
Evaluation of Optical and Radar Based Motion Capturing Technologies for Characterizing Hand Movement in Rheumatoid Arthritis—A Pilot Study


 ,
,  , , , ,
, , , ,
Abstract
1. Introduction
2. Methods
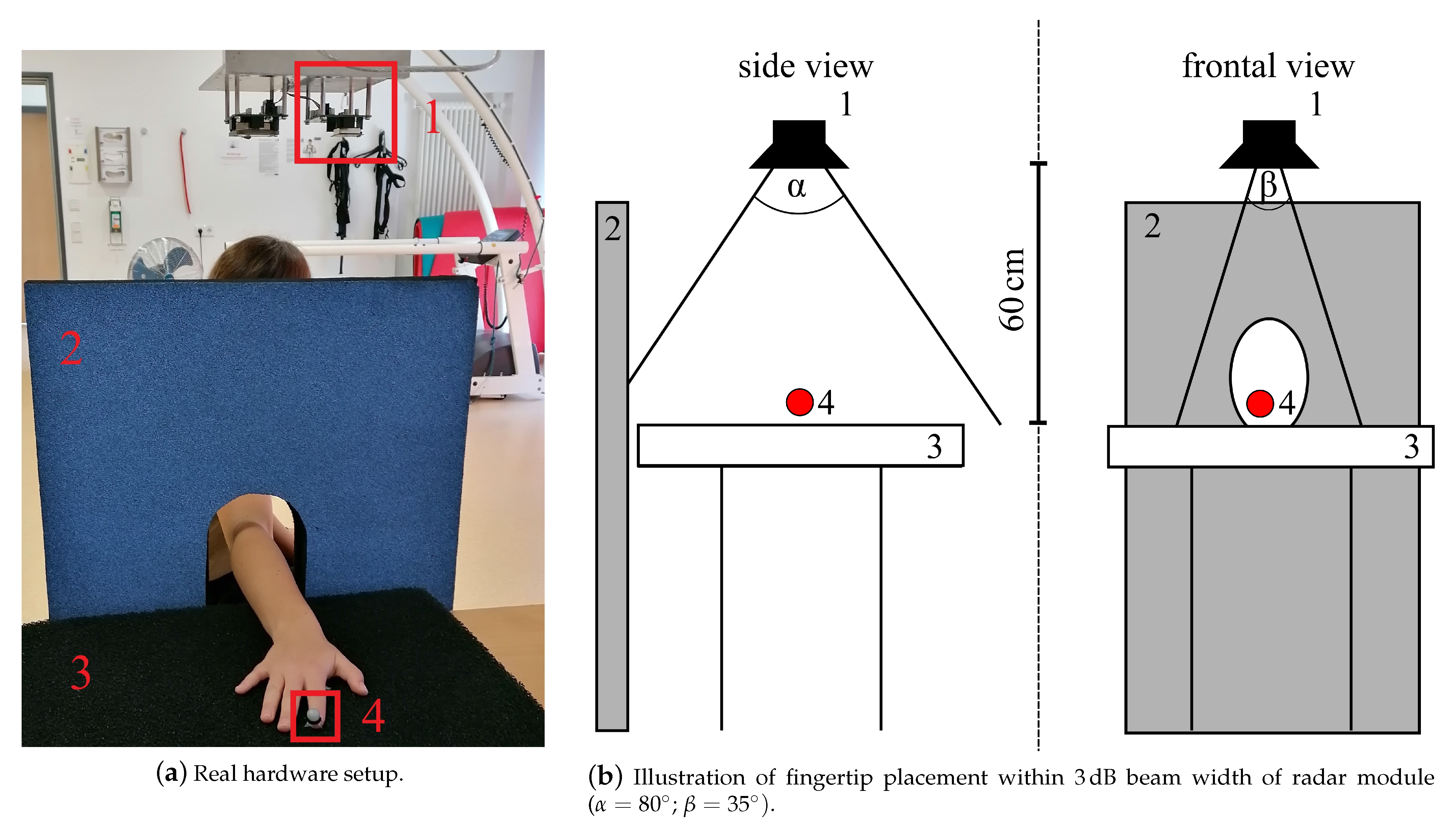
2.1. Experimental Setup
2.1.1. Subject Characteristics and Clinical Hand Function Assessment
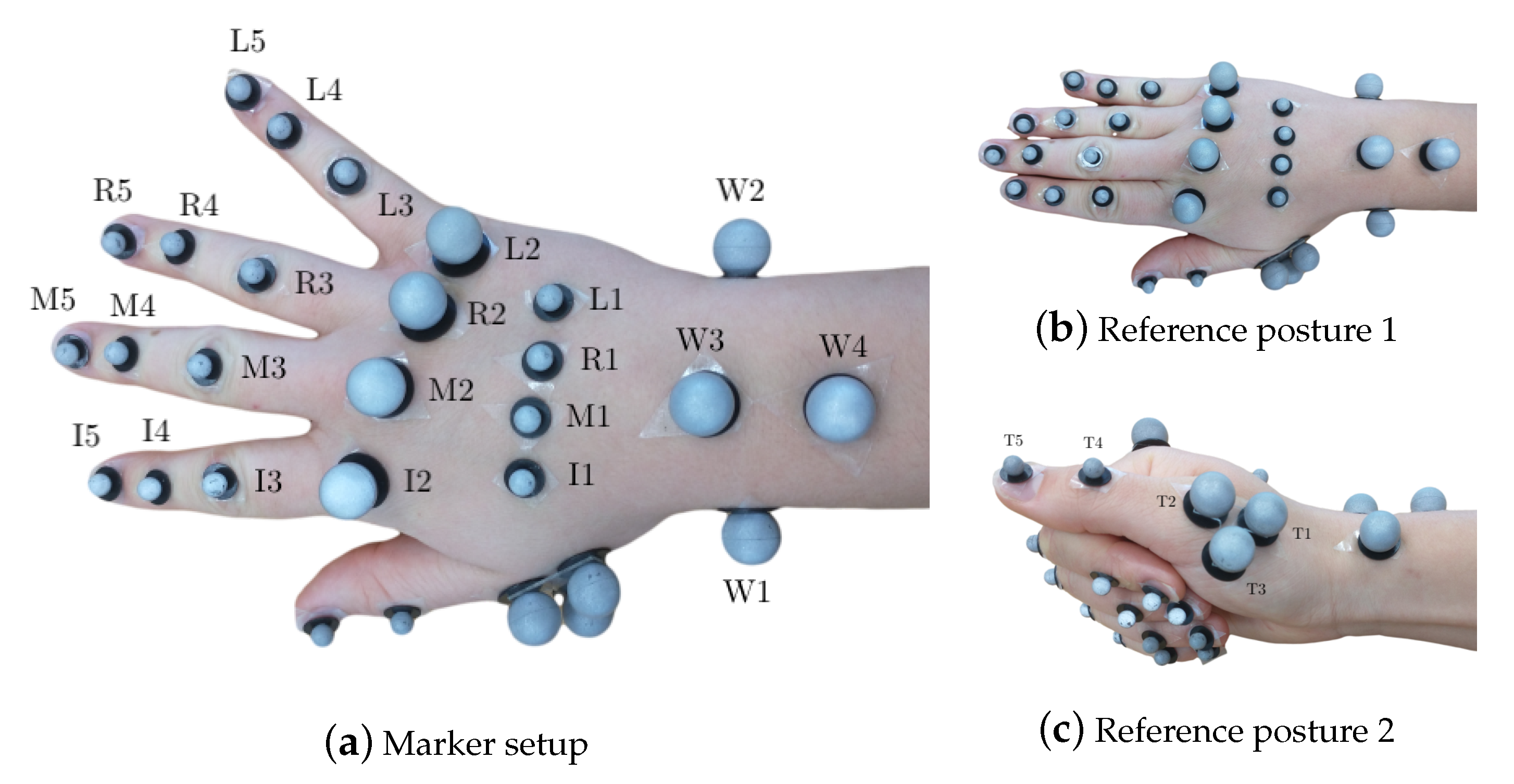
2.1.2. Optoelectronic Measurement System
2.1.3. Doppler Radar
2.1.4. Electromyography Measurement System
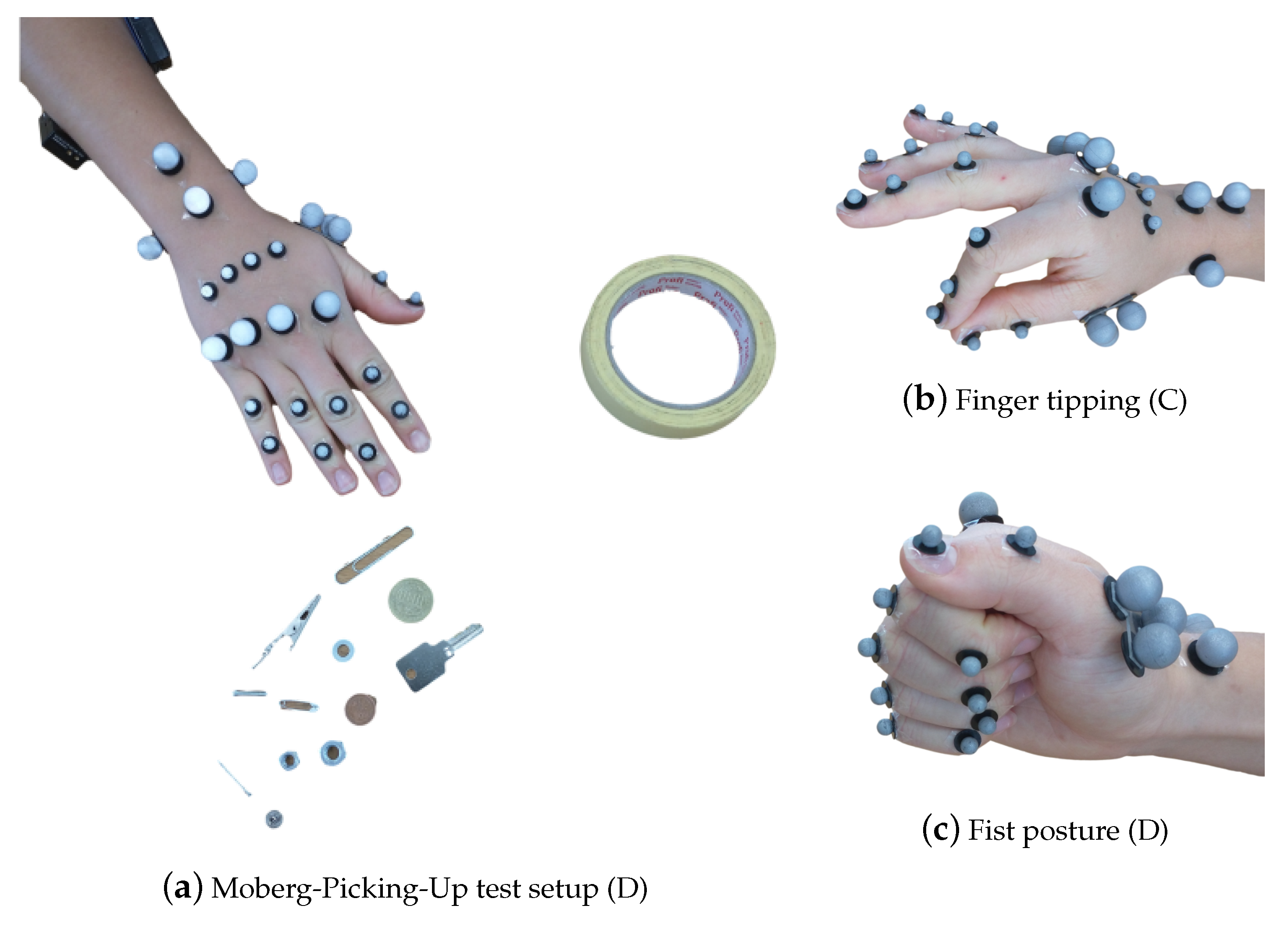
2.2. Data Collection
2.2.1. Clinical Data
2.2.2. OMS Data
2.2.3. Doppler Radar
2.3. Data Processing
2.3.1. Clinical Data
2.3.2. Marker Data Processing
2.3.3. Radar Signal Processing
2.3.4. Statistical Analysis
3. Results
3.1. Clinical Results and OMS Measures Outcomes
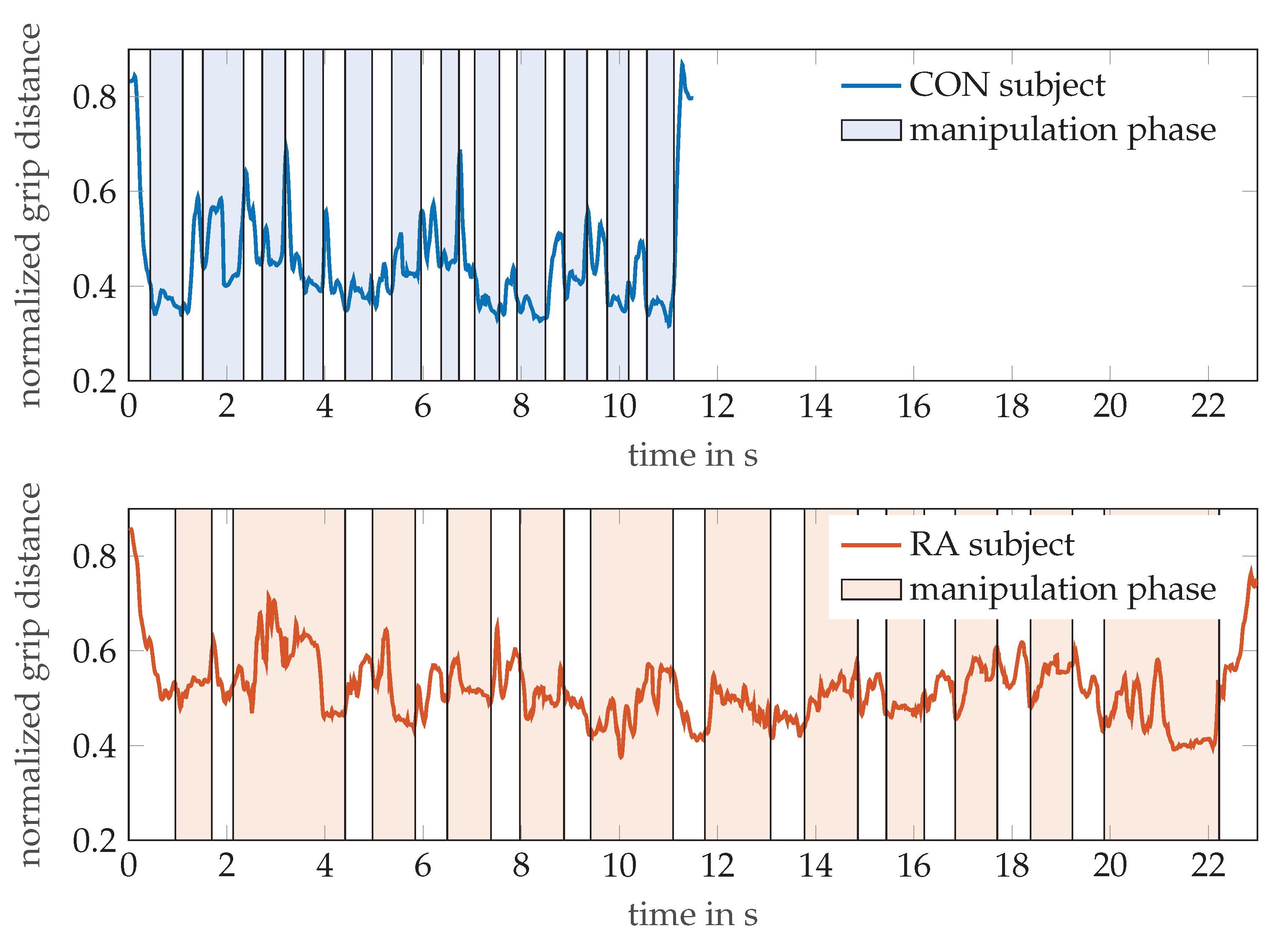
3.2. Radar Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McInnes, I.B. The pathogenesis of rheumatoid arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Conigliaro, P.; Triggianese, P.; Ippolito, F.; Lucchetti, R.; Chimenti, M.S.; Perricone, R. Insights on the role of physical activity in patients with rheumatoid arthritis: Physical Activity in RA. Drug Dev. Res. 2014, 75, S54–S56. [Google Scholar] [CrossRef]
- Eurenius, E.; Stenström, C.H.; The Para Study Group. Physical activity, physical fitness, and general health perception among individuals with rheumatoid arthritis: Physical Activity in RA. Arthritis Care Res. 2005, 53, 48–55. [Google Scholar] [CrossRef]
- Massy-Westropp, N.; Rankin, W.; Ahern, M.; Krishnan, J.; Hearn, T.C. Measuring grip strength in normal adults: Reference ranges and a comparison of electronic and hydraulic instruments. J. Hand Surg. 2004, 29, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Rolland, Y.; Cruz-Jentoft, A.J.; Bauer, J.M.; Sieber, C.; Cooper, C.; Al-Daghri, N.; Araujo de Carvalho, I.; Bautmans, I.; Bernabei, R.; et al. Assessment of muscle function and physical performance in daily clinical practice: A position paper endorsed by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Calcif. Tissue Int. 2019, 105, 1–14. [Google Scholar] [CrossRef]
- Ng, C.L.; Ho, D.D.; Chow, S.P. The Moberg pickup test: Results of testing with a standard protocol. J. Hand Ther. Off. J. Am. Soc. Hand Ther. 1999, 12, 309–312. [Google Scholar] [CrossRef]
- Liphardt, A.M.; Manger, E.; Liehr, S.; Bieniek, L.; Kleyer, A.; Simon, D.; Tascilar, K.; Sticherling, M.; Rech, J.; Schett, G.; et al. Similar impact of psoriatic arthritis and rheumatoid arthritis on objective and subjective parameters of hand function. ACR Open Rheumatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Goekoop-Ruiterman, Y.D.; de Vries-Bouwstra, J.; Allaart, C.; Van Zeben, D.; Kerstens, P.; Hazes, J.; Zwinderman, A.; Ronday, H.; Han, K.; Westedt, M.; et al. Clinical and radiographic outcomes of four different treatment strategies in patients with early rheumatoid arthritis (the BeSt study): A randomized, controlled trial. Arthritis Rheum. 2005, 52, 3381–3390. [Google Scholar] [CrossRef]
- van der Kruk, E.; Reijne, M.M. Accuracy of human motion capture systems for sport applications; state-of-the-art review. Eur. J. Sport Sci. 2018, 18, 806–819. [Google Scholar] [CrossRef]
- Turner, D.E.; Helliwell, P.S.; Siegel, K.L.; Woodburn, J. Biomechanics of the foot in rheumatoid arthritis: Identifying abnormal function and the factors associated with localised disease ‘impact’. Clin. Biomech. 2008, 23, 93–100. [Google Scholar] [CrossRef]
- Turner, D.E.; Woodburn, J. Characterising the clinical and biomechanical features of severely deformed feet in rheumatoid arthritis. Gait Posture 2008, 28, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Aleixo, P.; Vaz Patto, J.; Cardoso, A.; Moreira, H.; Abrantes, J. Ankle kinematics and kinetics during gait in healthy and rheumatoid arthritis post-menopausal women. Somatosens. Mot. Res. 2019, 36, 171–178. [Google Scholar] [CrossRef]
- Frize, M.; Karsh, J.; Herry, C.; Adea, C.; Aleem, I.; Payeur, P. Preliminary results of severity of illness measures of rheumatoid arthritis using infrared imaging. In Proceedings of the 2009 IEEE International Workshop on Medical Measurements and Applications, Cetraro, Italy, 29–30 May 2009; pp. 187–192. [Google Scholar]
- Holland, S.; Straatman, L.; MacDermid, J.; Sinden, K.; Lalone, E. The development of a novel grip motion analysis technique using the Dartfish movement analysis software to evaluate hand movements during activities of daily living. Med Eng. Phys. 2020, 85, 104–112. [Google Scholar] [CrossRef]
- Sancho-Bru, J.; Jarque-Bou, N.; Vergara, M.; Pérez-González, A. Validity of a simple videogrammetric method to measure the movement of all hand segments for clinical purposes. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2014. [Google Scholar] [CrossRef]
- Kuo, L.C.; Su, F.C.; Chiu, H.Y.; Yu, C.Y. Feasibility of using a video-based motion analysis system for measuring thumb kinematics. J. Biomech. 2002, 35, 1499–1506. [Google Scholar] [CrossRef]
- Yun, M.H.; Cannon, D.; Freivalds, A.; Thomas, G. An instrumented glove for grasp specification in virtual-reality-based point-and-direct telerobotics. IEEE Trans. Syst. Man Cybern. Part B (Cybern.) 1997, 27, 835–846. [Google Scholar] [CrossRef]
- Dipietro, L.; Sabatini, A.M.; Dario, P. Evaluation of an instrumented glove for hand-movement acquisition. J. Rehabil. Res. Dev. 2003, 40, 181. [Google Scholar] [CrossRef]
- Barlow, E.J. Doppler radar. Proc. IRE 1949, 37, 340–355. [Google Scholar] [CrossRef]
- Chen, V.; Fayin, L.; Shen-Shyang, H.; Wechsler, H. Micro-doppler effect in radar: Phenomenon, model, and simulation study. IEEE Trans. Aerosp. Electron. Syst. 2006, 42, 2–21. [Google Scholar] [CrossRef]
- Chen, K.; Misra, D.; Wang, H.; Chuang, H.; Postow, E. An X-Band microwave life-detection system. IEEE Trans. Biomed. Eng. 1986, BME-33, 697–701. [Google Scholar] [CrossRef]
- Chan, K.H.; Lin, J.C. Microprocessor-based cardiopulmonary rate monitor. Med. Biol. Eng. Comput. 1987, 25, 41–44. [Google Scholar] [CrossRef]
- Liang, X.; Lv, T.; Zhang, H.; Gao, Y.; Fang, G. Through-wall human being detection using UWB impulse radar. EURASIP J. Wirel. Commun. Netw. 2018, 2018, 46. [Google Scholar] [CrossRef]
- Boric-Lubecke, O.; Lubecke, V.M.; Host-Madsen, A.; Samardzija, D.; Cheung, K. Doppler radar sensing of multiple subjects in single and multiple antenna systems. In Proceedings of the TELSIKS 2005—2005th International Conference on Telecommunication in ModernSatellite, Cable and Broadcasting Services, Nis, Serbia, 28–30 September 2005; Volume 1, pp. 7–11. [Google Scholar] [CrossRef]
- Sacco, G.; Pisa, S. A Mimo Radar for Vital Signs Recording. In Proceedings of the 2019 PhotonIcs Electromagnetics Research Symposium—Spring (PIERS-Spring), Rome, Italy, 17–20 June 2019; pp. 387–393. [Google Scholar] [CrossRef]
- Peng, Z.; Muñoz-Ferreras, J.; Gómez-García, R.; Li, C. FMCW radar fall detection based on ISAR processing utilizing the properties of RCS, range, and Doppler. In Proceedings of the 2016 IEEE MTT-S International Microwave Symposium (IMS), San Francisco, CA, USA, 22–27 May 2016; pp. 1–3. [Google Scholar]
- Rivera, L.R.; Ulmer, E.; Zhang, Y.D.; Tao, W.; Amin, M.G. Radar-based fall detection exploiting time-frequency features. In Proceedings of the 2014 IEEE China Summit International Conference on Signal and Information Processing (ChinaSIP), Xi’an, China, 9–13 July 2014; pp. 713–717. [Google Scholar] [CrossRef]
- Raj, R.; Chen, V.; Lipps, R. Analysis of radar human gait signatures. IET Signal Process. 2010, 4, 234. [Google Scholar] [CrossRef]
- Seifert, A.K.; Grimmer, M.; Zoubir, A.M. Doppler radar for the extraction of biomechanical parameters in gait analysis. arXiv 2020, arXiv:2005.05280. [Google Scholar] [CrossRef]
- Vignaud, L.; Ghaleb, A.; Kernec, J.L.; Nicolas, J. Radar high resolution range & micro-Doppler analysis of human motions. In Proceedings of the 2009 International Radar Conference “Surveillance for a Safer World” (RADAR 2009), Bordeaux, France, 12–16 October 2009; pp. 1–6, ISSN 1097-5764. [Google Scholar]
- Saho, K.; Uemura, K.; Sugano, K.; Matsumoto, M. Using micro-Doppler radar to measure gait features associated with cognitive functions in elderly adults. IEEE Access 2019, 7, 24122–24131. [Google Scholar] [CrossRef]
- Amin, M.G.; Zeng, Z.; Shan, T. Hand gesture recognition based on radar micro-Doppler signature envelopes. In Proceedings of the 2019 IEEE Radar Conference (RadarConf), Boston, MA, USA, 22–26 April 2019; pp. 1–6. [Google Scholar] [CrossRef]
- Kim, Y.; Toomajian, B. Hand gesture recognition using micro-Doppler signatures with convolutional neural network. IEEE Access 2016, 4, 7125–7130. [Google Scholar] [CrossRef]
- Ritchie, M.; Jones, A.; Brown, J.; Griffiths, H.D. Hand gesture classification using 24 GHz FMCW dual polarised radar. In Proceedings of the International Conference on Radar Systems (Radar 2017), Belfast, UK, 23–26 October 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Zhang, S.; Li, G.; Ritchie, M.; Fioranelli, F.; Griffiths, H. Dynamic hand gesture classification based on radar micro-Doppler signatures. In Proceedings of the 2016 CIE International Conference on Radar (RADAR), Guangzhou, China, 10–13 October 2016; pp. 1–4. [Google Scholar] [CrossRef]
- Blunt, S.D.; Mokole, E.L. Overview of radar waveform diversity. IEEE Aerosp. Electron. Syst. Mag. 2016, 31, 2–42. [Google Scholar] [CrossRef]
- Skolnik, M. Radar Handbook, Second Edition; McGraw-Hill: New York, NY, USA, 1990. [Google Scholar]
- Fishler, E.; Haimovich, A.; Blum, R.; Chizhik, D.; Cimini, L.; Valenzuela, R. MIMO radar: An idea whose time has come. In Proceedings of the 2004 IEEE Radar Conference (IEEE Cat. No.04CH37509), Philadelphia, PA, USA, 29 April 2004; pp. 71–78. [Google Scholar]
- Li, C.; Lubecke, V.M.; Boric-Lubecke, O.; Lin, J. Sensing of Life Activities at the Human-Microwave Frontier. IEEE J. Microw. 2021, 1, 66–78. [Google Scholar] [CrossRef]
- Baan, H.; Dubbeldam, R.; Nene, A.V.; van de Laar, M.A. Gait analysis of the lower limb in patients with rheumatoid arthritis: A systematic review. In Seminars in Arthritis and Rheumatism; Elsevier: Amsterdam, The Netherlands, 2012; Volume 41, pp. 768–788. [Google Scholar]
- Barn, R.; Rafferty, D.; Turner, D.E.; Woodburn, J. Reliability study of tibialis posterior and selected leg muscle EMG and multi-segment foot kinematics in rheumatoid arthritis associated pes planovalgus. Gait Posture 2012, 36, 567–571. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Burtner, P.A.; Anderson, J.B.; Marcum, M.L.; Poole, J.L.; Qualls, C.; Picchiarini, M.S. A comparison of static and dynamic wrist splints using electromyography in individuals with rheumatoid arthritis. J. Hand Ther. 2003, 16, 320–325. [Google Scholar] [CrossRef]
- Brorsson, S.; Nilsdotter, A.; Thorstensson, C.; Bremander, A. Differences in muscle activity during hand-dexterity tasks between women with arthritis and a healthy reference group. BMC Musculoskelet. Disord. 2014, 15, 154. [Google Scholar] [CrossRef]
- Bedell, S.E.; Bush, B.T. Erythrocyte sedimentation rate. From folklore to facts. Am. J. Med. 1985, 78, 1001–1009. [Google Scholar] [CrossRef]
- Prevoo, M.; Van’T Hof, M.; Kuper, H.; Van Leeuwen, M.; Van De Putte, L.; Van Riel, P. Modified disease activity scores that include twenty-eight-joint counts development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1995, 38, 44–48. [Google Scholar] [CrossRef]
- Stamm, T.A.; Ploner, A.; Machold, K.P.; Smolen, J. Moberg picking-up test in patients with inflammatory joint diseases: A survey of suitability in comparison with button test and measures of disease activity. Arthritis Rheum. 2003, 49, 626–632. [Google Scholar] [CrossRef]
- Chung, K.C.; Hamill, J.B.; Walters, M.R.; Hayward, R.A. The Michigan Hand Outcomes Questionnaire (MHQ): Assessment of responsiveness to clinical change. Ann. Plast. Surg. 1999, 42, 619–622. [Google Scholar] [CrossRef]
- Chung, K.C.; Hamill, J.B.; Kim, H.M.; Walters, M.R.; Wilkins, E.G. Predictors of patient satisfaction in an outpatient plastic surgery clinic. Ann. Plast. Surg. 1999, 42, 56–60. [Google Scholar] [CrossRef]
- Chang, L.Y.; Pollard, N.S.; Mitchell, T.M.; Xing, E.P. Feature selection for grasp recognition from optical markers. In Proceedings of the 2007 IEEE/RSJ International Conference on Intelligent Robots and Systems, San Diego, CA, USA, 29 October–2 November 2007; pp. 2944–2950. [Google Scholar]
- Schröder, M.; Maycock, J.; Botsch, M. Reduced Marker Layouts for Optical Motion Capture of Hands. In Proceedings of the 8th ACM SIGGRAPH Conference on Motion in Games (MIG ’15), Paris, France, 16–18 November 2015; Association for Computing Machinery: New York, NY, USA, 2015; pp. 7–16. [Google Scholar] [CrossRef]
- Cooney, W.P.; Lucca, M.J.; Chao, E.Y.; Linscheid, R.L. The kinesiology of the thumb trapeziometacarpal joint. J. Bone Jt. Surg. Am. Vol. 1981, 63, 1371–1381. [Google Scholar] [CrossRef]
- Ghapanchizadeh, H.; Ahmad, S.A.; Ishak, A.J. Recommended surface EMG electrode position for wrist extension and flexion. In Proceedings of the 2015 IEEE Student Symposium in Biomedical Engineering Sciences (ISSBES), Shah Alam, Malaysia, 4 November 2015; pp. 108–112. [Google Scholar] [CrossRef]
- Konrad, P. The abc of emg. Pract. Introd. Kinesiol. Electromyogr. 2005, 1, 30–35. [Google Scholar]
- Lin, J.; Wu, Y.; Huang, T. Modeling the constraints of human hand motion. In Proceedings of the IEEE Workshop on Human MotionAustin, Austin, TX, USA, 7–8 November 2000; pp. 121–126. [Google Scholar] [CrossRef]
- Santello, M.; Flanders, M.; Soechting, J.F. Postural hand synergies for tool use. J. Neurosci. 1998, 18, 10105–10115. [Google Scholar] [CrossRef]
- Jarque-Bou, N.J.; Atzori, M.; Müller, H. A large calibrated database of hand movements and grasps kinematics. Sci. Data 2020, 7, 1–10. [Google Scholar] [CrossRef]
- Feix, T.; Romero, J.; Schmiedmayer, H.B.; Dollar, A.M.; Kragic, D. The grasp taxonomy of human grasp types. IEEE Trans. Hum.-Mach. Syst. 2015, 46, 66–77. [Google Scholar] [CrossRef]
- Wu, G.; Van der Helm, F.C.; Veeger, H.D.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Held, I.; Klein, O.; Chen, A.; Ma, V. Low complexity digital IQ imbalance correction in OFDM WLAN receivers. In Proceedings of the 2004 IEEE 59th Vehicular Technology Conference. VTC 2004-Spring (IEEE Cat. No.04CH37514), Milan, Italy, 17–19 May 2004; Volume 2, pp. 1172–1176. [Google Scholar] [CrossRef]
- Chen, V.C.; Tahmoush, D.; Miceli, W.J. (Eds.) Radar Micro-Doppler Signatures: Processing and Applications; Number Volume 34 in IET Radar, Sonar and Navigation Series; Institution of Engineering and Technology: Stevenage, UK, 2014. [Google Scholar]
- Braeunig, J.; Liphardt, A.M.; Penner, J.; Leyendecker, S.; Kleyer, A.; Schett, G.; Carlowitz, C.; Vossiek, M. A 24G Hz CW Radar Based Measurement Concept for Contactless Assessment of Finger Motion. Manuscript submitted for publication.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Test | Repetitions | Markers | EMG | Radar | |
|---|---|---|---|---|---|
| A | grip strength | 3 | - | - | - |
| Moberg-Picking-Up Test | 3 | - | - | - | |
| B | reference posture 1 | 1 | 29 | - | - |
| reference posture 2 | 1 | 29 | - | - | |
| C | joint relation | 1 | 29 | 2 | - |
| finger tipping | 1 | 29 | 2 | - | |
| grasping: spheres | 1 | 29 | 2 | - | |
| grasping: cylinders | 1 | 29 | 2 | - | |
| D | fist | 1 | 25 | 2 | - |
| grip strength | 2 | 25 | 2 | - | |
| Moberg-Picking-Up Test | 2 | 25 | 2 | - | |
| E | tapping index finger: frequency | 1 | 1 | - | 1 |
| tapping index finger: amplitude | 1 | 1 | - | 1 | |
| tapping little finger: frequency | 1 | 1 | - | 1 | |
| tapping little finger: amplitude | 1 | 1 | - | 1 |
| ALL () | CON () | RA () | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| min | mean (sd) | max | min | mean (sd) | max | min | mean (sd) | max | ||
| grip strength in lbs | clinical | 32 | 82.3 (34.6) | 178 | 44 | 91.7 (35.7) | 178 | 32 | 71.8 (29.8) | 134 |
| OMS | 19 | 64.0 (28.6) | 140 | 19 | 71.5 (29.6) | 140 | 20 | 55.4 (24.7) | 102 | |
| MPUT times in s | clinical | 9.2 | 15.6 (4.7) | 31.4 | 9.2 | 14.1 (4.1) | 31.4 | 12.2 | 17.5 (4.7) | 30.1 |
| OMS | 11.1 | 18.0 (6.2) | 41.0 | 11.1 | 16.0 (4.5) | 31.9 | 12.2 | 20.3 (7.1) | 41.0 | |
| Outcome | RA-Effect, 95% CI | p-Value | |||
|---|---|---|---|---|---|
| clinical | MPUT time in s | 3.87 | (1.36 to 6.39) | 0.004 | |
| grip strength in lbs | −23.61 | (−42.34 to −4.88) | 0.017 | ||
| OMS | MPUT time in s | 5.07 | (1.56 to 8.57) | 0.007 | |
| grip strength in lbs | −19.62 | (−35.01 to −4.23) | 0.016 | ||
| index finger | ang. vel. up in deg/s | −14.37 | (−82.05 to 53.31) | 0.679 | |
| ang. vel. down in deg/s | −2.95 | (−85.06 to 79.16) | 0.944 | ||
| num. cycles | −4.58 | (−9.96 to 0.81) | 0.103 | ||
| hyper-ext. in deg | −4.46 | (−10.12 to 1.21) | 0.131 | ||
| little finger | ang. vel. up in deg/s | −29.42 | (−86.50 to 27.67) | 0.318 | |
| ang. vel. down in deg/s | −9.41 | (−72.99 to 54.17) | 0.773 | ||
| num. cycles | −7.79 | (−14.96 to −0.62) | 0.039 | ||
| hyper-ext. in deg | −3.53 | (−9.50 to 2.44) | 0.253 | ||
| ALL () | CON () | RA () | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| min | mean (sd) | max | min | mean (sd) | max | min | mean (sd) | max | ||
| index finger | ang. vel. up in deg/s | 118 | 381 (113) | 729 | 174 | 381 (113) | 729 | 118 | 371 (124) | 598 |
| ang. vel. down in deg/s | 187 | 438 (142) | 760 | 228 | 436 (125) | 713 | 187 | 441 (160) | 760 | |
| num. cycles | 15 | 46.0 (10.2) | 82 | 33 | 48.0 (9.5) | 82 | 15 | 43.5 (10.4) | 58 | |
| hyper-ext. in deg | 13.4 | 38.1 (10.4) | 68.4 | 20.2 | 40.0 (10.8) | 68.4 | 13.4 | 35.6 (9.3) | 51.3 | |
| little finger | ang. vel. up in deg/s | 87.1 | 237 (100) | 562 | 87.1 | 248 (101) | 562 | 90.5 | 225 (97) | 461 |
| ang. vel. down in deg/s | 127 | 317 (116) | 675 | 127 | 319 (113) | 675 | 127 | 315 (120) | 579 | |
| num. cycles | 5 | 33.5 (13.1) | 63 | 7 | 37.1 (10.0) | 63 | 5 | 29.0 (13.6) | 57 | |
| hyper-ext. in deg | 8.4 | 26.4 (10.8) | 57.5 | 8.4 | 27.9 (10.8) | 53.9 | 10.6 | 24.6 (10.4) | 57.5 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phutane, U.; Liphardt, A.-M.; Bräunig, J.; Penner, J.; Klebl, M.; Tascilar, K.; Vossiek, M.; Kleyer, A.; Schett, G.; Leyendecker, S. Evaluation of Optical and Radar Based Motion Capturing Technologies for Characterizing Hand Movement in Rheumatoid Arthritis—A Pilot Study. Sensors 2021, 21, 1208. https://doi.org/10.3390/s21041208
Phutane U, Liphardt A-M, Bräunig J, Penner J, Klebl M, Tascilar K, Vossiek M, Kleyer A, Schett G, Leyendecker S. Evaluation of Optical and Radar Based Motion Capturing Technologies for Characterizing Hand Movement in Rheumatoid Arthritis—A Pilot Study. Sensors. 2021; 21(4):1208. https://doi.org/10.3390/s21041208
Chicago/Turabian StylePhutane, Uday, Anna-Maria Liphardt, Johanna Bräunig, Johann Penner, Michael Klebl, Koray Tascilar, Martin Vossiek, Arnd Kleyer, Georg Schett, and Sigrid Leyendecker. 2021. "Evaluation of Optical and Radar Based Motion Capturing Technologies for Characterizing Hand Movement in Rheumatoid Arthritis—A Pilot Study" Sensors 21, no. 4: 1208. https://doi.org/10.3390/s21041208
APA StylePhutane, U., Liphardt, A.-M., Bräunig, J., Penner, J., Klebl, M., Tascilar, K., Vossiek, M., Kleyer, A., Schett, G., & Leyendecker, S. (2021). Evaluation of Optical and Radar Based Motion Capturing Technologies for Characterizing Hand Movement in Rheumatoid Arthritis—A Pilot Study. Sensors, 21(4), 1208. https://doi.org/10.3390/s21041208