
BactoSpin: Novel Technology for Rapid Bacteria Detection and Antibiotic Susceptibility Testing

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
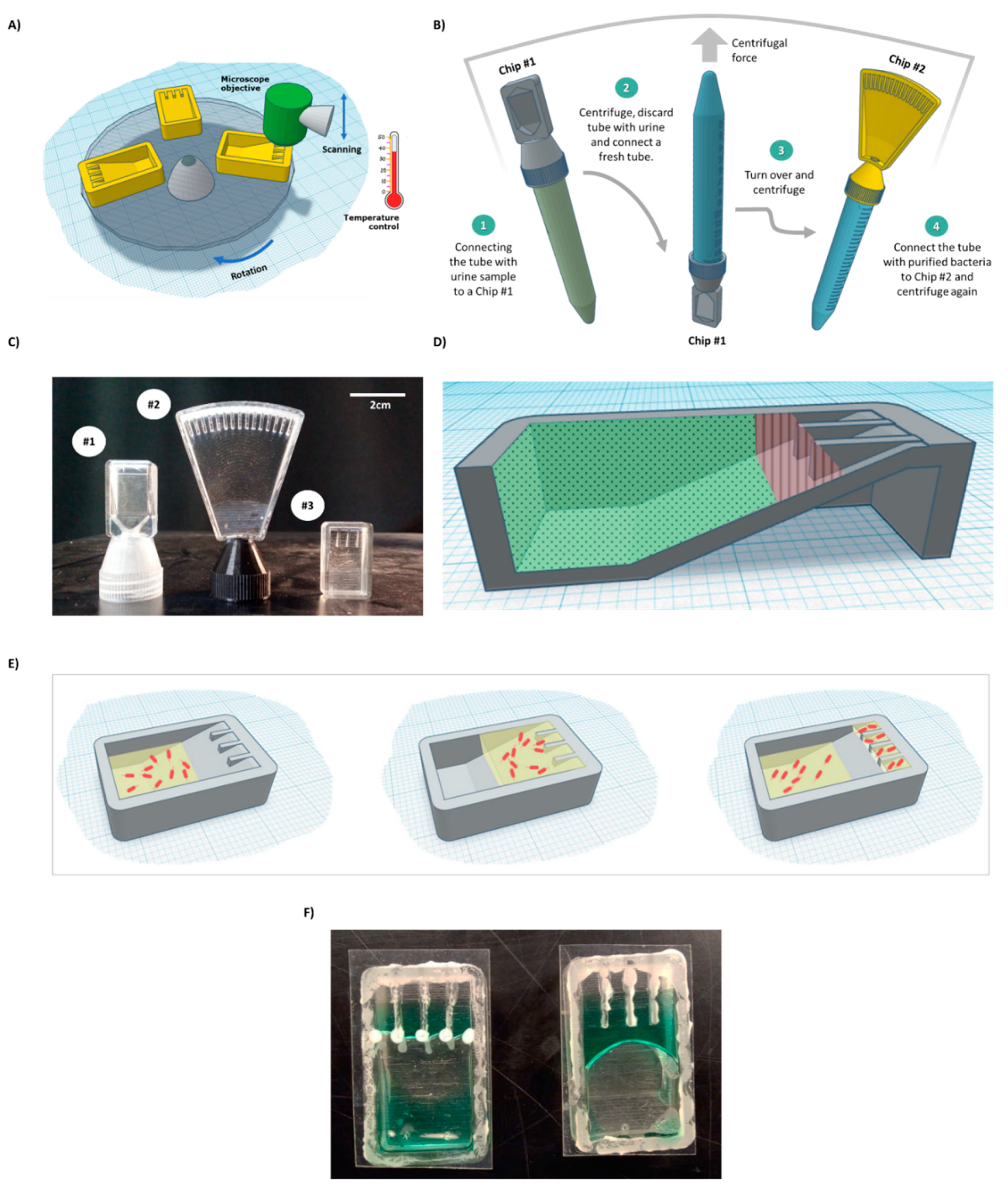
2.2. Chip Design and Production
2.3. Bacteria Detection in 10 mL Sample
2.4. Monitoring Bacterial Reaction to Antibiotics in the Chip
2.5. Machine Learning for AST
2.6. Human Urine Sample
3. Results and Discussion
3.1. System Design
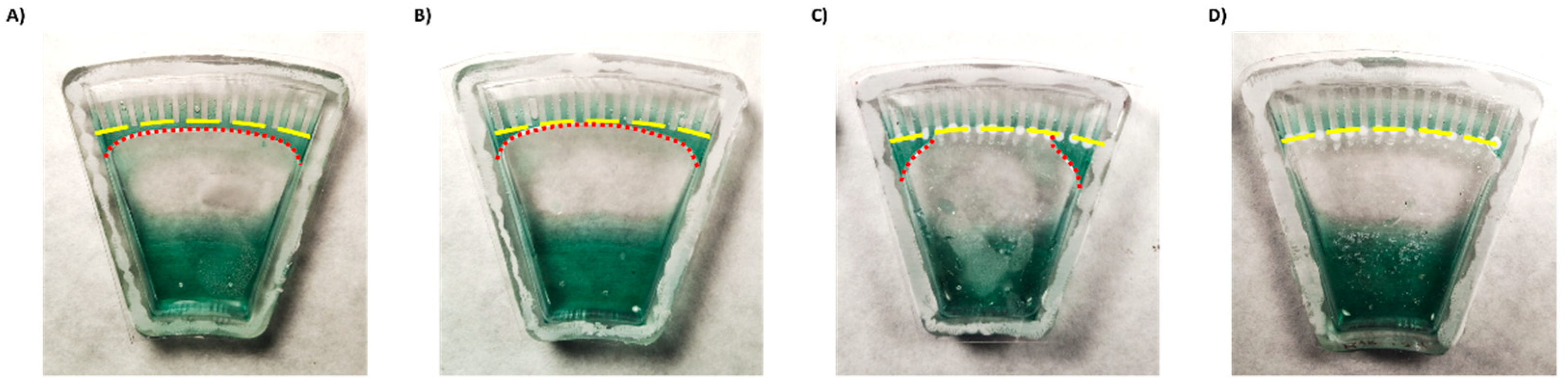
3.2. Designing a Chip for AST
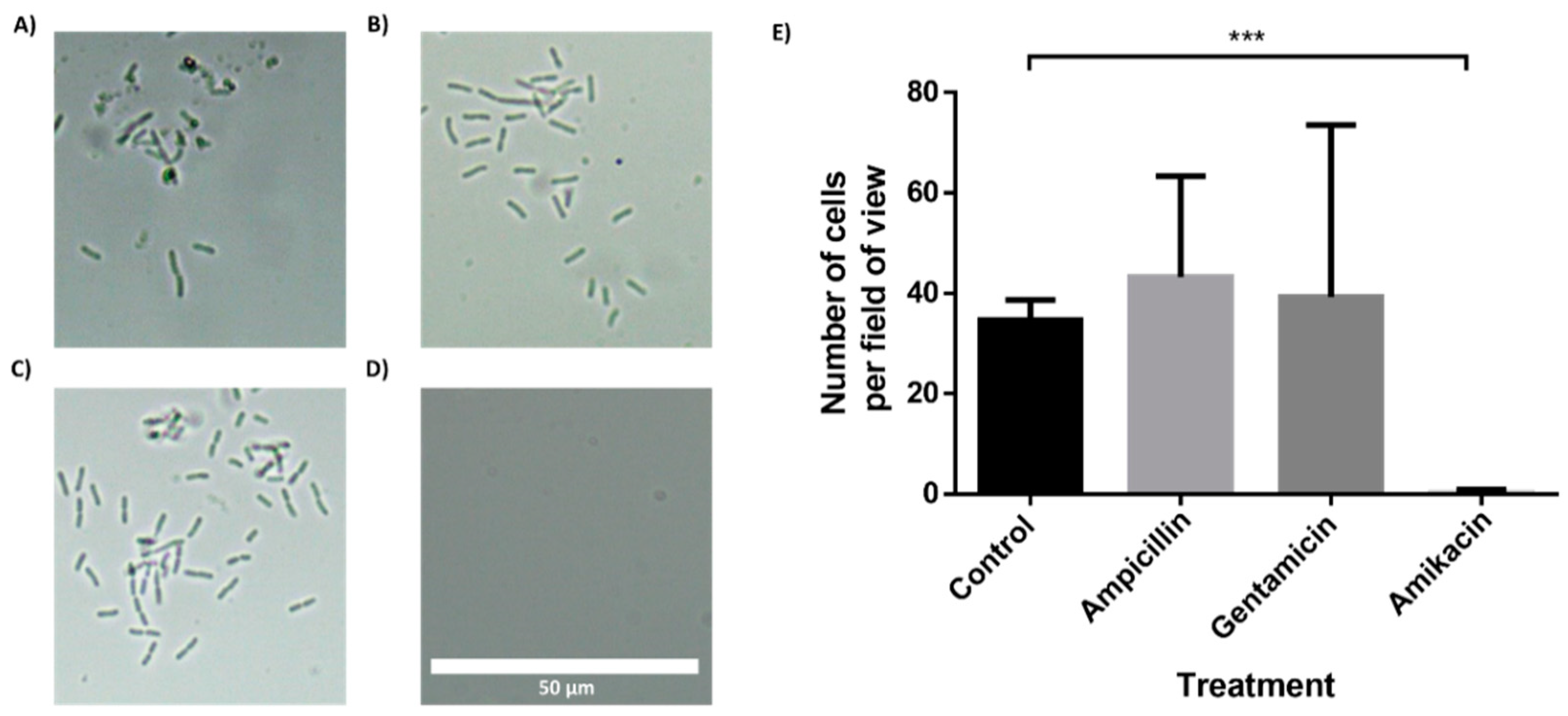
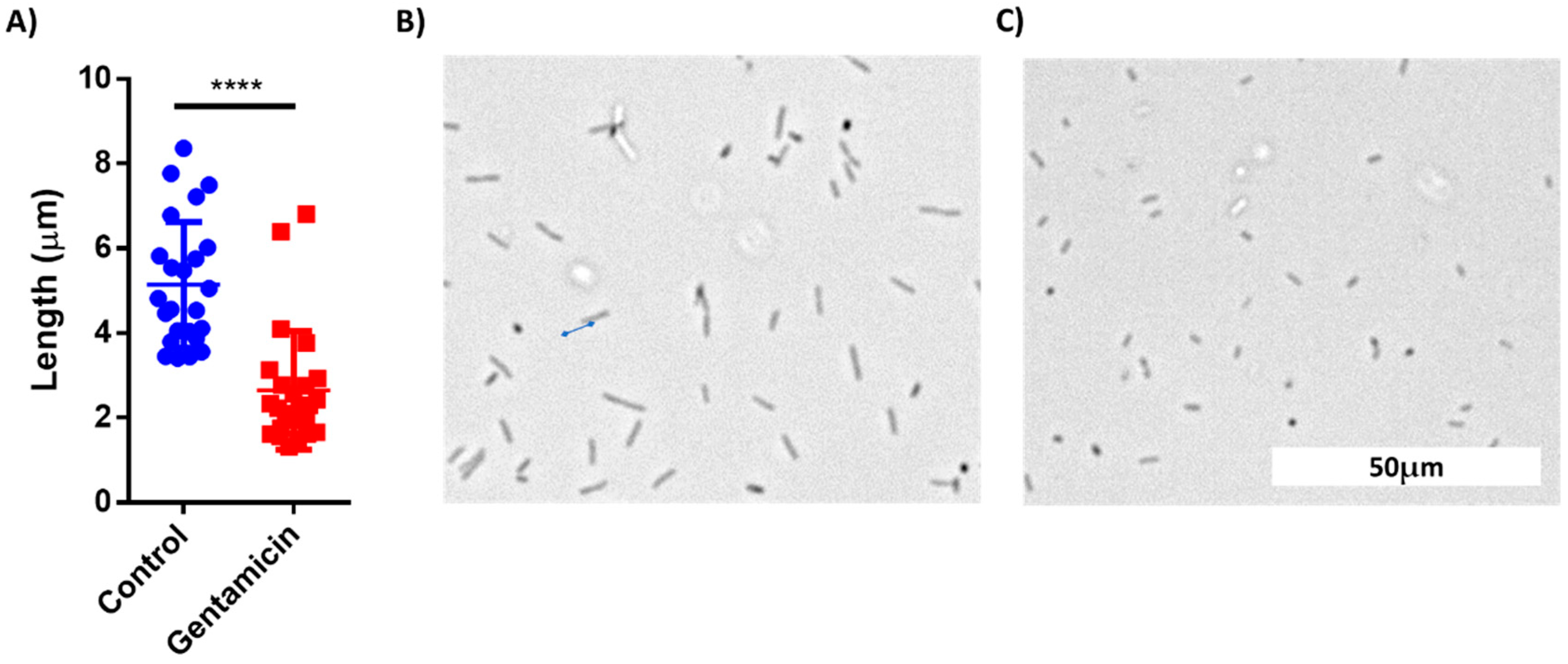
3.3. In-Chip AST of E. coli Cells
3.4. In-Chip AST of Bacteria Isolated from a Clinical Urine Sample
3.5. Application of Machine Learning for Classification of Microscopic Images of Bacterial Cells for AST
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviations | Full Name |
| UTIs | Urinary tract infections |
| AST | Antibiotic susceptibility test |
| K. pneumonia | Klebsiella pneumonia |
| E. coli | Escherichia coli |
| CDC | Disease Control and Prevention |
| GDP | Gross domestic product |
| CFUs | Colony-forming units |
| POC | Point-of-care |
| FOTS | 1H,1H,2H,2H-perfluorooctyltriethoxysilane |
| FDA | Food and Drug Administration |
| LB | Lysogeny broth |
| ResNet | Residual neural network |
| ML | Machine Learning |
References
- Centers for Disease Control and Prevention (U.S.), National Center for Emerging Zoonotic and Infectious Diseases (U.S.), Division of Healthcare Quality Promotion. Antibiotic Resistance Coordination and Strategy Unit. Antibiotic resistance threats in the United States. 2019 AR Threats Report, 2019. [Google Scholar] [CrossRef] [Green Version]
- Balouiri, M.; Sadiki, M.; Ibnsouda, S.K. Methods for in vitro evaluating antimicrobial activity: A review. J. Pharm. Anal. 2016, 6, 71–79. [Google Scholar] [CrossRef] [Green Version]
- Naylor, N.R.; Atun, R.; Zhu, N.; Kulasabanathan, K.; Silva, S.; Chatterjee, A.; Robotham, J.V. Estimating the burden of antimicrobial resistance: A systematic literature review. Antimicrob. Resist. Infect. Control 2018, 7, 58. [Google Scholar] [CrossRef]
- Dietvorst, J.; Vilaplana, L.; Uria, N.; Marco, M.P.; Muñoz-Berbel, X. Current and near-future technologies for antibiotic susceptibility testing and resistant bacteria detection. TrAC–Trends Anal. Chem. 2020, 127, 115891. [Google Scholar] [CrossRef]
- Albrich, W.C.; Monnet, D.L.; Harbarth, S. Antibiotic Selection Pressure and Resistance in Streptococcus pneumoniae and Streptococcus pyogenes. Emerg. Infect Dis. 2004, 10, 514–517. [Google Scholar] [CrossRef]
- Li, W.; Sun, E.; Wang, Y.; Pan, H.; Zhang, Y.; Li, Y.; Zhang, X.; Li, C.; Du, L.; Wang, C. Rapid Identification and Antimicrobial Susceptibility Testing for Urinary Tract Pathogens by Direct Analysis of Urine Samples Using a MALDI-TOF MS-Based Combined Protocol. Front. Microbiol. 2019, 10, 1182. [Google Scholar] [CrossRef]
- Al-Badr, A.; Al-Shaikh, G. Recurrent urinary tract infections management in women: A review. Sultan Qaboos Univ. Med. J. 2013, 13, 359–367. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, V.P.; Hannan, T.J.; Nielsen, H.V.; Hultgren, S.J. Drug and Vaccine Development for the Treatment and Prevention of Urinary Tract Infections. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Terlizzi, M.E.; Gribaudo, G.; Maffei, M.E. UroPathogenic Escherichia coli (UPEC) infections: Virulence factors, bladder responses, antibiotic, and non-antibiotic antimicrobial strategies. Front. Microbiol. 2017, 8, 1566. [Google Scholar] [CrossRef] [PubMed]
- Mambatta, A.; Rashme, V.; Menon, S.; Jayarajan, J.; Harini, S.; Kuppusamy, J. Reliability of dipstick assay in predicting urinary tract infection. J. Fam. Med. Prim. Care 2015, 4, 265. [Google Scholar] [CrossRef]
- Simati, B.; Kriegsman, B.; Safranek, S. Dipstick Urinalysis for the Diagnosis of Acute UTI. Am. Fam. Physician. 2013, 87, 10. [Google Scholar]
- Foudraine, D.E.; Bauer, M.P.; Russcher, A.; Kusters, E.; Cobbaert, C.M.; Van Der Beek, M.T.; Stalenhoef, J.E. Use of automated urine microscopy analysis in clinical diagnosis of urinary tract infection: Defining an optimal diagnostic score in an academic medical center population. J. Clin. Microbiol. 2018, 56, e02030-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraoka, M.; Hida, Y.; Tuchida, S.; Tsukahara, H.; Yamashita, M.; Kuroda, M.; Sudo, M. Diagnosis of urinary tract infection by urine microscopy using a disposable counting chamber. Scand. J. Clin. Lab. Investig. 1993, 53, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Váradi, L.; Luo, J.L.; Hibbs, D.E.; Perry, J.D.; Anderson, R.J.; Orenga, S.; Groundwater, P.W. Methods for the detection and identification of pathogenic bacteria: Past, present, and future. Chem. Soc. Rev. 2017, 46, 4818–4832. [Google Scholar] [CrossRef] [PubMed]
- Mach, K.E.; Wong, P.K.; Liao, J.C. Biosensor diagnosis of urinary tract infections: A path to better treatment? Trends Pharmacol. Sci. 2011, 32, 330–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devillé, W.L.J.M.; Yzermans, J.C.; Van Duijn, N.P.; Bezemer, P.D.; Van Der Windt, D.A.W.M.; Bouter, L.M. The urine dipstick test useful to rule out infections. A meta-analysis of the accuracy. BMC Urol. 2004, 4, 1–14. [Google Scholar] [CrossRef]
- Franco-Duarte, R.; Černáková, L.; Kadam, S.; Kaushik, K.S.; Salehi, B.; Bevilacqua, A.; Corbo, M.R.; Antolak, H.; Dybka-Stępień, K.; Leszczewicz, M.; et al. Advances in chemical and biological methods to identify microorganisms—from past to present. Microorganisms 2019, 7, 130. [Google Scholar] [CrossRef] [Green Version]
- Premasiri, W.R.; Chen, Y.; Williamson, P.M.; Bandarage, D.C.; Pyles, C.; Ziegler, L.D. Rapid urinary tract infection diagnostics by surface-enhanced Raman spectroscopy (SERS): Identification and antibiotic susceptibilities. Anal. Bioanal. Chem. 2017, 409, 3043–3054. [Google Scholar] [CrossRef]
- Behera, B.; Anil Vishnu, G.K.; Chatterjee, S.; Sitaramgupta, V.V.S.N.; Sreekumar, N.; Nagabhushan, A.; Rajendran, N.; Prathik, B.H.; Pandya, H.J. Emerging technologies for antibiotic susceptibility testing. Biosens. Bioelectron. 2019, 142, 111552. [Google Scholar] [CrossRef]
- Seng, P.; Drancourt, M.; Gouriet, F.; Scola BLa Fournier, P.E.; Rolain, J.M.; Raoult, D. Ongoing revolution in bacteriology: Routine identification of bacteria by matrix-assisted laser desorption ionization time-of-flight mass spectrometry. Clin. Infect. Dis. 2009, 49, 543–551. [Google Scholar] [CrossRef]
- Grover, W.H.; Ivester, R.H.C.; Jensen, E.C.; Mathies, R.A. Development and multiplexed control of latching pneumatic valves using microfluidic logical structures. Lab Chip 2006, 6, 623–631. [Google Scholar] [CrossRef]
- Zoval, J.V.; Madou, M.J. Centrifuge-based fluidic platforms. Proc. IEEE 2004, 92, 140–153. [Google Scholar] [CrossRef]
- Gorkin, R.; Park, J.; Siegrist, J.; Amasia, M.; Lee, B.S.; Park, J.M.; Kim, J.; Kim, H.; Madouab, M.; Cho, Y. Centrifugal microfluidics for biomedical applications. Lab Chip 2010, 10, 1758–1773. [Google Scholar] [CrossRef] [Green Version]
- Ae, J.M.C.; Huang, P.-C.; Lin, M.-G. Analysis and experiment of capillary valves for microfluidics on a rotating disk. Microfluid. Nanofluidics 2008, 4, 427–437. [Google Scholar]
- Hwang, G.B.; Patir, A.; Page, K.; Lu, Y.; Allan, E.; Parkin, I.P. Buoyancy increase and drag-reduction through a simple superhydrophobic coating. Nanoscale 2017, 9, 7588–7594. [Google Scholar] [CrossRef] [PubMed]
- FDA. Breakpoints Interpretive Categories Used for Susceptibility Testing of Salmonella and E.Coli. 2015. Available online: https://www.fda.gov/media/108180/download (accessed on 9 August 2021).
- Olafenwa, M. OlafenwaMoses/ImageAI: A Python Library Built to Empower Developers to Build Applications and Systems with Self-Contained Computer Vision Capabilities. 2018. Available online: https://github.com/OlafenwaMoses/ImageAI (accessed on 9 August 2021).
- Akagawa, Y.; Kimata, T.; Akagawa, S.; Fujishiro, S.; Kato, S.; Yamanouchi, S.; Tsuji, S.; Kino, M.; Kaneko, K. Optimal bacterial colony counts for the diagnosis of upper urinary tract infections in infants. Clin. Exp. Nephrol. 2020, 24, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Stratton, Y.-W. Advanced Techniques in Diagnostic Microbiology; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Jorgensen, J.H.; Ferraro, M.J. Antimicrobial susceptibility testing: A review of general principles and contemporary practices. Clin. Infect. Dis. 2009, 49, 1749–1755. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shumeiko, V.; Hidas, G.; Nowogrodski, C.; Pinto, Y.; Gofrit, O.; Duvdevani, M.; Shoseyov, O. BactoSpin: Novel Technology for Rapid Bacteria Detection and Antibiotic Susceptibility Testing. Sensors 2021, 21, 5902. https://doi.org/10.3390/s21175902
Shumeiko V, Hidas G, Nowogrodski C, Pinto Y, Gofrit O, Duvdevani M, Shoseyov O. BactoSpin: Novel Technology for Rapid Bacteria Detection and Antibiotic Susceptibility Testing. Sensors. 2021; 21(17):5902. https://doi.org/10.3390/s21175902
Chicago/Turabian StyleShumeiko, Vlad, Guy Hidas, Chen Nowogrodski, Yariv Pinto, Ofer Gofrit, Mordechai Duvdevani, and Oded Shoseyov. 2021. "BactoSpin: Novel Technology for Rapid Bacteria Detection and Antibiotic Susceptibility Testing" Sensors 21, no. 17: 5902. https://doi.org/10.3390/s21175902
APA StyleShumeiko, V., Hidas, G., Nowogrodski, C., Pinto, Y., Gofrit, O., Duvdevani, M., & Shoseyov, O. (2021). BactoSpin: Novel Technology for Rapid Bacteria Detection and Antibiotic Susceptibility Testing. Sensors, 21(17), 5902. https://doi.org/10.3390/s21175902