
Enhancing System Acceptance through User-Centred Design: Integrating Patient Generated Wellness Data †


Abstract
:1. Introduction
2. Materials and Methods
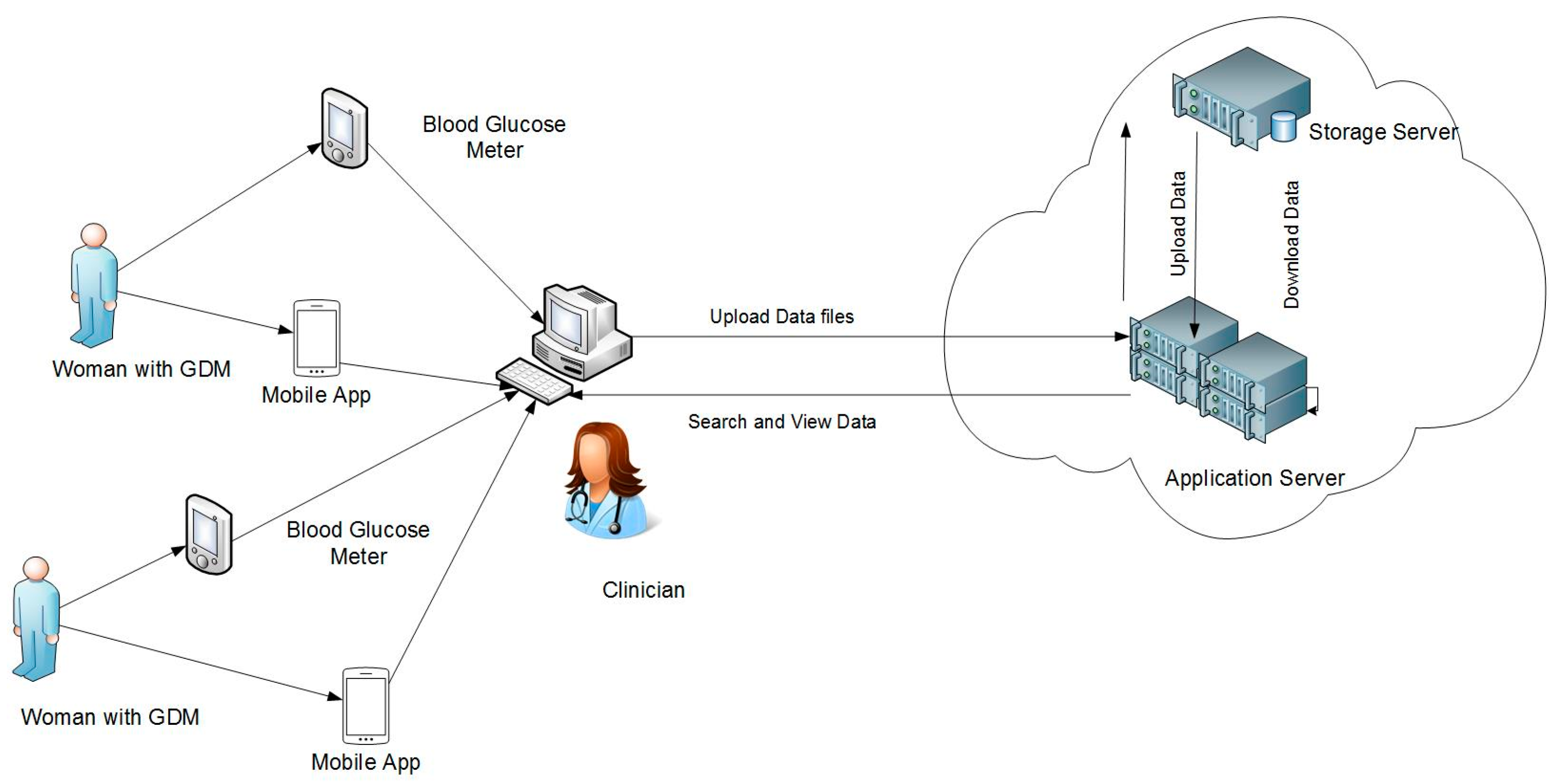
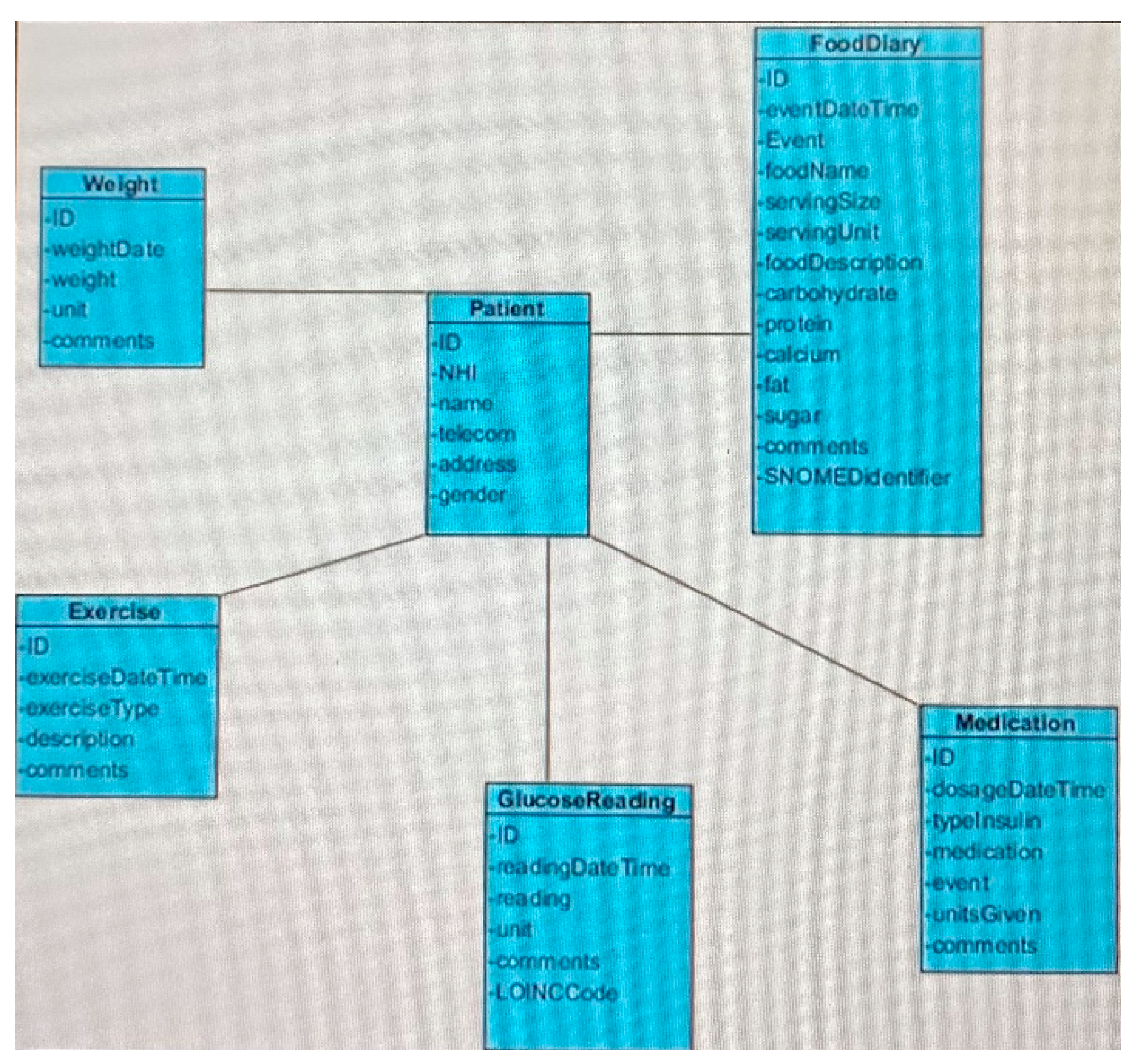
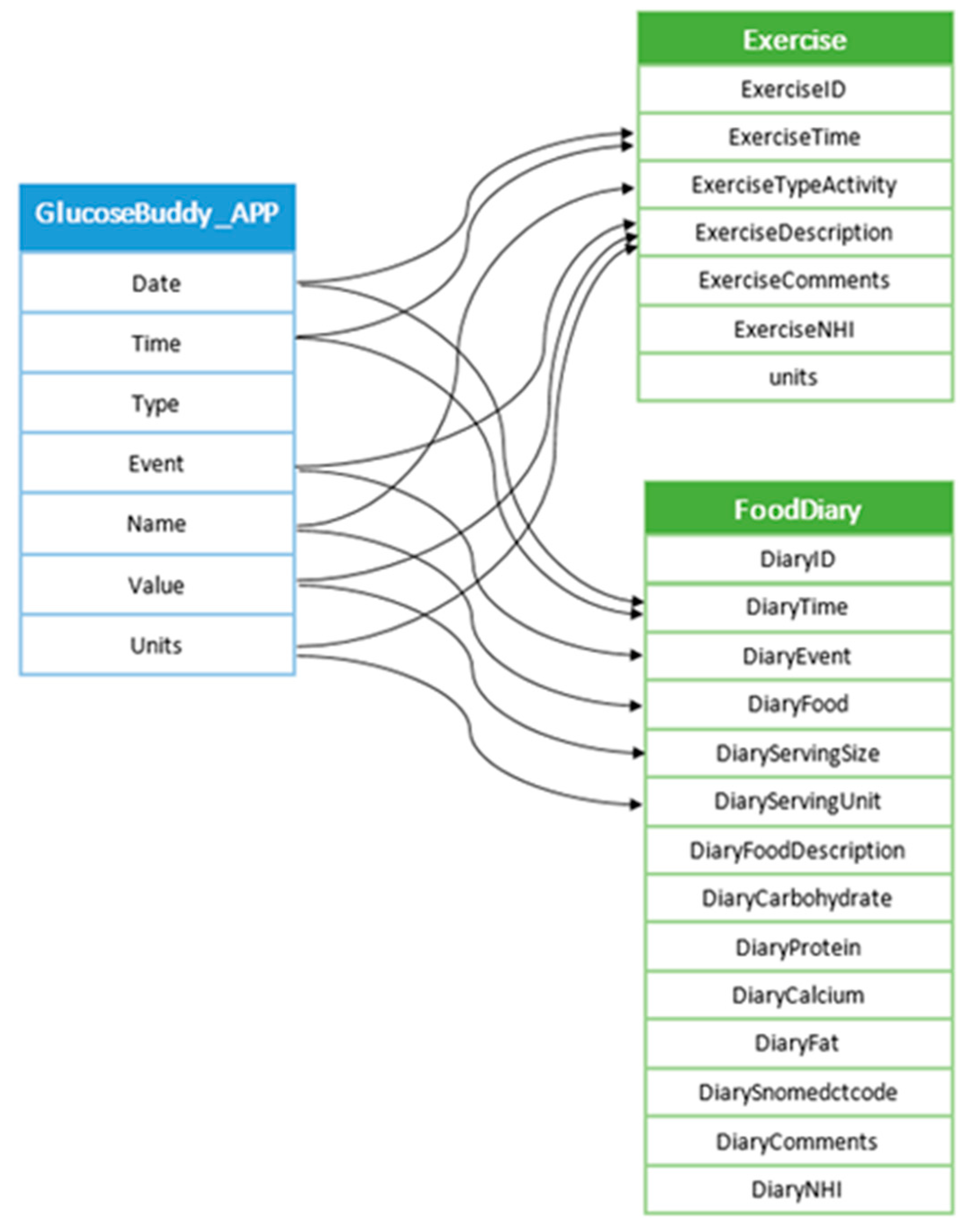
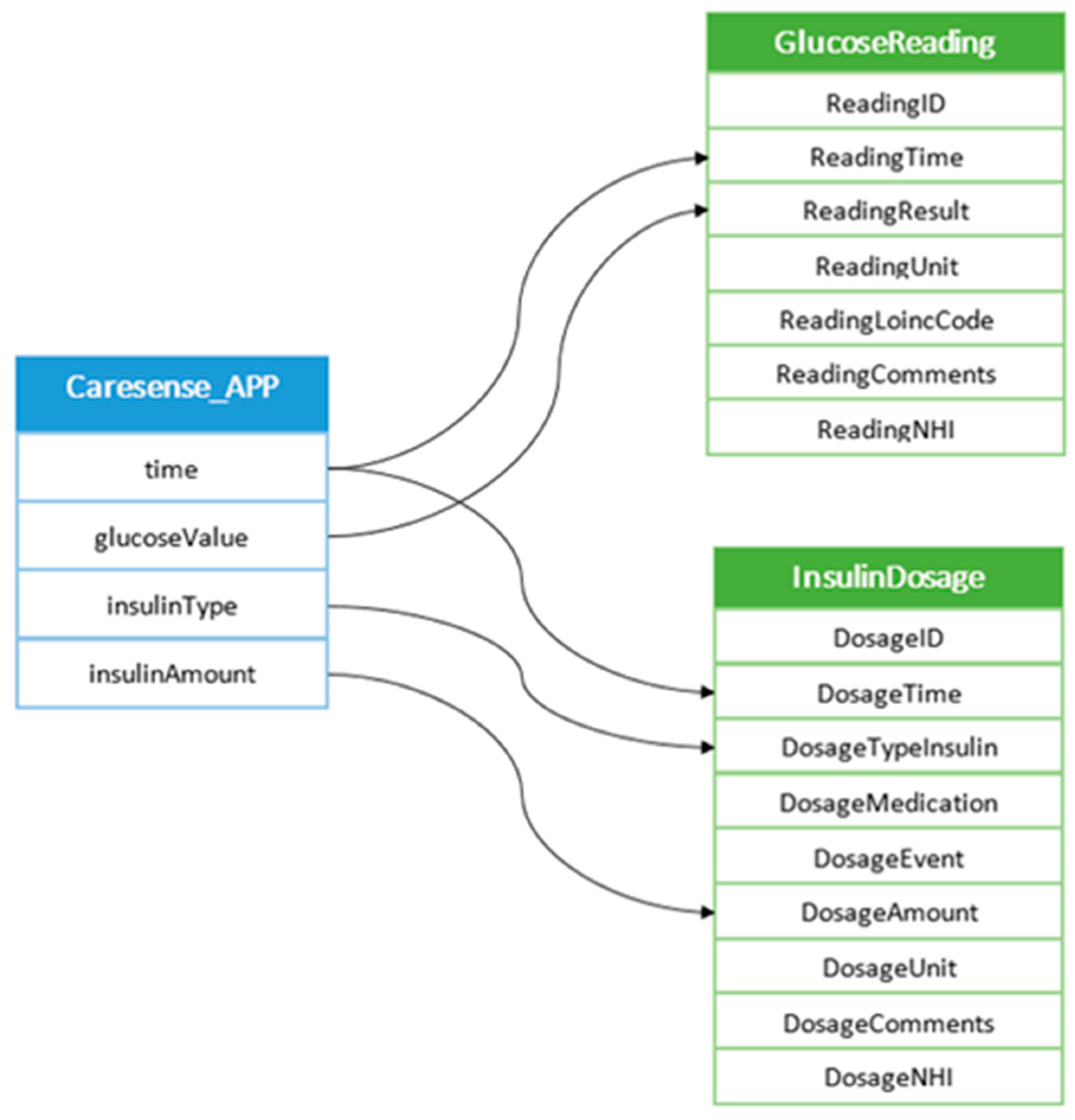
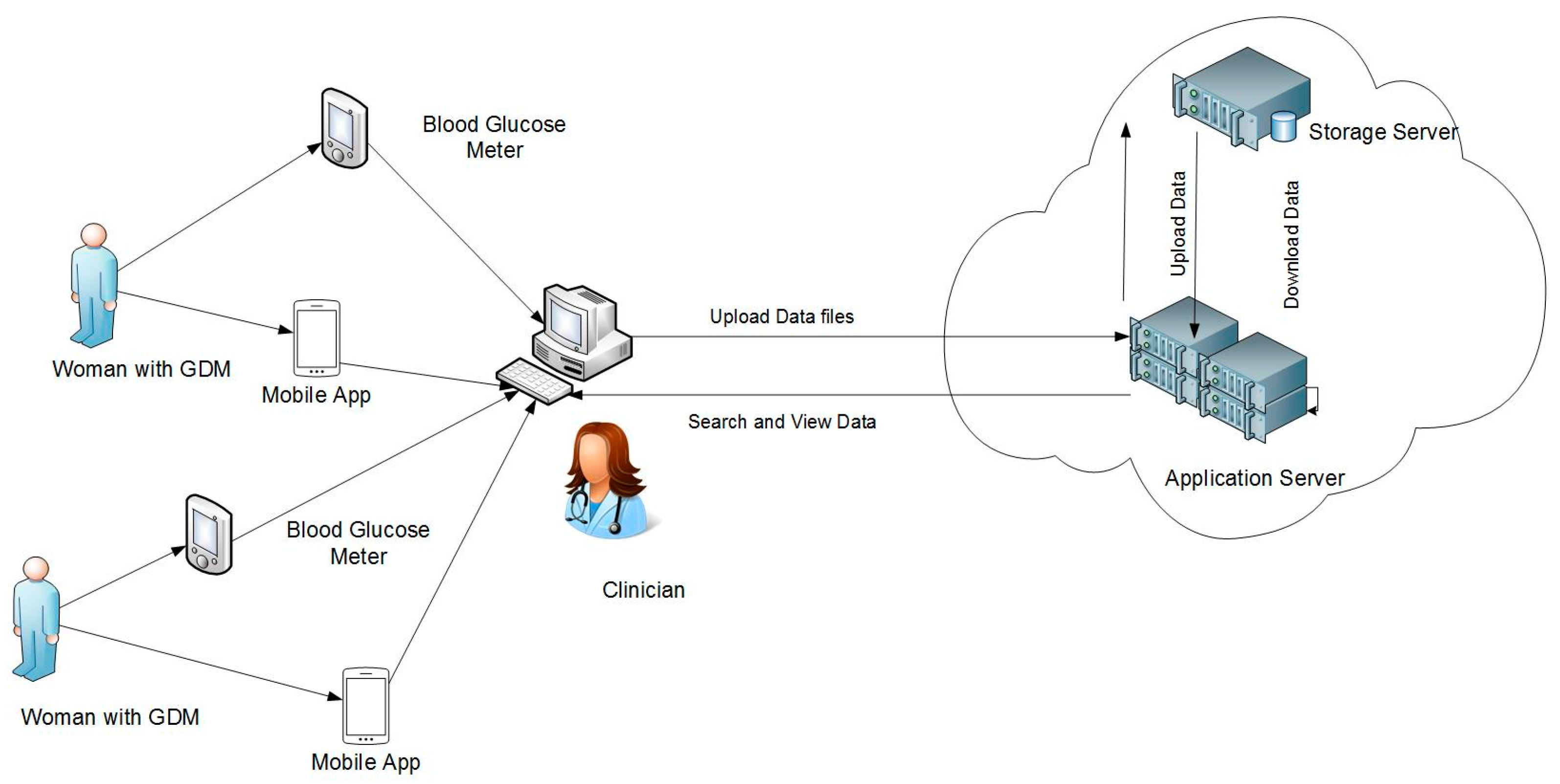
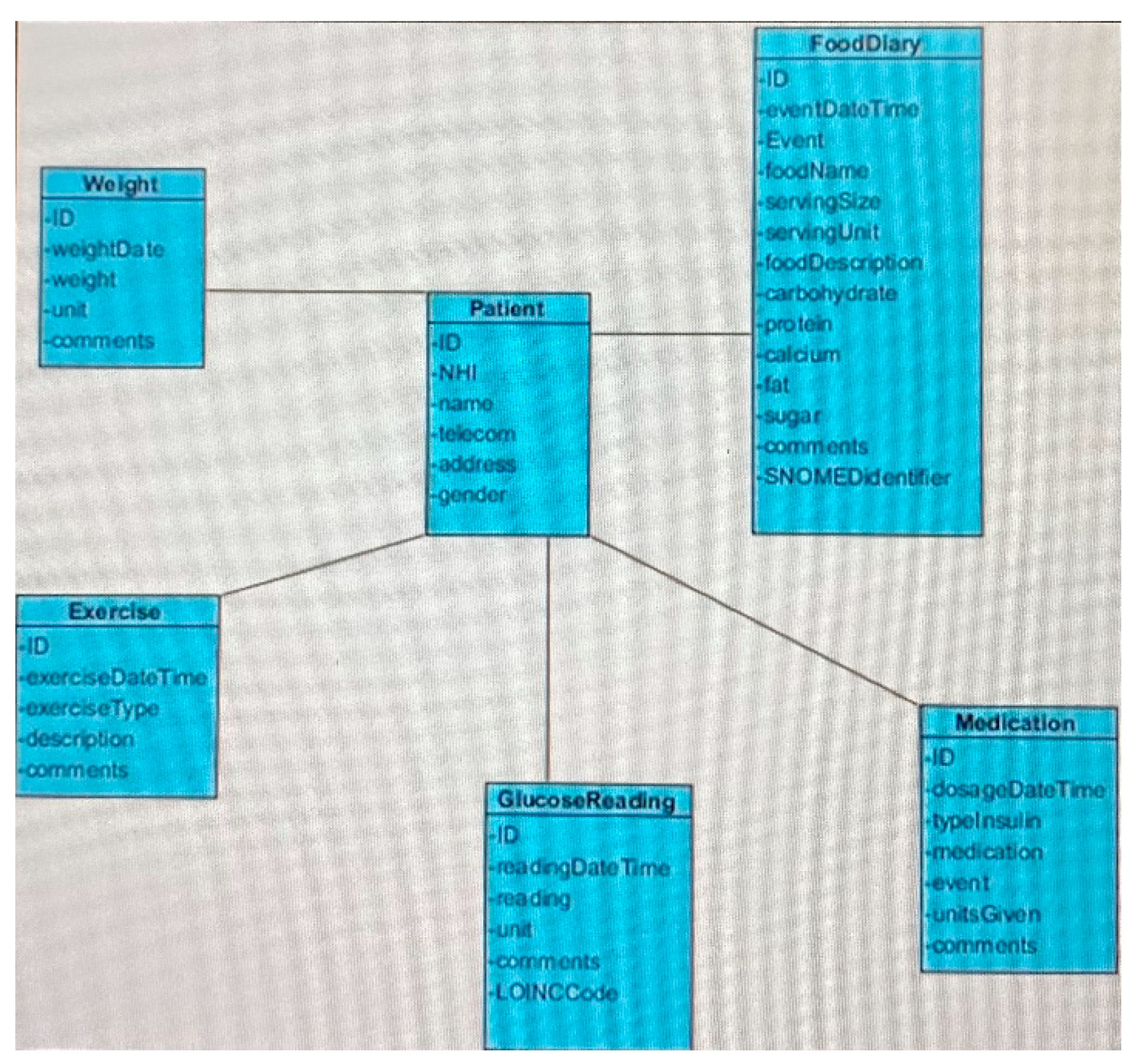
2.1. Clinical Ecosystem Architecture
2.2. Study Participants
2.3. Data Gathering and Analysis Methods
2.4. System Evaluation Process
- Open ended semi-structured interviews (INT1) with five participants were conducted to elicit the requirements of the system prototype. Paper mockups of the interface design and navigation were prepared and discussed with the participants. A requirement analysis document was created and shared with the participating clinicians by email. It included screenshots of the interface design, a review of the selected mobile apps and a conceptual description of the database design, including the wellness data to be stored.
- Videos of a prototype demonstration were created and sent to clinicians. A user manual presenting the main functionalities of the prototype illustrated with screenshots was also distributed. The second set of interviews (INT2) with clinicians was organised. The prototype was demonstrated interactively to individual participants, who could query the functionalities and the design of the prototype. Usability issues were highlighted at this stage.
- A TA session (TAP1) was conducted to check whether participants (clinicians) were comfortable undertakings basic tasks such as uploading wellness data into the system and viewing the system outputs as a series of combined daily reports containing blood glucose levels, a food and exercise diary, and insulin dosage. Further usability issues were raised.
- A third set of interviews (INT3) was organised, involving the clinicians who had participated so far, five other clinicians and women with GDM. The prototype was demonstrated to those individuals who were new to the system. The demonstration was interactive, with participants exploring the functionalities and the design of the prototype.
- A second TA session (TAP2) was conducted. Its first aim was to check whether the new group of participants (the clinicians and women with GDP who participated in INT3) were comfortable undertaking the basic tasks already introduced at the TAP1 session. Second, participating clinicians were asked to complete two new tasks which aimed at enhancing the clinical value of the data (e.g., adding a nutrition value to a food item).
3. Results
3.1. System Usefulness and User Acceptance
- All data in one report: in current practice, data about blood glucose levels, food intake (food diary), exercise and insulin dosage are generated by different sources and communicated through different channels (e.g., on paper, or in an email). The new system would be useful if it collated these data and presented them in one single report.
- Blood glucose reading labeled: blood glucose reading data were not always precise about timing (e.g., after or before a meal). The new system needed to provide these details and highlight readings above the norm.
- Food portion size: the system needed to capture data about the size of the food portion (not only about the food type) and to provide for adding the relevant LOINC code to improve accuracy.
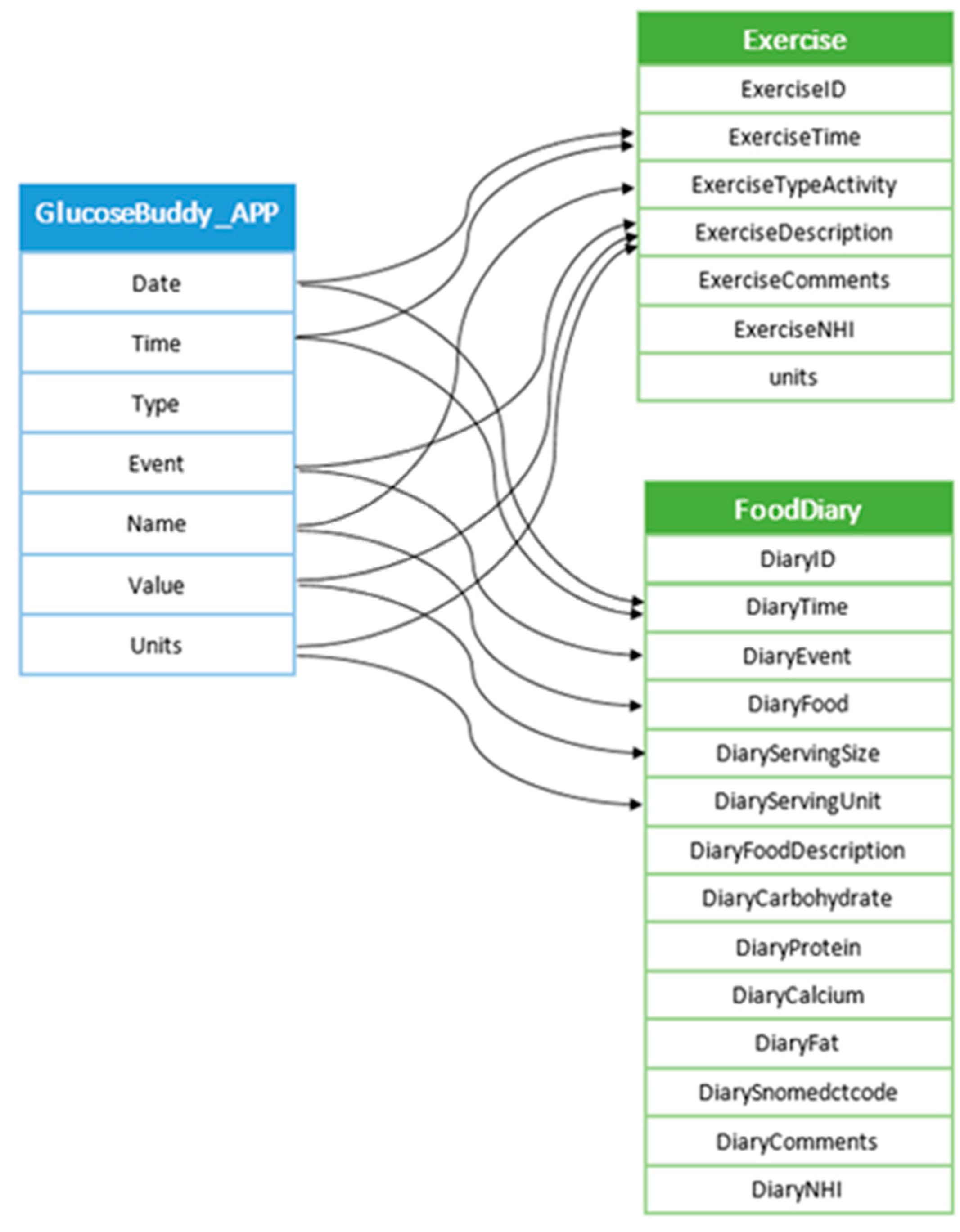
- Food description: the apps that generated the wellness data needed to contain food descriptions, to enable accurate and effortless data entry.
- Exercise data needed to be captured, if provided by a wellness app.
- Weight data needed to be captured, if provided by an app (or entered manually).
- Provide for adding SNOMED terms to food items to enable exporting patient-generated wellness data to other clinical systems.
- Theme TU1 (sharing patient data with the clinical team): the system displays, together, blood glucose readings, insulin dosage, food diary and exercise data, which saves time looking for pieces of information from various sources.
- Theme TU2 (combining food intake data and blood sugar data): the system receives input about the food intake and glucose readings on daily basis, stores the data in a single database and generates a combined report (not possible given the current hospital systems).
- Theme TU3 (pattern identification in combined data): women with GDM maintain frequent contact with midwives but have limited access to a dietician (only if their condition deteriorates). The system presents an integrated view of patient data that allows for the identification of odd patterns and provides support for subsequent consultations.
- Theme TU4 (downloading accurate data): for a number of reasons, a woman with GDM may try to conceal a high BG reading by replacing it with a lower value. Automatic downloading removes the opportunity to manipulate BG readings.
- Theme TU5 (patient self-awareness): self-management is facilitated by being aware of the current measurements of the factors related to their condition, such as blood sugar level, diet and weight.
- Theme TU6 (help with food recall): with mobile apps, women with GDM will be able to complete food diary entries immediately rather than retrospectively. This will improve the accuracy of the shared data.
- Theme TU7 (essential nutrients required): certain nutrients such as iron, calcium and protein are important for pregnancy and should be part of the data. However, women may not be experts in identifying the nutrients in their food diary. Hence, they should record everything they eat to allow the dietician to analyse their diet and complete a nutrition assessment.
- Theme TU8 (time saving): it saves time when a physician, obstetrician or dietician can see the patient without the need for the physical file held by the midwife. Additionally, most of the data entry is completed by women in their own time, with no need for clinicians to feed data into the hospital systems retrospectively (and potentially, not accurately (once the ecosystem prototype is integrated with the hospital system)).
- Theme TU9 (remotely manage patients): once educated about managing the device and apps and able to self-manage, women with GDM will need to visit the clinic less frequently. Clinicians can access data about women’s conditions and recommend a diet or insulin dosage change.
- Theme TU10 (educating women about carbohydrates and insulin dosage): women with GDM have to learn how to manage their condition in a short timeframe. It helps them not to need to count carbohydrates and record food in grams but rather to keep track of food intake measured in cups or other convenient units and still be able to adjust insulin dosage.
- Theme TU11 (food diary): it may be impractical to go through each day’s food diary and extract information about nutrient values from food databases. Women could self-manage this in their own time if the prototype had an interface for the women (especially as food intake entries are only checked if their sugar levels are outside the norm).
- Theme TU12 (willing to accept): the proposed system will be useful, as clinicians can see all information together in one place. The system will be especially useful for women who need clinical advice on changing their diet or insulin dosage. Specific benefits include logging food intake anytime and anywhere (helpful for food recall and allows one to feed inaccurate data) and enabling dieticians to make diet changes on a daily basis.
3.2. User Evaluation of System Usability/Ease of Use
- Theme TE1 (navigation): the participants associated the prototype with systems used in the clinic and commented on the navigation with reference to their prior experience. For example, when completing a task and moving to the next one, most participants attempted to ’find’ the patient again even though this was not needed. Similarly, participants could not always follow the correct order of actions (represented by buttons) needed to complete the task.
- Theme TE2 (system output): participants suggested to redesign the screen layout (where possible) to facilitate quick reading. For example, the system output (the combined report) was planned to display meal times in a 24-h column format since women with GDM need to take their glucose readings with respect to meal times (that are not fixed). Five meal timing sections were designed, to accommodate breakfast from 01:00 to 10:00 morning tea from 10:00 to 12:00, lunch from 12:00 to 15:00, afternoon tea from 15:00 to 17:00 and dinner from 17:00 to 24:00. Blood glucose readings were to be displayed in the hourly columns, close to the food diary data. A similar approach was to be followed for displaying exercise data. However, compared to the format in which blood glucose and insulin readings were displayed, food data entries were rather longer; the hourly columns in the report were narrow and the food descriptions normally broke into multiple lines (e.g., a chicken sandwich is described as two brown bread slices, 25 g of chicken, 1 tablespoon of mayonnaise sauce, 1 tablespoon of mustard sauce, rocket leaves, 2 slices of tomato and 2 tablespoons of mashed avocado). Participants found that the detailed record displaying each and every ingredient of the food item was too hard to follow. An alternative would be to ‘hide’ the ingredient description and display it when a mouse hovered over it (but losing the ability to compare the ingredients of different food items). As a result of these issues above, viewing the system output (the combined report containing the blood glucose, insulin dosage, food diary and exercise data) was rather hard as it did not fit in one screen. Reading the report required significant scrolling. Another issue was the 24-h format (e.g., ‘from 15:00 to 17:00’ meaning ‘from 3:00 p.m. to 5:00 p.m.’). To resolve the readability problems, the time slots were re-labeled and the columns were made re-sizeable; a pdf version of the report was added. Users found that the pdf file was easy to scale on the screen and the user could easily view all data for the day across one screen. Another impediment to the screen readability was the insufficient contrast, but this issue was not addressed by the developer.
- Theme TE3 (feedback): in general, clinicians found the system easy to use as its functions were aligned with their everyday work practice and environment. However, the labels on some of the navigation buttons confused them: an interesting example was the ‘Back’ button, which needed to be pressed after completing a task. Participants perceived moving to the next task as going forwards, not backwards. They also felt the need to receive system feedback on completing a task (acknowledgment or confirmation). Users found the error messages generated by the system easy to understand and follow, helping one to continue with the task at hand; adding more guidance on the screen would have been helpful too.
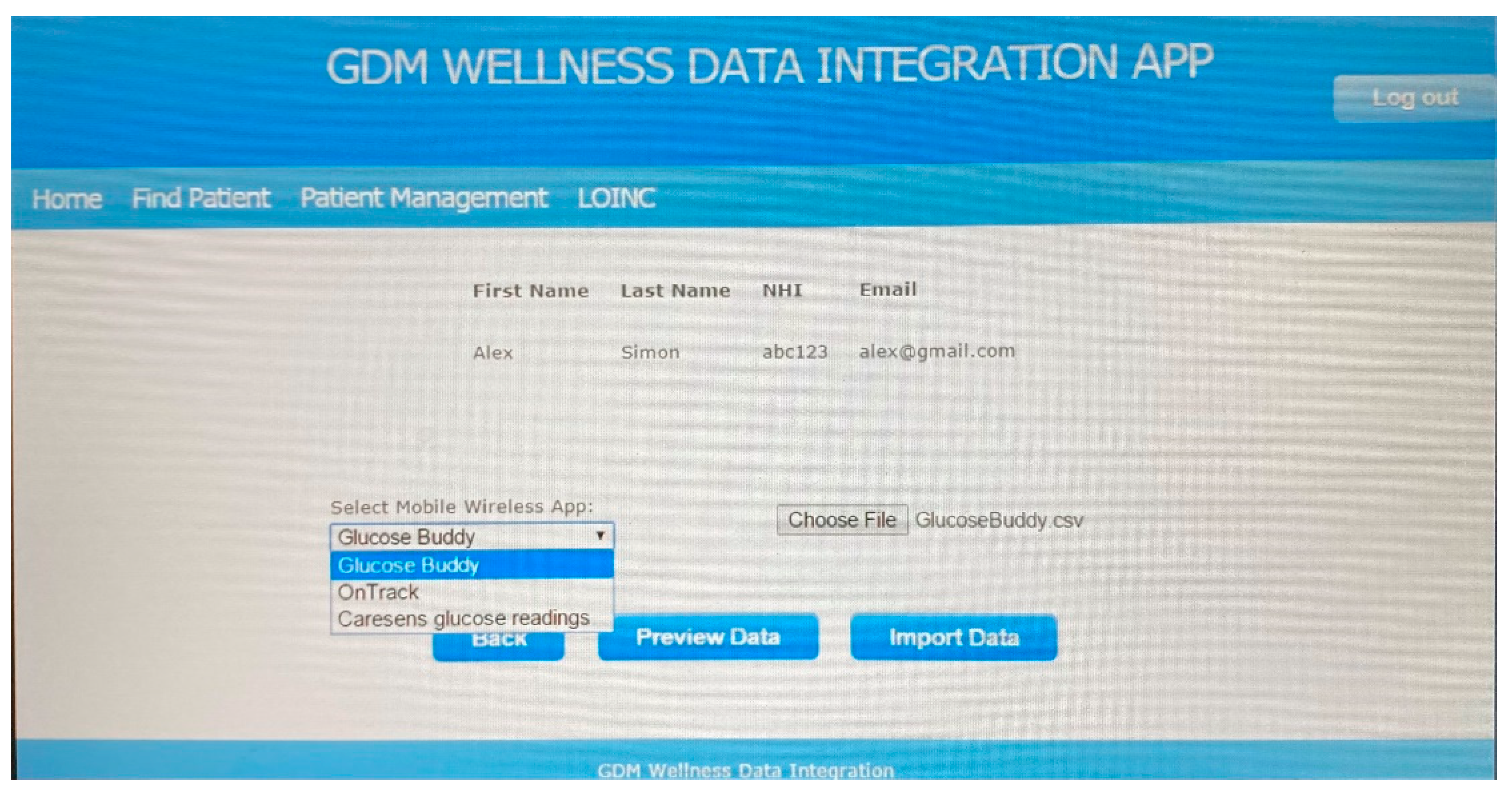
- Theme TE4 (terminology): clinicians were at ease with the medical terminology used in the system interface but found some of the ‘IT’ terms less than intuitive. For example, the options to ‘Export data’ and ‘Import data” were hard to interpret correctly, and this slowed down the completion of the related tasks. Once participants got more familiar with the system functions, they accepted some of the terms, for example, ‘Import data’ was retained as it was correctly understood as transferring data from external devices, to the system. The ‘Export data’ option data was considered better named as ‘Report’ as it referred to generating the combined report that consolidated data from various sources. Another major impediment to completing the tasks was that clinicians were not used to annotate patient generated using medical terminology such as LOINC codes.
- Theme TE5 (comments): comments were useful for clinicians to make notes alongside the data readings. Some of the comments would reflect the activity, food intake or insulin dosage.
- Theme TE6 (existing experience): women with GDM who reviewed Prototype 2 did not have much feedback to offer about the interface and design as the system was built primarily for clinicians. However, most participants were able to complete the first three tasks without difficulty as they were familiar with computers and smart phones.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saeedi, M.; Cao, Y.; Fadl, H.; Gustafson, H.; Simmons, D. Increasing prevalence of gestational diabetes mellitus when implementing the IADPSG criteria: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2020, 172, 108642. [Google Scholar] [CrossRef] [PubMed]
- Auckland DHB. Available online: https://nationalwomenshealth.adhb.govt.nz/assets/Womens-health/Documents/ACR/2020-Annual-Clinical-Report.pdf (accessed on 23 October 2021).
- Tobias, D.K.; Hu, F.B.; Chavarro, J.; Rosner, B.; Mozaffarian, D.; Zhang, C. Healthful Dietary Patterns and Type 2 Diabetes Mellitus Risk Among Women With a History of Gestational Diabetes Mellitus. Arch. Intern. Med. 2012, 172, 1566–1572. [Google Scholar] [CrossRef] [Green Version]
- Landon, M.B. Is there a benefit to the treatment of mild gestational diabetes mellitus? Am. J. Obstet. Gynecol. 2010, 202, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, L.; Poulsen, C.W.; Kampmann, U.; Smedegaard, S.B.; Ovesen, P.G.; Fuglsang, J. Diet and Healthy Lifestyle in the Management of Gestational Diabetes Mellitus. Nutrients 2020, 12, 3050. [Google Scholar] [CrossRef]
- MacKillop, L.; Hirst, J.E.; Bartlett, K.J.; Birks, J.S.; Clifton, L.; Farmer, A.J.; Gibson, O.; Kenworthy, Y.; Levy, J.C.; Loerup, L.; et al. Comparing the Efficacy of a Mobile Phone-Based Blood Glucose Management System With Standard Clinic Care in Women With Gestational Diabetes: Randomized Controlled Trial. JMIR mHealth uHealth 2018, 6, e71. [Google Scholar] [CrossRef]
- MacKillop, L.H.; Bartlett, K.; Birks, J.; Farmer, A.J.; Gibson, O.J.; Kevat, D.A.; Kenworthy, Y.; Levy, J.C.; Loerup, L.; Tarassenko, L.; et al. Trial protocol to compare the efficacy of a smartphone-based blood glucose management system with standard clinic care in the gestational diabetic population. BMJ Open 2016, 6, e009702. [Google Scholar] [CrossRef]
- Skar, J.B.; Garnweidner-Holme, L.M.; Lukasse, M.; Terragni, L. Women’s experiences with using a smartphone app (the Pregnant+ app) to manage gestational diabetes mellitus in a randomised controlled trial. Midwifery 2018, 58, 102–108. [Google Scholar] [CrossRef]
- Guo, H.; Zhang, Y.; Li, P.; Zhou, P.; Chen, L.-M.; Li, S.-Y. Evaluating the effects of mobile health intervention on weight management, glycemic control and pregnancy outcomes in patients with gestational diabetes mellitus. J. Endocrinol. Investig. 2018, 42, 709–714. [Google Scholar] [CrossRef]
- Pais, S.; Parry, D.; Petrova, K.; Rowan, J. Acceptance of using an ecosystem of mobile apps for use in diabetes clinic for self-management of gestational diabetes mellitus. In MEDINFO 2017: Precision Healthcare through Informatics; Gundlapalli, A.V., Jaulent, M.-C., Zhao, D., Eds.; IOS Press: Amsterdam, The Netherlands, 2018; Volume 245, pp. 188–192. [Google Scholar]
- Taherdoost, H. A review of technology acceptance and adoption models and theories. Procedia Manuf. 2018, 22, 960–967. [Google Scholar] [CrossRef]
- Harst, L.; Lantzsch, H.; Scheibe, M. Theories Predicting End-User Acceptance of Telemedicine Use: Systematic Review. J. Med. Internet Res. 2019, 21, e13117. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, A.; Rasul, T.; Yousaf, A.; Zaman, U. Understanding Factors Influencing Elderly Diabetic Patients’ Continuance Intention to Use Digital Health Wearables: Extending the Technology Acceptance Model (TAM). J. Open Innov. Technol. Mark. Complex. 2020, 6, 81. [Google Scholar] [CrossRef]
- Rahimi, B.; Nadri, H.; Afshar, H.L.; Timpka, T. A Systematic Review of the Technology Acceptance Model in Health Informatics. Appl. Clin. Inform. 2018, 9, 604–634. [Google Scholar] [CrossRef] [Green Version]
- Alsswey, A.; Al-Samarraie, H. Elderly users’ acceptance of mHealth user interface (UI) design-based culture: The moderator role of age. J. Multimodal User Interfaces 2019, 14, 49–59. [Google Scholar] [CrossRef]
- Deng, Z.; Hong, Z.; Ren, C.; Zhang, W.; Xiang, F. What Predicts Patients’ Adoption Intention Toward mHealth Services in China: Empirical Study. JMIR mHealth uHealth 2018, 6, e172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tao, D.; Wang, T.; Wang, T.; Zhang, T.; Zhang, X.; Qu, X. A systematic review and meta-analysis of user acceptance of consumer-oriented health information technologies. Comput. Hum. Behav. 2019, 104, 106147. [Google Scholar] [CrossRef]
- Sobrinho, A.; Da Silva, L.D.; Perkusich, A.; Pinheiro, M.E.; Cunha, P. Design and evaluation of a mobile application to assist the self-monitoring of the chronic kidney disease in developing countries. BMC Med. Inform. Decis. Mak. 2018, 18, 1–14. [Google Scholar] [CrossRef]
- Calvillo-Arbizu, J.; Roa-Romero, L.M.; Estudillo-Valderrama, M.A.; Salgueira-Lazo, M.; Aresté-Fosalba, N.; Del-Castillo-Rodríguez, N.L.; González-Cabrera, F.; Marrero-Robayna, S.; López-De-La-Manzana, V.; Martínez, I.R. User-centred design for developing e-Health system for renal patients at home (AppNephro). Int. J. Med. Inform. 2019, 125, 47–54. [Google Scholar] [CrossRef]
- De Luca, V.; Lazic, V.; Birov, S.; Piesche, K.; Beyhan, O.; Pengo, M.F.; Melgara, M.; Sherman, M.H.; Lilja, M.; Balenovic, A.; et al. Digitally Enabled Health Service for the Integrated Management of Hypertension: A Participatory User-Centred Design Process. Int. J. Environ. Res. Public Health 2021, 18, 12442. [Google Scholar] [CrossRef] [PubMed]
- Dopp, A.R.; Parisi, K.E.; Munson, S.A.; Lyon, A.R. Integrating implementation and user-centred design strategies to enhance the impact of health services: Protocol from a concept mapping study. Health Res. Policy Syst. 2019, 17, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Cornet, V.P.; Toscos, T.; Bolchini, D.; Ghahari, R.R.; Ahmed, R.; Daley, C.; Mirro, M.J.; Holden, R.J. Untold Stories in User-Centered Design of Mobile Health: Practical Challenges and Strategies Learned From the Design and Evaluation of an App for Older Adults With Heart Failure. JMIR mHealth uHealth 2020, 8, e17703. [Google Scholar] [CrossRef]
- Vaisson, G.; Provencher, T.; Dugas, M.; Trottier, M.; Dansokho, S.C.; Colquhoun, H.; Fagerlin, A.; Giguere, A.M.C.; Hakim, H.; Haslett, L.; et al. User Involvement in the Design and Development of Patient Decision Aids and Other Personal Health Tools: A Systematic Review. Med. Decis. Mak. 2021, 41, 261–274. [Google Scholar] [CrossRef]
- Shachak, A.; Kuziemsky, C.; Petersen, C. Beyond TAM and UTAUT: Future directions for HIT implementation research. J. Biomed. Inform. 2019, 100, 103315. [Google Scholar] [CrossRef]
- Wolcott, M.D.; Lobczowski, N.G. Using cognitive interviews and think-aloud protocols to understand thought processes. Curr. Pharm. Teach. Learn. 2020, 13, 181–188. [Google Scholar] [CrossRef]
- Kilsdonk, E.; Peute, L.; Riezebos, R.; Kremer, L.; Jaspers, M. Uncovering healthcare practitioners’ information processing using the think-aloud method: From paper-based guideline to clinical decision support system. Int. J. Med. Inform. 2016, 86, 10–19. [Google Scholar] [CrossRef] [Green Version]
- Richardson, S.; Mishuris, R.; O’Connell, A.; Feldstein, D.; Hess, R.; Smith, P.; McCullagh, L.; McGinn, T.; Mann, D. “Think aloud” and “Near live” usability testing of two complex clinical decision support tools. Int. J. Med. Inform. 2017, 106, 1–8. [Google Scholar] [CrossRef]
- Malterud, K.; Siersma, V.D.; Dorrit Guassora, A. Sample size in qualitative interview studies: Guided by information power. Qual. Health Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef]
- Maramba, I.; Chatterjee, A.; Newman, C. Methods of usability testing in the development of eHealth applications: A scoping review. Int. J. Med. Inform. 2019, 126, 95–104. [Google Scholar] [CrossRef]
- Bolle, S.; Romijn, G.; Smets, E.M.A.; Loos, E.F.; Kunneman, M.; Van Weert, J.C.M. Older Cancer Patients’ User Experiences With Web-Based Health Information Tools: A Think-Aloud Study. J. Med. Internet Res. 2016, 18, e208. [Google Scholar] [CrossRef]
- Ozok, A.A.; Wu, H.; Garrido, M.; Pronovost, P.J.; Gurses, A.P. Usability and perceived usefulness of personal health records for preventive health care: A case study focusing on patients' and primary care providers' perspectives. Appl. Ergon. 2013, 45, 613–628. [Google Scholar] [CrossRef]
- Money, A.G.; Atwal, A.; Young, K.L.; Day, Y.; Wilson, L.; Money, K.G. Using the Technology Acceptance Model to explore community dwelling older adults' perceptions of a 3D interior design application to facilitate pre-discharge home adaptations. BMC Med. Inform. Decis. Mak. 2015, 15, 73. [Google Scholar] [CrossRef] [Green Version]
- Cervera, M.; Albert, M.; Torres, V.; Pelechano, V. On the usefulness and ease of use of a model-driven Method Engineering approach. Inf. Syst. 2015, 50, 36–50. [Google Scholar] [CrossRef] [Green Version]
- Lindgren, B.-M.; Lundman, B.; Graneheim, U.H. Abstraction and interpretation during the qualitative content analysis process. Int. J. Nurs. Stud. 2020, 108, 103632. [Google Scholar] [CrossRef]
- Kirwan, M.; Duncan, M.J.; Vandelanotte, C.; Mummery, W.K. Design, development, and formative evaluation of a smartphone application for recording and monitoring physical activity levels: The 10,000 Steps ‘iStepLog’. Health Educ. Behav. 2013, 40, 140–151. [Google Scholar] [CrossRef]
- Pais, S.; Petrova, K.; Parry, D. Integrating Patient-Generated Wellness Data: A User-Centered Approach. In Proceedings of the ACSW '20 Australasian Computer Science Week Multiconference, Melbourne, VIC, Australia, 4–6 February 2020. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Role | Profile | Involvement |
|---|---|---|
| Dietician | Nutrition assessment of patients with gestational diabetes | Semi-structured interviews INT1, INT2 and INT3. TA sessions TAP1 and TAP2 |
| Obstetrician | Provides care during pregnancy and birth and deals with complications caused by GDM | Semi-structured interviews INT1, INT2 and INT3. TA sessions TAP1 and TAP2 |
| Midwife | Provides primary care related to GDM during pregnancy, monitors weekly/fortnightly progress. | Semi-structured interviews INT1, INT2 and INT3. TA sessions TAP1 and TAP2 |
| Woman with GDP | Pregnant woman diagnosed with GDM, with no prior diabetes condition | Semi-structured interview INT3. TA session TAP2 |
| Ex-/Post-Ante | Evaluation Material | Evaluation Method | Participants | Main Focus | |
|---|---|---|---|---|---|
| 1 | Ex-ante | Mock-up prototype on (paper) | Structured interview INT1 | Clinicians (5) | Identifying key user needs/requirements for a useful clinical system |
| 2 | Ex-ante | Prototype 1 | Semi-structured interview INT2 | Clinicians (5) | Review of system functionality. Initial feedback on system interface and navigation |
| 3 | Ex-post | Prototype 1 | TA tasks: session TAP1 | Clinicians (5) | Examining system usability and ease of use |
| 4 | Ex-post | Prototype 2 | Semi-structured interview INT3 | Clinicians (10), women with GDM (5) | Further review of system functionality; gauging user acceptance |
| 5 | Ex-post | Prototype 2 | TA tasks: session TAP2 | Clinicians (10), women with GDM (5) | Further examination of system usability and ease of use; gauging user acceptance |
| Theme | Interview Excerpts |
|---|---|
| TU1 | “The prototype helps share data within the team and I do not have to ask the midwife for the patient file” |
| TU2 | “Yes, it includes pretty much everything that you want to know about: BG 1, FD 1, exercise”; “You need an app which gets the calories, carbohydrate breakdown, protein and fat”; “Wellness data is representative. Easy to compare FD, exercise, insulin dosage in comparison with BG”; “Reflects physical activity and FD together with treatment and dosage and sugar level” |
| TU3 | “I can see people’s pattern of their eating and timings as well”; “You notice the frequency and when people are doing something different which is part of the learning and teaching we give a lot of information”; “…Useful, I see the patients once, and could just run an eye over the report thereafter even if I don’t have an appointment” |
| TU4 | “BG readings are fudged to please the midwife”; “The issue with patients using apps is about accuracy and telling the truth”; Patients do not like having their health records saved specially when they have high readings” |
| TU5 | “Self-awareness help women keep their sugar and their weight under control” |
| TU6 | “App could help with recall…”; “Patients should have knowledge of what they are eating and record it correctly in the app” |
| TU7 | “Calories will not tell you what you have eaten… I want to know everything they are eating”; “What’s the carbohydrate amount is important, also accessing them for nutrient adequacy” |
| TU8 | “When a woman comes to my room, I don’t have to find a midwife what she said to her and we don’t waste time” |
| TU9 | “We can all log into our computers and access the information about the patient whom we want to see” |
| TU10 | “I know my patients would find it helpful to know how many carbohydrates”; “It may help quantify how much insulin to take or adjust to… it is sufficient for them to say 2 slices brown bread, ½ cup rice” |
| TU11 | “It is nice that it incorporates with food database… But the amount of time we get to be with the women there is probably not much time”; “They only need to write down only if they have been eating only for that time what they have had high blood sugars” |
| TU12 | “I would absolutely use it and comfortable to share the data with a clinician if suitable apps are available”; “…data is available for clinicians at their fingertips. It can be entered into the system directly, taking out the need for unnecessary paperwork which can be time consuming. Also once data is available it can be analysed in various ways for the betterment of patients suffering from gestational diabetes”; …I think probably 70% of people don’t mind, they don’t mind, you know, to be honest” |
| Theme | Interview Excerpts |
|---|---|
| TE1 | “Sometimes for our bookings for … ultrasound say, so we have got one screen then next another screen, we click next and it is self-explanatory”; ”It looks like it finishes there (on screen seeing part of the data). So it is not very good” |
| TE2 | “Text in narrow column breaking into multiple lines”; “Challenging if all details are entered, difficult to fit in narrow columns”; “(Viewing the pdf) This is much nicer to look at. You can see what exactly the readings were, when the readings were taken and what has been eaten with different meals on different days. It is much easier to see in pdf than the first report that was generated (on screen)”; “Time in hours as heading across is ideal to read”; “Easy to compare FD, exercise, insulin dosage in comparison with BG”; “Hard to read the update on the blue background”; “I think colour scheme and it is not just black and white. Maybe it is easier to read”; “Glucose readings across the day with carbohydrate intake is preferred” |
| TE3 | “Easy. Should not be difficult as it is work related”; “I might have little problem in the beginning about navigation. How to move forward when the button on screen says ‘Back’”; “Once you have learned the navigation and menu it won’t be a problem” |
| TE4 | “I have clicked one reading and not sure what LOINC readings are?”; “It is pretty user friendly”; “I go edit and use drop down menu to select one code fasting and non-fasting?” |
| TE5 | “I might write a comment saying if I know she forgets her insulin, she did more exercise than usual, or she had a big slice of cake (baby shower), maybe that kind of thing I might write.” |
| TE6 | “Most women don’t mind doing email. Most women are on email so emailing blood/sugars… I think probably 70% of people don’t mind, they don’t mind, you know, to be honest…”; “…used Fitness pal, step counter”; “And if you offer them an app I am sure the young ones especially would be [interested]…” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pais, S.; Petrova, K.; Parry, D. Enhancing System Acceptance through User-Centred Design: Integrating Patient Generated Wellness Data. Sensors 2022, 22, 45. https://doi.org/10.3390/s22010045
Pais S, Petrova K, Parry D. Enhancing System Acceptance through User-Centred Design: Integrating Patient Generated Wellness Data. Sensors. 2022; 22(1):45. https://doi.org/10.3390/s22010045
Chicago/Turabian StylePais, Sarita, Krassie Petrova, and Dave Parry. 2022. "Enhancing System Acceptance through User-Centred Design: Integrating Patient Generated Wellness Data" Sensors 22, no. 1: 45. https://doi.org/10.3390/s22010045
APA StylePais, S., Petrova, K., & Parry, D. (2022). Enhancing System Acceptance through User-Centred Design: Integrating Patient Generated Wellness Data. Sensors, 22(1), 45. https://doi.org/10.3390/s22010045