
On the Automatic Detection and Classification of Skin Cancer Using Deep Transfer Learning



Abstract
:1. Introduction
- Develop an artificial intelligence-based screening system for skin cancer (melanoma and non-melanoma) using dermoscopic images of the skin lesions as input. Such a system can aid in clinical screening tests, reduce errors, and improve early diagnosis;
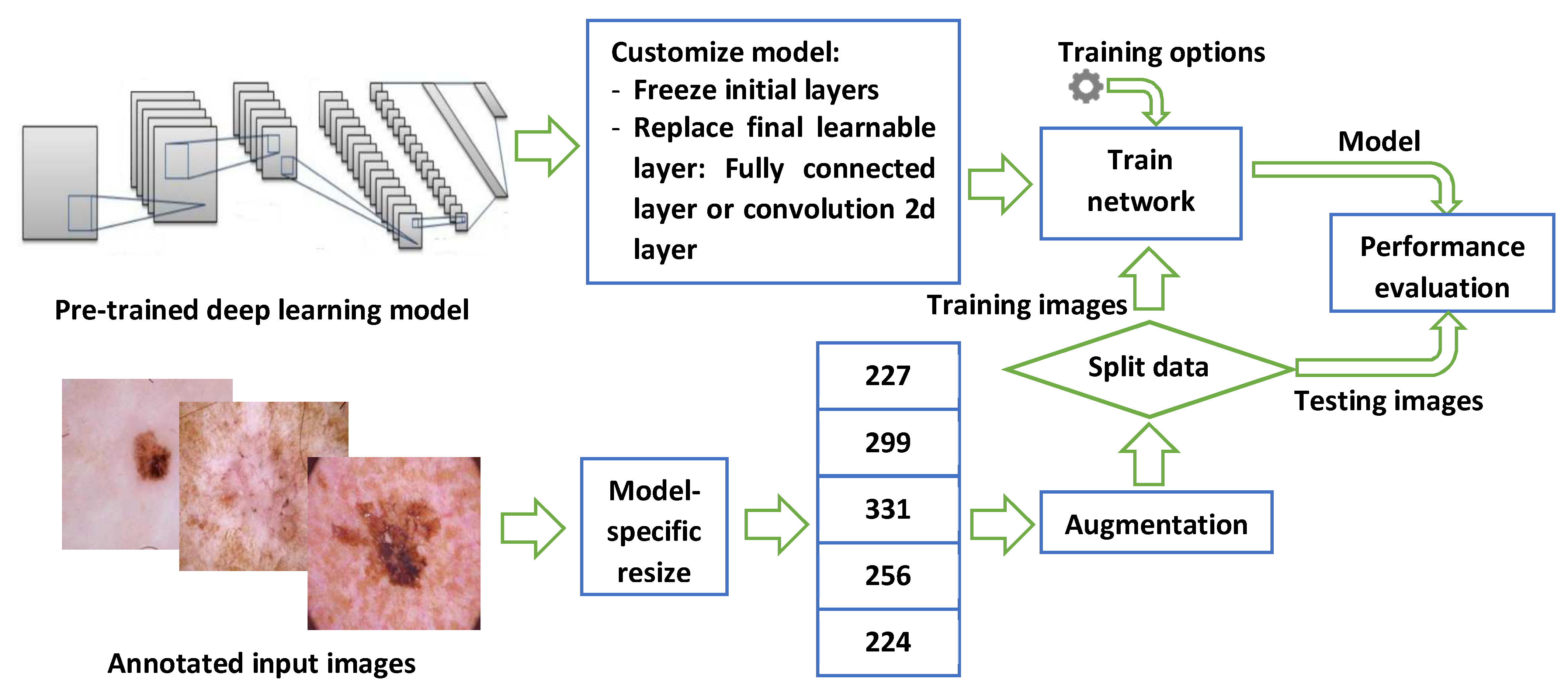
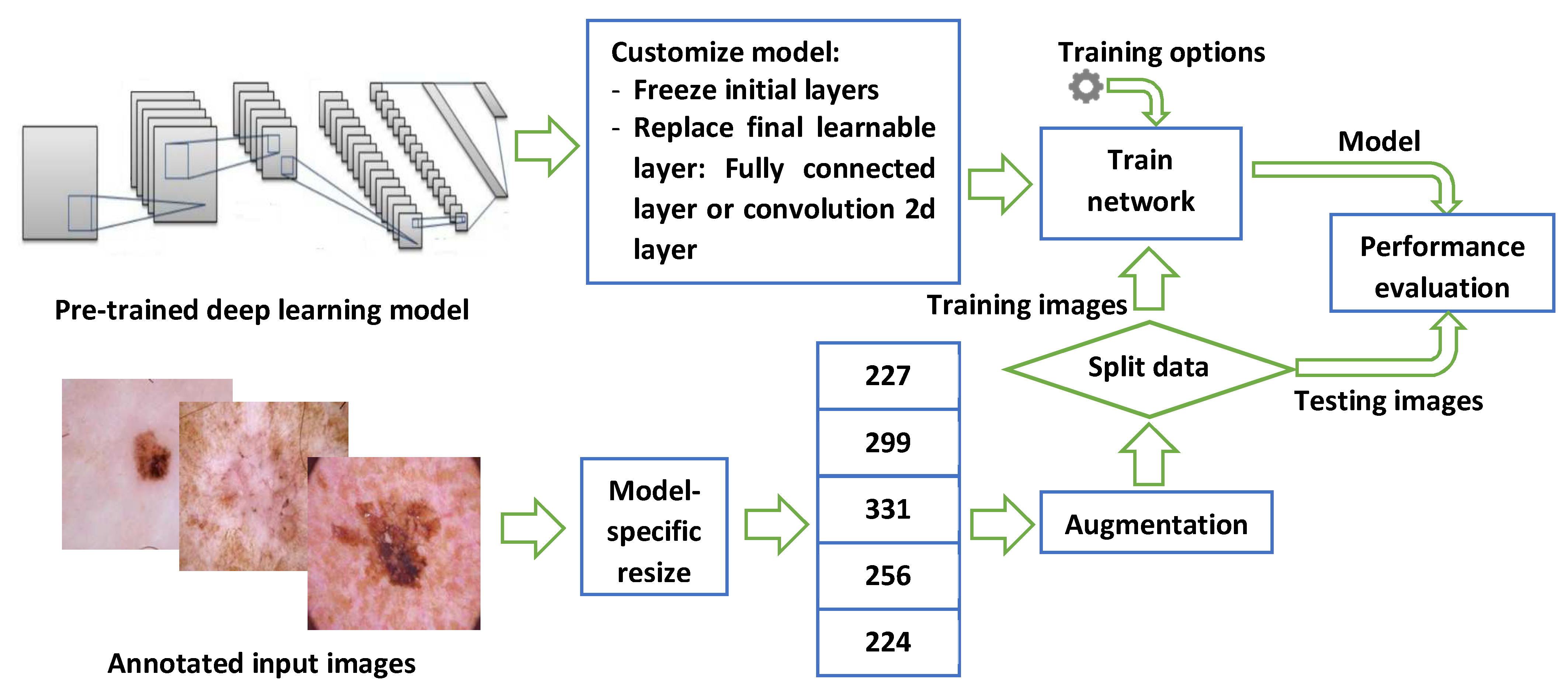
- Implement transfer learning of 13 deep convolutional neural networks models for the classification of skin lesion images into seven categories, including melanoma, benign keratosis-like lesions, and five other non-melanoma cancers;
- Evaluate classification performance using common relevant metrics for all models. In addition, the training behavior and time requirements were also included.
2. Related Work
3. Materials and Methods
3.1. Dataset
3.2. Deep Learning Models
3.3. Performance Evaluation Metrics and Setup
4. Results and Discussion
Special Cases
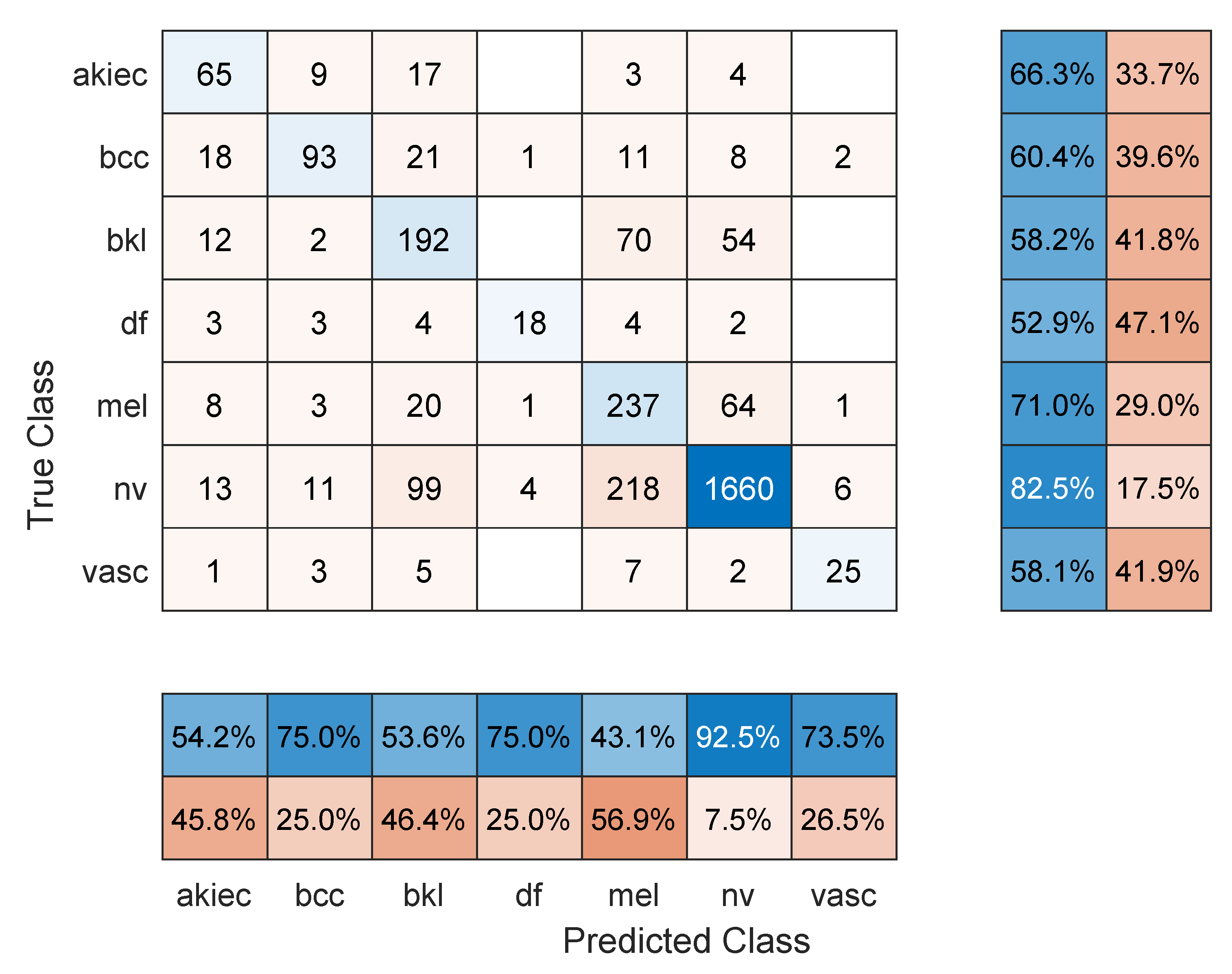
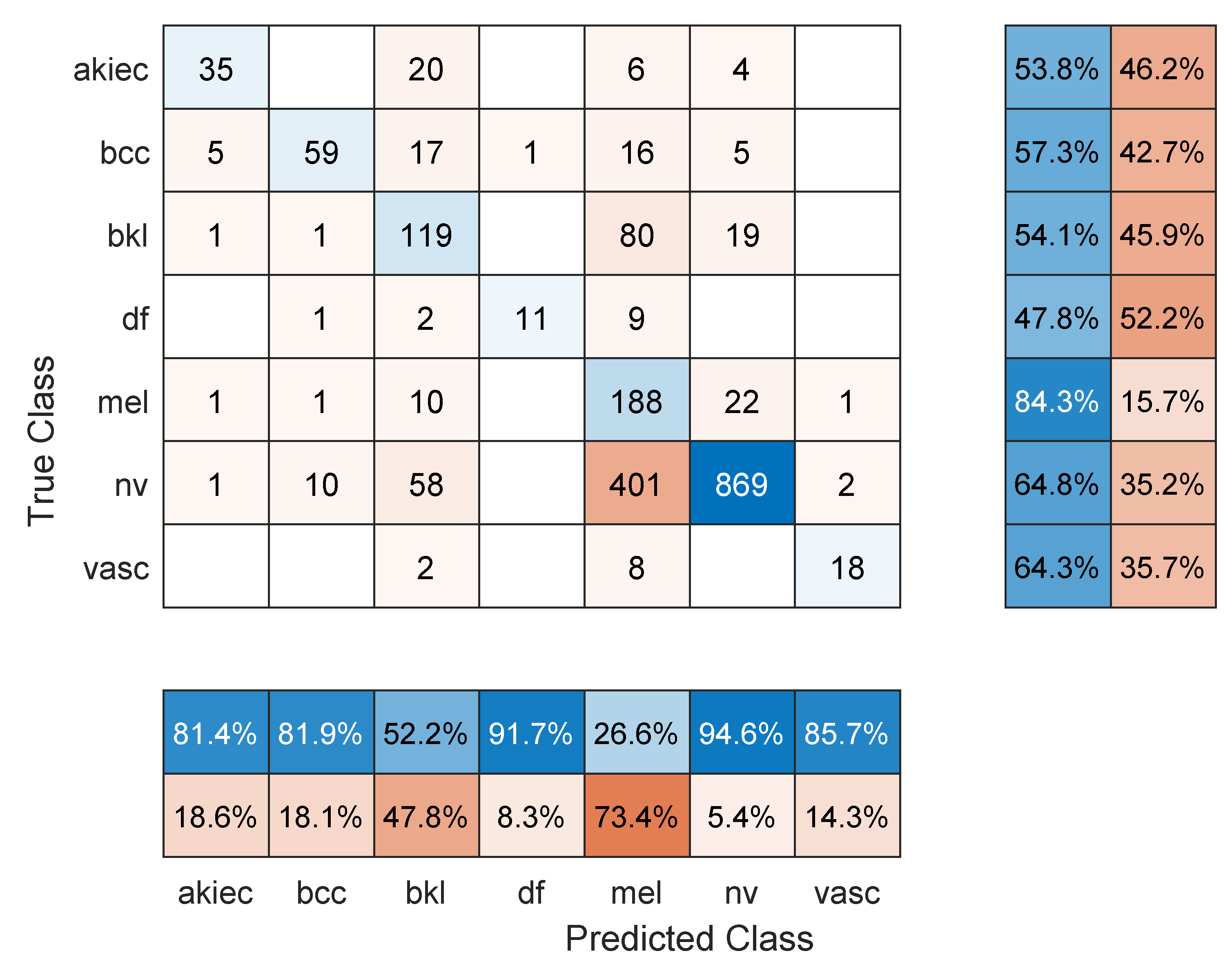
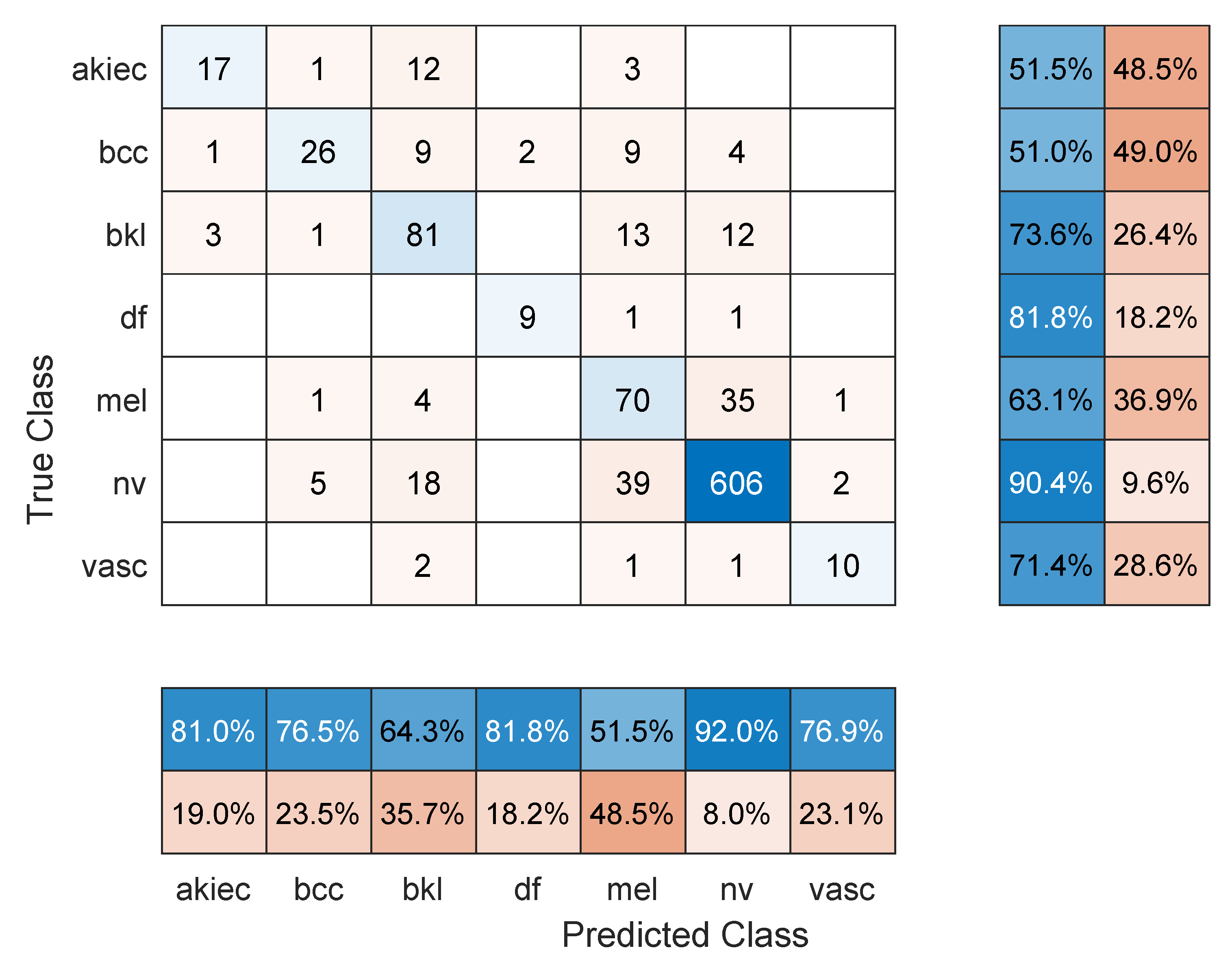
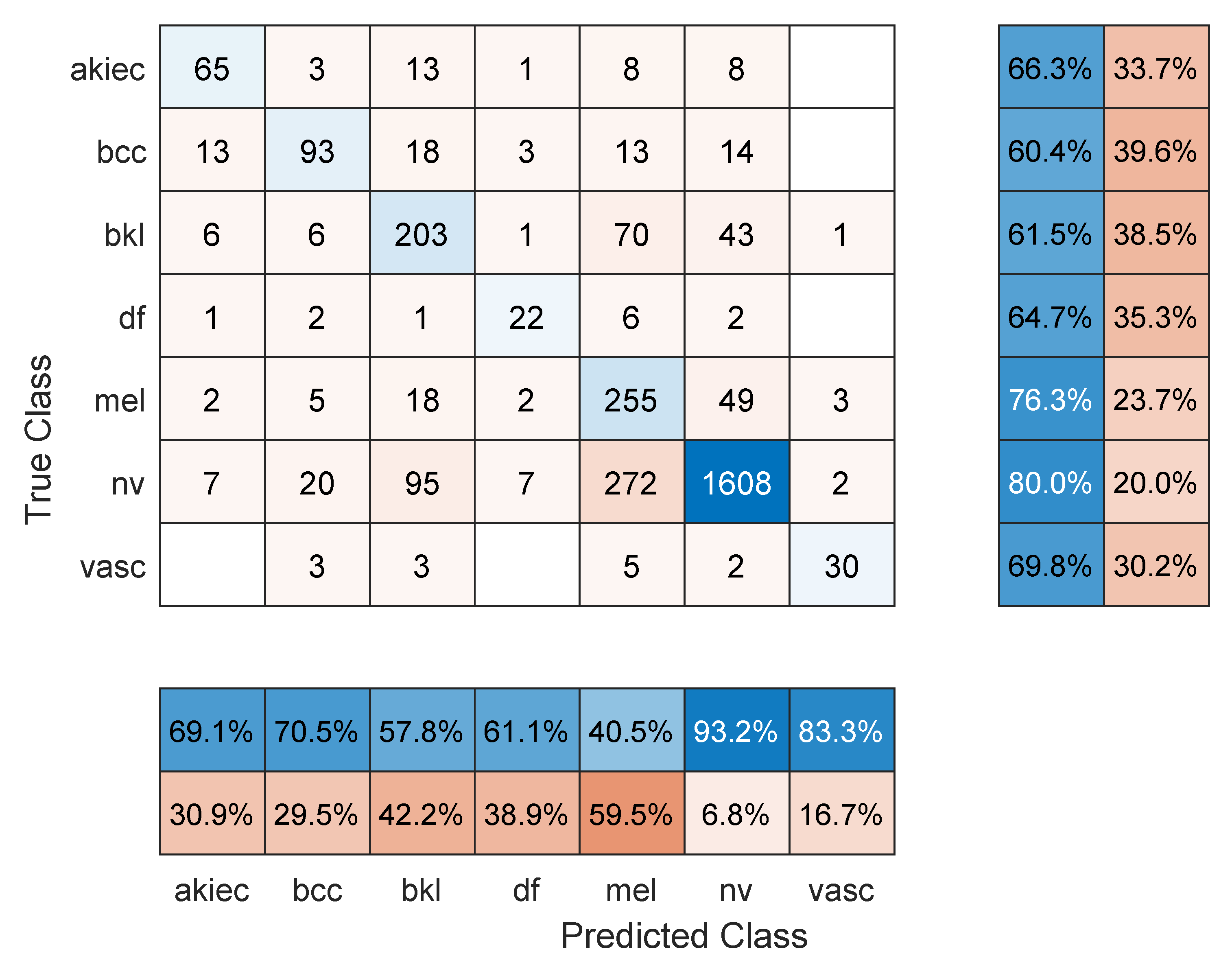
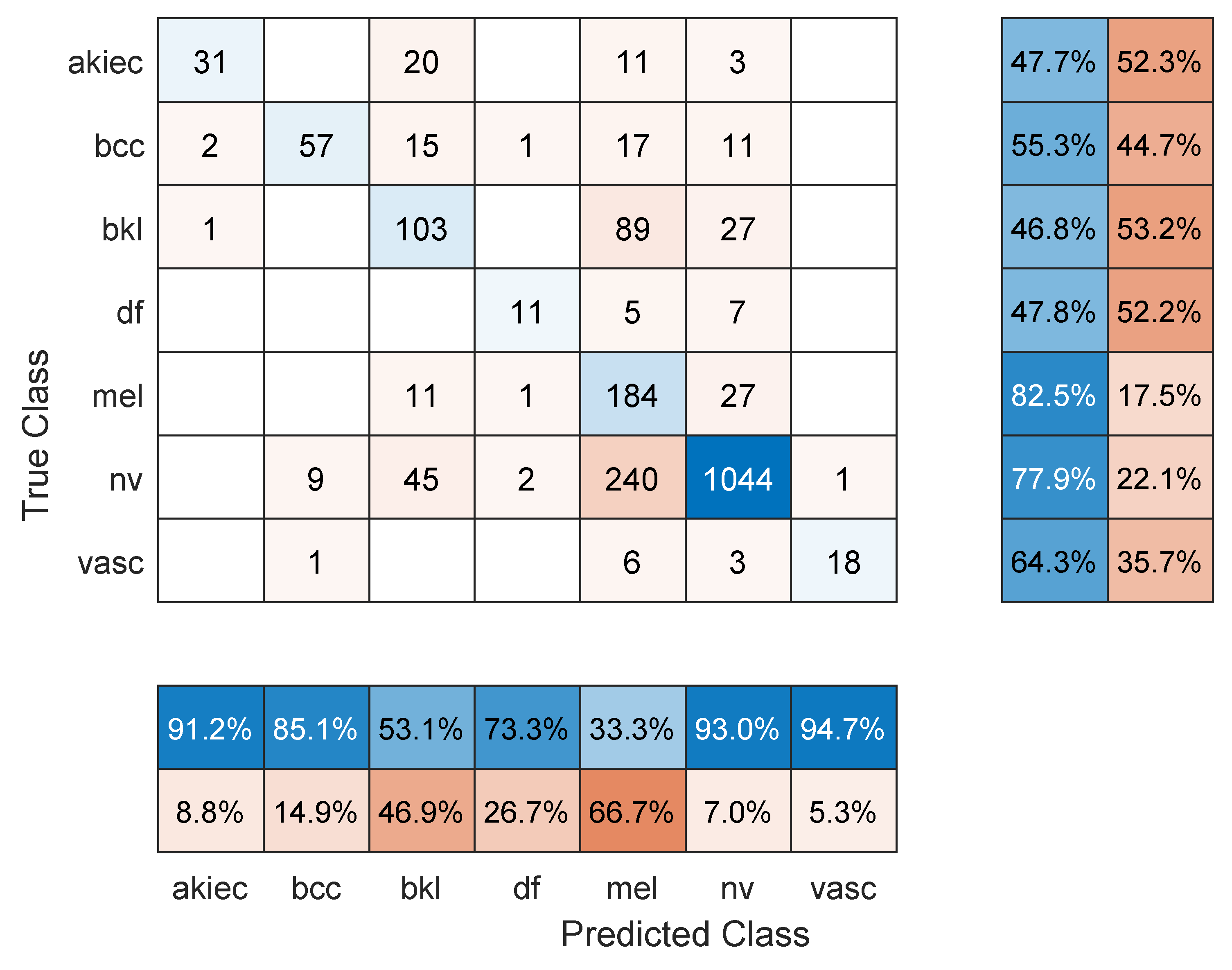
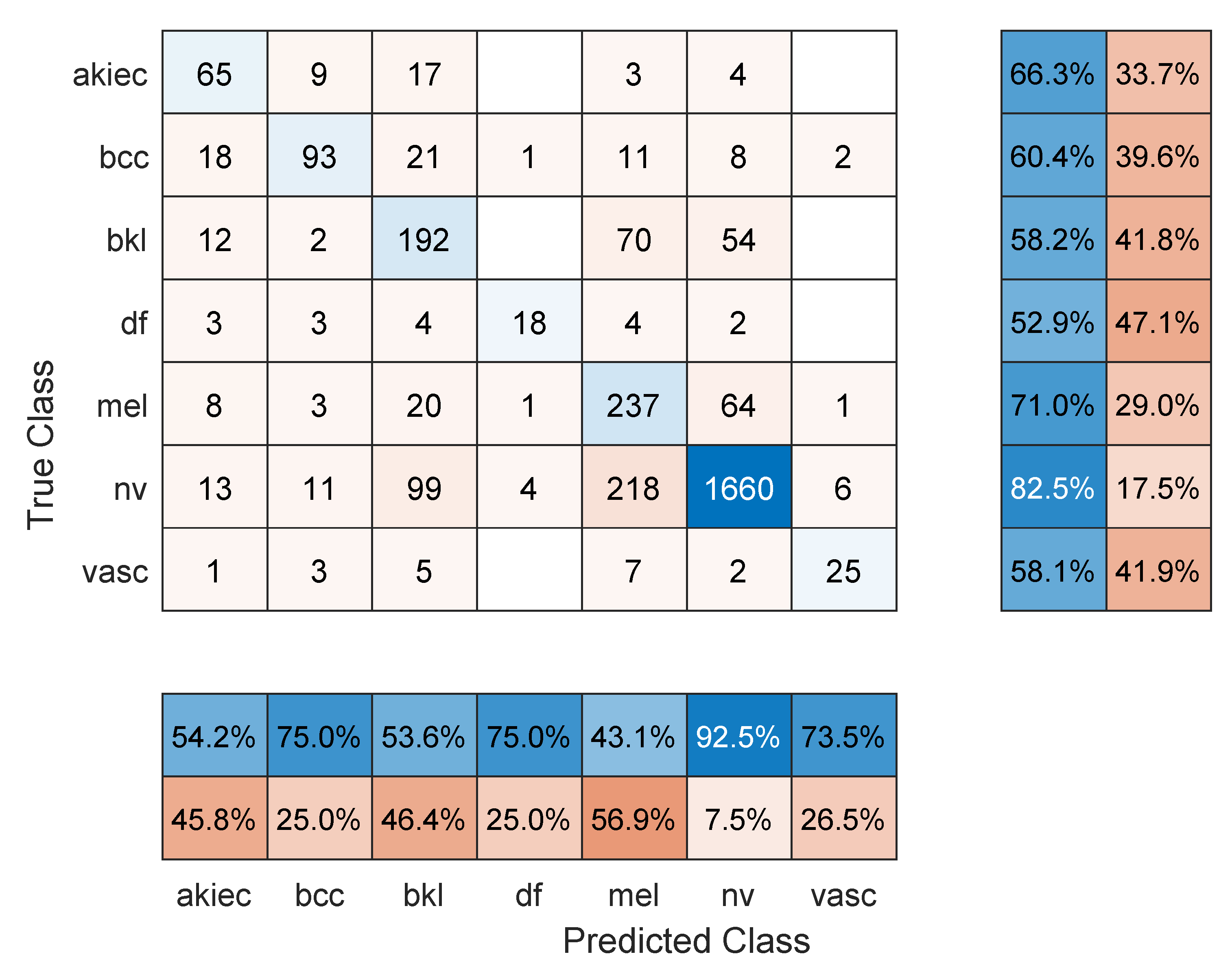
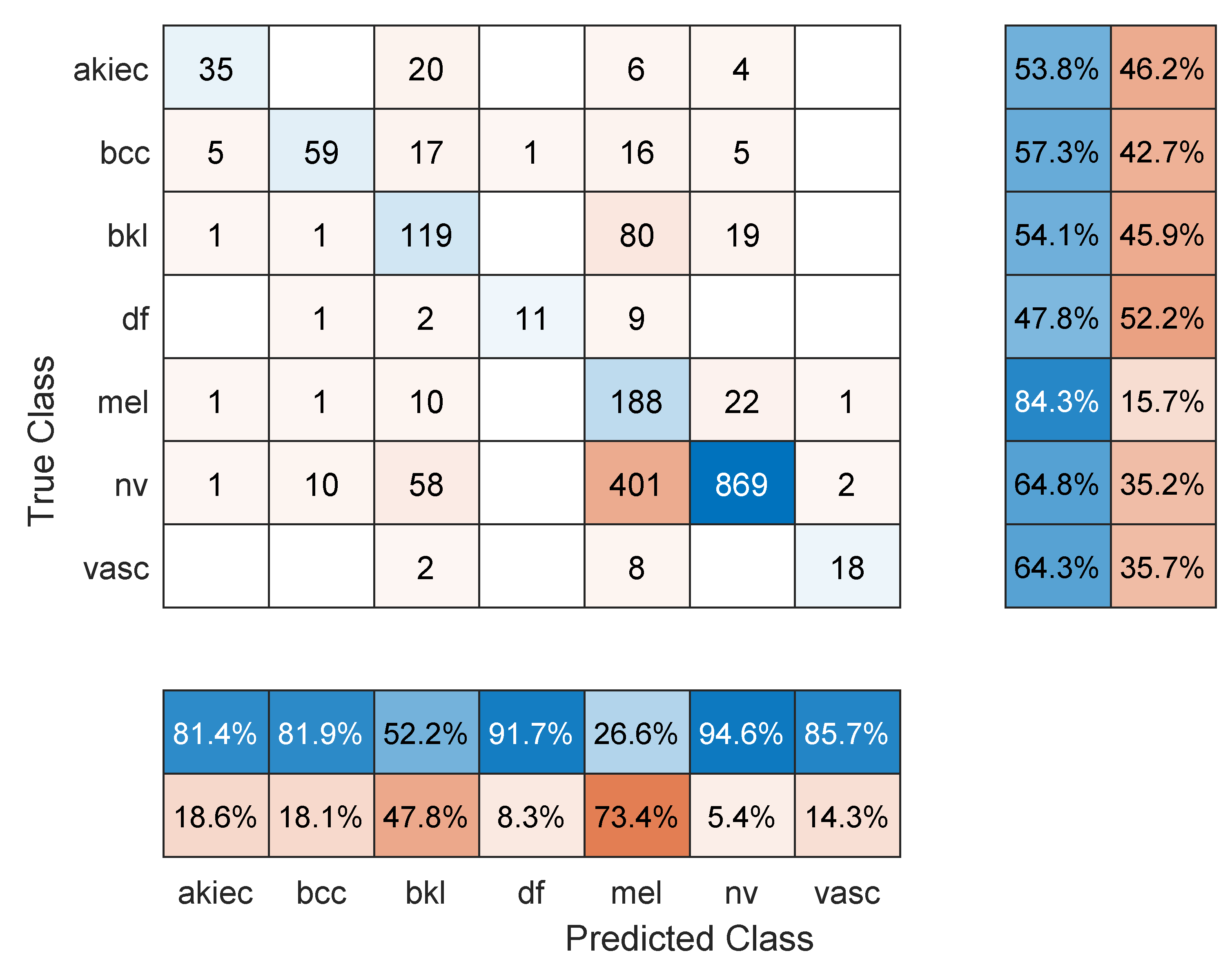
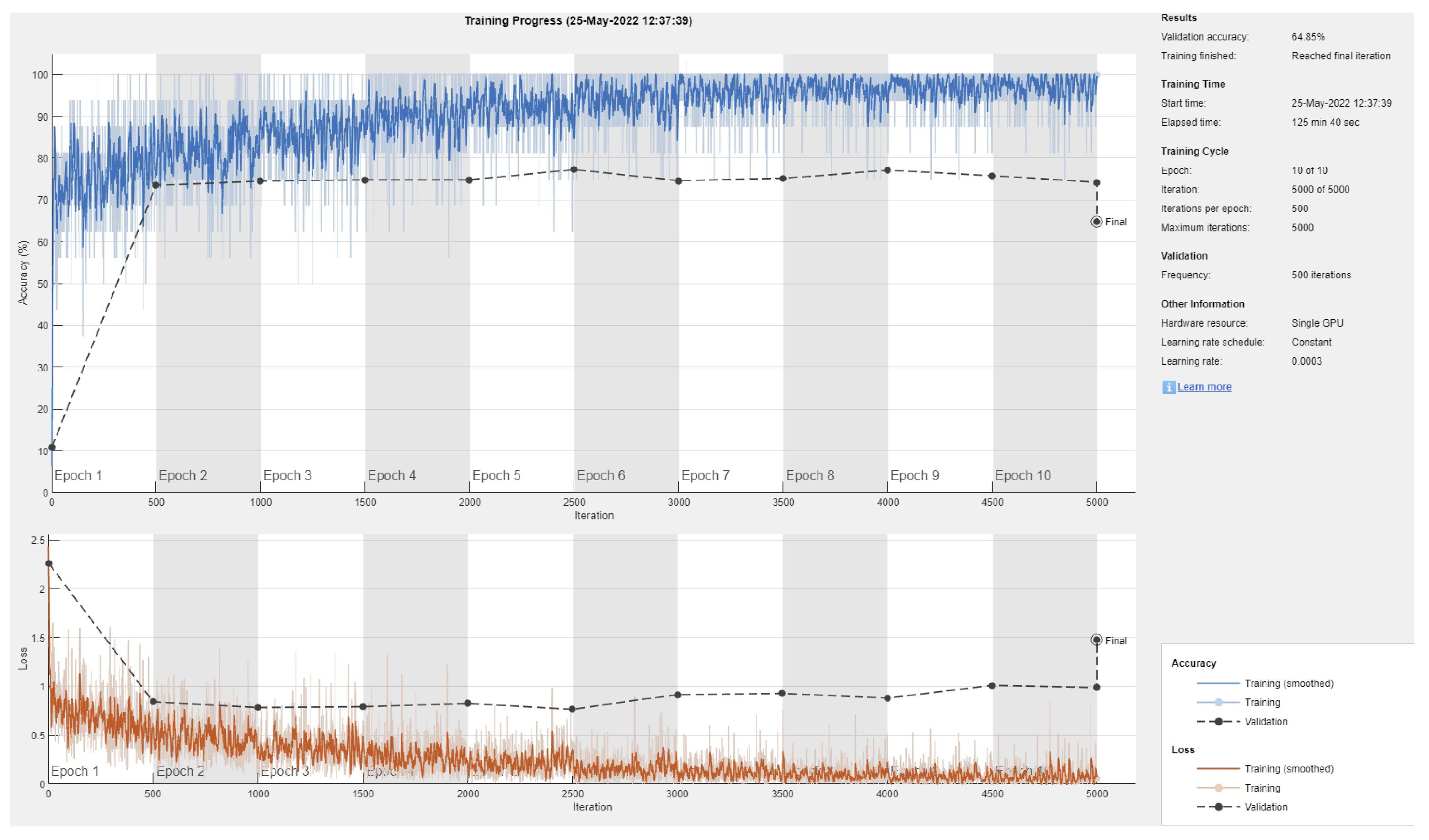
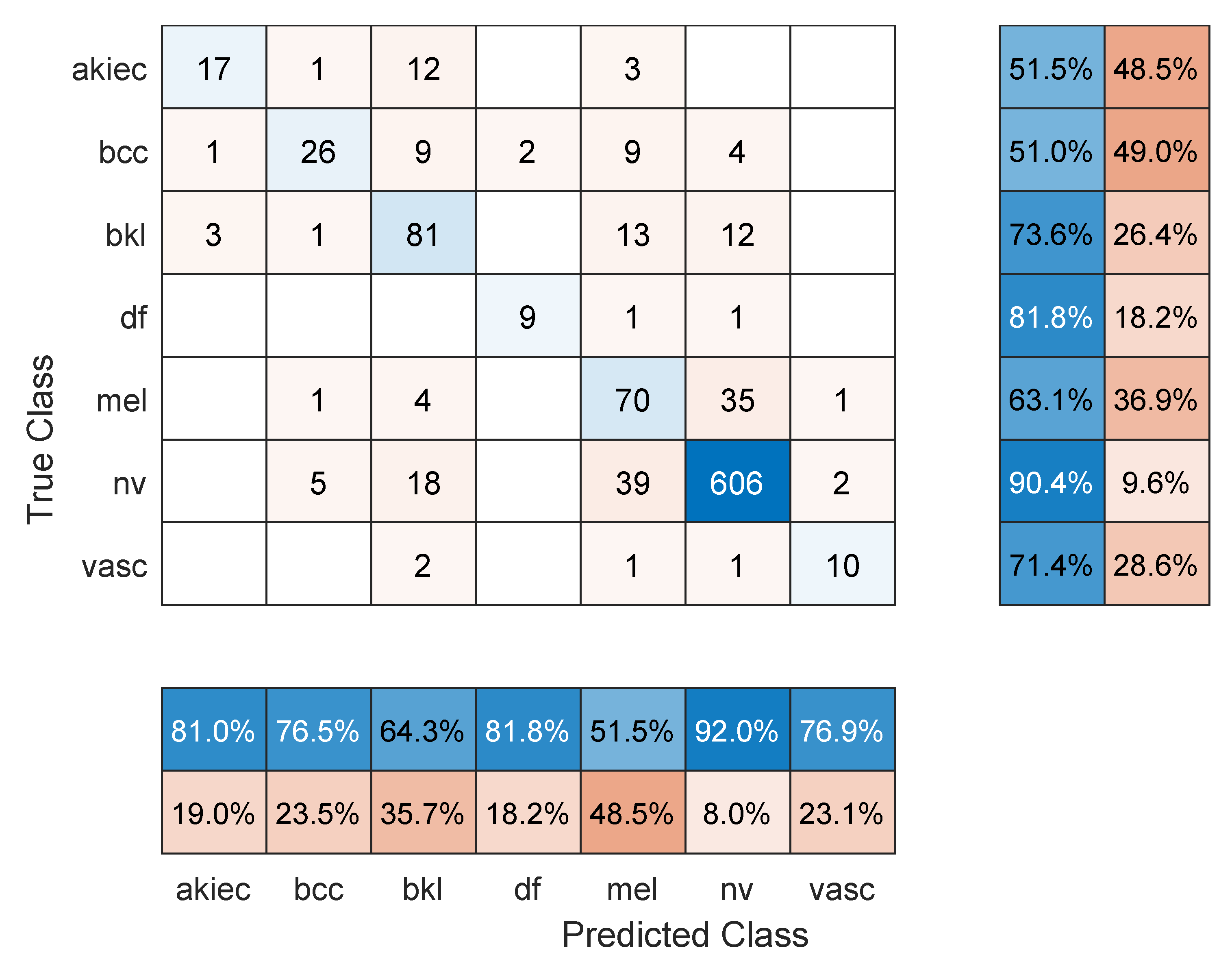
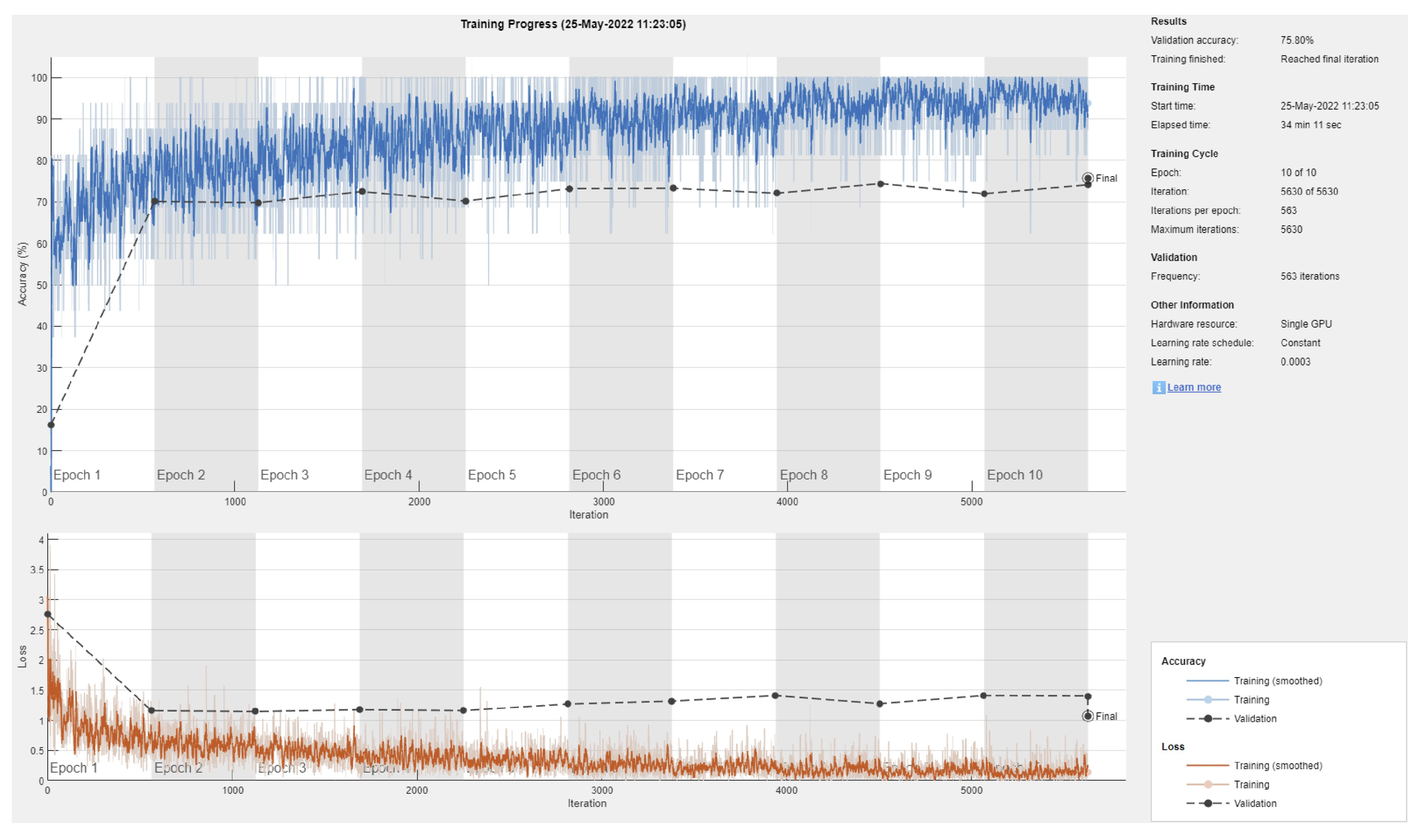
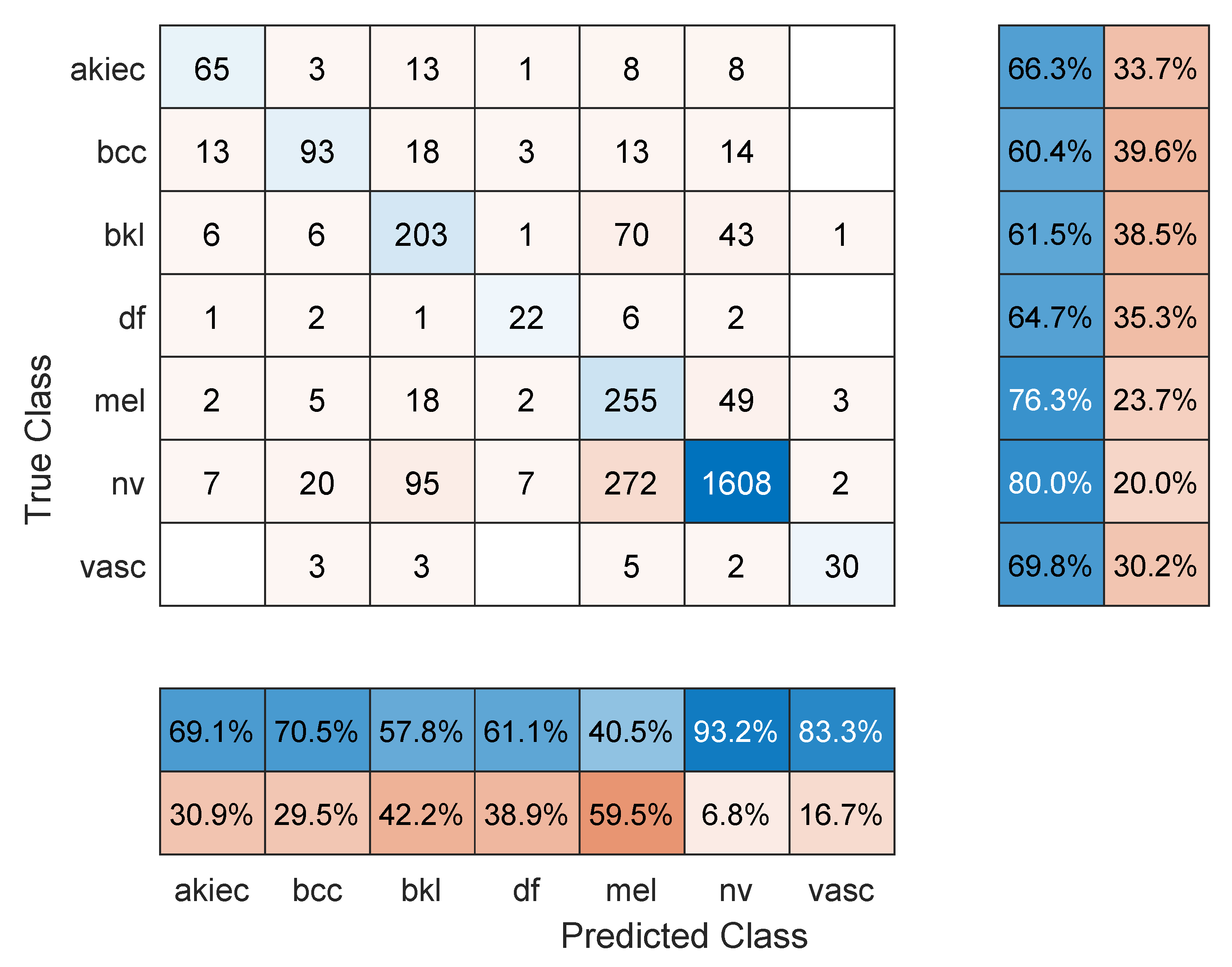
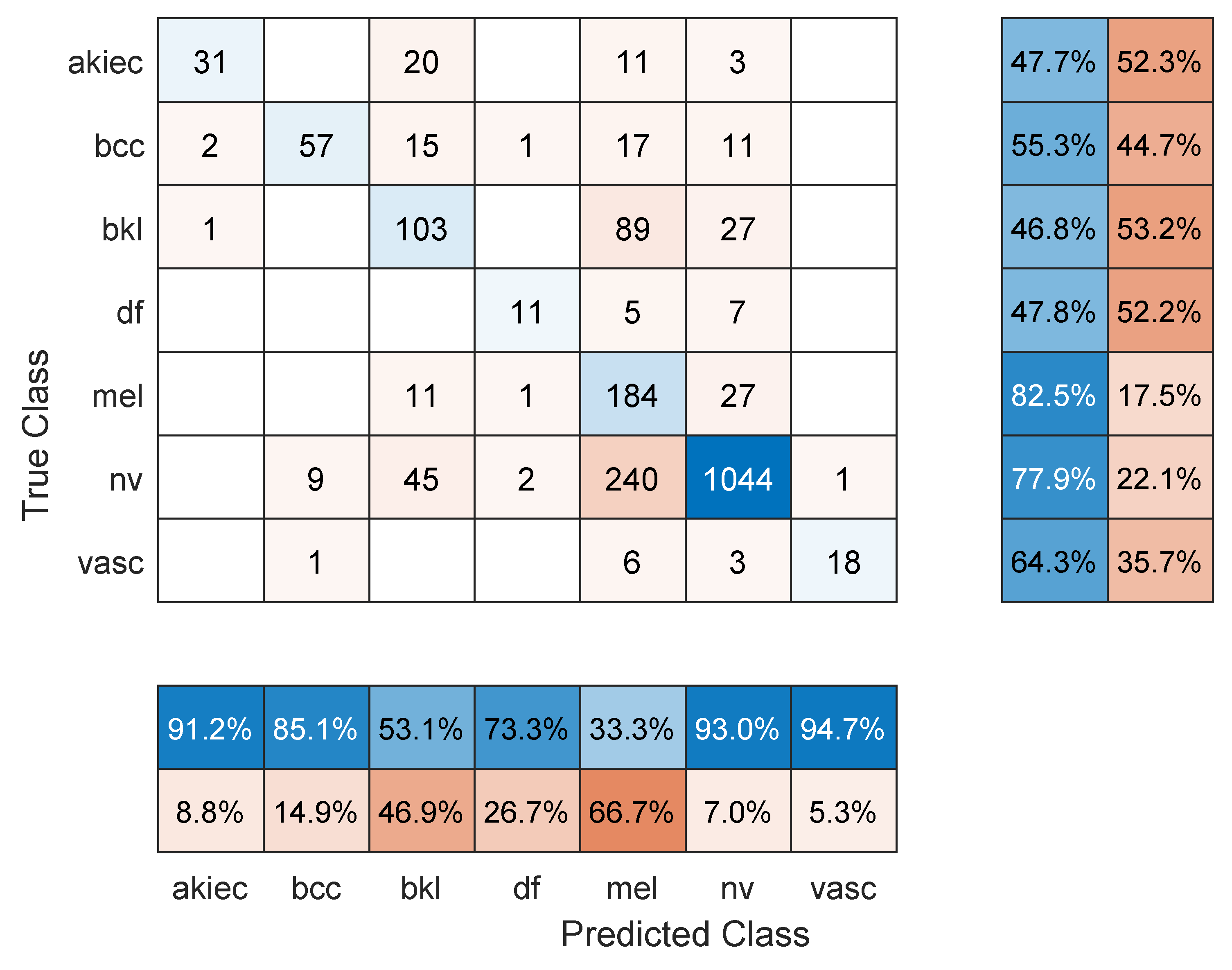
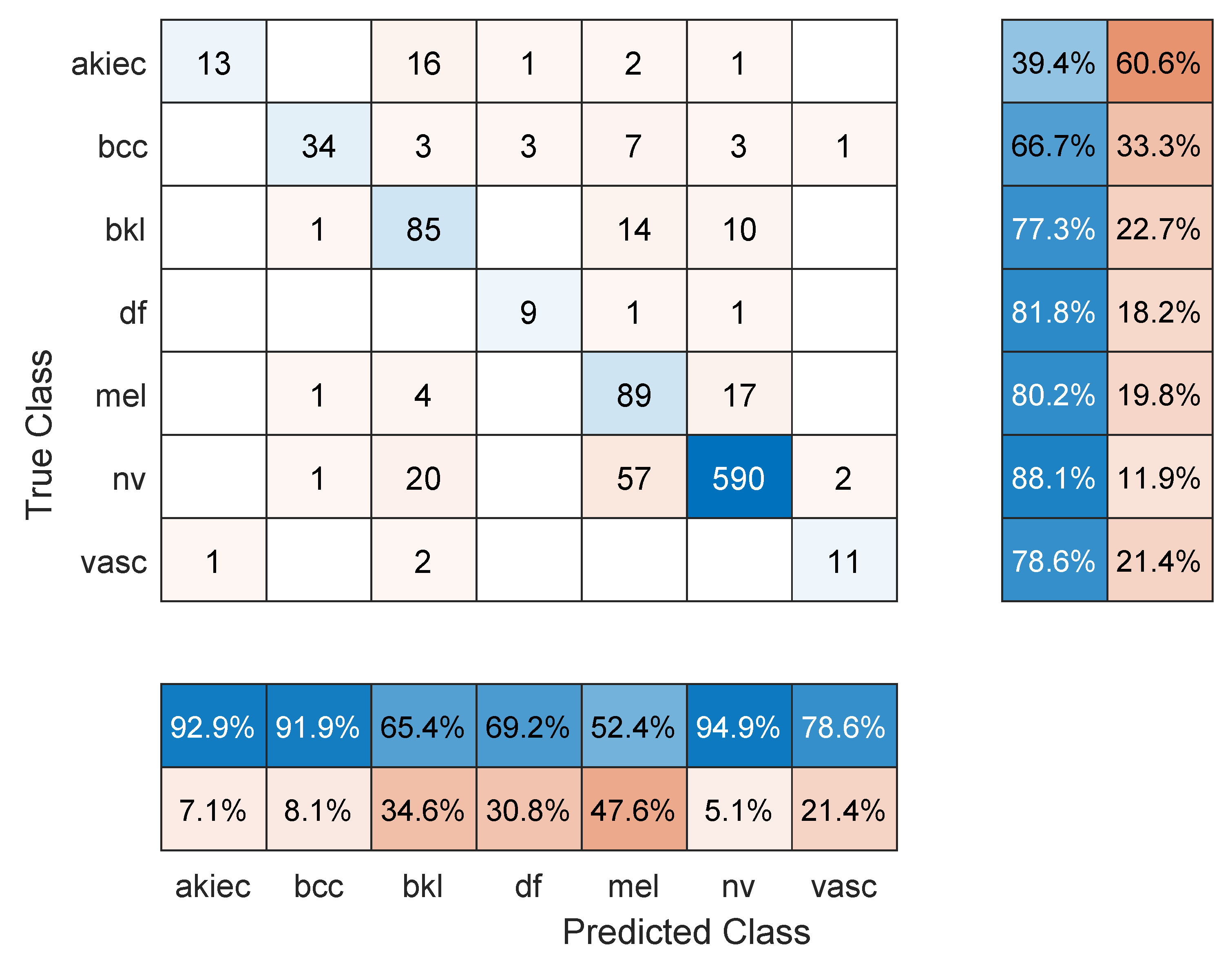
- Maximum number of epochs. Increasing the number of epochs will require more training time and may achieve better performance if the model has more room to learn, especially in large datasets. However, an exaggerated value for this hyper-parameter may lead to overfitting. Three models were retrained with a maximum number of epochs = 50. These were: Resnet101 with a 70/30 data split, DenseNet201 with an 80/20 data split, and DarkNet-53 with a 90/10 data split. In comparison to the values in Table 1, Table 2 and Table 3, the F1 score for Resnet101 improved slightly to 67.2% (was 64.3%), DenseNet201 performed a little worse with an F1-score of 63.7%, down from 66.1% in Table 2 (i.e., the model started to overfit the training data), and Darknet-53 improved to an F1-score of 83.1%. The other performance metrics showed similar trends to the F1 score. Figure 8, Figure 9 and Figure 10 show the corresponding confusion matrices;
- Classifying a lesser number of skin cancer types. Since the dataset is highly imbalanced with some classes having a significantly smaller number of images in the dataset (e.g., 115 DF and 142 VASC), it is worthwhile to explore several subsets of the classification problem as follows:
- −
- Eliminate the DF and VASC classes and perform 5-class classification. The same three models and corresponding data split as in the previous case with a maximum number of epochs = 10 were used. Surprisingly, in comparison to Table 1, Table 2 and Table 3, the F1 score displayed very small change (Resnet101: 64.8%, DenseNet201: 65.2%, and DarkNet-53: 67.1%), which was similar to the trend in the other performance metrics;
- −
- Eliminate the BCC (514 images), AKIEC (327 images), DF, and VASC classes and perform 3-class classification. The Resnet101 (70/30 data split), DenseNet201 (80/20 data split), and DarkNet-53 (90/10) were used with a maximum number of epochs =10. An easier classification problem has resulted in an improved F1 score for Resnet101 and DarkNet-53 of 71.1% and 72.8%, respectively. However, DenseNet201 performed worse at 62.3%, probably due to overfitting;
- −
- Using the same setup as above, perform pair-wise 2-class classification on the three classes, NV, MEL, and BKL. For the MEL vs. BKL classification, the F1 score of Resnet101 = 80.6%, DenseNet = 73.44%, and DarkNet201 = 83.7%. For the NV vs. MEL classification, all models performed badly. The F1 score for Resnet101 = 58.8%, DenseNet201 = 55.13%, and DarkNet-53 = 63.4%. Although the two classes have a good number of images, it seems like the similarities between the two types are too difficult to spot. Moreover, the lack of proper image cropping (i.e., elimination of useless parts of the images and keeping the lesion) contributed to this factor as it consumes a significant part of the image representation, especially that these algorithms require a scaled-down copy of the input, as mentioned in Section 3. The last pair-wise classification problem is NV vs. BKL, for which Resnet 101 achieved an F1 score = 72.8% (93% accuracy), DenseNet201 reported a 71.8% F1 score and 91.9% accuracy, and DarkNet-53 managed a 70.0% F1 score and 89.9% accuracy.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ABCD | Asymmetry, border, color, diameter |
| AI | Artificial intelligence |
| CNN | Convolutional neural networks |
| DHS | Digital hair removal |
| Intra-SSIM | Intra-structural similarity |
| ROI | Regions of interest |
| CIELAB | International Commission on Illumination Lightness A, B |
| RGB | Red, green, blue |
| FrCN | Full-resolution convolutional networks |
| SVM | Support-vector machine |
| LLP | Logistic label propagation |
| KNN | K-nearest neighbors |
| HAM | Human against machine |
| AKIEC | Actinic keratoses and intraepithelial carcinoma |
| BCC | Basal cell carcinoma |
| BLS | Benign keratosis-like lesions |
| DF | Dermatofibroma |
| Mel | Melanoma |
| NV | Melanocytic nevi |
| VASC | Vascular lesions |
| TP | True positive |
| TN | True negative |
| FN | False negative |
| FP | False positive |
| N | Negatives |
| P | Positives |
| SGDM | Stochastic gradient descent with momentum |
References
- Li, W.; Raj, A.N.J.; Tjahjadi, T.; Zhuang, Z. Digital hair removal by deep learning for skin lesion segmentation. Pattern Recognit. 2021, 117, 107994. [Google Scholar] [CrossRef]
- Tschandl, P.; Rosendahl, C.; Kittler, H. The HAM10000 dataset, a large collection of multi-source dermatoscopic images of common pigmented skin lesions. Sci. Data 2018, 5, 180161. [Google Scholar] [CrossRef]
- Arora, R.; Raman, B.; Nayyar, K.; Awasthi, R. Automated skin lesion segmentation using attention-based deep convolutional neural network. Biomed. Signal Process. Control 2021, 65, 102358. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X. Melanoma segmentation based on deep learning. Comput. Assist. Surg. 2017, 22, 267–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, R.B.; Filho, M.E.; Ma, Z.; Papa, J.P.; Pereira, A.S.; Tavares, J.M.R. Computational methods for the image segmentation of pigmented skin lesions: A review. Comput. Methods Programs Biomed. 2016, 131, 127–141. [Google Scholar] [CrossRef] [Green Version]
- das Chagas, J.V.S.; Ivo, R.F.; Guimarães, M.T.; de A. Rodrigues, D.; de S. Rebouças, E.; Filho, P.P.R. Fast fully automatic skin lesions segmentation probabilistic with Parzen window. Comput. Med. Imaging Graph. 2020, 85, 101774. [Google Scholar] [CrossRef]
- Mahbod, A.; Schaefer, G.; Wang, C.; Dorffner, G.; Ecker, R.; Ellinger, I. Transfer learning using a multi-scale and multi-network ensemble for skin lesion classification. Comput. Methods Programs Biomed. 2020, 193, 105475. [Google Scholar] [CrossRef]
- Borges, A.L.; Nicoletti, S.; Dufrechou, L.; Centanni, A.N. Dermatoscopy in the Public Health Environment. In Dermatology in Public Health Environments; Springer International Publishing: Berlin/Heidelberg, Germany, 2017; pp. 1157–1188. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, A.; Gul, N.; Anjum, M.A.; Nisar, M.W.; Azam, F.; Bukhari, S.A.C. Integrated design of deep features fusion for localization and classification of skin cancer. Pattern Recognit. Lett. 2020, 131, 63–70. [Google Scholar] [CrossRef]
- Pathan, S.; Prabhu, K.G.; Siddalingaswamy, P. Techniques and algorithms for computer aided diagnosis of pigmented skin lesions—A review. Biomed. Signal Process. Control 2018, 39, 237–262. [Google Scholar] [CrossRef]
- Chatterjee, S.; Dey, D.; Munshi, S.; Gorai, S. Extraction of features from cross correlation in space and frequency domains for classification of skin lesions. Biomed. Signal Process. Control 2019, 53, 101581. [Google Scholar] [CrossRef]
- Premaladha, J.; Ravichandran, K.S. Novel Approaches for Diagnosing Melanoma Skin Lesions Through Supervised and Deep Learning Algorithms. J. Med. Syst. 2016, 40, 96. [Google Scholar] [CrossRef]
- Kasmi, R.; Mokrani, K. Classification of malignant melanoma and benign skin lesions: Implementation of automatic ABCD rule. IET Image Process. 2016, 10, 448–455. [Google Scholar] [CrossRef]
- Yu, Z.; Jiang, F.; Zhou, F.; He, X.; Ni, D.; Chen, S.; Wang, T.; Lei, B. Convolutional descriptors aggregation via cross-net for skin lesion recognition. Appl. Soft Comput. 2020, 92, 106281. [Google Scholar] [CrossRef]
- Celebi, M.E.; Kingravi, H.A.; Uddin, B.; Iyatomi, H.; Aslandogan, Y.A.; Stoecker, W.V.; Moss, R.H. A methodological approach to the classification of dermoscopy images. Comput. Med. Imaging Graph. 2007, 31, 362–373. [Google Scholar] [CrossRef] [Green Version]
- Goel, N.; Yadav, A.; Singh, B.M. Breast Cancer Segmentation Recognition Using Explored DCT-DWT based Compression. Recent Patents Eng. 2022, 16, 55–64. [Google Scholar] [CrossRef]
- Hosny, K.M.; Kassem, M.A.; Foaud, M.M. Classification of skin lesions using transfer learning and augmentation with Alex-net. PLoS ONE 2019, 14, e0217293. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, R.B.; Pereira, A.S.; Tavares, J.M.R. Skin lesion computational diagnosis of dermoscopic images: Ensemble models based on input feature manipulation. Comput. Methods Programs Biomed. 2017, 149, 43–53. [Google Scholar] [CrossRef] [Green Version]
- Khasawneh, N.; Fraiwan, M.; Fraiwan, L.; Khassawneh, B.; Ibnian, A. Detection of COVID-19 from Chest X-ray Images Using Deep Convolutional Neural Networks. Sensors 2021, 21, 5940. [Google Scholar] [CrossRef]
- Shorten, C.; Khoshgoftaar, T.M. A survey on Image Data Augmentation for Deep Learning. J. Big Data 2019, 6. [Google Scholar] [CrossRef]
- Kim, H.E.; Cosa-Linan, A.; Santhanam, N.; Jannesari, M.; Maros, M.E.; Ganslandt, T. Transfer learning for medical image classification: A literature review. BMC Med. Imaging 2022, 22, 69. [Google Scholar] [CrossRef]
- Liu, L.; Mou, L.; Zhu, X.X.; Mandal, M. Automatic skin lesion classification based on mid-level feature learning. Comput. Med. Imaging Graph. 2020, 84, 101765. [Google Scholar] [CrossRef]
- Pour, M.P.; Seker, H. Transform domain representation-driven convolutional neural networks for skin lesion segmentation. Expert Syst. Appl. 2020, 144, 113129. [Google Scholar] [CrossRef]
- Al-masni, M.A.; Al-antari, M.A.; Choi, M.T.; Han, S.M.; Kim, T.S. Skin lesion segmentation in dermoscopy images via deep full resolution convolutional networks. Comput. Methods Programs Biomed. 2018, 162, 221–231. [Google Scholar] [CrossRef]
- Dash, M.; Londhe, N.D.; Ghosh, S.; Semwal, A.; Sonawane, R.S. PsLSNet: Automated psoriasis skin lesion segmentation using modified U-Net-based fully convolutional network. Biomed. Signal Process. Control 2019, 52, 226–237. [Google Scholar] [CrossRef]
- Xie, F.; Yang, J.; Liu, J.; Jiang, Z.; Zheng, Y.; Wang, Y. Skin lesion segmentation using high-resolution convolutional neural network. Comput. Methods Programs Biomed. 2020, 186, 105241. [Google Scholar] [CrossRef]
- Serte, S.; Demirel, H. Gabor wavelet-based deep learning for skin lesion classification. Comput. Biol. Med. 2019, 113, 103423. [Google Scholar] [CrossRef]
- Manzo, M.; Pellino, S. Bucket of Deep Transfer Learning Features and Classification Models for Melanoma Detection. J. Imaging 2020, 6, 129. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Singhania, U.; Tripathy, B.; Nasr, E.A.; Aboudaif, M.K.; Kamrani, A.K. Deep Learning-Based Transfer Learning for Classification of Skin Cancer. Sensors 2021, 21, 8142. [Google Scholar] [CrossRef] [PubMed]
- Fraiwan, M.; Audat, Z.; Fraiwan, L.; Manasreh, T. Using deep transfer learning to detect scoliosis and spondylolisthesis from X-ray images. PLoS ONE 2022, 17, e0267851. [Google Scholar] [CrossRef] [PubMed]
- Fraiwan, M.; Fraiwan, L.; Alkhodari, M.; Hassanin, O. Recognition of pulmonary diseases from lung sounds using convolutional neural networks and long short-term memory. J. Ambient. Intell. Humaniz. Comput. 2021. [Google Scholar] [CrossRef]
- Iandola, F.N.; Moskewicz, M.W.; Ashraf, K.; Han, S.; Dally, W.J.; Keutzer, K. SqueezeNet: AlexNet-level accuracy with 50x fewer parameters and <1MB model size. arXiv 2016, arXiv:1602.07360. [Google Scholar]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar] [CrossRef] [Green Version]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A.A. Inception-v4, Inception-ResNet and the Impact of Residual Connections on Learning. In Proceedings of the Thirty-First AAAI Conference on Artificial Intelligence, AAAI’17, San Francisco, CA, USA, 4–9 February 2017; AAAI Press: Menlo Park, CA, USA, 2017; pp. 4278–4284. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2261–2269. [Google Scholar] [CrossRef] [Green Version]
- Chollet, F. Xception: Deep Learning with Depthwise Separable Convolutions. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 1800–1807. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zhou, X.; Lin, M.; Sun, J. ShuffleNet: An Extremely Efficient Convolutional Neural Network for Mobile Devices. In Proceedings of the 2018 IEEE/CVF Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 6848–6856. [Google Scholar] [CrossRef] [Green Version]
- Redmon, J. Darknet: Open Source Neural Networks in C, 2013–2016. Available online: https://pjreddie.com/darknet (accessed on 21 June 2022).
- Tan, M.; Le, Q. EfficientNet: Rethinking Model Scaling for Convolutional Neural Networks. In Proceedings of the 36th International Conference on Machine Learning, Long Beach, CA, USA, 10–15 June 2019; Chaudhuri, K., Salakhutdinov, R., Eds.; PMLR: London, UK, 2019; Volume 97, pp. 6105–6114. [Google Scholar]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Fei-Fei, L. ImageNet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar] [CrossRef] [Green Version]
- Tharwat, A. Classification assessment methods. Appl. Comput. Inform. 2020, 17, 168–192. [Google Scholar] [CrossRef]
- Najafabadi, M.M.; Villanustre, F.; Khoshgoftaar, T.M.; Seliya, N.; Wald, R.; Muharemagic, E. Deep learning applications and challenges in big data analytics. J. Big Data 2015, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Bailly, A.; Blanc, C.; Francis, É.; Guillotin, T.; Jamal, F.; Wakim, B.; Roy, P. Effects of dataset size and interactions on the prediction performance of logistic regression and deep learning models. Comput. Methods Programs Biomed. 2022, 213, 106504. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | F1 Score | Precision | Recall | Specificity | Accuracy |
|---|---|---|---|---|---|
| SqueezeNet | 51.2% | 63.1% | 49.6% | 93.8% | 71.7% |
| GoogLeNet | 55.4% | 63.2% | 53.4% | 94.3% | 74.0% |
| Inceptionv3 | 61.5% | 65.5% | 60.7% | 94.5% | 74.2% |
| DenseNet201 | 64.8% | 70.9% | 62.7% | 94.7% | 75.8% |
| MobileNetv2 | 61.0% | 67.2% | 58.4% | 94.1% | 75.6% |
| Resnet101 | 64.3% | 67.6% | 63.8% | 95.0% | 76.7% |
| Resnet50 | 63.4% | 68.5% | 62.4% | 94.7% | 74.4% |
| Resnet18 | 59.3% | 64.7% | 57.8% | 94.6% | 75.3% |
| Xception | 60.9% | 66.5% | 59.2% | 94.7% | 75.4% |
| Inception-ResNet-v2 | 61.4% | 65.3% | 60.8% | 94.4% | 75.5% |
| ShuffleNet | 60.6% | 64.9% | 58.7% | 93.5% | 74.6% |
| DarkNet-53 | 61.9% | 66.8% | 61.9% | 94.5% | 71.6% |
| EfficientNetb0 | 57.6% | 70.3% | 53.7% | 94.1% | 73.8% |
| Model | F1 Score | Precision | Recall | Specificity | Accuracy |
|---|---|---|---|---|---|
| SqueezeNet | 52.6% | 64.0% | 50.8% | 93.4% | 68.0% |
| GoogLeNet | 56.2% | 70.0% | 53.8% | 93.4% | 68.5% |
| Inceptionv3 | 61.1% | 64.2% | 62.6% | 94.0% | 68.8% |
| DenseNet201 | 66.1% | 74.7% | 63.3% | 94.3% | 73.5% |
| MobileNetv2 | 61.5% | 65.9% | 60.2% | 93.9% | 73.0% |
| Resnet101 | 62.3% | 69.0% | 62.2% | 94.2% | 70.2% |
| Resnet50 | 63.2% | 71.7% | 61.8% | 93.9% | 67.7% |
| Resnet18 | 62.2% | 64.7% | 63.2% | 93.8% | 69.6% |
| Xception | 56.1% | 61.3% | 55.9% | 94.0% | 70.2% |
| Inception-ResNet-v2 | 58.5% | 63.9% | 59.7% | 93.8% | 67.4% |
| ShuffleNet | 61.2% | 70.2% | 57.8% | 93.3% | 70.0% |
| DarkNet-53 | 61.4% | 70.7% | 58.5% | 93.6% | 70.2% |
| EfficientNetb0 | 56.0% | 69.8% | 52.6% | 93.6% | 72.2% |
| Model | F1 Score | Precision | Recall | Specificity | Accuracy |
|---|---|---|---|---|---|
| SqueezeNet | 52.7% | 67.1% | 48.0% | 92.7% | 75.0% |
| GoogLeNet | 54.5% | 64.2% | 53.1% | 94.5% | 73.4% |
| Inceptionv3 | 67.9% | 69.9% | 70.1% | 95.3% | 79.3% |
| DenseNet201 | 74.4% | 78.5% | 73.6% | 96.0% | 82.9% |
| MobileNetv2 | 63.5% | 68.8% | 63.4% | 94.8% | 74.9% |
| Resnet101 | 71.7% | 71.1% | 74.5% | 96.3% | 81.2% |
| Resnet50 | 67.8% | 72.6% | 68.3% | 95.5% | 77.8% |
| Resnet18 | 67.9% | 72.3% | 68.3% | 95.1% | 79.0% |
| Xception | 59.5% | 65.0% | 58.5% | 94.4% | 72.1% |
| Inception-ResNet-v2 | 64.4% | 66.6% | 66.8% | 94.8% | 73.9% |
| ShuffleNet | 65.8% | 74.0% | 61.8% | 94.3% | 79.0% |
| DarkNet-53 | 66.3% | 70.0% | 66.1% | 95.1% | 80.8% |
| EfficientNetb0 | 61.3% | 73.4% | 57.0% | 94.7% | 76.7% |
| Data Split | 70/30 | 80/20 | 90/10 |
|---|---|---|---|
| Model | |||
| SqueezeNet | 377.0 | 400.4 | 422.6 |
| GoogLeNet | 726.8 | 795 | 855.0 |
| Inceptionv3 | 2182.9 | 2419.9 | 2655.2 |
| DenseNet201 | 7190.8 | 7884.7 | 8686.6 |
| MobileNetv2 | 3266.3 | 3678.5 | 4028.5 |
| Resnet101 | 2196.5 | 2449.5 | 2682.7 |
| Resnet50 | 992.2 | 1100.0 | 1192.9 |
| Resnet18 | 413.6 | 439.9 | 470.0 |
| Xception | 9076.2 | 10,111.1 | 11,094.8 |
| Inception-ResNet-v2 | 6698.0 | 7495.4 | 8254.3 |
| ShuffleNet | 2386.9 | 2641.0 | 2916.0 |
| DarkNet-53 | 1761 | 1974.6 | 2126.3 |
| EfficientNet-b0 | 5432.4 | 6028.4 | 6737.5 |
| Study | Objective | Dataset | Approach | Performance |
|---|---|---|---|---|
| Li et al. (2020) [23] | Two-class classification: melanoma and seborrheic keratosis | 600 images | Mid-level features and segmentation according to ROI | Area under the receiver-operating characteristic curve, ResNet (89.00%), DenseNet (88.85%), Fusion(90.67%) |
| Pezhman Pour and Seker [24] | Lesion segmentation | 3879 images | Dermoscopic feature segmentation using CNN | 2% and 7% improvement in Jaccard index and sensitivity, respectively |
| Al-masni et al. [25] | Three-class classification: melanoma, benign, and seborrheic keratosis | 2950 images | Segmentation using FrCN | Segmentation accuracy of 95.62% (clinical benign cases), 90.78% (melanoma, and 91.29% (seborrheic keratosis) |
| Dash et al. [26] | Three-class classification: moderate, severe, and very severe | 6267 images | Segmentation using modified U-Net architecture | 93.03% Dice coefficient, 94.8% accuracy, 89.6% sensitivity, and 97.60% specificity |
| Xie et al. [27] | Segmentation into two semantic classes: lesion and background | 1479 images | Segmentation of dermoscopy images preserving edge details | Jaccard indices of 0.783, 0.858, and 0.857 |
| Serte et al. [28] | Two-class classification: melanoma and seborrheic keratosis | 2000 images | Gabor wavelet-based deep learning model for melanoma and seborrheic keratosis | Average area under the receiver-operating characteristic curve, 91% |
| Li et al. [1] | Optimal hair removal (reduce over/under removal) | 1751 dermoscopic images with hair occlusion | Digital hair removal from images of skin lesion using CNN | Accuracy (99.08%), Specificity (99.85%), F1 score (94.43%), precision (99.09%), sensitivity (95.74%) |
| This work | Seven-class classification | 10015 dermoscopic images | Deep transfer learning of a CNN | Accuracy (82.9%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fraiwan, M.; Faouri, E. On the Automatic Detection and Classification of Skin Cancer Using Deep Transfer Learning. Sensors 2022, 22, 4963. https://doi.org/10.3390/s22134963
Fraiwan M, Faouri E. On the Automatic Detection and Classification of Skin Cancer Using Deep Transfer Learning. Sensors. 2022; 22(13):4963. https://doi.org/10.3390/s22134963
Chicago/Turabian StyleFraiwan, Mohammad, and Esraa Faouri. 2022. "On the Automatic Detection and Classification of Skin Cancer Using Deep Transfer Learning" Sensors 22, no. 13: 4963. https://doi.org/10.3390/s22134963
APA StyleFraiwan, M., & Faouri, E. (2022). On the Automatic Detection and Classification of Skin Cancer Using Deep Transfer Learning. Sensors, 22(13), 4963. https://doi.org/10.3390/s22134963