
Machine Learning-Based Predicted Age of the Elderly on the Instrumented Timed Up and Go Test and Six-Minute Walk Test


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
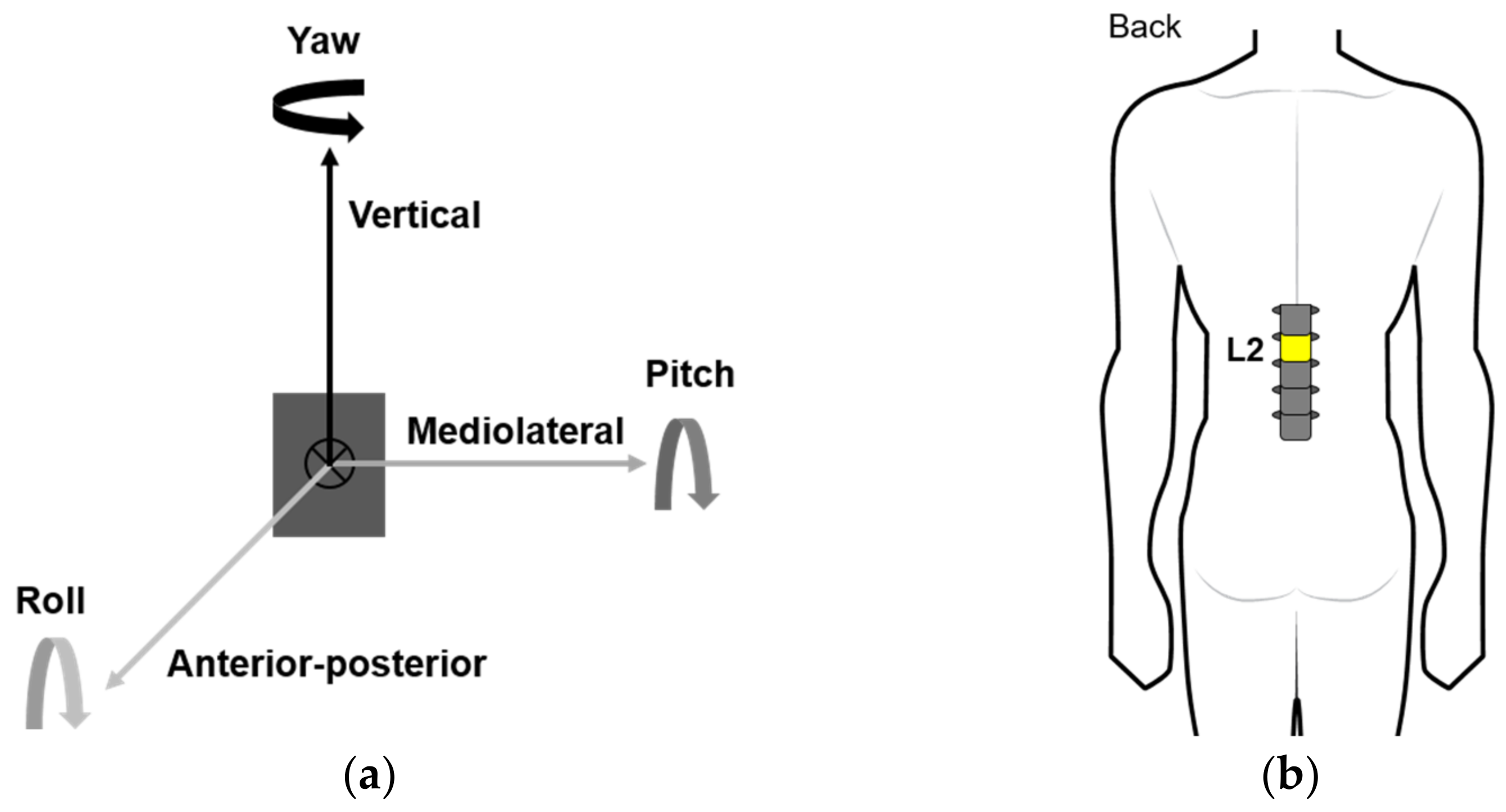
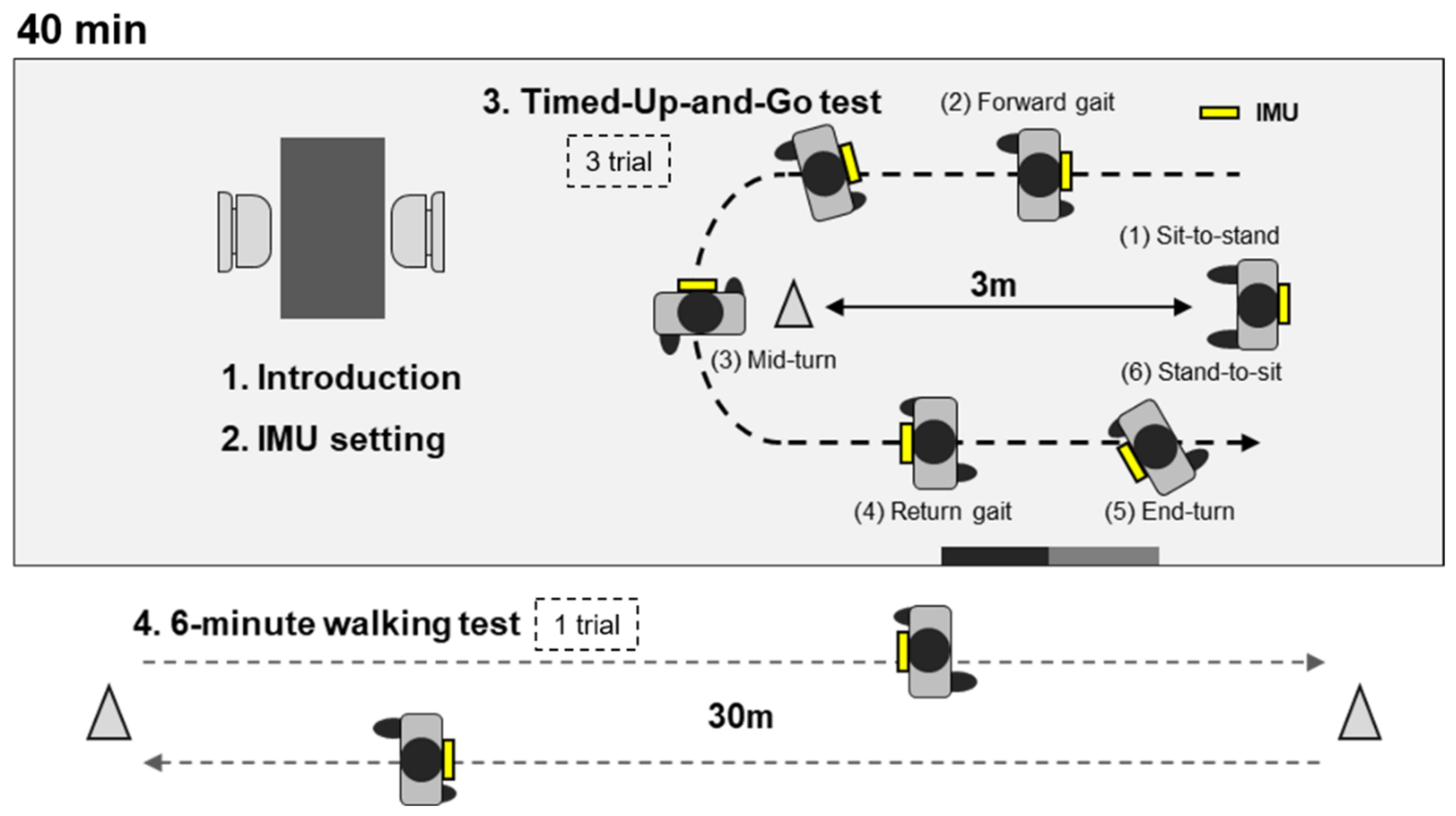
2.2. Data Collection
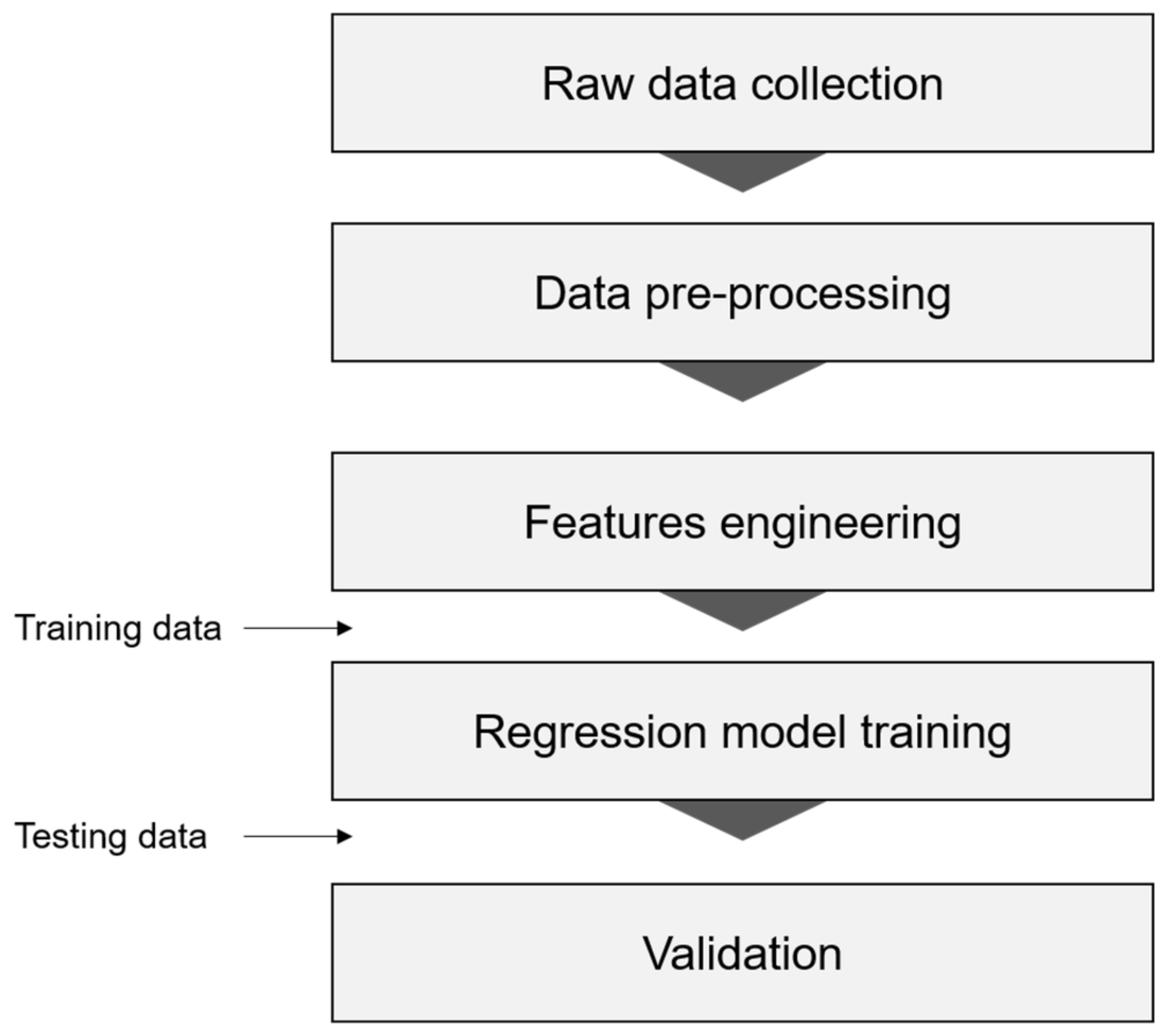
2.3. Data Analysis
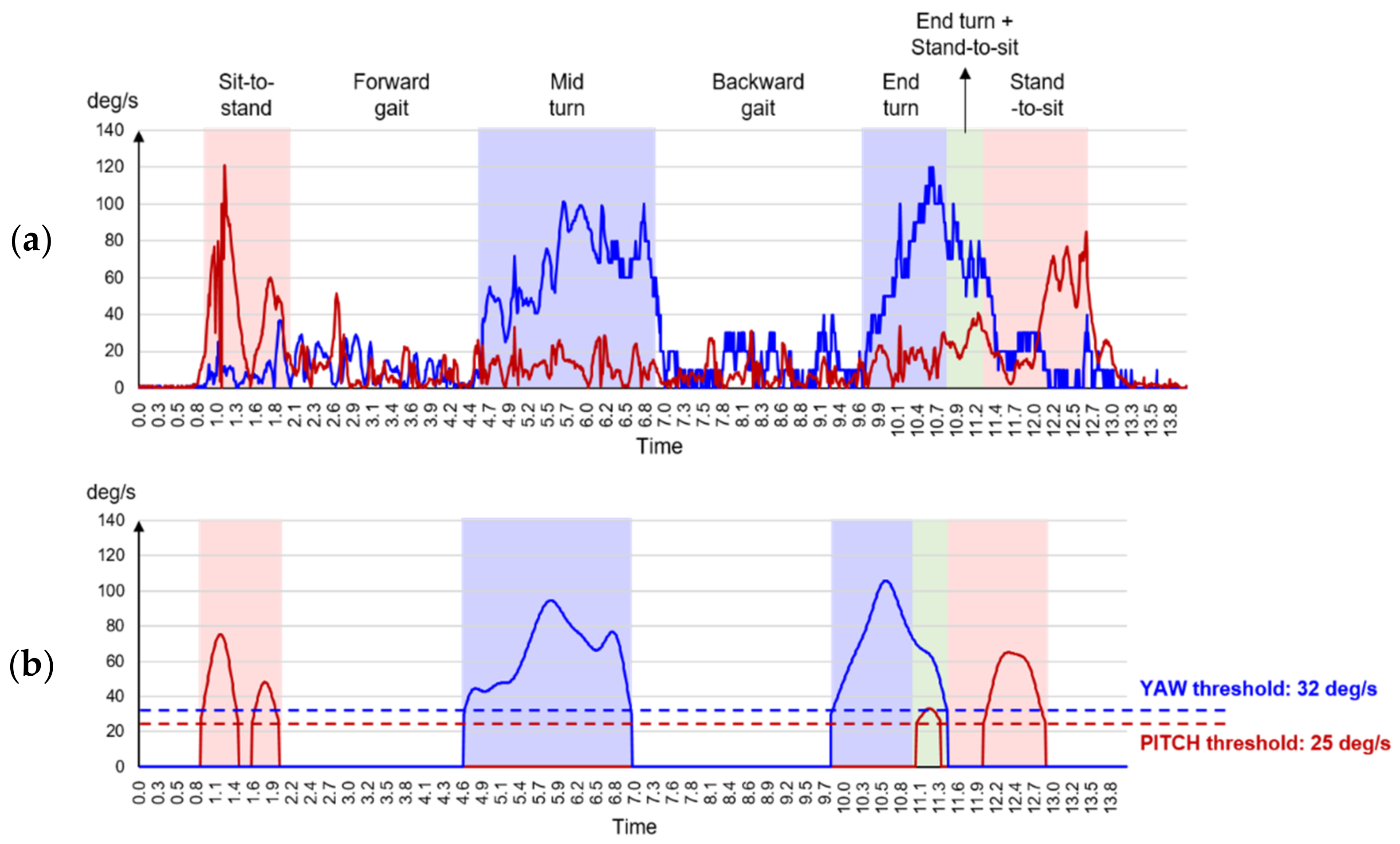
2.3.1. Raw Data Extraction
2.3.2. Data Pre-Processing
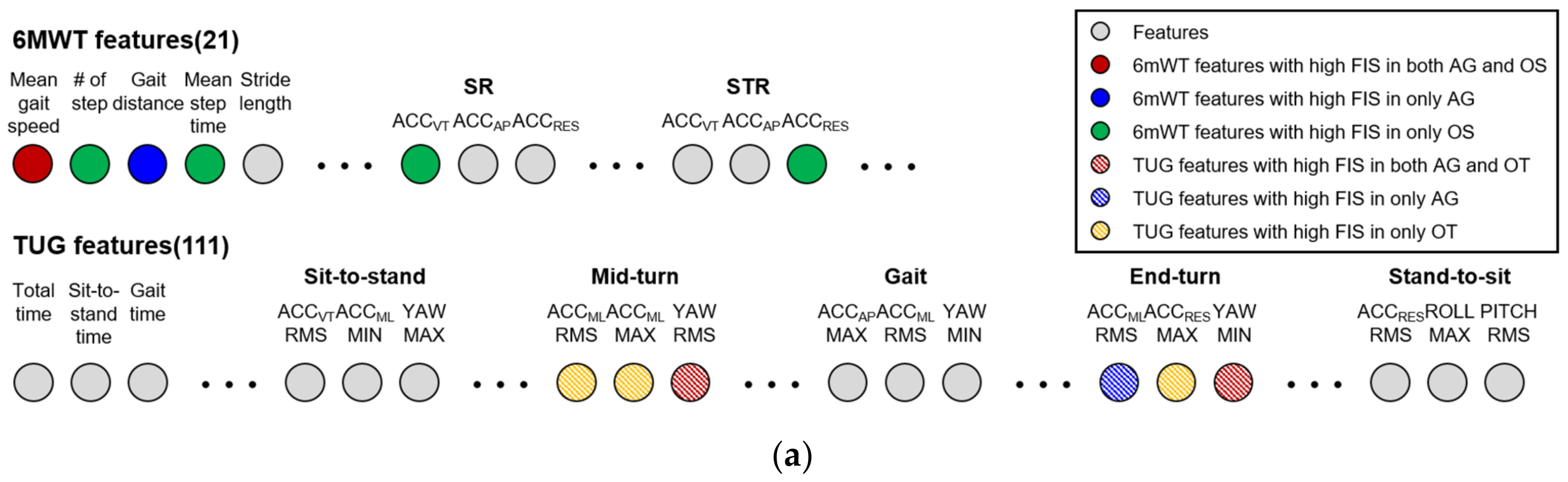
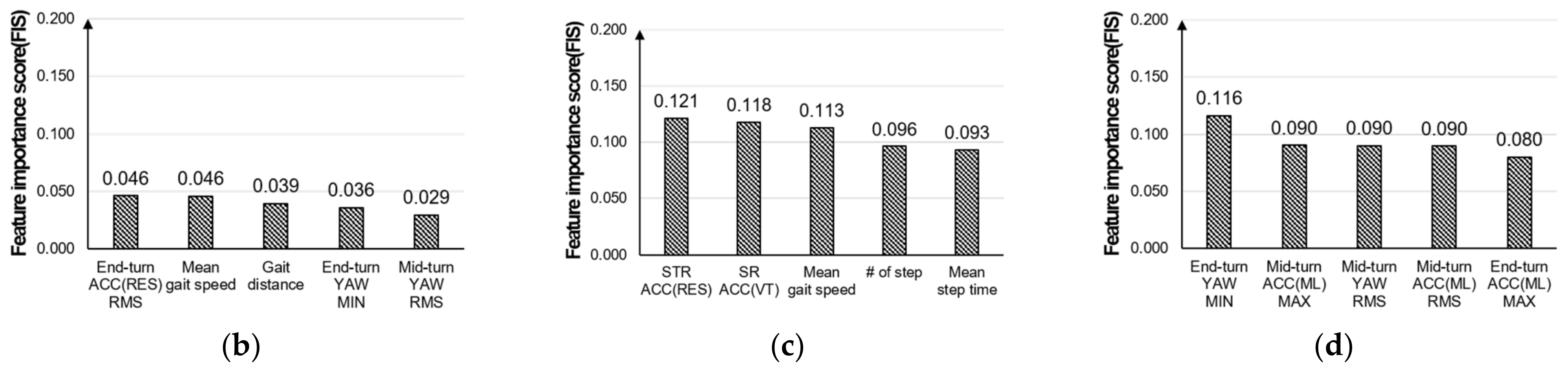
2.3.3. Features Engineering
2.3.4. ML-Based Regression
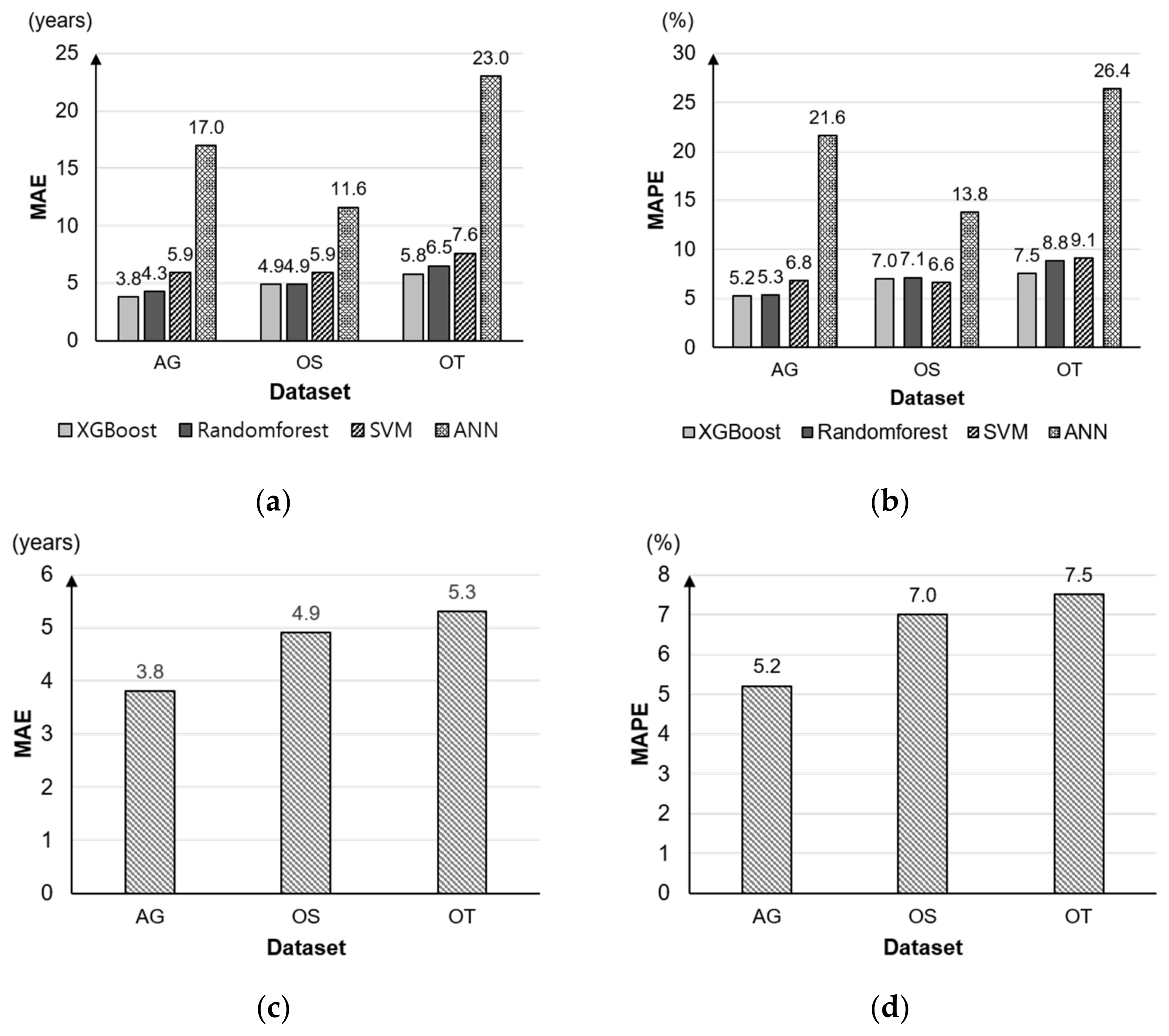
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of Illness in the Aged: The Index of ADL: A Standardized Measure of Biological and Psychosocial Function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Wiener, J.M.; Hanley, R.J.; Clark, R.; Van Nostrand, J.F. Measuring the activities of daily living: Comparisons across national surveys. J. Gerontol. 1990, 45, S229–S237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aloulou, H.; Mokhtari, M.; Abdulrazak, B. Pilot Site Deployment of an IoT Solution for Older Adults’ Early Behavior Change Detection. Sensors 2020, 20, 1888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Onofrio, G.; Fiorini, L.; Toccafondi, L.; Rovini, E.; Russo, S.; Ciccone, F.; Giuliani, F.; Sancarlo, D.; Cavallo, F. Pilots for Healthy and Active Ageing (PHArA-ON) Project: Definition of New Technological Solutions for Older People in Italian Pilot Sites Based on Elicited User Needs. Sensors 2022, 22, 163. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Stroud, M.W., 3rd. Functional assessment in geriatrics. A review of progress and directions. J. Am. Geriatr. Soc. 1989, 37, 267–271. [Google Scholar] [CrossRef]
- Raymakers, J.A.; Samson, M.M.; Verhaar, H.J. The assessment of body sway and the choice of the stability parameter(s). Gait Posture 2005, 21, 48–58. [Google Scholar] [CrossRef]
- Greene, B.R.; Doheny, E.P.; O’Halloran, A.; Anne Kenny, R. Frailty status can be accurately assessed using inertial sensors and the TUG test. Age Ageing 2014, 43, 406–411. [Google Scholar] [CrossRef] [Green Version]
- Novak, A.C.; Komisar, V.; Maki, B.E.; Fernie, G.R. Age-related differences in dynamic balance control during stair descent and effect of varying step geometry. Appl. Ergon. 2016, 52, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Neptune, R.; Vistamehr, A. Dynamic Balance during Human Movement: Measurement and Control Mechanisms. J. Biomech. Eng. 2018, 141, 0708011–07080110. [Google Scholar] [CrossRef]
- Cleary, K.; Skornyakov, E. Predicting falls in older adults using the four square step test. Physiother. Theory Pract. 2017, 33, 766–771. [Google Scholar] [CrossRef]
- Volpato, S.; Cavalieri, M.; Sioulis, F.; Guerra, G.; Maraldi, C.; Zuliani, G.; Fellin, R.; Guralnik, J.M. Predictive value of the Short Physical Performance Battery following hospitalization in older patients. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Gadelha, A.B.; Neri, S.G.R.; Oliveira, R.J.; Bottaro, M.; David, A.C.; Vainshelboim, B.; Lima, R.M. Severity of sarcopenia is associated with postural balance and risk of falls in community-dwelling older women. Exp. Aging Res. 2018, 44, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Caballer, V.B.; Lisón, J.F.; Rosado-Calatayud, P.; Amer-Cuenca, J.J.; Segura-Orti, E. Factors associated with the 6-minute walk test in nursing home residents and community-dwelling older adults. J. Phys. Ther. Sci. 2015, 27, 3571–3578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, R.; Michel, B.; Russo, D.; Mora, N.; Matrella, G.; Ciampolini, P.; Cocchi, F.; Montanari, E.; Nunziata, S.; Brunschwiler, T. An Unsupervised Behavioral Modeling and Alerting System Based on Passive Sensing for Elderly Care. Future Internet 2021, 13, 6. [Google Scholar] [CrossRef]
- Richmond, S.B.; Dames, K.D.; Goble, D.J.; Fling, B.W. Leveling the playing field: Evaluation of a portable instrument for quantifying balance performance. J. Biomech. 2018, 75, 102–107. [Google Scholar] [CrossRef]
- Yorozu, A.; Moriguchi, T.; Takahashi, M. Improved Leg Tracking Considering Gait Phase and Spline-Based Interpolation during Turning Motion in Walk Tests. Sensors 2015, 15, 22451–22472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eltoukhy, M.A.; Kuenze, C.; Oh, J.; Signorile, J.F. Validation of Static and Dynamic Balance Assessment Using Microsoft Kinect for Young and Elderly Populations. IEEE J. Biomed. Health Inform. 2018, 22, 147–153. [Google Scholar] [CrossRef]
- Attal, F.; Mohammed, S.; Dedabrishvili, M.; Chamroukhi, F.; Oukhellou, L.; Amirat, Y. Physical Human Activity Recognition Using Wearable Sensors. Sensors 2015, 15, 31314–31338. [Google Scholar] [CrossRef] [Green Version]
- Arif, M.; Kattan, A. Physical Activities Monitoring Using Wearable Acceleration Sensors Attached to the Body. PLoS ONE 2015, 10, e0130851. [Google Scholar] [CrossRef] [Green Version]
- Hu, B.; Li, S.; Chen, Y.; Kavi, R.; Coppola, S. Applying deep neural networks and inertial measurement unit in recognizing irregular walking differences in the real world. Appl. Ergon. 2021, 96, 103414. [Google Scholar] [CrossRef]
- Zakaria, N.A.; Kuwae, Y.; Tamura, T.; Minato, K.; Kanaya, S. Quantitative analysis of fall risk using TUG test. Comput. Methods Biomech. Biomed. Engin. 2015, 18, 426–437. [Google Scholar] [CrossRef]
- Lepetit, K.; Mansour, K.B.; Letocart, A.; Boudaoud, S.; Kinugawa, K.; Grosset, J.F.; Marin, F. Optimized scoring tool to quantify the functional performance during the sit-to-stand transition with a magneto-inertial measurement unit. Clin. Biomech. 2019, 69, 109–114. [Google Scholar] [CrossRef]
- Petrushin, A.; Freddolini, M.; Barresi, G.; Bustreo, M.; Laffranchi, M.; Del Bue, A.; De Michieli, L. IoT-Powered Monitoring Systems for Geriatric Healthcare: Overview. In Internet of Things for Human-Centered Design: Application to Elderly Healthcare; Scataglini, S., Imbesi, S., Marques, G., Eds.; Springer Nature: Singapore, 2022; pp. 99–122. [Google Scholar]
- Johnston, W.; O’Reilly, M.; Dolan, K.; Reid, N.; Coughlan, G.; Caulfield, B. Objective Classification of Dynamic Balance Using a Single Wearable Sensor. In Proceedings of the 4th International Congress on Sport Sciences Research and Technology Support, Porto, Portugal, 7–9 November 2016; pp. 15–24. [Google Scholar]
- Gao, L.; Bourke, A.K.; Nelson, J. Evaluation of accelerometer based multi-sensor versus single-sensor activity recognition systems. Med. Eng. Phys. 2014, 36, 779–785. [Google Scholar] [CrossRef]
- Ko, J.B.; Yoon, J.S.; Lee, C.K.; Byeon, T.M.; Hong, J.S. A Study on the Determining the Optimal Location of IMU Sensors in Dynamic Balance Measurement by Comparing Absolute Percentage Error between the 3D Motion Capture System and IMU Sensor. J. Ergon. Soc. Korea 2019, 38, 419–434. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Savva, G.M.; Donoghue, O.A.; Horgan, F.; O’Regan, C.; Cronin, H.; Kenny, R.A. Using timed up-and-go to identify frail members of the older population. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 441–446. [Google Scholar] [CrossRef]
- Butland, R.J.; Pang, J.; Gross, E.R.; Woodcock, A.A.; Geddes, D.M. Two-, six-, and 12-minute walking tests in respiratory disease. Br. Med. J. (Clin. Res. Ed.) 1982, 284, 1607–1608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boxer, R.; Kleppinger, A.; Ahmad, A.; Annis, K.; Hager, D.; Kenny, A. The 6-minute walk is associated with frailty and predicts mortality in older adults with heart failure. Congest. Heart Fail. 2010, 16, 208–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, V.; Naylor, J.M.; Harris, I.A.; Crosbie, J.; Yeo, A.E. The six-minute walk test is an excellent predictor of functional ambulation after total knee arthroplasty. BMC Musculoskelet. Disord. 2013, 14, 145. [Google Scholar] [CrossRef] [Green Version]
- Rikli, R.E.; Jones, C.J. The Reliability and Validity of a 6-Minute Walk Test as a Measure of Physical Endurance in Older Adults. J. Aging Phys. Act. 1998, 6, 363–375. [Google Scholar] [CrossRef]
- Kervio, G.; Carre, F.; Ville, N.S. Reliability and intensity of the six-minute walk test in healthy elderly subjects. Med. Sci. Sports Exerc. 2003, 35, 169–174. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Mirelman, A.; Weiss, A.; Buchman, A.S.; Bennett, D.A.; Giladi, N.; Hausdorff, J.M. Association between performance on Timed Up and Go subtasks and mild cognitive impairment: Further insights into the links between cognitive and motor function. J. Am. Geriatr. Soc. 2014, 62, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Beyea, J.; McGibbon, C.A.; Sexton, A.; Noble, J.; O’Connell, C. Convergent Validity of a Wearable Sensor System for Measuring Sub-Task Performance during the Timed Up-and-Go Test. Sensors 2017, 17, 934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amjad, F.; Khan, M.H.; Nisar, M.A.; Farid, M.S.; Grzegorzek, M. A Comparative Study of Feature Selection Approaches for Human Activity Recognition Using Multimodal Sensory Data. Sensors 2021, 21, 2368. [Google Scholar] [CrossRef]
- Vervoort, D.; Vuillerme, N.; Kosse, N.; Hortobágyi, T.; Lamoth, C.J. Multivariate Analyses and Classification of Inertial Sensor Data to Identify Aging Effects on the Timed-Up-and-Go Test. PLoS ONE 2016, 11, e0155984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coni, A.; Ancum, J.M.V.; Bergquist, R.; Mikolaizak, A.S.; Mellone, S.; Chiari, L.; Maier, A.B.; Pijnappels, M. Comparison of Standard Clinical and Instrumented Physical Performance Tests in Discriminating Functional Status of High-Functioning People Aged 61–70 Years Old. Sensors 2019, 19, 449. [Google Scholar] [CrossRef] [Green Version]
- Moe-Nilssen, R.; Helbostad, J.L. Estimation of gait cycle characteristics by trunk accelerometry. J. Biomech. 2004, 37, 121–126. [Google Scholar] [CrossRef]
- Kobayashi, H.; Kakihana, W.; Kimura, T. Combined effects of age and gender on gait symmetry and regularity assessed by autocorrelation of trunk acceleration. J. NeuroEng. Rehabil. 2014, 11, 109. [Google Scholar] [CrossRef] [Green Version]
- Kobsar, D.; Olson, C.; Paranjape, R.; Hadjistavropoulos, T.; Barden, J.M. Evaluation of age-related differences in the stride-to-stride fluctuations, regularity and symmetry of gait using a waist-mounted tri-axial accelerometer. Gait Posture 2014, 39, 553–557. [Google Scholar] [CrossRef]
- Martínez-Ramírez, A.; Martinikorena, I.; Gómez, M.; Lecumberri, P.; Millor, N.; Rodríguez-Mañas, L.; García García, F.J.; Izquierdo, M. Frailty assessment based on trunk kinematic parameters during walking. J. Neuroeng. Rehabil. 2015, 12, 48. [Google Scholar] [CrossRef] [Green Version]
- Menz, H.B.; Lord, S.R.; Fitzpatrick, R.C. Acceleration patterns of the head and pelvis when walking on level and irregular surfaces. Gait Posture 2003, 18, 35–46. [Google Scholar] [CrossRef]
- Brach, J.S.; McGurl, D.; Wert, D.; Vanswearingen, J.M.; Perera, S.; Cham, R.; Studenski, S. Validation of a measure of smoothness of walking. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Roche, J.L.; Lowry, K.A.; Vanswearingen, J.M.; Brach, J.S.; Redfern, M.S. Harmonic ratios: A quantification of step to step symmetry. J. Biomech. 2013, 46, 828–831. [Google Scholar]
- Martinikorena, I.; Martínez-Ramírez, A.; Gómez, M.; Lecumberri, P.; Casas-Herrero, A.; Cadore, E.L.; Millor, N.; Zambom-Ferraresi, F.; Idoate, F.; Izquierdo, M. Gait Variability Related to Muscle Quality and Muscle Power Output in Frail Nonagenarian Older Adults. J. Am. Med. Dir. Assoc. 2016, 17, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Pincus, S.M. Approximate entropy as a measure of system complexity. Proc. Natl. Acad. Sci. USA 1991, 88, 2297–2301. [Google Scholar] [CrossRef] [Green Version]
- Drucker, H.; Cortes, C.; Jackel, L.D.; LeCun, Y.; Vapnik, V. Boosting and Other Ensemble Methods. Neural Comput. 1994, 6, 1289–1301. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, Association for Computing Machinery, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Steffen, T.M.; Hacker, T.A.; Mollinger, L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Phys. Ther. 2002, 82, 128–137. [Google Scholar] [PubMed] [Green Version]
- Dite, W.; Temple, V.A. Development of a clinical measure of turning for older adults. Am. J. Phys. Med. Rehabil. 2002, 81, 857–866, quiz 867–868. [Google Scholar] [CrossRef] [PubMed]
- Nordin, E.; Rosendahl, E.; Lundin-Olsson, L. Timed “Up & Go” test: Reliability in older people dependent in activities of daily living--focus on cognitive state. Phys. Ther. 2006, 86, 646–655. [Google Scholar] [PubMed]
- Bean, J.F.; Kiely, D.K.; Leveille, S.G.; Herman, S.; Huynh, C.; Fielding, R.; Frontera, W. The 6-minute walk test in mobility-limited elders: What is being measured? J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M751–M756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montgomery, G.; McPhee, J.; Pääsuke, M.; Sipilä, S.; Maier, A.B.; Hogrel, J.Y.; Degens, H. Determinants of Performance in the Timed Up-and-Go and Six-Minute Walk Tests in Young and Old Healthy Adults. J. Clin. Med. 2020, 9, 1561. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | Definition | |
|---|---|---|
| Time features | Total time | Total time on the TUG test |
| Sit-to-stand time | Time from sit on a chair to stand | |
| Gait time | Average time on forward gait and backward gait in the TUG test | |
| Mid-turn time | Time on rotation at return point | |
| End-turn time | Time on rotation for sit on a chair | |
| Stand-to-sit time | Time from stand to sit on a chair | |
| Descriptive statistics features | Root mean square (RMS) | Arithmetic mean of the squares of a set of values |
| Min | The smallest value | |
| Max | The greatest value |
| Features | Definition | |
|---|---|---|
| GP | Number of steps | Number of steps taken during 6 min |
| Step/s | Step per second | |
| Step time | Mean time between each step | |
| Stride length | Distance between steps | |
| Gait distance | Walking distance for 6 min | |
| Average gait speed | Average walking speed for 6 min | |
| GS | Step regularity | Symmetry between steps as identified by ACCVT, ACCAP, ACCRES for walking |
| Stride regularity | Symmetry between strides as identified by ACCVT, ACCAP, ACCRES for walking | |
| Symmetry index | Gait symmetry index | |
| HR | Harmonic ratio | Smoothness of acceleration signals measured for walking |
| ApEn | Approximate entropy | Regularity of acceleration signals measured for walking |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, J.B.; Hong, J.S.; Shin, Y.S.; Kim, K.B. Machine Learning-Based Predicted Age of the Elderly on the Instrumented Timed Up and Go Test and Six-Minute Walk Test. Sensors 2022, 22, 5957. https://doi.org/10.3390/s22165957
Ko JB, Hong JS, Shin YS, Kim KB. Machine Learning-Based Predicted Age of the Elderly on the Instrumented Timed Up and Go Test and Six-Minute Walk Test. Sensors. 2022; 22(16):5957. https://doi.org/10.3390/s22165957
Chicago/Turabian StyleKo, Jeong Bae, Jae Soo Hong, Young Sub Shin, and Kwang Bok Kim. 2022. "Machine Learning-Based Predicted Age of the Elderly on the Instrumented Timed Up and Go Test and Six-Minute Walk Test" Sensors 22, no. 16: 5957. https://doi.org/10.3390/s22165957
APA StyleKo, J. B., Hong, J. S., Shin, Y. S., & Kim, K. B. (2022). Machine Learning-Based Predicted Age of the Elderly on the Instrumented Timed Up and Go Test and Six-Minute Walk Test. Sensors, 22(16), 5957. https://doi.org/10.3390/s22165957