
Detection and Classification of Stroke Gaits by Deep Neural Networks Employing Inertial Measurement Units

 ,
,  ,
,
Abstract
1. Introduction
- (1)
- (2)
- The circumduction gait [18,19,20,21,22,23]: This gait is also known as the neurological or hemiplegia gait. The knee and hip movements are insufficient to allow the foot to clear the ground, so the patients adopt an abnormal walking pattern by taking the leg away from the body and swinging the leg forward in a semicircular fashion when walking.
- (3)
- (4)
- The back knee gait [26,27,28,29]: This gait is also known as genu recurvatum, which is defined as full extension or hyperextension of the knee in the stance phase [27]. Genu recurvatum can lead to functional mobility limitations and early degenerative changes of knee joint due to progressive knee hyperextension [28].
2. Collection and Processing
3. Deep Neural Network Model
- (1)
- The Activation Function: The neural network applied nonlinear activation functions in neurons. We selected the rectified linear unit (ReLU) [39], as shown in Figure 5a, as the activation function for the hidden layers:where z is the neuron input and ReLU(z) is the neuron output. This function can effectively overcome the vanishing gradient problem when updating the model parameters by back propagation [40]. The neural network would not continue training when the learning gradient is small. Moreover, the computing load is reduced because the function judges whether the input is greater than 0. That is, the ReLU function is a complete transfer for positive gradients with a derivative of 1. If the input , then ReLU(z) = 0 and this neuron is directly deleted, thereby achieving a reduction in neurons and allowing rapid convergence.Conversely, we selected the following sigmoid function [41] as the activation function of the output layers:where z is the neuron input and is the neuron output. The sigmoid function converts a scalar number to [0, 1], as shown in Figure 5b. If is greater than a threshold of 0.5, it is considered to belong to the labelled category. The sigmoid function is the optimized fitting function of the binary classification problem, where its output corresponds to the loss function mentioned in the next section. Because the probability of each label is independent, the sigmoid function is usually used as the activation function of the output layer for multi-label classification.
- (2)
- The Loss Function: The loss function is applied to evaluate how well the algorithms interpret the given data. This function evaluates the loss of the model and updates the weights to reduce the loss on the next evaluation. We applied the following cross-entropy [42] as the loss function:where is the distribution of the true output and is the distribution of the predicted output. Cross entropy can measure and quantify the similarity between and . In addition, it can help to avoid learning rate decreases in the gradient descent [43] by simultaneously applying the cross-entropy as the loss function and the sigmoid function as the activation function to the output layer.
- (3)
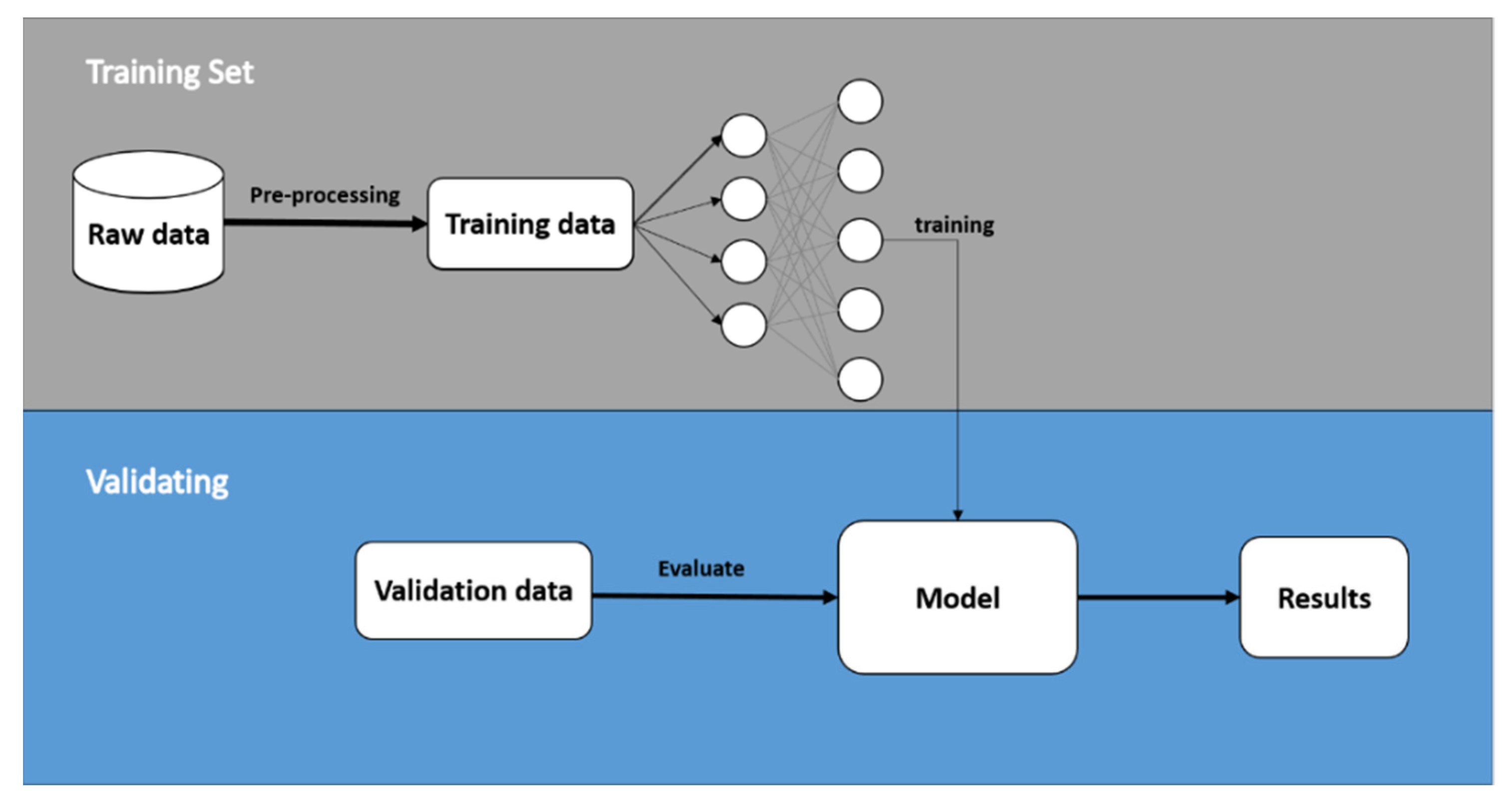
4. Model Training and Validation
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B




Appendix C
Appendix D

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stroke Subject | ||||||||
|---|---|---|---|---|---|---|---|---|
| Subject | Gender | Age | Height (cm) | Weight (kg) | Paretic Side | MMSE (Score) | BS (Stage) | FAC (Stage) |
| Sv1 | Male | 41 | 171 | 70 | left | 30 | 4 | 6 |
| Sv2 | Female | 50 | 155 | 52 | left | 30 | 3 | 6 |
References
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 20 January 2020).
- Hall, M.J.; Levant, S.; DeFrances, C.J. Hospitalization for stroke in US hospitals, 1989–2009. Diabetes 2012, 95, 1–8. [Google Scholar]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; De Ferranti, S.; Després, J.-P.; Fullerton, H.J.; Howard, V.J.; et al. Executive Summary: Heart Disease and Stroke Statistics—2015 Update: A report from the American Heart Association. Circulation 2015, 131, 434–441. [Google Scholar] [CrossRef]
- Jørgensen, H.S.; Nakayama, H.; Raaschou, H.O.; Olsen, T.S. Recovery of walking function in stroke patients: The copenhagen stroke study. Arch. Phys. Med. Rehabil. 1995, 76, 27–32. [Google Scholar] [CrossRef]
- Chen, G.; Patten, C.; Kothari, D.H.; Zajac, F.E. Gait differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds. Gait Posture 2005, 22, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, H.T.; Van Limbeek, J.; Geurts, A.C.; Zwarts, M.J. Motor recovery after stroke: A systematic review of the literature. Arch. Phys. Med. Rehabil. 2002, 83, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Wang, Z.; Qiu, S.; Wang, J.; Xu, F.; Wang, Z.; Shen, Y. Adaptive gait detection based on foot-mounted inertial sensors and multi-sensor fusion. Inf. Fusion 2019, 52, 157–166. [Google Scholar] [CrossRef]
- Wang, F.-C.; Li, Y.-C.; Wu, K.-L.; Chen, P.-Y.; Fu, L.-C. Online Gait Detection with an Automatic Mobile Trainer Inspired by Neuro-Developmental Treatment. Sensors 2020, 20, 3389. [Google Scholar] [CrossRef] [PubMed]
- Knutsson, E.; Richards, C. Different Types of Disturbed Motor Control in Gait of Hemiparetic Patients. Brain 1979, 102, 405–430. [Google Scholar] [CrossRef]
- Wong, A.M.; Pei, Y.-C.; Hong, W.-H.; Chung, C.-Y.; Lau, Y.-C.; Chen, C.P. Foot contact pattern analysis in hemiplegic stroke patients: An implication for neurologic status determination. Arch. Phys. Med. Rehabil. 2004, 85, 1625–1630. [Google Scholar] [CrossRef]
- Wahid, F.; Begg, R.K.; Hass, C.J.; Halgamuge, S.; Ackland, D.C. Classification of Parkinson’s Disease Gait Using Spatial-Temporal Gait Features. IEEE J. Biomed. Health Inform. 2015, 19, 1794–1802. [Google Scholar] [CrossRef] [PubMed]
- Daliri, M.R. Chi-square distance kernel of the gaits for the diagnosis of Parkinson’s disease. Biomed. Signal Process. Control. 2013, 8, 66–70. [Google Scholar] [CrossRef]
- Dolatabadi, E.; Taati, B.; Mihailidis, A. An Automated Classification of Pathological Gait Using Unobtrusive Sensing Technology. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 2336–2346. [Google Scholar] [CrossRef]
- Li, M.; Tian, S.; Sun, L.; Chen, X. Gait Analysis for Post-Stroke Hemiparetic Patient by Multi-Features Fusion Method. Sensors 2019, 19, 1737. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.D. Foot drop: Where, why and what to do? Pr. Neurol. 2008, 8, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Pramod Kerkar, M.D.; Ffarcsi, D.A. Foot Drop: Symptoms, Treatment, Exercises, Recovery. Available online: https://www.epainassist.com/sports-injuries/foot-and-heel-injuries/foot-drop (accessed on 16 January 2021).
- Mayo Clinic. Drop Foot. Available online: https://www.mayoclinic.org/diseases-conditions/foot-drop/diagnosis-treatment/drc-20372633 (accessed on 16 January 2021).
- Kerrigan, D.C.; Frates, E.P.; Rogan, S.; Riley, P.O. Hip Hiking and Circumduction: Quantitative definitions. Am. J. Phys. Med. Rehabil. 2000, 79, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Crisostomo, P.R.; Wang, M.; Herring, C.M.; Markel, T.A.; Meldrum, K.K.; Lillemoe, K.D.; Meldrum, D.R. Gender differences in injury induced mesenchymal stem cell apoptosis and VEGF, TNF, IL-6 expression: Role of the 55 kDa TNF receptor (TNFR1). J. Mol. Cell. Cardiol. 2007, 42, 142–149. [Google Scholar] [CrossRef]
- Paci, M. Physiotherapy Based on The Bobath Concept for Adults with Post-Stroke Hemiplegia: A Review of Effectiveness Studies. J. Rehabil. Med. 2003, 35, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Ouellette, M.M.; Lebrasseur, N.K.; Bean, J.F.; Phillips, E.; Stein, J.; Frontera, W.R.; Fielding, R.A. High-Intensity Resistance Training Improves Muscle Strength, Self-Reported Function, and Disability in Long-Term Stroke Survivors. Stroke 2004, 35, 1404–1409. [Google Scholar] [CrossRef] [PubMed]
- Pohl, M.; Mehrholz, J.; Ritschel, C.; Rückriem, S. Speed-Dependent Treadmill Training in Ambulatory Hemiparetic Stroke Patients: A randomized controlled trial. Stroke 2002, 33, 553–558. [Google Scholar] [CrossRef]
- Salbach, N.M.; Mayo, N.E.; Wood-Dauphinee, S.; Hanley, J.A.; Richards, C.L.; Côté, R. A task-orientated intervention enhances walking distance and speed in the first year post stroke: A randomized controlled trial. Clin. Rehabil. 2004, 18, 509–519. [Google Scholar] [CrossRef]
- Eng, J.J.; Tang, P.F. Gait training strategies to optimize walking ability in people with stroke: A synthesis of the evidence. Expert Rev. Neurother. 2007, 7, 1417–1436. [Google Scholar] [CrossRef] [PubMed]
- Stanhope, V.A.; Knarr, B.A.; Reisman, D.S.; Higginson, J.S. Frontal plane compensatory strategies associated with self-selected walking speed in individuals post-stroke. Clin. Biomech. 2014, 29, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.E.; Matyas, T.A.; Bach, T.M.; Goldie, P.A. Electrogoniometric feedback: Its effect on genu recurvatum in stroke. Arch. Phys. Med. Rehabil. 1992, 73, 1147–1154. [Google Scholar] [PubMed]
- Bleyenheuft, C.; Hanson, P.; Deltombe, T. Treatment of genu recurvatum in hemiparetic adult patients: A systematic literature review. Ann. Phys. Rehabil. Med. 2010, 53, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.; Alghamdi, G.A.; Alghamdi, M.A.; Altowaijri, A.; Richardson, S. The relationship of lower limb muscle strength and knee joint hyperextension during the stance phase of gait in hemiparetic stroke patients. Physiother. Res. Int. 2012, 17, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Loudon, J.K.; Goist, H.L.; Loudon, K.L. Genu Recurvatum Syndrome. J. Orthop. Sports Phys. Ther. 1998, 27, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, H. The Brunnstrom Stages of Stroke Recovery. Saebo. Available online: https://www.saebo.com/the-stages-of-stroke-recovery/ (accessed on 16 January 2021).
- Holden, M.K.; Gill, K.M.; Magliozzi, M.R. Gait assessment for neurologically impaired patients: Standards for outcome assessment. Phys Ther. 1986, 66, 1530–1539. [Google Scholar] [CrossRef]
- Mungas, D. Iii-Office Mental Status Testing: A Practical Guide. Geriatrics 1991, 46, 54–58. [Google Scholar]
- National Taiwan University Hospital. Clinical Trial Center. Available online: https://www.ntuh.gov.tw/NCTRC/training/training.aspx (accessed on 16 January 2021).
- Díaz, S.; Stephenson, J.B.; Labrador, M.A. Use of Wearable Sensor Technology in Gait, Balance, and Range of Motion Analysis. Appl. Sci. 2019, 10, 234. [Google Scholar] [CrossRef]
- Nguyen, M.D.; Mun, K.R.; Jung, D.; Han, J.; Park, M.; Kim, J.; Kim, J. IMU-based spectrogram approach with deep convolutional neural networks for gait classification. In Proceedings of the 2020 IEEE International Conference on Consumer Electronics (ICCE), Las Vegas, NV, USA, 4–6 January 2020; pp. 1–6. [Google Scholar] [CrossRef]
- Apdm, Inc. Opal User Guide. Available online: https://www.apdm.com/ (accessed on 16 January 2021).
- Aminian, K.; Najafi, B.; Büla, C.; Leyvraz, P.-F.; Robert, P. Spatio-temporal parameters of gait measured by an ambulatory system using miniature gyroscopes. J. Biomech. 2002, 35, 689–699. [Google Scholar] [CrossRef]
- EpoMedicine. Physical Examination: Gait. Available online: http://epomedicine.com/clinical-medicine/physical-examination-gait/ (accessed on 16 January 2021).
- Nair, V.; Hinton, G.E. Rectified linear units improve restricted boltzmann machines. In Proceedings of the 27th International Conference on Machine Learning (ICML), Haifa, Israel, 21–24 June 2010; pp. 807–814. Available online: https://www.cs.toronto.edu/~fritz/absps/reluICML.pdf (accessed on 16 January 2021).
- Pascanu, R.; Mikolov, T.; Bengio, Y. Understanding the exploding gradient problem. Comput. Sci. 2012, 1–11. Available online: https://arxiv.org/pdf/1211.5063v1.pdf (accessed on 16 January 2021).
- Han, J.; Moraga, C. The influence of the sigmoid function parameters on the speed of backpropagation learning. In International Workshop on Artificial Neural Networks; Springer: Berlin/Heidelberg, Germany, 1995; pp. 195–201. [Google Scholar] [CrossRef]
- De Boer, P.-T.; Kroese, D.P.; Mannor, S.; Rubinstein, R.Y. A Tutorial on the Cross-Entropy Method. Ann. Oper. Res. 2005, 134, 19–67. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Kingma, D.P.; Ba, J. Adam: A Method for Stochastic Optimization. Available online: https://arxiv.org/pdf/1412.6980.pdf (accessed on 16 January 2021).
- Duchi, J.; Hazan, E.; Singer, Y. Adaptive subgradient methods for online learning and stochastic optimization. J. Mach. Learn. Res. 2011, 12, 2121–2159. [Google Scholar]
- Hinton, G.; Srivastava, N.; Swersky, K. Neural Networks for Machine Learning. Available online: https://www.cs.toronto.edu/~tijmen/csc321/slides/lecture_slides_lec6.pdf (accessed on 16 January 2021).
- Kohavi, R. A study of cross-validation and bootstrap for accuracy estimation and model selection. In Proceedings of the 14th International Joint Conference on Artificial Intelligence (IJCAI), Montreal, QC, Canada, 20–25 August 1995; pp. 1137–1145. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Powers, D.M. Evaluation: From Precision, Recall and F-Measure to ROC, Informedness, Markedness and Correlation. 2011. Available online: https://arxiv.org/abs/2010.16061 (accessed on 16 January 2021).
- Reiss, A.; Stricker, D. Introducing a new benchmarked dataset for activity monitoring. In Proceedings of the 16th International Symposium on Wearable Computers 2012, Newcastle, UK, 18–22 June 2012; pp. 108–109. [Google Scholar]
- UCI Machine Learning Repository. Available online: http://archive.ics.uci.edu/ml/datasets/PAMAP2+Physical+Activity+Monitoring (accessed on 16 January 2021).






| Stroke Subject | ||||||||
|---|---|---|---|---|---|---|---|---|
| Subject | Gender | Age | Height (cm) | Weight (kg) | Paretic Side | MMSE (Score) | BS (Stage) | FAC (Stage) |
| P1 | Male | 51 | 174 | 66 | Right | 30 | 3 | 6 |
| P2 | Male | 48 | 168 | 61 | Right | 28 | 3 | 6 |
| P3 | Female | 61 | 161 | 56 | Right | 29 | 4 | 6 |
| P4 | Male | 53 | 162 | 75 | Left | 29 | 3 | 6 |
| P5 | Male | 52 | 173 | 81 | Right | 27 | 3 | 6 |
| P6 | Male | 72 | 168 | 75 | Left | 29 | 5 | 6 |
| P7 | Male | 64 | 158 | 61 | Left | 30 | 5 | 6 |
| P8 | Female | 69 | 156 | 90 | Right | 30 | 4 | 6 |
| Healthy Subject | ||||
|---|---|---|---|---|
| Subject | Gender | Age | Height (cm) | Weight (kg) |
| H1 | Male | 24 | 185 | 85 |
| H2 | Male | 24 | 178 | 70 |
| H3 | Male | 25 | 170 | 63 |
| H4 | Male | 25 | 164 | 70 |
| H5 | Male | 24 | 172 | 75 |
| H6 | Male | 26 | 172 | 76 |
| H7 | Male | 23 | 166 | 62 |
| Subject | Number of Gaits | NG | SG | SGwDF | SGwC | SGwHH | SGwBK | |
|---|---|---|---|---|---|---|---|---|
| P1 | left | 50 | 0 | 1 | 0 | 0 | 0 | 0 |
| right | 39 | 0 | 1 | 0 | 0 | 1 | 1 | |
| P2 | left | 68 | 0 | 1 | 0 | 0 | 0 | 0 |
| right | 52 | 0 | 1 | 1 | 0 | 1 | 0 | |
| P3 | left | 92 | 0 | 1 | 0 | 0 | 0 | 0 |
| right | 76 | 0 | 1 | 0 | 1 | 0 | 0 | |
| P4 | left | 187 | 0 | 1 | 0 | 1 | 1 | 1 |
| right | 190 | 0 | 1 | 0 | 0 | 0 | 0 | |
| P5 | left | 169 | 0 | 1 | 0 | 0 | 0 | 0 |
| right | 158 | 0 | 1 | 1 | 1 | 1 | 1 | |
| P6 | left | 158 | 0 | 1 | 1 | 0 | 0 | 1 |
| right | 171 | 0 | 1 | 0 | 0 | 0 | 0 | |
| P7 | left | 139 | 0 | 1 | 0 | 0 | 1 | 0 |
| right | 158 | 0 | 1 | 0 | 0 | 0 | 0 | |
| P8 | left | 155 | 0 | 1 | 0 | 0 | 0 | 0 |
| right | 175 | 0 | 1 | 1 | 0 | 1 | 0 | |
| Healthy Subjects | left | 1000 | 1 | 0 | 0 | 0 | 0 | 0 |
| right | 1000 | 1 | 0 | 0 | 0 | 0 | 0 |
| Actual | |||
|---|---|---|---|
| Positive | Negative | ||
| Predicted | Positive | TP | FP |
| Negative | FN | TN | |
| Actual | Normal Gait | Stroke Gait | ||||
|---|---|---|---|---|---|---|
| Predicted | Positive | Negative | Positive | Negative | ||
| Model 1 | validation by Fold 1 | Positive | 496 | 3 | 497 | 5 |
| Negative | 4 | 497 | 3 | 495 | ||
| Model 2 | validation by Fold 2 | Positive | 495 | 2 | 500 | 8 |
| Negative | 5 | 498 | 0 | 492 | ||
| Model 3 | validation by Fold 3 | Positive | 498 | 2 | 497 | 2 |
| Negative | 2 | 498 | 3 | 498 | ||
| Model 4 | validation by Fold 4 | Positive | 496 | 3 | 497 | 3 |
| Negative | 4 | 497 | 3 | 497 | ||
| Actual | Stroke Gait | Drop Foot | Circumduction | Hip Hiking | Back Knee | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Predicted | P | N | P | N | P | N | P | N | P | N | |
| Model 1 | P | 497 | 5 | 77 | 5 | 77 | 0 | 154 | 10 | 105 | 8 |
| N | 0 | 0 | 2 | 418 | 20 | 405 | 17 | 321 | 21 | 368 | |
| Model 2 | P | 500 | 8 | 96 | 7 | 98 | 11 | 178 | 14 | 112 | 5 |
| N | 0 | 0 | 4 | 401 | 0 | 399 | 4 | 312 | 20 | 371 | |
| Model 3 | P | 497 | 2 | 101 | 4 | 113 | 2 | 197 | 5 | 131 | 8 |
| N | 0 | 0 | 6 | 388 | 4 | 380 | 10 | 287 | 1 | 359 | |
| Model 4 | P | 497 | 3 | 89 | 7 | 98 | 9 | 168 | 13 | 123 | 4 |
| N | 0 | 0 | 4 | 400 | 4 | 489 | 5 | 314 | 19 | 354 | |
| Detection | Classification | |||
|---|---|---|---|---|
| Accuracy | F1-Score | Accuracy | F1-Score | |
| Model 1 | 0.9925 | 0.9925 | 0.9649 | 0.9539 |
| Model 2 | 0.9925 | 0.9925 | 0.9717 | 0.9642 |
| Model 3 | 0.9955 | 0.9955 | 0.9831 | 0.9802 |
| Model 4 | 0.9935 | 0.9935 | 0.9728 | 0.9663 |
| Average | 0.9935 | 0.9935 | 0.9731 | 0.9662 |
| Actual | PAMAP2 Test | Sv1 and Sv2 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Predicted | P | N | Accuracy | F1-Score | P | N | Accuracy | F1-Score | |
| Model 1 | P | 1005 | 0 | 1 | 1 | 219 | 0 | 0.9909 | 0.9909 |
| N | 0 | 0 | 2 | 0 | |||||
| Model 2 | P | 1004 | 0 | 0.9990 | 0.9995 | 219 | 0 | 0.9909 | 0.9909 |
| N | 1 | 0 | 2 | 0 | |||||
| Model 3 | P | 1005 | 0 | 1 | 1 | 217 | 0 | 0.9819 | 0.9841 |
| N | 0 | 0 | 4 | 0 | |||||
| Model 4 | P | 1003 | 0 | 0.9980 | 0.9990 | 218 | 0 | 0.9864 | 0.9864 |
| N | 2 | 0 | 3 | 0 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, F.-C.; Chen, S.-F.; Lin, C.-H.; Shih, C.-J.; Lin, A.-C.; Yuan, W.; Li, Y.-C.; Kuo, T.-Y. Detection and Classification of Stroke Gaits by Deep Neural Networks Employing Inertial Measurement Units. Sensors 2021, 21, 1864. https://doi.org/10.3390/s21051864
Wang F-C, Chen S-F, Lin C-H, Shih C-J, Lin A-C, Yuan W, Li Y-C, Kuo T-Y. Detection and Classification of Stroke Gaits by Deep Neural Networks Employing Inertial Measurement Units. Sensors. 2021; 21(5):1864. https://doi.org/10.3390/s21051864
Chicago/Turabian StyleWang, Fu-Cheng, Szu-Fu Chen, Chin-Hsien Lin, Chih-Jen Shih, Ang-Chieh Lin, Wei Yuan, You-Chi Li, and Tien-Yun Kuo. 2021. "Detection and Classification of Stroke Gaits by Deep Neural Networks Employing Inertial Measurement Units" Sensors 21, no. 5: 1864. https://doi.org/10.3390/s21051864
APA StyleWang, F.-C., Chen, S.-F., Lin, C.-H., Shih, C.-J., Lin, A.-C., Yuan, W., Li, Y.-C., & Kuo, T.-Y. (2021). Detection and Classification of Stroke Gaits by Deep Neural Networks Employing Inertial Measurement Units. Sensors, 21(5), 1864. https://doi.org/10.3390/s21051864