
A Sensor-Based Perspective in Early-Stage Parkinson’s Disease: Current State and the Need for Machine Learning Processes


 ,
, 



Abstract
:1. Introduction
2. Early Detection and the Need for Sensor-Based Approaches

{kind=link}
{kind=link}
| Type of Sensor | Targeting/Monitoring | Ref. |
|---|---|---|
| Single-walled carbon nanotubes fabricated by sodium dodecyl sulfate | Simultaneous electrocatalytic determination of ascorbic acid (AA), dopamine (DA) and uric acid (UA) | [21] |
| Nanosized copper oxide/multiwall carbon nanotubes | Electrocatalytic oxidation of dopamine monitoring | [23] |
| Microneedle sensing platform | Electrochemical monitoring of levodopa (enzymatic–amperometric and nonenzymatic voltammetric detection) | [25] |
| Electroanalytical assay using alpha-synuclein modified electrodes | a-synuclein detection through autoantibodies sampling | [27] |
| Semiconductor quantum dots (CdSe/ZnS) | Mitochondrial complex I activity fluorescence monitoring | [28] |
| DNA electrochemical biosensor through an imprinted polymer layer fabricated on a gold electrode | Nucleic acid degradation products determination (8-hydroxyguanine) | [29] |
| Antibody-based biosensor on multiblock nanorods (Au and Ag)/biotinylated aptamers immobilization | Dopamine detection | [30,31] |
| A segmented double-integration algorithm | Calculation of step length and step time from wearable inertial measurement units, spatiotemporal gait parameters measurement | [36] |
| Embedded triaxial accelerometers from consumer smartwatches and multitask classification models | Assessment of the amplitude and constancy of resting tremor | [37] |
| MCPD-Net, a multimodal deep learning model using visions accelerometer sensors | Effective representations of human movements prediction | [38] |
| mKinetikos, a mobile-based system (mHealth system) | Continuous and remote monitoring of PD patients’ functional mobility and global clinical status | [39] |
| Flexible wearable sensors attached to the hands, arms and thighs | Detection of bradykinesia and tremor in the upper extremities | [40] |
3. The Sensor Perspective
4. Recent Machine Learning Advancements in Sensor-Based Data
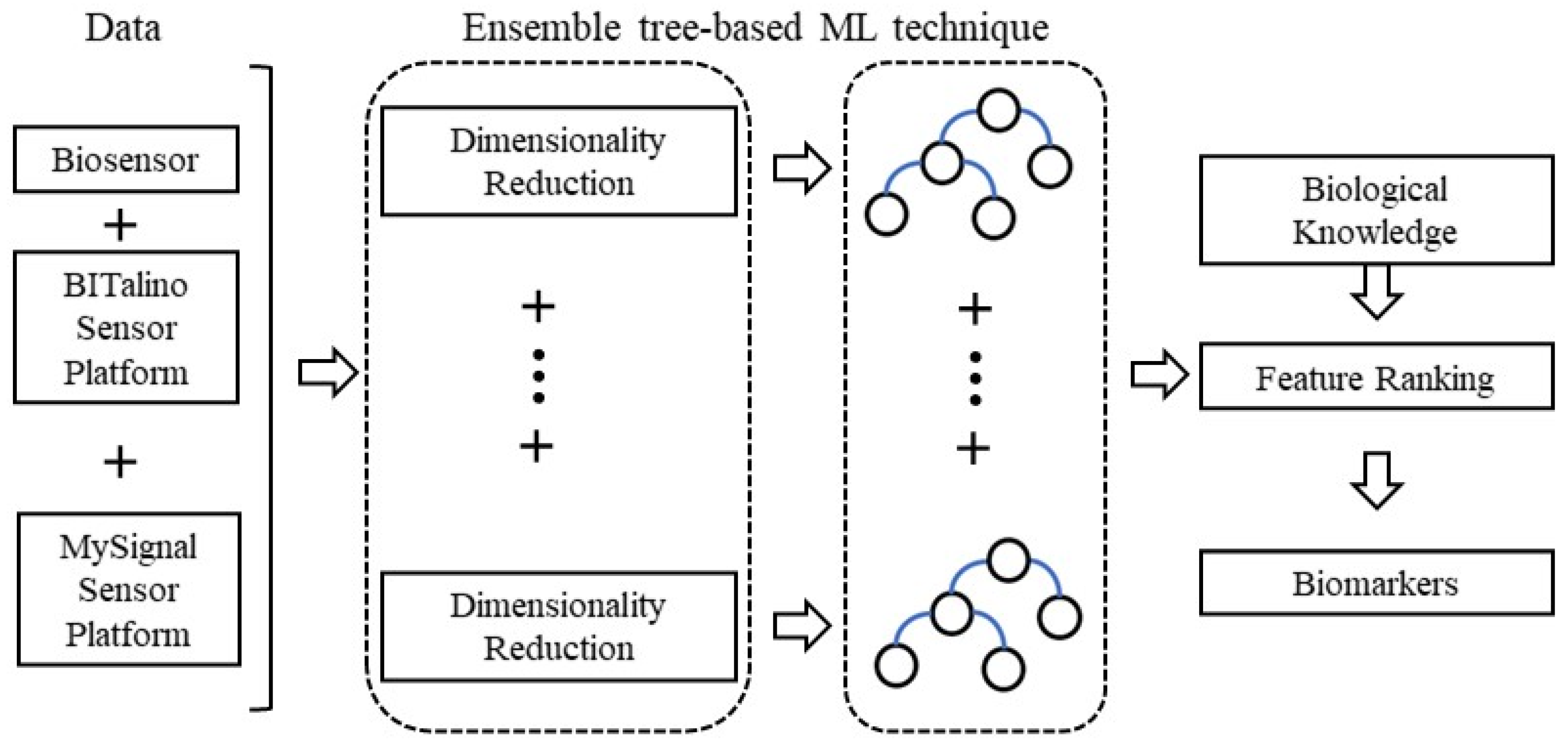
5. Ensemble Methods in Sensor-Based Data—Towards the Future Big Challenge
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Poewe, W.; Seppi, K.; Tanner, C.M.; Halliday, G.M.; Brundin, P.; Volkmann, J.; Schrag, A.E.; Lang, A.E. Parkinson disease. Nat. Rev. Dis. Primers 2017, 23, 17013. [Google Scholar] [CrossRef]
- Klein, C.; Westenberger, A. Genetics of Parkinson’s disease. Cold Spring Harb. Perspect. Med. 2012, 2, a008888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, H.X.; Shi, Y.; Yang, Y.; Ahmeti, K.B.; Miller, N.; Huang, C.; Cheng, L.; Zhai, H.; Deng, S. Identification of TMEM230 mutations in familial Parkinson’s disease. Nat. Genet. 2016, 48, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Waragai, M.; Wei, J.; Fujita, M.; Nakai, M.; Ho, G.J.; Masliah, E.; Akatsu, H.; Yamada, T.; Hashimoto, M. Increased DJ-1 in the cerebrospinal fluids of sporadic Parkinson’s disease. Biochim. Biophys. Res. Commun. 2006, 345, 967–972. [Google Scholar] [CrossRef] [PubMed]
- De Fazio, R.; De Vittorio, M.; Visconti, P. Innovative IoT Solutions and Wearable Sensing Systems for Monitoring Human Biophysical Parameters: A Review. Electronics 2021, 10, 1660. [Google Scholar] [CrossRef]
- Fisher, J.M.; Hammerla, N.Y.; Ploetz, T.; Andras, P.; Rochester, L.; Walker, R.W. Unsupervised home monitoring of Parkinson’s disease motor symptoms using body-worn accelerometers. Parkinsonism Relat. Disord. 2016, 33, 44–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubota, K.J.; Chen, J.A.; Little, M.A. Machine learning for large-scale wearable sensor data in Parkinson’s disease: Concepts, promises, pitfalls, and futures. Mov. Disord. 2016, 31, 1314–1326. [Google Scholar] [CrossRef]
- Harris, J.P.; Burrell, J.C.; Struzyna, L.A.; Chen, H.I.; Serruya, M.D.; Wolf, J.A.; Duda, J.E.; Cullen, D.K. Emerging regenerative medicine and tissue engineering strategies for Parkinson’s disease. NPJ Parkinsons Dis. 2020, 6, 4. [Google Scholar] [CrossRef] [Green Version]
- Noyce, A.J.; Lees, A.J.; Schrag, A.E. The prediagnostic phase of Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2016, 87, 871–878. [Google Scholar] [CrossRef] [Green Version]
- Poewe, W. Clinical measures of progression in Parkinson’s disease. Mov. Disord. 2009, 24, S671–S676. [Google Scholar] [CrossRef]
- Pagano, G.; Niccolini, F.; Politis, M. Imaging in Parkinson’s disease. Clin. Med. 2016, 16, 371–375. [Google Scholar] [CrossRef]
- Mollenhauer, B.; Locascio, J.J.; Schulz-Schaeffer, W.; Sixel-Döring, F.; Trenkwalder, C.; Schlossmacher, M.G. α-synuclein and tau concentrations in cerebrospinal fluid of patients presenting with parkinsonism: A cohort study. Lancet Neurol. 2011, 10, 230–240. [Google Scholar] [CrossRef]
- Costa, A.; Peppe, A.; Carlesimo, G.A.; Zabberoni, S.; Scalici, F.; Caltagirone, C.; Angelucci, F. Brain-derived neurotrophic factor serum levels correlate with cognitive performance in Parkinson’s disease patients with mild cognitive impairment. Front. Behav. Neurosci. 2015, 9, 253. [Google Scholar] [CrossRef]
- Picillo, M.; Erro, R.; Santangelo, G.; Pivonello, R.; Longo, K.; Pivonello, C.; Vitale, C.; Amboni, M.; Moccia, M.; Colao, A.; et al. Insulin-like growth factor-1 and progression of motor symptoms in early, drug-naïve Parkinson’s disease. J. Neurol. 2013, 260, 1724–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garretti, F.; Agalliu, D.; Lindestam Arlehamn, C.S.; Sette, A.; Sulzer, D. Autoimmunity in Parkinson’s Disease: The Role of α-Synuclein-Specific T Cells. Front. Immunol. 2019, 10, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krokidis, M.G.; Exarchos, T.P.; Vlamos, P. Data-driven biomarker analysis using computational omics approaches to assess neurodegenerative disease progression. Math. Biosci. Eng. 2021, 18, 1813–1832. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Papapetropoulos, S.; Xiong, M.; Kieburtz, K. The First Frontier: Digital Biomarkers for Neurodegenerative Disorders. Digit. Biomark. 2017, 1, 6–13. [Google Scholar] [CrossRef]
- Bhalla, N.; Jolly, P.; Formisano, N.; Estrela, P. Introduction to biosensors. Essays Biochem. 2016, 60, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Naresh, V.; Lee, N. A Review on Biosensors and Recent Development of Nanostructured Materials-Enabled Biosensors. Sensors 2021, 21, 1109. [Google Scholar] [CrossRef]
- Kim, J.; Campbell, A.S.; de Ávila, B.E.-F.; Wang, J. Wearable biosensors for healthcare monitoring. Nat. Biotechnol. 2019, 37, 389–406. [Google Scholar] [CrossRef]
- Li, Y.; Du, J.; Yang, J.; Liu, D.; Lu, X. Electrocatalytic detection of dopamine in the presence of ascorbic acid and uric acid using single-walled carbon nanotubes modified electrode. Colloids Surf. B Biointerfaces 2012, 97, 32–36. [Google Scholar] [CrossRef]
- Moreno, M.; Arribas, A.S.; Bermejo, E.; Chicharro, M.; Zapardiel, A.; Rodríguez, M.C.; Jalit, Y.; Rivas, G.A. Selective detection of dopamine in the presence of ascorbic acid using carbon nanotube modified screen-printed electrodes. Talanta 2010, 80, 2149–2156. [Google Scholar] [CrossRef]
- Yang, S.; Li, G.; Yin, Y.; Yang, R.; Li, J.; Qu, L. Nano-sized copper oxide/multi-wall carbon nanotube/Nafion modified electrode for sensitive detection of dopamine. J. Electroanal. Chem. 2013, 703, 45–51. [Google Scholar] [CrossRef]
- Aravind, S.J.; Ramaprabhu, S. Noble metal dispersed multiwalled carbon nanotubes immobilized ss-DNA for selective detection of dopamine. Sens. Actuators B Chem. 2011, 155, 679–686. [Google Scholar] [CrossRef]
- Goud, K.Y.; Moonla, C.; Mishra, R.K.; Yu, C.; Narayan, R.; Litvan, I.; Wang, J. Wearable Electrochemical Microneedle Sensor for Continuous Monitoring of Levodopa: Toward Parkinson Management. ACS Sens. 2019, 4, 2196–2204. [Google Scholar] [CrossRef]
- Jauhiainen, M.; Puustinen, J.; Mehrang, S.; Ruokolainen, J.; Holm, A.; Vehkaoja, A.; Nieminen, H. Identification of Motor Symptoms Related to Parkinson Disease Using Motion-Tracking Sensors at Home (KÄVELI): Protocol for an Observational Case-Control Study. JMIR Res. Protoc. 2019, 8, e12808. [Google Scholar] [CrossRef]
- Bryan, T.; Luo, X.; Forsgren, L.; Morozova-Roche, L.A.; Davis, J.J. The robust electrochemical detection of a Parkinson’s disease marker in whole blood sera. Chem. Sci. 2012, 3, 3468–3473. [Google Scholar] [CrossRef]
- Ma, W.; Qin, L.-X.; Liu, F.-T.; Gu, Z.; Wang, J.; Pan, Z.G.; James, T.D.; Long, Y.-T. Ubiquinone-quantum dot bioconjugates for in vitro and intracellular complex I sensing. Sci. Rep. 2013, 3, srep01537. [Google Scholar] [CrossRef] [Green Version]
- Martins, G.; Marques, A.; Fortunato, E.; Sales, M.G.F. 8-hydroxy-2′-deoxyguanosine (8-OHdG) biomarker detection down to picoMolar level on a plastic antibody film. Biosens. Bioelectron. 2016, 86, 225–234. [Google Scholar] [CrossRef]
- Choi, Y.; Choi, J.-H.; Liu, L.; Oh, B.-K.; Park, S. Optical Sensitivity Comparison of Multiblock Gold–Silver Nanorods toward Biomolecule Detection: Quadrupole Surface Plasmonic Detection of Dopamine. Chem. Mater. 2013, 25, 919–926. [Google Scholar] [CrossRef]
- Kim, E.; Paeng, I.R. Advantageous Sensitivity in the DNA Homolog of the RNA Dopamine Aptamer. J. Immunoass. Immunochem. 2014, 35, 83–100. [Google Scholar] [CrossRef] [PubMed]
- Kakkos, I.; Miloulis, S.T.; Gkiatis, K.; Dimitrakopoulos, G.N.; Matsopoulos, G.K. Human–Machine interfaces for motor rehabilitation. In Advanced Computational Intelligence in Healthcare-7; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–16. [Google Scholar]
- Soufineyestani, M.; Dowling, D.; Khan, A. Electroencephalography (EEG) Technology Applications and Available Devices. Appl. Sci. 2020, 10, 7453. [Google Scholar] [CrossRef]
- Majumder, S.; Takahashi, N.; Chari, S.T. Wearable Sensors for Remote Health Monitoring. Sensors 2017, 17, 130. [Google Scholar] [CrossRef]
- Rovini, E.; Maremmani, C.; Cavallo, F. A Wearable System to Objectify Assessment of Motor Tasks for Supporting Parkinson’s Disease Diagnosis. Sensors 2020, 20, 2630. [Google Scholar] [CrossRef] [PubMed]
- Muthukrishnan, N.; Abbas, J.J.; Krishnamurthi, N. A Wearable Sensor System to Measure Step-Based Gait Parameters for Parkinson’s Disease Rehabilitation. Sensors 2020, 20, 6417. [Google Scholar] [CrossRef] [PubMed]
- Sigcha, L.; Pavón, I.; Costa, N.; Costa, S.; Gago, M.; Arezes, P.; López, J.M.; De Arcas, G. Automatic Resting Tremor Assessment in Parkinson’s Disease Using Smartwatches and Multitask Convolutional Neural Networks. Sensors 2021, 21, 291. [Google Scholar] [CrossRef]
- Heidarivincheh, F.; McConville, R.; Morgan, C.; McNaney, R.; Masullo, A.; Mirmehdi, M.; Whone, A.; Craddock, I. Multimodal Classification of Parkinson’s Disease in Home Environments with Resiliency to Missing Modalities. Sensors 2021, 21, 4133. [Google Scholar] [CrossRef]
- Bouça-Machado, R.; Pona-Ferreira, F.; Leitão, M.; Clemente, A.; Vila-Viçosa, D.; Kauppila, L.A.; Costa, R.M.; Matias, R.; Ferreira, J.J. Feasibility of a Mobile-Based System for Unsupervised Monitoring in Parkinson’s Disease. Sensors 2021, 21, 4972. [Google Scholar] [CrossRef]
- Lonini, L.; Dai, A.; Shawen, N.; Simuni, T.; Poon, C.; Shimanovich, L.; Daeschler, M.; Ghaffari, R.; Rogers, J.A.; Jayaraman, A. Wearable sensors for Parkinson’s disease: Which data are worth collecting for training symptom detection models. NPJ Digit. Med. 2018, 1, 1–8. [Google Scholar] [CrossRef]
- Del Din, S.; Godfrey, A.; Mazzà, C.; Lord, S.; Rochester, L. Free-living monitoring of Parkinson’s disease: Lessons from the field. Mov. Disord. 2016, 31, 1293–1313. [Google Scholar] [CrossRef]
- Mehrotra, P. Biosensors and their applications—A review. J. Oral Biol. Craniofac. Res. 2016, 6, 153–159. [Google Scholar] [CrossRef] [Green Version]
- Arumugam, S.; Colburn, D.A.M.; Sia, S.K. Biosensors for Personal Mobile Health: A System Architecture Perspective. Adv. Mater. Technol. 2020, 5, 1900720. [Google Scholar] [CrossRef] [PubMed]
- Kaur, G.; Adhikari, R.; Cass, P.; Bown, M.; Gunatillake, P. Electrically conductive polymers and composites for biomedical applications. RSC Adv. 2015, 5, 37553–37567. [Google Scholar] [CrossRef]
- Boeva, Z.A.; Sergeyev, V.G. Polyaniline: Synthesis, properties, and application. Polym. Sci. Ser. C 2014, 56, 144–153. [Google Scholar] [CrossRef]
- Yoo, J.E.; Cross, J.L.; Bucholz, T.L.; Lee, K.S.; Espe, M.P.; Loo, Y.-L. Improving the electrical conductivity of polymer acid-doped polyaniline by controlling the template molecular weight. J. Mater. Chem. 2007, 17, 1268–1275. [Google Scholar] [CrossRef]
- Bayer, C.L.; Konuk, A.A.; Peppas, N.A. Development of a protein sensing device utilizing interactions between polyaniline and a polymer acid dopant. Biomed. Microdevices 2010, 12, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, D.A.; Molinnus, D.; Beging, S.; Siqueira, J.R., Jr.; Schöning, M.J. Biosensor Based on Self-Assembled Films of Graphene Oxide and Polyaniline Using a Field-Effect Device Platform. Phys. Status Solidi (A) 2021, 218, 2000747. [Google Scholar] [CrossRef]
- Fujisaki, T.; Kashima, K.; Serrano-Luginbühl, S.; Kissner, R.; Bajuk-Bogdanović, D.; Milojević-Rakić, M.; Ćirić-Marjanović, G.; Busato, S.; Lizundia, E.; Walde, P. Effect of template type on the preparation of the emeraldine salt form of polyaniline (PANI-ES) with horseradish peroxidase isoenzyme C (HRPC) and hydrogen peroxide. RSC Adv. 2019, 9, 33080–33095. [Google Scholar] [CrossRef] [Green Version]
- Wagner, R.; da Silva, H.P.; Gramann, K. Validation of a Low-Cost Electrocardiography (ECG) System for Psychophysiological Research. Sensors 2021, 21, 4485. [Google Scholar] [CrossRef]
- Ponciano, V.; Pires, I.M.; Ribeiro, F.R.; Villasana, M.V.; Crisóstomo, R.; Teixeira, M.C.; Zdravevski, E. Mobile Computing Technologies for Health and Mobility Assessment: Research Design and Results of the Timed up and Go Test in Older Adults. Sensors 2020, 20, 3481. [Google Scholar] [CrossRef]
- Kutt, K.; Drążyk, D.; Bobek, S.; Nalepa, G.J. Personality-Based Affective Adaptation Methods for Intelligent Systems. Sensors 2021, 21, 163. [Google Scholar] [CrossRef] [PubMed]
- Ben Hassen, H.; Dghais, W.; Hamdi, B. An E-health system for monitoring elderly health based on Internet of Things and Fog computing. Health Inf. Sci. Syst. 2019, 7, 24. [Google Scholar] [CrossRef]
- Vizitiu, C.; Bîră, C.; Dinculescu, A.; Nistorescu, A.; Marin, M. Exhaustive Description of the System Architecture and Prototype Implementation of an IoT-Based eHealth Biometric Monitoring System for Elders in Independent Living. Sensors 2021, 21, 1837. [Google Scholar] [CrossRef]
- Islam, M.S.; Islam, M.T.; Almutairi, A.F.; Beng, G.K.; Misran, N.; Amin, N. Monitoring of the Human Body Signal through the Internet of Things (IoT) Based LoRa Wireless Network System. Appl. Sci. 2019, 9, 1884. [Google Scholar] [CrossRef] [Green Version]
- Johnston, S.J.; Cox, S.J. The Raspberry Pi: A Technology Disrupter, and the Enabler of Dreams. Electronics 2017, 6, 51. [Google Scholar] [CrossRef] [Green Version]
- Weiler, G.; Schröder, C.; Schera, F.; Dobkowicz, M.; Kiefer, S.; Heidtke, K.R.; Hänold, S.; Nwankwo, I.; Forgó, N.; Stanulla, M.; et al. p-BioSPRE—An information and communication technology framework for transnational biomaterial sharing and access. Ecancermedicalscience 2014, 8, 401. [Google Scholar] [PubMed]
- Lowe, H.J.; Ferris, T.A.; Hernandez, P.M.; Weber, S.C. STRIDE—An Integrated Standards-Based Translational Research Informatics Platform. AMIA Annu. Symp. Proc. 2009, 2009, 391–395. [Google Scholar] [PubMed]
- Michael, J. Fox Foundation for Parkinson’s Research. Fox Insight Clinical Trials NCT02668835 and NCT02474329. 2016. Available online: https://foxinsight.michaeljfox.org (accessed on 20 November 2021).
- Arora, S.; Venkataraman, V.; Zhan, A.; Donohue, S.; Biglan, K.M.; Dorsey, E.R.; Little, M.A. Detecting and monitoring the symptoms of Parkinson’s disease using smartphones: A pilot study. Parkinsonism Relat. Disord. 2015, 21, 650–653. [Google Scholar] [CrossRef] [Green Version]
- Lipsmeier, F.; Taylor, K.I.; Kilchenmann, T.; Wolf, D.; Scotland, A.; Schjodt-Eriksen, J.; Cheng, W.Y.; Fernandez-Garcia, I.; Siebourg-Polster, J.; Jin, L.; et al. Evaluation of smartphone-based testing to generate exploratory outcome measures in a phase 1 Parkinson’s disease clinical trial. Mov. Disord. 2018, 33, 1287–1297. [Google Scholar] [CrossRef] [PubMed]
- Zhan, A.; Mohan, S.; Tarolli, C.; Schneider, R.B.; Adams, J.L.; Sharma, S.; Elson, M.J.; Spear, K.L.; Glidden, A.M.; Little, M.A.; et al. Using smartphones and machine learning to quantify Parkinson disease severity: The mobile Parkinson disease score. JAMA Neurol. 2018, 75, 876–880. [Google Scholar] [CrossRef]
- Evers, L.J.; Raykov, Y.P.; Krijthe, J.H.; de Lima, A.L.S.; Badawy, R.; Claes, K.; Heskes, T.M.; Little, M.A.; Meinders, M.J.; Bloem, B.R. Real-Life Gait Performance as a Digital Biomarker for Motor Fluctuations: The Parkinson@Home Validation Study. J. Med. Internet Res. 2020, 22, e19068. [Google Scholar] [CrossRef]
- Warmerdam, E.; Romijnders, R.; Welzel, J.; Hansen, C.; Schmidt, G.; Maetzler, W. Quantification of Arm Swing during Walking in Healthy Adults and Parkinson’s Disease Patients: Wearable Sensor-Based Algorithm Development and Validation. Sensors 2020, 20, 5963. [Google Scholar] [CrossRef]
- Johri, A.; Tripathi, A. Parkinson disease detection using deep neural networks. In Proceedings of the 2019 Twelfth International Conference on Contemporary Computing (IC3), Noida, India, 8–10 August 2019; pp. 1–4. [Google Scholar]
- Aversano, L.; Bernardi, M.L.; Cimitile, M.; Pecori, R. Early Detection of Parkinson Disease using Deep Neural Networks on Gait Dynamics. In Proceedings of the 2020 International Joint Conference on Neural Networks (IJCNN), Glasgow, UK, 19–24 July 2020; pp. 1–8. [Google Scholar]
- Wan, K.R.; Maszczyk, T.; See, A.A.Q.; Dauwels, J.; King, N.K.K. A review on microelectrode recording selection of features for machine learning in deep brain stimulation surgery for Parkinson’s disease. Clin. Neurophysiol. 2019, 130, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Jane, Y.N.; Nehemiah, H.K.; Arputharaj, K. A Q-backpropagated time delay neural network for diagnosing severity of gait disturbances in Parkinson’s disease. J. Biomed. Inform. 2016, 60, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.A.; Houghten, S.; Brown, J.A. Models of Parkinson’s Disease Patient Gait. IEEE J. Biomed. Health Inform. 2019, 24, 3103–3110. [Google Scholar] [CrossRef] [PubMed]
- Al-Sarem, M.; Saeed, F.; Boulila, W.; Emara, A.H.; Al-Mohaimeed, M.; Errais, M. Feature Selection and Classification Using CatBoost Method for Improving the Performance of Predicting Parkinson’s Disease. In Advances on Smart and Soft Computing; Springer: Singapore, 2020; pp. 189–199. [Google Scholar] [CrossRef]
- Almeida, J.S.; Rebouças Filho, P.P.; Carneiro, T.; Wei, W.; Damaševičius, R.; Maskeliūnas, R.; de Albuquerque, V.H.C. Detecting Parkinson’s disease with sustained phonation and speech signals using machine learning techniques. Pattern Recognit. Lett. 2019, 125, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Nahar, N.; Ara, F.; Neloy, A.I.; Biswas, A.; Hossain, M.S.; Andersson, K. Feature Selection Based Machine Learning to Improve Prediction of Parkinson Disease. In International Conference on Brain Informatics; Springer: Cham, Switzerland, 2021; pp. 496–508. [Google Scholar]
- Zhou, Z.H. Ensemble learning. In Machine; Springer: Singapore, 2021; pp. 181–210. [Google Scholar]
- Vrahatis, A.; Tasoulis, S.; Georgakopoulos, S.; Plagianakos, V. Ensemble Classification through Random Projections for Single-Cell RNA-Seq Data. Information 2020, 11, 502. [Google Scholar] [CrossRef]
- Chen, W.; Xu, Y.; Yu, Z.; Cao, W.; Chen, C.L.P.; Han, G. Hybrid Dimensionality Reduction Forest with Pruning for High-Dimensional Data Classification. IEEE Access 2020, 8, 40138–40150. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krokidis, M.G.; Dimitrakopoulos, G.N.; Vrahatis, A.G.; Tzouvelekis, C.; Drakoulis, D.; Papavassileiou, F.; Exarchos, T.P.; Vlamos, P. A Sensor-Based Perspective in Early-Stage Parkinson’s Disease: Current State and the Need for Machine Learning Processes. Sensors 2022, 22, 409. https://doi.org/10.3390/s22020409
Krokidis MG, Dimitrakopoulos GN, Vrahatis AG, Tzouvelekis C, Drakoulis D, Papavassileiou F, Exarchos TP, Vlamos P. A Sensor-Based Perspective in Early-Stage Parkinson’s Disease: Current State and the Need for Machine Learning Processes. Sensors. 2022; 22(2):409. https://doi.org/10.3390/s22020409
Chicago/Turabian StyleKrokidis, Marios G., Georgios N. Dimitrakopoulos, Aristidis G. Vrahatis, Christos Tzouvelekis, Dimitrios Drakoulis, Foteini Papavassileiou, Themis P. Exarchos, and Panayiotis Vlamos. 2022. "A Sensor-Based Perspective in Early-Stage Parkinson’s Disease: Current State and the Need for Machine Learning Processes" Sensors 22, no. 2: 409. https://doi.org/10.3390/s22020409
APA StyleKrokidis, M. G., Dimitrakopoulos, G. N., Vrahatis, A. G., Tzouvelekis, C., Drakoulis, D., Papavassileiou, F., Exarchos, T. P., & Vlamos, P. (2022). A Sensor-Based Perspective in Early-Stage Parkinson’s Disease: Current State and the Need for Machine Learning Processes. Sensors, 22(2), 409. https://doi.org/10.3390/s22020409