
A RULA-Based Comparison of the Ergonomic Risk of Typical Working Procedures for Dentists and Dental Assistants of General Dentistry, Endodontology, Oral and Maxillofacial Surgery, and Orthodontics

 ,
, 
 ,
, 


Abstract
:1. Background
2. Materials and Methods
2.1. Subjects
2.2. Dental Tasks
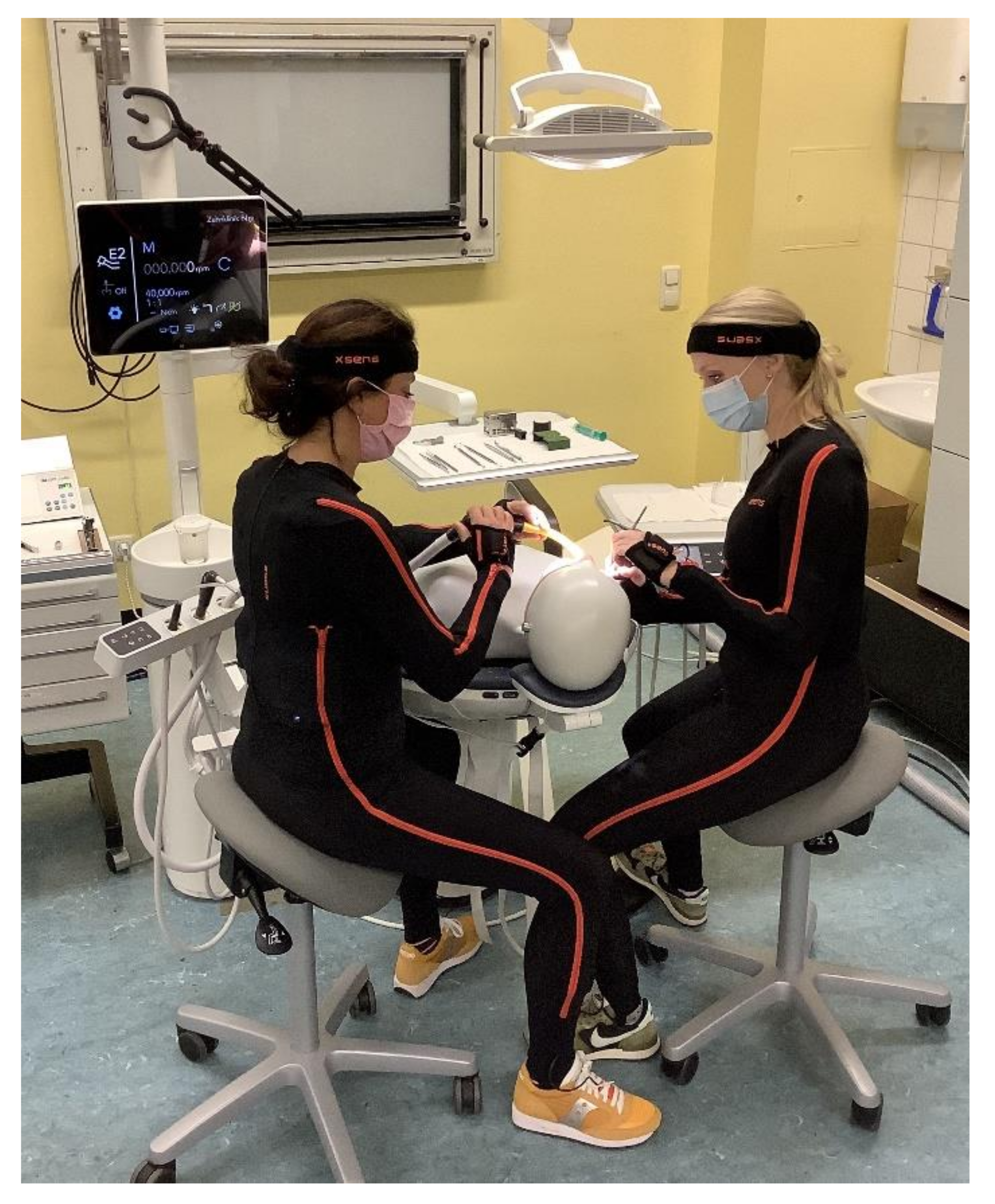
2.3. Measurement System
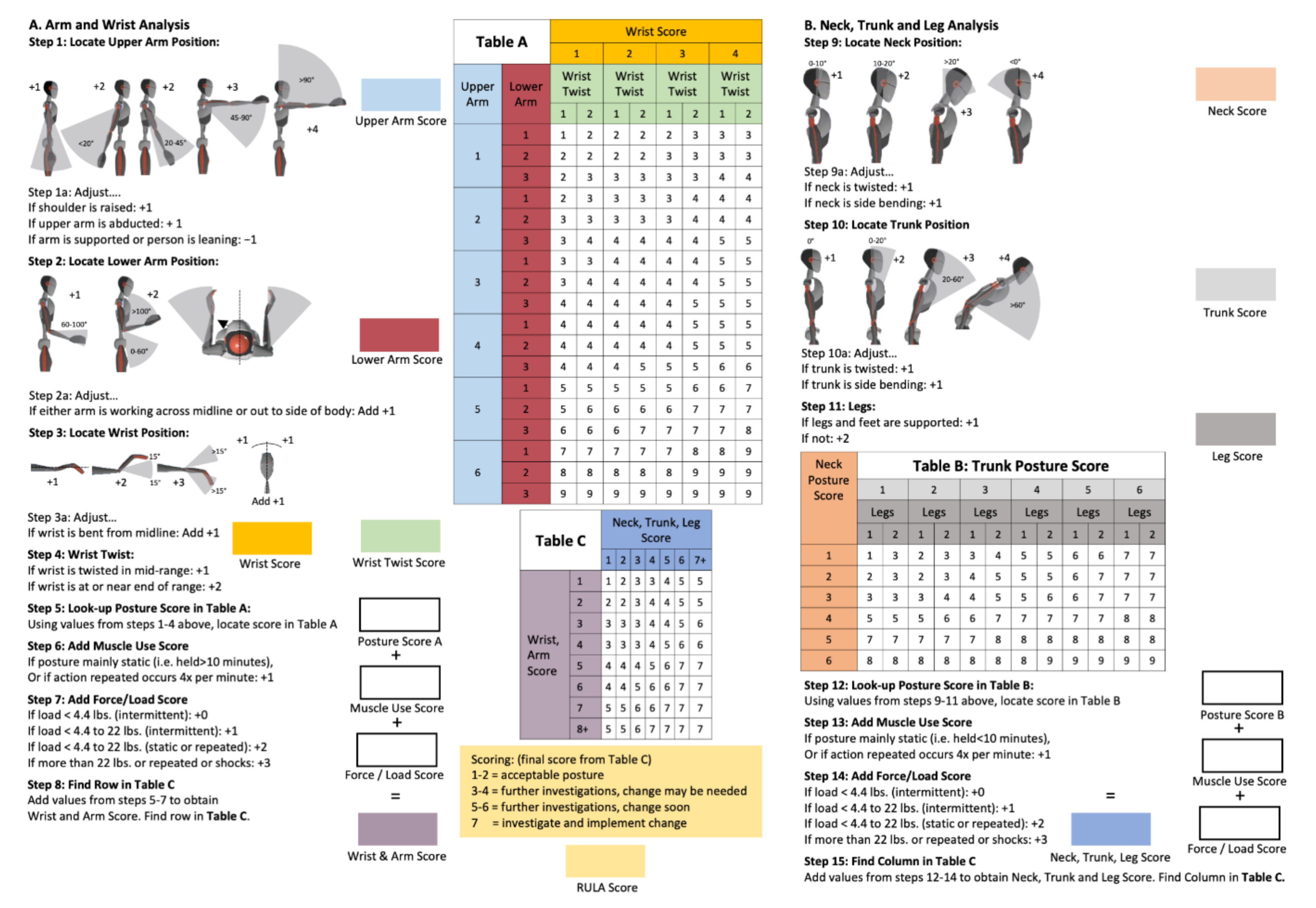
2.4. Rapid Upper Limb Assessment (RULA)
2.5. Measurement Protocol
2.6. Data Analysis
- median + interquartile distance (IQD)
- relative average risk score over the time (Rel. av. RST)
- ergonomic risk potential (ERP)
- 1.
- Neck Score - RULA Step 9
- 2.
- Trunk Score - RULA Step 10
- 3.
- Upper Arm Score (left and right) - RULA Step 1
- 4.
- Lower Arm Score (left and right) - RULA Step 2
- 5.
- Wrist Score (left and right) - RULA Steps 3 + 4
3. Statistical Analysis
4. Results
4.1. Differences between the Fields of Dental Specialization
4.2. Dental Assistants
4.3. Dentists
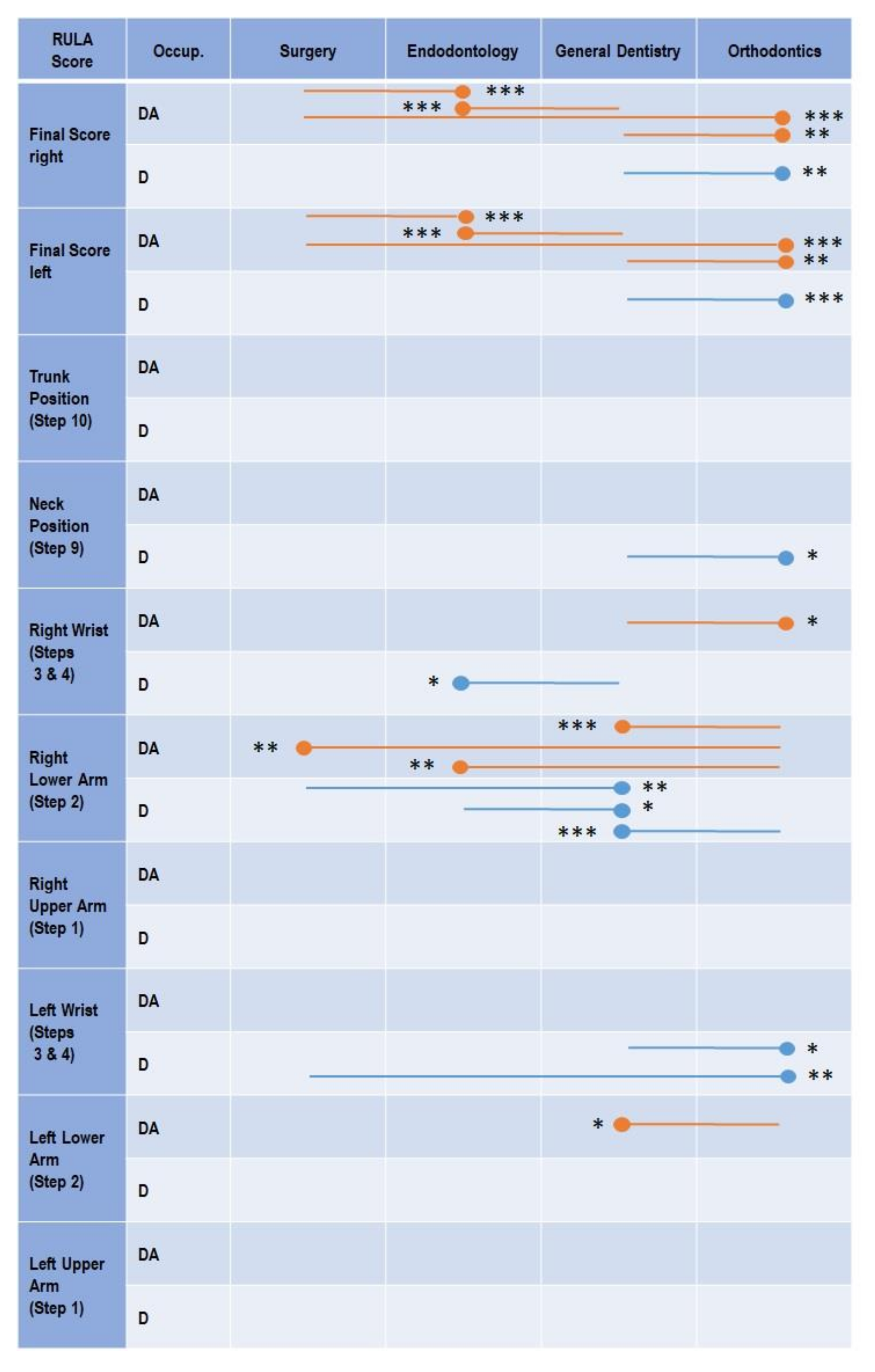
4.4. Differences in the Ergonomic Risk between Dentists and Dental Assistants According to Their Field of Dental Specialization
4.5. Oral and Maxillofacial Surgery
4.6. Endodontology
4.7. General Dentistry
4.8. Orthodontics
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lietz, J.; Kozak, A.; Nienhaus, A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: A systematic literature review and meta-analysis. PLoS ONE 2018, 13, e0208628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, M.; Cockrell, D.; Smith, D.R. A systematic review of musculoskeletal disorders among dental professionals. Int. J. Dent. Hyg. 2009, 7, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.; Zamparini, F.; Spinelli, A.; Risi, A.; Prati, C. Musculoskeletal Disorders among Italian Dentists and Dental Hygienists. Int. J. Environ. Res. Public Health 2021, 18, 2705. [Google Scholar] [CrossRef]
- Ohlendorf, D.; Haas, Y.; Naser, A.; Haenel, J.; Maltry, L.; Holzgreve, F.; Erbe, C.; Betz, W.; Wanke, E.M.; Brüggmann, D.; et al. Prevalence of Muscular Skeletal Disorders among Qualified Dental Assistants. Int. J. Environ. Res. Public Health 2020, 17, 3490. [Google Scholar] [CrossRef] [PubMed]
- Ohlendorf, D.; Naser, A.; Haas, Y.; Haenel, J.; Fraeulin, L.; Holzgreve, F.; Erbe, C.; Betz, W.; Wanke, E.M.; Brueggmann, D.; et al. Prevalence of Musculoskeletal Disorders among Dentists and Dental Students in Germany. Int. J. Environ. Res. Public Health 2020, 17, 8740. [Google Scholar] [CrossRef] [PubMed]
- Ohlendorf, D.; Maltry, L.; Hänel, J.; Betz, W.; Erbe, C.; Maurer-Grubinger, C.; Holzgreve, F.; Wanke, E.M.; Brüggmann, D.; Nienhaus, A.; et al. SOPEZ: Study for the optimization of ergonomics in the dental practice-musculoskeletal disorders in dentists and dental assistants: A study protocol. J. Occup. Med. Toxicol. 2020, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Marklin, R.W.; Cherney, K. Working postures of dentists and dental hygienists. J. Calif. Dent. Assoc. 2005, 33, 133–136. [Google Scholar] [PubMed]
- Ohlendorf, D.; Erbe, C.; Hauck, I.; Nowak, J.; Hermanns, I.; Ditchen, D.; Ellegast, R.; Groneberg, D.A. Restricted posture in dentistry—A kinematic analysis of orthodontists. BMC Musculoskelet. Disord. 2017, 18, 275. [Google Scholar] [CrossRef] [Green Version]
- Morse, T.; Bruneau, H.; Dussetschleger, J. Musculoskeletal disorders of the neck and shoulder in the dental professions. Work 2010, 35, 419–429. [Google Scholar] [CrossRef]
- Ohlendorf, D.; Erbe, C.; Nowak, J.; Hauck, I.; Hermanns, I.; Ditchen, D.; Ellegast, R.; Groneberg, D.A. Constrained posture in dentistry—A kinematic analysis of dentists. BMC Musculoskelet. Disord. 2017, 18, 291. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.; Bhat, M.; Mohammed, T.; Bansal, N.; Gupta, G. Ergonomics in dentistry. Int. J. Clin. Pediatr. Dent. 2014, 7, 30. [Google Scholar] [CrossRef]
- Sakzewski, L.; Naser-Ud-Din, S. Work-related musculoskeletal disorders in dentists and orthodontists: A review of the literature. Work 2014, 48, 37–45. [Google Scholar] [CrossRef]
- Ohlendorf, D.; Fraeulin, L.; Haenel, J.; Betz, W.; Erbe, C.; Holzgreve, F.; Wanke, E.M.; Brueggmann, D.; Nienhaus, A.; Maurer-Grubinger, C.; et al. Ergonomic Comparison of Four Dental Workplace Concepts Using Inertial Motion Capture for Dentists and Dental Assistants. Int. J. Environ. Res. Public Health 2021, 18, 10453. [Google Scholar] [CrossRef]
- Alexopoulos, E.C.; Stathi, I.-C.; Charizani, F. Prevalence of musculoskeletal disorders in dentists. BMC Musculoskelet. Disord. 2004, 5, 16. [Google Scholar] [CrossRef] [Green Version]
- Alnaser, M.Z.; Almaqsied, A.M.; Alshatti, S.A. Risk factors for work-related musculoskeletal disorders of dentists in Kuwait and the impact on health and economic status. Work 2021, 68, 213–221. [Google Scholar] [CrossRef]
- Brown, J.; Burke, F.J.T.; Macdonald, E.B.; Gilmour, H.; Hill, K.B.; Morris, A.J.; White, D.A.; Muirhead, E.K.; Murray, K. Dental practitioners and ill health retirement: Causes, outcomes and re-employment. Br. Dent. J. 2010, 209, E7. [Google Scholar] [CrossRef]
- Dajpratham, P.; Ploypetch, T.; Kiattavorncharoen, S.; Boonsiriseth, K. Prevalence and associated factors of musculoskeletal pain among the dental personnel in a dental school. J. Med. Assoc. Thail. = Chotmaihet Thangphaet 2010, 93, 714–721. [Google Scholar]
- Finsen, L.; Christensen, H.; Bakke, M. Musculoskeletal disorders among dentists and variation in dental work. Appl. Ergon. 1998, 29, 119–125. [Google Scholar] [CrossRef]
- Harris, M.L.; Sentner, S.M.; Doucette, H.J.; Brillant, M.G.S. Musculoskeletal disorders among dental hygienists in Canada. Can. J. Dent. Hyg. 2020, 54, 61–67. [Google Scholar]
- Lalumandier, J.A.; McPhee, S.D.; Parrott, C.B.; Vendemia, M. Musculoskeletal pain: Prevalence, prevention, and differences among dental office personnel. Gen. Dent. 2001, 49, 160–166. [Google Scholar]
- Leggat, P.; Kedjarune, U.; Smith, D. Occupational Health Problems in Modern Dentistry: A Review. Ind. Health 2007, 45, 611–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netanely, S.; Luria, S.; Langer, D. Musculoskeletal disorders among dental hygienist and students of dental hygiene. Int. J. Dent. Hyg. 2020, 18, 210–216. [Google Scholar] [CrossRef]
- Puriene, A.; Janulyte, V.; Musteikyte, M.; Bendinskaite, R. General health of dentists. Literature review. Stomatologija 2007, 9, 10–20. [Google Scholar] [PubMed]
- Radanović, B.; Vučinić, P.; Janković, T.; Mahmutović, E.; Penjašković, D. Musculoskeletal symptoms of the neck and shoulder among dental practitioners. J. Back Musculoskelet. Rehabil. 2017, 30, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Rafeemanesh, E.; Jafari, Z.; Kashani, F.O.; Rahimpour, F. A study on job postures and musculoskeletal illnesses in dentists. Int. J. Occup. Med. Environ. Health 2013, 26, 615–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratzon, N.; Yaros, T.; Mizlik, A.; Kanner, T. Musculoskeletal symptoms among dentists in relation to work posture. Work 2000, 15, 153–158. [Google Scholar] [PubMed]
- Valachi, B.; Valachi, K. Mechanisms leading to musculoskeletal disorders in dentistry. J. Am. Dent. Assoc. 2003, 134, 1344–1350. [Google Scholar] [CrossRef]
- Newell, T.; Kumar, S. Prevalence of musculoskeletal disorders among orthodontists in Alberta. Int. J. Ind. Ergon. 2004, 33, 99–107. [Google Scholar] [CrossRef]
- Uppada, U.K.; Susmitha, M.; Hussaini, S.W.U.; Virk, I.; Yadav, T.G.; Khader, M.A. Ergonomics among dentists in the states of Telangana and Andhra Pradesh. Natl. J. Maxillofac. Surg. 2020, 11, 253–257. [Google Scholar] [CrossRef]
- La Rochelle, N.R. Work-Related Musculoskeletal Disorders among Dentists and Orthodontists. Master’s Thesis, Virginia Commonwealth University, Richmond, VA, USA, 2017. [Google Scholar]
- Holzgreve, F.; Haas, Y.; Naser, A.; Haenel, J.; Fraeulin, L.; Erbe, C.; Betz, W.; Wanke, E.; Brueggmann, D.; Nienhaus, A.; et al. Prevalence of Musculoskeletal Disorders in Germany—A Comparison between Dentists and Dental Assistants. Appl. Sci. 2021, 11, 6956. [Google Scholar] [CrossRef]
- Ohlendorf, D.; Erbe, C.; Hauck, I.; Nowak, J.; Hermanns, I.; Ditchen, D.; Ellegast, R.; Groneberg, D.A. Kinematic analysis of work-related musculoskeletal loading of trunk among dentists in Germany. BMC Musculoskelet. Disord. 2016, 17, 427. [Google Scholar] [CrossRef] [Green Version]
- Kapitán, M.; Hodačová, L.; Čermáková, E.; Machač, S.; Schmidt, J.; Pilbauerová, N. The Development of Musculoskeletal Disorders during Undergraduate Dentistry Studies—A Long-Term Prospective Study. Int. J. Environ. Res. Public Health 2021, 18, 7662. [Google Scholar] [CrossRef]
- Hill, K.B.; Burke, F.J.T.; Brown, J.; Macdonald, E.B.; Morris, A.J.; White, D.A.; Murray, K. Dental practitioners and ill health retirement: A qualitative investigation into the causes and effects. Br. Dent. J. 2010, 209, E8. [Google Scholar] [CrossRef] [Green Version]
- McAtamney, L.; Corlett, E.N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Vignais, N.; Bernard, F.; Touvenot, G.; Sagot, J.-C. Physical risk factors identification based on body sensor network combined to videotaping. Appl. Ergon. 2017, 65, 410–417. [Google Scholar] [CrossRef]
- Vignais, N.; Miezal, M.; Bleser, G.; Mura, K.; Gorecky, D.; Marin, F. Innovative system for real-time ergonomic feedback in industrial manufacturing. Appl. Ergon. 2013, 44, 566–574. [Google Scholar] [CrossRef]
- Maurer-Grubinger, C.; Holzgreve, F.; Fraeulin, L.; Betz, W.; Erbe, C.; Brueggmann, D.; Wanke, E.; Nienhaus, A.; Groneberg, D.; Ohlendorf, D. Combining Ergonomic Risk Assessment (RULA) with Inertial Motion Capture Technology in Dentistry—Using the Benefits from Two Worlds. Sensors 2021, 21, 4077. [Google Scholar] [CrossRef]
- Van Der Straaten, R.; Bruijnes, A.K.B.D.; Vanwanseele, B.; Jonkers, I.; De Baets, L.; Timmermans, A. Reliability and Agreement of 3D Trunk and Lower Extremity Movement Analysis by Means of Inertial Sensor Technology for Unipodal and Bipodal Tasks. Sensors 2019, 19, 141. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.-T.; Novak, A.; Brouwer, B.; Li, Q. Concurrent validation of Xsens MVN measurement of lower limb joint angular kinematics. Physiol. Meas. 2013, 34, N63–N69. [Google Scholar] [CrossRef]
- Blume, K.S.; Holzgreve, F.; Fraeulin, L.; Erbe, C.; Betz, W.; Wanke, E.M.; Brueggmann, D.; Nienhaus, A.; Maurer-Grubinger, C.; Groneberg, D.A.; et al. Ergonomic Risk Assessment of Dental Students—RULA Applied to Objective Kinematic Data. Int. J. Environ. Res. Public Health 2021, 18, 10550. [Google Scholar] [CrossRef]
- Maltry, F.H.; Maurer, C.; Wanke, E.M.; Ohlendorf, D. Präzisere ergonomische Risikobeurteilung durch die Kombination von Inertialsensoren mit observatorischen Methoden am Beispiel von RULA. Zent. Arb. Arb. Ergon. 2020, 70, 236–239. [Google Scholar] [CrossRef] [Green Version]
- Kimmel, K. Der zahnärztliche Arbeitsplatz: Funktion und Gestaltung. Zahnärztl. Welt 1980, 89, 40–52. [Google Scholar]
- Kimmel, K. Die Basiskonzepte Grundlage der Behandlungsplatzgestaltung. Quintessenz Zahntech. 1989, 40, 2251–2258. [Google Scholar]
- Kimmel, K. Ein Identifikationssystem für die zahnärztliche Ausrüstung. Zahnarztl. Mitt 1973, 65, 522–527. [Google Scholar]
- Li, G.; Buckle, P. Current techniques for assessing physical exposure to work-related musculoskeletal risks, with emphasis on posture-based methods. Ergonomics 1999, 42, 674–695. [Google Scholar] [CrossRef] [PubMed]
- Lobo, D.; Anuarbe, P.; López-Higuera, J.M.; Viera-Artiles, J.; Castillo, N.; Megía, R. Estimation of surgeons’ ergonomic dynamics with a structured light system during endoscopic surgery. Int. Forum Allergy Rhinol. 2019, 9, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch Institute. Gesundheitsberichterstattung des Bundes—Gemeinsam Getragen von RKI und Destatis; Robert Koch Institute: Berlin, Germany, 2015. [Google Scholar]
- Haas, Y.; Naser, A.; Haenel, J.; Fraeulin, L.; Holzgreve, F.; Erbe, C.; Betz, W.; Wanke, E.M.; Brueggmann, D.; Nienhaus, A.; et al. Prevalence of self-reported musculoskeletal disorders of the hand and associated conducted therapy approaches among dentists and dental assistants in Germany. PLoS ONE 2020, 15, e0241564. [Google Scholar] [CrossRef] [PubMed]
- Katano, K.; Nakajima, K.; Saito, M.; Kawano, Y.; Takeda, T.; Fukuda, K. Effects of Line of Vision on Posture, Muscle Activity and Sitting Balance During Tooth Preparation. Int. Dent. J. 2021, 71, 399–406. [Google Scholar] [CrossRef]
- Bud, M.; Jitaru, S.; Lucaciu, O.; Korkut, B.; Dumitrascu-Timis, L.; Ionescu, C.; Cimpean, S.; Delean, A. The advantages of the dental operative microscope in restorative dentistry. Med. Pharm. Rep. 2020, 94, 22–27. [Google Scholar] [CrossRef]
- Bud, M.; Pricope, R.; Pop, R.C.; Onaca, R.; Swerts, P.; Lucaciu, O.; Delean, A. Comparative analysis of preclinical dental students’ working postures using dental loupes and dental operating microscope. Eur. J. Dent. Educ. 2020, 15, 33–37. [Google Scholar] [CrossRef]
- Wajngarten, D.; Botta, A.C.; Garcia, P.P.N.S. Magnification loupes in dentistry: A qualitative study of dental students’ perspectives. Eur. J. Dent. Educ. 2020, 25, 305–309. [Google Scholar] [CrossRef]
- Kamal, A.M.; Ahmed, D.R.M.; Habib, S.F.K.; Al-Mohareb, R.A. Ergonomics of preclinical dental students and potential musculoskeletal disorders. J. Dent. Educ. 2020, 84, 1438–1446. [Google Scholar] [CrossRef]
- Moodley, R.; Naidoo, S.; Van Wyk, J.M. The prevalence of occupational health-related problems in dentistry: A review of the literature. J. Occup. Health 2018, 60, 111–125. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Field of Specialization | Occup. | Sex | Work Years | Age (Years) | Height (cm) | Weight (kg) |
|---|---|---|---|---|---|---|
| Generalists | D | 8 f/7 m | 9.1 ± 12.0 | 37.1 ± 12.1 | 164.4 ± 47.1 | 72.1 ± 11.5 |
| DA | 10 f/5 m | 5.5 ± 5.0 | 28.4 ± 6.0 | 146.6 ± 64.9 | 70.7 ± 15.1 | |
| Oral and maxillofacial surgeons | D | 3 f/12 m | 9.5 ± 9.0 | 36.3 ± 9.6 | 177.8 ± 8.2 | 75.5 ± 12.0 |
| DA | 12 f/3 m | 5.0 ± 2.4 | 26.7 ± 2.5 | 172.9 ± 9.2 | 68.3 ± 7.8 | |
| Endodontologists | D | 8 f/7 m | 6.6 ± 4.3 | 32.8 ± 4.1 | 176.4 ± 9.1 | 68.2 ± 10.1 |
| DA | 14 f/1 m | 5.1 ± 6.0 | 26.2 ± 7.0 | 163.1 ± 73.2 | 69.3 ± 9.2 | |
| Orthodontists | D | 8 f/7 m | 6.1 ± 2.7 | 32.6 ± 3.4 | 179.2 ± 10.9 | 69.5 ± 14.4 |
| DA | 13 f/2 m | 6.6 ± 4.7 | 29.1 ± 4.1 | 158.6 ± 48.3 | 68.2 ± 12.1 |
| Task | Quadrant 1 | Quadrant 2 | Quadrant 3 | Quadrant 4 | ||
|---|---|---|---|---|---|---|
| General Dentistry | Tooth filling of tooth 16 | Preparation of tooth 25 for crown uptake | Root canal treatment on tooth 36 | Tartar removal in the 4th quadrant | ||
| 1 | D | Prepare tooth cavity with a cylindrical diamond bur and the use of wedges. | Occlusal reduction using an occlusal reducer. | Performing an entrance cavity and trepanation on tooth 36 using a diamond-coated cylinder. | Removal of supra- and subgingival tartar/calculus using scalers and curettes. | |
| 1 | DA | Suction during preparation of the cavity. | Suction during preparation and retracting the cheek with a mirror if requested by the dentist. | Suction during preparation and retracting the cheek with a mirror if requested by the dentist. | Suction during curettage. | |
| 2 | D | Create a Tofflemire die using a die clamp. | Chamfer preparation using a torpedo-shaped diamond bur and approximal reducer. | Find the channel entrance using an endo file. | ||
| 2 | DA | Activating and blending Ketac for the tooth filling using a Ketac-set and mixing device and passing it to the dentist. | Suction during preparation and retracting the cheek with a mirror if requested by the dentist. | Retracting the cheek with a mirror if requested by the dentist. | ||
| 3 | D | Tooth filling with Ketac while using a Ketac-set, a cougar/Heidemann and a ball-shaped plugger, followed by the removal of the Tofflemire clamp. | Manual preparation of the canal using an ISO 20–40 endo file with regular irrigation using an irrigation cannula. | |||
| 3 | DA | No task. | Suction during irrigation and retracting the cheek with a mirror if requested by the dentist. | |||
| Endodontology | Root canal treatment of tooth 16 | Root canal treatment of tooth 26 | Root canal treatment of tooth 36 | Root canal treatment of tooth 46 | ||
| 1 | D | Application of the rubber dam. | Application of the rubber dam. | Application of the rubber dam. | Application of the rubber dam. | |
| 1 | DA | Helping to apply the rubber dam. | Helping to apply the rubber dam. | Helping to apply the rubber dam. | Helping to applicate the rubber dam. | |
| 2 | D | Trepanation of the tooth and access preparation including the enlarging of the root canal entrance. | Trepanation of the tooth and access preparation including the enlarging of the root canal entrance. | Trepanation of the tooth and access preparation including the enlarging of the root canal entrance. | Trepanation of the tooth and access preparation including the enlarging of the root canal entrance | |
| 2 | DA | Suction during trepanation and possibly the application of a file ISO 20. | Suction during trepanation and possibly the application of a file ISO 20. | Suction during trepanation and possibly the application of a file ISO 20. | Suction during trepanation and possibly the application of a file ISO 20. | |
| 3 | D | Root canal preparation with hand files at a certain working length, irrigation after each file and removal of the rubber dam. | Root canal preparation with hand files at a certain working length, irrigation after each file and removal of the rubber dam. | Root canal preparation with hand files at a certain working length, irrigation after each file and removal of the rubber dam. | Root canal preparation with hand files at a certain working length, irrigation after each file and removal of the rubber dam. | |
| 3 | DA | Setting the working lengths of the ISO 35, 40, 45 files to 18 mm each and aspirating the rinsing liquid. | Setting the working lengths of the ISO 35, 40, 45 files to 18 mm each and aspirating the rinsing liquid. | Setting the working lengths of the ISO 35, 40, 45 files to 18 mm each and aspirating the rinsing liquid. | Setting the working lengths of the ISO 35, 40, 45 files to 18 mm each and aspirating the rinsing liquid. | |
| 4 | D | Removal of the rubber dam. | Removal of the rubber dam. | Removal of the rubber dam. | Removal of the rubber dam. | |
| 4 | DA | Help with the rubber dam removal. | Help with the rubber dam removal. | Help with the rubber dam removal. | Help with the rubber dam removal. | |
| Orthodontics | Multiband Treatment | Multiband Treatment | Multiband Treatment | Multiband Treatment | ||
| 1 | D | Acid etching. | Acid etching. | Acid etching. | Acid etching. | |
| 1 | DA | Assisting: applying etching gel, aspiration. | Assisting: applying etching gel, aspiration. | Assisting: applying etching gel, aspiration. | Assisting: applying etching gel, aspiration. | |
| 2 | D | Direct bonding of braces on teeth 1, 3, 4, and 6 and opening of self-ligating braces. | Direct bonding of braces on teeth 1, 3, 4, and 6 and opening of self-ligating braces. | Direct bonding of braces on teeth 1, 3, 4, and 6 and opening of self-ligating braces. | Direct bonding of braces on teeth 1, 3, 4, and 6 and opening of self-ligating braces. | |
| 2 | DA | Assisting: coat brackets with composite and apply, cure with UV lamp. | Assisting: coat brackets with composite and apply, cure with UV lamp. | Assisting: coat brackets with composite and apply, cure with UV lamp. | Assisting: coat brackets with composite and apply, cure with UV lamp. | |
| 3 | D | Insertion of the archwire. | Insertion of the archwire. | Insertion of the archwire. | Insertion of the archwire. | |
| 3 | DA | Pre-shortening of the archwire. | Pre-shortening of the archwire. | Pre-shortening of the archwire. | Pre-shortening of the archwire. | |
| 4 | D | Integration of bracket 3 using elastic ligation. | Integration of bracket 3 using elastic ligation. | Integration of bracket 3 using elastic ligation. | Integration of brackets 3 using elastic ligation. | |
| 4 | DA | Picking up and applying Alastic with needle holder. | Picking up and applying Alastic with needle holder. | Picking up and applying Alastic with needle holder. | Picking up and applying Alastic with needle holder. | |
| 5 | D | Integration of brackets 1 and 4 using metal ligation. | Integration of brackets 1 and 4 using metal ligation. | Integration of brackets 1 and 4 using metal ligation. | Integration of brackets 1 and 4 using metal ligation. | |
| 5 | DA | Assisting: picking up and applying metal ligature with needle holder. | Assisting: picking up and applying metal ligature with needle holder. | Assisting: picking up and applying metal ligature with needle holder. | Assisting: picking up and applying metal ligature with needle holder. | |
| 6 | D | Debonding of bracket. | Debonding of bracket. | Debonding of bracket. | Debonding of bracket. | |
| 6 | DA | Assisting: applying the tongs for debonding. | Assisting: applying the tongs for debonding. | Assisting: applying the tongs for debonding. | Assisting: applying the tongs for debonding. | |
| Oral and maxillofacialsurgery | Surgical removal of tooth 13 | Surgical removal of tooth 23 | Surgical removal of tooth 38 | Surgical removal of tooth 48 | ||
| 1 | D | Palatinal and marginal incision in regions 16 to 11. | Vestibular and marginal incision in regions 21 to 25. | Crestal incision in region 38 with a mesial relieving incision. | Crestal incision in regions 48 to 44. | |
| 1 | DA | Suctioning with the small suction cup. | Suctioning with the small suction cup. | Suctioning with the small suction cup. | Suctioning with the small suction cup. | |
| 2 | D | Exposure of the palatinal impacted tooth 13 by osteotomy using a surgical round bur. If necessary, cut through the tooth using a Lindemann bur. Removal of the tooth 13 using a Bein root elevator or dental forceps. Curettage of the dental sac. | Exposure of the vestibular impacted tooth 23 by osteotomy using a surgical round bur. If necessary, cut through the tooth using a Lindemann bur. Removal of the tooth 23 using a Bein root elevator or dental forceps. Curettage of the dental sac. | Exposure of the impacted tooth 38 by osteotomy using a surgical round bur. Removal of the tooth 38 using a Bein root elevator or dental forceps. Curettage of the dental sac. | Exposure of the impacted tooth 48 by osteotomy using a surgical round bur. If necessary, cutting through the tooth using a Lindemann bur. Removal of the tooth 48 using a Bein root elevator or dental forceps. Curettage of the dental sac. | |
| 2 | DA | Aspirating and holding of the flap with an instrument of choice, handing instruments as requested by the dentist. | Aspirating and holding of the flap with an instrument of choice, handing instruments as requested by the dentist. | Aspirating and holding of the flap with an instrument of choice, handing instruments as requested by the dentist. | Aspirating and holding of the flap with an instrument of choice, handing instruments as requested by the dentist. | |
| 3 | D | Wound closure with single loop interrupted sutures. | Wound closure with single loop interrupted sutures. | Wound closure with single loop interrupted sutures. | Wound closure with single loop interrupted sutures. | |
| 3 | DA | Clamping the needle in the needle holder and cutting the seam with the scissors. | Clamping the needle in the needle holder and cutting the seam with the scissors. | Clamping the needle in the needle holder and cutting the seam with the scissors. | Clamping the needle in the needle holder and cutting the seam with the scissors. |
| RULA Score | Occupation | Oral and Maxillofacial Surgery | Endodontology | General Dentistry | Orthodontics | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median (IQD) | Rel. Av. RST | ERP (%) | Median (IQD) | Rel. Av. RST | ERP (%) | Median (IQD) | Rel. Av. RST | ERP (%) | Median (IQD) | Rel. Av. RST | ERP (%) | ||
| Final right (Max. Score 7) | DA | 5 (1) | 5.19 | 74.12 | 4.25 (1) | 4.66 | 66.54 | 5 (1) | 5.23 | 74.70 | 5 (1) | 4.75 | 67.91 |
| D | 5 (1) * | 5.00 | 71.49 | 5 (1) | 4.87 | 69.51 | 5 (1) | 5.05 | 72.13 | 5 (1) | 4.66 | 66.57 | |
| Final left (Max. Score 7) | DA | 5.5 (1) | 5.22 | 74.59 | 4 (1) | 4.63 | 66.11 | 5.5 (1) | 5.26 | 75.15 | 5 (1) | 4.81 | 68.78 |
| D | 5 (1) * | 4.98 * | 71.13 | 5 (1) | 4.78 | 68.35 | 5 (1) | 5.19 | 74.10 | 4 (1) | 4.49 | 64.08 | |
| Trunk Position-Step 10 | DA | 3 (1) | 2.66 | 44.28 | 2 (0) | 2.19 | 36.58 | 2 (0.75) * | 2.30 | 38.25 | 2 (0) | 2.17 | 36.21 |
| D | 2.50 (1) | 2.52 | 42.08 | 2.5 (1) | 2.51 | 41.81 | 3 (0.75) | 2.73 | 45.47 | 2 (0.75) | 2.32 | 38.73 | |
| Neck Position-Step 9 | DA | 3.5 (0.5) | 3.68 | 61.42 | 3 (1) | 3.45 | 57.56 | 3.75 (1) | 3.63 | 60.49 | 3.5 (1) | 3.62 | 60.37 |
| D | 3 (1) | 3.48 | 57.98 | 3 (1) | 3.46 | 57.63 | 3.25 (1) | 3.52 | 58.69 | 3 (1) * | 3.37 ** | 56.21 | |
| Right Wrist-Steps 3 and 4 | DA | 4 (0.75) | 4.20 | 70.01 | 5 (1) | 4.52 | 75.31 | 4.75 (1) | 4.56 | 76.05 | 4 (0.75) | 4.17 | 69.46 |
| D | 4 (1) | 4.34 | 72.3 | 4 (1) ** | 4.20 * | 70.01 | 4.5 (1) | 4.51 | 75.20 | 4 (1) | 4.31 | 71.84 | |
| Right Lower Arm-Step 2 | DA | 2 (1) | 2.45 | 81.73 | 2.25 (1) | 2.45 | 81.73 | 2.25 (1) | 2.37 | 79.07 | 3 (1) | 2.69 | 89.71 |
| D | 2(1) | 2.34 | 78.13 | 2(1) | 2.31 | 76.92 | 2 (0) * | 2.12 ** | 70.77 | 2 (1) ** | 2.41 *** | 80.35 | |
| Right Upper Arm-Step 1 | DA | 2 (0.75) | 1.74 ** | 28.96 | 2 (1) | 1.67 * | 27.78 | 2 (0.5) | 1.79 | 29.85 | 2 (1) | 1.78 | 29.66 |
| D | 2 (0.25) | 1.89 | 31.55 | 2(1.25) | 1.91 | 31.80 | 2 (0.5) | 1.90 | 31.68 | 2 (1) | 1.73 | 28.84 | |
| Left Wrist-Steps 3 and 4 | DA | 4.5 (0.5) | 4.47 | 74.45 | 4 (1) | 4.20 | 69.99 | 4.5 (1) | 4.35 | 72.52 | 4 (1) | 4.23 | 70.49 |
| D | 5 (1) | 4.53 | 75.52 | 4 (1) | 4.33 | 72.23 | 5 (0.75) | 4.71 | 78.53 | 4 (0.5) | 4.17 | 69.49 | |
| Left Lower Arm-Step 2 | DA | 2 (1) | 2.37 | 79.17 | 2.25 (1) | 2.40 | 80.00 | 2.25 (1) | 2.38 | 79.25 | 3 (1) | 2.61 | 87.07 |
| D | 3 (1) | 2.66 | 88.77 | 2 (1) | 2.42 | 80.73 | 2.5 (1) | 2.40 | 79.94 | 2 (1) ** | 2.28 *** | 76.01 | |
| Left Upper Arm-Step 1 | DA | 1.5 (0.5) | 1.56 | 26.06 | 1.5 (1) | 1.49 | 24.88 | 1.5 (1) | 1.63 | 27.22 | 1.5(1) | 1.59 | 26.43 |
| D | 1.5 (1) | 1.51 | 25.11 | 1.5 (1) | 1.55 | 25.87 | 1 (0.75) | 1.36 | 22.59 | 2 (1) | 1.71 | 28.48 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holzgreve, F.; Fraeulin, L.; Betz, W.; Erbe, C.; Wanke, E.M.; Brüggmann, D.; Nienhaus, A.; Groneberg, D.A.; Maurer-Grubinger, C.; Ohlendorf, D. A RULA-Based Comparison of the Ergonomic Risk of Typical Working Procedures for Dentists and Dental Assistants of General Dentistry, Endodontology, Oral and Maxillofacial Surgery, and Orthodontics. Sensors 2022, 22, 805. https://doi.org/10.3390/s22030805
Holzgreve F, Fraeulin L, Betz W, Erbe C, Wanke EM, Brüggmann D, Nienhaus A, Groneberg DA, Maurer-Grubinger C, Ohlendorf D. A RULA-Based Comparison of the Ergonomic Risk of Typical Working Procedures for Dentists and Dental Assistants of General Dentistry, Endodontology, Oral and Maxillofacial Surgery, and Orthodontics. Sensors. 2022; 22(3):805. https://doi.org/10.3390/s22030805
Chicago/Turabian StyleHolzgreve, Fabian, Laura Fraeulin, Werner Betz, Christina Erbe, Eileen M. Wanke, Dörthe Brüggmann, Albert Nienhaus, David A. Groneberg, Christian Maurer-Grubinger, and Daniela Ohlendorf. 2022. "A RULA-Based Comparison of the Ergonomic Risk of Typical Working Procedures for Dentists and Dental Assistants of General Dentistry, Endodontology, Oral and Maxillofacial Surgery, and Orthodontics" Sensors 22, no. 3: 805. https://doi.org/10.3390/s22030805
APA StyleHolzgreve, F., Fraeulin, L., Betz, W., Erbe, C., Wanke, E. M., Brüggmann, D., Nienhaus, A., Groneberg, D. A., Maurer-Grubinger, C., & Ohlendorf, D. (2022). A RULA-Based Comparison of the Ergonomic Risk of Typical Working Procedures for Dentists and Dental Assistants of General Dentistry, Endodontology, Oral and Maxillofacial Surgery, and Orthodontics. Sensors, 22(3), 805. https://doi.org/10.3390/s22030805