
Blindness and the Reliability of Downwards Sensors to Avoid Obstacles: A Study with the EyeCane

 , , ,
, , ,  , and
, and 
Abstract
1. Introduction

2. Materials and Methods
2.1. Participants and Ethics
2.2. Apparatus
2.3. Experimental Procedure
2.3.1. Obstacle Course
2.3.2. Training Phase
2.3.3. Test Phase
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Influence of Visual Experience
4.2. The EyeCane as a Primary Mobility Aid
4.3. Implications for ETA Design
- (1)
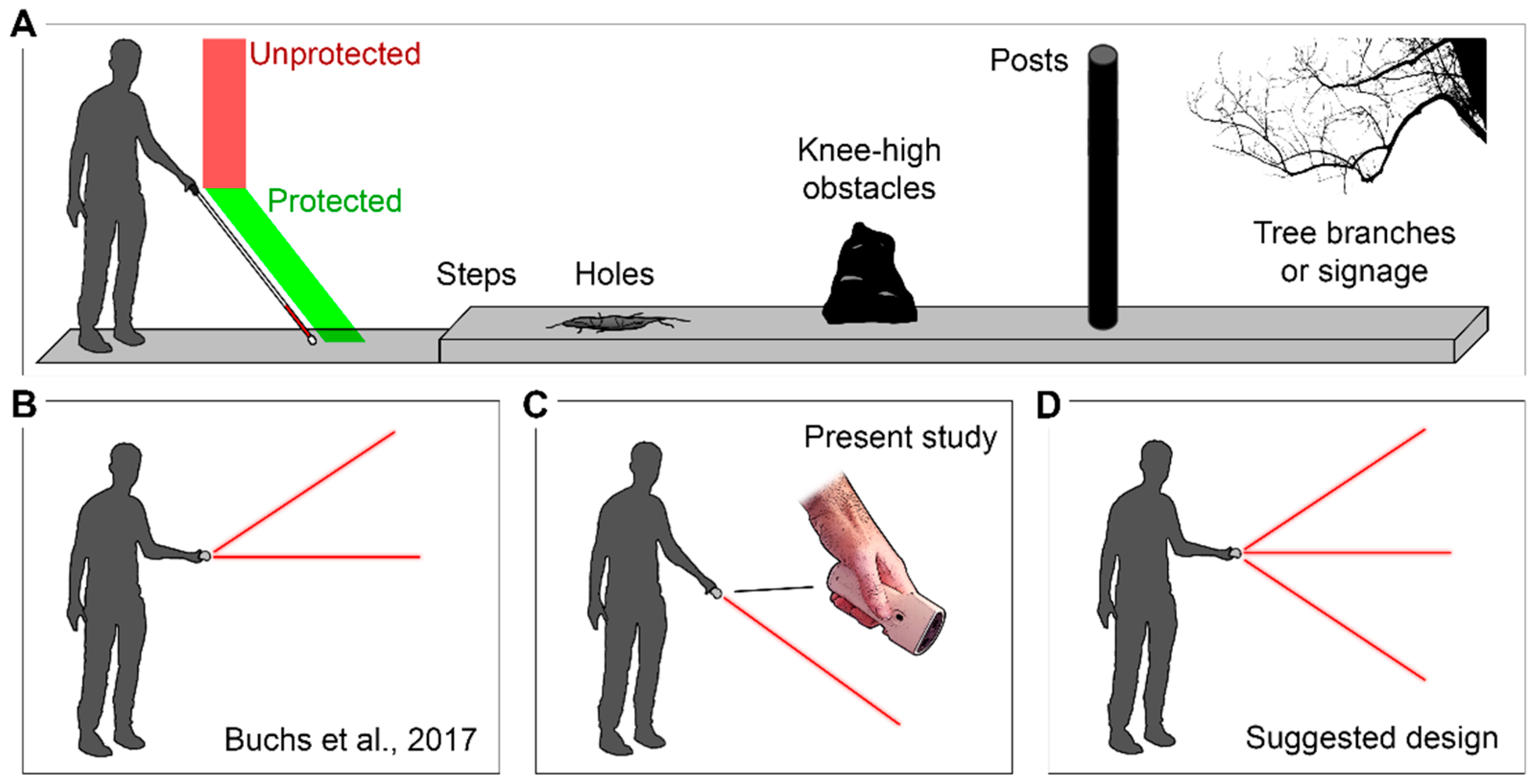
- Loss of physical contact with the ground. The white cane contact assures a high level of reliability in detecting ground obstacles and drop-offs such as curbs [49], and its replacement with the present downward sensor leads to less confidence in detecting drop-offs and ground obstacles.
- (2)
- Added complexity. While the EyeCane’s main advantage has always been its simplicity, ease of operation, and intuitive feedback, adding multiple sensors would add complexity and significantly increase the required training time. Indeed, a three-sensor design would necessitate feedback of a different nature (i.e., different modalities or frequency coding) for each sensor, as they each provide different spatial information that must be discriminated by the user.
- (3)
- User identification. As the white cane allows pedestrians and drivers to identify the blind user and to assure his/her safety [3], a three-sensor EyeCane might lead to the loss of user identification and impede safety.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schinazi, V.R.; Thrash, T.; Chebat, D.R. Spatial navigation by congenitally blind individuals. Wires Cogn. Sci. 2016, 7, 37–58. [Google Scholar] [CrossRef]
- Ptito, M.; Bleau, M.; Djerourou, I.; Paré, S.; Schneider, F.C.; Chebat, D.-R. Brain-Machine Interfaces to Assist the Blind. Front. Hum. Neurosci. 2021, 15, 638887. [Google Scholar] [CrossRef]
- Suterko, S. Long cane training: Its advantages and problems. In Proceedings of the Conference for Mobility Trainers and Technologists; Massachusetts Institute of Technology: Cambridge, MA, USA, 1967; pp. 13–18. [Google Scholar]
- Manduchi, R.; Kurniawan, S. Mobility-related accidents experienced by people with visual impairment. AER J. Res. Pract. Vis. Impair. Blind. 2011, 4, 44–54. [Google Scholar]
- Beggs, W. Coping, adjustment, and mobility-related feelings of newly visually impaired young adults. J. Vis. Impair. Blind. 1992, 86, 136–140. [Google Scholar] [CrossRef]
- Chebat, D.-R.; Harrar, V.; Kupers, R.; Maidenbaum, S.; Amedi, A.; Ptito, M. Sensory substitution and the neural correlates of navigation in blindness. In Mobility of Visually Impaired People; Springer: Berlin/Heidelberg, Germany, 2018; pp. 167–200. [Google Scholar]
- Kaczmarek, K.A. The tongue display unit (TDU) for electrotactile spatiotemporal pattern presentation. Sci. Iran. 2011, 18, 1476–1485. [Google Scholar] [CrossRef] [PubMed]
- Ptito, M.; Matteau, I.; Zhi Wang, A.; Paulson, O.B.; Siebner, H.R.; Kupers, R. Crossmodal Recruitment of the Ventral Visual Stream in Congenital Blindness. Neural Plast. 2012, 2012, 304045. [Google Scholar] [CrossRef] [PubMed]
- Matteau, I.; Kupers, R.; Ricciardi, E.; Pietrini, P.; Ptito, M. Beyond visual, aural and haptic movement perception: hMT+ is activated by electrotactile motion stimulation of the tongue in sighted and in congenitally blind individuals. Brain Res. Bull. 2010, 82, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Kupers, R.; Chebat, D.R.; Madsen, K.H.; Paulson, O.B.; Ptito, M. Neural correlates of virtual route recognition in congenital blindness. Proc. Natl. Acad. Sci. USA 2010, 107, 12716–12721. [Google Scholar] [CrossRef]
- Pamir, Z.; Canoluk, M.U.; Jung, J.-H.; Peli, E. Poor resolution at the back of the tongue is the bottleneck for spatial pattern recognition. Sci. Rep. 2020, 10, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Richardson, M.L.; Lloyd-Esenkaya, T.; Petrini, K.; Proulx, M.J. Reading with the Tongue: Individual Differences Affect the Perception of Ambiguous Stimuli with the BrainPort. In Proceedings of the 2020 CHI Conference on Human Factors in Computing Systems, Honolulu, HI, USA, 25–30 April 2020; pp. 1–10. [Google Scholar]
- Chebat, D.R.; Schneider, F.C.; Kupers, R.; Ptito, M. Navigation with a sensory substitution device in congenitally blind individuals. Neuroreport 2011, 22, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Elli, G.V.; Benetti, S.; Collignon, O. Is there a future for sensory substitution outside academic laboratories? Multisens. Res. 2014, 27, 271–291. [Google Scholar] [CrossRef]
- Pissaloux, E.; Velázquez, R. On spatial cognition and mobility strategies. In Mobility of Visually Impaired People; Springer: Berlin/Heidelberg, Germany, 2018; pp. 137–166. [Google Scholar]
- Islam, M.M.; Sadi, M.S.; Zamli, K.Z.; Ahmed, M.M. Developing walking assistants for visually impaired people: A review. IEEE Sens. J. 2019, 19, 2814–2828. [Google Scholar] [CrossRef]
- Cardillo, E.; Caddemi, A. Insight on electronic travel aids for visually impaired people: A review on the electromagnetic technology. Electronics 2019, 8, 1281. [Google Scholar] [CrossRef]
- Mattia, V.D.; Manfredi, G.; Leo, A.D.; Russo, P.; Scalise, L.; Cerri, G.; Caddemi, A.; Cardillo, E. A feasibility study of a compact radar system for autonomous walking of blind people. In Proceedings of the 2016 IEEE 2nd International Forum on Research and Technologies for Society and Industry Leveraging a Better Tomorrow (RTSI), Bologna, Italy, 7–9 September 2016; pp. 1–5. [Google Scholar]
- Islam, M.M.; Sadi, M.S.; Bräunl, T. Automated Walking Guide to Enhance the Mobility of Visually Impaired People. IEEE Trans. Med. Robot. Bionics 2020, 2, 485–496. [Google Scholar] [CrossRef]
- Hersh, M.; Johnson, M.A. Assistive Technology for Visually Impaired and Blind People; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Cardillo, E.; Mattia, V.D.; Manfredi, G.; Russo, P.; Leo, A.D.; Caddemi, A.; Cerri, G. An Electromagnetic Sensor Prototype to Assist Visually Impaired and Blind People in Autonomous Walking. IEEE Sens. J. 2018, 18, 2568–2576. [Google Scholar] [CrossRef]
- Maidenbaum, S.; Abboud, S.; Amedi, A. Sensory substitution: Closing the gap between basic research and widespread practical visual rehabilitation. Neurosci. Biobehav. Rev. 2014, 41, 3–15. [Google Scholar] [CrossRef]
- Maidenbaum, S.; Hanassy, S.; Abboud, S.; Buchs, G.; Chebat, D.R.; Levy-Tzedek, S.; Amedi, A. The “EyeCane”, a new electronic travel aid for the blind: Technology, behavior & swift learning. Restor. Neurol. Neurosci. 2014, 32, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Chebat, D.R.; Maidenbaum, S.; Amedi, A. Navigation using sensory substitution in real and virtual mazes. PLoS ONE 2015, 10, e126307. [Google Scholar] [CrossRef]
- Maidenbaum, S.; Levy-Tzedek, S.; Chebat, D.-R.; Amedi, A. Increasing Accessibility to the Blind of Virtual Environments, Using a Virtual Mobility Aid Based On the “EyeCane”: Feasibility Study. PLoS ONE 2013, 8, e72555. [Google Scholar] [CrossRef]
- Buchs, G.; Simon, N.; Maidenbaum, S.; Amedi, A. Waist-up protection for blind individuals using the EyeCane as a primary and secondary mobility aid. Restor. Neurol. Neurosci. 2017, 35, 225–235. [Google Scholar] [CrossRef]
- Meaidi, A.; Jennum, P.; Ptito, M.; Kupers, R. The sensory construction of dreams and nightmare frequency in congenitally blind and late blind individuals. Sleep Med. 2014, 15, 586–595. [Google Scholar] [CrossRef]
- Innet, S.; Ritnoom, N. An application of infrared sensors for electronic white stick. In Proceedings of the 2008 International Symposium on Intelligent Signal Processing and Communications Systems, Bangkok, Thailand, 8–11 February 2009; pp. 1–4. [Google Scholar]
- Chebat, D.-R.; Maidenbaum, S.; Amedi, A. The transfer of non-visual spatial knowledge between real and virtual mazes via sensory substitution. In Proceedings of the 2017 International Conference on Virtual Rehabilitation (ICVR), Montreal, QC, Canada, 19–22 June 2017; pp. 1–7. [Google Scholar]
- LaGrow, S.J. Improving Perception for Orientation and Mobility. In Foundations of Orientation and Mobility, 3rd ed.; Wiener, W.R., Welsh, R.L., Blasch, B.B., Eds.; American Foundation for the Blind Press: New York, NY, USA, 2010; Volume 2, pp. 3–26. [Google Scholar]
- La Grow, S.J.; Long, R. Orientation and Mobility: Techniques for Independence; Association for Education and Rehabilitation of the Blind and Visually Impaired: Alexandria, VA, USA, 2011. [Google Scholar]
- JASP Team. JASP (Version 0.14.1) [Computer Software]; JASP Team: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Hartcher-O’Brien, J.; Auvray, M. The Process of Distal Attribution Illuminated Through Studies of Sensory Substitution. Multisens. Res. 2014, 27, 421–441. [Google Scholar] [CrossRef]
- Kupers, R.; Ptito, M. Compensatory plasticity and cross-modal reorganization following early visual deprivation. Neurosci. Biobehav. Rev. 2014, 41, 36–52. [Google Scholar] [CrossRef]
- Paré, S.; Bleau, M.; Djerourou, I.; Malotaux, V.; Kupers, R.; Ptito, M. Spatial navigation with horizontally spatialized sounds in early and late blind individuals. PLoS ONE 2021, 16, e0247448. [Google Scholar] [CrossRef]
- Hoffmann, R.; Spagnol, S.; Kristjánsson, Á.; Unnthorsson, R. Evaluation of an audio-haptic sensory substitution device for enhancing spatial awareness for the visually impaired. Optom. Vis. Sci. 2018, 95, 757. [Google Scholar] [CrossRef]
- Stronks, H.C.; Nau, A.C.; Ibbotson, M.R.; Barnes, N. The role of visual deprivation and experience on the performance of sensory substitution devices. Brain Res. 2015, 1624, 140–152. [Google Scholar] [CrossRef]
- Iachini, T.; Ruggiero, G.; Ruotolo, F. Does blindness affect egocentric and allocentric frames of reference in small and large scale spaces? Behav. Brain Res. 2014, 273, 73–81. [Google Scholar] [CrossRef]
- Pasqualotto, A.; Spiller, M.J.; Jansari, A.S.; Proulx, M.J. Visual experience facilitates allocentric spatial representation. Behav. Brain Res. 2013, 236, 175–179. [Google Scholar] [CrossRef]
- Ptito, M.; Fumal, A.; de Noordhout, A.M.; Schoenen, J.; Gjedde, A.; Kupers, R. TMS of the occipital cortex induces tactile sensations in the fingers of blind Braille readers. Exp. Brain Res. 2008, 184, 193–200. [Google Scholar] [CrossRef]
- Goldreich, D.; Kanics, I.M. Performance of blind and sighted humans on a tactile grating detection task. Percept. Psychophys. 2006, 68, 1363–1371. [Google Scholar] [CrossRef]
- Stevens, J.C.; Foulke, E.; Patterson, M.Q. Tactile acuity, aging, and braille reading in long-term blindness. J. Exp. Psychol. Appl. 1996, 2, 91–106. [Google Scholar] [CrossRef]
- Gagnon, L.; Schneider, F.C.; Siebner, H.R.; Paulson, O.B.; Kupers, R.; Ptito, M. Activation of the hippocampal complex during tactile maze solving in congenitally blind subjects. Neuropsychologia 2012, 50, 1663–1671. [Google Scholar] [CrossRef]
- Chebat, D.R.; Schneider, F.C.; Ptito, M. Neural Networks Mediating Perceptual Learning in Congenital Blindness. Sci. Rep. 2020, 10, 495. [Google Scholar] [CrossRef]
- Chan, C.C.H.; Wong, A.W.K.; Ting, K.-H.; Whitfield-Gabrieli, S.; He, J.; Lee, T.M.C. Cross auditory-spatial learning in early-blind individuals. Hum. Brain Mapp. 2012, 33, 2714–2727. [Google Scholar] [CrossRef]
- Reislev, N.H.; Dyrby, T.B.; Siebner, H.R.; Lundell, H.; Ptito, M.; Kupers, R. Thalamocortical Connectivity and Microstructural Changes in Congenital and Late Blindness. Neural Plast. 2017, 2017, 9807512. [Google Scholar] [CrossRef]
- Sadato, N.; Pascual-Leone, A.; Grafman, J.; Ibañez, V.; Deiber, M.-P.; Dold, G.; Hallett, M. Activation of the primary visual cortex by Braille reading in blind subjects. Nature 1996, 380, 526–528. [Google Scholar] [CrossRef] [PubMed]
- Ptito, M.; Moesgaard, S.M.; Gjedde, A.; Kupers, R. Cross-modal plasticity revealed by electrotactile stimulation of the tongue in the congenitally blind. Brain 2005, 128, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Blasch, B.; LaGrow, S.J.; De l’Aune, W. Three aspects of coverage provided by the long cane: Object, surface, and foot-placement preview. J. Vis. Impair. Blind. 1996, 90, 295–301. [Google Scholar] [CrossRef]
- Buchs, G.; Maidenbaum, S.; Amedi, A. Obstacle identification and avoidance using the ‘EyeCane’: A tactile sensory substitution device for blind individuals. In Proceedings of the International Conference on Human Haptic Sensing and Touch Enabled Computer Applications, Versailles, France, 24–26 June 2014; pp. 96–103. [Google Scholar]
- Hoyle, B.; Waters, D. Mobility AT: The Batcane (UltraCane). In Assistive Technology for Visually Impaired and Blind People; Hersh, M.A., Johnson, M.A., Eds.; Springer London: London, UK, 2008; pp. 209–229. [Google Scholar]
- WeWALK. WeWALK Smart Cane. Available online: https://wewalk.io/en/ (accessed on 11 April 2021).
- Li, K. Electronic Travel Aids for Blind Guidance—An Industry Landscape Study; ECS: Berkeley, CA, USA, 2015. [Google Scholar]
- Phillips, B.; Zhao, H. Predictors of assistive technology abandonment. Assist. Technol. 1993, 5, 36–45. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Age | Sex | Age of Onset of Blindness | Blindness Duration Index | Cause of Blindness | Residual Perception |
|---|---|---|---|---|---|---|
| LB1 | 55 | F 1 | 24 | 0.56 | Retinitis pigmentosa | yes |
| LB2 | 25 | M 2 | 17 | 0.32 | Retinitis pigmentosa | - |
| LB3 | 70 | M | 38 | 0.46 | Meningitis | - |
| LB4 | 38 | F | 20 | 0.64 | Retinal cancer | - |
| LB5 | 46 | M | 40 | 0.13 | Meningitis | - |
| LB6 | 56 | F | 20 | 0.47 | Retinal cancer | - |
| LB7 | 47 | F | 22 | 0.53 | Diabetic retinopathy | - |
| LB8 | 44 | F | 17 | 0.61 | Glaucoma | - |
| LB9 | 59 | F | 57 | 0.03 | Retinitis pigmentosa | yes |
| EB1 | 48 | M | Perinatal | - | Retinopathy of prematurity | - |
| EB2 | 33 | M | Perinatal | - | Retinopathy of prematurity | - |
| EB3 | 63 | M | Perinatal | - | Retinopathy of prematurity | - |
| EB4 | 54 | M | Perinatal | - | Retinopathy of prematurity | - |
| EB5 | 56 | M | Perinatal | - | Retinopathy of prematurity | - |
| EB6 | 36 | M | Perinatal | - | Retinopathy of prematurity | - |
| EB7 | 31 | M | Perinatal | - | Retinopathy of prematurity | - |
| EB8 | 40 | M | Perinatal | - | Retinopathy of prematurity | - |
| EB9 | 33 | F | Perinatal | - | Retinopathy of prematurity | - |
| EB10 | 51 | M | Perinatal | - | Meningitis | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bleau, M.; Paré, S.; Djerourou, I.; Chebat, D.R.; Kupers, R.; Ptito, M. Blindness and the Reliability of Downwards Sensors to Avoid Obstacles: A Study with the EyeCane. Sensors 2021, 21, 2700. https://doi.org/10.3390/s21082700
Bleau M, Paré S, Djerourou I, Chebat DR, Kupers R, Ptito M. Blindness and the Reliability of Downwards Sensors to Avoid Obstacles: A Study with the EyeCane. Sensors. 2021; 21(8):2700. https://doi.org/10.3390/s21082700
Chicago/Turabian StyleBleau, Maxime, Samuel Paré, Ismaël Djerourou, Daniel R. Chebat, Ron Kupers, and Maurice Ptito. 2021. "Blindness and the Reliability of Downwards Sensors to Avoid Obstacles: A Study with the EyeCane" Sensors 21, no. 8: 2700. https://doi.org/10.3390/s21082700
APA StyleBleau, M., Paré, S., Djerourou, I., Chebat, D. R., Kupers, R., & Ptito, M. (2021). Blindness and the Reliability of Downwards Sensors to Avoid Obstacles: A Study with the EyeCane. Sensors, 21(8), 2700. https://doi.org/10.3390/s21082700