
Automatic Classification System for Periapical Lesions in Cone-Beam Computed Tomography

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
Related Works
2. Artificial Neural Network
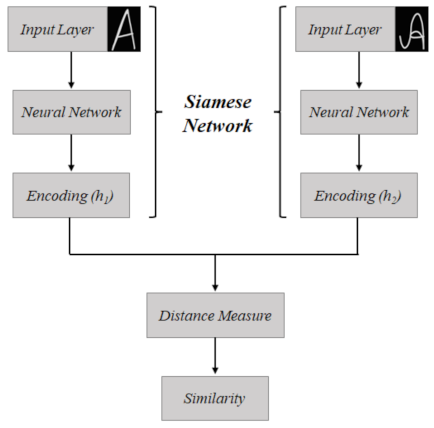
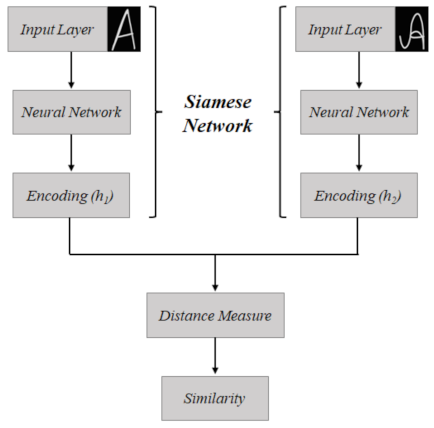
2.1. Siamese Network
2.2. Transfer Learning
3. Imaging Exams in Dentistry
4. Materials and Methods
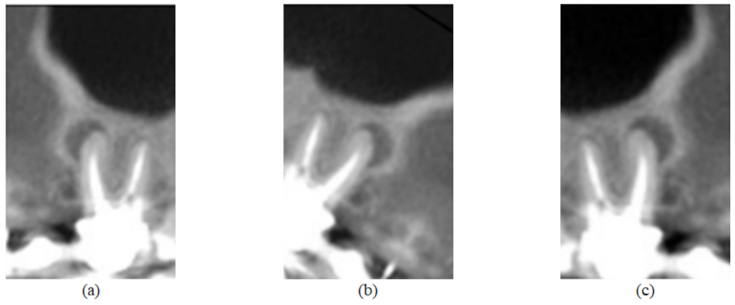
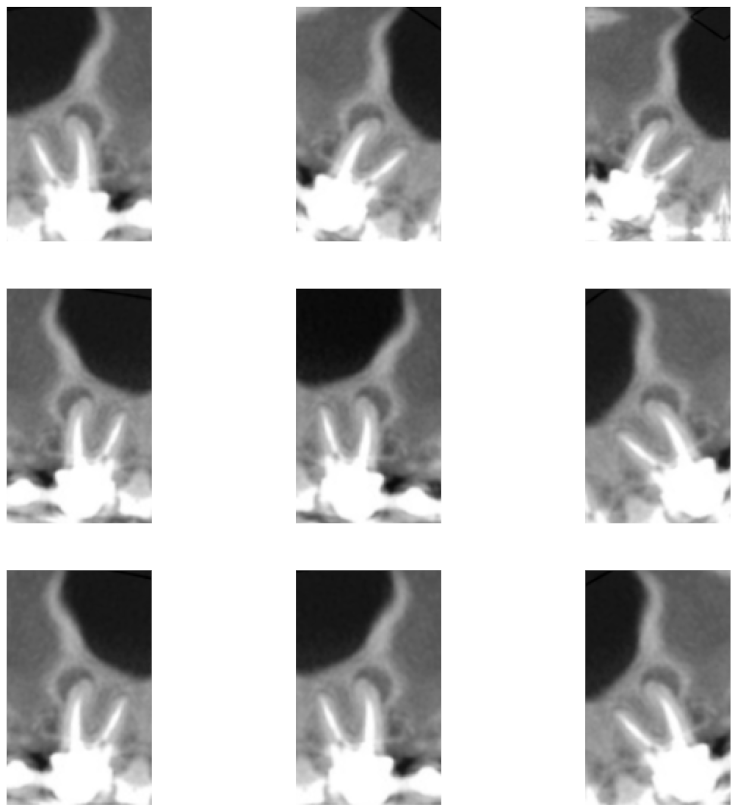
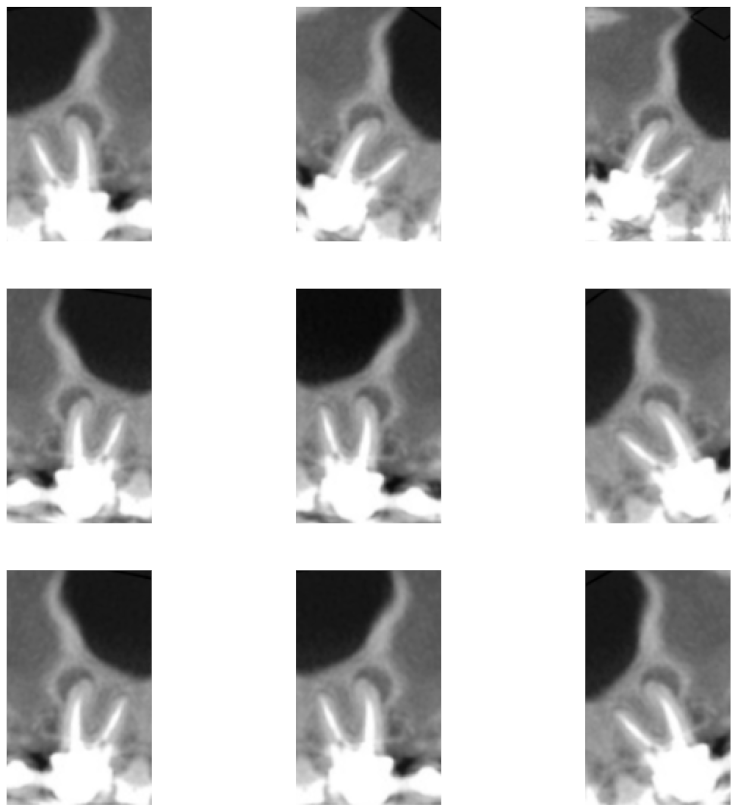
4.1. Database
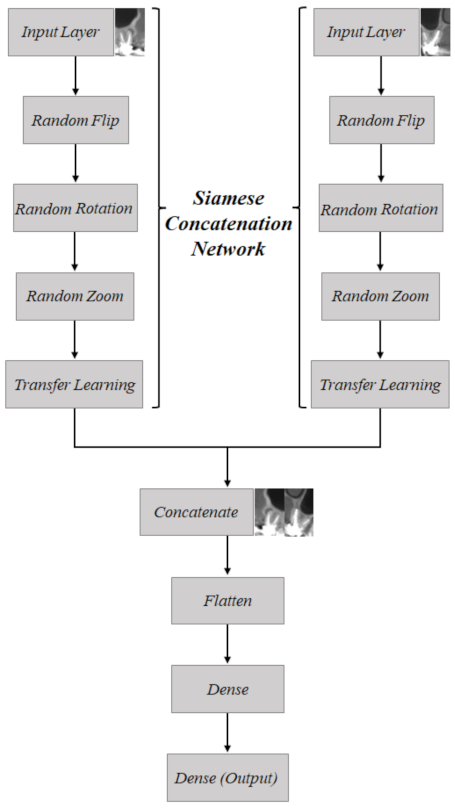
4.2. Proposed System
- Complete base: 1000 pairs of images are considered. It includes the whole set of images presented in this article—that is, teeth without lesion, teeth with small lesion, and teeth with large lesion.
- Base with large lesions: 724 pairs of images, which correspond to cases of teeth without lesion and teeth with large lesion.
- Base with small lesions: 730 pairs of images, which correspond to cases of teeth without lesions and teeth with small lesion.
5. Results and Discussion
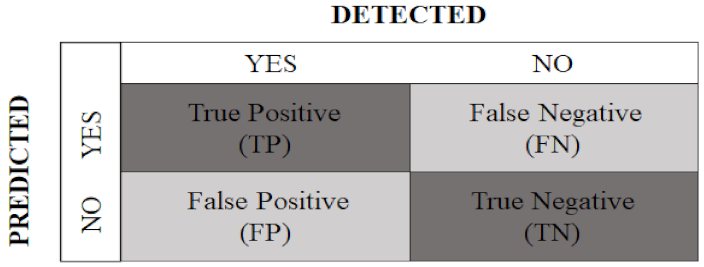
- Accuracy: provides the percentage of successful classifications, among all those performed, given by
- Recall: reports the percentage of true positive ratings among all true ratings, calculated as follows:
- Precision: indicates the percentage of true positive ratings, among all positive ratings, calculated as follows:
- Specificity: presents the percentage of true negative ratings, among all negative ratings, obtained by
- F1-score: calculated as the harmonic mean between recall and precision:
6. Conclusions
- Introduction of an image segmentation step as part of the classification system. It is worth mentioning that authors [65] report benefits of using image segmentation in machine-learning-based classification systems.
- Application of the proposed Siamese Concatenated Network framework in other classification tasks that involve the use of pairs of images.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations and Abbreviations
Abbreviations
Abbreviations
| UPE | Universidade de Pernambuco |
| UFRPE | Universidade Federal Rural de Pernambuco |
| UFPE | Universidade Federal de Pernambuco |
| CBCT | Cone-Beam Computed Tomography |
| CNN | Convolutional Neural Network |
| ANN | Artificial Neural Network |
| ILSVRC | ImageNet Large-Scale Visual Recognition Challenge |
| VGG | Visual Geometry Group |
| AI | Artificial Intelligence |
| FOV | Field of View |
| ReLU | Rectified Linear Unit |
| TP | True Positive |
| TN | True Negative |
| FP | False Positive |
| FN | False Negative |
References
- Nelson, S.J. Wheeler’s Dental Anatomy, Physiology and Occlusion-E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Scarfe, W.C.; Farman, A.G.; Sukovic, P. Clinical applications of cone-beam computerized tomography in dental practice. J. Can. Dent. Assoc. 2006, 72, 75–80. [Google Scholar] [PubMed]
- Garib, D.G.; Raymundo, R., Jr.; Raymundo, M.V.; Raymundo, D.V.; Ferreira, S.N. Tomografia computadorizada de feixe cônico (Cone beam): Entendendo este novo método de diagnóstico por imagem com promissora aplicabilidade na Ortodontia. Rev. Dent. Press Ortod. E Ortop. Facial 2007, 12, 139–156. [Google Scholar] [CrossRef]
- Mozzo, P.; Procacci, C.; Tacconi, A.; Martini, P.T.; Andreis, I.B. A new volumetric CT machine for dental imaging based on the cone-beam technique: Preliminary results. Eur. Radiol. 1998, 8, 1558–1564. [Google Scholar] [CrossRef] [PubMed]
- Ludlow, J.B.; Ivanovic, M. Comparative dosimetry of dental CBCT devices and 64-slice CT for oral and maxillofacial radiology. Oral Surgery Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 106, 106–114. [Google Scholar] [CrossRef]
- Costa, C.C.A.; Moura-Netto, C.; Koubik, A.C.G.A.; Michelotto, A.L.C. Aplicações clínicas da tomografia computadorizada cone beam na endodontia. J. Health Sci. Inst. 2009, 27, 279–286. [Google Scholar]
- Aminoshariae, A.; Kulild, J.; Nagendrababu, V. Artificial intelligence in endodontics: Current applications and future directions. J. Endod. 2021, 47, 1352–1357. [Google Scholar] [CrossRef]
- Kora, P.; Ooi, C.P.; Faust, O.; Raghavendra, U.; Gudigar, A.; Chan, W.Y.; Meenakshi, K.; Swaraja, K.; Plawiak, P.; Rajendra Acharya, U. Transfer learning techniques for medical image analysis: A review. Biocybern. Biomed. Eng. 2021, 42, 79–107. [Google Scholar] [CrossRef]
- Khanagar, S.B.; Al-ehaideb, A.; Maganur, P.C.; Vishwanathaiah, S.; Patil, S.; Baeshen, H.A.; Sarode, S.C.; Bhandi, S. Developments, application, and performance of artificial intelligence in dentistry—A systematic review. J. Dent. Sci. 2021, 16, 508–522. [Google Scholar] [CrossRef]
- Moran, M.; Faria, M.; Giraldi, G.; Bastos, L.; Conci, A. Do radiographic assessments of periodontal bone loss improve with deep learning methods for enhanced image resolution? Sensors 2021, 21, 2013. [Google Scholar] [CrossRef]
- Wang, C.W.; Huang, C.T.; Lee, J.H.; Li, C.-H. A benchmark for comparison of dental radiography analysis algorithms. Med Image Anal. 2016, 31, 63–76. [Google Scholar] [CrossRef]
- Schwendicke, F.; Golla, T.; Dreher, M.; Krois, J. Convolutional neural networks for dental image diagnostics: A scoping review. J. Dent. 2019, 91, 103226. [Google Scholar] [CrossRef]
- Shen, C.; Nguyen, D.; Zhou, Z.; Jiang, S.B.; Dong, B.; Jia, X. An introduction to deep learning in medical physics: Advantages, potential, and challenges. Phys. Med. Biol. 2020, 65, 05TR01. [Google Scholar] [CrossRef] [PubMed]
- Montero, A.B.; Javaid, U.; Valdés, G.; Nguyen, D.; Desbordes, P.; Macq, B.; Willems, S.; Vandewinckele, L.; Holmström, M.; Löfman, F.; et al. Artificial intelligence and machine learning for medical imaging: A technology review. Phys. Medica 2021, 83, 242–256. [Google Scholar] [CrossRef] [PubMed]
- Son, L.H.; Tuan, T.M.; Fujita, H.; Dey, N.; Ashour, A.S.; Ngoc, V.T.N.; Anh, L.Q.; Chu, D.T. Dental diagnosis from X-Ray images: An expert system based on fuzzy computing. Biomed. Signal Process. Control 2018, 39, 64–73. [Google Scholar] [CrossRef]
- Root and canal morphology of maxillary premolars and their relationship with the crown morphology. J. Oral Biosci. 2022, 64, 148–154. [CrossRef]
- Girão, R.S.; Aguiar-Oliveira, M.H.; Andrade, B.M.; Bittencourt, M.A.; Salvatori, R.; Silva, E.V.; Santos, A.L.; Cunha, M.M.; Takeshita, W.M.; Oliveira, A.H.; et al. Dental arches in inherited severe isolated growth hormone deficiency. Growth Horm. IGF Res. 2022, 62, 101444. [Google Scholar] [CrossRef]
- Ghoncheh, Z.; Zade, B.M.; Kharazifard, M.J. Root morphology of the maxillary first and second molars in an Iranian population using cone beam computed tomography. J. Dent. 2017, 14, 115. [Google Scholar]
- Galler, K.M.; Weber, M.; Korkmaz, Y.; Widbiller, M.; Feuerer, M. Inflammatory response mechanisms of the dentine–pulp complex and the periapical tissues. Int. J. Mol. Sci. 2021, 22, 1480. [Google Scholar] [CrossRef] [PubMed]
- Kruse, C.; Spin-Neto, R.; Wenzel, A.; Kirkevang, L.L. Cone beam computed tomography and periapical lesions: A systematic review analysing studies on diagnostic efficacy by a hierarchical model. Int. Endod. J. 2015, 48, 815–828. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Tang, R.; Gao, A.; Hao, Y.; Lin, Z. Cross-sectional study of posterior tooth root fractures in 2015 and 2019 in a Chinese population. Clin. Oral Investig. 2022, 2, 1–7. [Google Scholar] [CrossRef]
- Pauwels, R.; Araki, K.; Siewerdsen, J.; Thongvigitmanee, S.S. Technical aspects of dental CBCT: State of the art. Dentomaxillofacial Radiol. 2015, 44, 20140224. [Google Scholar] [CrossRef] [PubMed]
- Setzer, F.C.; Shi, K.J.; Zhang, Z.; Yan, H.; Yoon, H.; Mupparapu, M.; Li, J. Artificial intelligence for the computer-aided detection of periapical lesions in cone-beam computed tomographic images. J. Endod. 2020, 46, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Yan, H.; Setzer, F.C.; Shi, K.J.; Mupparapu, M.; Li, J. Anatomically constrained deep learning for automating dental CBCT segmentation and lesion detection. IEEE Trans. Autom. Sci. Eng. 2021, 18, 603–614. [Google Scholar] [CrossRef]
- Endres, M.G.; Hillen, F.; Salloumis, M.; Sedaghat, A.R.; Niehues, S.M.; Quatela, O.; Hanken, H.; Smeets, R.; Beck-Broichsitter, B.; Rendenbach, C.; et al. Development of a deep learning algorithm for periapical disease detection in dental radiographs. Diagnostics 2020, 10, 430. [Google Scholar] [CrossRef]
- Koch, G.; Zemel, R.; Salakhutdinov, R. Siamese neural networks for one-shot image recognition. In Proceedings of the International Conference on Machine Learning (ICML), Lille, France, 6–1 July 2015; Volume 2. [Google Scholar]
- Huang, G.; Liu, Z.; Maaten, L.V.; Weinberger, K.Q. Densely connected convolutional Networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.; van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef]
- Miki, Y.; Muramatsu, C.; Hayashi, T.; Zhou, X.; Hara, T.; Katsumata, A.; Fujita, H. Classification of teeth in cone-beam CT using deep convolutional neural network. Comput. Biol. Med. 2017, 80, 24–29. [Google Scholar] [CrossRef]
- Khanagar, S.B.; Vishwanathaiah, S.; Naik, S.; A. Al-Kheraif, A.; Devang Divakar, D.; Sarode, S.C.; Bhandi, S.; Patil, S. Application and performance of artificial intelligence technology in forensic odontology—A systematic review. Leg. Med. 2021, 48, 101826. [Google Scholar] [CrossRef]
- Lee, J.H.; Jeong, S.N. Efficacy of deep convolutional neural network algorithm for the identification and classification of dental implant systems, using panoramic and periapical radiographs: A pilot study. Medicine 2020, 99, e20787. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, D.H.; Jeong, S.N.; Choi, S.H. Detection and diagnosis of dental caries using a deep learning-based convolutional neural network algorithm. J. Dent. 2018, 77, 106–111. [Google Scholar] [CrossRef]
- Choi, J.; Eun, H.; Kim, C. Boosting proximal dental caries detection via combination of variational methods and convolutional neural network. J. Signal Process. Syst. 2018, 90, 87–97. [Google Scholar] [CrossRef]
- Haghanifar, A.; Majdabadi, M.M.; Ko, S.B. Automated teeth extraction from dental panoramic x-ray images using genetic algorithm. In Proceedings of the 2020 IEEE International Symposium on Circuits and Systems (ISCAS), Seville, Spain, 12–14 October 2020; IEEE: New York, NY, USA, 2020; pp. 1–5. [Google Scholar]
- Leo, L.M.; Reddy, T.K. Learning compact and discriminative hybrid neural network for dental caries classification. Microprocess. Microsystems 2021, 82, 103836. [Google Scholar]
- Kim, J.; Lee, H.S.; Song, I.S.; Jung, K.H. DeNTNet: Deep neural transfer network for the detection of periodontal bone loss using panoramic dental radiographs. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, D.H.; Jeong, S.N.; Choi, S.H. Diagnosis and prediction of periodontally compromised teeth using a deep learning-based convolutional neural network algorithm. J. Periodontal Implant Sci. 2018, 48, 114–123. [Google Scholar] [CrossRef] [Green Version]
- Ezhov, M.; Gusarev, M.; Golitsyna, M.; Yates, J.M.; Kushnerev, E.; Tamimi, D.; Aksoy, S.; Shumilov, E.; Sanders, A.; Orhan, K. Clinically applicable artificial intelligence system for dental diagnosis with CBCT. Sci. Rep. 2021, 11, 1–16. [Google Scholar] [CrossRef]
- Haykin, S. Neural Networks and Learning Machines; Pearson Education: London, UK, 2009. [Google Scholar]
- Simard, P.Y.; LeCun, Y.A.; Denker, J.S.; Victorri, B. Transformation invariance in pattern recognition—Tangent distance and tangent propagation. In Neural Networks: Tricks of the Trade; Springer: Berlin/Heidelberg, Germany, 1998; pp. 239–274. [Google Scholar]
- Hubel, D.H.; Wiesel, T.N. Receptive fields, binocular interaction and functional architecture in the cat’s visual cortex. J. Physiol. 1962, 160, 106–154. [Google Scholar] [CrossRef]
- Hubel, D.H.; Wiesel, T.N. Receptive fields and functional architecture of monkey striate cortex. J. Physiol. 1968, 195, 215–243. [Google Scholar] [CrossRef]
- O’Shea, K.; Nash, R. An introduction to convolutional neural networks. arXiv 2015, arXiv:1511.08458. [Google Scholar]
- Zhuang, F.; Qi, Z.; Duan, K.; Xi, D.; Zhu, Y.; Zhu, H.; Xiong, H.; He, Q. A comprehensive survey on transfer learning. Proc. IEEE 2020, 109, 43–76. [Google Scholar] [CrossRef]
- Bromley, J.; Bentz, J.W.; Bottou, L.; Guyon, I.; LeCun, Y.; Moore, C.; Säckinger, E.; Shah, R. Signature verification using a “siamese” time delay neural network. Int. J. Pattern Recognit. Artif. Intell. 1993, 7, 669–688. [Google Scholar] [CrossRef]
- Saedi, C.; Dras, M. Siamese networks for large-scale author identification. Comput. Speech Lang. 2021, 70, 101241. [Google Scholar] [CrossRef]
- Mitchell, B.R.; Cohen, M.C.; Cohen, S. Dealing with multi-dimensional data and the burden of annotation: Easing the burden of annotation. Am. J. Pathol. 2021, 191, 1709–1716. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.J.; Yang, Q. A survey on transfer learning. IEEE Trans. Knowl. Data Eng. 2010, 22, 1345–1359. [Google Scholar] [CrossRef]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Fei-Fei, L. ImageNet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar]
- Barua, P.D.; Muhammad Gowdh, N.F.; Rahmat, K.; Ramli, N.; Ng, W.L.; Chan, W.Y.; Kuluozturk, M.; Dogan, S.; Baygin, M.; Yaman, O.; et al. Automatic COVID-19 detection using exemplar hybrid deep features with X-ray images. Int. J. Environ. Res. Public Health 2021, 18, 8052. [Google Scholar] [CrossRef]
- Kang, J.; Ullah, Z.; Gwak, J. MRI-Based brain tumor classification using ensemble of deep features and machine learning classifiers. Sensors 2021, 21, 2222. [Google Scholar] [CrossRef]
- Zhu, Y.; Newsam, S. DenseNet for dense flow. In Proceedings of the 2017 IEEE International Conference on Image Processing (ICIP), Beijing, China, 17–20 September 2017; pp. 790–794. [Google Scholar]
- Durack, C.; Patel, S. Cone beam computed tomography in endodontics. Braz. Dent. J. 2012, 23, 179–191. [Google Scholar] [CrossRef]
- Patel, S.; Brown, J.; Pimentel, T.; Kelly, R.; Abella, F.; Durack, C. Cone beam computed tomography in endodontics—A review of the literature. Int. Endod. J. 2019, 52, 1138–1152. [Google Scholar] [CrossRef]
- Karamifar, K.; Tondari, A.; Saghiri, M.A. Endodontic periapical lesion: An overview on the etiology, diagnosis and current treatment modalities. Eur. Endod. J. 2020, 5, 54. [Google Scholar] [CrossRef]
- Nascimento, E.H.L.; Gaêta-Araujo, H.; Andrade, M.F.S.; Freitas, D.Q. Prevalence of technical errors and periapical lesions in a sample of endodontically treated teeth: A CBCT analysis. Clin. Oral Investig. 2018, 22, 2495–2503. [Google Scholar] [CrossRef]
- Liang, X.; Jacobs, R.; Hassan, B.; Li, L.; Pauwels, R.; Corpas, L.; Souza, P.C.; Martens, W.; Shahbazian, M.; Alonso, A.; et al. A comparative evaluation of cone beam computed tomography (CBCT) and multi-slice CT (MSCT): Part I. On subjective image quality. Eur. J. Radiol. 2010, 75, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Ker, J.; Wang, L.; Rao, J.; Lim, T. Deep learning applications in medical image analysis. IEEE Access 2018, 6, 9375–9389. [Google Scholar] [CrossRef]
- Heo, M.S.; Kim, J.E.; Hwang, J.J.; Han, S.S.; Kim, J.S.; Yi, W.J.; Park, I.W. Artificial intelligence in oral and maxillofacial radiology: What is currently possible? Dentomaxillofacial Radiol. 2021, 50, 20200375. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.C.; Nejaim, Y.; Silva, A.I.; Haiter-Neto, F.; Cohenca, N.; Zaia, A.A.; Silva, E.J.N.L. Influence of endodontic treatment and coronal restoration on status of periapical tissues: A cone-beam computed tomographic study. J. Endod. 2015, 41, 1614–1618. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, T. An introduction to ROC analysis. Pattern Recognit. Lett. 2006, 27, 861–874. [Google Scholar] [CrossRef]
- Kruse, C.; Spin-Neto, R.; Reibel, J.; Wenzel, A.; Kirkevang, L.L. Diagnostic validity of periapical radiography and CBCT for assessing periapical lesions that persist after endodontic surgery. Dentomaxillofacial Radiol. 2017, 46, 20170210. [Google Scholar] [CrossRef]
- Gonzalez, R.C.; Woods, R.C. Digital Image Processing; Pearson India: Noida, India, 2018. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. | Year | CNN Architecture | Dataset | Plane |
|---|---|---|---|---|
| [23] | 2020 | U-Net | 20 CBCT scan images | Coronal |
| [24] | 2020 | U-Net | 20 CBCT scan images | Coronal |
| [25] | 2021 | U-Net | 2902 Panoramic Radiograph images | Coronal |
| [39] | 2021 | Not stated | 2800 CBCT scan images | Sagittal |
| Classification | Number of Samples | Features |
|---|---|---|
| Healthy | 454 | Teeth without lesion |
| Small Lesion | 276 | Teeth with lesion of 0.5 to 1.9 mm |
| Large Lesion | 270 | Teeth with lesion of 2.0 mm or greater |
| Methods | Metrics | ||||
|---|---|---|---|---|---|
| Accuracy | F1-Score | Specificity | Precision | Recall | |
| DenseNet-121 | 0.7000 | 0.6970 | 0.7634 | 0.7582 | 0.6449 |
| VGG-16 | 0.6800 | 0.6832 | 0.7204 | 0.7263 | 0.6449 |
| [25] | — | 0.58 | — | 0.67 | 0.51 |
| Methods | Metrics | ||||
|---|---|---|---|---|---|
| Accuracy | F1-Score | Specificity | Precision | Recall | |
| DenseNet-121 | 0.7917 | 0.6591 | 0.9239 | 0.8055 | 0.5577 |
| VGG-16 | 0.8125 | 0.6582 | 0.9100 | 0.7429 | 0.5910 |
| Methods | Metrics | ||||
|---|---|---|---|---|---|
| Accuracy | F1-score | Specificity | Precision | Recall | |
| DenseNet-121 | 0.6667 | 0.4494 | 0.8571 | 0.6060 | 0.3571 |
| VGG-16 | 0.6599 | 0.4318 | 0.8041 | 0.5000 | 0.3800 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calazans, M.A.A.; Ferreira, F.A.B.S.; Alcoforado, M.d.L.M.G.; Santos, A.d.; Pontual, A.d.A.; Madeiro, F. Automatic Classification System for Periapical Lesions in Cone-Beam Computed Tomography. Sensors 2022, 22, 6481. https://doi.org/10.3390/s22176481
Calazans MAA, Ferreira FABS, Alcoforado MdLMG, Santos Ad, Pontual AdA, Madeiro F. Automatic Classification System for Periapical Lesions in Cone-Beam Computed Tomography. Sensors. 2022; 22(17):6481. https://doi.org/10.3390/s22176481
Chicago/Turabian StyleCalazans, Maria Alice Andrade, Felipe Alberto B. S. Ferreira, Maria de Lourdes Melo Guedes Alcoforado, Andrezza dos Santos, Andréa dos Anjos Pontual, and Francisco Madeiro. 2022. "Automatic Classification System for Periapical Lesions in Cone-Beam Computed Tomography" Sensors 22, no. 17: 6481. https://doi.org/10.3390/s22176481
APA StyleCalazans, M. A. A., Ferreira, F. A. B. S., Alcoforado, M. d. L. M. G., Santos, A. d., Pontual, A. d. A., & Madeiro, F. (2022). Automatic Classification System for Periapical Lesions in Cone-Beam Computed Tomography. Sensors, 22(17), 6481. https://doi.org/10.3390/s22176481