
Measuring Outdoor Walking Capacities Using Global Positioning System in People with Multiple Sclerosis: Clinical and Methodological Insights from an Exploratory Study


 and
and
Abstract
1. Introduction
- highlight methodological issues that may occur when implementing an outdoor walking evaluation with GPS measurements in people with MS; and
- explore the construct validity of outdoor maximal walking distance and outdoor usual walking speed as functional outcomes in people with MS.
2. Materials and Methods
2.1. Recruitment and Framework of the Study
2.2. Protocol
- ≤4 (can walk about 500 m or more without assistance or rest and can perform all their daily life activities);
- 4.5 (can walk about 300 m without assistance or rest and can perform almost all their daily life activities);
- 5.0 (can walk about 200 m without assistance or rest and cannot perform all their daily life activities);
- 5.5 (can walk about 100 m without assistance or rest and cannot work part-time without provisions);
- 6.0 (needs assistance [rest, aid, presence of another person] to walk about 100 m).
2.3. GPS Data Analysis
- Step 1, preparation of the dataset to have the required data in an appropriate format for further analysis (this step included the addition, in the dataset, of the altitude data from the French National Institute of Geography map projections obtained using CartoExploreur3 [version 3.11.0, build 2.8.10.14, Bayo, Ltd., Abrest, France] and that corresponded to the latitude and longitude data recorded by the GPS device; an illustration of the procedure to get these data is provided elsewhere [20]).
- Step 2, selection, based on graphical visualization, of the time period of interest (i.e., a few seconds before the first walking bout of the session to a few seconds after the last walking bout of the session); this step also allowed us to graphically confirm data validity (i.e., absence of spurious GPS signals that could prevent the possibility to detect the occurrence of a walking bout or a stopping bout).
- Step 3, calculations of the mean (), the standard deviation (), and the coefficient of variation (CV(ν)) of speed using a representative 120-s period (or less if not possible) to allow for the configuration of appropriate speed signal filters [13].
- Step 4, processing the speed data to remove noise and artifacts from the speed signal [13]. This step consisted of implementing several filtering and smoothing procedures (Figure 1). First, a filter was used to manage speed values that were greater than twice . Such values were replaced by the mean of the speed values corresponding to the five following epochs. Then, a second filter was used to set to 0 the speed values that were lower than a threshold value computed as follows: -K × ; K being a coefficient set according to the value of CV(ν). When CV(ν) was ≥15%, K was set to 2, and when CV(ν) was <15%, K was set to 5. Then, a series of smoothing actions were sequentially performed on the speed data to remove very short walking and stopping bouts (i.e., bouts that corresponded to one or two 1-s epochs only). These actions were as follows:
- Action 1: For a given epoch i, if the speed value of the epoch i − 1 was 0 and the considered epoch i was greater than 0, then the value of the epoch i was shifted to the mean of the five following epochs.
- Action 2: For a given epoch i, if the speed value was 0 and the values of the epochs i − 2, i − 1, i + 2, and i + 3 were greater than 0, then the value of the epoch i was shifted to the mean of the speed values corresponding to the epochs i − 2, i − 1, i + 2, and i + 3.
- Action 3: Same action as Action 2.
- Action 4: For a given epoch i, if the speed value was greater than 0 and the values of the epochs i − 2, i − 1, i + 2, and i + 3 were 0, then the value of the epoch i was shifted to the mean of the speed values corresponding to the epochs i− 2, i − 1, i + 2, and i + 3, that is 0.
- Action 5: Same action as Action 4.
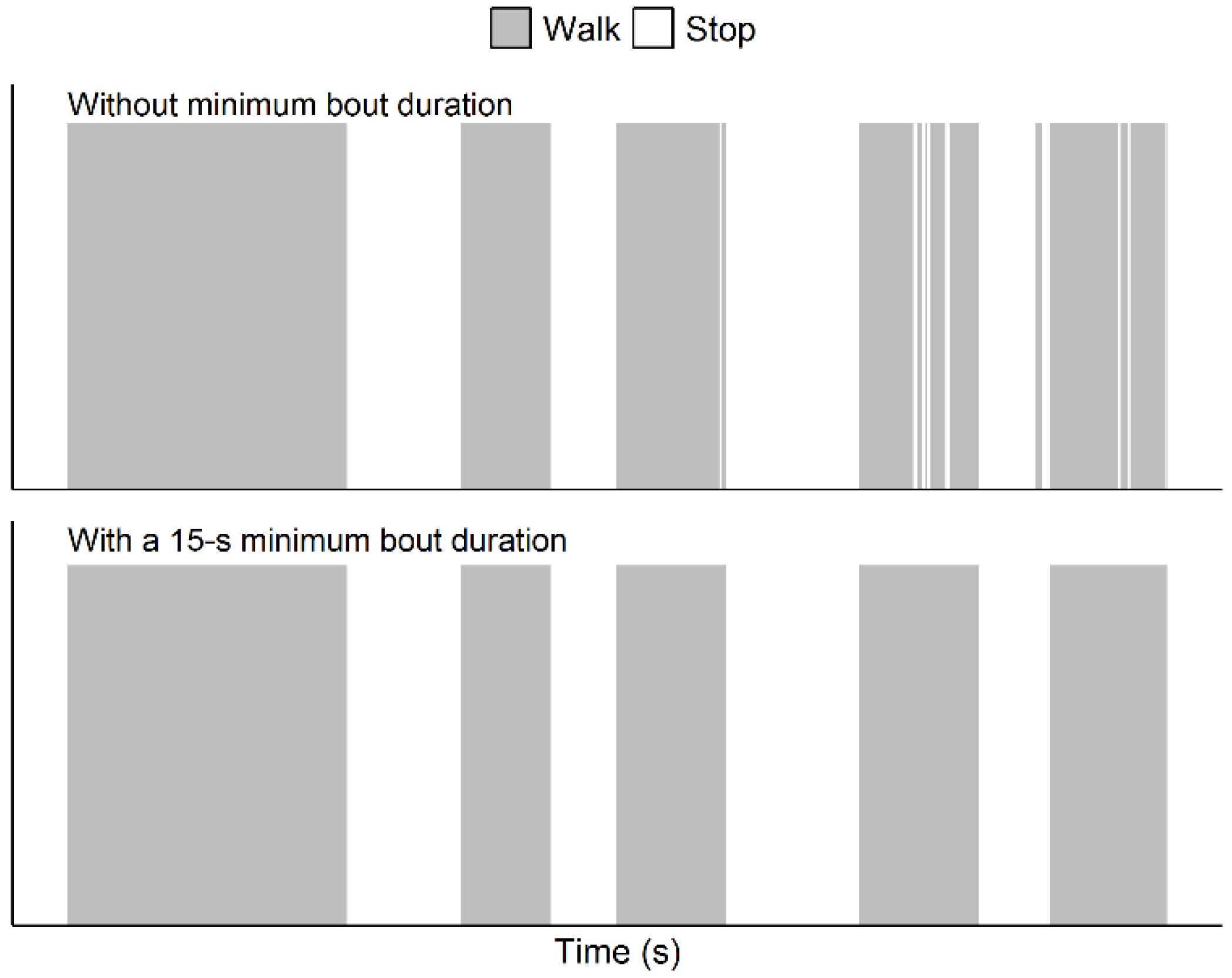
Of note, this methodology actually managed shorter artifactual bouts than in the papers by Le Faucheur et al. [13] and Noury-Desvaux et al. [14]. Indeed, in the present study the methodology was implemented using epochs of a shorter duration (i.e., with epochs of 1 s due to a 1-Hz recording rate) than previously performed (i.e., with epochs of 2 s due to a 0.5-Hz recording rate [13]). In these previous studies [13,14], more than 90% of the walking and stopping bouts could be correctly detected using the speed processing methodology, with a typical error expressed as a coefficient of variation for estimating speed and distance <5% whatever the speeds and distances tested using the DG100 GPS receiver [14]. - Step 5, identification of the walking and stopping bouts based on speed information and a minimum bout duration of 15 s [13]. For this last step, the duration of a given bout was incremented using the durations of the subsequent detected bouts as long as that the bouts lasted less than 15 s, as illustrated in Figure 2. The minimum duration of 15 s to validate a shift from a walking bout to a stopping bout (and vice versa) was chosen because previous work [13] showed this was the shortest duration beyond which all bouts could be correctly detected using the present methodology, and this duration was thought to be sufficiently short to not correspond to a true and meaningful walking bout or stopping bout.
2.4. Statistical Analysis
2.5. Data and R Code Availability
3. Results
3.1. Participants Characteristics
3.2. The Outdoor Walking Capacities
3.3. Methodological Issues
3.4. Relationships Between Outdoor Walking Capacities and 6-min Total Walking Distance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2016 Multiple Sclerosis Collaborators, Global, regional, and national burden of multiple sclerosis 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 269–285. [CrossRef]
- Brownlee, W.J.; Hardy, T.A.; Fazekas, F.; Miller, D.H. Diagnosis of multiple sclerosis: Progress and challenges. Lancet 2017, 389, 1336–1346. [Google Scholar] [CrossRef]
- Sutliff, M.H. Contribution of impaired mobility to patient burden in multiple sclerosis. Curr. Med. Res. Opin. 2010, 26, 109–119. [Google Scholar] [CrossRef]
- Buoite Stella, A.; Morelli, M.E.; Giudici, F.; Sartori, A.; Manganotti, P.; di Prampero, P.E. Comfortable walking speed and energy cost of locomotion in patients with multiple sclerosis. Eur. J. Appl. Physiol. 2020, 120, 551–566. [Google Scholar] [CrossRef] [PubMed]
- Sandroff, B.M.; Klaren, R.E.; Motl, R.W. Relationships among physical inactivity, deconditioning, and walking impairment in persons with multiple sclerosis. J. Neurol. Phys. Ther. 2015, 39, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Sparaco, M.; Lavorgna, L.; Conforti, R.; Tedeschi, G.; Bonavita, S. The role of wearable devices in multiple sclerosis. Mult. Scler. Int. 2018, 2018, 7627643. [Google Scholar] [CrossRef]
- Le Faucheur, A.; Noury-Desvaux, B.; Mahe, G.; Sauvaget, T.; Saumet, J.L.; Leftheriotis, G.; Abraham, P. Variability and short-term determinants of walking capacity in patients with intermittent claudication. J. Vasc. Surg. 2010, 51, 886–892. [Google Scholar] [CrossRef][Green Version]
- Gernigon, M.; Le Faucheur, A.; Noury-Desvaux, B.; Mahe, G.; Abraham, P.; Post-GPS Study Coinvestigators Group. Applicability of global positioning system for the assessment of walking ability in patients with arterial claudication. J. Vasc. Surg. 2014, 60, 973–981.e1. [Google Scholar] [CrossRef]
- Créange, A.; Serre, I.; Levasseur, M.; Audry, D.; Nineb, A.; Boerio, D.; Moreau, T.; Maison, P.; Reseau, S.-S. Walking capacities in multiple sclerosis measured by global positioning system odometer. Mult. Scler. 2007, 13, 220–223. [Google Scholar] [CrossRef]
- Dalla-Costa, G.; Radaelli, M.; Maida, S.; Sangalli, F.; Colombo, B.; Moiola, L.; Comi, G.; Martinelli, V. Smart watch, smarter EDSS: Improving disability assessment in multiple sclerosis clinical practice. J. Neurol. Sci. 2017, 383, 166–168. [Google Scholar] [CrossRef]
- Le Faucheur, A.; Abraham, P.; Jaquinandi, V.; Bouye, P.; Saumet, J.L.; Noury-Desvaux, B. Measurement of walking distance and speed in patients with peripheral arterial disease: A novel method using a global positioning system. Circulation 2008, 117, 897–904. [Google Scholar] [CrossRef]
- Gernigon, M.; Le Faucheur, A.; Fradin, D.; Noury-Desvaux, B.; Landron, C.; Mahe, G.; Abraham, P. Global positioning system use in the community to evaluate improvements in walking after revascularization: A prospective multicenter study with 6-month follow-up in patients with peripheral arterial disease. Medicine 2015, 94, e838. [Google Scholar] [CrossRef] [PubMed]
- Le Faucheur, A.; Abraham, P.; Jaquinandi, V.; Bouye, P.; Saumet, J.L.; Noury-Desvaux, B. Study of human outdoor walking with a low-cost GPS and simple spreadsheet analysis. Med. Sci. Sports Exerc. 2007, 39, 1570–1578. [Google Scholar] [CrossRef] [PubMed]
- Noury-Desvaux, B.; Abraham, P.; Mahe, G.; Sauvaget, T.; Leftheriotis, G.; Le Faucheur, A. The accuracy of a simple, low-cost GPS data logger/receiver to study outdoor human walking in view of health and clinical studies. PLoS ONE 2011, 6, e23027. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- American Thoracic Society. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Abraham, P.; Noury-Desvaux, B.; Gernigon, M.; Mahe, G.; Sauvaget, T.; Leftheriotis, G.; Le Faucheur, A. The inter- and intra-unit variability of a low-cost GPS data logger/receiver to study human outdoor walking in view of health and clinical studies. PLoS ONE 2012, 7, e31338. [Google Scholar] [CrossRef]
- SFSEP. Société Francophone de la Sclérose en Plaques. Available online: https://sfsep.org/echelle-fss/ (accessed on 28 February 2019).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 26 April 2019).
- De Müllenheim, P.Y.; Chaudru, S.; Gernigon, M.; Mahé, G.; Bickert, S.; Prioux, J.; Noury-Desvaux, B.; Le Faucheur, A. Accuracy of a low-cost global positioning system receiver for estimating grade during outdoor walking. Physiol. Meas. 2016, 37, 1741–1756. [Google Scholar] [CrossRef]
- Mangiafico, S.S. Summary and Analysis of Extension Program Evaluation in R, Version 1.18.1. 2016. Available online: https://rcompanion.org/ (accessed on 30 September 2020).
- Nordanstig, J.; Broeren, M.; Hensater, M.; Perlander, A.; Osterberg, K.; Jivegard, L. Six-minute walk test closely correlates to “real-life” outdoor walking capacity and quality of life in patients with intermittent claudication. J. Vasc. Surg. 2014, 60, 404–409. [Google Scholar] [CrossRef]
- Murtagh, E.M.; Mair, J.L.; Aguiar, E.; Tudor-Locke, C.; Murphy, M.H. Outdoor walking speeds of apparently healthy adults: A systematic review and meta-analysis. Sports Med. 2021, 51, 125–141. [Google Scholar] [CrossRef]
- Cederberg, K.L.J.; Sikes, E.M.; Bartolucci, A.A.; Motl, R.W. Walking endurance in multiple sclerosis: Meta-analysis of six-minute walk test performance. Gait. Posture. 2019, 73, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, H.; Wotzel, C.; Erasmus, L.P.; Kleinpeter, M.; Konig, N.; Pollmann, W. Day-to-day variability of maximum walking distance in MS patients can mislead to relevant changes in the Expanded Disability Status Scale (EDSS): Average walking speed is a more constant parameter. Mult. Scler. J. 2001, 7, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Taoum, A.; Chaudru, S.; de Müllenheim, P.Y.; Congnard, F.; Emily, M.; Noury-Desvaux, B.; Bickert, S.; Carrault, G.; Mahe, G.; Le Faucheur, A. Comparison of activity monitors accuracy in assessing intermittent outdoor walking. Med. Sci. Sports Exerc. 2021, in press. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Women, n (%) | 11 (92) |
|---|---|
| Age, yr | 55 [48–61] |
| Height, m | 1.64 [1.59–1.67] |
| Body mass, kg | 62 [57–64] |
| Body mass index, kg·m−2 | 21.75 [20.46–25.56] |
| EDSS score, n (%) | |
| ≤4.0 | 4 (33) |
| 4.5 | 4 (33) |
| 5.0 | 1 (8) |
| 6.0 | 3 (25) |
| 6-min walking test | |
| FSS score the day of the test | 5.5 [4.2–6.0] |
| Total walking distance, m | 312 [278–338] |
| Device assistance | |
| No assistive device, n (%) | 8 (67) |
| Cane or crutch, n (%) | 4 (33) |
| All Participants (N = 12) | |
|---|---|
| FSS score | 5.25 [4.38–5.85] |
| Session duration, min | 30.4 [29.0–50.5] (28.8; 47.3) |
| Total walking time, min | 23.6 [19.5–49.7] (19.5; 45.6) |
| Total walking distance, m | 978 [709–2832] (710; 2190) |
| Mean speed over all the walking bouts, km/h | 2.52 [2.19–3.04] (2.17; 2.93) |
| Participants with ≥1 stop (N = 10),% | 83 (56; 97) |
| Participants with ≥1 stop (N = 10) | |
| Walking distance | |
| Max, m | 410 [252–1615] (226; 1350) |
| Mean, m | 251 [153–1263] (152; 1110) |
| CV,% (N = 7 with ≥2 walking bouts) | 52.9 [49.1–69.7] (41.2; 58.9) |
| Walking speed | |
| Mean, km/h | 2.46 [2.20–2.82] (2.13; 2.74) |
| CV,% | 6.1 [5.2–14.4] (4.2; 10.9) |
| Stop duration | |
| Mean, min | 2.5 [1.4–3.5] (1.3; 3.5) |
| CV,% (N = 5 with ≥2 stops) | 70.4 [60.3–138.8] (34.4; 139.0) |
| Participants with the greatest walking distance recorded during the second bout or a subsequent one (N = 4),% | 40 (15; 70) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delahaye, C.; Chaves, D.; Congnard, F.; Noury-Desvaux, B.; de Müllenheim, P.-Y.; on behalf of the SOCOS Group. Measuring Outdoor Walking Capacities Using Global Positioning System in People with Multiple Sclerosis: Clinical and Methodological Insights from an Exploratory Study. Sensors 2021, 21, 3189. https://doi.org/10.3390/s21093189
Delahaye C, Chaves D, Congnard F, Noury-Desvaux B, de Müllenheim P-Y, on behalf of the SOCOS Group. Measuring Outdoor Walking Capacities Using Global Positioning System in People with Multiple Sclerosis: Clinical and Methodological Insights from an Exploratory Study. Sensors. 2021; 21(9):3189. https://doi.org/10.3390/s21093189
Chicago/Turabian StyleDelahaye, Coralie, Dorine Chaves, Florian Congnard, Bénédicte Noury-Desvaux, Pierre-Yves de Müllenheim, and on behalf of the SOCOS Group. 2021. "Measuring Outdoor Walking Capacities Using Global Positioning System in People with Multiple Sclerosis: Clinical and Methodological Insights from an Exploratory Study" Sensors 21, no. 9: 3189. https://doi.org/10.3390/s21093189
APA StyleDelahaye, C., Chaves, D., Congnard, F., Noury-Desvaux, B., de Müllenheim, P.-Y., & on behalf of the SOCOS Group. (2021). Measuring Outdoor Walking Capacities Using Global Positioning System in People with Multiple Sclerosis: Clinical and Methodological Insights from an Exploratory Study. Sensors, 21(9), 3189. https://doi.org/10.3390/s21093189