1. Introduction
Artificial intelligence (AI) has proven to be a significant success in every field of life [
1]. Artificial intelligence is the mimic of human intelligence used by computer programs. It has a subset named the machine learning (ML) technique that helps to train algorithms in making decisions [
2]. Currently, deep learning technology has become a promising approach for clinical detection systems [
3]. A deep learning computer-aided diagnosis system has been used to analyze medical images, which has proven to be a remarkable advancement in various medical applications [
4]. Deep learning algorithms have the potential to solve real-world complex problems, especially in image analysis and computer vision [
5]. Convolutional neural network (CNN) is a deep learning technique used in image and text recognition [
6]. CNN has proven to have remarkable performance in understanding image segmentation, image classification problems, and detection [
7]. Medical imaging is a core standard for the early diagnosis, detection, and treatment of several diseases. Medical images are kept in Digital Imaging and Communications in Medicine (DICOM) format, which can be quickly accessed for quantitative and qualitative analysis [
8].
Medical imaging modalities comprise multidisciplinary techniques to attain an accurate diagnosis of various diseases. There are various medical image modalities such as computed tomography, X-ray angiography, mammography, digital radiography, radio fluoroscopy, and computed radiography that are used to analyze image processing [
9]. Computed tomography (CT) images are an easier and more accurate method for the correct detection of various diseases [
10]. However, it is tedious for medical experts to manually analyze CT scans without any error [
11]. In the last few years, a low-dose CT scan has been used to screen for lung cancer diseases that has led to a decrease in the mortality rate of lung cancer [
12].
The authors of [
13] presented a framework based on deep learning to detect lung cancer and pneumonia abnormalities. The deep learning technique, named Modified AlexNet (MAN), was presented to detect two classes, normal and pneumonia class, by using X-ray images. The MAN technique was applied to classify lung cancer by using a support vector machine (SVM) model. The MAN method performance was evaluated with other deep learning approaches such as ResNet50, VGG19, VGG16, and AlexNet and achieved 97.27% accuracy by using the LIDC-IDRI dataset. Another study [
14] presented a network based on a deep convolutional neural network, named AlexNet. The network consisted of an eight-layer two-architecture deep CNN to classify malignant and benign nodules. The network extracted the features automatically from CT scan images. Binary cross-entropy was applied to improve precision in the training phase as well as validation accuracy. The lung nodule classification model achieved 99% training precision and 97% validation accuracy. Similarly, the authors of [
15] introduced a lung cancer detection method based on a deep learning algorithm using the segmentation method. Five-fold cross-validation was applied to train and validate the deep learning-based model. In another study, the authors of [
16] presented a CAD system for pulmonary pure ground-glass nodules based on the convolutional neural network. In line with the above, various research works have been presented where diverse optimization algorithms have been applied to achieve an improvement in performance for the detection of lung cancer diseases. In this research work, we have investigated and explored an optimization algorithm based on a convolutional neural network to detect lung cancer. Furthermore, this work exploited the optimizers RMSprop, Adam, and SGD as well as their implementation with CNN architectures.
The remaining part of the paper has been organized as follows:
Section 2 discusses prior works published in recent years.
Section 3 introduces the materials and methods based on CNN, and
Section 4 demonstrates the experimental results.
Section 5 discusses the present, and finally, limitations and future works are discussed in
Section 6.
2. Related Work
Convolutional neural networks have been implemented to solve various visual problems since the late 1980s. LeCun et al. used a first-time backpropagation algorithm in multilayered CNN, namely ConvNet, to recognize handwritten zip codes in 1989 [
14]. Khehrah et al. presented a pulmonary nodule detection system using shape-based and statistical features in CT images [
17]. Another study [
18] introduced lung nodule detection based on an artificial neural network using texture and shape features. The model achieved an accuracy of 89.62%. Similarly, the authors of [
19] proposed a lung cancer detection model based on ANN that achieved 96.67% accuracy. Miah et al. [
20] presented a lung cancer detection system using a neural network from CT images that obtained 96.67% accuracy. LeCun et al. [
21] suggested another advanced version of ConvNet called LeNet-5 to classify characters in a document in 1998.
In [
22], the researchers applied the LeNet-5 model to classify benign and malignant pulmonary nodules in thoracic CT images. Lung Image Database Consortium and Image Database Resource Initiative (LIDC-IDRI) datasets were obtained for the experimental results. The 10-folder cross-validation was implemented to evaluate the model classification. The LeNet-5 achieved 97.041% accuracy in classifying benign and malignant nodules and 96.685% accuracy in classifying mild malignancies and serious malignancies. Another study [
23] presented a hybrid version of a convolutional neural network for the classification of pulmonary nodules based on LeNet and AlexNet. The hybrid framework used LeNet’s layers and parameters of AlexNet. A total number of 1018 CT images was obtained from the LIDC-IDRI dataset to train and evaluate the agile convolutional neural network. Various parameters such as kernel size, batch size, learning rate, and weight initialization played an important role in achieving high accuracy. The framework achieved 0.822 accuracy and 0.877 area under the curve, with the kernel size set to 7 × 7, the batch size at 32, and the learning rate at 0.005. Gaussian and dropout were also applied in this work.
Krizhevsky et al. [
24], introduced the first deep convolutional neural network named AlexNet in 2012. AlexNet outperformed in the ImageNet Large Scale Visual Recognition Challenge (ILSVRC)-2012 and proved to be a pervasive breakthrough in the performance of CNN.
Agarwal et al. [
25] investigated a framework to detect and classify lung cancer based on AlexNet CNN. In the first step, the green channel extracted was from the original color CT image. Multilevel thresholding was used to extract lung regions. The morphological and thresholding segmentation methods were applied to separate non-affected and affected regions. After segmentation of the tumor regions, AlexNet-CNN was classified into benign and malignant with 96% accuracy.
In [
26], the researchers recommended two architectures named straight 3D-CNN and hybrid 3D-CNN for the classification of pulmonary nodules. The features extraction method was the same in both models, but the classifiers differed. The model 3D-CNN used a softmax classifier to classify the pulmonary CT images, and the hybrid 3D-CNN used the radial basis function (RBF)-based support vector machine (SVM) classifier for classification purposes. The experimental results indicated that the hybrid 3D-CNN and straight 3D-CNN models achieved better accuracy. Nevertheless, the approach obtained an accuracy of 91.8%, specificity of 94.23%, sensitivity of 88.53%, and precision of 91.9% as compared to the 3D-CNN model with a softmax classifier.
Rao et al. [
27] exploited the classification of lung tumors by using convolutional neural networks. The suggested CanNet approach consisted of two convolution layers, a pooling layer, a dropout layer, and a final fully connected layer. Lung Image Database Consortium (LIDC) was used to train and evaluate an artificial neural network, LeNet, and CanNet networks. The dataset comprised 1018 patients’ CT scan data, and each CT scan consisted of almost 150 to 550 DICOM images. Artificial neural networks, LeNet, and CanNet achieved accuracies of 72.50%, 56.0%, and 76.00%, respectively. The CanNet model outperformed compared to the ANN and LeNet networks.
Lin et al. [
28] presented a lung nodule classification model comprising a Taguchi-based convolutional neural network. Useful information obtained with fewer experiments is the most significant advantage of the Taguchi technique. A total number of 245,931 images including CT scans and X-ray images were obtained to evaluate the performance of the AlexNet model. The experimental results demonstrated that AlexNet with the Taguchi-based model used less training time as compared to other approaches.
The authors of [
29] introduced a computer-aided scheme based on a convolutional neural network with AlexNet architecture to diagnose and classify lung cancer. The lung cancer CT scan dataset was collected from Iraqi Hospitals that were used to train and test the system. For training purposes, 70% was used to train and 30% was used for testing. The dataset was classified into three categories: normal, benign, and malignant, and consisted of 110 CT scans. The system achieved 93.548% accuracy, 97.102% precision, 95% specificity, 95.714% sensitivity, and 96.403% F1 score. The authors of [
30] investigated the effects of Visual Geometry Group 16 (VGG16) and Visual Geometry Group 19 (VGG19) on ImageNet Challenge 2014. VGG16 and VGG19 consisted of 16 and 19 weight layers, respectively. The input size comprised 224 × 224 RGB images, and a convolutional filter size of 3 × 3 was used in both networks, providing significant improvements in the image recognition process. The experimental results exploited that the depth representation is beneficial to classifying problems and increased state-of-the-art accuracy. Both networks were also tested on other datasets and achieved high accuracy as compared to other techniques.
Another study [
31] introduced a technique to detect early lung cancer by using a deep learning genetic algorithm. In the preprocessing method, three techniques were applied: the histogram stretching technique was used to enhance the contrast of the raw image; the Wiener filter was used to remove noise; the image was cropped into 224 × 224 for VGG16 and 227 × 227 for VGG19 for the AlexNet architecture. Low-dose computed tomography (LDCT) images were used, and three CNN architectures, VGG16, VGG19, and AlexNet, were applied to extract features. A genetic algorithm was applied to select the most relevant features. Finally, K-nearest neighbor (KNN), decision tree, and SVM classifiers were investigated to classify pulmonary lung nodules. The experimental results indicated that VGG19 with a support vector machine classifier obtained a remarkable 96.3% accuracy, sensitivity of 97.5%, and specificity of 95% as compared to other CNN models and classifiers.
The authors of [
32] presented an accurate lung segmentation technique based on VGG-16 and dilated convolution network. Dilated convolution used a dilation rate parameter and indicated an expansion of the size of the respective field. The hypercolumn features technique was used to fuse multi-scale convolution features to enhance the robustness of the lung segmentation technique. The modified VGG16 was used, followed by the multilayer perceptron (MLP) and ReLU activation function. The method achieved a dice similarity coefficient of 0.9867.
Another study based on VGG16 [
33] introduced VGG16 with a boosting technique for the identification of the pathological types of lung cancer. The dataset consisted of 125 patients with early-stage lung cancer and was enhanced by using reproducing, shifting, and revolving operations. VGG16-T comprised five convolution layers with a kernel size of 3 × 3. It was found that the boosting strategy enhanced the accuracy, and three weak classifiers can be adequate enough to make a strong classifier. Finally, the softmax function was applied to identify the pathological type of lung cancer by using CT images. The experimental results of VGG16-T with boosting achieved 85% accuracy, which was better than the other techniques, ResNet-34, DenseNet, and AlexNet.
Similarly, the authors of [
34] presented a lung cancer detection system by using a transfer learning technique. The suggested method reduced the processing time by using a maximum dropout ratio, and it decreased overfitting in the learning phase. GoogleNet, AlexNet, and ResNet50 transfer learning convolutional neural network architectures were applied to detect lung cancer. LIDC, a publicly available dataset, was used to train and test the pre-trained model as well as the suggested model and achieved high accuracy as compared to pre-trained methods.
Another study [
35] based on ResNet architecture presented a method for pulmonary nodule classification. The proposed model was based on 18 layers of ResNet and achieved 89.90% accuracy using LIDC-IDRI. In [
36], an inception module CNN classifier achieved 88.67% validation accuracy for the detection of pulmonary nodules on the AIA-INF publicly available dataset. Similarly, in [
37], the Darknet-53 CNN-based architecture was applied for pulmonary nodule detection and achieved 70.5% to 73.9% accuracy on the LUNA16 dataset. Many other studies covered other cancer types such as thyroid, breast, skin, colon, and blood cancers. In [
38], the Xception neural network was applied to thyroid cancer for the early detection of malignant nodules. The framework adopted three-level multi-channel and real-world datasets, which were used to evaluate the proposed approach. Another cancer type, colon carcinoma [
39], was adopted to be used in a convolutional neural network for classification task. A study [
40] conducted on the early detection of breast cancer was based on fused and deep learning approaches; similarly, another study [
41], empowered with a deep learning technique, exploited breast cancer and its stages, such as mucinous carcinoma, papillary carcinoma, ductal carcinoma, and lobular carcinoma. A comprehensive study [
42] was investigated for the automatic detection of skin lesions based on various CNN architectures. Similarly, another framework [
43] based on an optimal CNN exploited the automatic detection of skin cancer. The proposed framework comprised an advanced version of the whale optimization algorithm, and the results were analyzed with 10 different techniques.
A summary of previous related work is mentioned in
Table 1. The limitations of previous studies are mentioned, such as deep knowledge [
17,
18,
19,
20], which is required to obtain handcrafted features. The studies [
25,
29,
31] were based on lesser amounts of images and on imbalanced datasets. The research works [
22,
23,
26] focused on hybrid techniques that created complexity of the model, while different architectures were used in some research works [
35,
36,
37] to improve accuracy.
The following are this work’s key contributions:
- (a)
The main contribution of this study is to provide a performance-oriented analysis by combining deep learning algorithms with different optimizers for the classification of lung cancer.
- (b)
We have implemented CNN architectures with Adam, SGD, and RMSprop optimizers on the LUNA16 publicly available dataset.
- (c)
It was observed that the AlexNet architecture with the SGD optimizer achieved the best results on the LUNA16 dataset.
- (d)
Finally, AlexNet with the SGD optimizer approach achieved the highest accuracy as compared with other existing techniques for lung cancer classification.
3. Materials and Methods
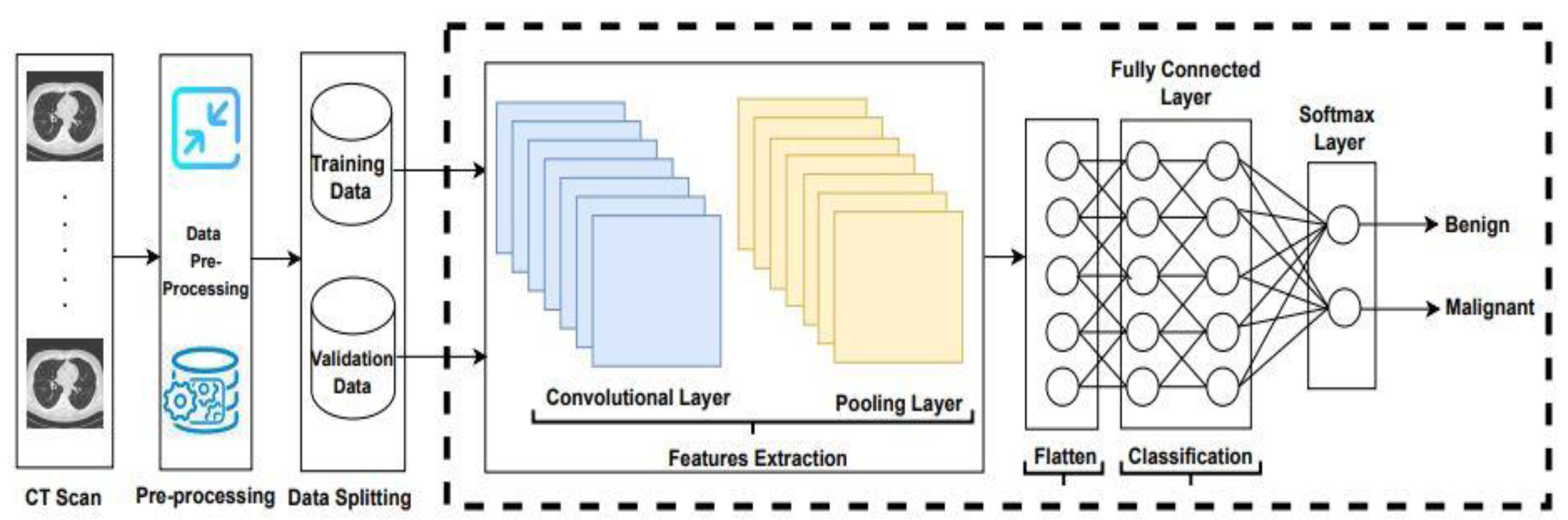
Lung cancer has become the main reason for cancer deaths all over the world, as its symptoms appear late. Consequently, a significant detection system is required to detect lung cancer in patients at its early stages. In this study, the existing algorithms LeNet, AlexNet, VGG16, ResNet-50, and Inception-V1, with the Adam, SGD, and RMSprop optimizers were applied to classify lung cancer, and an example is shown in
Figure 1.
The overall procedure adopted to apply convolutional neural network architectures is demonstrated in
Figure 1. In the first step, the LUng Nodule Analysis 2016 (LUNA-16) dataset obtains from the publicly available lung cancer nodules [
44]. The LIDC-IDRI database is publicly available from The Cancer Imaging Archive (TCIA). This database contains a total number of 1018 CT scans. CT scan images are associated with XML files annotated by four experienced radiologists. Thin-slice CT scans play a significant role in the detection of pulmonary nodules; therefore, the authors of [
45] discarded slices that were greater than 3 mm thick, missing slices, and those with inconsistent slice spacing. A total number of 888 scans provided as MetaImage (.mhd) images are accessible from the LUNA-16 website. Two methods are applied on LUNA16 for training and validation purposes. In the first method, a dataset is randomly split into 80% and 20%, and the second method is based on 5-fold cross-validation. After splitting and 5-fold cross-validation, the dataset is forwarded to the CNN architectures to extract the features.
CNNs have various parameters and hyperparameters such as neurons, number of layers, weights, biases, stride, filter size, activation function, learning rate, etc. Convolution operation plays a significant role in image feature extraction [
46]. Two types of filters, large size filters and small size filters, are used to extract various information. Large-sized filters are used to extract coarse-grained information, and small-sized filters are used to extract fine-grained information.
LeNet was developed by LeCun in 1998 for zip code recognition. In LeNet, a convolve filter size of 5 × 5 with a stride of 1 was used, and in the subsampling (pooling) layer, a filter size of 2 × 2 was applied with a stride of 2. AlexNet was the first CNN-based method that won the ImageNet Scale Visual Recognition Challenge in 2012. AlexNet comprises 5 convolutions, 3 pooling, and 3 fully connected (FC) layers. The input image size was 227 × 227 × 3, and the rectified linear unit (ReLU) was applied for the first time in AlexNet. The visual geometric group (VGG) has two versions: VGG16 with 16 layers and VGG19 with 19 layers. In VGG16 and VGG19, the number of layers increases, but the size of the filters decreases. In this study, we applied LeNet, AlexNet, VGG16, ResNet-50, and Inception-V1 to classify lung cancer on the LUNA16 dataset.
Optimizers are methods or algorithms applied to minimize a loss function and to maximize the efficiency of the model. Optimizers are mathematical functions that are based on the model’s learnable parameters, and they assist to reduce the losses with updated learning rates and weights of the neural network. The learning rate (LR) is known as a tuning parameter that works in an optimization algorithm. LR determines the step size in an optimization algorithm at each iteration when moving toward finding a minimum of the loss function.
Root mean square propagation [
47] is also an adaptive learning method to resolve destructive learning rates. RMSprop determines the learning rate after each iteration by using an exponentially weighted average [
41].
where
η: initial learning rate;
: exponential average of gradients along wj;
: gradient at time t along wj;
: exponential average of squares of gradients along wj;
ϒ: hyperparameter.
The adaptive moment estimation (Adam) method computes adaptive learning rates for every parameter at each iteration. It is easy to implement with less memory requirements, and it is computationally efficient. Adam uses a combination of RMSprop and gradient descent with momentum to determine the parameter values [
41].
where
Ƞ: initial learning rate;
: exponential average of gradients along wj;
: gradient at time t along wj;
: exponential average of squares of gradients along wj;
and : hyperparameters.
A stochastic gradient descent (SGD) focuses on performing updates to the model parameters one at a time; therefore, it is much faster. After each iteration, the cost function minimizes, and SGD performs frequent updates of the model parameter that causes the cost function to fluctuate heavily, which leads the gradient to jump to the global minimum. It requires less memory and permits the use of enormous datasets [
41].
where
η: initial learning rate;
x: parameters;
n: training dataset;
loss function;
stochastic gradient.
In this study, CNN architectures with LeNet, AlexNet, VGG16, ResNet-50, Inception-V1 with the Adam, RMSprop, and SGD optimizers were applied to extract features from the LUNA16 dataset. Subsequently, the flattened layer converts the matrix to vector form and is fed to the fully connected layer for classification purposes. Finally, the classifier softmax classifies lung cancer into benign and malignant.
4. Results and Discussion
In this study, the comparison between state-of-the-art CNN architectures LeNet, AlexNet, VGG16, ResNet-50, and Inception-V1 for the detection of lung cancer is explained in detail by using the different optimizers, Adam, RMSprop, and SGD. The performances of the LeNet, AlexNet, VGG16, ResNet-50, and Inception-V1 architectures were validated and evaluated in terms of accuracy. These deep learning networks use binary cross-entropy loss. In this section, the results presented were achieved by LeNet, AlexNet, VGG16, ResNet-50, and Inception-V1 detection algorithms.
In this study, the performance analysis was implemented in the Keras tool using Python 3.8. The Adam, SGD, and RMSprop optimizers were employed with a learning rate of 0.001, batch size of 20, and 200 epoch values. To measure the performance of LeNet, AlexNet, VGG16, ResNet-50, and Inception-V1, various optimizers such as RMSprop, Adam, and SGD were applied, and various statistical parameters were measured to detect lung cancer.
Various statistical parameters such as accuracy [
48], sensitivity [
49], specificity [
50], positive predictive value [
51], negative predictive value [
52], false omission rate [
53], and F1 score were applied to evaluate the performance of the convolutional neural network architectures with the optimizers.
The validation confusion matrix of the LeNet architecture is shown in
Table 2, and the validation performance factors of the LeNet model with different optimizers are shown in
Table 3. LeNet with the SGD optimizer achieved a 95.92% accuracy, which is higher than the RMSprop and Adam optimizers. The other statistical parameters of LeNet with the SGD optimizer such as accuracy, sensitivity, specificity, PPV, NPV, FOR, and F1-score were 95.92%, 94.76%, 97.25%, 97.51%, 94.22%, 5.78%, and 96.11%, respectively.
The validation confusion matrix of AlexNet is shown in
Table 4, and the validation performance of the AlexNet model with different optimizers is shown in
Table 5. AlexNet with the SGD optimizer achieved 97.42% accuracy, which was higher than the RMSprop and Adam optimizers. The other statistical parameters of AlexNet with the SGD optimizer such as sensitivity, specificity, PPV, NPV, FOR, and F1-score were 97.58%, 97.25%, 97.58%, 97.25%, 2.75%, and 97.58%, respectively.
The VGG16 validation confusion matrix is shown in
Table 6, and the validation performance of the VGG16 model with different optimizers is shown in
Table 7. VGG16 with the SGD optimizer achieved 93.56% accuracy, which was higher than the RMSprop and Adam optimizers. The other statistical parameters of VGG16 with the SGD optimizer such as sensitivity, specificity, PPV, NPV, FOR, and F1-score were 91.53%, 95.87%, 96.19%, 90.87%, 9.13%, and 93.80%, respectively.
The ResNet 50 validation confusion matrix is shown in
Table 8, and the validation performance of the ResNet 50 model with different optimizers is shown in
Table 9. ResNet 50 with the SGD optimizer achieved 96.35% accuracy, which was higher than the RMSprop and Adam optimizers. The other statistical parameters of ResNet 50 with the SGD optimizer such as sensitivity, specificity, PPV, NPV, FOR, and F1-score were 91.53%, 95.87%, 96.19%, 90.87%, 9.13%, and 93.80%, respectively.
The Inception-V1 validation confusion matrix is shown in
Table 10, and the validation performance of the Inception-V1 model with different optimizers is shown in
Table 11. Inception-V1 with the SGD optimizer achieved 93.56% accuracy, which was higher than the RMSprop and Adam optimizers. The other statistical parameters of Inception-V1 with the SGD optimizer such as sensitivity, specificity, PPV, NPV, FOR, and F1-score were 91.53%, 95.87%, 96.19%, 90.87%, 9.13%, and 93.80%, respectively.
Table 12 demonstrates the results obtained from AlexNet with the SGD optimizer on the Luna16 dataset. The original image was benign, and the CNN architecture AlexNet with the SGD optimizer detected the image as benign. Next, the image was benign and AlexNet with the SGD detected the image as malignant, which was wrongly predict by AlexNet. The next image was malignant, and AlexNet with the SGD optimizer detected it as benign. Finally, the actual image was malignant, and AlexNet with the SGD optimizer detected it as malignant.
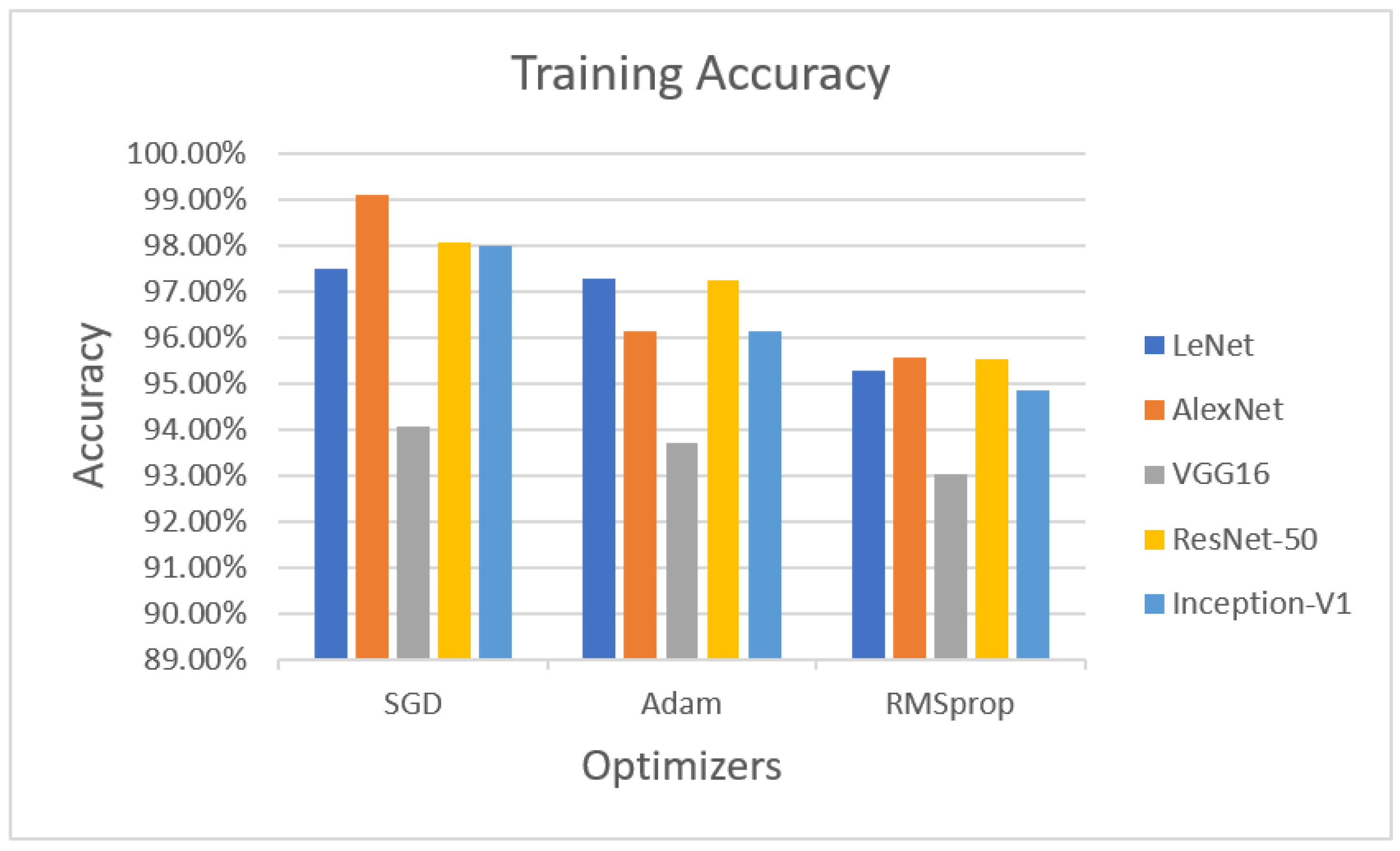
In the training phase, the accuracies of LeNet, AlexNet, VGG16 ResNet-50 and Inception-V1 with the optimizers are illustrated in
Figure 2. LeNet with the SGD optimizer achieved 97.47% accuracy, whereas AlexNet with the SGD optimizer obtained 99.09% accuracy. VGG16 with the SGD optimizer achieved 94.07% accuracy. ResNet-50 with the SGD optimizer obtained 98.05% accuracy, while Inception-V1 with the SGD optimizer achieved 97.99% accuracy.
The next optimizer, Adam, was performed on LeNet, AlexNet, VGG16, ResNet-50, and Inception-V1. LeNet with the Adam optimizer achieved 97.26% accuracy, whereas AlexNet with Adam obtained 96.13% accuracy, VGG16 with Adam achieved 93.71% accuracy, ResNet-50 with Adam achieved 97.24% accuracy, and Inception-V1 with Adam achieved 96.12% accuracy.
The last optimizer, RMSprop, also measured for training purposes. LeNet with RMSprop achieved 95.27%, AlexNet with RMSprop obtained 95.54% accuracy, VGG16 with RMSprop achieved 93.01% accuracy, ResNet-50 obtained 95.53% accuracy, and Inception-V1 achieved 94.86% accuracy using the RMSprop optimizer.
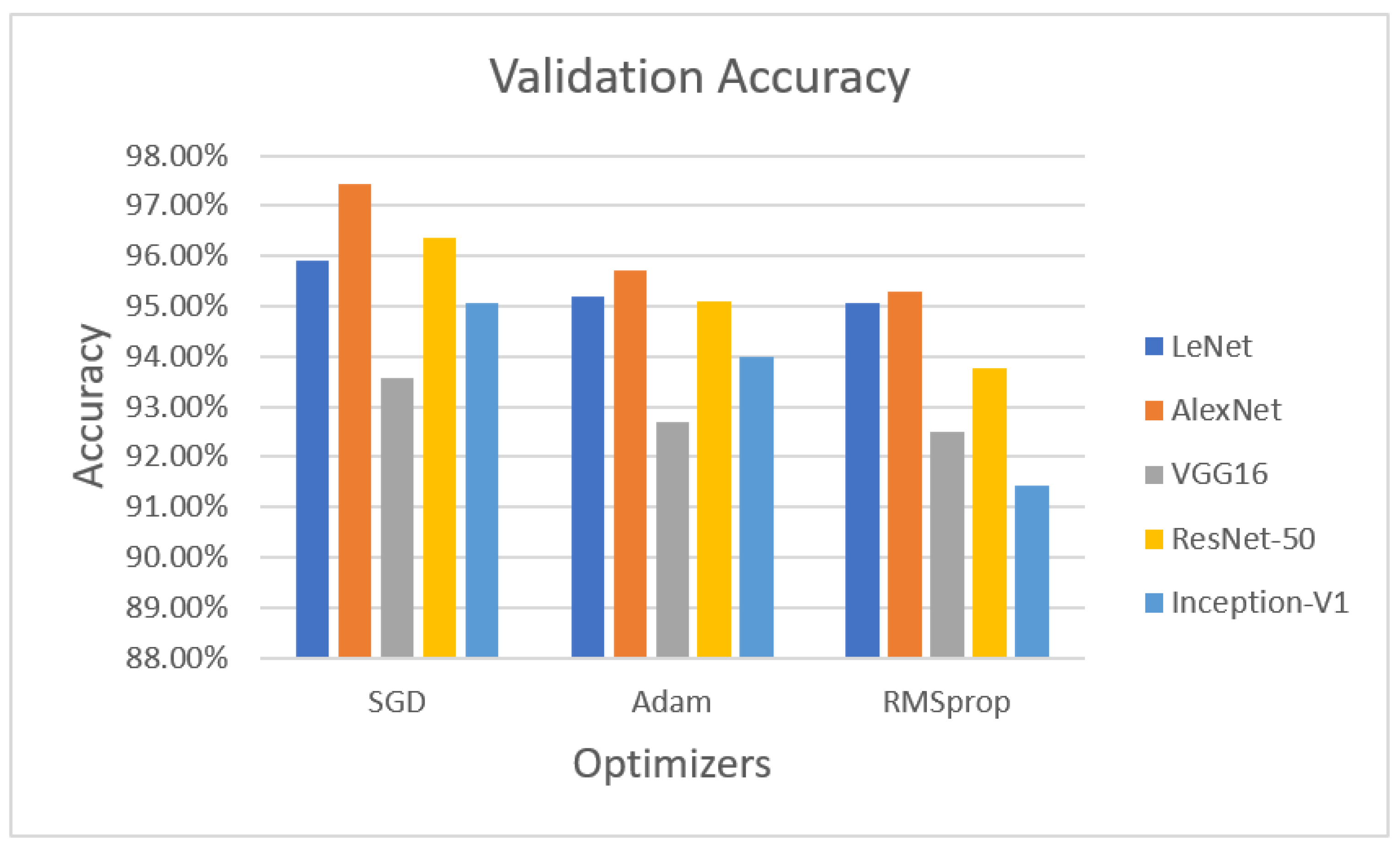
Figure 3 demonstrates the validation phase, the LeNet algorithm with the SGD optimizer achieved 95.92% validation accuracy. AlexNet with the SGD optimizer obtained 97.42% accuracy, VGG16 with the SGD optimizer obtained 93.56% validated accuracy, ResNet-50 with the SGD optimizer achieved 96.35% validation accuracy, and Inception-V1 with the SGD optimizer obtained 95.06% accuracy.
The next optimizer, Adam, was performed on LeNet, AlexNet, and VGG16. LeNet with the Adam optimizer achieved 95.18% accuracy, whereas AlexNet with Adam obtained 95.71% accuracy, VGG16 achieved 92.70% accuracy, ResNet-50 with the Adam optimizer achieved 95.09% validation accuracy, and Inception-V1 with Adam obtained 93.99% accuracy.
The last optimizer RMSprop also measured for validation purposes. LeNet with RMSprop achieved 95.06%, AlexNet with RMSprop obtained 95.28% accuracy, VGG16 with RMSprop achieved 92.49% accuracy, ResNet-50 with the RMSprop optimizer achieved 93.78% accuracy, and Inception-V1 with RMSprop achieved 91.42% validation accuracy on theLUNA16 dataset.
The second method, five-fold cross-validation, was adopted to train and validate the CNN architectures with the SGD optimizer. The validation statistical analysis is shown in
Table 13. When the five-fold cross-validation approach was applied, the AlexNet–SGD optimizer achieved 95.73%, 95.20%, 96.33%, 96.75%, 94.59%, 5.41% and 95.97% accuracy, sensitivity, specificity, PPV, NPV, FOR, and F1-score, respectively, which were the highest scores compared with the other CNN architectures.
The CNN-based architectures LeNet, AlexNet, VGG16, ResNet-50, and Inception-V1, with different optimizers, were evaluated in this study. It was found that AlexNet with the SGD optimizer achieved the highest accuracy of 97.42%.
Table 14 presents the performance analysis of AlexNet with the SGD technique with different methods. Comparatively, the accuracy of AlexNet with the SGD was higher than the other state-of-the-art approaches. Various existing publications used different methods on the different datasets, including LIDC-IDRI, LUNA16, IQ-OTH/NCCD, ELCAP, and private lung datasets for the detection of lung cancer. AlexNet with SGD and with the five-fold cross-validation method obtained 95.73% accuracy and a 4.27% misclassification rate. AlexNet with the SGD achieved the highest accuracy of 97.42% and 2.58% of misclassification rate.


 ,
, 





{kind=link}
{kind=link}
{kind=link}



