
A Multi-Center Disclusion Time Reduction (DTR) Randomized Controlled Occlusal Adjustment Study Using Occlusal Force and Timing Sensors Synchronized with Muscle Physiology Sensors

 , , and
, , and
Abstract
:1. Background
2. Materials and Methods
2.1. The Inclusion Criteria
- A history of chronic muscular myofascial pain dysfunction symptoms;
- A fully dentulous state of at least 28 teeth;
- Near normal occlusal relations with opposing molar and premolar teeth in contact in right and left excursions;
- Angles Class I and Class III subjects with anterior guiding teeth that were either in contact, or near to contact.
2.2. The Exclusion Criteria
- Severe Class II and Class III malocclusions;
- Large anterior open occlusions absent of anterior guidance contacts;
- A previous history of trauma to the TMJ region;
- Patients who had undergone prior treatment for Temporomandibular Disorder;
- Patients who had undergone prior occlusal adjustment treatment.
2.3. Pretreatment or Preplacebo Clinical Photogrpahs
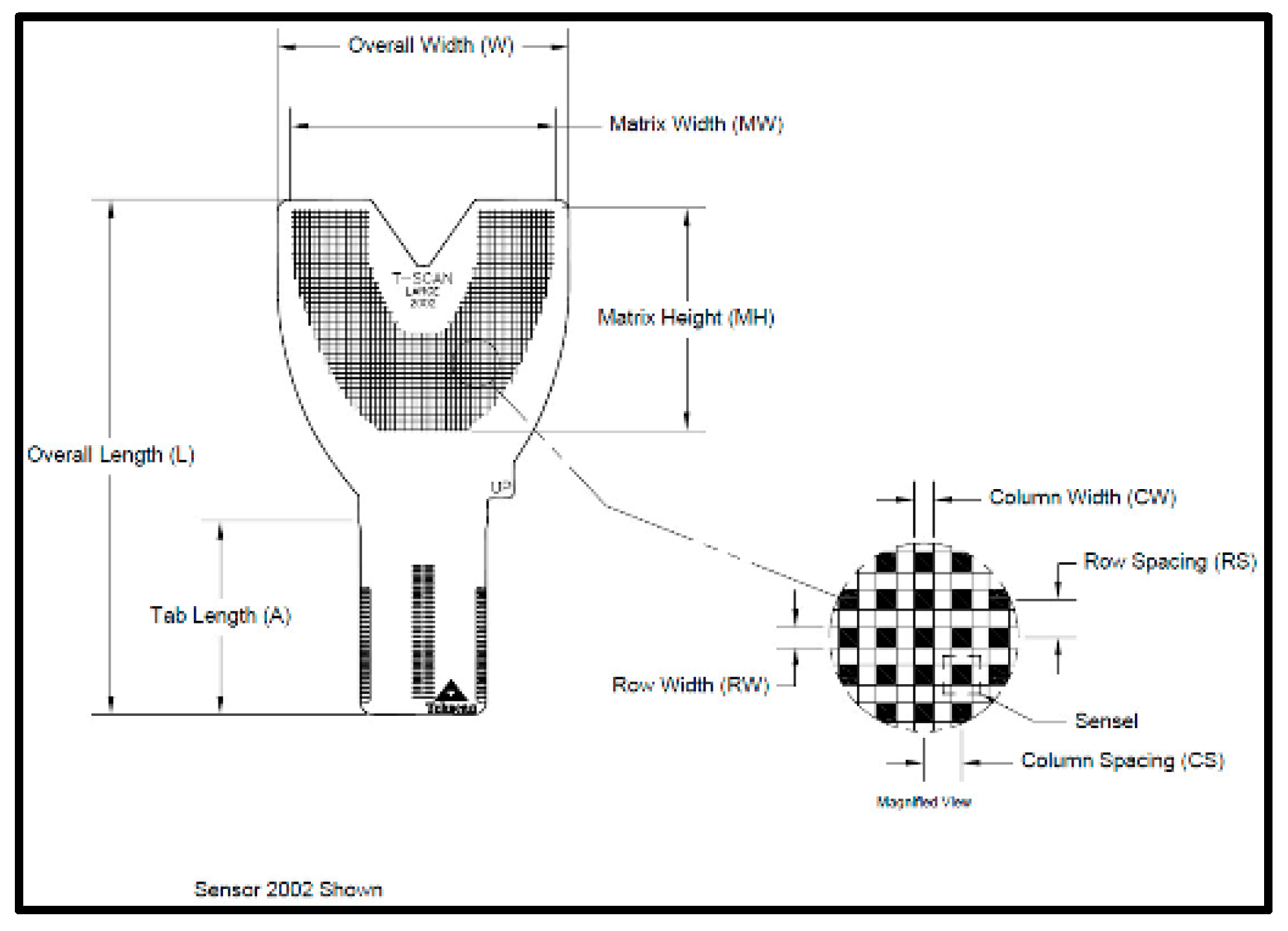
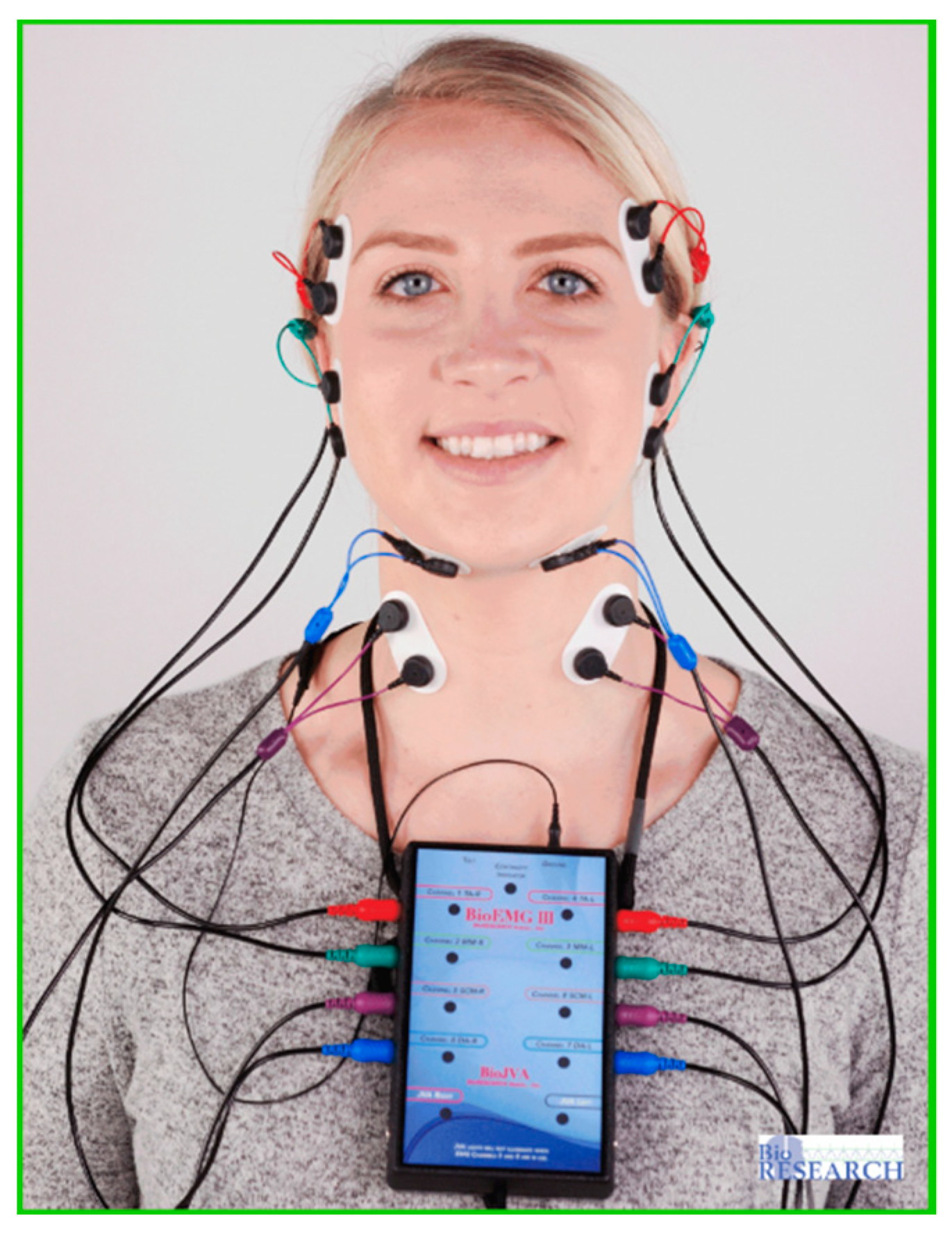
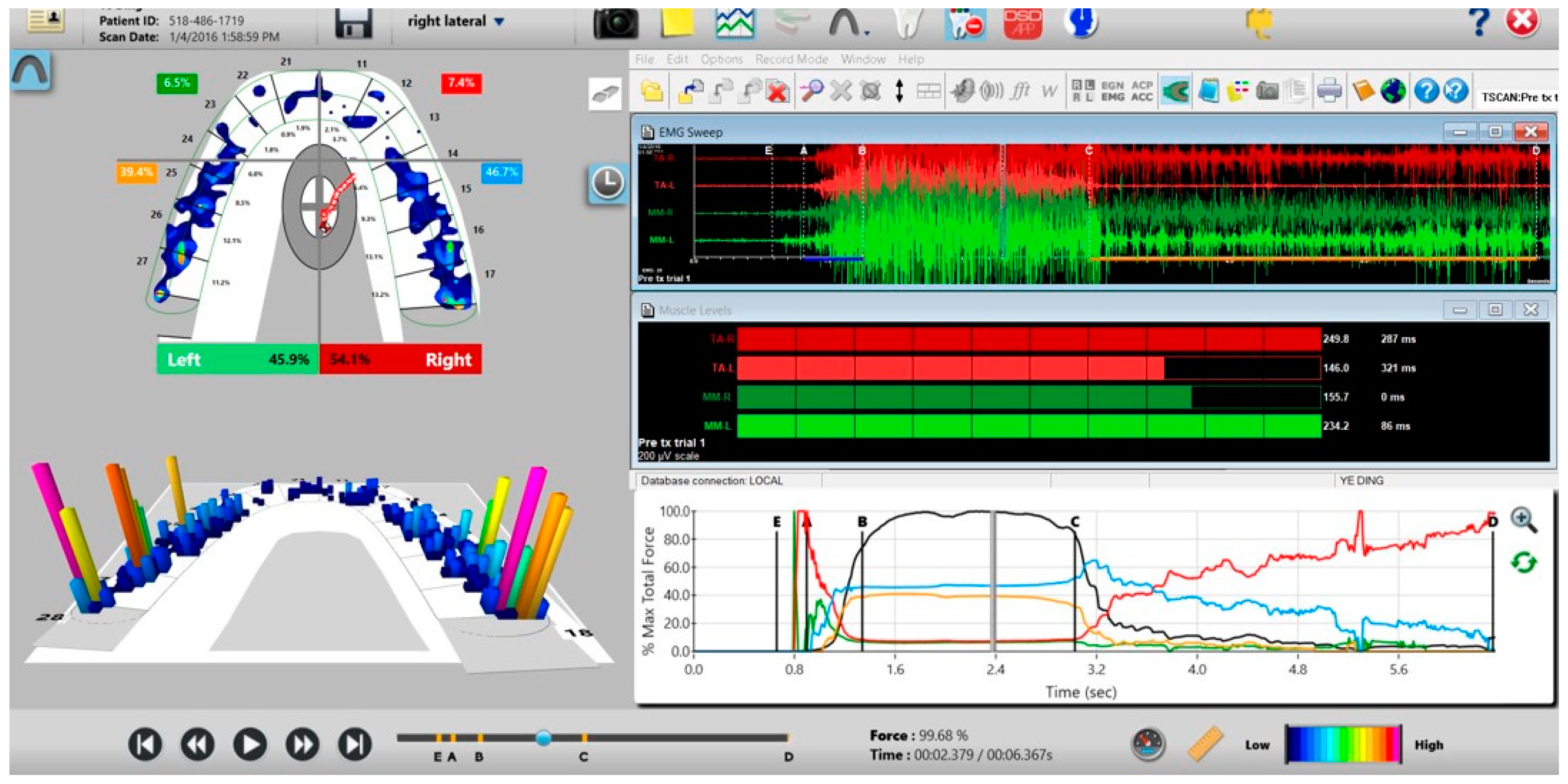
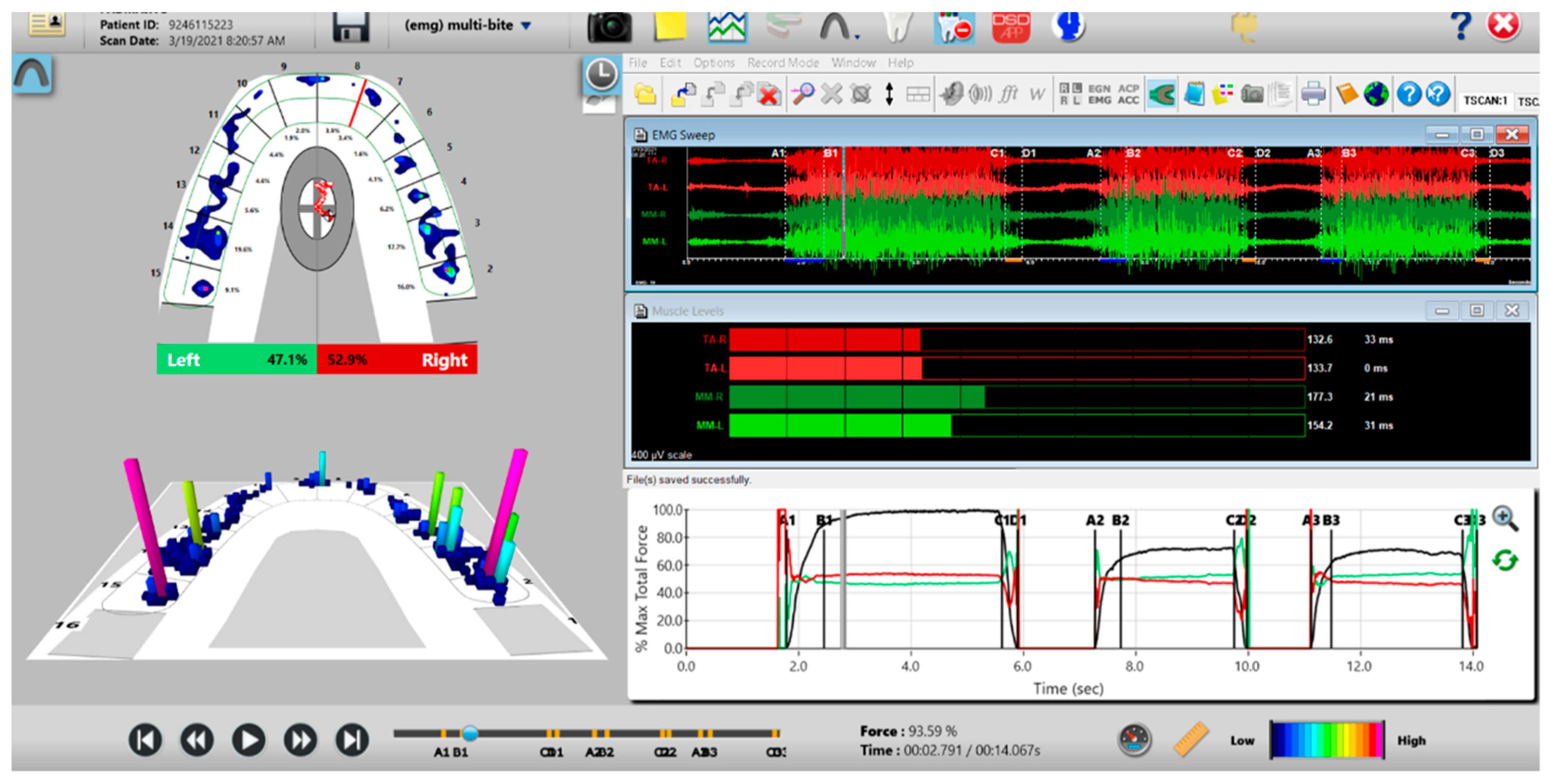
2.4. Pretreatment or Preplacebo T-Scan 10/BioEMG III Data Aquisition
2.5. ICAGD Occlusal Adjustment Procedure Performed on the Treated Group
2.6. ICAGD Was Considered Completed When
- All Class I, II, and III lateral excursive interferences had been visually removed;
- Disclusion of all posterior teeth in the right and left excursions was visible with the subject experiencing easier lateral movements than pre-ICAGD (Figure 13);
- All linear contacts had been removed;
- The remaining pattern of habitual closure contacts were located solely on cusp tips, fossae, and marginal ridges (Figure 14).


2.7. Procedures Performed for the Placebo Group—Mock ICAGD
2.8. Method of Symptom Assessment
3. Results
3.1. Disclusion Times
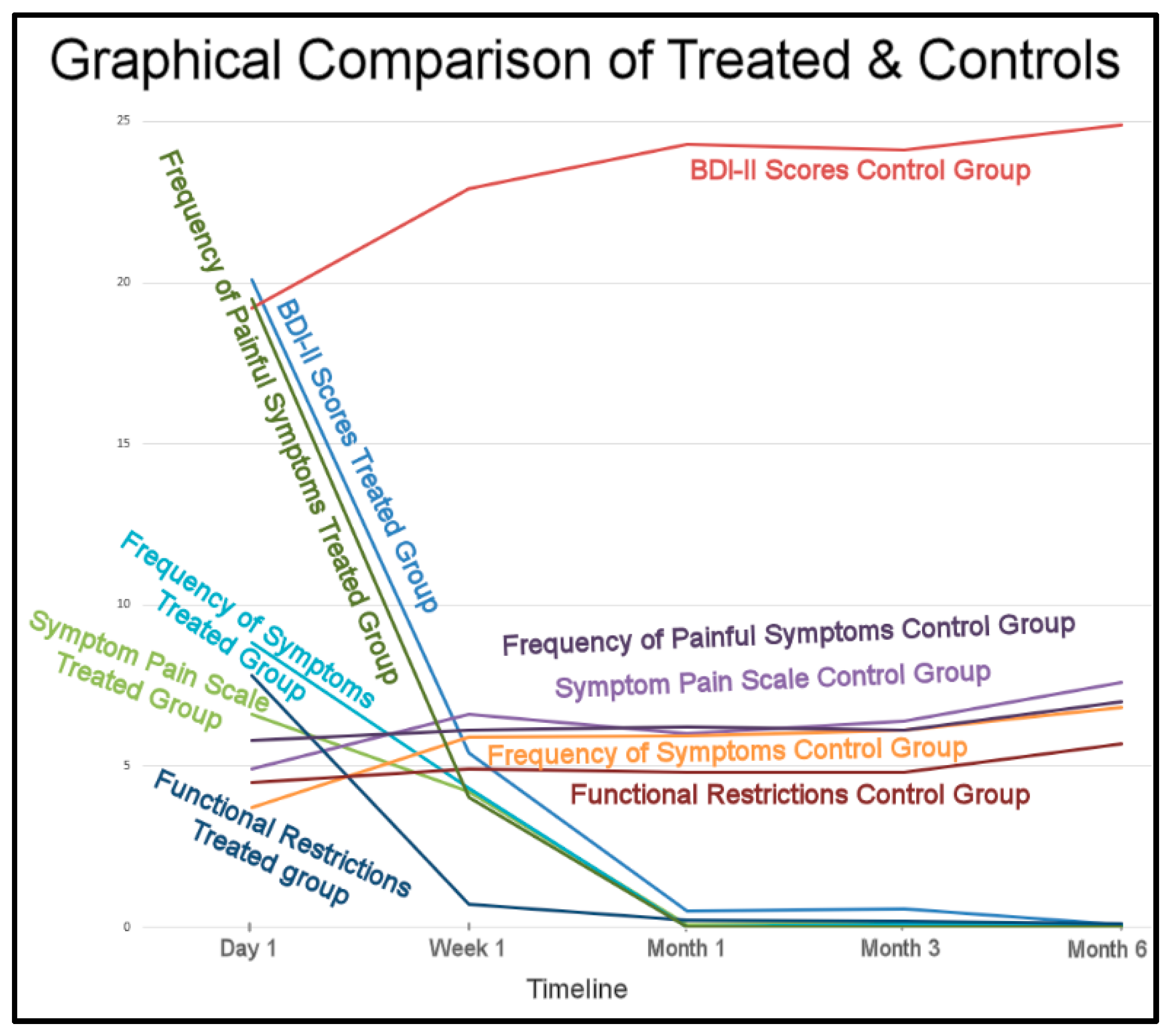
3.2. Mean BDI-II Scores
3.3. Mean Symptom Pain Scale Scores
3.4. Mean Frequency of Symptoms Scores
3.5. Mean Functional Restrictions Scores
3.6. Mean Frequency of Painful Symptoms Scores
4. Discussion
4.1. Corroboration of Prior Findings
4.2. ICAGD Is Defined by Numerical Occlusal Adjustment Endpoints
4.3. T-Scan High Definition Novus Sensor Demonstrate Repeatability and Durability
4.4. The EMG Electrodes Work in Concert with T-Scan Sensors to Measure the Occluso-Muscle Neurophysiology
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Anselmi, R. T-Scan 10 Recording dynamics, system features, and clinician user skills required for T-Scan chairside mastery. In Handbook of Research on Clinical Applications of Computerized Occlusal Analysis in Dental Medicine; Kerstein, R.B., Ed.; IGI Global Publishers: Hershey, PA, USA, 2020; pp. 130–224. [Google Scholar] [CrossRef]
- Kerstein, R.B. Time-sequencing and force-mapping with integrated electromyography to measure occlusal parameters. In Informatics in Oral Medicine; Daskalaki, A., Ed.; IGI Global Publishers: Hershey, PA, USA, 2010; pp. 88–110. [Google Scholar]
- Kerstein, R.B.; Radke, J. Average chewing pattern improvements following Disclusion Time reduction. CRANIO® 2017, 35, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Kerstein, R.B.; Wright, N. Electromyographic and computer analyses of patients suffering from chronic myofascial pain-dysfunction syndrome: Before and after treatment with immediate complete anterior guidance development. J. Prosthet. Dent. 1991, 66, 677–686. [Google Scholar] [CrossRef]
- Kerstein, R.B. Reducing chronic masseter and temporalis muscular hyperactivity with computer guided occlusal adjustments. Comp. Contin. Ed. Dent. 2010, 31, 530–534, 536, 538. [Google Scholar]
- Kerstein, R.B.; Radke, J. The effect of Disclusion Time reduction on maximal clench muscle activity levels. CRANIO® 2006, 24, 156–165. [Google Scholar] [CrossRef] [PubMed]
- Kerstein, R.B.; Radke, J. Masseter and temporalis excursive hyperactivity decreased by measured anterior guidance development. CRANIO® 2012, 30, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Thumati, P.; Manwani, R.; Mahantshetty, M. The effect of reduced Disclusion Time in the treatment of myofascial pain dysfunction syndrome using immediate complete anterior guidance development protocol monitored by digital analysis of occlusion. CRANIO® 2014, 32, 289–299. [Google Scholar] [CrossRef]
- Yiannios, N.; Kerstein, R.B.; Radke, J. Treatment of frictional dental hypersensitivity (FDH) with computer-guided occlusal adjustments. CRANIO® 2017, 35, 347–357. [Google Scholar] [CrossRef]
- Thumati, P.; Thumati, R.P. The effect of Disocclusion Time Reduction therapy to treat chronic myofascial pain: A single group interventional study with 3-year follow-up of 100 cases. J. Ind. Prosthodont. Soc. 2016, 16, 234–241. [Google Scholar] [CrossRef]
- Thumati, P. The influence of immediate complete anterior guidance development technique on subjective symptoms in Myofascial pain patients: Verified using digital analysis of occlusion (Tekscan) for analysing occlusion: A 3-year clinical observation. J. Ind. Prosthodont. Soc. 2015, 15, 218–223. [Google Scholar] [CrossRef]
- Thumati, P.; Sutter, B.; Kerstein, R.B.; Yiannios, N.; Radke, J. Changes in the Beck Depression Inventory-II Scores of TMD Subjects after Measured Occlusal Treatment. Adv. Dent. Technol. 2018, 1, 1–13. [Google Scholar]
- Thumati, P.; Poovani, S.; Bharathi, B.; Mounika, A.; Kerstein, R.B.; Radke, J. A Disclusion Time Reduction Randomized Controlled Occlusal Adjustment Trial. Adv. Dent. Technol. 2020, 2, 1–23. [Google Scholar]
- Baldini, A.; Nota, A.; Cozza, P. The association between occlusion time and temporomandibular disorders. J. Electromyogr. Kinesiol. 2015, 25, 151–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerstein, R.B. Disclusion time measurement studies: Stability of Disclusion Time—A 1-year follow-up. J. Prosthet. Dent. 1994, 72, 164–168. [Google Scholar] [CrossRef]
- Kerstein, R.B. Disclusion time measurement studies: A comparison of Disclusion Time between chronic myofascial pain dysfunction patients and non-patients: A population analysis. J. Prosthet. Dent. 1994, 72, 473–480. [Google Scholar] [CrossRef]
- Kerstein, R.B. Treatment of myofascial pain dysfunction syndrome with occlusal therapy to reduce lengthy Disclusion Time—A recall evaluation. CRANIO® 1995, 13, 105–115. [Google Scholar] [CrossRef]
- Kerstein, R.B.; Chapman, R.; Klein, M. A comparison of ICAGD (immediate complete anterior guidance development) to ‘mock ICAGD’ for symptom reductions in chronic myofascial pain dysfunction patients. CRANIO® 1997, 15, 21–37. [Google Scholar] [CrossRef]
- Sierpinska, T.; Kuc, J.; Golebiewska, M. Assessment of masticatory muscle activity and occlusion time in patients with advanced tooth wear. Arch. Oral Biol. 2015, 60, 1346–1355. [Google Scholar] [CrossRef]
- Stocka, A.; Sierpinska, T.; Kuc, J.; Golebiewska, M. Relationship between depression and masticatory muscles function in a group of adolescents. J. Craniomandib. Sleep Pract. 2018, 36, 390–395. [Google Scholar] [CrossRef]
- Sierpinska, T. Tooth Wear—Prevention, treatment and monitoring using the T-Scan/BioEMG Synchronization Module. Handbook of Research on Clinical Applications of Computerized Occlusal Analysis in Dental Medicine; Kerstein, R.B., Ed.; IGI Global Publishers: Hershey, PA, USA, 2020; pp. 879–944. [Google Scholar] [CrossRef]
- Meinert, C.L. Organization of multicenter clinical trials. Control. Clin. Trials 1981, 1, 305–312. [Google Scholar] [CrossRef]
- Schneider, D.; Weber, F.E.; Grunder, U.; Andreoni, C.; Burkhardt, R.; Jung, R.E. A randomized controlled clinical multicenter trial comparing the clinical and histological performance of a new, modified polylactide-co-glycolide acid membrane to an expanded polytetrafluorethylene membrane in guided bone regeneration procedures. Clin. Oral Implants Res. 2014, 25, 150–158. [Google Scholar] [CrossRef]
- Tasman, W. Cryotherapy for Retinopathy of Prematurity Cooperative Group and the National Eye Institute, Bethesda, Md. Multicenter trial of cryotherapy for retinopathy of prematurity. Preliminary results. Arch. Ophthalmol. 1988, 106, 471–479. [Google Scholar] [CrossRef]
- Geering, A. Occlusal interferences and functional disturbances of the masticatory system. J. Clin. Periodontics 1974, 1, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Forssell, H.; Kirveskari, P.; Kangasniemi, P. Effect of Occlusal Adjustment on Mandibular Dysfunction. A Double-Blind Study. Acta. Odontol. Scand. 1986, 44, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Wenneberg, B.; Nystrom, T.; Carlsson, G.E. Occlusal equilibration and other stomatognathic treatment in patients with mandibular dysfunction and headache. J. Prosthet. Dent. 1988, 59, 478–483. [Google Scholar] [CrossRef]
- Tsolka, P.; Morris, R.W.; Preiskel, H.W. Occlusal adjustment therapy for craniomandibular disorders: A clinical assessment by a doubleblind method. J. Prosthet. Dent. 1992, 68, 957–964. [Google Scholar] [CrossRef]
- Tsolka, P.; Preiskel, H.W. Kinesiographic and electromyographic assessment of the effects of occlusal adjustment therapy on craniomandibular disorders by a doubleblind method. J. Prosthet. Dent. 1993, 69, 85–92. [Google Scholar] [CrossRef]
- Watanabe, E.K.; Yatani, H.; Kuboki, T.; Matsuka, Y.; Terada, S.; Orsini, M.G.; Yamashita, A. The relationship between signs and symptoms of temporomandibular disorders and bilateral occlusal contact patterns during lateral excursions. J. Oral Rehabil. 1998, 25, 409–415. [Google Scholar] [CrossRef]
- Fujii, T. Occlusal conditions just after the relief of temporomandibular joint and masticatory muscle pain. J. Oral Rehabil. 2002, 29, 323–329. [Google Scholar] [CrossRef]
- Kerstein, R.B. Disclusion time reduction therapy with immediate complete anterior guidance development: The technique. Quintessence Int. 1992, 23, 735–747. [Google Scholar]
- Haines, D.E. Neuroanatomy: An Atlas of Structures, Sections, and Systems, 8th ed.; Lippincott Williams Wilkins: Baltimore, MD, USA, 2012; pp. 199, 227. [Google Scholar]
- Kerstein, R.B. A comparison of traditional occlusal equilibration and immediate complete anterior guidance development. J. Craniomandib. Pract. 1993, 11, 126–140. [Google Scholar] [CrossRef]
- Morley, S.; Williams, A.C.; Black, S. A confirmatory factor analysis of the Beck Depression Inventory in chronic pain. Pain 2002, 99, 289–298. [Google Scholar] [CrossRef]
- Poole, H.; Bramwell, R.; Murphy, P. Factor Structure of the Beck Depression Inventory II in patients with chronic pain. Clin. J. Pain 2006, 22, 790–798. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.; Kaplan, C.; Jason, L. Factor analysis of the Beck Depression Inventory-II with patients with chronic fatigue syndrome. J. Health Psychol. 2012, 17, 799–808. [Google Scholar] [CrossRef]
- Vanheule, S.; Desmet, M.; Groenvynck, H.; Rosseel, Y.; Fontaine, J. The factor structure of the Beck Depression Inventory-II: An evaluation. Assessment 2008, 15, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Thumati, P.; Poovani, S.; Ayinala, M. A retrospective five-year survey on the treatment outcome of disclusion time reduction (DTR) therapy in treating temporomandibular dysfunction patients. CRANIO® 2021, 9, 1–7. [Google Scholar] [CrossRef]
- Magri, L.V.; Bataglion, C.; Leite-Panissi, C.R. Follow-up results of a randomized clinical trial for low-level laser therapy in painful TMD of muscular origins. J. Craniomandib. Sleep Pract. 2019, 4, 1–8. [Google Scholar] [CrossRef]
- Vallon, D.; Ekberg, E.; Nilner, M.; Kopp, S. Occlusal adjustment in patients with craniomandibular disorders including headaches. A 3- and 6-month follow-up. Acta Odontol. Scand. 1995, 53, 55–59. [Google Scholar] [CrossRef]
- Goodman, P.; Greene, C.S.; Laskin, D.M. Response of patients with myofascial pain dysfunction syndrome to mock equilibration. J. Am. Dent. Assoc. 1976, 92, 755–758. [Google Scholar] [CrossRef]
- Yiannios, N.; Sutter, B.; Radke, J.; Kerstein, R.B. TMJ vibration changes following immediate complete anterior guidance development. Adv. Dent. Technol. 2018, 1, 13–28. [Google Scholar]
- Carey, J.P.; Craig, M.; Kerstein, R.B.; Radke, J. Determining a relationship between applied occlusal load and articulating paper mark area. Open Dent. J. 2007, 1, 1–7. [Google Scholar] [CrossRef]
- Saad, M.; Weiner, S.; Ehrenberg, D.; Weiner, G. Effects of load and indicator type upon occlusal contact markings. J. Biomed. Mater Res. Part B Appl. Biomater 2008, 85B, 18–22. [Google Scholar] [CrossRef]
- Qadeer, S.; Kerstein, R.B.; Yung-Kim, R.J.; Huh, J.B.; Shin, S.W. Relationship between articulation paper mark size and percentage of force measured with computerized occlusal analysis. J. Adv. Prosthodont. 2012, 4, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Kerstein, R.B.; Radke, J. Clinician accuracy when subjectively interpreting articulating paper markings. J. Craniomandib. Sleep Pract. 2013, 32, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Sutter, B.A. A digital poll of dentists testing the accuracy of paper mark subjective interpretation. CRANIO® 2017, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Basson, E.; Kerstein, R.B.; Radke, J. Ability to correctly select high force occlusal contacts from articulating paper markings. Adv. Dent. Technol. 2020, 2, 101–110. [Google Scholar]
- Qadeer, S.; Van Pelt, H.; Ozcan, M.; Edelhoff, D. The Accuracy, reliability, and clinical implications of static occlusal indicators compared to quantifiable occlusal indicators. Eur. J. Prosthodont. Rest. Dent. 2021, 29, 130–141. [Google Scholar] [CrossRef]
- Harty, M.; Lowe, M.; Kerstein, R.B.; Radke, J. A Force reproduction analysis of two recording sensors of a computerized occlusal analysis system. J. Craniomandib. Pract. 2006, 24, 15–24. [Google Scholar]
- Koos, B.; Godt, A.; Schille, C.; Göz, G. Precision of an instrumentation-based method of analyzing occlusion and its resulting distribution of forces in the dental arch. J. Orofacial. Orthop. 2010, 71, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Koos, B.; Höller, J.; Schille, C.; Godt, A. Time-dependent analysis and representation of force distribution and occlusion contact in the masticatory cycle. J. Orofacial. Orthop. 2012, 73, 204–214. [Google Scholar] [CrossRef]
- Da Silva Martins, M.J.; Caramelo, F.J.; da Fonseca, J.A.R.; Nicolau, P.M.G. In vitro study on the sensibility and reproducibility of the new T-Scan® III HD system. Rev. Port. Estomatol. Med. Dentária Circ. Maxilofac. 2014, 55, 14–22. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Comparison of Disclusion Times—Treated vs. Controls | Left Disclusion Time Pre-TX (s) | Right Disclusion Time Pre-TX (s) | Left DT Post-DTR Day 1 (s) | Right DT Post-DTR Day 1 (s) | Left DT 1 Week Post-Tx (s) | Right DT 1 Week Post-Tx (s) |
|---|---|---|---|---|---|---|
| Pre-Treatment | 1 Day Post-Treatment | 1 Week Post-Treatment | ||||
| Treatment Group | 2.99 | 2.75 | 0.33 | 0.33 | 0.32 | 0.31 |
| Control Group | 2.87 | 3.02 | 2.95 | 3.25 | ||
| Student’s t test p | >0.05 | >0.05 | <0.05 | <0.05 | ||
| Left DT 1 month Post-Tx (s) | Right DT 1 month Post-Tx (s) | Left DT 3 months Post-Tx (s) | Right DT 3 months Post-Tx (s) | Left DT 6 months Post-Tx (s) | Right DT 6 months Post-Tx (s) | |
| 1 month Post-Treatment | 3 months Post-Treatment | 6 months Post-Treatment | ||||
| Treatment Group | 0.30 | 0.30 | 0.30 | 0.29 | 0.28 | 0.27 |
| Control Group | 2.98 | 3.17 | 2.93 | 3.09 | 3.05 | 3.15 |
| Student’s t test p | <0.05 | <0.05 | <0.05 | <0.05 | <0.05 | <0.05 |
| Beck Depression Inventory-II Scores | Treated Group Scores (0–63) | Control Group Scores (0–63) | |
|---|---|---|---|
| Day 1 | Mean | 20.1 | 19.2 |
| (Pre-treatment) | SD | 4.98 | 7.26 |
| Median | 21 | 18 | |
| Initial relation of treated to controls | p > 0.05 | ||
| 1 week | Mean | 5.4 | 22.9 |
| (Post-treatment) | SD | 6.93 | 6.56 |
| Median | 4 | 23 | |
| Treated to controls at 1 week | p < 0.00001 | ||
| 1 month | Mean | 0.48 | 24.3 |
| (Post-treatment) | SD | 1.45 | 6.79 |
| Median | 0 | 23 | |
| Treated to controls at 1 month | p < 0.00001 | ||
| 3 months | Mean | 0.56 | 24.1 |
| (Post-treatment) | SD | 0.51 | 7.73 |
| Median | 0 | 23 | |
| Treated to controls at 3 months | p < 0.000013 | ||
| 6 months | Mean | 0.06 | 24.9 |
| (Post-treatment) | SD | 0.24 | 6.02 |
| Median | 0 | 24 | |
| Treated to controls at 6 months | p < 0.00001 | ||
| Symptom Pain Scale Levels (0–4) | Treated Group Scores (0–48) | Control Group Scores (0–48) | |
|---|---|---|---|
| Day 1 | Mean | 6.6 | 4.9 |
| (Pre-treatment) | SD | 5.96 | 4.28 |
| Median | 5 | 5 | |
| Initial relation of treated to controls | p > 0.05 | ||
| 1 week | Mean | 4.2 | 6.6 |
| (Post-treatment) | SD | 2.51 | 5.21 |
| Median | 4 | 6 | |
| Treated to controls at 1 week | p < 0.0056 | ||
| 1 month | Mean | 0.06 | 6.0 |
| (Post-treatment) | SD | 0.24 | 5.20 |
| Median | 0 | 5 | |
| Treated to controls at 1 month | p < 0.00001 | ||
| 3 months | Mean | 0.16 | 6.4 |
| (Post-treatment) | SD | 0.51 | 5.24 |
| Median | 0 | 6 | |
| Treated to controls at 3 months | p < 0.00001 | ||
| 6 months | Mean | 0.08 | 7.6 |
| (Post-treatment) | SD | 0.27 | 4.99 |
| Median | 0 | 7 | |
| Treated to controls at 6 months | p < 0.00001 | ||
| Frequency of Symptoms Scale (0–3) | Treated Group Scores (0–33) | Control Group Scores (0–33) | |
|---|---|---|---|
| Day 1 | Mean | 8.84 | 3.7 |
| (Pre-treatment) | SD | 4.10 | 3.78 |
| Median | 9 | 3 | |
| Initial relation of treated to controls | p < 0.05 | ||
| 1 week | Mean | 4.3 | 5.9 |
| (Post-treatment) | SD | 2.75 | 5.01 |
| Median | 4 | 5 | |
| Treated to controls at 1 week | p = 0.1868 | ||
| 1 month | Mean | 0.02 | 5.92 |
| (Post-treatment) | SD | 0.14 | 4.99 |
| Median | 0 | 5 | |
| Treated to controls at 1 month | p < 0.00001 | ||
| 3 months | Mean | 0.06 | 6.1 |
| (Post-treatment) | SD | 0.24 | 5.03 |
| Median | 0 | 5 | |
| Treated to controls at 3 months | p < 0.00001 | ||
| 6 months | Mean | 0.04 | 6.8 |
| (Post-treatment) | SD | 0.198 | 4.89 |
| Median | 0 | 6 | |
| Treated to controls at 6 months | p < 0.00001 | ||
| Functional Restrictions (0–3) | Treated Group Scores (0–27) | Control Group Scores (0–27) | |
|---|---|---|---|
| Day 1 | Mean | 7.8 | 4.5 |
| (Pre-treatment) | SD | 2.73 | 2.95 |
| Median | 7 | 4 | |
| Initial relation of treated to controls | p < 0.05 | ||
| 1 week | Mean | 0.7 | 4.9 |
| (Post-treatment) | SD | 1.41 | 3.05 |
| Median | 0 | 4 | |
| Treated to controls at 1 week | p < 0.00001 | ||
| 1 month | Mean | 0.22 | 4.8 |
| (Post-treatment) | SD | 0.74 | 2.99 |
| Median | 0 | 4 | |
| Treated to controls at 1 month | p < 0.00001 | ||
| 3 months | Mean | 0.18 | 4.8 |
| (Post-treatment) | SD | 0.6 | 3.01 |
| Median | 0 | 0 | |
| Treated to controls at 3 months | p < 0.00001 | ||
| 6 months | Mean | 0.12 | 5.7 |
| (Post-treatment) | SD | 0.39 | 2.73 |
| Median | 0 | 6 | |
| Treated to controls at 6 months | p < 0.00001 | ||
| Frequency of Painful Symptoms (0–3) | Treated Group Scores (0–30) | Control Group Scores (0–30) | |
|---|---|---|---|
| Day 1 | Mean | 19.5 | 5.8 |
| (Pre-treatment) | SD | 5.51 | 4.65 |
| Median | 20 | 5 | |
| Initial relation of treated to controls | p < 0.05 | ||
| 1 week | Mean | 4.04 | 6.1 |
| (Post-treatment) | SD | 1.67 | 4.68 |
| Median | 4 | 5 | |
| Treated to controls at 1 week | p = 0.0043 | ||
| 1 month | Mean | 0.02 | 6.2 |
| (Post-treatment) | SD | 0.14 | 4.57 |
| Median | 0 | 5 | |
| Treated to controls at 1 month | p < 0.00001 | ||
| 3 months | Mean | 0.02 | 6.1 |
| (Post-treatment) | SD | 0.14 | 4.66 |
| Median | 0 | 5 | |
| Treated to controls at 3 months | p < 0.00001 | ||
| 6 months | Mean | 0.02 | 6.98 |
| (Post-treatment) | SD | 0.14 | 4.25 |
| Median | 0 | 7 | |
| Treated to controls at 6 months | p < 0.00001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thumati, P.; Thumati, R.P.; Poovani, S.; Sattur, A.P.; Srinivas, S.; Kerstein, R.B.; Radke, J. A Multi-Center Disclusion Time Reduction (DTR) Randomized Controlled Occlusal Adjustment Study Using Occlusal Force and Timing Sensors Synchronized with Muscle Physiology Sensors. Sensors 2021, 21, 7804. https://doi.org/10.3390/s21237804
Thumati P, Thumati RP, Poovani S, Sattur AP, Srinivas S, Kerstein RB, Radke J. A Multi-Center Disclusion Time Reduction (DTR) Randomized Controlled Occlusal Adjustment Study Using Occlusal Force and Timing Sensors Synchronized with Muscle Physiology Sensors. Sensors. 2021; 21(23):7804. https://doi.org/10.3390/s21237804
Chicago/Turabian StyleThumati, Prafulla, Roshan P Thumati, Shwetha Poovani, Atul P Sattur, Srividya Srinivas, Robert B Kerstein, and John Radke. 2021. "A Multi-Center Disclusion Time Reduction (DTR) Randomized Controlled Occlusal Adjustment Study Using Occlusal Force and Timing Sensors Synchronized with Muscle Physiology Sensors" Sensors 21, no. 23: 7804. https://doi.org/10.3390/s21237804
APA StyleThumati, P., Thumati, R. P., Poovani, S., Sattur, A. P., Srinivas, S., Kerstein, R. B., & Radke, J. (2021). A Multi-Center Disclusion Time Reduction (DTR) Randomized Controlled Occlusal Adjustment Study Using Occlusal Force and Timing Sensors Synchronized with Muscle Physiology Sensors. Sensors, 21(23), 7804. https://doi.org/10.3390/s21237804