
A Week of Sleep Restriction Does Not Affect Nighttime Glucose Concentration in Healthy Adult Males When Slow-Wave Sleep Is Maintained



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Continuous Glucose Monitoring Device
2.3. Capillary Blood Sampling Device
2.4. Sleep Monitoring
2.5. Activity Monitoring
2.6. Laboratory Setting
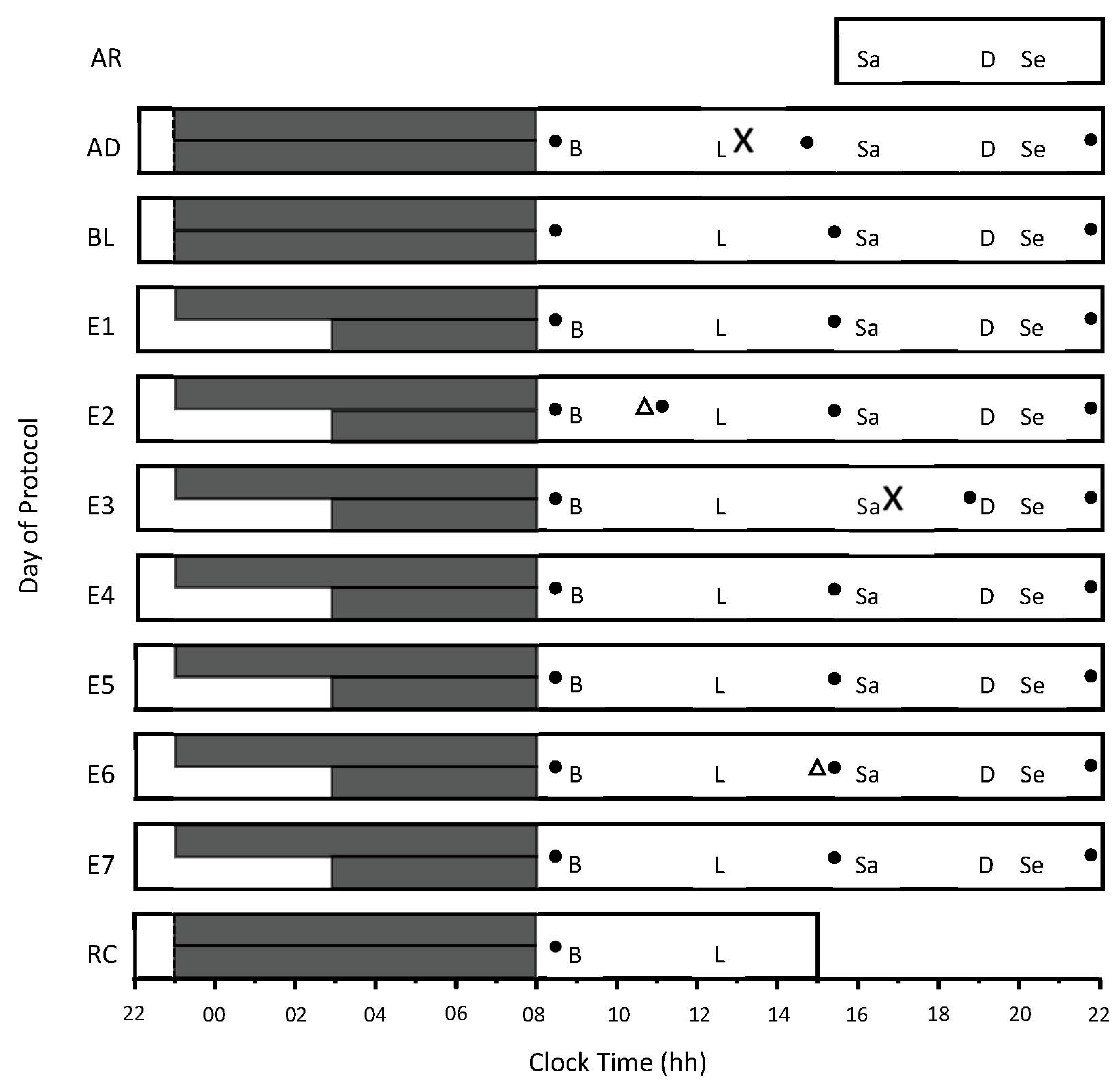
2.7. Experimental Design
2.8. Meals and Caloric Intake
2.9. Data Analysis
2.10. Statistical Analysis
3. Results
3.1. Sleep
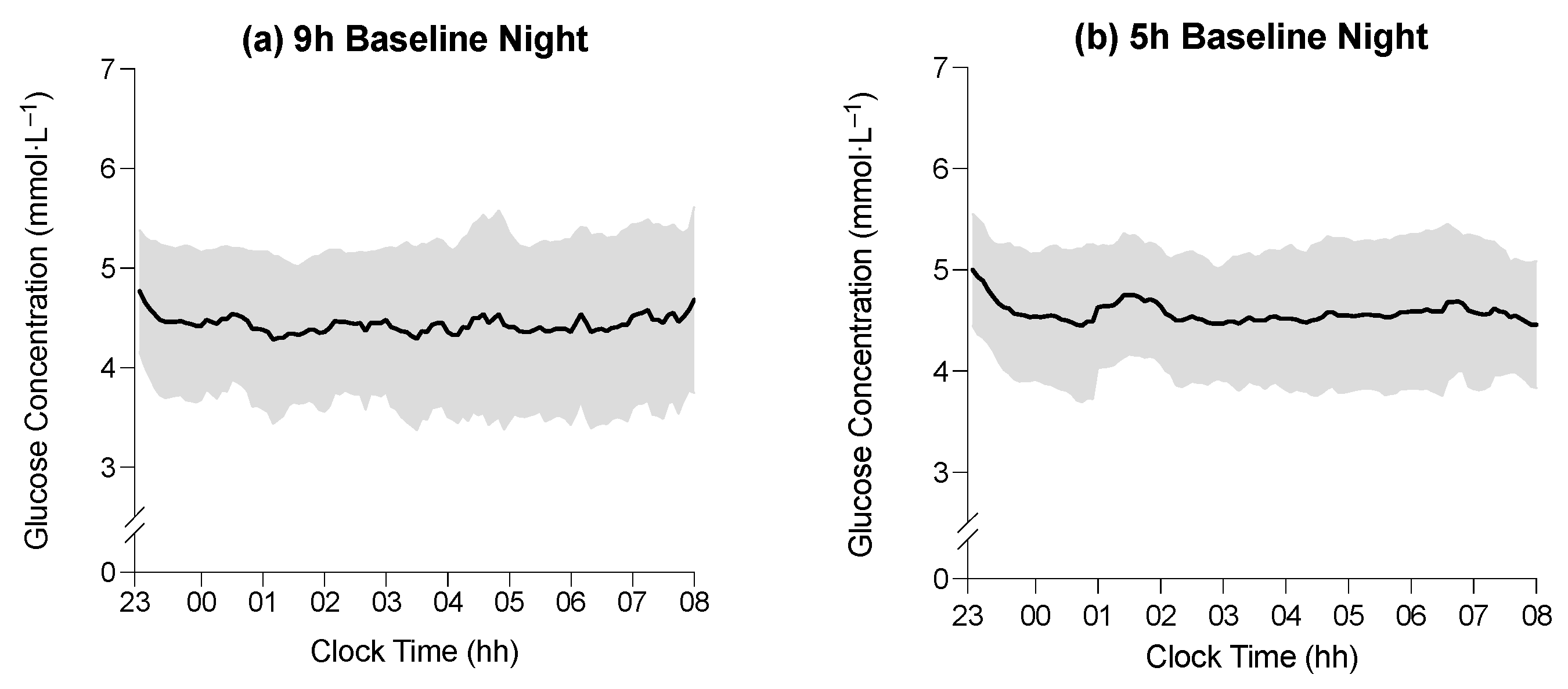
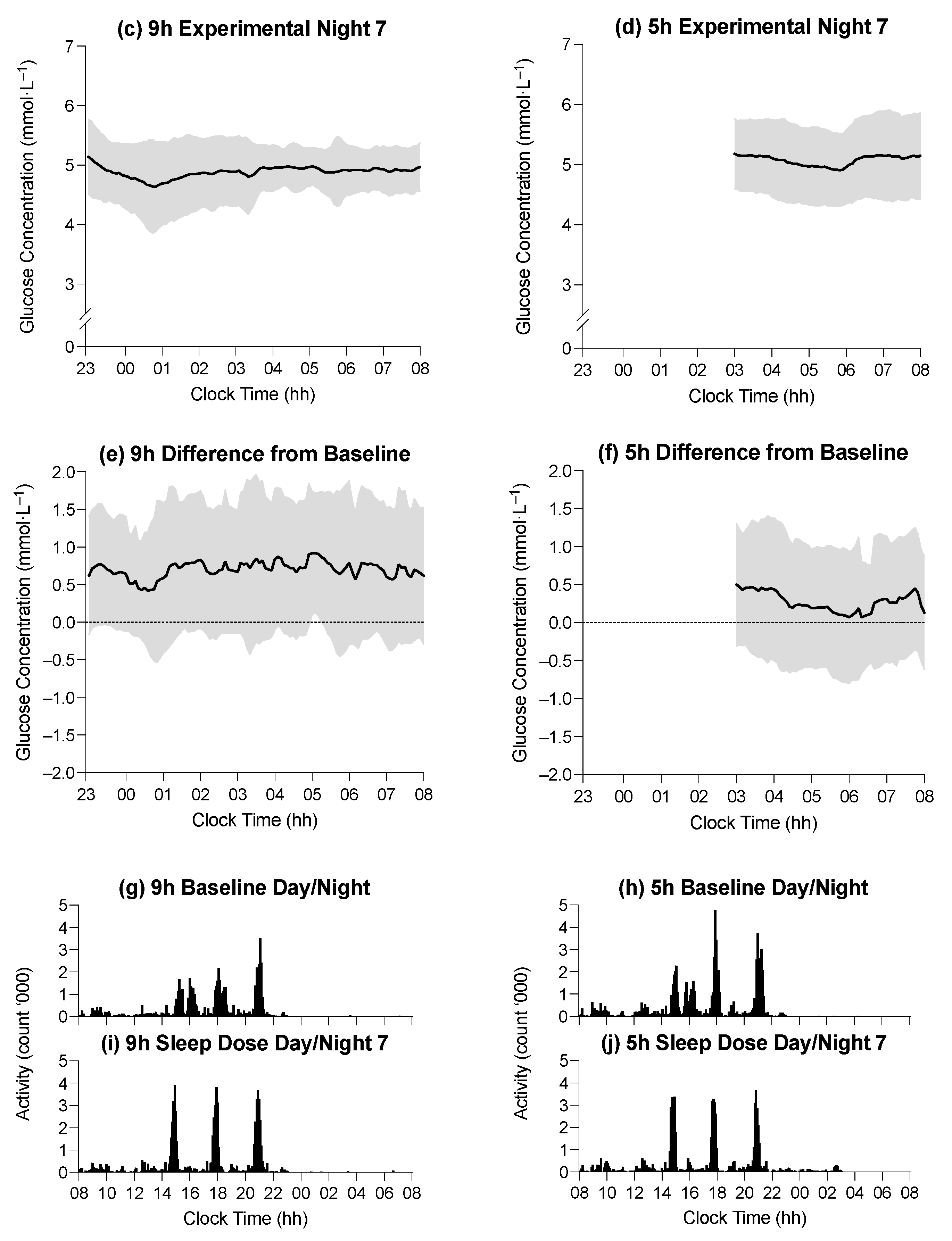
3.2. The Effect of Time in Bed on Average Glucose Concentration during Sleep

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Condition | |
|---|---|---|
| 9 h | 5 h | |
| Baseline | ||
| Glucose concentration during time in bed (mmol·L−1) | 4.4 ± 0.1 | 4.6 ± 0.1 |
| Glucose concentration during stage N2 (mmol·L−1) | 4.4 ± 0.9 | 4.5 ± 0.6 |
| Glucose concentration during stage N3 (mmol·L−1) | 4.5 ± 0.8 | 4.5 ± 0.6 |
| Glucose concentration during stage REM (mmol·L−1) | 4.6 ± 0.9 | 4.6 ± 0.6 |
| Glucose concentration during WASO (mmol·L−1) | 4.7 ± 0.6 | 4.7 ± 0.6 |
| Experimental Day 7 | ||
| Glucose concentration during time in bed (mmol·L−1) | 5.1 ± 0.1 | 5.1 ± 0.1 |
| Glucose concentration during stage N2 (mmol·L−1) | 5.3 ± 0.5 | 5.1 ± 0.7 |
| Glucose concentration during stage N3 (mmol·L−1) | 5.2 ± 0.6 | 5.1 ± 0.6 |
| Glucose concentration during stage REM (mmol·L−1) | 5.3 ± 0.5 | 5.1 ± 0.7 |
| Glucose concentration during WASO (mmol·L−1) | 5.5 ± 0.7 | 5.1 ± 0.5 |
3.3. The Effect of Time in Bed on Average Glucose Concentration during Sleep Stages
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aronoff, S.L.; Berkowitz, K.; Shreiner, B.; Want, L. Glucose Metabolism and Regulation: Beyond Insulin and Glucagon. Diabetes Spectr. 2004, 17, 8. [Google Scholar] [CrossRef]
- Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Colditz, G.; Liu, S.; Solomon, C.G.; Willett, W.C. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. N. Engl. J. Med. 2001, 345, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Lyssenko, V.; Jonsson, A.; Almgren, P.; Pulizzi, N.; Isomaa, B.; Tuomi, T.; Berglund, G.; Altshuler, D.; Nilsson, P.; Groop, L. Clinical risk factors, DNA variants, and the development of type 2 diabetes. N. Engl. J. Med. 2008, 359, 2220–2232. [Google Scholar] [CrossRef] [PubMed]
- Holliday, E.G.; Magee, C.A.; Kritharides, L.; Banks, E.; Attia, J. Short sleep duration is associated with risk of future diabetes but not cardiovascular disease: A prospective study and meta-analysis. PLoS ONE 2013, 8, e82305. [Google Scholar] [CrossRef] [PubMed]
- Iftikhar, I.H.; Donley, M.A.; Mindel, J.; Pleister, A.; Soriano, S.; Magalang, U.J. Sleep Duration and Metabolic Syndrome. An Updated Dose-Risk Metaanalysis. Ann. Am. Thorac. Soc. 2015, 12, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Ju, S.Y.; Choi, W.S. Sleep duration and metabolic syndrome in adult populations: A meta-analysis of observational studies. Nutr. Diabetes 2013, 3, e65. [Google Scholar] [CrossRef] [PubMed]
- Wu, I.H.; Heredia, N.; Dong, Q.; McNeill, L.H.; Balachandran, D.D.; Lu, Q.; Chang, S. Sleep duration and type 2 diabetes risk: A prospective study in a population-based Mexican American cohort. Sleep Health 2021, 7, 168–176. [Google Scholar] [CrossRef]
- Wang, X.; Greer, J.; Porter, R.R.; Kaur, K.; Youngstedt, S.D. Short-term moderate sleep restriction decreases insulin sensitivity in young healthy adults. Sleep Health 2016, 2, 63–68. [Google Scholar] [CrossRef]
- Zhu, B.; Shi, C.; Park, C.G.; Zhao, X.; Reutrakul, S. Effects of sleep restriction on metabolism-related parameters in healthy adults: A comprehensive review and meta-analysis of randomized controlled trials. Sleep Med. Rev. 2019, 45, 18–30. [Google Scholar] [CrossRef]
- Spiegel, K.; Leproult, R.; Van Cauter, E. Impact of sleep debt on metabolic and endocrine function. Lancet 1999, 354, 1435–1439. [Google Scholar] [CrossRef]
- Donga, E.; Van Dijk, M.; Van Dijk, J.G.; Biermasz, N.R.; Lammers, G.-J.; Van Kralingen, K.W.; Corssmit, E.P.M.; Romijn, J.A. A single night of partial sleep deprivation induces insulin resistance in multiple metabolic pathways in healthy subjects. J. Clin. Endocrinol. Metab. 2010, 95, 2963–2968. [Google Scholar] [CrossRef]
- Sweeney, E.L.; Peart, D.J.; Kyza, I.; Harkes, T.; Ellis, J.G.; Walshe, I.H. Impaired Insulin Profiles Following a Single Night of Sleep Restriction: The Impact of Acute Sprint Interval Exercise. Int. J. Sport Nutr. Exerc. Metab. 2020, 30, 139–144. [Google Scholar] [CrossRef]
- Buxton, O.M.; Pavlova, M.; Reid, E.W.; Wang, W.; Simonson, D.C.; Adler, G.K. Sleep restriction for 1 week reduces insulin sensitivity in healthy men. Diabetes 2010, 59, 2126–2133. [Google Scholar] [CrossRef]
- Leung, G.K.W.; Huggins, C.E.; Ware, R.S.; Bonham, M.P. Time of day difference in postprandial glucose and insulin responses: Systematic review and meta-analysis of acute postprandial studies. Chronobiol. Int. 2020, 37, 311–326. [Google Scholar] [CrossRef]
- Davis, R.; Bonham, M.P.; Nguo, K.; Huggins, C.E. Glycaemic response at night is improved after eating a high protein meal compared with a standard meal: A cross-over study. Clin. Nutr. 2020, 39, 1510–1516. [Google Scholar] [CrossRef]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef]
- Belenky, G.; Wesensten, N.J.; Thorne, D.R.; Thomas, M.L.; Sing, H.C.; Redmond, D.P.; Russo, M.B.; Balkin, T.J. Patterns of performance degradation and restoration during sleep restriction and subsequent recovery: A sleep dose-response study. J. Sleep Res. 2003, 12, 1–12. [Google Scholar] [CrossRef]
- Van Dongen, H.P.; Maislin, G.; Mullington, J.M.; Dinges, D.F. The cumulative cost of additional wakefulness: Dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep 2003, 26, 117–126. [Google Scholar] [CrossRef]
- Bialasiewicz, P.; Pawlowski, M.; Nowak, D.; Loba, J.; Czupryniak, L. Decreasing concentration of interstitial glucose in REM sleep in subjects with normal glucose tolerance. Diabet. Med. J. Br. Diabet. Assoc. 2009, 26, 339–344. [Google Scholar] [CrossRef]
- Boyle, P.J.; Scott, J.C.; Andrew, J.; Krentz, R.J.N.; Comstock, E.; Hoffman, C. Diminished brain glucose, metabolism is a significant determiniant for falling rates of systemic glucose utilisation during sleep in normal humans. J. Clin. Investig. 1994, 93, 7. [Google Scholar] [CrossRef]
- Clore, J.N.; Nestler, J.E.; Blackard, W.G. Sleep-associated fall in glucose disposal and hepatic glucose output in normal humans. Putative signaling mechanism linking peripheral and hepatic events. Diabetes 1989, 38, 285–290. [Google Scholar]
- Brandt, R.; Chapotot, F.; Rashid, M.; Broussard, J.; Cinar, A.; Tasali, E. 0109 Slow Wave Sleep and REM Sleep Differentially Affect Nocturnal Glucose Levels. Sleep 2019, 42, A45. [Google Scholar] [CrossRef]
- Dawson, A.; Abel, S.L.; Loving, R.T.; Dailey, G.; Shadan, F.F.; Cronin, J.W.; Kripke, D.F.; Kline, L.E. CPAP therapy of obstructive sleep apnea in type 2 diabetics improves glycemic control during sleep. J. Clin. Sleep Med. 2008, 4, 538–542. [Google Scholar] [CrossRef]
- Broussard, J.L.; Chapotot, F.; Abraham, V.; Day, A.; Delebecque, F.; Whitmore, H.R.; Tasali, E. Sleep restriction increases free fatty acids in healthy men. Diabetologia 2015, 58, 791–798. [Google Scholar] [CrossRef]
- Reynolds, A.C.; Dorrian, J.; Liu, P.Y.; Van Dongen, H.P.; Wittert, G.A.; Harmer, L.J.; Banks, S. Impact of five nights of sleep restriction on glucose metabolism, leptin and testosterone in young adult men. PLoS ONE 2012, 7, e41218. [Google Scholar] [CrossRef]
- Iber, C. The AASM Manual for the Scoring of Sleep and Associated Events: Rules Terminology and Technical Specification; American Academy of Medicine: Westchester, IL, USA, 2007. [Google Scholar]
- Roach, G.D.; Schmidt, W.F.; Aughey, R.; Bourdon, P.C.; Soria, R.; Claros, J.C.J.; Garvican-Lewis, L.A.; Buchheit, M.; Simpson, B.M.; Hammond, K.; et al. The sleep of elite athletes at sea level and high altitude: A comparison of sea-level natives and high-altitude natives (ISA3600). Br. J. Sports Med. 2013, 47, i114–i120. [Google Scholar] [CrossRef]
- Rosenberger, M.E.; Haskell, W.L.; Albinali, F.; Mota, S.; Nawyn, J.; Intille, S. Estimating activity and sedentary behavior from an accelerometer on the hip or wrist. Med. Sci. Sports Exerc. 2013, 45, 964–975. [Google Scholar] [CrossRef]
- Boivin, D.B.; Duffy, J.F.; Kronauer, R.E.; Czeisler, C.A. Dose-response relationships for resetting of human circadian clock by light. Nature 1996, 379, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Roza, A.M.; Shizgal, H.M. The Harris Benedict equation reevaluated: Resting energy requirements and the body cell mass. Am. J. Clin. Nutr. 1984, 40, 168–182. [Google Scholar] [CrossRef] [PubMed]
- Black, A.E. Physical activity levels from a meta-analysis of doubly labeled water studies for validating energy intake as measured by dietary assessment. Nutr. Rev. 1996, 54, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Douglas, C.C.; Lawrence, J.C.; Bush, N.C.; Oster, R.A.; Gower, B.A.; Darnell, B.E. Ability of the Harris Benedict formula to predict energy requirements differs with weight history and ethnicity. Nutr. Res. 2007, 27, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Kontou, T.G.; Sargent, C.; Roach, G.D. Glucose Concentrations from Continuous Glucose Monitoring Devices Compared to those from Blood Plasma During an Oral Glucose Tolerance Test in Healthy Participants. Int. J. Environ. Res. Public Health 2021, 11, 12994. [Google Scholar] [CrossRef]
- Monnier, L.; Colette, C. Target for glycemic control: Concentrating on glucose. Diabetes Care 2009, 32 (Suppl. 2), S199–S204. [Google Scholar] [CrossRef]
- Donga, E.; van Dijk, M.; van Dijk, J.G.; Biermasz, N.R.; Lammers, G.-J.; van Kralingen, K.; Hoogma, R.P.; Corssmit, E.P.; Romijn, J.A. Partial sleep restriction decreases insulin sensitivity in type 1 diabetes. Diabetes Care 2010, 33, 1573–1577. [Google Scholar] [CrossRef]
- Buxton, O.M.; Cain, S.W.; O’Connor, S.P.; Porter, J.H.; Duffy, J.F.; Wang, W.; Czeisler, C.A.; Shea, S.A. Adverse metabolic consequences in humans of prolonged sleep restriction combined with circadian disruption. Sci. Transl. Med. 2012, 4, 129ra143. [Google Scholar] [CrossRef]
- Nedeltcheva, A.V.; Kessler, L.; Imperial, J.; Penev, P.D. Exposure to recurrent sleep restriction in the setting of high caloric intake and physical inactivity results in increased insulin resistance and reduced glucose tolerance. J. Clin. Endocrinol. Metab. 2009, 94, 3242–3250. [Google Scholar] [CrossRef]
- Schmid, S.M.; Hallschmid, M.; Jauch-Chara, K.; Wilms, B.; Lehnert, H.; Born, J.; Schultes, B. Disturbed glucoregulatory response to food intake after moderate sleep restriction. Sleep 2011, 34, 371–377. [Google Scholar] [CrossRef]
- The Royal Australian College of General Practitioners. Management of Type 2 Diabetes: A Handbook for General Practice; Royal Australian College of General Practitioners: East Melbourne, VIC, Australia, 2020. [Google Scholar]
- Tasali, E.; Leproult, R.; Ehrmann, D.A.; Van Cauter, E. Slow-wave sleep and the risk of type 2 diabetes in humans. Proc. Natl. Acad. Sci. USA 2008, 105, 1044–1049. [Google Scholar] [CrossRef]
- Herzog, N.; Jauch-Chara, K.; Hyzy, F.; Richter, A.; Friedrich, A.; Benedict, C.; Oltmanns, K.M. Selective slow wave sleep but not rapid eye movement sleep suppression impairs morning glucose tolerance in healthy men. Psychoneuroendocrinology 2013, 38, 2075–2082. [Google Scholar] [CrossRef]
- Gonnissen, H.K.; Hursel, R.; Rutters, F.; Martens, E.A.; Westerterp-Plantenga, M.S. Effects of sleep fragmentation on appetite and related hormone concentrations over 24 h in healthy men. Br. J. Nutr. 2013, 109, 748–756. [Google Scholar] [CrossRef]
- Bosy-Westphal, A.; Hinrichs, S.; Jauch-Chara, K.; Hitze, B.; Later, W.; Wilms, B.; Settler, U.; Peters, A.; Kiosz, D.; Müller, M.J. Influence of partial sleep deprivation on energy balance and insulin sensitivity in healthy women. Obes. Facts 2008, 1, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007, 116, 1081. [Google Scholar] [CrossRef] [PubMed]
- Mikus, C.R.; Oberlin, D.J.; Libla, J.L.; Taylor, A.M.; Booth, F.W.; Thyfault, J.P. Lowering physical activity impairs glycemic control in healthy volunteers. Med. Sci. Sports Exerc. 2012, 44, 225. [Google Scholar] [CrossRef] [PubMed]
- Vincent, G.E.; Jay, S.M.; Sargent, C.; Kovac, K.; Vandelanotte, C.; Ridgers, N.D.; Ferguson, S.A. The impact of breaking up prolonged sitting on glucose metabolism and cognitive function when sleep is restricted. Neurobiol. Sleep Circadian Rhythm. 2018, 4, 17–23. [Google Scholar] [CrossRef]
- Spaeth, A.M.; Dinges, D.F.; Goel, N. Effects of Experimental Sleep Restriction on Weight Gain, Caloric Intake, and Meal Timing in Healthy Adults. Sleep 2013, 36, 981–990. [Google Scholar] [CrossRef]
- Luckhaupt, S.E.; Tak, S.; Calvert, G.M. The Prevalence of Short Sleep Duration by Industry and Occupation in the National Health Interview Survey. Sleep 2010, 33, 12. [Google Scholar] [CrossRef]
- Härmä, M.; Suvanto, S.; Popkin, S.; Pulli, K.; Mulder, M.; Hirvonen, K. A dose–response study of total sleep time and the ability to maintain wakefulness. J. Sleep Res. 1998, 7, 167–174. [Google Scholar] [CrossRef]

| Variable | Condition | |
|---|---|---|
| 9 h | 5 h | |
| Breakfast | ||
| Protein (%) | 17 ± 2 | 17 ± 3 |
| Fat (%) | 25 ± 3 | 26 ± 4 |
| Carbohydrate (%) | 59 ± 6 | 58 ± 5 |
| Energy (kJ) | 2309 ± 265 | 2301 ± 284 |
| Lunch | ||
| Protein (%) | 23 ± 5 | 22 ± 5 |
| Fat (%) | 40 ± 13 | 43 ± 13 |
| Carbohydrate (%) | 37 ± 6 | 35 ± 8 |
| Energy (kJ) | 2545 ± 623 | 2848 ± 733 |
| Afternoon Snack | ||
| Protein (%) | 18 ± 6 | 19 ± 6 |
| Fat (%) | 48 ± 13 | 47 ± 14 |
| Carbohydrate (%) | 33 ± 7 | 35 ± 7 |
| Energy (kJ) | 2371 ± 624 | 2616 ± 691 |
| Dinner | ||
| Protein (%) | 25 ± 17 | 24 ± 4 |
| Fat (%) | 40 ± 29 | 40 ± 13 |
| Carbohydrate (%) | 36 ± 6 | 36 ± 4 |
| Energy (kJ) | 2992 ± 644 | 3183 ± 662 |
| Evening Snack | ||
| Protein (%) | 13 ± 3 | 12 ± 2 |
| Fat (%) | 32 ± 12 | 31 ± 15 |
| Carbohydrate (%) | 56 ± 19 | 56 ± 15 |
| Energy (kJ) | 1056 ± 358 | 1017 ± 322 |
| Variable | Condition | F | p-Value | |
|---|---|---|---|---|
| 9 h | 5 h | |||
| Baseline | ||||
| TST (min) | 477.7 ± 40.0 | 490.6 ± 22.5 | 1.45 | 0.236 |
| Stage N2 (min) | 199.8 ± 28.2 | 217.0 ± 37.5 | 2.53 | 0.120 |
| Stage N3 (min) | 124.0 ± 33.8 | 118.6 ± 35.0 | 0.23 | 0.639 |
| Stage REM (min) | 121.33 ± 25.5 | 126.7 ± 24.3 | 0.43 | 0.567 |
| WASO (min) | 41.1 ± 26.3 | 32.9 ± 20.9 | 1.10 | 0.323 |
| Experimental Day 7 | ||||
| TST (min) | 465.7 ± 40.9 | 292.1 ± 4.9 | 336.8 | <0.001 |
| Stage N2 (min) | 196.3 ± 36.5 | 83.7 ± 19.5 | 148.1 | <0.001 |
| Stage N3 (min) | 120.2 ± 45.9 | 119.3 ± 25.0 | 0.01 | 0.940 |
| Stage REM (min) | 118.4 ± 20.7 | 81.1 ± 16.3 | 42.0 | <0.001 |
| WASO (min) | 48.7 ± 30.5 | 6.1 ± 4.5 | 36.3 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kontou, T.G.; Sargent, C.; Roach, G.D. A Week of Sleep Restriction Does Not Affect Nighttime Glucose Concentration in Healthy Adult Males When Slow-Wave Sleep Is Maintained. Sensors 2022, 22, 6962. https://doi.org/10.3390/s22186962
Kontou TG, Sargent C, Roach GD. A Week of Sleep Restriction Does Not Affect Nighttime Glucose Concentration in Healthy Adult Males When Slow-Wave Sleep Is Maintained. Sensors. 2022; 22(18):6962. https://doi.org/10.3390/s22186962
Chicago/Turabian StyleKontou, Thomas G., Charli Sargent, and Gregory D. Roach. 2022. "A Week of Sleep Restriction Does Not Affect Nighttime Glucose Concentration in Healthy Adult Males When Slow-Wave Sleep Is Maintained" Sensors 22, no. 18: 6962. https://doi.org/10.3390/s22186962
APA StyleKontou, T. G., Sargent, C., & Roach, G. D. (2022). A Week of Sleep Restriction Does Not Affect Nighttime Glucose Concentration in Healthy Adult Males When Slow-Wave Sleep Is Maintained. Sensors, 22(18), 6962. https://doi.org/10.3390/s22186962