
Validation of a Laser Ranged Scanner-Based Detection of Spatio-Temporal Gait Parameters Using the aTUG Chair

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
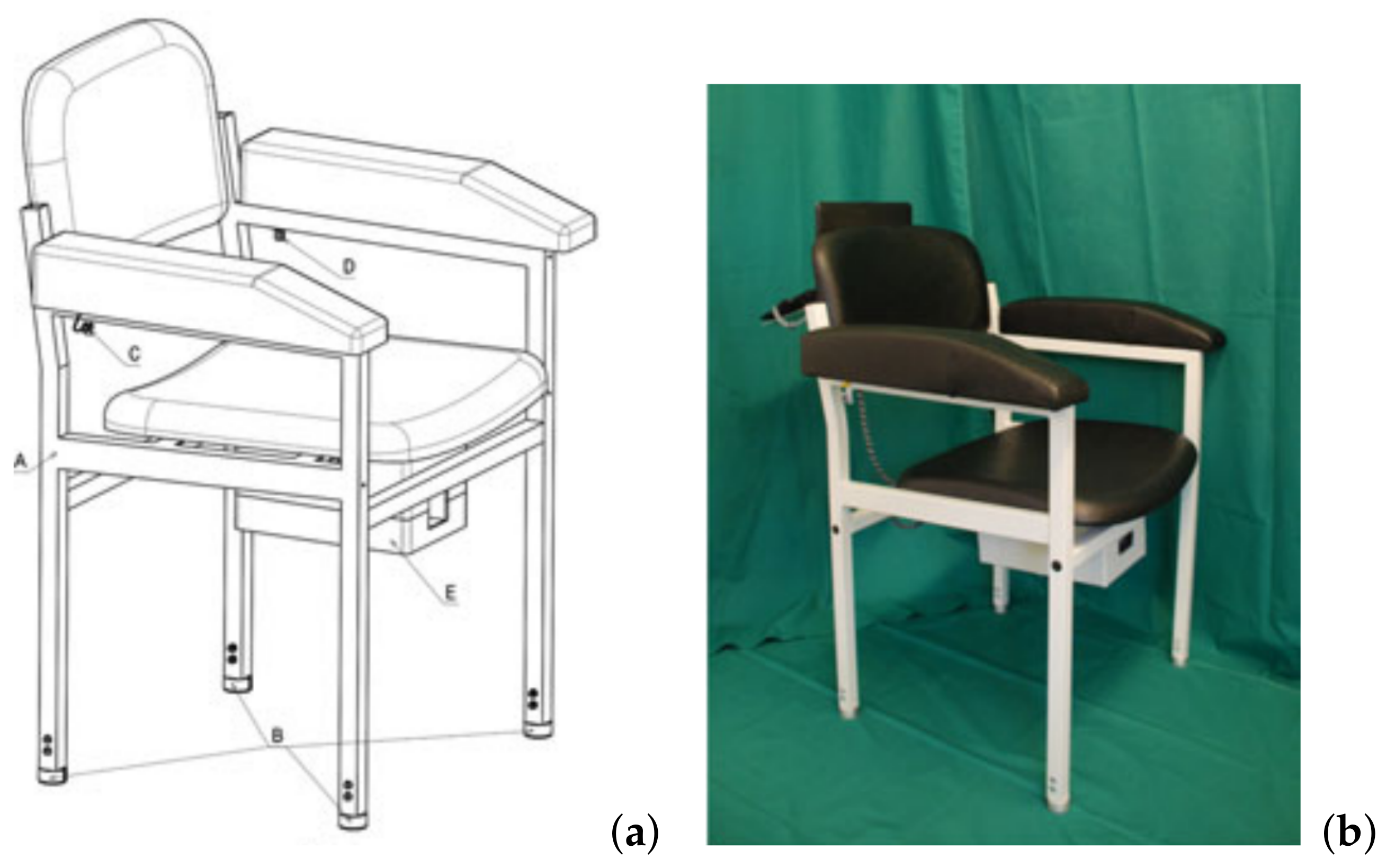
2.1. Composition of the aTUG Chair
2.2. Computation of aTUG Gait Parameters
2.3. Study Design and Recruitment
2.4. Measurements and Assessments
- The Berg Balance Scale (BBS) is a 14-item test battery for assessing balance and mobility in older people. Each item is rated between 0 and 4 points, leading to total of 0 to 56 points [56].
- The Tinetti Test (TT) [57] measures static and dynamic balance ability and consists of 20 items that are either rated dichotomous or on a scale between 0 and 2 points. The total score of the TT has a range between 0 and 28 points.
- The Activities-Specific Balance Confidence-(ABC)-Scale [58] consists of 16 items asking participants about their confidence in performing certain activities of daily living without losing their balance. While the original scale asked participants to rate their confidence for each item as a percentage value, Filatrault et al. (2007) established a simplified version of the ABC-scale with a 0–3-point-Likert scale, with 3 points representing a participant being “very confident” to maintain balance in a given task and 0 points being “not at all confident” [59]. In this study, we used the validated German version of the ABC scale [60] with the 4-point-Likert scale. For all additional tests, higher results represent better functional ability and less disability.
2.5. Data Pre-Processing and Statistical Analysis
3. Results
3.1. Study Sample
3.2. Statistical Evaluation
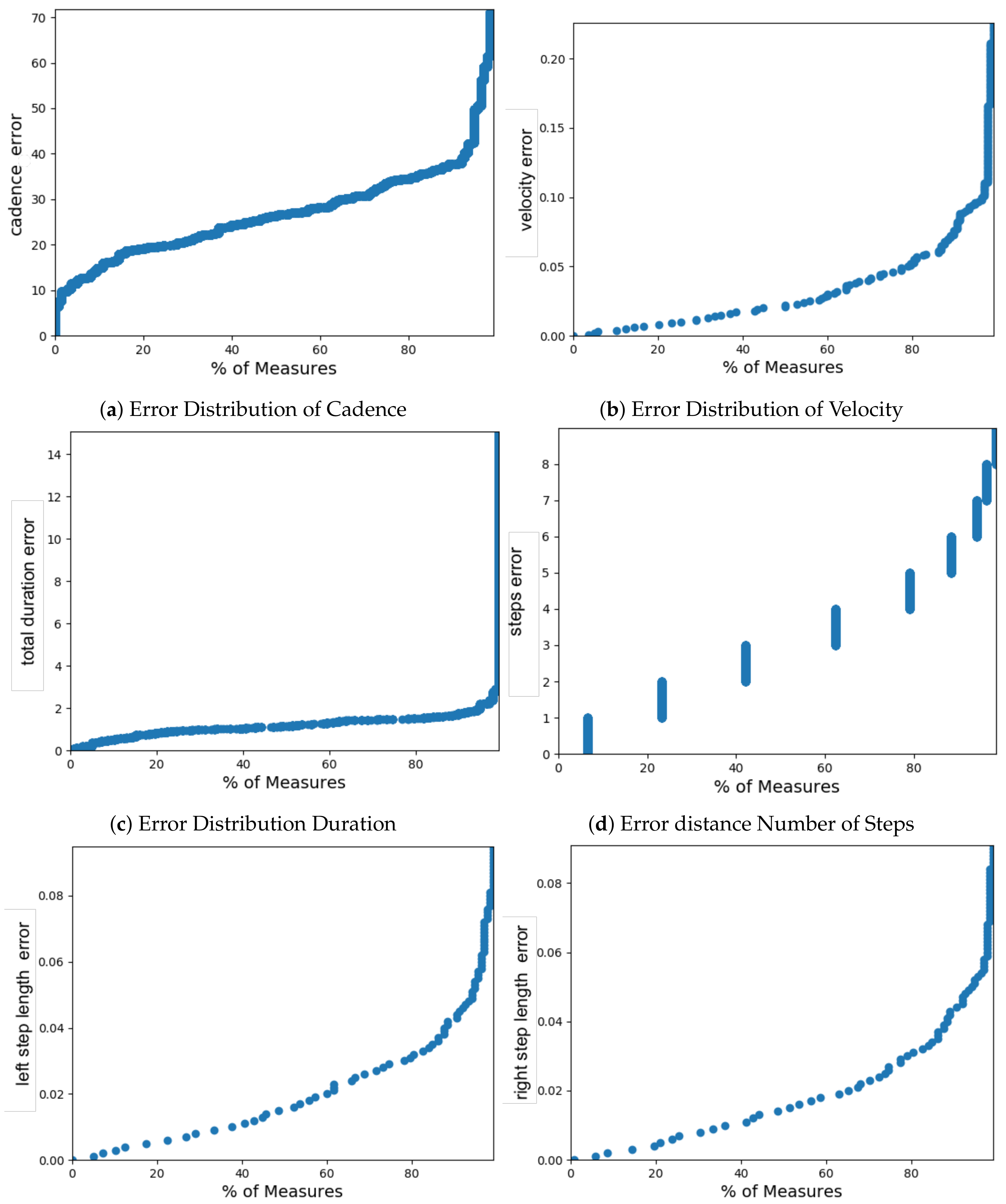
3.2.1. Sensitivity of Spatio-Temporal Gait Parameters of the aTUG chair
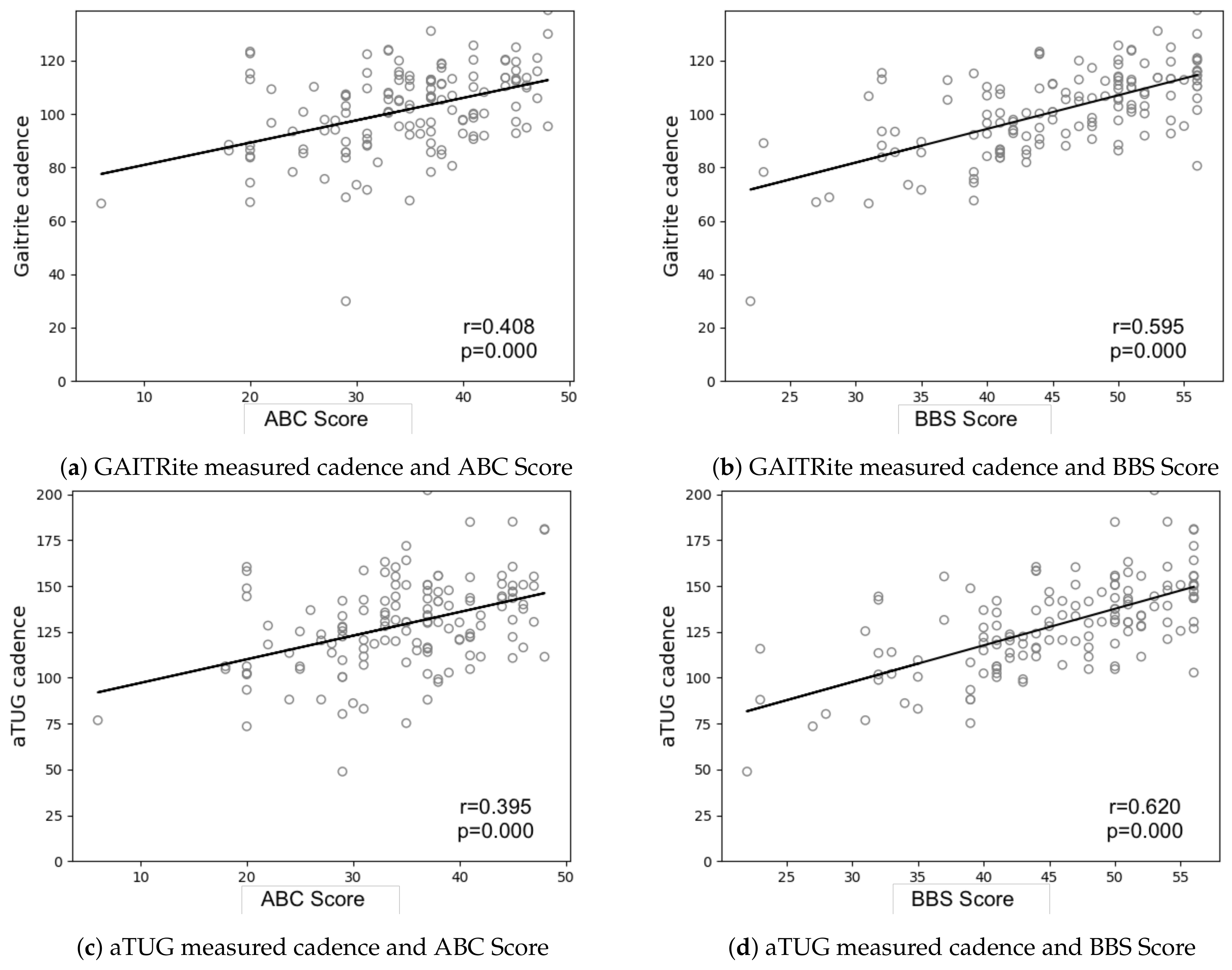
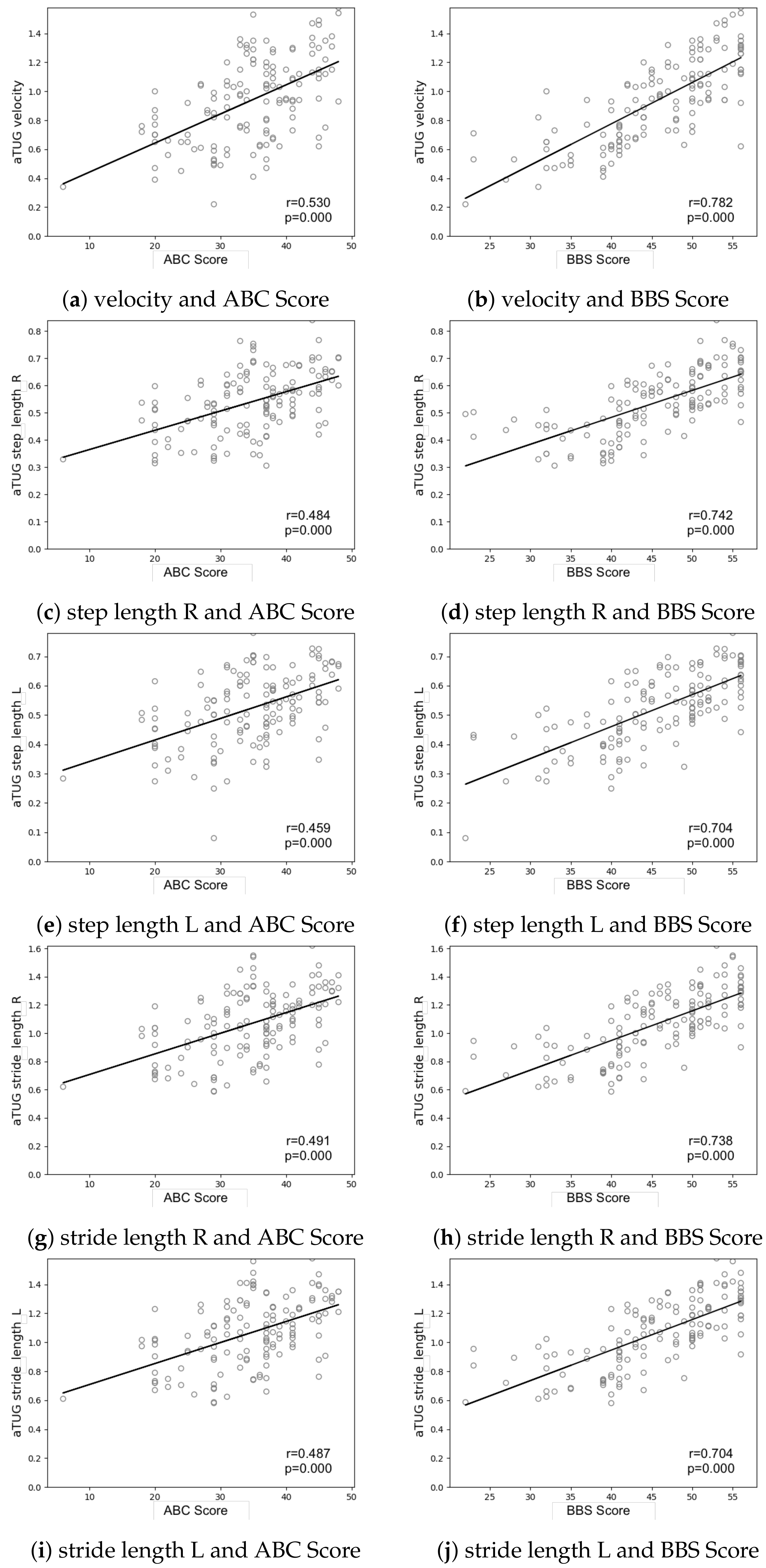
3.2.2. Influence of BBS and ABC Score on Spatio-Temporal Gait Parameters
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADL | activities of the daily living |
| aTUG | ambient TUG |
| CC | correlation coefficient |
| FS | force sensor |
| IQR | interquartile range |
| LB | light barrier |
| LRS | laser range-scanner |
| SD | standard deviation |
| TUG | Timed “Up & Go” |
References
- Ferrucci, L.; Cooper, R.; Shardell, M.; Simonsick, E.M.; Schrack, J.A.; Kuh, D. Age-Related Change in Mobility: Perspectives From Life Course Epidemiology and Geroscience. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1184–1194. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Larrañaga, A.; Vetrano, D.L.; Ferrucci, L.; Mercer, S.W.; Marengoni, A.; Onder, G.; Eriksdotter, M.; Fratiglioni, L. Multimorbidity and functional impairment-bidirectional interplay, synergistic effects and common pathways. J. Internal Med. 2018, 285, 255–271. [Google Scholar] [CrossRef]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Samaniego, L.L.; Rodríguez-Mañas, L.; Bernabei, R.; Graziano, O.; et al. Frailty and Multimorbidity: A Systematic Review and Meta-analysis. J. Gerontol. Ser. A 2018, 74, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Biol. Sci. Med. Sci. 2001, 56, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, S.A.; Schwartz, A.W.; Karunananthan, S.; Bergman, H.; Clarfield, A.M. The Identification of Frailty: A Systematic Literature Review. J. Am. Geriatr. Soc. 2011, 59, 2129–2138. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, J.; Neyens, J.C.; van Rossum, E.; Spreeuwenberg, M.D.; de Witte, L.P. Predicting ADL disability in community-dwelling elderly people using physical frailty indicators: A systematic review. BMC Geriatr. 2011, 11, 33. [Google Scholar] [CrossRef]
- van der Vorst, A.; het Veld, L.P.O.; Witte, N.D.; Schols, J.M.; Kempen, G.I.; Zijlstra, G.R. The impact of multidimensional frailty on dependency in activities of daily living and the moderating effects of protective factors. Arch. Gerontol. Geriatr. 2018, 78, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.E.; Phillips, L.H.; Cooper, C.L.; Gray, S.; Allan, J.L. Effect of Different Types of Physical Activity on Activities of Daily Living in Older Adults: Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2017, 25, 653–670. [Google Scholar] [CrossRef]
- Fallah, N.; Mitnitski, A.; Searle, S.D.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. Transitions in Frailty Status in Older Adults in Relation to Mobility: A Multistate Modeling Approach Employing a Deficit Count. J. Am. Geriatr. Soc. 2011, 59, 524–529. [Google Scholar] [CrossRef]
- Hsieh, T.J.; Chang, H.Y.; Wu, I.C.; Chen, C.C.; Tsai, H.J.; Chiu, Y.F.; Chuang, S.C.; Hsiung, C.A.; Hsu, C.C. Independent association between subjective cognitive decline and frailty in the elderly. PLoS ONE 2018, 13, e0201351. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Jivraj, S.; Walters, K. Association between frailty and quality of life among community-dwelling older people: A systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Mulasso, A.; Roppolo, M.; Gobbens, R.J.; Rabaglietti, E. Mobility, balance and frailty in community-dwelling older adults: What is the best 1-year predictor of falls? Geriatr. Gerontol. Int. 2016, 17, 1463–1469. [Google Scholar] [CrossRef] [PubMed]
- Esbrí-Víctor, M.; Huedo-Rodenas, I.; López-Utiel, M.; Navarro-López, J.L.; Martínez-Reig, M.; Serra-Rexach, J.A.; Romero-Rizos, L.; Abizanda, P. Frailty and Fear of Falling: The FISTAC Study. J. Frailty Aging (JFA) 2017, 6, 136–140. [Google Scholar] [CrossRef]
- Jefferis, B.J.; Iliffe, S.; Kendrick, D.; Kerse, N.; Trost, S.; Lennon, L.T.; Ash, S.; Sartini, C.; Morris, R.W.; Wannamethee, S.G.; et al. How are falls and fear of falling associated with objectively measured physical activity in a cohort of community-dwelling older men? BMC Geriatr. 2014, 14, 114. [Google Scholar] [CrossRef]
- Birkelbach, O.; Mörgeli, R.; Balzer, F.; Olbert, M.; Treskatsch, S.; Kiefmann, R.; Müller-Werdan, U.; Reisshauer, A.; Schwedtke, C.; Neuner, B.; et al. Warum und wie sollte ich Frailty erfassen?–ein Ansatz für die Anästhesieambulanz. AINS-Anästhesiol. Intensivmed. Notfallmed. Schmerzther. 2017, 52, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Watt, J.; Tricco, A.C.; Talbot-Hamon, C.; Pham, B.; Rios, P.; Grudniewicz, A.; Wong, C.; Sinclair, D.; Straus, S.E. Identifying older adults at risk of harm following elective surgery: A systematic review and meta-analysis. BMC Med. 2018, 16, 2. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Walters, K. Frailty index as a predictor of mortality: A systematic review and meta-analysis. Age Ageing 2017, 47, 193–200. [Google Scholar] [CrossRef]
- de Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials. BMC Geriatr. 2015, 15, 154. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Fairhall, N.; Wallbank, G.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S. Exercise for preventing falls in older people living in the community: An abridged Cochrane systematic review. Br. J. Sports Med. 2019, 54, 885–891. [Google Scholar] [CrossRef]
- Sherrington, C.; Fairhall, N.J.; Wallbank, G.K.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S.E. Exercise for preventing falls in older people living in the community. Cochr. Database Syst. Rev. 2019. [Google Scholar] [CrossRef] [PubMed]
- Buta, B.J.; Walston, J.D.; Godino, J.G.; Park, M.; Kalyani, R.R.; Xue, Q.L.; Bandeen-Roche, K.; Varadhan, R. Frailty assessment instruments: Systematic characterization of the uses and contexts of highly-cited instruments. Ageing Res. Rev. 2016, 26, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Kan, G.A.V.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.; Gillette-Guyonnet, S.; Inzitari, M.; et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef]
- Cesari, M.; Kritchevsky, S.B.; Penninx, B.W.H.J.; Nicklas, B.J.; Simonsick, E.M.; Newman, A.B.; Tylavsky, F.A.; Brach, J.S.; Satterfield, S.; Bauer, D.C.; et al. Prognostic Value of Usual Gait Speed in Well-Functioning Older Peopleâ Results from the Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2005, 53, 1675–1680. [Google Scholar] [CrossRef]
- Clegg, A.; Rogers, L.; Young, J. Diagnostic test accuracy of simple instruments for identifying frailty in community-dwelling older people: A systematic review. Age Ageing 2014, 44, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Thaler-Kall, K.; Peters, A.; Thorand, B.; Grill, E.; Autenrieth, C.S.; Horsch, A.; Meisinger, C. Description of spatio-temporal gait parameters in elderly people and their association with history of falls: Results of the population-based cross-sectional KORA-Age study. BMC Geriatr. 2015, 15, 32. [Google Scholar] [CrossRef]
- Kirkwood, R.N.; Borém, I.L.; Sampaio, R.F.; Ferreira, V.K.G.; de Almeida, J.C.; Guimarães, S.B.B.; de Souza Moreira, B. Frailty Status and Gait Parameters of Older Women with Type 2 Diabetes. Can. J. Diabetes 2019, 43, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Turner, G.; Clegg, A. Best practice guidelines for the management of frailty: A British Geriatrics Society, Age UK and Royal College of General Practitioners report. Age Ageing 2014, 43, 744–747. [Google Scholar] [CrossRef]
- Chow, W.B.; Rosenthal, R.A.; Merkow, R.P.; Ko, C.Y.; Esnaola, N.F. Optimal Preoperative Assessment of the Geriatric Surgical Patient: A Best Practices Guideline from the American College of Surgeons National Surgical Quality Improvement Program and the American Geriatrics Society. J. Am. Coll. Surg. 2012, 215, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Eagles, D.; Perry, J.J.; Sirois, M.J.; Lang, E.; Daoust, R.; Lee, J.; Griffith, L.; Wilding, L.; Neveu, X.; Emond, M. Timed Up and Go predicts functional decline in older patients presenting to the emergency department following minor trauma. Age Ageing 2016, 46, 214–218. [Google Scholar] [CrossRef]
- Robinson, T.N.; Wu, D.S.; Pointer, L.; Dunn, C.L.; Cleveland, J.C.; Moss, M. Simple frailty score predicts postoperative complications across surgical specialties. Am. J. Surg. 2013, 206, 544–550. [Google Scholar] [CrossRef]
- Botolfsen, P.; Helbostad, J.L.; Moe-nilssen, R.; Wall, J.C. Reliability and concurrent validity of the Expanded Timed Up-and-Go test in older people with impaired mobility. Physiother. Res. Int. 2008, 13, 94–106. [Google Scholar] [CrossRef]
- Sprint, G.; Cook, D.J.; Weeks, D.L. Toward Automating Clinical Assessments: A Survey of the Timed Up and Go. IEEE Rev. Biomed. Eng. 2015, 8, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Hellmers, S.; Izadpanah, B.; Dasenbrock, L.; Diekmann, R.; Bauer, J.M.; Hein, A.; Fudickar, S. Towards an Automated Unsupervised Mobility Assessment for Older People Based on Inertial TUG Measurements. Sensors 2018, 18, 3310. [Google Scholar] [CrossRef]
- Sheehan, K.; Greene, B.; Cunningham, C.; Crosby, L.; Kenny, R. Early identification of declining balance in higher functioning older adults, an inertial sensor based method. Gait Posture 2014, 39, 1034–1039. [Google Scholar] [CrossRef]
- Fudickar, S.; Hellmers, S.; Lau, S.; Diekmann, R.; Bauer, J.M.; Hein, A. Measurement System for Unsupervised Standardized Assessment of Timed “Up & Go” and Five Times Sit to Stand Test in the Community—A Validity Study. Sensors 2020, 20, 2824. [Google Scholar] [CrossRef]
- Dubois, A.; Bihl, T.; Bresciani, J.P. Automating the Timed Up and Go Test Using a Depth Camera. Sensors 2017, 18, 14. [Google Scholar] [CrossRef] [PubMed]
- Dibble, L.E.; Lange, M. Predicting Falls In Individuals with Parkinson Disease. J. Neurol. Phys. Ther. 2006, 30, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Nakakubo, S.; Doi, T.; Makizako, H.; Tsutsumimoto, K.; Hotta, R.; Kurita, S.; Kim, M.; Suzuki, T.; Shimada, H. Association of walk ratio during normal gait speed and fall in community-dwelling elderly people. Gait Posture 2018, 66, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Molinero, A.; Herrero-Larrea, A.; Miñarro, A.; Narvaiza, L.; Gálvez-Barrón, C.; León, N.G.; Valldosera, E.; de Mingo, E.; Macho, O.; Aivar, D.; et al. The spatial parameters of gait and their association with falls, functional decline and death in older adults: A prospective study. Sci. Rep. 2019, 9, 8813. [Google Scholar] [CrossRef]
- Fankhauser, P.; Bloesch, M.; Rodriguez, D.; Kaestner, R.; Hutter, M.; Siegwart, R. Kinect v2 for Mobile Robot Navigation: Evaluation and Modeling. In Proceedings of the 2015 International Conference on Advanced Robotics (ICAR), Istanbul, Turkey, 27–31 July 2015. [Google Scholar] [CrossRef]
- Kiselev, J.; Haesner, M.; Gövercin, M.; Steinhagen-Thiessen, E. Implementation of a Home-Based Interactive Training System for Fall Prevention: Requirements and Challenges. J. Gerontol. Nurs. 2014, 41, 14–19. [Google Scholar] [CrossRef]
- Frenken, T.; Brell, M.; Gövercin, M.; Wegel, S.; Hein, A. aTUG: Technical apparatus for gait and balance analysis within component-based Timed Up & Go using mutual ambient sensors. J. Ambient Intell. Humaniz. Comput. 2012, 4, 759–778. [Google Scholar] [CrossRef]
- Frenken, T.; Lohmann, O.; Frenken, M.; Steen, E.E.; Hein, A. Performing gait analysis within the timed up & go assessment test: Comparison of aTUG to a marker-based tracking system. Inform. Health Soc. Care 2014, 39, 232–248. [Google Scholar] [CrossRef]
- Fudickar, S.; Kiselev, J.; Frenken, T.; Wegel, S.; Dimitrowska, S.; Steinhagen-Thiessen, E.; Hein, A. Validation of the ambient TUG chair with light barriers and force sensors in a clinical trial. Assist. Technol. 2017, 32. [Google Scholar] [CrossRef]
- Yorozu, A.; Nishiguchi, S.; Yamada, M.; Aoyama, T.; Moriguchi, T.; Takahashi, M. Gait Measurement System for the Multi-Target Stepping Task Using a Laser Range Sensor. Sensors 2015, 15, 11151–11168. [Google Scholar] [CrossRef]
- Yorozu, A.; Moriguchi, T.; Takahashi, M. Improved Leg Tracking Considering Gait Phase and Spline-Based Interpolation during Turning Motion in Walk Tests. Sensors 2015, 15, 22451–22472. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Yorozu, A.; Adachi, D.; Takahashi, M.; Aoyama, T. Association between mild cognitive impairment and trajectory-based spatial parameters during timed up and go test using a laser range sensor. J. Neuroeng. Rehabil. 2017, 14, 78. [Google Scholar] [CrossRef] [PubMed]
- Iwai, M.; Koyama, S.; Tanabe, S.; Osawa, S.; Takeda, K.; Motoya, I.; Sakurai, H.; Kanada, Y.; Kawamura, N. The validity of spatiotemporal gait analysis using dual laser range sensors: A cross-sectional study. Arch. Physiother. 2019, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Perry, J.; Burnfield, J.M. Gait Analysis: Normal and Pathological Function. J. Sports Sci. Med. 2010, 9, 353. [Google Scholar] [CrossRef]
- Frenken, T.; Lipprandt, M.; Brell, M.; Goevercin, M.; Wegel, S.; Steinhagen-Thiessen, E.; Hein, A. Novel Approach to Unsupervised Mobility Assessment Tests: Field Trial For aTUG. In Proceedings of the 6th International Conference on Pervasive Computing Technologies for Healthcare (IEEE), San Diego, CA, USA, 21–24 May 2012. [Google Scholar] [CrossRef]
- Fudickar, S.; Stolle, C.; Volkening, N.; Hein, A. Scanning Laser Rangefinders for the Unobtrusive Monitoring of Gait Parameters in Unsupervised Settings. Sensors 2018, 18, 3424. [Google Scholar] [CrossRef]
- Li, J.; Fine, J. On sample size for sensitivity and specificity in prospective diagnostic accuracy studies. Stat. Med. 2004, 23, 2537–2550. [Google Scholar] [CrossRef] [PubMed]
- Bilney, B.; Morris, M.; Webster, K. Concurrent related validity of the GAITRite® walkway system for quantification of the spatial and temporal parameters of gait. Gait Posture 2003, 17, 68–74. [Google Scholar] [CrossRef]
- Webster, K.E.; Wittwer, J.E.; Feller, J.A. Validity of the GAITRite® walkway system for the measurement of averaged and individual step parameters of gait. Gait Posture 2005, 22, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.O.; Maki, B.E.; Williams, J.I.; Holliday, P.J.; Wood-Dauphinee, S.L. Clinical and laboratory measures of postural balance in an elderly population. Arch. Phys. Med. Rehabil. 1992, 73, 1073–1080. [Google Scholar]
- Tinetti, M.E. Performance-Oriented Assessment of Mobility Problems in Elderly Patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef]
- Powell, L.E.; Myers, A.M. The Activities-specific Balance Confidence (ABC) Scale. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1995, 50A, M28–M34. [Google Scholar] [CrossRef]
- Filiatrault, J.; Gauvin, L.; Fournier, M.; Parisien, M.; Robitaille, Y.; Laforest, S.; Corriveau, H.; Richard, L. Evidence of the Psychometric Qualities of a Simplified Version of the Activities-specific Balance Confidence Scale for Community-Dwelling Seniors. Arch. Phys. Med. Rehabil. 2007, 88, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Schott, N. Deutsche Adaptation der “Activities-Specific Balance Confidence (ABC) Scale, zur Erfassung der sturzassoziierten Selbstwirksamkeit. Z. Gerontol. Geriatr. 2008, 41, 475–485. [Google Scholar] [CrossRef]
- Beauchet, O.; Allali, G.; Annweiler, C.; Bridenbaugh, S.; Assal, F.; Kressig, R.W.; Herrmann, F.R. Gait Variability among Healthy Adults: Low and High Stride-to-Stride Variability Are Both a Reflection of Gait Stability. Gerontology 2009, 55, 702–706. [Google Scholar] [CrossRef]
- Schwenk, M.; Howe, C.; Saleh, A.; Mohler, J.; Grewal, G.; Armstrong, D.; Najafi, B. Frailty and Technology: A Systematic Review of Gait Analysis in Those with Frailty. Gerontology 2014, 60, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Osoba, M.Y.; Rao, A.K.; Agrawal, S.K.; Lalwani, A.K. Balance and gait in the elderly: A contemporary review. Laryngoscope Investig. Otolaryngol. 2019, 4, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Vitorino, L.M.; Teixeira, C.A.B.; Boas, E.L.V.; Pereira, R.L.; dos Santos, N.O.; Rozendo, C.A. Fear of falling in older adults living at home: Associated factors. Rev. Escola Enferm. USP 2017, 51, e03215. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.K.; Voaklander, D.; Perry, D.; Jones, C.A. Falls and fear of falling in older adults with total joint arthroplasty: A scoping review. BMC Musculoskelet. Disord. 2019, 20, 599. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gait Parameter | Description | Algorithm | Separately Per Foot |
|---|---|---|---|
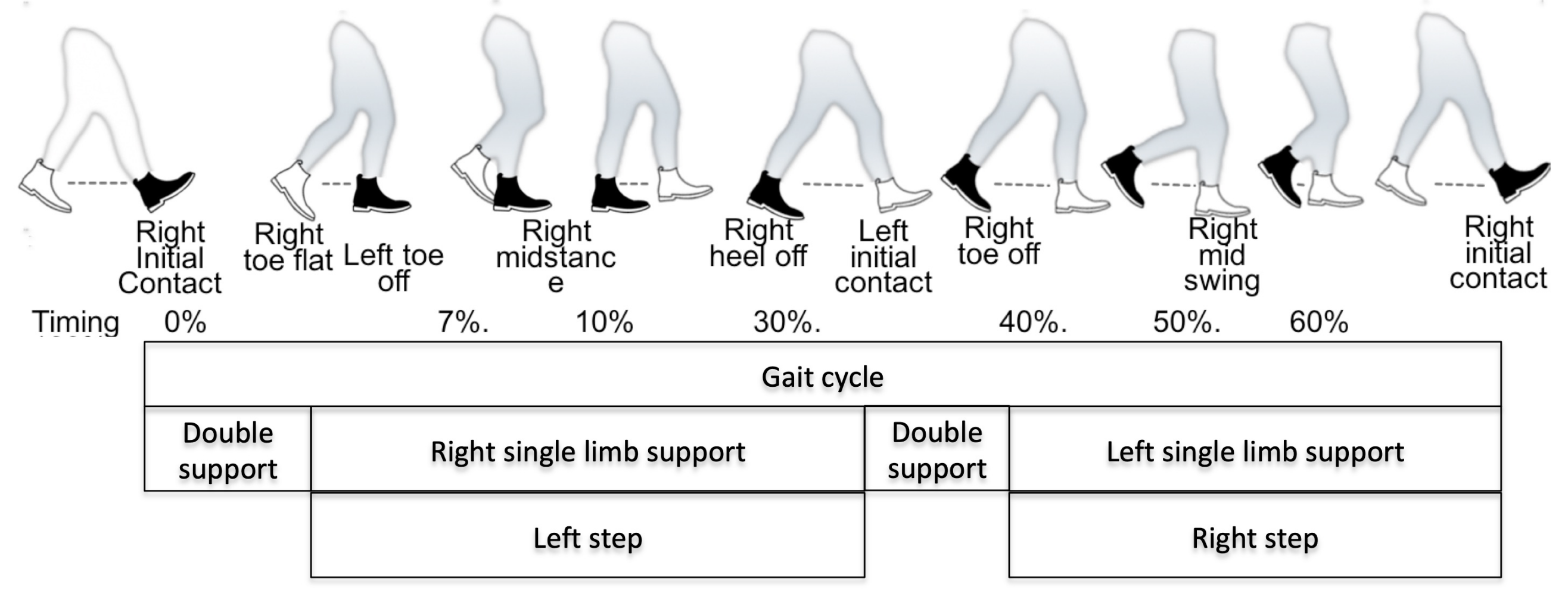
| Step length [m] | Distance between the toe of one foot to the heel of the next one along walking direction (see left and right step in Figure 2) | distance passed from toe off to initial contact. | x |
| Cadence [1/min] | Step frequency | number of steps/time [min] | |
| Velocity [m/min] | Gait speed | distance [m]/time [min] = stride_length [m] × cadence [1/min]/ 2 | |
| Stride length [m] | Distance from one foot hitting the ground to its next ground contact (see full gait cycle shown in Figure 2 as example for right stride). | step_lengthLeft + step_lengthRight | x |
| Mean | STD | Min | Max | |
|---|---|---|---|---|
| Age (years) | 73.5 | 6.8 | 58 | 92 |
| Height (cm) | 166.2 | 8.6 | 150 | 185 |
| Weight (kg) | 72.9 | 14.7 | 45 | 111 |
| BMI | 26.4 | 4.8 | 16.9 | 41.6 |
| BBS | 45.2 | 8.1 | 22 | 56 |
| ABC | 34.7 | 8.3 | 6 | 48 |
| Error | CC | |||||||
|---|---|---|---|---|---|---|---|---|
| Parameter | Mean | Std | Min | 25% | 50% | 75% | Max | |
| Velocity (m/s) | 0.034 | 0.036 | 0.001 | 0.01 | 0.022 | 0.046 | 0.227 | 0.992 |
| Stride Length Left (m) | 0.022 | 0.020 | 0 | 0.007 | 0.018 | 0.033 | 0.108 | 0.992 |
| Stride Length Right (m) | 0.025 | 0.026 | 0.0003 | 0.008 | 0.018 | 0.032 | 0.145 | 0.989 |
| Step Length Left (m) | 0.020 | 0.018 | 0.000 | 0.006 | 0.015 | 0.029 | 0.096 | 0.976 |
| Step Length Right (m) | 0.019 | 0.017 | 0 | 0.007 | 0.015 | 0.027 | 0.091 | 0.977 |
| Cadence (steps/min) | 27.248 | 11.065 | 6.49 | 19.94 | 26.365 | 33.398 | 71.84 | 0.959 |
| Steps (count) | 3.094 | 1.985 | 0 | 2 | 3 | 4 | 9 | 0.820 |
| Stance Time Left (m) | 0.293 | 0.145 | 0.146 | 0.229 | 0.263 | 0.319 | 1.657 | 0.876 |
| Stance Time Right (m) | 0.290 | 0.193 | 0.047 | 0.225 | 0.273 | 0.317 | 2.324 | 0.798 |
| Swing Time Left (s) | 0.078 | 0.130 | 0.001 | 0.019 | 0.048 | 0.090 | 1.316 | 0.607 |
| Swing Time Right (s) | 0.071 | 0.079 | 0 | 0.025 | 0.050 | 0.098 | 0.720 | 0.708 |
| Score | Parameter | Sensor | Slope | Intercept | R Value | p-Value | Std-Error |
|---|---|---|---|---|---|---|---|
| BBS | cadence | aTUG | 1.995 | 37.837 | 0.620 | 0.000 | 0.205 |
| GAITRite | 1.261 | 43.963 | 0.595 | 0.000 | 0.132 | ||
| velocity | aTUG | 0.029 | −0.367 | 0.782 | 0.000 | 0.002 | |
| GAITRite | 0.028 | −0.362 | 0.798 | 0.000 | 0.002 | ||
| step length R | aTUG | 0.010 | 0.087 | 0.742 | 0.000 | 0.001 | |
| GAITRite | 0.010 | 0.097 | 0.729 | 0.000 | 0.001 | ||
| step length L | aTUG | 0.011 | 0.024 | 0.704 | 0.000 | 0.001 | |
| GAITRite | 0.011 | −0.002 | 0.743 | 0.000 | 0.001 | ||
| stride length R | aTUG | 0.021 | 0.108 | 0.738 | 0.000 | 0.002 | |
| GAITRite | 0.021 | 0.093 | 0.756 | 0.000 | 0.002 | ||
| stride length L | aTUG | 0.021 | 0.103 | 0.750 | 0.000 | 0.002 | |
| GAITRite | 0.021 | 0.096 | 0.757 | 0.000 | 0.002 | ||
| ABC | cadence | aTUG | 1.288 | 84.270 | 0.395 | 0.000 | 0.238 |
| GAITRite | 0.837 | 72.527 | 0.408 | 0.000 | 0.152 | ||
| velocity | aTUG | 0.020 | 0.241 | 0.530 | 0.000 | 0.003 | |
| GAITRite | 0.020 | 0.231 | 0.541 | 0.000 | 0.002 | ||
| step length R | aTUG | 0.007 | 0.294 | 0.484 | 0.000 | 0.001 | |
| GAITRite | 0.007 | 0.294 | 0.478 | 0.000 | 0.001 | ||
| step length L | aTUG | 0.007 | 0.268 | 0.459 | 0.000 | 0.001 | |
| GAITRite | 0.007 | 0.265 | 0.487 | 0.000 | 0.001 | ||
| stride length R | aTUG | 0.015 | 0.561 | 0.491 | 0.000 | 0.002 | |
| GAITRite | 0.014 | 0.560 | 0.497 | 0.000 | 0.002 | ||
| stride length L | aTUG | 0.015 | 0.563 | 0.487 | 0.000 | 0.002 | |
| GAITRite | 0.014 | 0.568 | 0.487 | 0.000 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fudickar, S.; Kiselev, J.; Stolle, C.; Frenken, T.; Steinhagen-Thiessen, E.; Wegel, S.; Hein, A. Validation of a Laser Ranged Scanner-Based Detection of Spatio-Temporal Gait Parameters Using the aTUG Chair. Sensors 2021, 21, 1343. https://doi.org/10.3390/s21041343
Fudickar S, Kiselev J, Stolle C, Frenken T, Steinhagen-Thiessen E, Wegel S, Hein A. Validation of a Laser Ranged Scanner-Based Detection of Spatio-Temporal Gait Parameters Using the aTUG Chair. Sensors. 2021; 21(4):1343. https://doi.org/10.3390/s21041343
Chicago/Turabian StyleFudickar, Sebastian, Jörn Kiselev, Christian Stolle, Thomas Frenken, Elisabeth Steinhagen-Thiessen, Sandra Wegel, and Andreas Hein. 2021. "Validation of a Laser Ranged Scanner-Based Detection of Spatio-Temporal Gait Parameters Using the aTUG Chair" Sensors 21, no. 4: 1343. https://doi.org/10.3390/s21041343
APA StyleFudickar, S., Kiselev, J., Stolle, C., Frenken, T., Steinhagen-Thiessen, E., Wegel, S., & Hein, A. (2021). Validation of a Laser Ranged Scanner-Based Detection of Spatio-Temporal Gait Parameters Using the aTUG Chair. Sensors, 21(4), 1343. https://doi.org/10.3390/s21041343