
Perturbations during Gait: A Systematic Review of Methodologies and Outcomes

 ,
,
Abstract
:1. Introduction
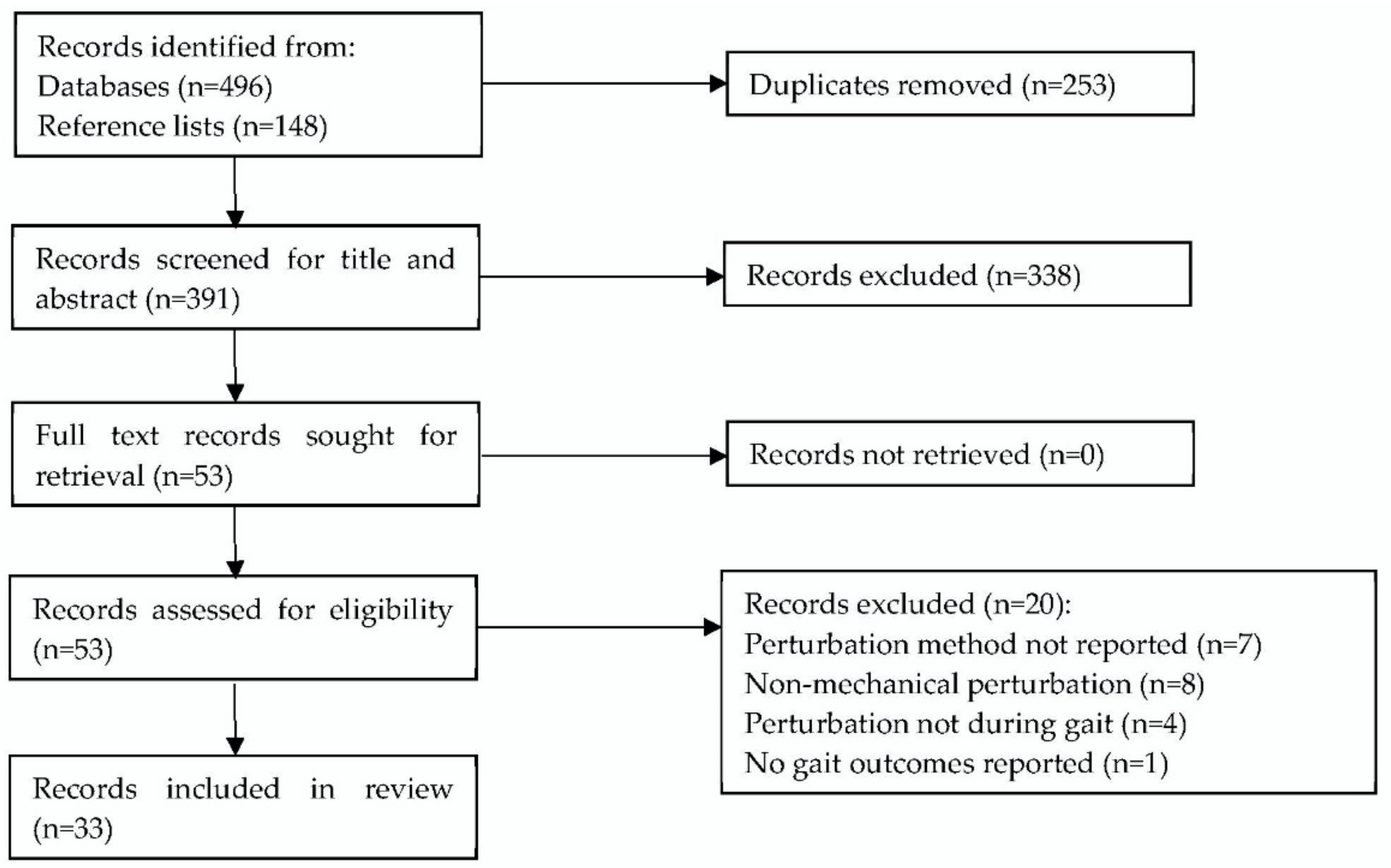
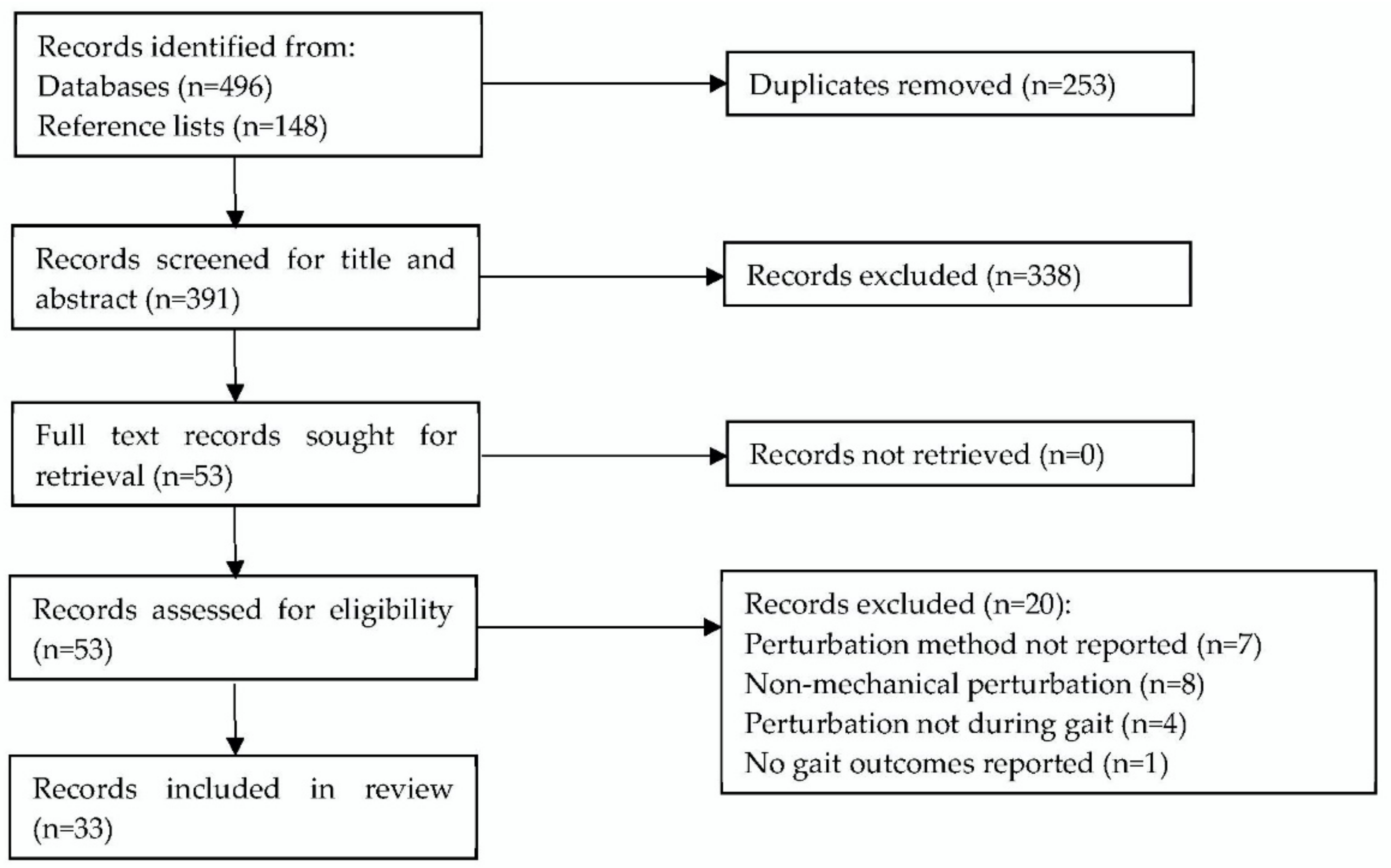
2. Materials and Methods
3. Results

{kind=link}
| Reference | Sample Size | Population | Age Years (SD) | Height m (SD) | Body Mass kg (SD) |
|---|---|---|---|---|---|
| Aprigliano et al. [20] | 5 | Healthy YA | 25.4 (3.1) | 1.7 (0.1) | 63.2 (11) |
| Aprigliano et al. [18] | 15 | Healthy YA | 26.1 (1.3) | 1.78 (0.06) | 68.8 (12.3) |
| Aprigliano et al. [19] | 6 | Healthy OA | 68.7 (5.2) | 1.76 (0.1) | 76.9 (7.9) |
| Arvin et al. [39] | 12 | Healthy YA | 27.3 (1.7) | 1.68 (0.11) | 60.6 (10.5) |
| 18 | Healthy OA | 70.8 (6.8) | 1.70 (0.86) | 80.1 (8.8) | |
| Best et al. [40] | 12 | Healthy YA | 21.8 (1.0) | 1.802 (0.092) | 72.3 ((11.2) |
| Capin et al. [47] | 40 | Post-operative ACL rupture | 23.0 (7.0) | 1.78 (0.07) | 86.0 (11.5) |
| Francis et al. [42] | 12 | Healthy YA | 23.6 (3.9) | 1.69 (0.25) | 70.7 (11.3) |
| 11 | Healthy OA | 71.2 (4.2) | 1.64 (0.06) | 66.9 (9.6) | |
| Golyski et al. [24] | 10 | Healthy YA | 24 (3) | 1.76 (0.11) | 74.1 (12.0) |
| Haarman et al. [25] | 10 | Paretic OA | 52 (16) | 1.75 (0.06) | 82.5 (13.6) |
| Hof and Duysens [38] | 9 | Healthy YA | 19–23 | Not reported | Not reported |
| Kao et al. [31] | 18 | Healthy YA | 20.4 (1.5) | 1.72 (0.10) | 69.2 (11.7) |
| Kreter et al. [41] | 5 | Healthy YA | 24 (5) | Not reported | Not reported |
| 5 | Concussed YA | 25 (5) | |||
| Kurz et al. [9] | 53 | Healthy OA | 80.1 (5.6) | 1.58 (0.09) | 68.3 (13.9) |
| Lee-Confer et al. [46] | 16 | Healthy YA | 21–35 | Not reported | Not reported |
| Madehkhaksar et al. [26] | 10 | Healthy YA | 26.4 (4.1) | 1.7 (0.08) | 64.4 (12.5) |
| Martelli et al. [35] | 8 | Healthy YA | 29.9 (4.9) | 1.68 (0.08) | 67.9 (9.4) |
| Martelli et al. [7] | 18 | Healthy YA | 23.9 (4.2) | 1.75 (0.08) | 70.3 (8.1) |
| McIntosh et al. [43] | 11 | Healthy YA | 23.8 (3.1) | 1.76 (0.01) | 71.2 (12.4) |
| 10 | Healthy OA | 71.1 (3.1) | 1.68 (0.01) | 72.6 (11.1) | |
| Nestico et al. [32] | 16 | Healthy YA | 20–35 | Not reported | Not reported |
| Onushko et al. [27] | 15 | Healthy YA | 21.3 (1.4) | 1.7 (0.1) | 68.8 (10.7) |
| Punt et al. [22] | 38 | Stroke Survivors OA | 60.2 (9.5) | 1.72 (0.12) | 85 (19.6) |
| Rieger et al. [21] | 30 | Healthy OA | 70.1 (4.5) | 1.72 (0.09) | 75.2 (10.2) |
| Roeles et al. [28] | 9 | Healthy YA | 25.1 (3.4) | 1.76 (0.09) | 76.6 (15.1) |
| 9 | Healthy OA | 70.1 (8.1) | 1.70 (0.11) | 77.9 (10.5) | |
| Rosenblum et al., 2020 [29] | 12 | Healthy YA | 26.9 (3.4) | 1.68 (0.07) | 63.67 (10.26) |
| 12 | Healthy OA | 69.5 (5.2) | 1.70 (0.07) | 78.34 (16.22) | |
| Rosenblum et al. [33] | 20 | Healthy YA | 27 (3) | 1.67 (0.08) | 62.5 (10.7) |
| Rutherford et al. [45] | 32 | Knee | 61 (6) | 1.69 (0.10) | 85.5 (14.3) |
| Osteoarthritis OA | |||||
| 44 | Healthy OA | 60 (6) | 1.68 (0.08) | 70.7 (13.0) | |
| Sheehan et al. [30] | 22 | Healthy YA | 27.2 (6.9) | 1.76 (0.095) | 84.8 (13.9) |
| Shulman et al. [44] | 18 | Healthy YA | 21.7 (2.6) | 1.80 (0.1) | 72.8 (11.0) |
| 16 | Healthy OA | 75.6 (5.3) | 1.70 (0.1) | 72.7 (13.4) | |
| Taborri et al. [34] | 12 | Healthy YA | 26 (3) | 1.71 (0.05) | 64.9 (9.6) |
| van Hal et al. [23] | 20 | Not reported | Not reported | Not reported | Not reported |
| Vervoort et al. [8] | 75 | Healthy YA and OA | 48.1 (17.95) | 1.75 (0.10) | 73.81 (10.81) |
| Vlutters et al. [36] | 10 | Healthy YA | 25 (2) | 1.8 (0.11) | 67 (12) |
| Zadravec et al. [37] | 7 | Healthy YA | 33.4 (8.5) | 1.81 (0.05) | 80.1 (11.6) |
| Reference | Perturbation Cause | Perturbation Details |
|---|---|---|
| Aprigliano et al. [20] | Split belt TM | Initiation at HS, 5 left belt perturbations 5 right belt |
| Aprigliano et al. [18] | Split belt TM | Initiation at HS, 5 left belt perturbations 5 right belt |
| Aprigliano et al. [19] | Split belt TM | Initiation at HS, anterior, or lateral translation of right belt |
| Arvin et al. [39] | Hip abductor vibration during gait | Mean vibration duration 0.41 s, 40% stance phase |
| Best et al. [40] | Pendula mass oscillating during gait | Pendula mass 6.4% of body mass, frequency at 130%, and 70% of strides |
| Capin et al. [47] | OG walking physical therapist perturbations | Lack of detail, progressive perturbation applied by trained physical therapist |
| Francis et al. [42] | Narrow TM walking, cognitive task | Perturbation was sum of sinusoids waves to the virtual hallway, amplitude 0.175 m |
| Golyski et al. [24] | Split belt TM | Initiation at 10, 15, 20, and 30% of gait cycle, individual belt acceleration then deceleration for 30% gait cycle duration, 10 each leg at each initiation point |
| Haarman et al. [25] | Movable TM | Initiation at toe-off, 150 ms block pulses equal to 4, 8, 12, and 16% of body mass |
| Hof and Duysens [38] | Waist belt, right side, pneumatics | Push and pulls of 100 ms throughout gait, at 2.7–12.4 kg m s−1 |
| Kao et al. [31] | Movable TM | Continuous pseudo-random amplitude ML translations with max amplitude 0.05 m for 150 s |
| Kreter et al. [41] | OG walking mechanised shoe | 5–12° ankle eversion randomly between 3rd and 6th stride of a 7.5 m walk |
| Kurz et al. [9] | Movable TM | Perturbation every 20–40 s for 14 min, 0.01–0.18 m, 0.5–16.0 m s−2 |
| Lee-Confer et al. [46] | OG low-friction floor | Floor surface was coated in mineral oil to induce slip |
| Madehkhaksar et al. [26] | Single belt TM | 16 perturbations of 2.5 m s−1, HS within four five min blocks |
| Martelli et al. [35] | Waist belt, cable pulleys | Pulsation rise, hold, fall time of 150 ms. 10, 15, 20% body mass, HS |
| Martelli et al. [7] | Waist belt, cable pulleys | Pulsation rise, hold, fall time of 150 ms. 10, 15, 20% BM, HS |
| McIntosh et al. [43] | OG walking floor translation | 0.15 m, 0.316 ms 2.4 m s−2, HS |
| Nestico et al. [32] | ML TM oscillations | ML translation 200 ms acceleration followed by 200 ms deceleration of 0.072 m at 1.8 m s−2 |
| Onushko et al. [27] | Single belt TM | ML ±0.08, 0.165, and 0.25 m oscillations initiated at HS |
| Punt et al. [22] | Split belt TM | 16 ML perturbations of 0.045 m separated by 15 s |
| Rieger et al. [21] | Split belt TM | 0.31 s, 0.05 m, 0.1613 m s−2, HS medial translation |
| Roeles et al. [28] | Single belt TM | 0.7 s, 0.05 m, 2.04 m s−2 |
| Rosenblum et al. [29] | ML TM oscillations | 0.15 m displacement in 0.92 s, initiated at HS |
| Rosenblum et al. [33] | ML TM oscillations | ML translation of 0.15 m for 0.92 s at single or double support |
| Rutherford et al. [45] | OG walking ML floor translation | ML translation of 0.01 or 0.03 m during mid-stance at 0.1 m s−1 |
| Sheehan et al. [30] | ML TM oscillations | Continuous 3 min ± 12 cm displacement from centre |
| Shulman et al. [44] | OG walking ML floor translation | 6 left, 4 right side prior to toe-off at 0.6 ms, 2 m s−2, 0.18 m |
| Taborri et al. [34] | Movable TM | AP acceleration at 0.5 m s−2 or ML translation of 0.16 m at 0.18 m s−2 |
| van Hal et al. [23] | Split belt TM | Initiation at HS, lateral pull, 0.66 m s2 of 0.05 m |
| Vervoort et al. [8] | Split belt TM | Randomly, one belt at 0.7 m s−1, one at 1.4 m s−1 |
| Vlutters et al. [36] | Waist belt, motors | 150 ms block pulses, forces 4, 8, 12, 16% BM |
| Zadravec et al. [37] | Waist belt | 5 repeats of 4 directions. 15% BM, 150 ms |
| Reference | Outcome Variables | Summary of Change in Outcome Variables |
|---|---|---|
| Aprigliano et al. [20] | Hip, knee, ankle joint angles, compensatory time, MoS | Joint angles altered, no detail. Increased compensatory time with perturbation intensity. Decreased MoS. |
| Aprigliano et al. [18] | Stride time, stance %, hip, knee, ankle joint angles. | Decreased stride time, stance %, hip, knee, thigh, shank, foot RoM. Increased ankle RoM. |
| Aprigliano et al. [19] | Dynamic stability, step width, single and double support time, hip, knee, ankle RoM. MoS. | Decreased dynamic stability, step width, single and double support time, knee, ankle RoM. Increased frontal plane hip RoM, sagittal and frontal plane MoS. No change sagittal plane hip RoM. |
| Arvin et al. [39] | CoM position, CoM velocity, step width. | Decreased step width at perturbation, increased step width post perturbation. No change CoM position or velocity. |
| Best et al. [40] | MoS, CoM amplitude, step width, step length, step time. | Increased MoS only in out of phase. Decreased CoM amplitude. No change step width, step length, step time. |
| Capin et al. [47] | Hip, knee and ankle joint angles, excursions, moment. | Decreased hip, knee, ankle excursions at loading. No change hip, knee, ankle joint angles, moments. |
| Francis et al. [42] | ML LDE, step width, step length, step width variability, step length variability, gait speed. | Decreased LDE on TM than OG. No change step width, step length, step width variability, step length variability, gait speed. |
| Golyski et al. [24] | Step width, step length, MoS. | Later perturbation onset increased AP, ML MoS, step width, and step length for perturbed step but lower AP MoS and step length for first recovery step. |
| Haarman et al. [25] | Gluteus medius EMG activation, CoM velocity, step width, support time, foot velocity, XCoM. | Increased swing time, gluteus medius activation CoM velocity variability. Increased lead foot ML distance from CoM, foot velocity increased. No change step width, step length, XCoM, double support time. |
| Hof and Duysens [38] | Tibialis anterior, plantar flexor, soleus EMG activation, CoP. | Increased tibialis anterior, plantar flexor, soleus activation. Decreased CoP motion. |
| Kao et al. [31] | LDE, step width, step length, stride time step width variability, step length variability, MoS, CoM variability, ankle, knee and hip angle variability. | Perturbation decreased AP MoS, step width, length and stride time and increased ML MoS and variability of step width, length and stride time, CoM movement, MoS and all joint angles. |
| Kreter et al. [41] | Step time, double support time, ML acceleration of foot and trunk. | Perturbation decreased double support time but no effect on step time and increased lateral acceleration of the foot at toe-off and less trunk lateral acceleration in concussed participants but no effect on trunk in control participants. |
| Kurz et al. [9] | CoM sway, sway velocity, sway area, foot contact time, voluntary stepping. | Decreased CoM AP and ML-sway, sway velocity, sway area. Interaction for foot contact time of the voluntary step execution. |
| Lee-Confer et al. [46] | Frontal and sagittal plane shoulder angles. | Frontal plane contralateral arm excursion is greater in perturbed than ipsilateral arm and was greater than sagittal plane excursion. |
| Madehkhaksar et al. [26] | Step length, step width, cadence, dynamic stability, MoS step length, step width, cadence, dynamic stability variability. | Increase step width, cadence, dynamic stability, step length variability, step width variability, cadence variability, dynamic stability variability, AP and ML MoS. Decrease step length. |
| Martelli et al. [35] | Dynamic stability, MoS, BoS, adaptive response, step length, step width. | Increased dynamic stability, MoS, BoS, adaptive response, step length. Decreased step width. |
| Martelli et al. [7] | Step length, step width, MoS, BoS. | Increased step length, MoS, step width at first perturbation. Decreased step width overall, AP and ML BoS, AP MoS, at first recovery step. No change at perturbation onset AP BoS, AP and ML MoS. |
| McIntosh et al. [43] | CoM velocity, CoM displacement, step width, step length, recovery step type. | Increase CoM velocity, CoM displacement range, normalised ML trunk CoM displacement, step width. Decrease step length. 85 of 840 recovery steps were cross-over. |
| Nestico et al. [32] | Short- and long-term variability (Poincare plots) of step length and width, number of recovery steps required. | Step width and long-term step width variability were greater in perturbed no effect on short term step length variability, no correlation between step width variability and number of recovery steps. |
| Onushko et al. [27] | Step length, step frequency, step width, MoS. | Increased step frequency, step width, ML MoS, ML MoS variability. Decreased step length. |
| Punt et al. [22] | Step length, step width, step time, MoS, dynamic stability. | Increase step length, step width, ML MoS, step time. Decrease AP MoS, dynamic stability. |
| Rieger et al. [21] | Step width, step time, swing time, stance time, step length, dynamic stability, LDE, recovery. | Increase dynamic stability, step time, swing time, stance time, step length, recovery performance. Decrease LDE, step width, recovery time. |
| Roeles et al. [28] | Step width, step length, step time, MoS. | Increased AP and ML MoS, step width. Decreased step length, step time. |
| Rosenblum et al. [29] | Step length, step width, recovery time. | Increased step length, step width. Total recovery occurred 4–6 s after perturbation. |
| Rosenblum et al. [33] | Vastus lateralis and tibialis anterior EMG spectral power, MoS. | MoS, total and individual muscle mean spectral power increased after perturbation. |
| Rutherford et al. [45] | Knee sagittal and frontal plane moment, knee sagittal RoM, hamstrings, quadriceps and gastrocnemius muscle EMG principal components. | Increased flexion RoM, sagittal and frontal knee moments and decreased muscle activity after perturbation. |
| Sheehan et al. [30] | Stride variability, angular momentum, gait phases. | Increased stride variability, range of angular momentum. Decreased angular momentum during second double support. |
| Shulman et al. [44] | BoS, step width, single support time, swing time, step length, gait speed. | Increased BoS, step width. Decreased single support time, swing time, step length. No change gait speed. |
| Taborri et al. [34] | Sagittal hip, knee and ankle joint range of motion, variability and continuous relative phase coordination. | Increased variability in joint angles, reduced flexion and change in relative phase of all joint combinations. |
| van Hal et al. [23] | vGRF kinetic, kinematic, spatio-temporal. | Preliminary trial paper, therefore no results. |
| Vervoort et al. [8] | Cadence, MoS, step length, single and double support time. | Increased cadence, ML MoS of slow leg. Decreased step length, single and double support time. |
| Vlutters et al. [36] | CoM velocity, CoP, GRF, step length, step width single and double support time. | Linear relationship between CoM velocity, CoP and GRF. Increased vGRF, step length, single and double support time. Decreased step width. |
| Zadravec et al. [37] | Step time, step width, step length. | Increase step time. Decrease step width, step length. No change in 82% of all stepping response parameters between OG and TM perturbations. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A
| Reference | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aprigliano et al. [20] | Y | Y | N | N | U | U | N | Y | Y | N | N | Y | U | N | Y | Y | Y | Y | N | Y |
| Aprigliano et al. [18] | Y | Y | N | Y | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | N | N | Y |
| Aprigliano et al. [19] | Y | Y | N | Y | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | N | N | Y |
| Arvin et al. [39] | Y | Y | N | Y | U | Y | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Best et al. [40] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Capin et al. [47] | Y | Y | N | Y | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Francis et al. [42] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Golyski et al. [24] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Haarman et al. [25] | Y | Y | N | Y | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Hof and Duysens [38] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | N | N | Y |
| Kao et al. [31] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Kreter et al. [41] | Y | Y | N | Y | Y | Y | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Kurz et al. [9] | Y | Y | N | Y | Y | Y | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Lee-Confer et al. [46] | Y | Y | N | Y | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Madehkhaksar et al. [26] | Y | Y | Y | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Martelli et al. [35] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Martelli et al. [7] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| McIntosh et al. [43] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Nestico et al. [32] | Y | Y | N | Y | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Onushko et al. [27] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Punt et al. [22] | Y | Y | N | Y | Y | Y | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Rieger et al. [21] | Y | Y | N | N | Y | Y | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Roeles et al. [28] | Y | Y | N | Y | U | Y | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Rosenblum et al. [29] | Y | Y | N | Y | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Rosenblum et al. [33] | Y | Y | Y | Y | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Rutherford et al. [45] | Y | Y | N | Y | Y | Y | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Sheehan et al. [30] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | N | N | Y |
| Shulman et al. [44] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
| Taborri et al. [34] | Y | Y | N | Y | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | N | N | Y |
| van Hal et al. [23] | Y | Y | N | Y | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | N | N | Y |
| Vervoort et al. [8] | Y | Y | N | Y | U | U | N | Y | Y | Y | Y | U | U | N | U | U | U | U | N | Y |
| Vlutters et al. [36] | Y | Y | N | Y | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | N | N | Y |
| Zadravec et al., 2017 [37] | Y | Y | N | N | U | U | N | Y | Y | Y | Y | Y | U | N | Y | Y | Y | Y | N | Y |
References
- Bhatt, T.; Espy, D.; Yang, F.; Pai, Y.-C. Dynamic Gait Stability, Clinical Correlates, and Prognosis of Falls Among Community-Dwelling Older Adults. Arch. Phys. Med. Rehabil. 2011, 92, 799–805. [Google Scholar] [CrossRef] [PubMed]
- NICE. Falls in Older People: Assessing Risk and Prevention. In Guidance and Guidelines; NICE: London, UK, 2013; pp. 20–21. [Google Scholar]
- Chien, J.-E.; Hsu, W.-L. Effects of Dynamic Perturbation-Based Training on Balance Control of Community-Dwelling Older Adults. Sci. Rep. 2018, 8, 17231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hof, A.L.; Vermerris, S.M.; Gjaltema, W.A. Balance responses to lateral perturbations in human treadmill walking. J. Exp. Biol. 2010, 213, 2655–2664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zadravec, M.; Olenšek, A.; Rudolf, M.; Bizovičar, N.; Goljar, N.; Matjačić, Z. Assessment of dynamic balancing responses following perturbations during slow walking in relation to clinical outcome measures for high-functioning post-stroke subjects. J. Neuroeng. Rehabil. 2020, 17, 85. [Google Scholar] [CrossRef]
- Thompson, J.D.; Franz, J.R. Do kinematic metrics of walking balance adapt to perturbed optical flow? Hum. Mov. Sci. 2017, 54, 34–40. [Google Scholar] [CrossRef]
- Martelli, D.; Vashista, V.; Micera, S.; Agrawal, S.K. Direction-Dependent Adaptation of Dynamic Gait Stability Following Waist-Pull Perturbations. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 24, 1304–1313. [Google Scholar] [CrossRef]
- Vervoort, D.; Buurke, T.J.W.; Vuillerme, N.; HortobÁGyi, T.; Den Otter, R.O.B.; Lamoth, C.J.C. Adaptive Control of Dynamic Balance across the Adult Lifespan. Med. Sci. Sports Exerc. 2020, 52, 2270–2277. [Google Scholar] [CrossRef]
- Kurz, I.; Gimmon, Y.; Shapiro, A.; Debi, R.; Snir, Y.; Melzer, I. Unexpected perturbations training improves balance control and voluntary stepping times in older adults—A double blind randomized control trial. BMC Geriatr. 2016, 16, 58. [Google Scholar] [CrossRef] [Green Version]
- Rogers, M.W.; Mille, M. Timing paradox of stepping and falls in ageing: Not so quick and quick (Er) on the trigger. J. Physiol. 2016, 594, 4537–4547. [Google Scholar] [CrossRef] [Green Version]
- McCrum, C.; Gerards, M.H.G.; Karamanidis, K.; Zijlstra, W.; Meijer, K. A systematic review of gait perturbation paradigms for improving reactive stepping responses and falls risk among healthy older adults. Eur. Rev. Aging Phys. Act. 2017, 14, 3. [Google Scholar] [CrossRef] [Green Version]
- Olson, M.; Lockhart, T.E.; Lieberman, A. Motor Learning Deficits in Parkinson’s Disease (PD) and Their Effect on Training Response in Gait and Balance: A Narrative Review. Front. Neurol. 2019, 10, 62. [Google Scholar] [CrossRef] [Green Version]
- Mansfield, A.; Aqui, A.; Danells, C.J.; Knorr, S.; Centen, A.; Depaul, V.G.; Schinkel-Ivy, A.; Brooks, D.; Inness, E.L.; Mochizuki, G. Does perturbation-based balance training prevent falls among individuals with chronic stroke? A randomised controlled trial. BMJ Open 2018, 8, e021510. [Google Scholar] [CrossRef] [PubMed]
- Lesinski, M.; Hortobágyi, T.; Muehlbauer, T.; Gollhofer, A.; Granacher, U. Effects of Balance Training on Balance Performance in Healthy Older Adults: A Systematic Review and Meta-analysis. Sports Med. 2015, 45, 1721–1738. [Google Scholar] [CrossRef] [Green Version]
- Tokur, D.; Grimmer, M.; Seyfarth, A. Review of balance recovery in response to external perturbations during daily activities. Hum. Mov. Sci. 2020, 69, 102546. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 372. [Google Scholar] [CrossRef]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [Green Version]
- Aprigliano, F.; Martelli, D.; Micera, S.; Monaco, V. Intersegmental coordination elicited by unexpected multidirectional slipping-like perturbations resembles that adopted during steady locomotion. J. Neurophysiol. 2016, 115, 728–740. [Google Scholar] [CrossRef]
- Aprigliano, F.; Monaco, V.; Tropea, P.; Martelli, D.; Vitiello, N.; Micera, S. Effectiveness of a Robot-Mediated Strategy While Counteracting Multidirectional Slippages. Robotica 2019, 37, 2119–2131. [Google Scholar] [CrossRef] [Green Version]
- Aprigliano, F.; Martelli, D.; Tropea, P.; Micera, S.; Monaco, V. Effects of slipping-like perturbation intensity on the dynamical stability. Proc. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. EMBS 2015, 2015, 5295–5298. [Google Scholar] [CrossRef]
- Rieger, M.M.; Papegaaij, S.; Pijnappels, M.; Steenbrink, F.; van Dieën, J.H. Transfer and retention effects of gait training with anterior-posterior perturbations to postural responses after medio-lateral gait perturbations in older adults. Clin. Biomech. 2020, 75, 104988. [Google Scholar] [CrossRef] [Green Version]
- Punt, M.; Bruijn, S.M.; Roeles, S.; van de Port, I.G.; Wittink, H.; van Dieen, J.H. Responses to gait perturbations in stroke survivors who prospectively experienced falls or no falls. J. Biomech. 2017, 55, 56–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Hal, E.S.; Hijmans, J.M.; Postema, K.; Otten, E. A prosthetic leg prototype for improved mediolateral balance control: Design of a case-control study. Cogent Eng. 2018, 5, 1520425. [Google Scholar] [CrossRef]
- Golyski, P.R.; Vazquez, E.; Leestma, J.K.; Sawicki, G.S. Onset timing of treadmill belt perturbations influences stability during walking. J. Biomech. 2021, 130, 110800. [Google Scholar] [CrossRef] [PubMed]
- Haarman, J.A.M.; Vlutters, M.; Olde Keizer, R.; van Asseldonk, E.H.F.; Buurke, J.H.; Reenalda, J.; Rietman, J.S.; van der Kooij, H. Paretic versus non-paretic stepping responses following pelvis perturbations in walking chronic-stage stroke survivors. J. Neuroeng. Rehabil. 2017, 14, 106. [Google Scholar] [CrossRef] [Green Version]
- Madehkhaksar, F.; Klenk, J.; Sczuka, K.; Gordt, K.; Melzer, I.; Schwenk, M. The effects of unexpected mechanical perturbations during treadmill walking on spatiotemporal gait parameters, and the dynamic stability measures by which to quantify postural response. PLoS ONE 2018, 13, e0195902. [Google Scholar] [CrossRef]
- Onushko, T.; Boerger, T.; Van Dehy, J.; Schmit, B.D. Dynamic stability and stepping strategies of young healthy adults walking on an oscillating treadmill. PLoS ONE 2019, 14, e0212207. [Google Scholar] [CrossRef]
- Roeles, S.; Rowe, P.J.; Bruijn, S.M.; Childs, C.R.; Tarfali, G.D.; Steenbrink, F.; Pijnappels, M. Gait stability in response to platform, belt, and sensory perturbations in young and older adults. Med. Biol. Eng. Comput. 2018, 56, 2325–2335. [Google Scholar] [CrossRef] [Green Version]
- Rosenblum, U.; Kribus-Shmiel, L.; Zeilig, G.; Bahat, Y.; Kimel-Naor, S.; Melzer, I.; Plotnik, M. Novel methodology for assessing total recovery time in response to unexpected perturbations while walking. PLoS ONE 2020, 15, e0233510. [Google Scholar] [CrossRef]
- Sheehan, R.C.; Beltran, E.J.; Dingwell, J.B.; Wilken, J.M. Mediolateral angular momentum changes in persons with amputation during perturbed walking. Gait Posture 2015, 41, 795–800. [Google Scholar] [CrossRef] [Green Version]
- Kao, P.-C.; Pierro, M.A. Motor adaptation to cognitive challenges and walking perturbations in healthy young adults. Gait Posture 2021, 92, 167–175. [Google Scholar] [CrossRef]
- Nestico, J.; Novak, A.; Perry, S.D.; Mansfield, A. Does increased gait variability improve stability when faced with an expected balance perturbation during treadmill walking? Gait Posture 2021, 86, 94–100. [Google Scholar] [CrossRef]
- Rosenblum, U.; Melzer, I.; Zeilig, G.; Plotnik, M. Muscle activation profile is modulated by unexpected balance loss in walking. Gait Posture 2022, 93, 64–72. [Google Scholar] [CrossRef]
- Taborri, J.; Santuz, A.; Brüll, L.; Arampatzis, A.; Rossi, S. Measuring Kinematic Response to Perturbed Locomotion in Young Adults. Sensors 2022, 22, 672. [Google Scholar] [CrossRef]
- Martelli, D.; Kang, J.; Agrawal, S.K. A Single Session of Perturbation-Based Gait Training with the A-TPAD Improves Dynamic Stability in Healthy Young Subjects. In Proceedings of the 2017 International Conference on Rehabilitation Robotics, London, UK, 17–20 July 2017; Amirabdollahian, F., Burdet, E., Masia, L., Eds.; IEEE: Piscataway, NJ, USA, 2017; pp. 479–484, ISBN 978-1-5386-2296-4. [Google Scholar]
- Vlutters, M.; Van Asseldonk, E.H.F.; Van Der Kooij, H. Center of mass velocity based predictions in balance recovery following pelvis perturbations during human walking. J. Exp. Biol. 2016, 219, 1514–1523. [Google Scholar] [CrossRef] [Green Version]
- Zadravec, M.; Olenšek, A.; Matjačić, Z. The comparison of stepping responses following perturbations applied to pelvis during overground and treadmill walking. Technol. Health Care 2017, 25, 781–790. [Google Scholar] [CrossRef] [Green Version]
- Hof, A.L.; Duysens, J. Responses of human ankle muscles to mediolateral balance perturbations during walking. Hum. Mov. Sci. 2018, 57, 69–82. [Google Scholar] [CrossRef]
- Arvin, M.; Hoozemans, M.J.M.; Pijnappels, M.; Duysens, J.; Verschueren, S.M.; van Dieën, J.H. Where to Step? Contributions of Stance Leg Muscle Spindle Afference to Planning of Mediolateral Foot Placement for Balance Control in Young and Old Adults. Front. Physiol. 2018, 9, 1134. [Google Scholar] [CrossRef] [Green Version]
- Best, A.N.; Martin, J.-P.; Li, Q.G.; Wu, A.R. Stepping behavior contributes little to balance control against continuous mediolateral trunk perturbations. J. Exp. Biol. 2019, 222, jeb212787. [Google Scholar] [CrossRef]
- Kreter, N.; Rogers, C.L.; Fino, P.C. Anticipatory and reactive responses to underfoot perturbations during gait in healthy adults and individuals with a recent mild traumatic brain injury. Clin. Biomech. 2021, 90, 105496. [Google Scholar] [CrossRef]
- Francis, C.A.; Franz, J.R.; O’Connor, S.M.; Thelen, D.G. Gait variability in healthy old adults is more affected by a visual perturbation than by a cognitive or narrow step placement demand. Gait Posture 2015, 42, 380–385. [Google Scholar] [CrossRef] [Green Version]
- McIntosh, E.I.; Zettel, J.L.; Vallis, L.A. Stepping Responses in Young and Older Adults Following a Perturbation to the Support Surface During Gait. J. Mot. Behav. 2016, 49, 288–298. [Google Scholar] [CrossRef]
- Shulman, D.; Spencer, A.; Vallis, L.A. Age-related alterations in reactive stepping following unexpected mediolateral perturbations during gait initiation. Gait Posture 2018, 64, 130–134. [Google Scholar] [CrossRef]
- Rutherford, D.; Baker, M.; Urquhart, N.; Stanish, W. The effect of a frontal plane gait perturbation bout on knee biomechanics and muscle activation in older adults and individuals with knee osteoarthritis. Clin. Biomech. 2022, 92, 105574. [Google Scholar] [CrossRef]
- Lee-Confer, J.S.; Bradley, N.S.; Powers, C.M. Quantification of reactive arm responses to a slip perturbation. J. Biomech. 2022, 133, 110967. [Google Scholar] [CrossRef]
- Capin, J.J.; Zarzycki, R.; Arundale, A.; Cummer, K.; Snyder-Mackler, L.; Capin, J.J. Report of the Primary Outcomes for Gait Mechanics in Men of the ACL-SPORTS Trial: Secondary Prevention with and Without Perturbation Training Does Not Restore Gait Symmetry in Men 1 or 2 Years After ACL Reconstruction. Clin. Orthop. Relat. Res. 2017, 475, 2513–2522. [Google Scholar] [CrossRef]
- Martelli, D.; Xia, B.; Prado, A.; Agrawal, S.K. Gait adaptations during overground walking and multidirectional oscillations of the visual field in a virtual reality headset. Gait Posture 2019, 67, 251–256. [Google Scholar] [CrossRef]
- Robinovitch, S.N.; Feldman, F.; Yang, Y.; Schonnop, R.; Leung, P.M.; Sarraf, T.; Sims-Gould, J.; Loughin, M. Video capture of the circumstances of falls in elderly people residing in long-term care: An observational study. Lancet 2013, 381, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Nazifi, M.M.; Beschorner, K.E.; Hur, P. Do Walking Muscle Synergies Influence Propensity of Severe Slipping? Front. Hum. Neurosci. 2019, 13, 383. [Google Scholar] [CrossRef] [Green Version]
- Huijben, B.; van Schooten, K.S.; van Dieën, J.H.; Pijnappels, M. The effect of walking speed on quality of gait in older adults. Gait Posture 2018, 65, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Kongsuk, J.; Brown, D.A.; Hurt, C.P. Dynamic stability during increased walking speeds is related to balance confidence of older adults: A pilot study. Gait Posture 2019, 73, 86–92. [Google Scholar] [CrossRef]
- Rabago, C.A.; Dingwell, J.B.; Wilken, J.M. Reliability and Minimum Detectable Change of Temporal-Spatial, Kinematic, and Dynamic Stability Measures during Perturbed Gait. PLoS ONE 2015, 10, e0142083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollman, J.H.; Watkins, M.K.; Imhoff, A.C.; Braun, C.E.; Akervik, K.A.; Ness, D.K. Complexity, fractal dynamics and determinism in treadmill ambulation: Implications for clinical biomechanists. Clin. Biomech. 2016, 37, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Okubo, Y.; Schoene, D.; Caetano, M.J.; Pliner, E.M.; Osuka, Y.; Toson, B.; Lord, S.R. Stepping impairment and falls in older adults: A systematic review and meta-analysis of volitional and reactive step tests. Ageing Res. Rev. 2021, 66, 101238. [Google Scholar] [CrossRef] [PubMed]
- Degani, A.M.; Leonard, C.T.; Danna-Dos-Santos, A. The effects of early stages of aging on postural sway: A multiple domain balance assessment using a force platform. J. Biomech. 2017, 64, 8–15. [Google Scholar] [CrossRef]
- Pai, Y.C.; Yang, F.; Wening, J.D.; Pavol, M.J. Mechanisms of limb collapse following a slip among young and older adults. J. Biomech. 2006, 39, 2194–2204. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taylor, Z.; Walsh, G.S.; Hawkins, H.; Inacio, M.; Esser, P. Perturbations during Gait: A Systematic Review of Methodologies and Outcomes. Sensors 2022, 22, 5927. https://doi.org/10.3390/s22155927
Taylor Z, Walsh GS, Hawkins H, Inacio M, Esser P. Perturbations during Gait: A Systematic Review of Methodologies and Outcomes. Sensors. 2022; 22(15):5927. https://doi.org/10.3390/s22155927
Chicago/Turabian StyleTaylor, Zoe, Gregory S. Walsh, Hannah Hawkins, Mario Inacio, and Patrick Esser. 2022. "Perturbations during Gait: A Systematic Review of Methodologies and Outcomes" Sensors 22, no. 15: 5927. https://doi.org/10.3390/s22155927
APA StyleTaylor, Z., Walsh, G. S., Hawkins, H., Inacio, M., & Esser, P. (2022). Perturbations during Gait: A Systematic Review of Methodologies and Outcomes. Sensors, 22(15), 5927. https://doi.org/10.3390/s22155927