
Sensor-Based Gait Retraining Lowers Knee Adduction Moment and Improves Symptoms in Patients with Knee Osteoarthritis: A Randomized Controlled Trial

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Sample Size Estimation
2.3. Participants
2.4. Baseline Measurement
2.4.1. Biomechanical Assessment
2.4.2. Clinical Assessment
2.5. Randomization
2.5.1. Gait Retraining Group
2.5.2. Walking Exercise Group
2.6. Reassessment
2.7. Statistics
3. Results
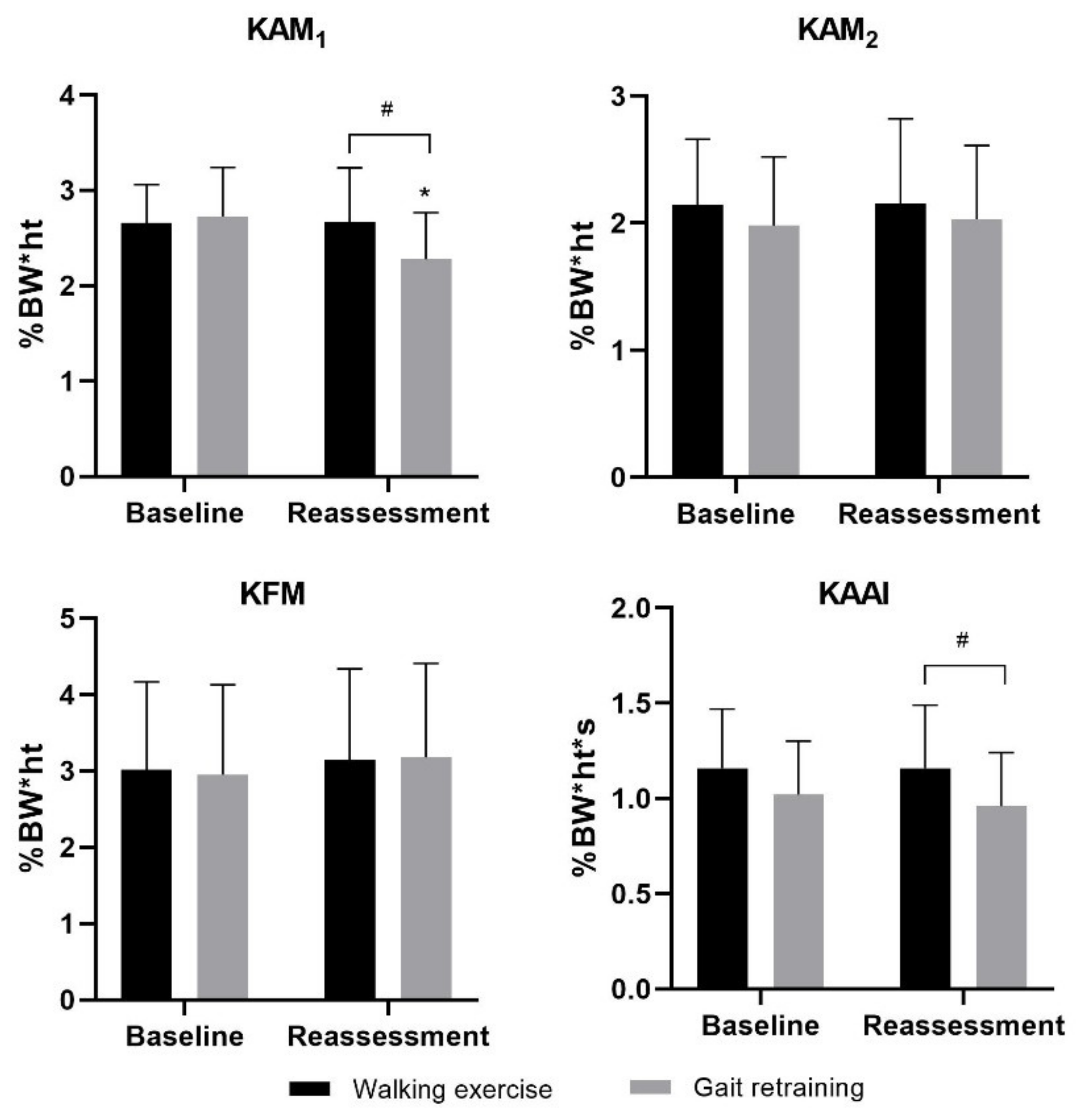
3.1. Primary Outcomes
3.2. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Woolf, A.D.; Pfleger, B. Burden of major musculoskeletal conditions. Bull. World Health Organ. 2003, 81, 646–656. [Google Scholar] [PubMed]
- Andriacchi, T.P. Dynamics of Knee Malalignment. Orthop. Clin. North Am. 1994, 25, 395–403. [Google Scholar] [CrossRef]
- Schipplein, O.D.; Andriacchi, T.P. Interaction between active and passive knee stabilizers during level walking. J. Orthop. Res. 1991, 9, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Banks, S.; Mitchell, K.H.; D’Lima, D.; Colwell, C.W.; Fregly, B.J. Correlation between the knee adduction torque and medial contact force for a variety of gait patterns. J. Orthop. Res. 2007, 25, 789–797. [Google Scholar] [CrossRef]
- Sharma, L.; Hurwitz, D.E.; Thonar, E.J.-M.A.; Sum, J.A.; Lenz, M.E.; Dunlop, D.D.; Schnitzer, T.J.; Kirwan-Mellis, G.; Andriacchi, T.P. Knee adduction moment, serum hyaluronan level, and disease severity in medial tibiofemoral osteoarthritis. Arthritis Rheum. 1998, 41, 1233–1240. [Google Scholar] [CrossRef]
- Miyazaki, T.; Wada, M.; Kawahara, H.; Sato, M.; Baba, H.; Shimada, S. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann. Rheum. Dis. 2002, 61, 617–622. [Google Scholar] [CrossRef]
- Richards, R.; Noort, J.C.V.D.; Dekker, J.; Harlaar, J. Gait Retraining With Real-Time Biofeedback to Reduce Knee Adduction Moment: Systematic Review of Effects and Methods Used. Arch. Phys. Med. Rehabil. 2017, 98, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Simic, M.; Hinman, R.; Wrigley, T.; Bennell, K.; Hunt, M.A. Gait modification strategies for altering medial knee joint load: A systematic review. Arthritis Care Res. 2010, 63, 405–426. [Google Scholar] [CrossRef]
- Wang, S.; Mo, S.; Chung, R.C.; Shull, P.B.; Ribeiro, D.C.; Cheung, R.T. How foot progression angle affects knee adduction moment and angular impulse in people with and without medial knee osteoarthritis: A meta-analysis. Arthritis Care Res. 2020. [Google Scholar] [CrossRef]
- Shull, P.B.; Silder, A.; Shultz, R.; Dragoo, J.L.; Besier, T.; Delp, S.L.; Cutkosky, M.R. Six-week gait retraining program reduces knee adduction moment, reduces pain, and improves function for individuals with medial compartment knee osteoarthritis. J. Orthop. Res. 2013, 31, 1020–1025. [Google Scholar] [CrossRef]
- Hunt, M.; Charlton, J.; Krowchuk, N.; Tse, C.; Hatfield, G. Clinical and biomechanical changes following a 4-month toe-out gait modification program for people with medial knee osteoarthritis: A randomized controlled trial. Osteoarthr. Cartil. 2018, 26, 903–911. [Google Scholar] [CrossRef]
- Cheung, R.; Ho, K.; Au, I.P.; An, W.; Zhang, J.; Chan, Z.; Deluzio, K.; Rainbow, M. Immediate and short-term effects of gait retraining on the knee joint moments and symptoms in patients with early tibiofemoral joint osteoarthritis: A randomized controlled trial. Osteoarthr. Cartil. 2018, 26, 1479–1486. [Google Scholar] [CrossRef]
- Xia, H.; Xu, J.; Wang, J.; Hunt, M.A.; Shull, P.B. Validation of a smart shoe for estimating foot progression angle during walking gait. J. Biomech. 2017, 61, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Uhlrich, S.D.; Silder, A.; Beaupre, G.S.; Shull, P.B.; Delp, S.L. Subject-specific toe-in or toe-out gait modifications reduce the larger knee adduction moment peak more than a non-personalized approach. J. Biomech. 2018, 66, 103–110. [Google Scholar] [CrossRef]
- Shen, Y.; Liu, T.; Li, Q.; Yi, J.; Xie, X.; Wen, B.; Inoue, Y. A wearable Sensor System for Knee Adduction Moment Measurement. In Proceedings of the 2016 IEEE International Conference on Real-Time Computing and Robotics (RCAR), Angkor Wat, Cambodia, 6–10 June 2016; pp. 7–12. [Google Scholar]
- Iwama, Y.; Harato, K.; Kobayashi, S.; Niki, Y.; Ogihara, N.; Matsumoto, M.; Nakamura, M.; Nagura, T. Estimation of the External Knee Adduction Moment during Gait Using an Inertial Measurement Unit in Patients with Knee Osteoarthritis. Sensors 2021, 21, 1418. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Chan, P.P.K.; Lam, B.M.F.; Wang, S.; Zhang, J.H.; Chan, Z.Y.S.; Chan, R.H.M.; Ho, K.K.W.; Cheung, R.T.H. Real-Time Estimation of Knee Adduction Moment for Gait Retraining in Patients with Knee Osteoarthritis. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 888–894. [Google Scholar] [CrossRef]
- Thorp, L.E.; Sumner, D.; Block, J.; Moisio, K.C.; Shott, S.; Wimmer, M.A. Knee joint loading differs in individuals with mild compared with moderate medial knee osteoarthritis. Arthritis Rheum. 2006, 54, 3842–3849. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Bowles, K.-A.; Wang, Y.; Cicuttini, F.; Davies-Tuck, M.; Hinman, R. Higher dynamic medial knee load predicts greater cartilage loss over 12 months in medial knee osteoarthritis. Ann. Rheum. Dis. 2011, 70, 1770–1774. [Google Scholar] [CrossRef]
- Richards, R.; Andersen, M.; Harlaar, J.; Noort, J.V.D. Relationship between knee joint contact forces and external knee joint moments in patients with medial knee osteoarthritis: Effects of gait modifications. Osteoarthr. Cartil. 2018, 26, 1203–1214. [Google Scholar] [CrossRef]
- Walter, J.P.; D’Lima, D.; Colwel, C.W., Jr.; Fregly, B.J. Decreased knee adduction moment does not guarantee decreased medial contact force during gait. J. Orthop. Res. 2010, 28, 1348–1354. [Google Scholar] [CrossRef]
- Wang, S.; Chan, K.H.; Lam, R.H.; Yuen, D.N.; Fan, C.K.; Chu, T.T.; Baur, H.; Cheung, R.T. Effects of foot progression angle adjustment on external knee adduction moment and knee adduction angular impulse during stair ascent and descent. Hum. Mov. Sci. 2019, 64, 213–220. [Google Scholar] [CrossRef]
- Cappozzo, A.; Catani, F.; Della Croce, U.; Leardini, A. Position and orientation in space of bones during movement: Anatomical frame definition and determination. Clin. Biomech. 1995, 10, 171–178. [Google Scholar] [CrossRef]
- Robbins, S.M.; Maly, M.R. The effect of gait speed on the knee adduction moment depends on waveform summary measures. Gait Posture 2009, 30, 543–546. [Google Scholar] [CrossRef] [PubMed]
- Shull, P.B.; Shultz, R.; Silder, A.; Dragoo, J.L.; Besier, T.; Cutkosky, M.R.; Delp, S.L. Toe-in gait reduces the first peak knee adduction moment in patients with medial compartment knee osteoarthritis. J. Biomech. 2013, 46, 122–128. [Google Scholar] [CrossRef]
- Rutherford, D.; Hubley-Kozey, C.; Deluzio, K.; Stanish, W.; Dunbar, M. Foot progression angle and the knee adduction moment: A cross-sectional investigation in knee osteoarthritis. Osteoarthr. Cartil. 2008, 16, 883–889. [Google Scholar] [CrossRef]
- Cheung, R.T.H.; Ngai, S.P.C.; Ho, K.K.W. Chinese adaptation and validation of the Knee Injury and Osteoarthritis Outcome Score (KOOS) in patients with knee osteoarthritis. Rheumatol. Int. 2016, 36, 1449–1454. [Google Scholar] [CrossRef]
- Roos, E.M.; Roos, H.P.; Lohmander, L.S.; Ekdahl, C.; Beynnon, B.D. Knee Injury and Osteoarthritis Outcome Score (KOOS)—Development of a Self-Administered Outcome Measure. J. Orthop. Sports Phys. Ther. 1998, 28, 88–96. [Google Scholar] [CrossRef]
- Pierce, C.A.; Block, R.A.; Aguinis, H. Cautionary Note on Reporting Eta-Squared Values from Multifactor ANOVA Designs. Educ. Psychol. Meas. 2004, 64, 916–924. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Simic, M.; Hunt, M.A.; Bennell, K.; Hinman, R.; Wrigley, T. Trunk lean gait modification and knee joint load in people with medial knee osteoarthritis: The effect of varying trunk lean angles. Arthritis Care Res. 2012, 64, 1545–1553. [Google Scholar] [CrossRef]
- Hunt, M.; Takacs, J. Effects of a 10-week toe-out gait modification intervention in people with medial knee osteoarthritis: A pilot, feasibility study. Osteoarthr. Cartil. 2014, 22, 904–911. [Google Scholar] [CrossRef]
- Bellamy, N.; Carette, S.; Ford, P.M.; Kean, W.F.; Le Riche, N.G.; Lussier, A.; Wells, G.A.; Campbell, J. Osteoarthritis antirheumatic drug trials. III. Setting the delta for clinical trials—Results of a consensus development (Delphi) exercise. J. Rheumatol. 1992, 19, 451–457. [Google Scholar] [PubMed]
- Roos, E.M.; Lohmander, L.S. The Knee injury and Osteoarthritis Outcome Score (KOOS): From joint injury to osteoarthritis. Health Qual. Life Outcomes 2003, 1, 64. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, W.H.; Burns, R.; Messier, S.P.; Applegate, W.; Rejeski, W.J.; Morgan, T.; Shumaker, S.; Berry, M.J.; O’Toole, M.; Monu, J.; et al. A Randomized Trial Comparing Aerobic Exercise and Resistance Exercise with a Health Education Program in Older Adults With Knee Osteoarthritis. JAMA 1997, 277, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Loew, L.; Brosseau, L.; Kenny, G.P.; Durand-Bush, N.; Poitras, S.; De Angelis, G.; Wells, G.A. An evidence-based walking program among older people with knee osteoarthritis: The PEP (participant exercise preference) pilot randomized controlled trial. Clin. Rheumatol. 2017, 36, 1607–1616. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Gait Retraining Group Mean (SD) | Walking Exercise Group Mean (SD) | p Value |
|---|---|---|---|
| Gender (male/female) | 15/16 | 14/17 | 0.800 |
| Age (year) | 59.1 (7.2) | 61.7 (6.8) | 0.157 |
| Body mass (kg) | 62.0 (11.0) | 64.2 (10.6) | 0.342 |
| Body height (m) | 1.65 (0.09) | 1.65 (0.08) | 0.940 |
| Kellgren & Lawrence grade | 1.000 | ||
| Grade I | 15 | 16 | |
| Grade II | 16 | 15 | |
| Walking speed (m/s) | 1.02 (0.15) | 1.01 (0.14) | 0.793 |
| Stance time (s) | 0.711 (0.063) | 0.766 (0.108) | 0.018 |
| Baseline biomechanics | |||
| FPA (°) | 12.1 (6.1) | 11.3 (4.4) | 0.565 |
| KAM1 (%BW*ht) | 2.73 (0.51) | 2.66 (0.40) | 0.548 |
| KAM2 (%BW*ht) | 1.98 (0.54) | 2.14 (0.52) | 0.242 |
| KFM (%BW*ht) | 3.14 (1.20) | 3.02 (1.15) | 0.694 |
| KAAI (%BW*ht*s) | 1.02 (0.28) | 1.16 (0.31) | 0.055 |
| Baseline symptoms | |||
| VASP (0–10) | 4.3 (2.2) | 4.5 (2.0) | 0.683 |
| KOOS | |||
| KOOS5 (0–100) | 70.0 (10.3) | 66.1 (15.0) | 0.208 |
| Pain (0–100) | 73.1 (7.9) | 72.5 (12.1) | 0.820 |
| Symptoms (0–100) | 69.7 (16.2) | 68.1 (20.3) | 0.730 |
| ADL (0–100) | 85.4 (8.4) | 81.9 (14.3) | 0.249 |
| Sport/Rec (0–100) | 65.2 (17.6) | 62.3 (21.2) | 0.560 |
| QOL (0–100) | 54.6 (14.0) | 46.7 (17.2) | 0.055 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, S.; Chan, P.P.K.; Lam, B.M.F.; Chan, Z.Y.S.; Zhang, J.H.W.; Wang, C.; Lam, W.K.; Ho, K.K.W.; Chan, R.H.M.; Cheung, R.T.H. Sensor-Based Gait Retraining Lowers Knee Adduction Moment and Improves Symptoms in Patients with Knee Osteoarthritis: A Randomized Controlled Trial. Sensors 2021, 21, 5596. https://doi.org/10.3390/s21165596
Wang S, Chan PPK, Lam BMF, Chan ZYS, Zhang JHW, Wang C, Lam WK, Ho KKW, Chan RHM, Cheung RTH. Sensor-Based Gait Retraining Lowers Knee Adduction Moment and Improves Symptoms in Patients with Knee Osteoarthritis: A Randomized Controlled Trial. Sensors. 2021; 21(16):5596. https://doi.org/10.3390/s21165596
Chicago/Turabian StyleWang, Sizhong, Peter P. K. Chan, Ben M. F. Lam, Zoe Y. S. Chan, Janet H. W. Zhang, Chao Wang, Wing Kai Lam, Kevin Ki Wai Ho, Rosa H. M. Chan, and Roy T. H. Cheung. 2021. "Sensor-Based Gait Retraining Lowers Knee Adduction Moment and Improves Symptoms in Patients with Knee Osteoarthritis: A Randomized Controlled Trial" Sensors 21, no. 16: 5596. https://doi.org/10.3390/s21165596
APA StyleWang, S., Chan, P. P. K., Lam, B. M. F., Chan, Z. Y. S., Zhang, J. H. W., Wang, C., Lam, W. K., Ho, K. K. W., Chan, R. H. M., & Cheung, R. T. H. (2021). Sensor-Based Gait Retraining Lowers Knee Adduction Moment and Improves Symptoms in Patients with Knee Osteoarthritis: A Randomized Controlled Trial. Sensors, 21(16), 5596. https://doi.org/10.3390/s21165596