
Identification of Ictal Tachycardia in Focal Motor- and Non-Motor Seizures by Means of a Wearable PPG Sensor

 , , , , , and
, , , , , and
Abstract
:1. Introduction
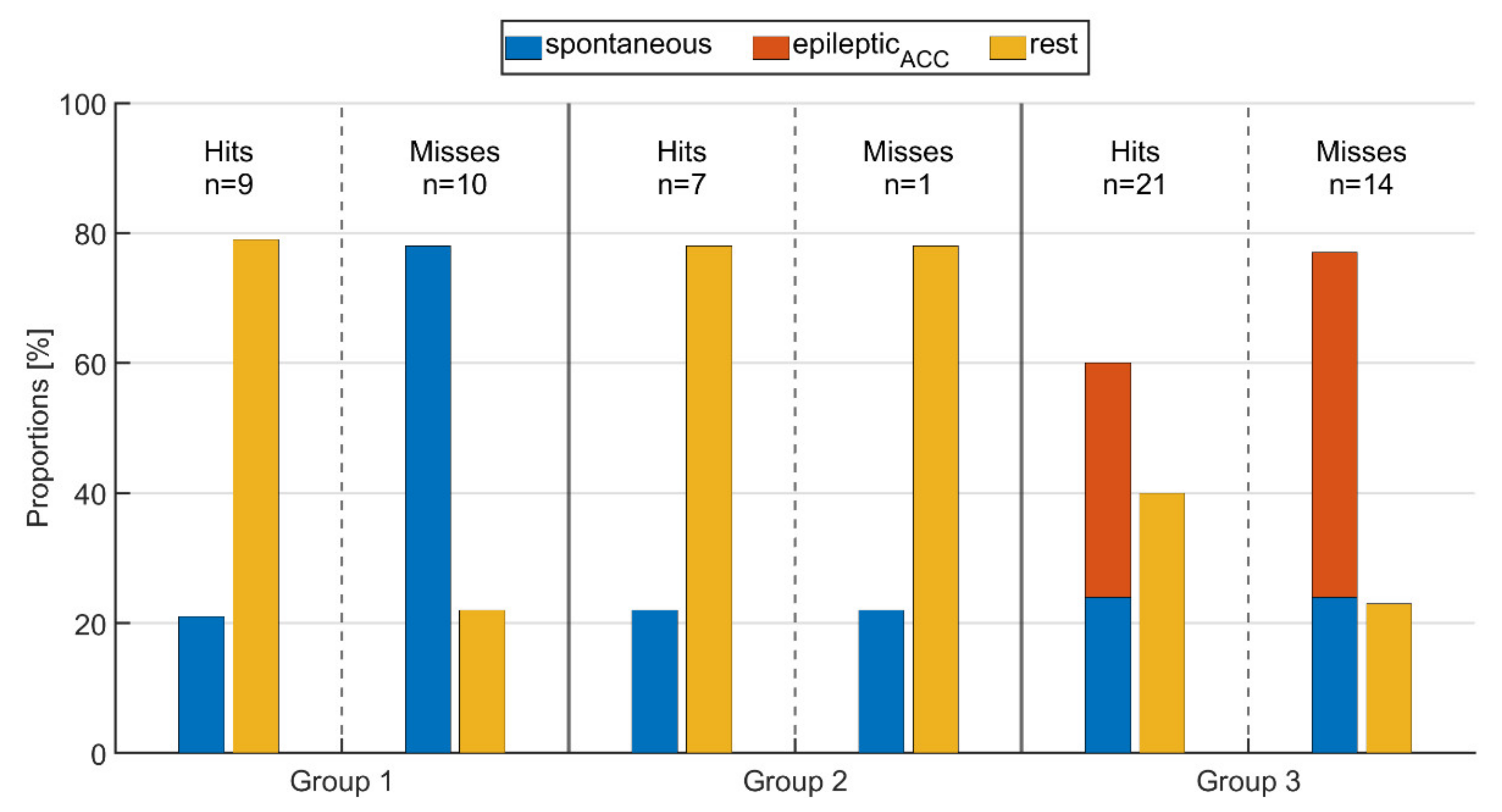
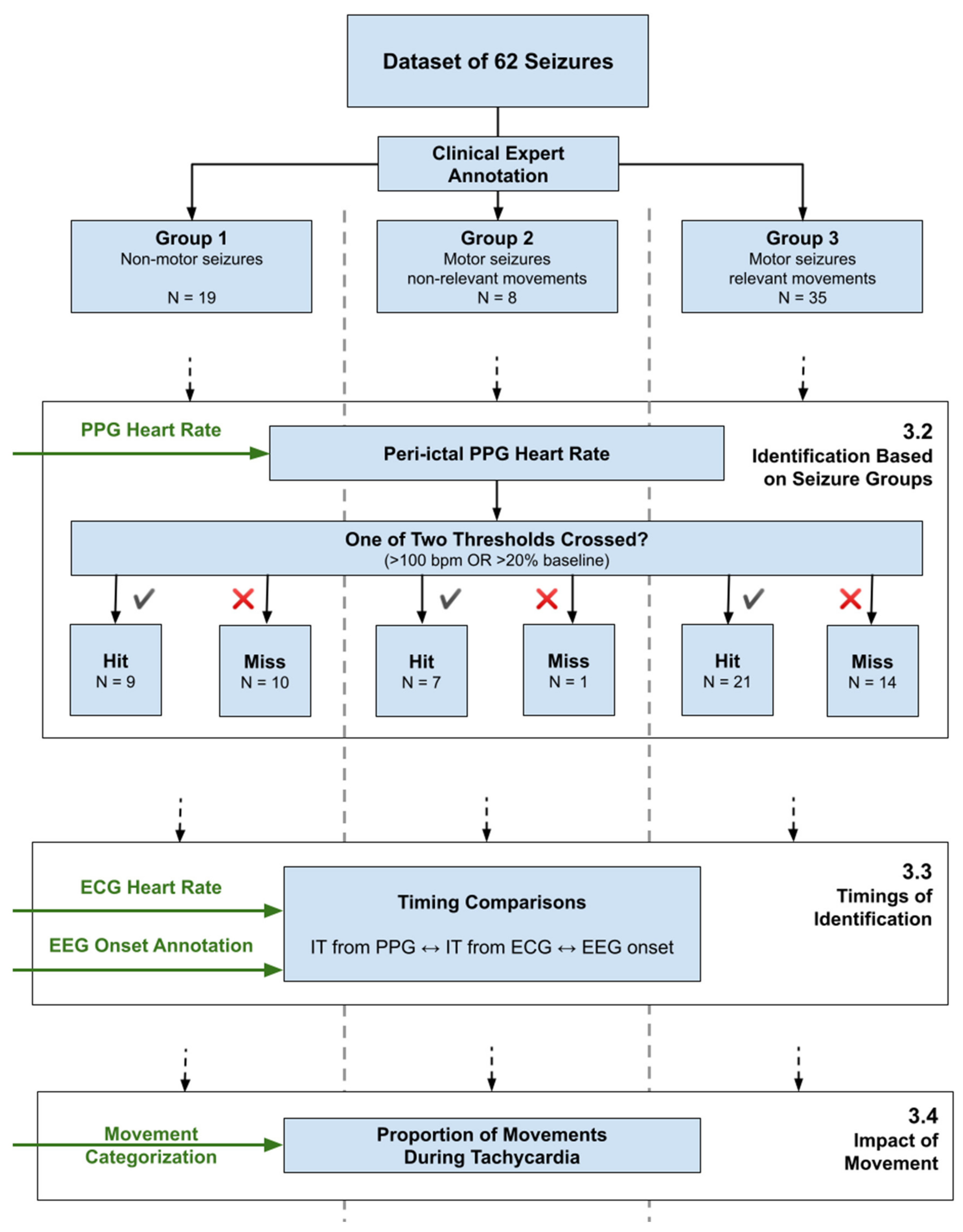
- Group 1: Seizures with IT and without epileptic movements (non-motor)
- Group 2: Seizures with IT and with epileptic motor symptoms not affecting the extremities, including oral automatisms or eye blinking (motor, non-relevant)
- Group 3: Seizures with IT and with epileptic movements involving arms or legs (motor, relevant)
2. Materials and Methods
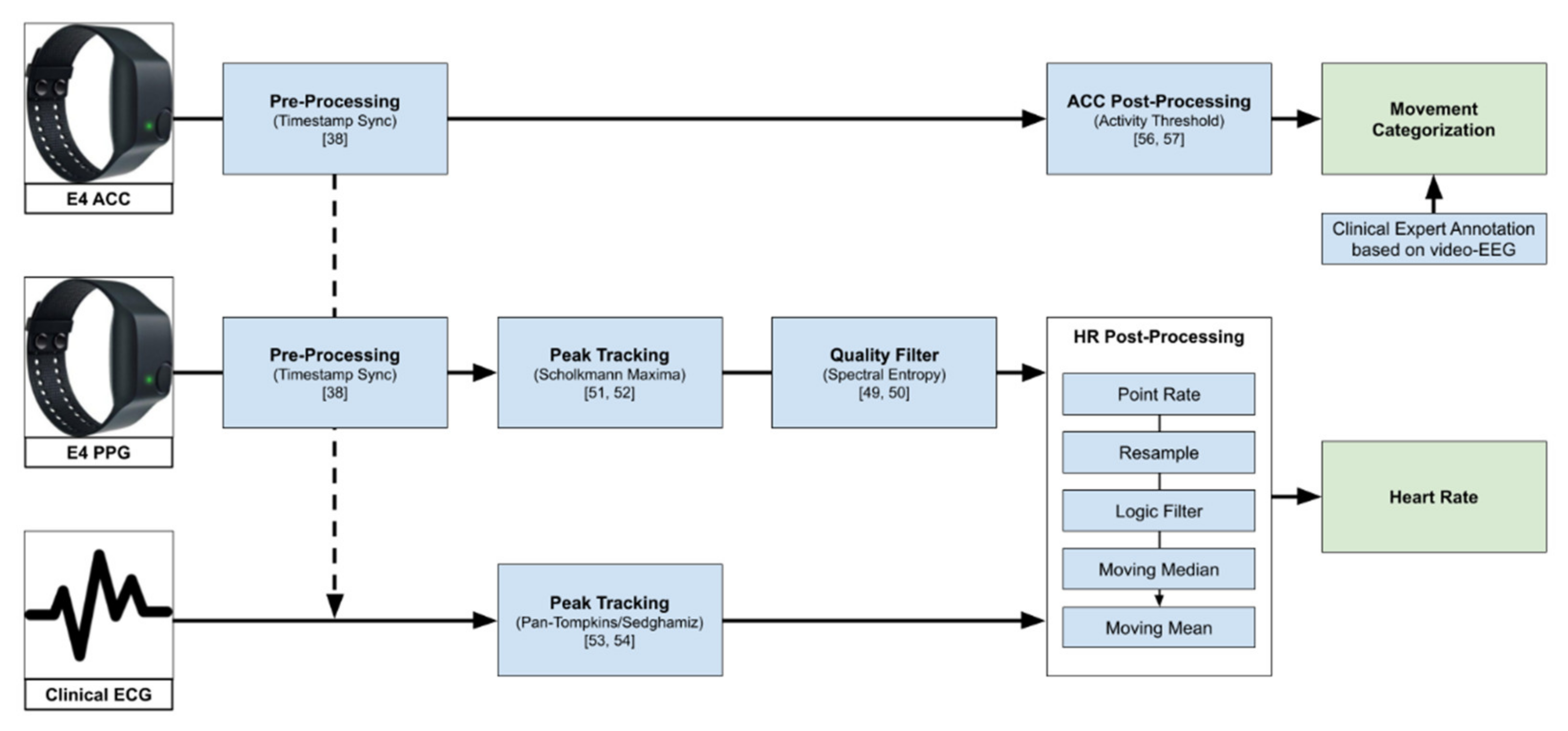
2.1. Data Acquisition
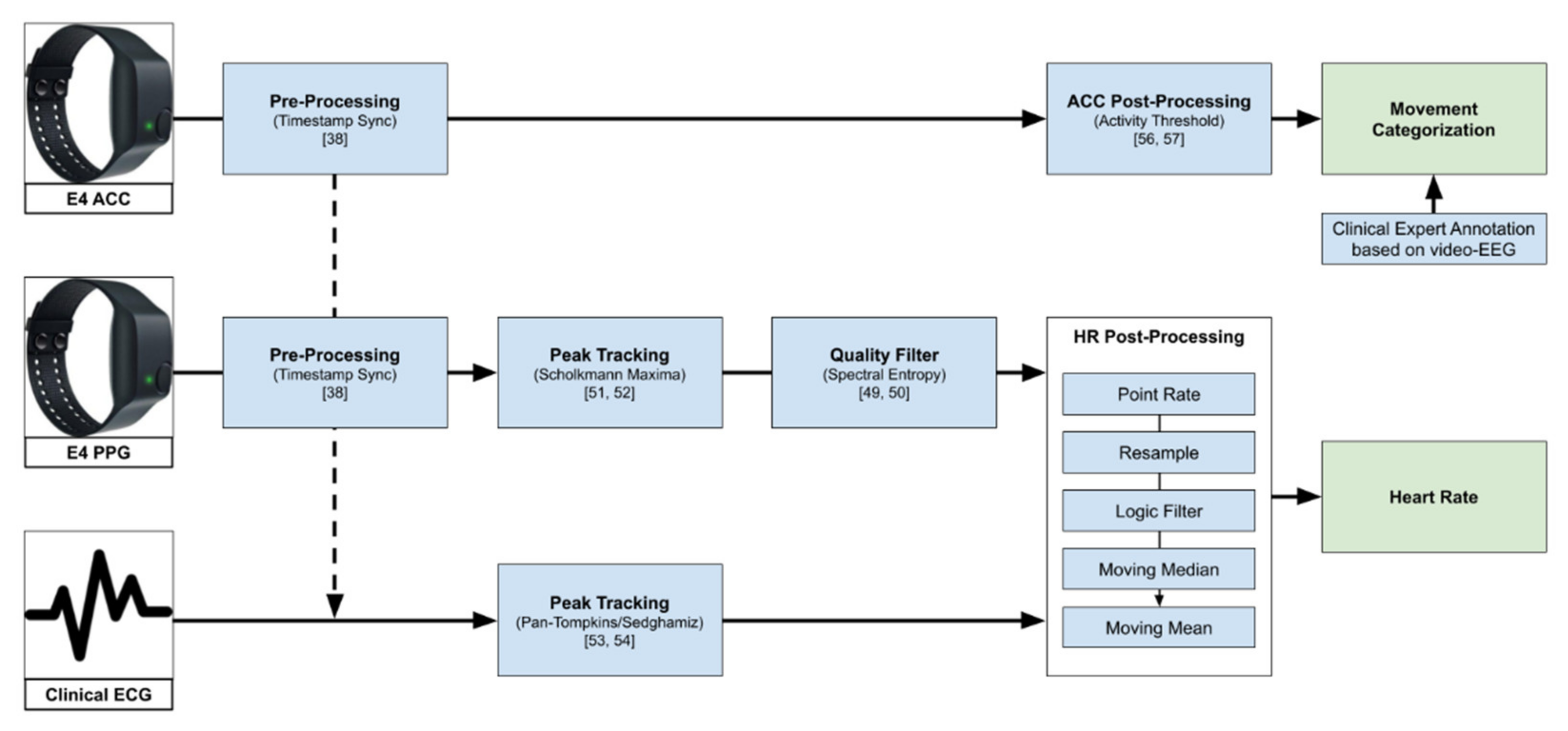
2.2. PPG Signal Quality Assessment
2.3. PPG and ECG Peak Tracker
2.4. Derivation of the ECG and PPG HR
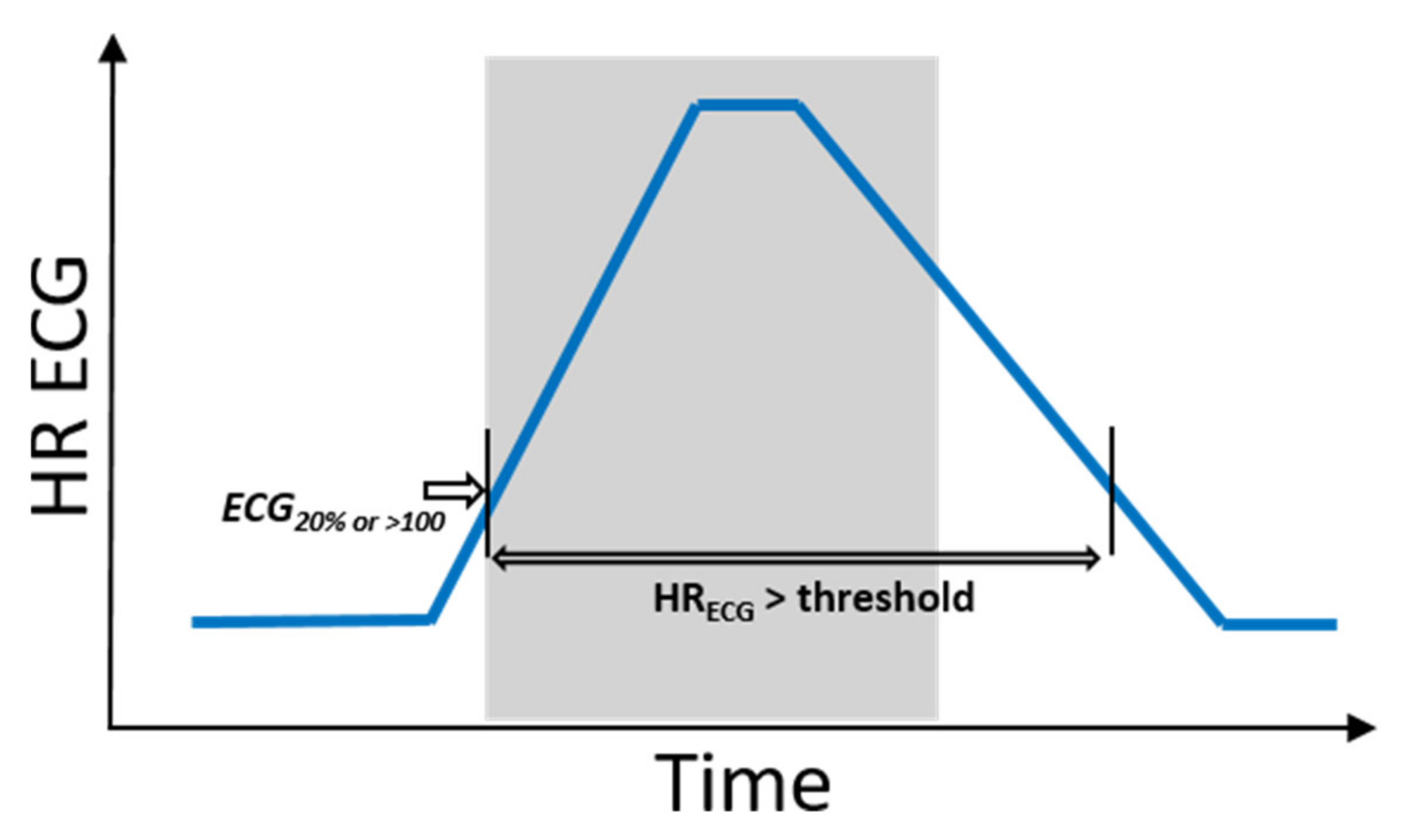
2.5. Determination of the Threshold Crossings
2.6. Definitions of Movement
2.7. Evaluation of ‘Hits’ and ‘Misses’
3. Results
3.1. Overall PPG-Based Identification
3.2. Identification Based on Seizure Groups
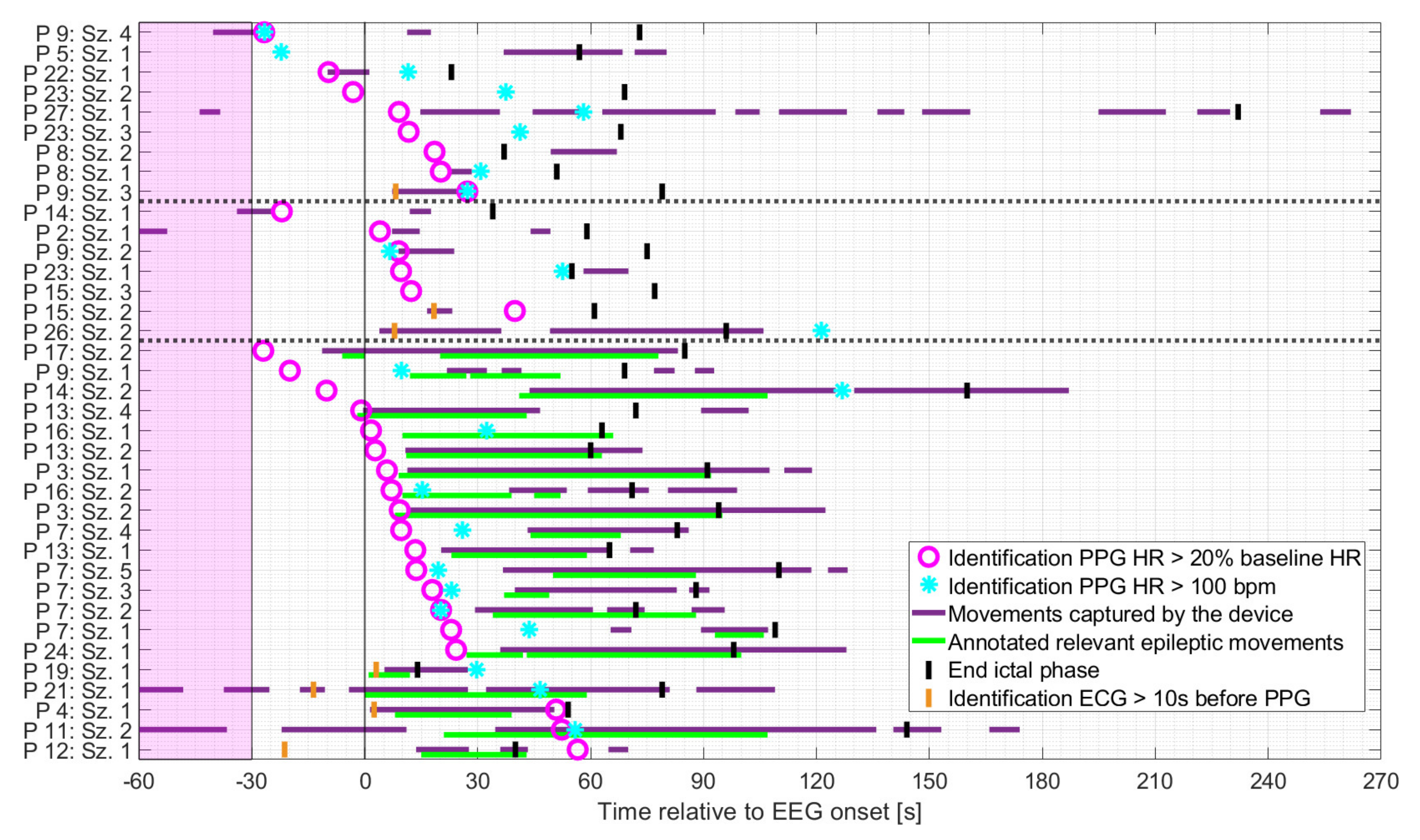
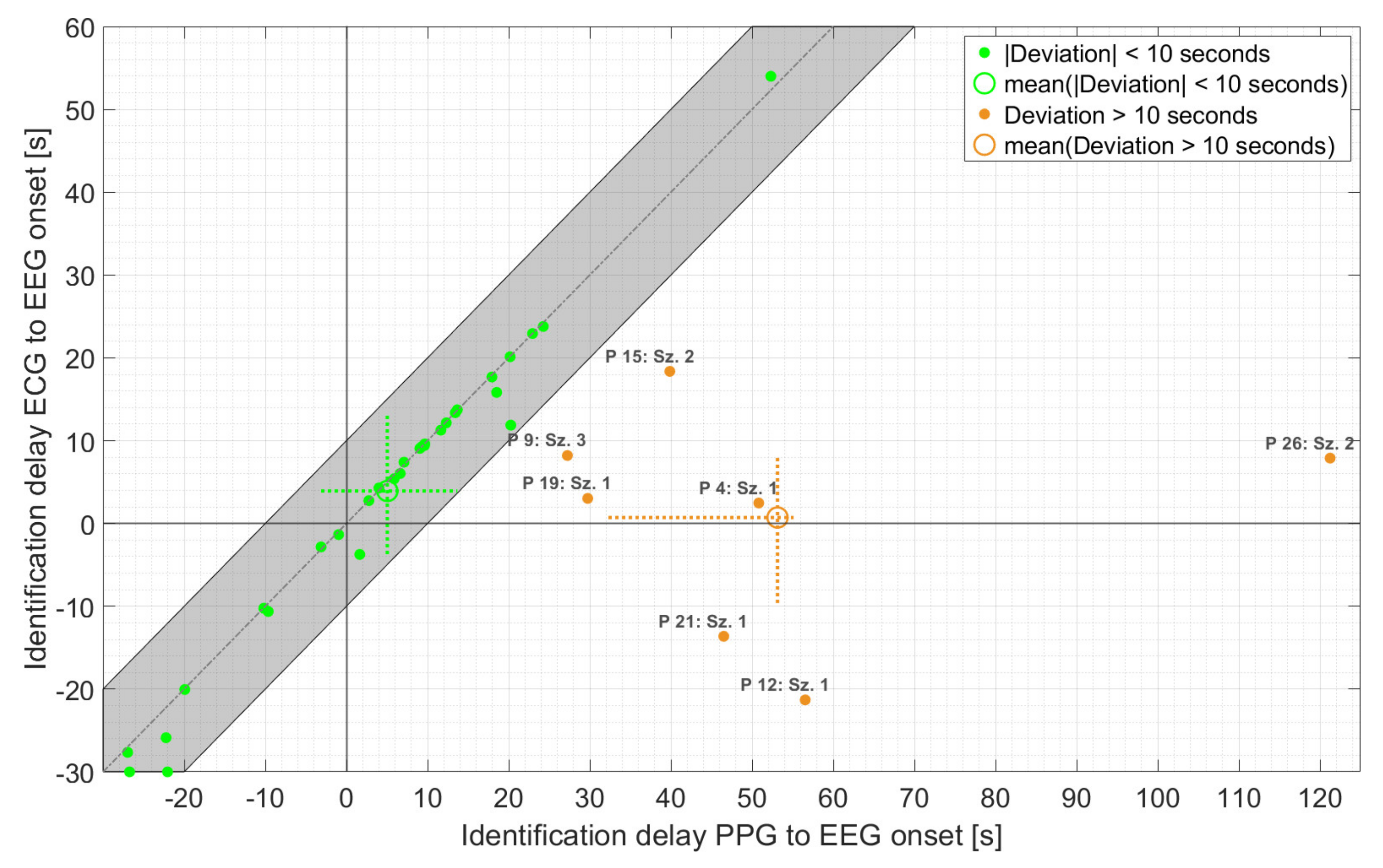
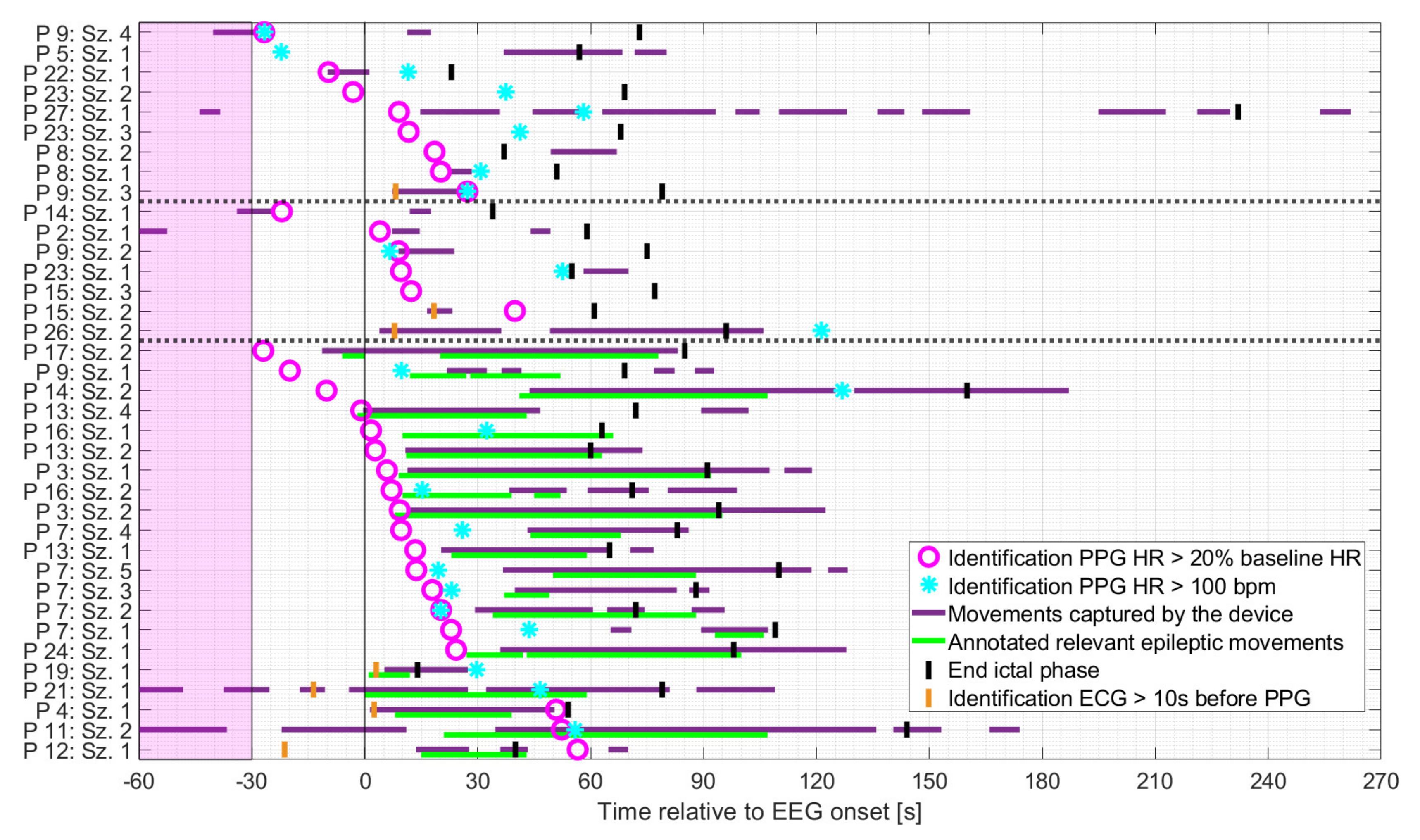
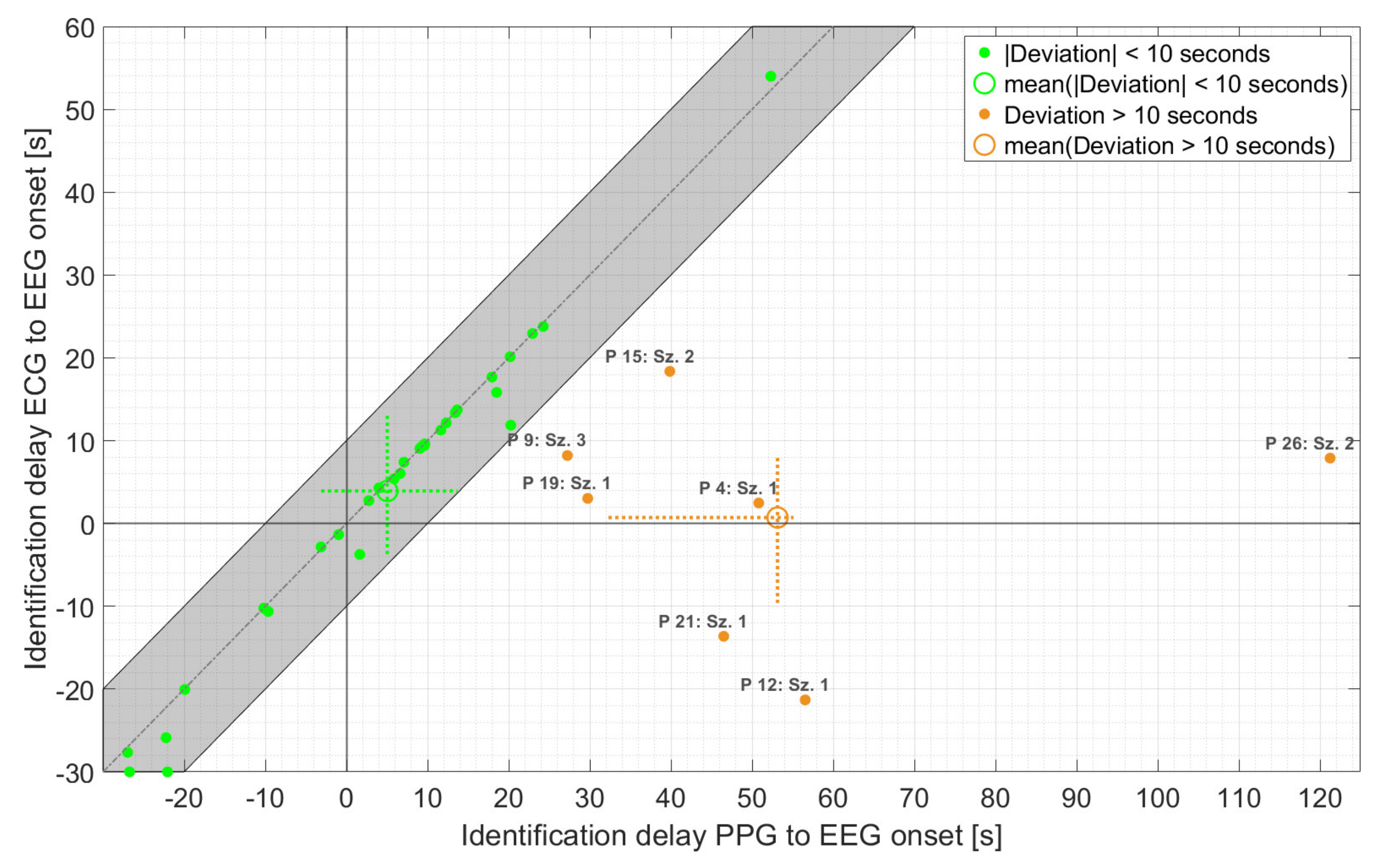
3.3. Timings of Identification
3.4. Impact of Movement on PPG-Based Identification
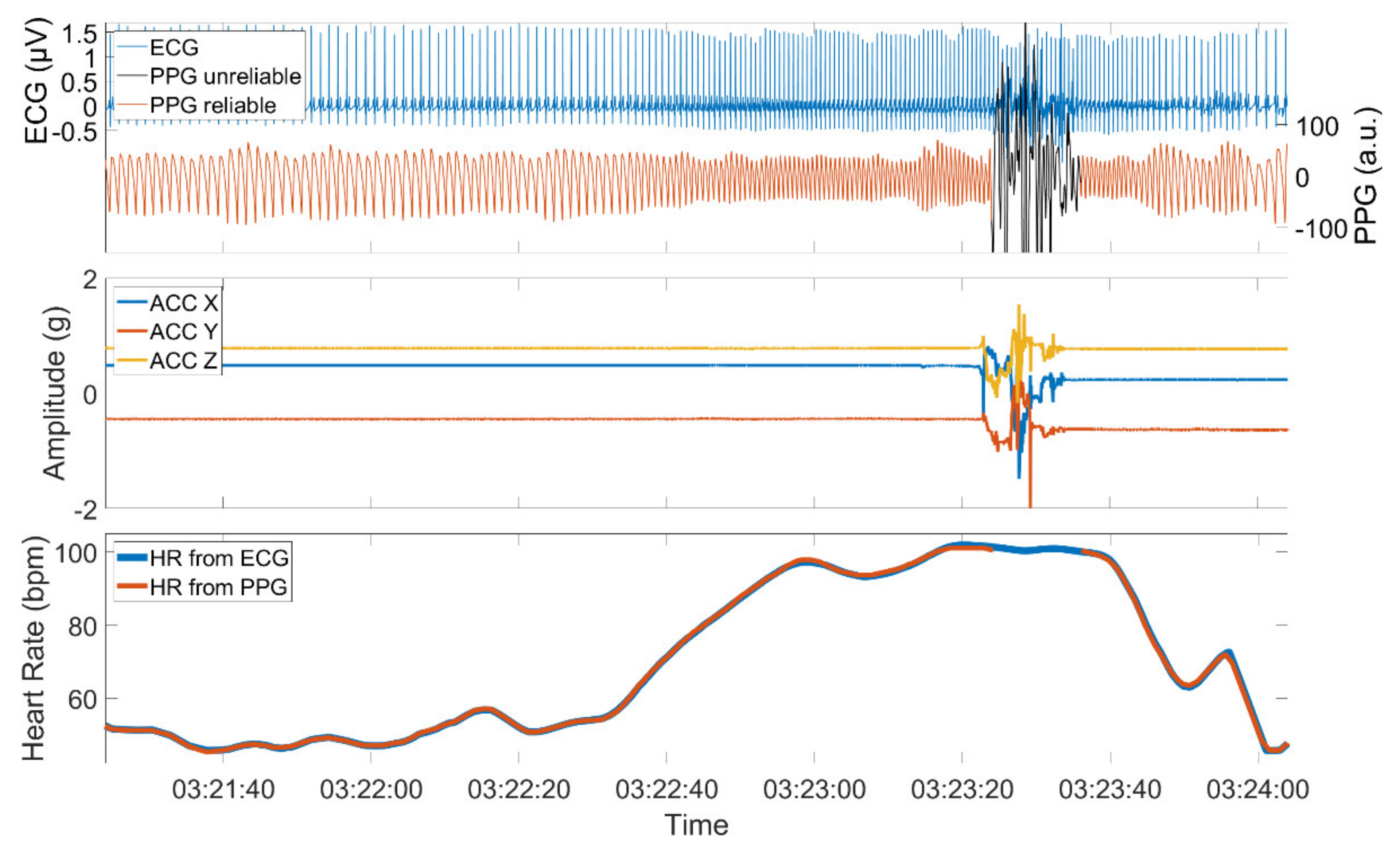
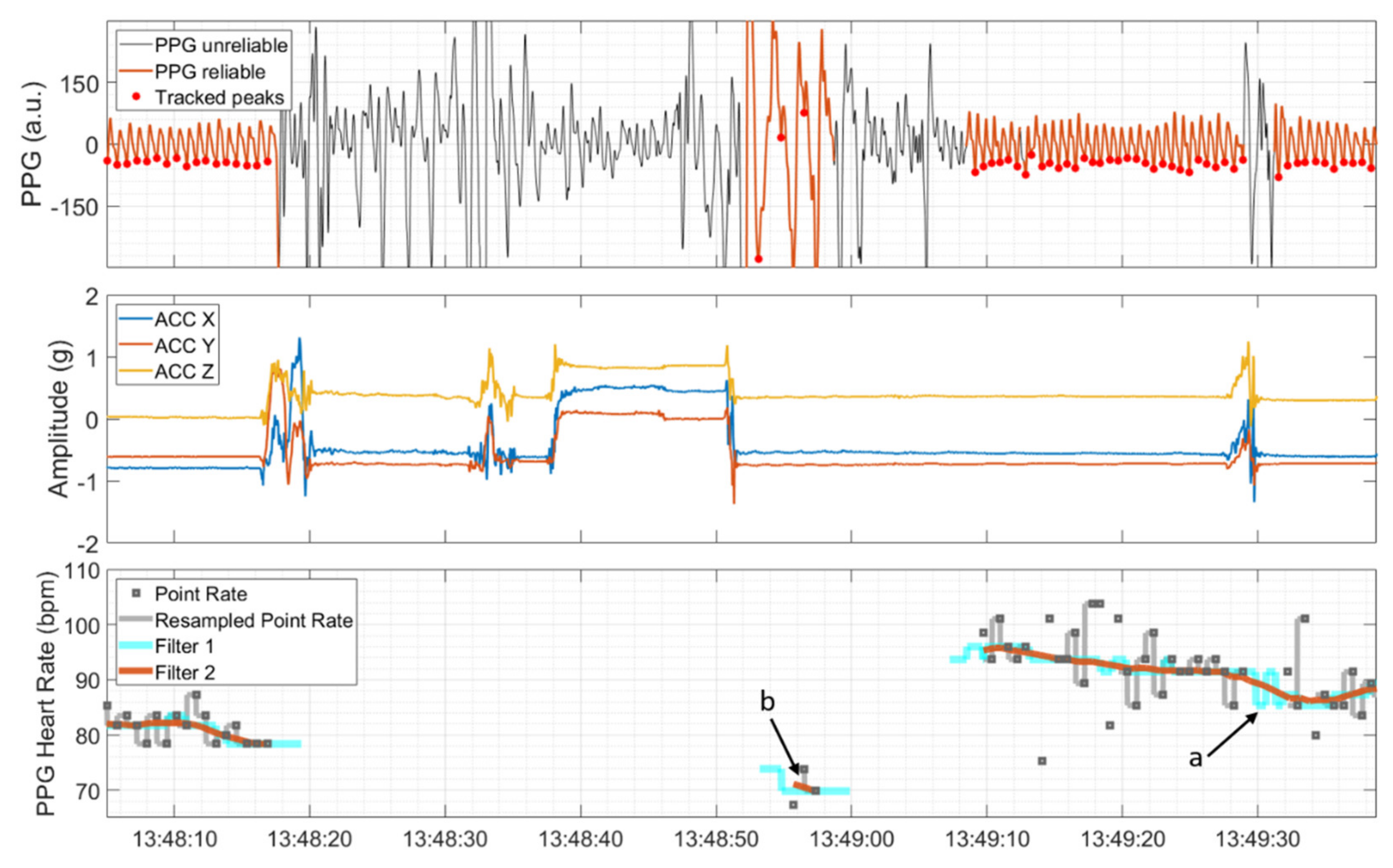
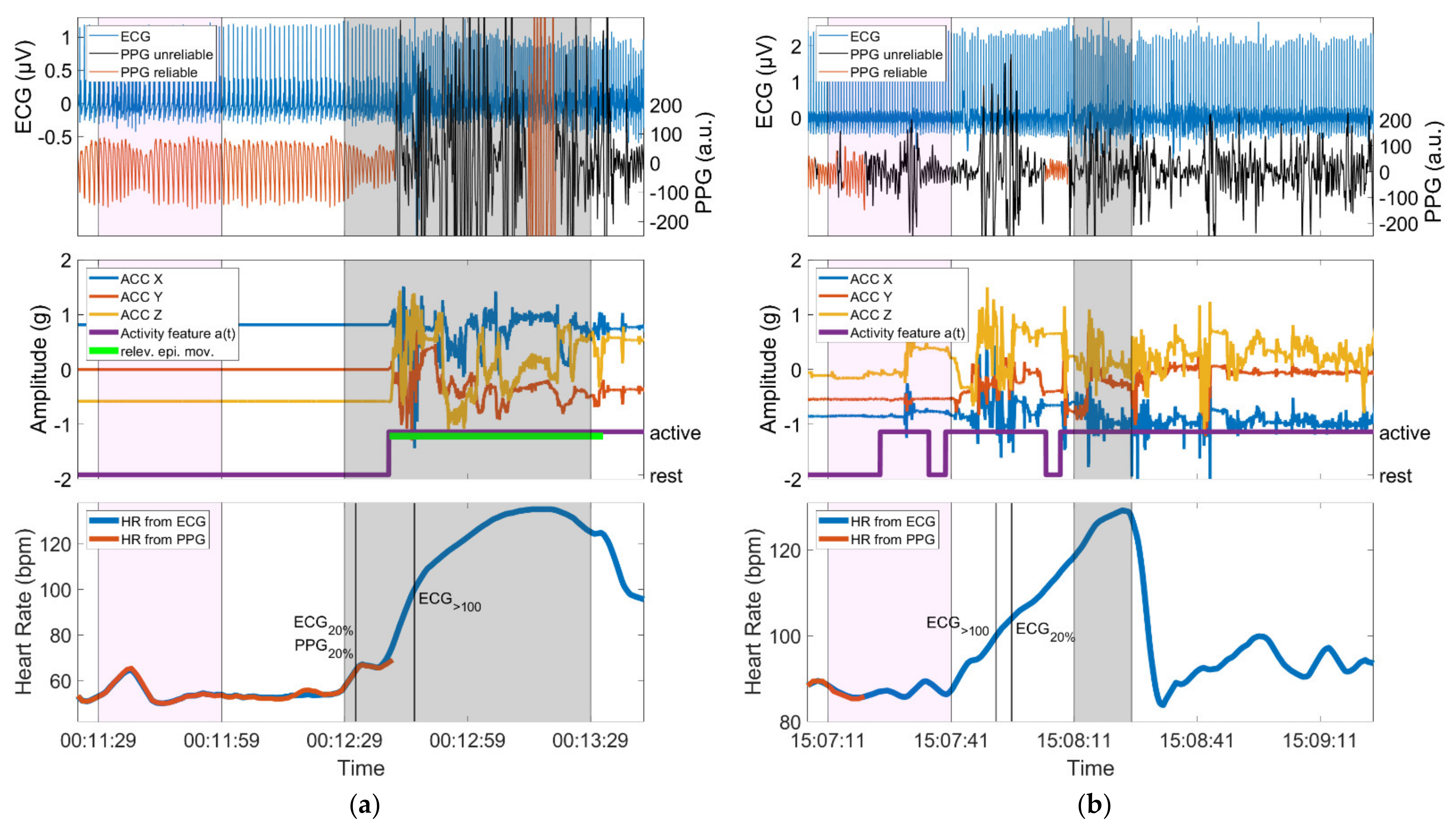
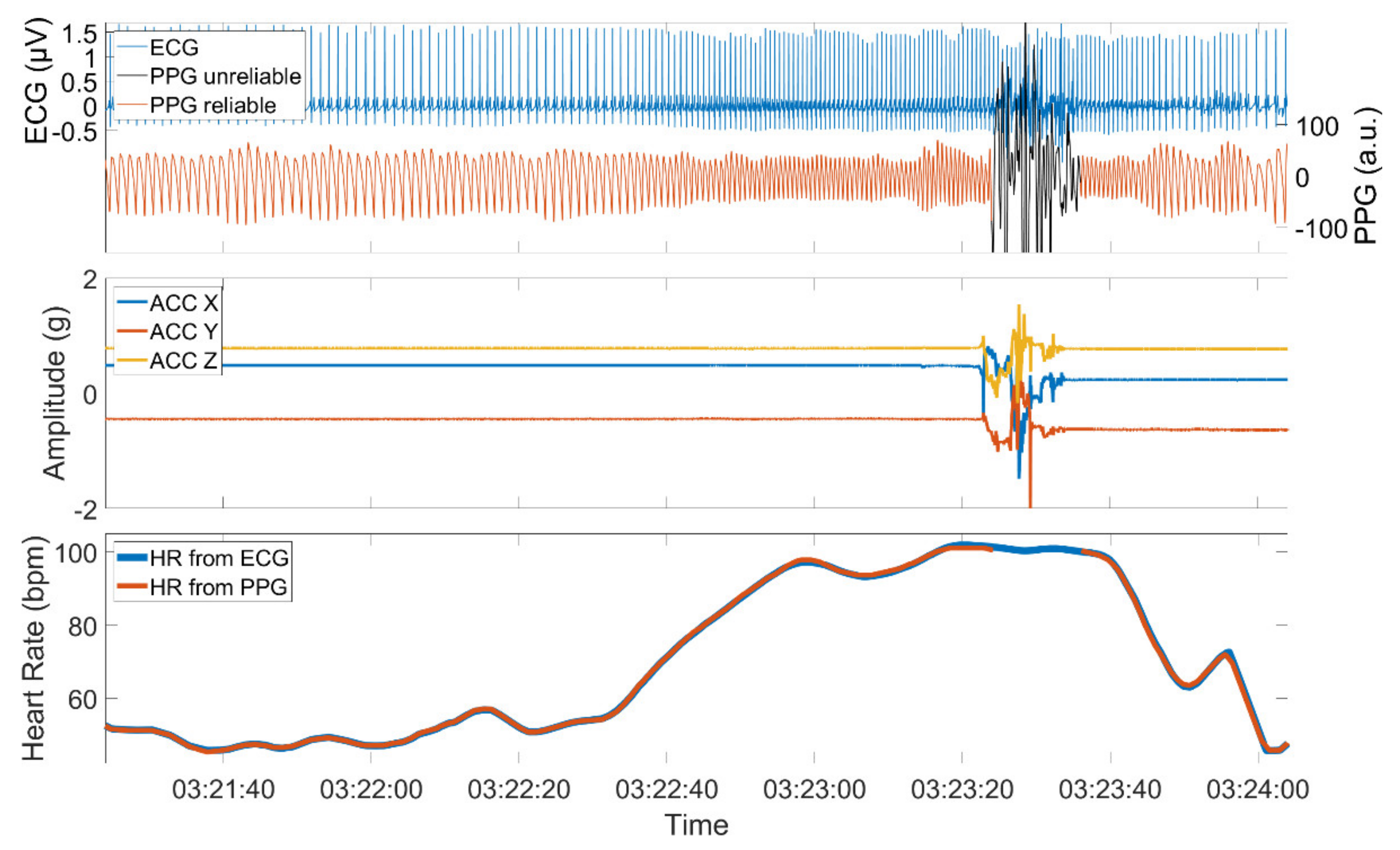
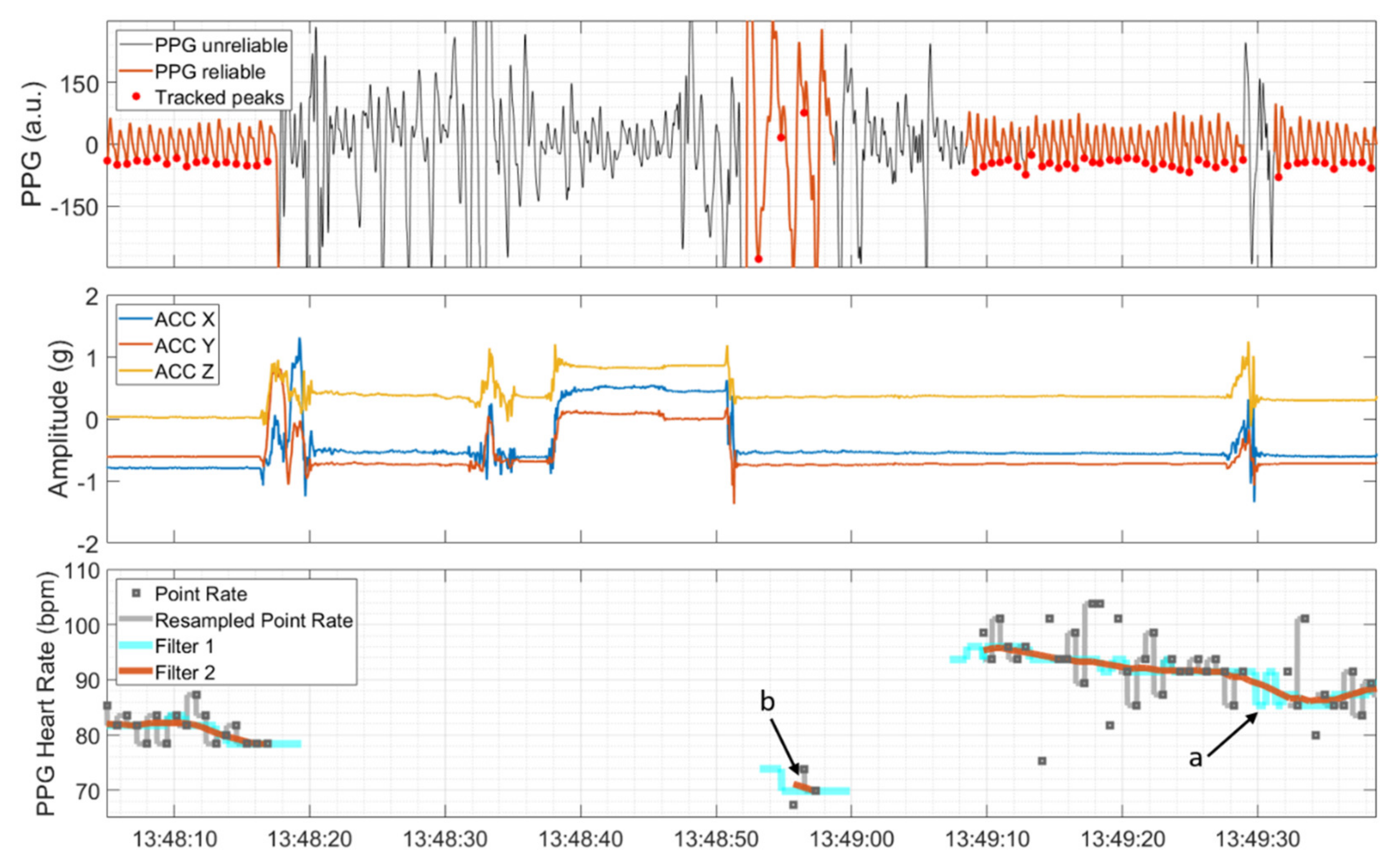
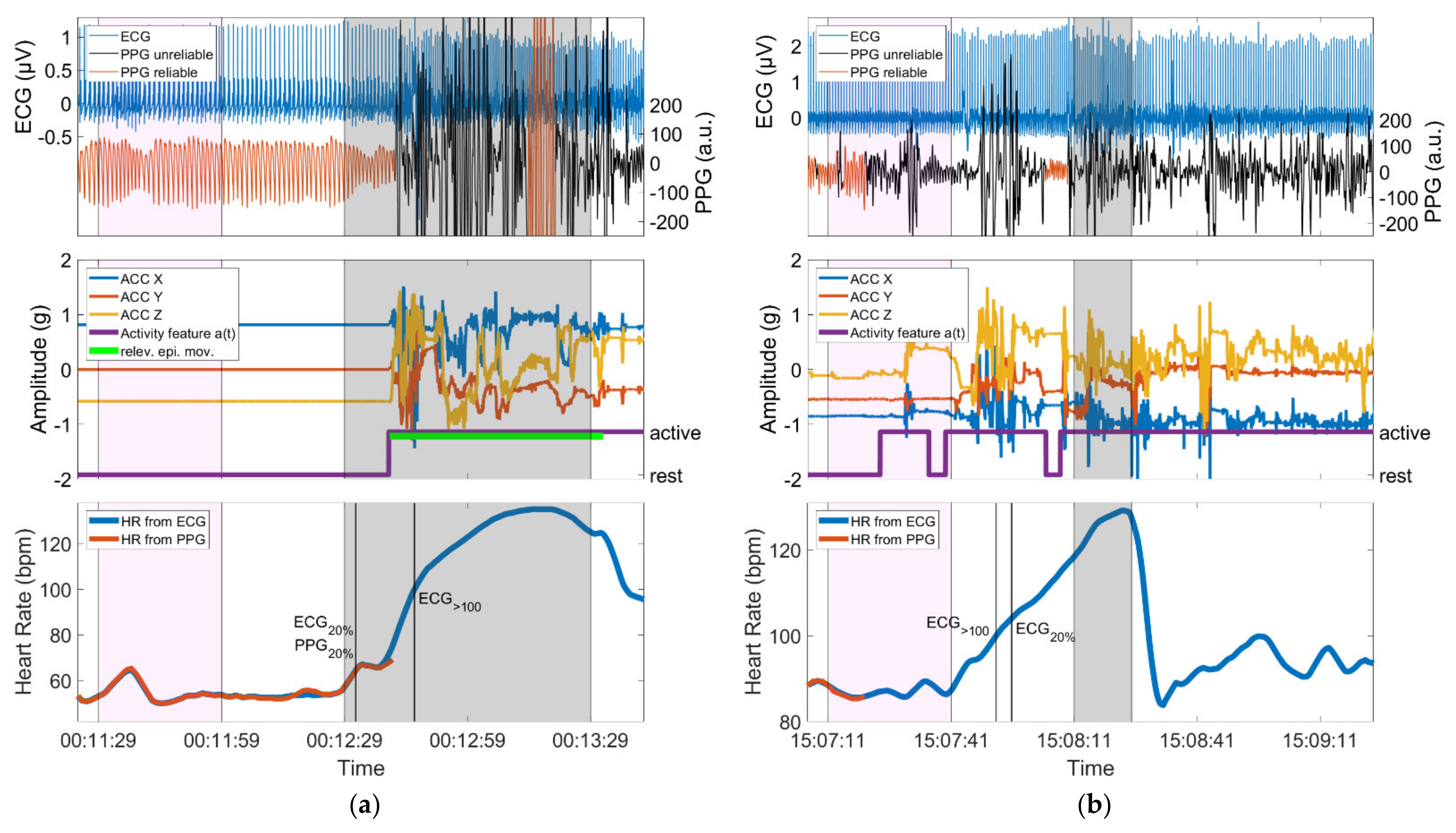
3.5. Examples
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age | Gender | Recording Duration (Days) | Epilepsy Origin | Epilepsy Type | Number of Seizures | Seizure Duration (s) [min, max] |
|---|---|---|---|---|---|---|---|
| 1 | 33 | m | 5 | structural | focal (TLE) | 1 | 101 |
| 2 | 32 | m | 5 | structural | focal (TLE) | 1 | 59 |
| 3 | 55 | m | 5 | structural | focal (TLE) | 5 | 77 [54, 94] |
| 4 | 9 | m | 3 | structural | focal (xTLE) | 1 | 54 |
| 5 | 19 | f | 4 | structural | focal (TLE) | 1 | 57 |
| 6 | 35 | f | 5 | unknown | focal (TLE) | 1 | 83 |
| 7 | 27 | f | 5 | structural | focal (TLE) | 5 | 92 [72, 110] |
| 8 | 53 | f | 5 | structural | focal (TLE) | 3 | 40 [32, 51] |
| 9 | 14 | f | 4 | structural | focal (xTLE) | 4 | 74 [69, 79] |
| 10 | 21 | f | 8 | structural | focal (TLE) | 5 | 53 [47, 61] |
| 11 | 69 | f | 7 | structural | focal (TLE) | 2 | 153 [144, 161] |
| 12 | 35 | f | 11 | structural | focal (TLE) | 1 | 40 |
| 13 | 27 | f | 5 | structural | focal (TLE) | 4 | 68 [60, 73] |
| 14 | 26 | f | 6 | structural | focal (TLE) | 2 | 97 [34, 160] |
| 15 | 48 | m | 14 | structural | focal (TLE) | 3 | 69 [61, 77] |
| 16 | 68 | f | 6 | structural | focal (TLE) | 2 | 67 [63, 71] |
| 17 | 34 | f | 4 | unknown | focal (TLE) | 2 | 71 [56, 85] |
| 18 | 56 | m | 8 | structural | focal (TLE) | 1 | 116 |
| 19 | 16 | m | 3 | structural | focal (TLE) | 1 | 14 |
| 20 | 26 | m | 6 | structural | focal (xTLE) | 5 | 118 [107, 123] |
| 21 | 48 | m | 8 | structural | focal (TLE) | 1 | 79 |
| 22 | 45 | m | 4 | structural | focal (TLE) | 1 | 23 |
| 23 | 41 | f | 8 | structural | focal (TLE) | 4 | 57 [37, 69] |
| 24 | 46 | f | 11 | structural | focal (TLE) | 1 | 98 |
| 25 | 25 | m | 4 | structural | focal (xTLE) | 1 | 162 |
| 26 | 58 | f | 7 | structural | focal (TLE) | 2 | 76 [55, 96] |
| 27 | 22 | m | 7 | structural | focal (TLE) | 1 | 232 |
| 28 | 27 | f | 8 | structural | focal (xTLE) | 1 | 14 |
| Motor Type | Hits Based on Either PPG20% or PPG>100 or Both | Misses Based on PPG | |
|---|---|---|---|
| Seizures with non-relevant epileptic movements | oral automatism | 6 | 1 |
| eye blinking | 1 | - | |
| Seizures with relevant epileptic movements | automatism | 9 | 1 |
| automatism, other | 2 | 2 | |
| automatism, clonic | 1 | 1 | |
| tonic, clonic | 3 | 3 | |
| tonic | 2 | 1 | |
| tonic, other | 2 | - | |
| to bilateral tonic-clonic | 1 | 1 | |
| to bilateral tonic-clonic, automatism | - | 2 | |
| to bilateral tonic-clonic, clonic, automatism | - | 1 | |
| to bilateral tonic-clonic, other | 1 | - | |
| other | - | 2 |

References
- Hoppe, C.; Feldmann, M.; Blachut, B.; Surges, R.; Elger, C.E.; Helmstaedter, C. Novel techniques for automated seizure registration: Patients’ wants and needs. Epilepsy Behav. 2015, 52, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Bruno, E.; Simblett, S.; Lang, A.; Biondi, A.; Odoi, C.; Schulze-Bonhage, A.; Wykes, T.; Richardson, M.P. Wearable technology in epilepsy: The views of patients, caregivers, and healthcare professionals. Epilepsy Behav. 2018, 85, 141–149. [Google Scholar] [CrossRef] [Green Version]
- Bruno, E.; Biondi, A.; Böttcher, S.; Lees, S.; Schulze-Bonhage, A.; Richardson, M.P. Day and night comfort and stability on the body of four wearable devices for seizure detection: A direct user-experience. Epilepsy Behav. 2020, 112, 107478. [Google Scholar] [CrossRef]
- Ulate-Campos, A.; Coughlin, F.; Gaínza-Lein, M.; Fernández, I.S.; Pearl, P.L.; Loddenkemper, T. Automated seizure detection systems and their effectiveness for each type of seizure. Seizure 2016, 40, 88–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Vel, A.; Cuppens, K.; Bonroy, B.; Milosevic, M.; Jansen, K.; Van Huffel, S.; Vanrumste, B.; Cras, P.; Lagae, L.; Ceulemans, B. Non-EEG seizure detection systems and potential SUDEP prevention: State of the art: Review and update. Seizure 2016, 41, 141–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halford, J.J.; Sperling, M.R.; Nair, D.R.; Dlugos, D.J.; Tatum, W.O.; Harvey, J.; French, J.A.; Pollard, J.R.; Faught, E.; Noe, K.H.; et al. Detection of generalized tonic–clonic seizures using surface electromyographic monitoring. Epilepsia 2017, 58, 1861–1869. [Google Scholar] [CrossRef] [Green Version]
- Arends, J.; Thijs, R.D.; Gutter, T.; Ungureanu, C.; Cluitmans, P.; Van Dijk, J.; Van Andel, J.; Tan, F.; De Weerd, A.; Vledder, B.; et al. Multimodal nocturnal seizure detection in a residential care setting A long-term prospective trial. Neurology 2018, 91, e2010–e2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poh, M.-Z.; Loddenkemper, T.; Reinsberger, C.; Swenson, N.C.; Goyal, S.; Madsen, J.R.; Picard, R.W. Autonomic changes with seizures correlate with postictal EEG suppression. Neurology 2012, 78, 1868–1876. [Google Scholar] [CrossRef] [Green Version]
- Kusmakar, S.; Karmakar, C.K.; Yan, B.; O’Brien, T.J.; Muthuganapathy, R.; Palaniswami, M. Automated Detection of Convulsive Seizures Using a Wearable Accelerometer Device. IEEE Trans. Biomed. Eng. 2019, 66, 421–432. [Google Scholar] [CrossRef]
- Regalia, G.; Onorati, F.; Lai, M.; Caborni, C.; Picard, R.W. Multimodal wrist-worn devices for seizure detection and advancing research: Focus on the Empatica wristbands. Epilepsy Res. 2019, 153, 79–82. [Google Scholar] [CrossRef]
- Onorati, F.; Regalia, G.; Caborni, C.; Migliorini, M.; Bender, D.; Poh, M.-Z.Z.; Frazier, C.; Kovitch Thropp, E.; Mynatt, E.D.; Bidwell, J.; et al. Multicenter clinical assessment of improved wearable multimodal convulsive seizure detectors. Epilepsia 2017, 58, 1870–1879. [Google Scholar] [CrossRef] [Green Version]
- Böttcher, S.; Manyakov, N.V.; Epitashvili, N.; Folarin, A.; Richardson, M.P.; Dümpelmann, M.; Schulze-Bonhage, A.; Van Laerhoven, K. Using multimodal biosignal data from wearables to detect focal motor seizures in individual epilepsy patients. In Proceedings of the 6th International Workshop on Sensor-based Activity Recognition and Interaction (iWOAR ’19). Association for Computing Machinery, New York, NY, USA, 16–17 September 2019; pp. 1–6. [Google Scholar] [CrossRef]
- Böttcher, S.; Bruno, E.; Manyakov, N.V.; Epitashvili, N.; Claes, K.; Glasstetter, M.; Thorpe, S.; Lees, S.; Dümpelmann, M.; Van Laerhoven, K.; et al. Detecting Tonic-Clonic Seizures in Multimodal Biosignal Data from Wearables: Methodology Design and Validation. JMIR Mhealth Uhealth 2021, in press. [Google Scholar] [CrossRef]
- Rukasha, T.; Woolley, S.I.; Kyriacou, T.; Collins, T. Evaluation of Wearable Electronics for Epilepsy: A Systematic Review. Electronics 2020, 9, 968. [Google Scholar] [CrossRef]
- Beniczky, S.; Wiebe, S.; Jeppesen, J.; Tatum, W.O.; Brazdil, M.; Wang, Y.; Herman, S.T.; Ryvlin, P. Automated seizure detection using wearable devices: A clinical practice guideline of the International League Against Epilepsy and the International Federation of Clinical Neurophysiology. Epilepsia 2021, 62, 632–646. [Google Scholar] [CrossRef] [PubMed]
- Vandecasteele, K.; De Cooman, T.; Gu, Y.; Cleeren, E.; Claes, K.; Van Paesschen, W.; Van Huffel, S.; Hunyadi, B. Automated epileptic seizure detection based on wearable ECG and PPG in a hospital environment. Sensors 2017, 17, 2338. [Google Scholar] [CrossRef] [PubMed]
- Opherk, C.; Coromilas, J.; Hirsch, L.J. Heart rate and EKG changes in 102 seizures: Analysis of influencing factors. Epilepsy Res. 2002, 52, 117–127. [Google Scholar] [CrossRef]
- Devinsky, O. Effects of Seizures on Autonomic and Cardiovascular Function. Epilepsy Curr. 2004, 4, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Arbune, A.A.; Jeppesen, J.; Conradsen, I.; Ryvlin, P.; Beniczky, S. Peri-ictal heart rate variability parameters as surrogate markers of seizure severity. Epilepsia 2020, 61, S55–S60. [Google Scholar] [CrossRef]
- Beniczky, S.; Arbune, A.A.; Jeppesen, J.; Ryvlin, P. Biomarkers of seizure severity derived from wearable devices. Epilepsia 2020, 61, S61–S66. [Google Scholar] [CrossRef]
- Jeppesen, J.; Fuglsang-Frederiksen, A.; Johansen, P.; Christensen, J.; Wüstenhagen, S.; Tankisi, H.; Qerama, E.; Beniczky, S. Seizure detection using heart rate variability: A prospective validation study. Epilepsia 2020, 61, S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Mohammadpour Touserkani, F.; Tamilia, E.; Coughlin, F.; Hammond, S.; El Atrache, R.; Jackson, M.; Bendsen-Jensen, M.; Kim, B.; Connolly, J.; Manganaro, S.; et al. Photoplethysmographic evaluation of generalized tonic-clonic seizures. Epilepsia 2020, 61, 1606–1616. [Google Scholar] [CrossRef] [PubMed]
- Vieluf, S.; Reinsberger, C.; El Atrache, R.; Jackson, M.; Schubach, S.; Ufongene, C.; Loddenkemper, T.; Meisel, C. Autonomic nervous system changes detected with peripheral sensors in the setting of epileptic seizures. Sci. Rep. 2020, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sevcencu, C.; Struijk, J.J. Autonomic alterations and cardiac changes in epilepsy. Epilepsia 2010, 51, 725–737. [Google Scholar] [CrossRef]
- Hirsch, M.; Altenmüller, D.-M.; Schulze-Bonhage, A. Latencies from intracranial seizure onset to ictal tachycardia: A comparison to surface EEG patterns and other clinical signs. Epilepsia 2015, 56, 1639–1647. [Google Scholar] [CrossRef] [PubMed]
- Leutmezer, F.; Schernthaner, C.; Lurger, S.; Pötzelberger, K.; Baumgartner, C. Electrocardiographic changes at the onset of epileptic seizures. Epilepsia 2003, 44, 348–354. [Google Scholar] [CrossRef]
- Van Westrhenen, A.; De Cooman, T.; Lazeron, R.H.C.; Van Huffel, S.; Thijs, R.D. Ictal autonomic changes as a tool for seizure detection: A systematic review. Clin. Auton. Res. 2019, 29, 161–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eggleston, K.S.; Olin, B.D.; Fisher, R.S. Ictal tachycardia: The head-heart connection. Seizure 2014, 23, 496–505. [Google Scholar] [CrossRef] [Green Version]
- Zijlmans, M.; Flanagan, D.; Gotman, J. Heart rate changes and ECG abnormalities during epileptic seizures: Prevalence and definition of an objective clinical sign. Epilepsia 2002, 43, 847–854. [Google Scholar] [CrossRef] [Green Version]
- Di Gennaro, G.; Quarato, P.P.; Sebastiano, F.; Esposito, V.; Onorati, P.; Grammaldo, L.G.; Meldolesi, G.N.; Mascia, A.; Falco, C.; Scoppetta, C.; et al. Ictal heart rate increase precedes EEG discharge in drug-resistant mesial temporal lobe seizures. Clin. Neurophysiol. 2004, 115, 1169–1177. [Google Scholar] [CrossRef] [PubMed]
- Jansen, K.; Varon, C.; Van Huffel, S.; Lagae, L. Peri-ictal ECG changes in childhood epilepsy: Implications for detection systems. Epilepsy Behav. 2013, 29, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Bruno, E.; Biondi, A.; Richardson, M.P. Pre-ictal heart rate changes: A systematic review and meta-analysis. Seizure 2018, 55, 48–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Pan, J.; Zhang, Z.; Wu, H.; Yao, N.; Cai, D.; Xu, Y.; Zhang, J.; Sun, G.; Wang, L.; et al. Ultrasensitive skin-like wearable optical sensors based on glass micro/nanofibers. Opto-Electron. Adv. 2020, 3, 19002201–19002207. [Google Scholar] [CrossRef]
- Xu, K.; Fujita, Y.; Lu, Y.; Honda, S.; Shiomi, M.; Arie, T.; Akita, S.; Takei, K. A Wearable Body Condition Sensor System with Wireless Feedback Alarm Functions. Adv. Mater. 2021, 33, 2008701. [Google Scholar] [CrossRef]
- Taylor, S.; Jaques, N.; Chen, W.; Fedor, S.; Sano, A.; Picard, R. Automatic identification of artifacts in electrodermal activity data. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 5 November 2015; pp. 1934–1937. [Google Scholar]
- Bent, B.; Goldstein, B.A.; Kibbe, W.A.; Dunn, J.P. Investigating sources of inaccuracy in wearable optical heart rate sensors. Npj Digit. Med. 2020, 3, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruno, E.; Böttcher, S.; Viana, P.F.; Amengual-Gual, M.; Joseph, B.; Epitashvili, N.; Dümpelmann, M.; Glasstetter, M.; Biondi, A.; Laerhoven, K.; et al. Wearable devices for seizure detection: Practical experiences and recommendations from the Wearables for Epilepsy And Research (WEAR) International Study Group. Epilepsia 2021, epi.17044. [Google Scholar] [CrossRef]
- Elgendi, M. On the Analysis of Fingertip Photoplethysmogram Signals. Curr. Cardiol. Rev. 2012, 8, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, R.; Natarajan, B.; Warren, S. Two-stage approach for detection and reduction of motion artifacts in photoplethysmographic data. IEEE Trans. Biomed. Eng. 2010, 57, 1867–1876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yousefi, R.; Nourani, M.; Ostadabbas, S.; Panahi, I. A motion-tolerant adaptive algorithm for wearable photoplethysmographic biosensors. IEEE J. Biomed. Health Inform. 2014, 18, 670–681. [Google Scholar] [CrossRef]
- Zhang, Z.; Pi, Z.; Liu, B. TROIKA: A general framework for heart rate monitoring using wrist-type photoplethysmographic signals during intensive physical exercise. IEEE Trans. Biomed. Eng. 2015, 62, 522–531. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z. Photoplethysmography-based heart rate monitoring in physical activities via joint sparse spectrum reconstruction. IEEE Trans. Biomed. Eng. 2015, 62, 1902–1910. [Google Scholar] [CrossRef] [Green Version]
- Ye, Y.; Cheng, Y.; He, W.; Hou, M.; Zhang, Z. Combining Nonlinear Adaptive Filtering and Signal Decomposition for Motion Artifact Removal in Wearable Photoplethysmography. IEEE Sens. J. 2016, 16, 7133–7141. [Google Scholar] [CrossRef]
- Karlen, W.; Raman, S.; Ansermino, J.M.; Dumont, G.A. Multiparameter respiratory rate estimation from the photoplethysmogram. IEEE Trans. Biomed. Eng. 2013, 60, 1946–1953. [Google Scholar] [CrossRef] [PubMed]
- Orphanidou, C.; Bonnici, T.; Charlton, P.; Clifton, D.; Vallance, D.; Tarassenko, L. Signal-quality indices for the electrocardiogram and photoplethysmogram: Derivation and applications to wireless monitoring. IEEE J. Biomed. Health Inform. 2015, 19, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Elgendi, M. Optimal signal quality index for photoplethysmogram signals. Bioengineering 2016, 3, 21. [Google Scholar] [CrossRef] [Green Version]
- Selvaraj, N.; Mendelson, Y.; Shelley, K.H.; Silverman, D.G.; Chon, K.H. Statistical approach for the detection of motion/noise artifacts in Photoplethysmogram. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Boston, MA, USA, 1 December 2011; pp. 4972–4975. [Google Scholar]
- Nasseri, M.; Nurse, E.; Glasstetter, M.; Böttcher, S.; Gregg, N.M.; Laks Nandakumar, A.; Joseph, B.; Pal Attia, T.; Viana, P.F.; Bruno, E.; et al. Signal quality and patient experience with wearable devices for epilepsy management. Epilepsia 2020, 61, S25–S35. [Google Scholar] [CrossRef] [PubMed]
- Harris, F.J. On the Use of Windows for Harmonic Analysis with the Discrete Fourier Transform. Proc. IEEE 1978, 66, 51–83. [Google Scholar] [CrossRef]
- Scholkmann, F.; Boss, J.; Wolf, M. An efficient algorithm for automatic peak detection in noisy periodic and quasi-periodic signals. Algorithms 2012, 5, 588–603. [Google Scholar] [CrossRef] [Green Version]
- Wójcikowski, M.; Pankiewicz, B. Photoplethysmographic time-domain heart rate measurement algorithm for resource-constrained wearable devices and its implementation. Sensors 2020, 20, 1783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, BME-32, 230–236. [Google Scholar] [CrossRef]
- Sedghamiz, H. Matlab Implementation of Pan Tompkins ECG QRS Detector. 2014, 1–3. Available online: https://www.researchgate.net/publication/313673153_Matlab_Implementation_of_Pan_Tompkins_ECG_QRS_detector (accessed on 3 September 2021). [CrossRef]
- Bruno, E.; Biondi, A.; Richardson, M.P.; On behalf of the RADAR-CNS Consortium. Digital semiology and time-evolution pattern of bio-signals in focal onset motor seizures. Seizure 2021, 87, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Parkka, J.; Ermes, M.; Korpipaa, P.; Mantyjarvi, J.; Peltola, J.; Korhonen, I. Activity Classification Using Realistic Data From Wearable Sensors. IEEE Trans. Inf. Technol. Biomed. 2006, 10, 119–128. [Google Scholar] [CrossRef]
- Bruno, E.; Böttcher, S.; Biondi, A.; Epitashvili, N.; Manyakov, N.V.; Lees, S.; Schulze-Bonhage, A.; Richardson, M.P. Post-ictal accelerometer silence as a marker of post-ictal immobility. Epilepsia 2020, 61, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- Guggisberg, A.G.; Hess, C.W.; Mathis, J. The significance of the sympathetic nervous system in the pathophysiology of periodic leg movements in sleep. Sleep 2007, 30, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Calandra-Buonaura, G.; Toschi, N.; Provini, F.; Corazza, I.; Bisulli, F.; Barletta, G.; Vandi, S.; Montagna, P.; Guerrisi, M.; Tinuper, P.; et al. Physiologic autonomic arousal heralds motor manifestations of seizures in nocturnal frontal lobe epilepsy: Implications for pathophysiology. Sleep Med. 2012, 13, 252–262. [Google Scholar] [CrossRef]
- San Antonio-Arce, V.; Schulze-Bonhage, A. Ictal tachycardia in patients with hypothalamic hamartoma. J. Neurol. Neurosurg. Psychiatry 2015, 86, 1163–1164. [Google Scholar] [CrossRef]
- De Cooman, T.; Varon, C.; Van De Vel, A.; Ceulemans, B.; Lagae, L.; Van Huffel, S. Semi-supervised one-class transfer learning for heart rate based epileptic seizure detection. In Proceedings of the Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017; pp. 1–4. [Google Scholar]
- Berens, P. CircStat: A MATLAB Toolbox for Circular Statistics. J. Stat. Softw. 2009, 31, 293–295. [Google Scholar] [CrossRef] [Green Version]


| Hits Based on PPG | Misses Based on PPG | Total ECG Thresholds | ||
|---|---|---|---|---|
| Identifications | 20% increase or >100 bpm | 37 (60%) | 25 (40%) | 62 |
| 20% increase | 33 (53%) | 29 (47%) | 62 | |
| >100 bpm | 23 (45%) | 28 (55%) | 51 |
| Hits Based on PPG20% or PPG>100 37/62 | Misses Based on PPG 25/62 | |
|---|---|---|
| Group 1 | 9 | 10 |
| Group 2 | 7 | 1 |
| Group 3 | 21 | 14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glasstetter, M.; Böttcher, S.; Zabler, N.; Epitashvili, N.; Dümpelmann, M.; Richardson, M.P.; Schulze-Bonhage, A. Identification of Ictal Tachycardia in Focal Motor- and Non-Motor Seizures by Means of a Wearable PPG Sensor. Sensors 2021, 21, 6017. https://doi.org/10.3390/s21186017
Glasstetter M, Böttcher S, Zabler N, Epitashvili N, Dümpelmann M, Richardson MP, Schulze-Bonhage A. Identification of Ictal Tachycardia in Focal Motor- and Non-Motor Seizures by Means of a Wearable PPG Sensor. Sensors. 2021; 21(18):6017. https://doi.org/10.3390/s21186017
Chicago/Turabian StyleGlasstetter, Martin, Sebastian Böttcher, Nicolas Zabler, Nino Epitashvili, Matthias Dümpelmann, Mark P. Richardson, and Andreas Schulze-Bonhage. 2021. "Identification of Ictal Tachycardia in Focal Motor- and Non-Motor Seizures by Means of a Wearable PPG Sensor" Sensors 21, no. 18: 6017. https://doi.org/10.3390/s21186017
APA StyleGlasstetter, M., Böttcher, S., Zabler, N., Epitashvili, N., Dümpelmann, M., Richardson, M. P., & Schulze-Bonhage, A. (2021). Identification of Ictal Tachycardia in Focal Motor- and Non-Motor Seizures by Means of a Wearable PPG Sensor. Sensors, 21(18), 6017. https://doi.org/10.3390/s21186017