; Ray, B.; Tuladhar, S.; Bhat, A.; Paneyala, S.; Patteswari, D.; Sakharkar, M.K.; Hamdan, H.; Ojcius, D.M.; Bolla, S.R.; et al. Does COVID-19 contribute to development of neurological disease? Immun. Inflamm. Dis. 2021, 9, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Onaolapo, A.; Onaolapo, O. COVID-19, the Brain, and the Future: Is Infection by the Novel Coronavirus a Harbinger of Neurodegeneration? CNS & Neurol. Disord. Drug Targets. Available online: https://www.eurekaselect.com/article/119626 (accessed on 5 January 2022). [CrossRef]
- Pinna, P.; Grewal, P.; Hall, J.P.; Tavarez, T.; Dafer, R.M.; Garg, R.; Osteraas, N.D.; Pellack, D.R.; Asthana, A.; Fegan, K.; et al. Neurological manifestations and COVID-19: Experiences from a tertiary care center at the frontline. J. Neurol. Sci. 2020, 415, 116969. [Google Scholar] [CrossRef] [PubMed]
- Varatharaj, A.; Thomas, N.; Ellul, M.A.; Davies, N.W.; Pollak, T.A.; Tenorio, E.L.; Sultan, M.; Easton, A.; Breen, G.; Zandi, M.; et al. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: A UK-wide surveillance study. Lancet Psychiatry 2020, 7, 875–882. [Google Scholar] [CrossRef]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic features in severe SARS-CoV-2 infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef]
- Chaumont, H.; San-Galli, A.; Martino, F.; Couratier, C.; Joguet, G.; Carles, M.; Roze, E.; Lannuzel, A. Mixed central and peripheral nervous system disorders in severe SARS-CoV-2 infection. J. Neurol. 2020, 267, 3121–3127. [Google Scholar] [CrossRef]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2021, 21, 703–709. [Google Scholar] [CrossRef]
- Findlay, J.M.; Walker, R. A model of saccade generation based on parallel processing and competitive inhibition. Behav. Brain Sci. 1999, 22, 661–674. [Google Scholar] [CrossRef]
- Leigh, J.; Zee, D.S. The Neurology of Eye Movements; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Pupil Labs. Getting Started—Hardware. Available online: https://docs.pupil-labs.com/core/hardware/ (accessed on 28 February 2021).
- Pupil Labs. Pupil Core—Tech Specs. Available online: https://pupil-labs.com/products/core/tech-specs/ (accessed on 1 March 2021).
- PsychoPy. PsychoPy—Now Running Studies Online. Available online: https://www.psychopy.org/ (accessed on 7 March 2021).
- Peirce, J.; Gray, J.R.; Simpson, S.; MacAskill, M.; Höchenberger, R.; Sogo, H.; Kastman, E.; Lindeløv, J.K. PsychoPy2: Experiments in behavior made easy. Behav. Res. Methods 2019, 51, 195–203. [Google Scholar] [CrossRef] [Green Version]
- Mosimann, U.; Müri, R.; Burn, D.; Felblinger, J.; O’Brien, J.; McKeith, I. Saccadic eye movement changes in Parkinson’s disease dementia and dementia with Lewy bodies. Brain 2005, 128, 1267–1276. [Google Scholar] [CrossRef] [Green Version]
- Jehangir, N.; Yu, C.Y.; Song, J.; Shariati, M.A.; Binder, S.; Beyer, J.; Santini, V.; Poston, K.; Liao, Y.J. Slower saccadic reading in Parkinson’s disease. PLoS ONE 2018, 13, e0191005. [Google Scholar]
- Antoniades, C.; Ettinger, U.; Gaymard, B.; Gilchrist, I.; Kristjánsson, A.; Kennard, C.; John-Leigh, R.; Noorani, I.; Pouget, P.; Smyrnis, N.; et al. An internationally standardised antisaccade protocol. Vis. Res. 2013, 84, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacAskill, M.; Anderson, T. Eye movements in neurodegenerative diseases. J. Neuro-Ophthalmol. Neuro-Otol. 2016, 29, 61–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, T.J.; Smith, E.S.; Berry, D.M. Eye gaze and aging: Selective and combined effects of working memory and inhibitory control. Front. Hum. Neurosci. 2017, 11, 563–573. [Google Scholar] [CrossRef] [Green Version]
- Larrazabal, A.J.; Garcia Cena, C.E.; Martínez, C.E. Eye corners tracking for head movement estimation. In Proceedings of the IEEE International Work Conference on Bioinspired Intelligence (IWOBI 2019), Budapest, Hungary, 3–5 July 2019; pp. 1–5. [Google Scholar]
- Garcia Cena, C.E.; Gomez Andres, D.; Pulido Valdeolivas, I. Measurement and Analysis of Eye Movements Performance to Predict Healthy Brain Aging. IEEE Access 2020, 8, 87201–87213. [Google Scholar] [CrossRef]
- Garcia Cena, C.E.; Gómez Andrés, D.; Pulido Valdeoliva, I.; Acebrón López, R.; Espinoza Gómez, R.; Ramos Vázquez, S. Device for Synchronized Measure of Ocular and Cephalic Movements. European Patent Nº EP3241488A1, 8 November 2017. [Google Scholar]
- Hernández, E.; Hernández, S.; Molina, D.; Acebrón, R.; García Cena, C.E. OSCANN: Technical characterization of a novel gaze tracking analyzer. Sensors 2018, 18, 522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulke, L.; Atkinson, J.; Braddick, O. Automatic Detection of Attention Shifts in Infancy: Eye Tracking in the Fixation Shift Paradigm. PLoS ONE 2015, 10, e0142505. [Google Scholar] [CrossRef] [PubMed]
- Kano, F.; Hirata, S.; Call, J.; Tomonaga, M. The visual strategy specific to humans among hominids: A study using the gap–overlap paradigm. Vis. Res. 2011, 51, 2348–2355. [Google Scholar] [CrossRef] [Green Version]
- FKalesnykas, R.P.; Hallett, P.E. The differentiation of visually guided and anticipatory saccades in gap and overlap paradigms. Exp. Brain Res. 1987, 68, 115–121. [Google Scholar]
- Özyurt, J.; Greenlee, M.W. Neural correlates of inter- and intra-individual saccadic reaction time differences in the gap/overlap paradigm. J. Neurophysiol. 2011, 105, 2438–2447. [Google Scholar] [CrossRef] [PubMed]
- Bucci, M.P.; Pouvreau, N.; Yang, Q.; Kapoula, Z. Influence of gap and overlap paradigms on saccade latencies and vergence eye movements in seven-year-old children. Exp. Brain Res. 2005, 164, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Takagi, M.; Frohman, E.M.; Zee, D.S. Gap-overlap effects on latencies of saccades, vergence and combined vergence-saccades in humans. Vis. Re Res. 1995, 35, 3373–3388. [Google Scholar] [CrossRef] [Green Version]
- Chehrehnegar, N.; Nejati, V.; Shati, M.; Esmaeili, M.; Rezvani, Z.; Haghi, M.; Foroughan, M. Behavioral and cognitive markers of mild cognitive impairment: Diagnostic value of saccadic eye movements and Simon task. Aging Clin. Exp. Res. 2019, 31, 1591–1600. [Google Scholar] [CrossRef]
- Polden, M.; Wilcockson, T.D.; Crawford, T.J. The disengagement of visual attention: An eye-tracking study of cognitive impairment, ethnicity and age. Brain Sci. 2020, 10, 461. [Google Scholar] [CrossRef]
- de Freitas Pereira, M.L.G.; de Arruda Camargo, M.v.Z.; Bellan, A.F.R.; Tahira, A.C.; Dos Santos, B.; Dos Santos, J.; Machado-Lima, A.; Nunes, F.L.; Forlenza, O.V. Visual Search Efficiency in Mild Cognitive Impairment and Alzheimer’s Disease: An Eye Movement Study. J. Alzheimer’s Dis. 2020, 75, 261–275. [Google Scholar] [CrossRef]
- Jin, Z.; Reeves, A. Attentional release in the saccadic gap effect. Vis. Res. 2009, 49, 2045–2055. [Google Scholar] [CrossRef] [Green Version]
- Pratt, J.; Lajonchere, C.M.; Abrams, R.A. Attentional modulation of the gap effect. Vis. Res. 2006, 46, 2602–2607. [Google Scholar] [CrossRef] [Green Version]
- Matsuo, Y.; Watanabe, M.; Taniike, M.; Mohri, I.; Kobashi, S.; Tachibana, M.; Kobayashi, Y.; Kitamura, Y. Gap effect abnormalities during a visually guided pro-saccade task in children with attention deficit hyperactivity disorder. PLoS ONE 2015, 10, e0125573. [Google Scholar] [CrossRef]
- Crawford, T.J.; Higham, S.; Mayes, J.; Dale, M.; Shaunak, S.; Lekwuwa, G. The role of working memory and attentional disengagement on inhibitory control: Effects of aging and Alzheimer’s disease. Age 2013, 35, 1637–1650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, E.H.; Myles, J.B.; Tan, E.J.; Neill, E.; Carruthers, S.P.; Sumner, P.J.; Bozaoglu, K.; Gurvich, C. Working memory and attention influence antisaccade error rate in schizophrenia. J. Int. Neuropsychol. Soc. JINS 2019, 25, 174–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schut, M.J.; Van der Stoep, N.; Postma, A.; Van der Stigchel, S. The cost of making an eye movement: A direct link between visual working memory and saccade execution. J. Vis. 2017, 17, 15–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epelboim, J.; Suppes, P. A model of eye movements and visual working memory during problem solving in geometry. Vis. Res. 2001, 41, 1561–1574. [Google Scholar] [CrossRef] [Green Version]
- Wenban-Smith, M.G.; Findlay, J.M. Express saccades: Is there a separate population in humans? Exp. Brain Res. 1991, 87, 218–222. [Google Scholar] [CrossRef]
- Koller, K.; Rafal, R.D. Saccade latency bias toward temporal hemifield: Evidence for role of retinotectal tract in mediating reflexive saccades. Neuropsychologia 2019, 128, 276–281. [Google Scholar] [CrossRef]
- White, B.J.; Munoz, D.P. The Superior Colliculus; Oxf. Handb. Eye Movements; Oxford University Press: New York, NY, USA, 2011. [Google Scholar]
- Reuter, B.; Kathmann, N. Using saccade tasks as a tool to analyze executive dysfunctions in schizophrenia. Acta Psychol. 2004, 115, 255–269. [Google Scholar] [CrossRef]
- Hutton, S.; Ettinger, U. The antisaccade task as a research tool in psychopathology: A critical review. Psychophysiology 2002, 43, 302–313. [Google Scholar] [CrossRef] [Green Version]
- Ettinger, U.; Kumari, V.; Crawford, T.J.; Corr, P.J.; Das, M.; Zachariah, E.; Hughes, C.; Sumich, A.L.; Rabe-Hesketh, S.; Sharma, T. Smooth pursuit and antisaccade eye movements in siblings discordant for schizophrenia. J. Psychiatr. Res. 2004, 38, 177–184. [Google Scholar] [CrossRef]
- Smyrnis, N.; Evdokimidis, I.; Stefanis, N.; Constantinidis, T.; Avramopoulos, D.; Theleritis, C.; Paximadis, C.; Efstratiadis, C.; Kastrinakis, G.; Stefanis, C. The antisaccade task in a sample of 2.006 young males. Effects of task parameters. Exp. Brain Res. 2002, 147, 53–63. [Google Scholar]
- Jóhannesson, Ó.I.; Tagu, J.; Kristjánsson, Á. Asymmetries of the visual system and their influence on visual performance and oculomotor dynamics. Eur. J. Neurosci. 2018, 48, 3426–3445. [Google Scholar] [CrossRef] [PubMed]
- Bargary, G.; Bosten, J.M.; Goodbourn, P.T.; Lawrance-Owen, A.J.; Hogg, R.E.; Mollon, J. Individual differences in human eye movements: An oculomotor signature? Vis. Res. 2017, 141, 157–169. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, U.; Antonova, E.; Crawford, T.J.; Mitterschiffthaler, M.T.; Goswani, S.; Sharma, T.; Kumari, V. Structural neural correlates of prosaccade and antisaccade eye movements in healthy humans. NeuroImage 2005, 24, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Jernajczyk, W.; Sobańska, A.; Czerwosz, L.; Szatkowska, E. The influence of age and gender on the latency of eye movement in healthy humans. J. Physiol. Pharmacol. 2005, 56, 93–100. [Google Scholar] [PubMed]
- Lai, H.Y.; Saavedra-Peña, G.; Sodini, C.G.; Sze, V.; Heldt, T. Measuring Saccade Latency Using Smartphone Cameras. IEEE J. Biomed. Health Inform. 2020, 24, 885–897. [Google Scholar] [CrossRef]
- Israël, I. Memory-guided saccades: What is memorized? Exp. Brain Res. 1992, 90, 221–224. [Google Scholar] [CrossRef]
- Brown, M.; DeSouza, J.; Goltz, H.C.; Ford, K.; Menon, R.S.; Goodale, M.A.; Everling, S. Comparison of Memory- and Visually Guided Saccades Using Event-Related fMRI. J. Neurophysiol. 2004, 91, 873–889. [Google Scholar] [CrossRef] [Green Version]
- Bonnet, C.; Hanuška, J.; Rusz, J.; Rivaud-Péchoux, S.; Sieger, T.; Majerová, V.; Serranová, T.; Gaymard, B.; Růžička, E. Horizontal and vertical eye movement metrics: What is important? Clin. Neurophysiol. 2013, 124, 2216–2229. [Google Scholar] [CrossRef]
- Azri, M.; Young, S.; Lin, H.; Tan, C.; Yang, Z. Diagnosis of Ocular Myasthenia Gravis by means of tracking eye parameters. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 1460–1464. [Google Scholar]
- Tagu, J.; Doré-Mazars, K.; Vergne, J.; Lemoine-Lardennois, C.; Vergilino-Perez, D. Recentering bias for temporal saccades only: Evidence from binocular recordings of eye movements. J. Vis. 2018, 18, 10. [Google Scholar] [CrossRef] [Green Version]
- Pierrot-Deseilligny, C.H.; Müri, R.M.; Nyffeler, T.; Milea, D. The role of the human dorsolateral prefrontal cortex in ocular motor behavior. Ann. N. Y. Acad. Sci. 2005, 1039, 239–521. [Google Scholar] [CrossRef]
- Pierrot-Deseilligny, C.; Müri, R.M.; Rivaud-Pechoux, S.; Gaymard, B.; Ploner, C.J. Cortical control of spatial memory in humans: The visuooculomotor model. Ann. Neurol. 2002, 52, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Ouerfelli-Ethier, J.; Salemme, R.; Fournet, R.; Urquizar, C.; Pisella, L.; Khan, A.Z. Impaired Spatial Inhibition Processes for Interhemispheric Anti-saccades following Dorsal Posterior Parietal Lesions. Cereb Cortex Commun. 2021, 2, tgab054. [Google Scholar] [CrossRef] [PubMed]
- Johnston, K.; Everling, S. Neurophysiology and neuroanatomy of reflexive and voluntary saccades in non-human primates. NeuroImage 2008, 68, 271–283. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Age (Range) | Sex | Cardiovascular Diseases | Diabetes Mellitus |
|---|---|---|---|---|
| H1 | 51–60 | Female | Arterial hypertension | No |
| H2 | <19 | Male | Arrhythmia | No |
| H3 | <19 | Male | None | No |
| H4 | 20–40 | Male | None | No |
| H5 | 20–40 | Male | None | No |
| H6 | 20–40 | Male | None | No |
| H7 | 20–40 | Female | None | No |
| H8 | 20–40 | Male | None | No |
| H9 | 41–50 | Male | None | No |
| Patient | Age | Sex | Laboral Activity | Cardiovascular Diseases | Diabetes Mellitus |
|---|---|---|---|---|---|
| VAMA01 | 59 | Female | Association coordinator | None | Yes |
| VAMA02 | 54 | Male | Commercial tasks | Supraventricular arrythmia (14y) | No |
| VAMA03 | 28 | Female | Housewife | None | No |
| VAMA04 | 44 | Female | Housewife | None | No |
| VAMA05 | 60 | Male | Caretaker and maintenance in a school | None | No |
| VAMA06 | 49 | Female | Cleaner | None | No |
| VAMA08 | 46 | Female | Call center | None | No |
| VAMA09 | 54 | Male | Worker | None | No |
| VAMA10 | 52 | Female | Call center | None | No |
| Patient | Diagnosis Date (mm/dd/yyyy) | Diarrhea | Pneumonia | Fever | Cough | Headache | Gastrointestinal Symptoms |
|---|---|---|---|---|---|---|---|
| VAMA01 | 04/04/2020 | X | X | X | - | - | - |
| VAMA02 | 03/03/2020 | - | X | X | X | - | - |
| VAMA03 | 08/28/2020 | X | - | X | - | X | X |
| VAMA04 | 12/17/2020 | - | X | X | X | X | Anorexia |
| VAMA05 | 09/03/2020 | - | X (bilateral) | X | X | - | Anorexia |
| VAMA06 | 12/29/2020 | - | - | X | X | - | - |
| VAMA08 | 12/29/2020 | - | - | X | - | X | - |
| VAMA09 | 12/02/2020 | - | Mild | Low-grade | - | - | - |
| VAMA10 | 03/15/2020 | X | - | - | X | X | X |
| Patient | Anosmia | Memory Complaints | Fatigue | Shortness of Breath |
|---|---|---|---|---|
| VAMA01 | X | X | X | - |
| VAMA02 | - | - | X | X |
| VAMA03 | - | X | - | X |
| VAMA04 | X | X | X | - |
| VAMA05 | - | - | X | X (on walking) |
| VAMA06 | - | X | X | - |
| VAMA08 | X | X | X | - |
| VAMA09 | - | X | X | X |
| VAMA10 | - | X | X | X (feeling of chest pressure) |
| ID | Blinks | [s] – | ± SD | ± SD | ||
|---|---|---|---|---|---|---|
| H1 | 0 | 0.198–0.272 | 0.223 ± 0.02 | 0.219 | 0.213 ± 0.02 | 0.214 |
| H2 | 3 | 0.132–0.451 | 0.212 ± 0.09 | 0.197 | 0.148 ± 0.02 | 0.178 |
| H3 | 0 | 0.151–0.383 | 0.212 ± 0.06 | 0.197 | 0.202 ± 0.06 | 0.178 |
| H4 | 4 | 0.156–0.280 | 0.198 ± 0.03 | 0.200 | 0.216 ± 0.03 | 0.183 |
| H5 | 0 | 0.154–0.267 | 0.192 ± 0.03 | 0.202 | 0.189 ± 0.03 | 0.184 |
| H6 | 2 | 0.132–0.239 | 0.181 ± 0.03 | 0.199 | 0.162 ± 0.05 | 0.180 |
| H7 | 8 | 0.151–0.269 | 0.180 ± 0.03 | 0.201 | 0.203 ± 0.07 | 0.185 |
| H8 | 0 | 0.137–0.233 | 0.176 ± 0.03 | 0.203 | 0.172 ± 0.02 | 0.188 |
| H9 | 3 | 0.214–0.338 | 0.297 ± 0.06 | 0.211 | 0.208 ± 0.02 | 0.200 |
| Mean Values | 2.2 | 0.158–0.303 | 0.209 ± 0.04 | 0.203 | 0.190 ± 0.03 | 0.187 |
| ID | Blinks | Success Rate |
|---|---|---|
| H1 | 3 | 100% |
| H2 | 12 | 100% |
| H3 | 0 | 100% |
| H4 | 2 | 100% |
| H5 | 0 | 90% |
| H6 | 2 | 100% |
| H7 | 21 | 90% |
| H8 | 4 | 100% |
| H9 | 3 | 100% |
| Mean Values | 5.2 | 97.77% |
| ID | Blinks | Correct | Reflexive | Success Rate | Latency [s] Min–Max | Mean ± SD |
|---|---|---|---|---|---|---|
| H1 | 2 | 100% | 37.5% | 62.5% | 0.160–0.659 | 0.316 ± 0.135 |
| H2 | 8 | 100% | 50% | 50% | 0.197–0.511 | 0.330 ± 0.092 |
| H3 | 0 | 100% | 60% | 40% | 0.219–0.612 | 0.336 ± 0.103 |
| H4 | 0 | 100% | 60% | 40% | 0.210–0.463 | 0.317 ± 0.078 |
| H5 | 1 | 80% | 40% | 40% | 0.216–0.679 | 0.396 ± 0.135 |
| H6 | 3 | 100% | 0% | 100% | 0.162–0.449 | 0.232 ± 0.079 |
| H7 | 0 | 70% | 40% | 30% | 0.122–0.672 | 0.368 ± 0.140 |
| H8 | 0 | 100% | 60% | 60% | 0.180–0.469 | 0.273 ± 0.092 |
| H9 | 1 | 100% | 50% | 50% | 0.197–0.398 | 0.315 ± 0.044 |
| Mean Values | 1.6 | 94.4% | 44.2% | 52.5% | 0.184–0.545 | 0.320 ± 0.099 |
| Patient | Blinks | [s] – | ± SD | ± SD |
|---|---|---|---|---|
| VAMA01 | 2 | 0.162–0.327 | 0.216 ± 0.04 | 0.200 ± 0.02 |
| VAMA02 | 0 | 0.168–0.741 | 0.264 ± 0.16 | 0.255 ± 0.07 |
| VAMA03 | 0 | 0.177–0.361 | 0.248 ± 0.05 | 0.223 ± 0.03 |
| VAMA04 | 9 | 0.182–0.342 | 0.233 ± 0.05 | 0.214 ± 0.05 |
| VAMA05 | 6 | 0.168–0.330 | 0.234 ± 0.05 | 0.212 ± 0.05 |
| VAMA06 | 54 | 0.170–0.274 | 0.210 ± 0.03 | 0.213 ± 0.01 |
| VAMA08 | 11 | 0.167–0.302 | 0.226 ± 0.04 | 0.214± 0.04 |
| VAMA09 | 22 | 0.164–0.255 | 0.216 ± 0.03 | 0.223 ± 0.03 |
| VAMA10 | 3 | 0.214–0.712 | 0.496 ± 0.16 | 0.433 ± 0.15 |
| Mean Values | 11.8 | 0.174–0.404 | 0.260 ± 0.07 | 0.243 ± 0.05 |
| Patient | Blinks | Success Rate |
|---|---|---|
| VAMA01 | 18 | 100% |
| VAMA02 | 0 | 80% |
| VAMA03 | 2 | 100% |
| VAMA04 | 18 | 100% |
| VAMA05 | 22 | 40% |
| VAMA06 | 53 | 0% |
| VAMA08 | 56 | 100% |
| VAMA09 | 20 | 100% |
| VAMA10 | 7 | 20% |
| Mean Values | 21.7 | 71.1% |
| Patient | Blinks | Correct | Reflexive | Success Rate | Latency [sec] Min–Max | Mean ± SD |
|---|---|---|---|---|---|---|
| VAMA01 | 9 | 100% | 10% | 90% | 0.227–0.630 | 0.438 ± 0.112 |
| VAMA02 | 1 | 60% | 100% | 0% | 0.177–0.737 | 0.472 ± 0.184 |
| VAMA03 | 0 | 100% | 90% | 10% | 0.272–0.934 | 0.417 ± 0.149 |
| VAMA04 | 5 | 100% | 60% | 40% | 0.240–0.831 | 0.432 ± 0.137 |
| VAMA05 | 4 | 100% | 40% | 60% | 0.219–0.860 | 0.333 ± 0.157 |
| VAMA06 | 34 | 70% | 40% | 30% | 0.227–1.499 | 0.461 ± 0.326 |
| VAMA08 | 26 | 90% | 30% | 60% | 0.257–0.574 | 0.358 ± 0.081 |
| VAMA09 | 27 | 90% | 70% | 20% | 0.246–0.888 | 0.468 ± 0.182 |
| VAMA10 | 7 | 80% | 60% | 20% | 0.275–0.948 | 0.499 ± 0.183 |
| Mean Values | 12.5 | 87.8% | 55.5% | 36.6% | 0.237–0.878 | 0.430 ± 0.167 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García Cena, C.; Costa, M.C.; Saltarén Pazmiño, R.; Santos, C.P.; Gómez-Andrés, D.; Benito-León, J. Eye Movement Alterations in Post-COVID-19 Condition: A Proof-of-Concept Study. Sensors 2022, 22, 1481. https://doi.org/10.3390/s22041481
García Cena C, Costa MC, Saltarén Pazmiño R, Santos CP, Gómez-Andrés D, Benito-León J. Eye Movement Alterations in Post-COVID-19 Condition: A Proof-of-Concept Study. Sensors. 2022; 22(4):1481. https://doi.org/10.3390/s22041481
Chicago/Turabian StyleGarcía Cena, Cecilia, Mariana Campos Costa, Roque Saltarén Pazmiño, Cristina Peixoto Santos, David Gómez-Andrés, and Julián Benito-León. 2022. "Eye Movement Alterations in Post-COVID-19 Condition: A Proof-of-Concept Study" Sensors 22, no. 4: 1481. https://doi.org/10.3390/s22041481
APA StyleGarcía Cena, C., Costa, M. C., Saltarén Pazmiño, R., Santos, C. P., Gómez-Andrés, D., & Benito-León, J. (2022). Eye Movement Alterations in Post-COVID-19 Condition: A Proof-of-Concept Study. Sensors, 22(4), 1481. https://doi.org/10.3390/s22041481