
Lower Back Injury Prevention and Sensitization of Hip Hinge with Neutral Spine Using Wearable Sensors during Lifting Exercises




Abstract
:1. Introduction
2. Materials and Methods
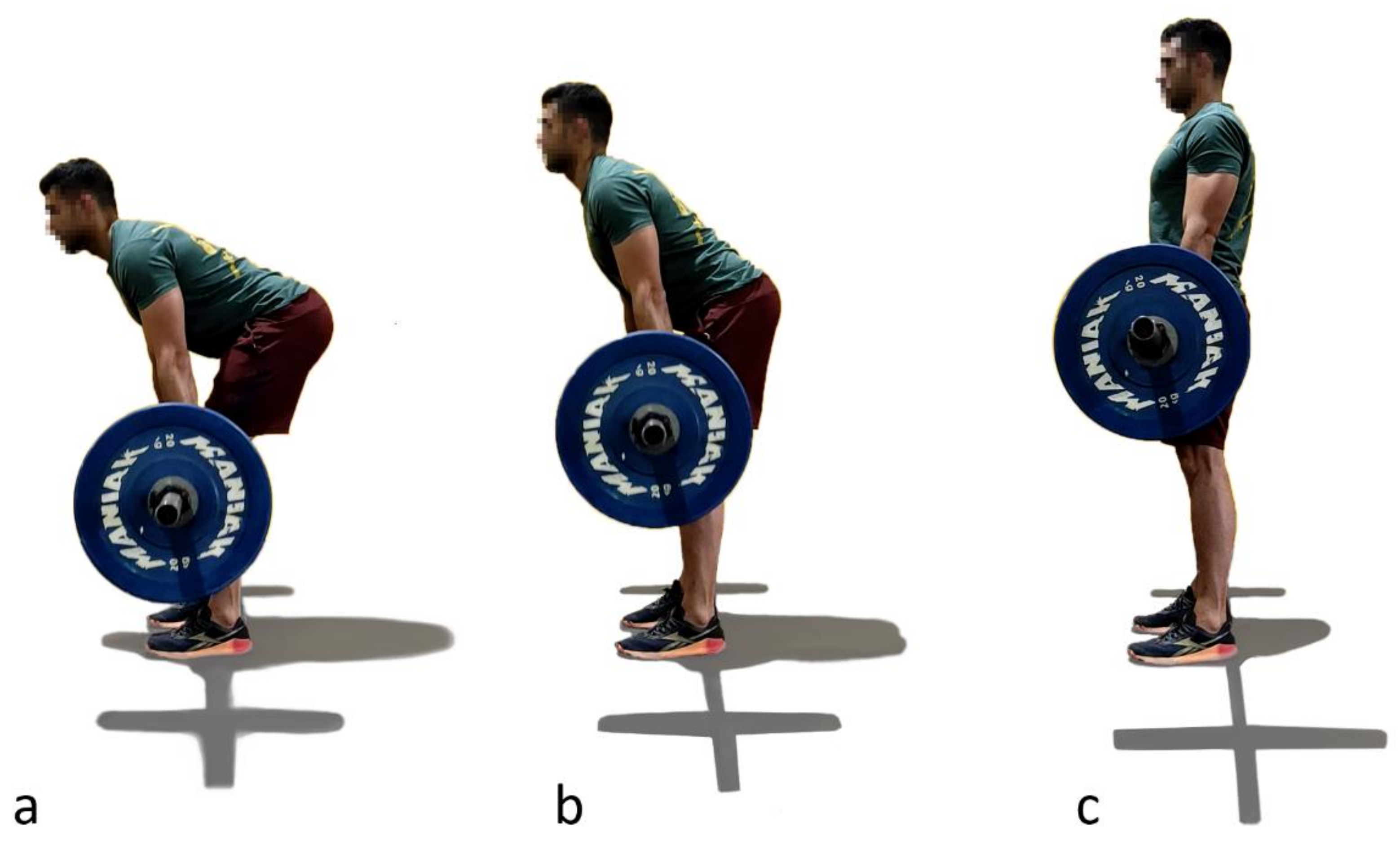
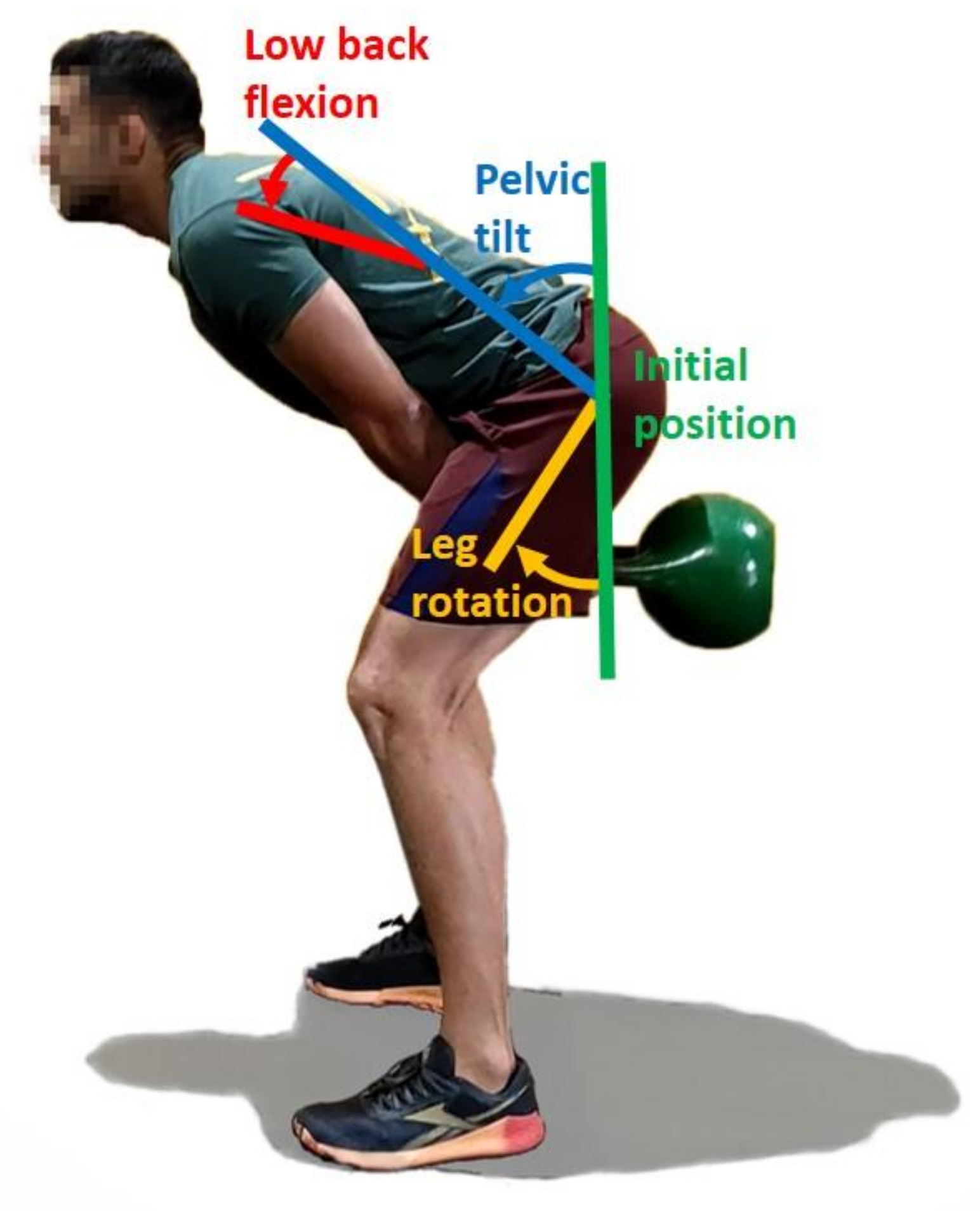
2.1. Lifting Techniques
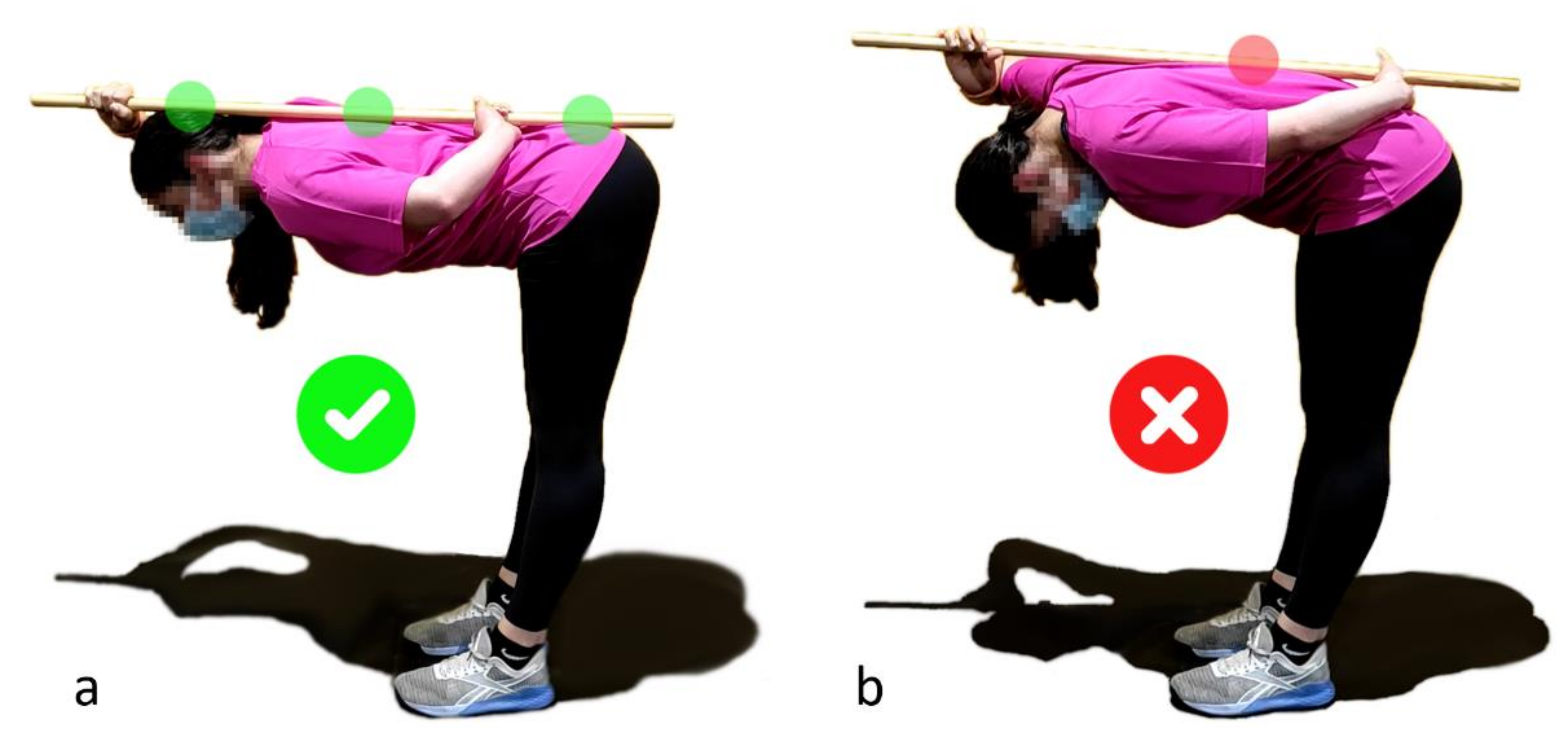
2.1.1. Hip Hinge and Lumbopelvic Dissociation
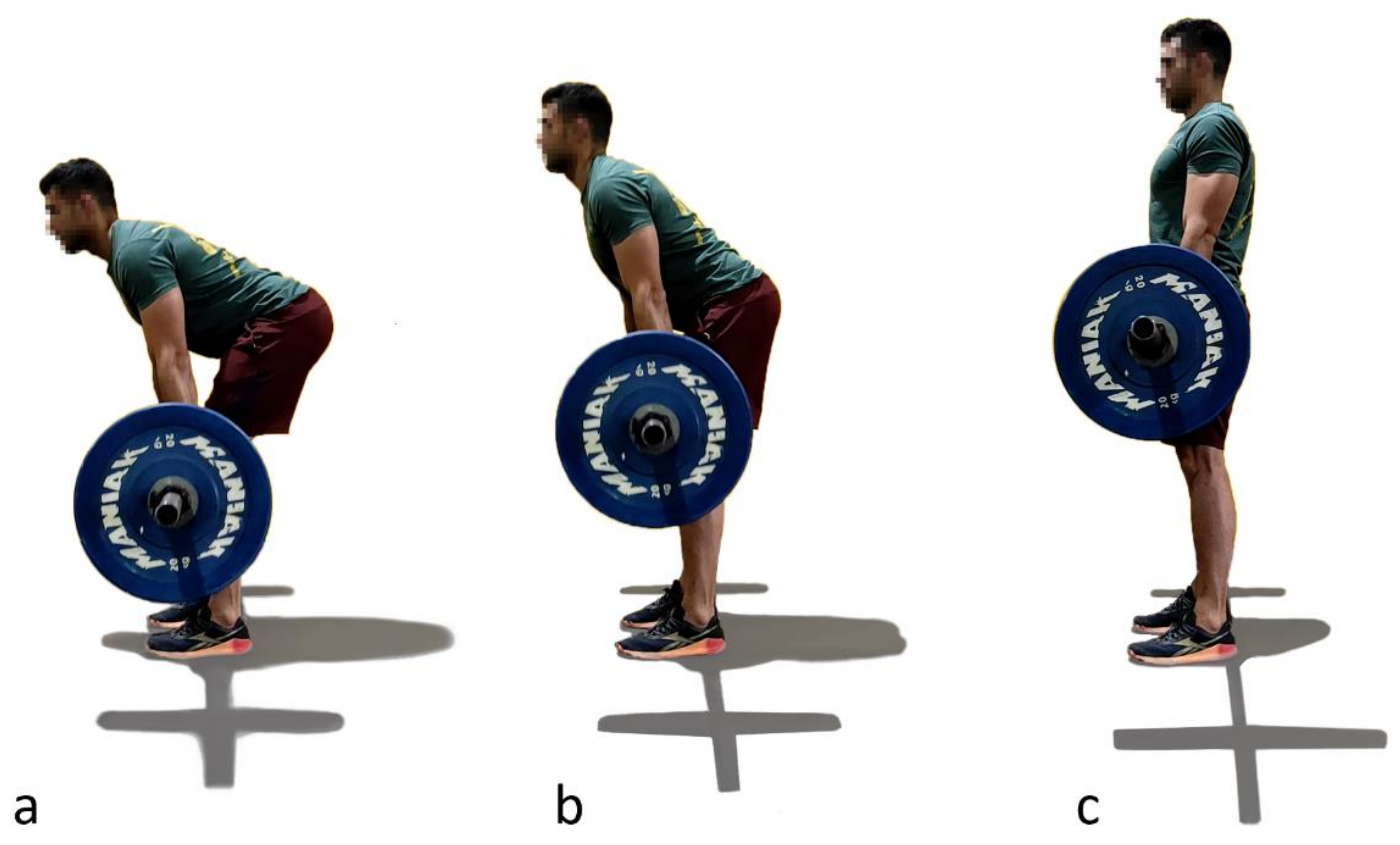
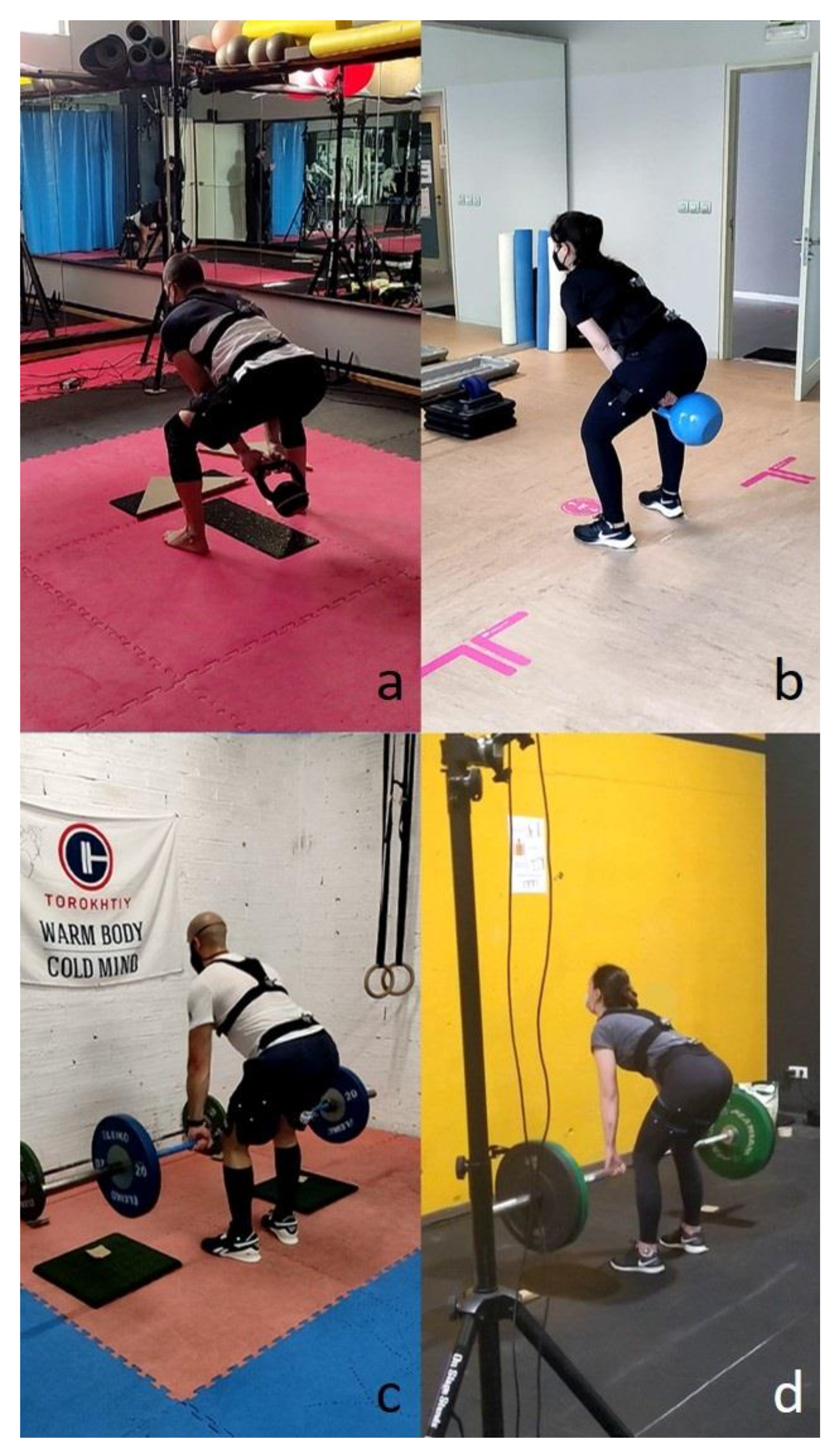
2.1.2. American Kettlebell Swing and Deadlift
2.2. Preliminary Test
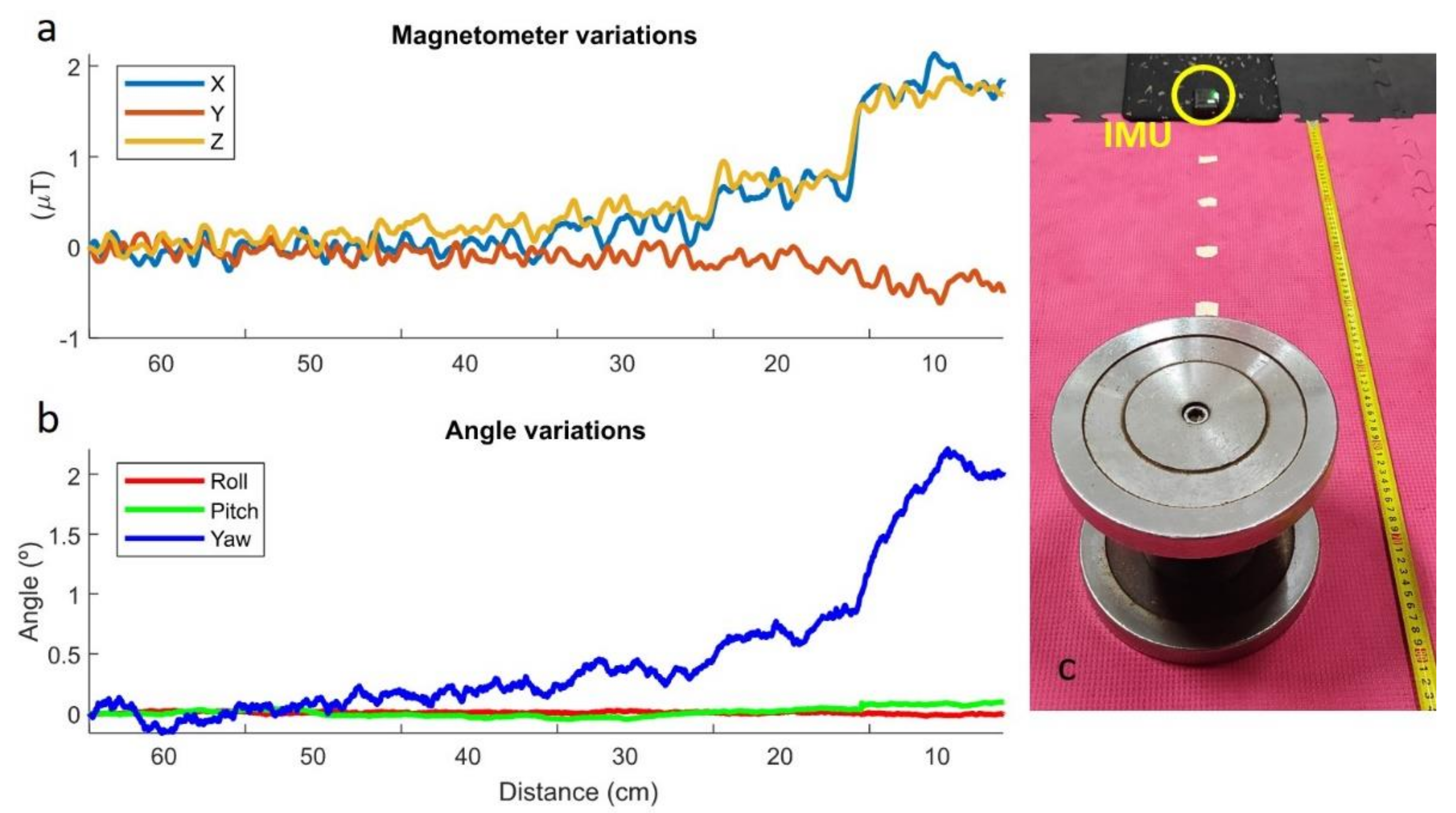
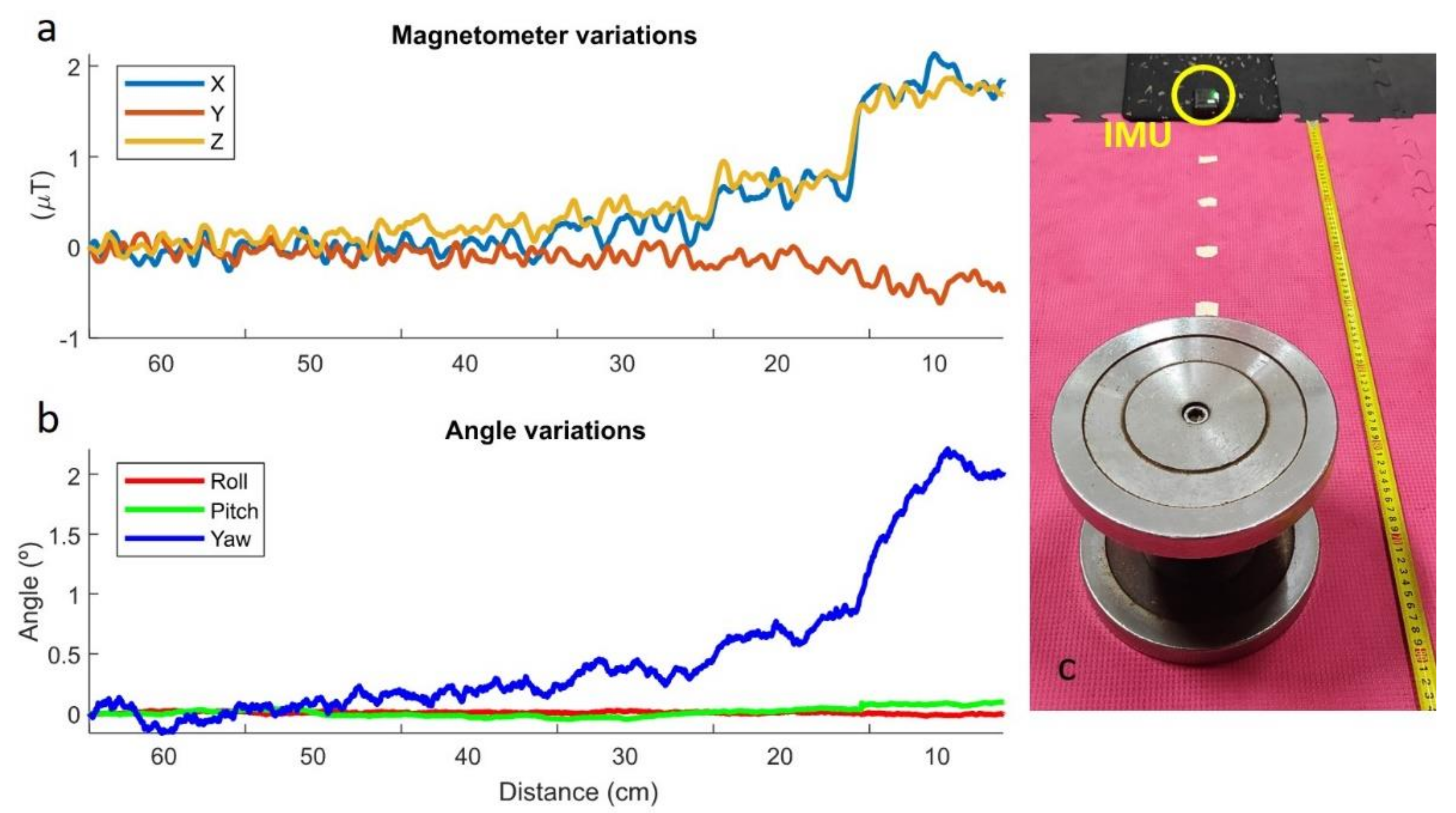
2.2.1. Static Perturbations
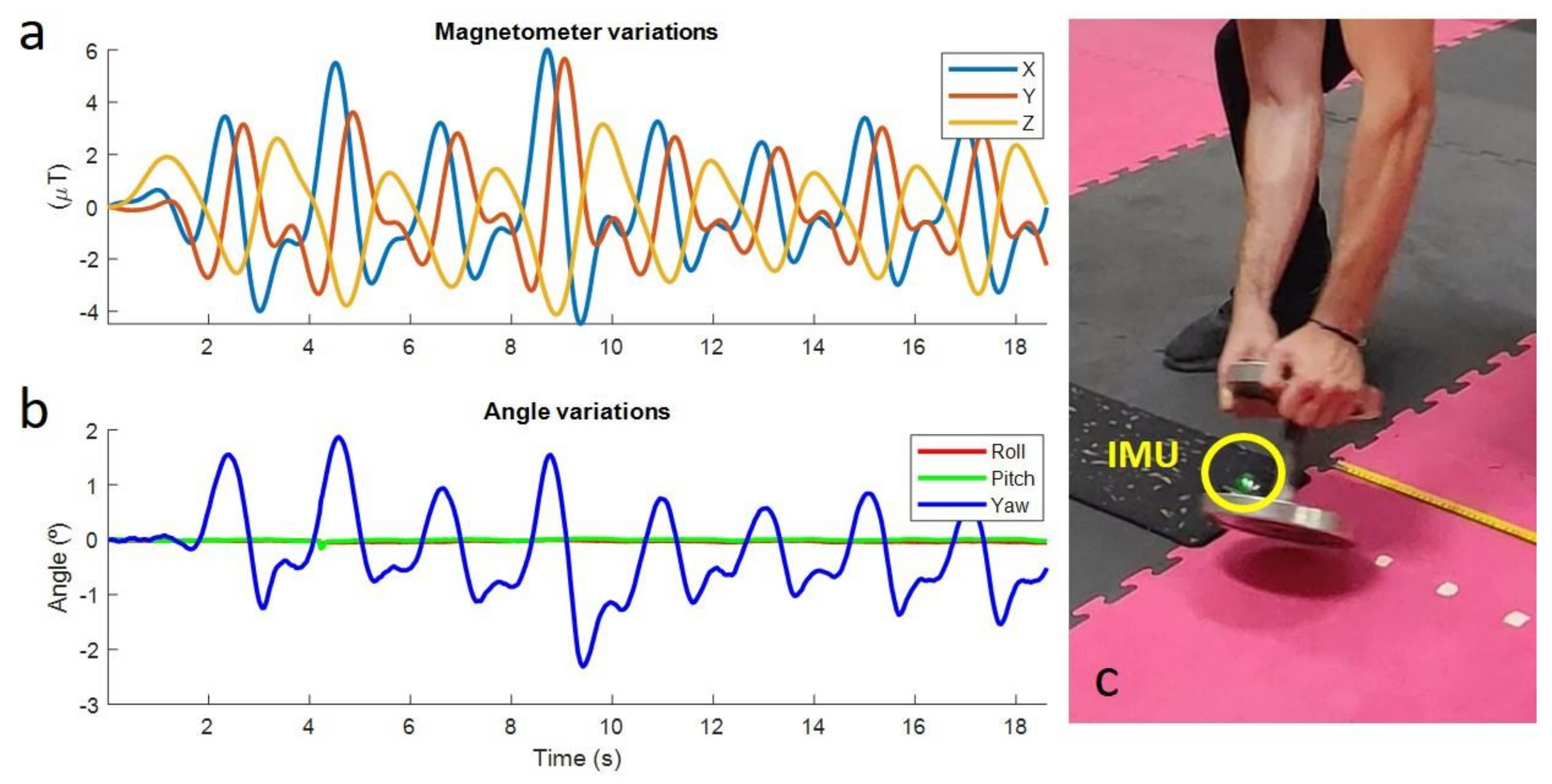
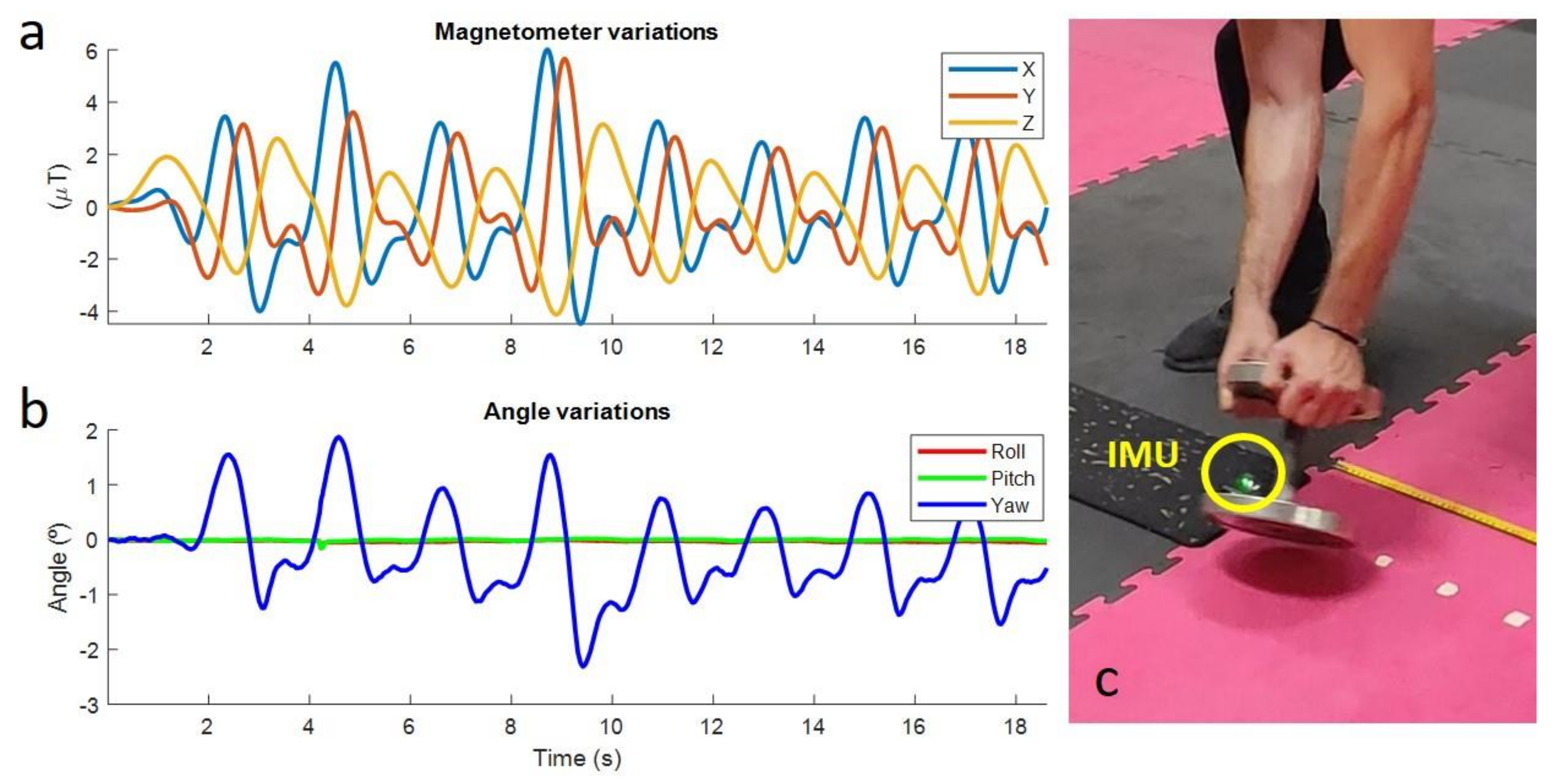
2.2.2. Dynamic Perturbations
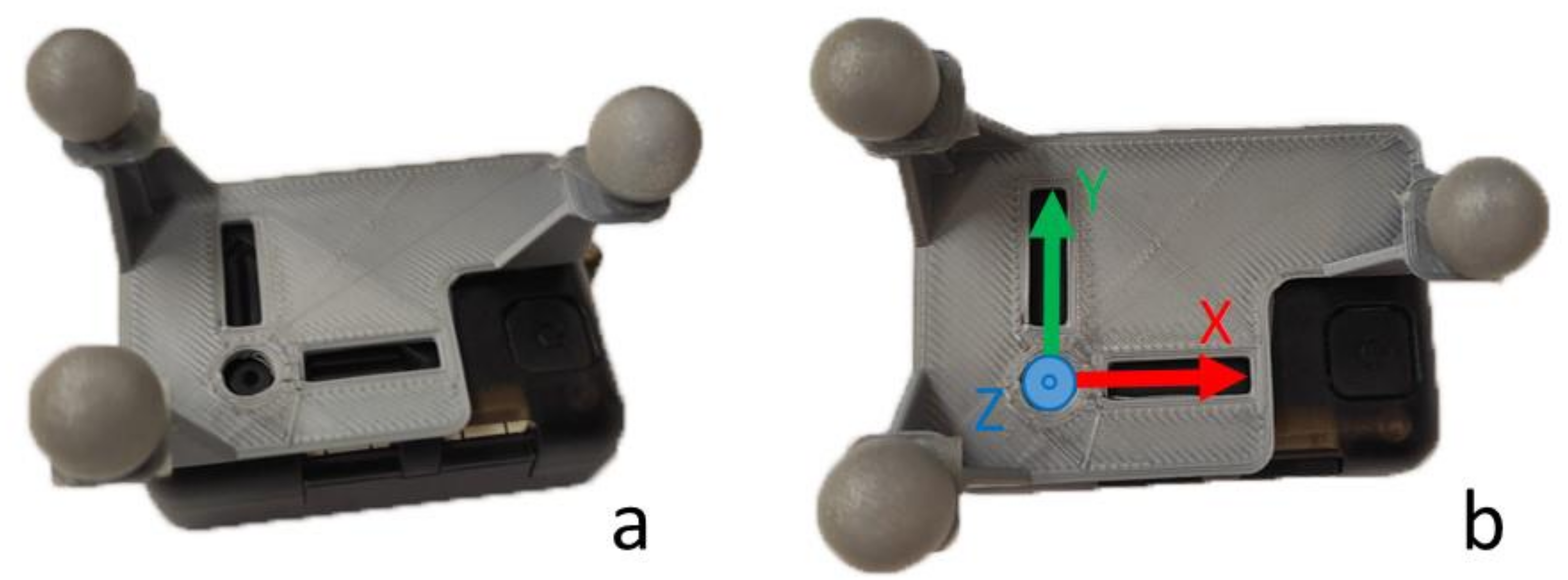
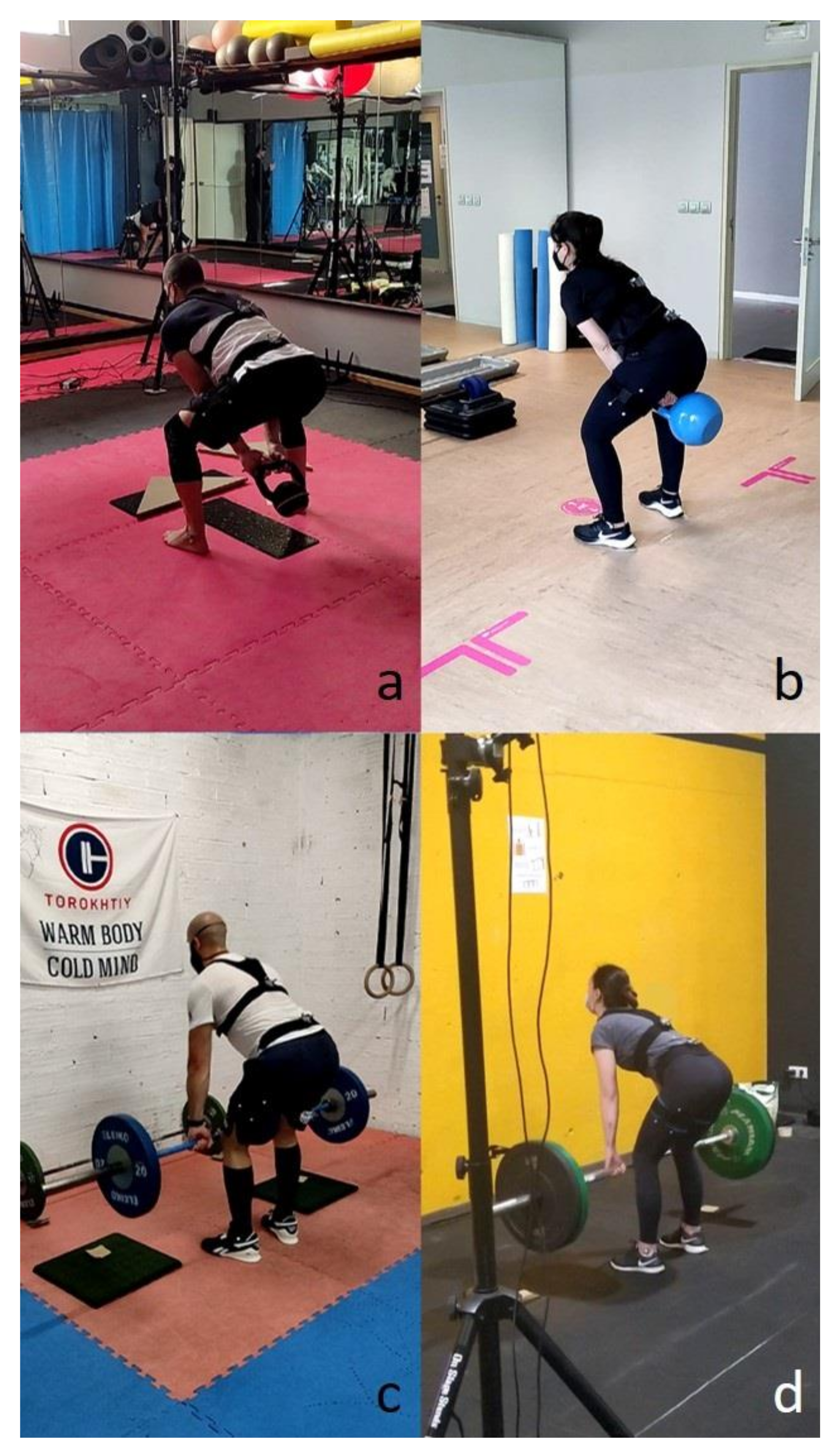
2.3. Experimental Data Collection
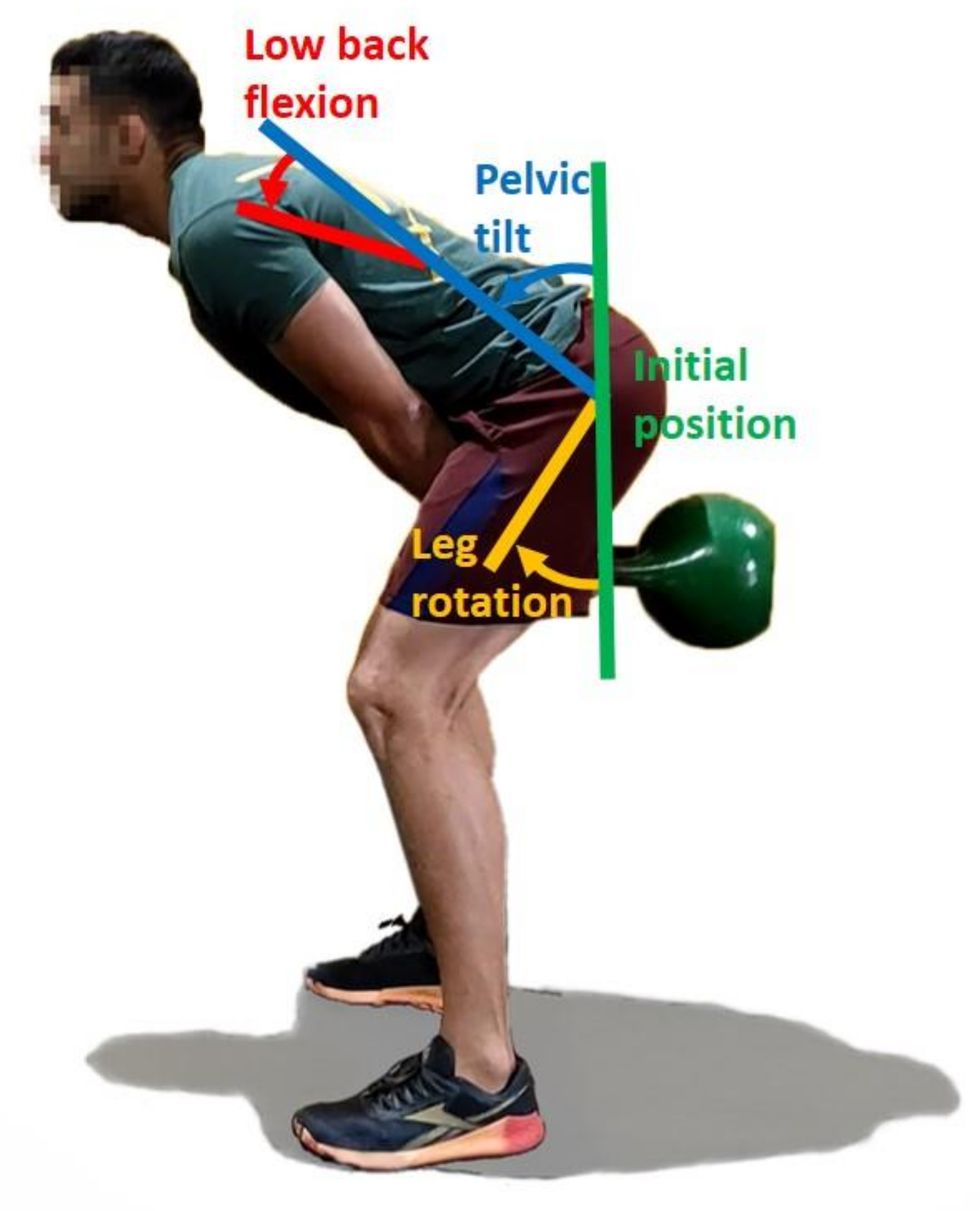
2.4. Calculation of Kinematic Parameters
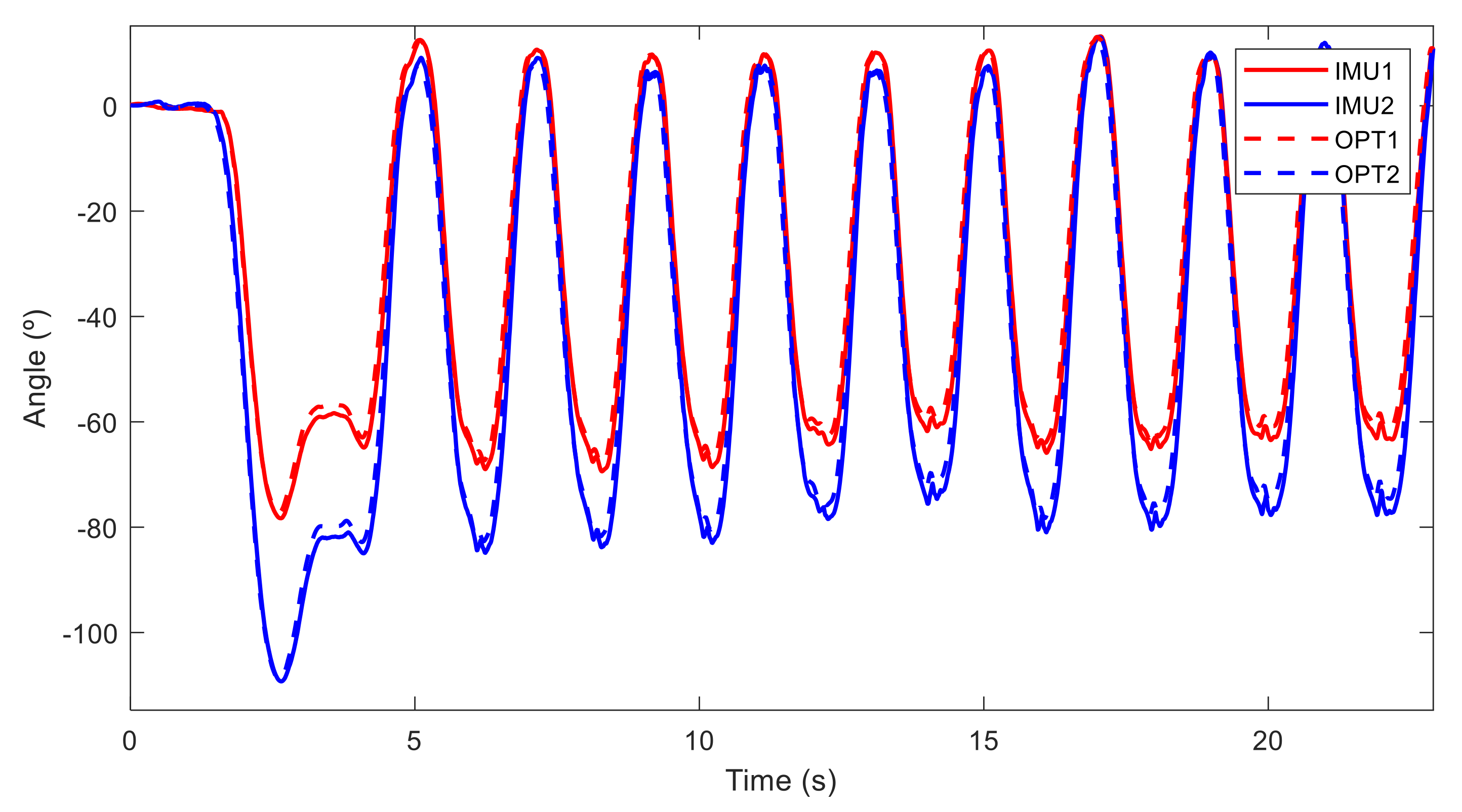
2.5. Motion Analysis and Statistical Differences
3. Results
4. Discussion and Limitations of the Study
5. Conclusions and Future Works
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Strömbäck, E.; Aasa, U.; Gilenstam, K.; Berglund, L. Prevalence and Consequences of Injuries in Powerlifting: A Cross-sectional Study. Orthop. J. Sports Med. 2018, 6, 5. [Google Scholar] [CrossRef] [Green Version]
- Howe, L.; Lehman, G. Getting out of neutral: The risks and rewards of lumbar spine flexion during lifting exercises. Prof. Strength Cond. J. 2021, 60, 19–31. [Google Scholar]
- Antwi-Afari, M.F.; Li, H.; Edwards, D.J.; Pärn, E.A.; Owusu-Manu, D.-G.; Seo, J.; Wong, A.Y.L. Identification of potential biomechanical risk factors for low back disorders during repetitive rebar lifting. Constr. Innov. 2018, 18, 2. [Google Scholar] [CrossRef]
- Southgate, D.F.L.; Prinold, J.A.I.; Weinert-Aplin, R.A.; Childs, P.R.N.; Bull, A.M.J. Motion Analysis in Sport. In Sports Innovation, Technology and Research; World Scientific (Europe): London, UK, 2016; pp. 3–30. [Google Scholar]
- Baker, R. The history of gait analysis before the advent of modern computers. Gait Posture 2007, 26, 331–342. [Google Scholar] [CrossRef]
- Winter, D.A. Biomechanics and Motor Control of Human Movement, 4th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Poitras, I.; Dupuis, F.; Bielmann, M.; Campeau-Lecours, A.; Mercier, C.; Bouyer, L.J.; Roy, J.-S. Validity and reliability of wearable sensors for joint angle estimation: A systematic review. Sensors 2019, 19, 1555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holden, D. Robust solving of optical motion capture data by denoising. ACM Trans. Graph. 2018, 37, 1–12. [Google Scholar] [CrossRef]
- Ghorbani, S.; Etemad, A.; Troje, N.F. Auto-labelling of Markers in Optical Motion Capture by Permutation Learning. In Computer Graphics International Conference; Springer: Cham, Switzerland, 2019; Volume 11542 LNCS, pp. 167–178. [Google Scholar] [CrossRef] [Green Version]
- Fong, D.T.-P.; Chan, Y.-Y. The Use of Wearable Inertial Motion Sensors in Human Lower Limb Biomechanics Studies: A Systematic Review. Sensors 2010, 10, 11556–11565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madgwick, S.O.H.; Harrison, A.J.L.; Vaidyanathan, R. Estimation of IMU and MARG orientation using a gradient descent algorithm. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–7. [Google Scholar] [CrossRef]
- Sabatini, A.M. Quaternion-Based Extended Kalman Filter for Determining Orientation by Inertial and Magnetic Sensing. IEEE Trans. Biomed. Eng. 2006, 53, 1346–1356. [Google Scholar] [CrossRef]
- Punchihewa, N.G.; Miyazaki, S.; Chosa, E.; Yamako, G. Efficacy of Inertial Measurement Units in the Evaluation of Trunk and Hand Kinematics in Baseball Hitting. Sensors 2020, 20, 7331. [Google Scholar] [CrossRef]
- Lapinski, M.; Medeiros, C.B.; Scarborough, D.M.; Berkson, E.; Gill, T.J.; Kepple, T.; Paradiso, J.A. A Wide-Range, Wireless Wearable Inertial Motion Sensing System for Capturing Fast Athletic Biomechanics in Overhead Pitching. Sensors 2019, 19, 3637. [Google Scholar] [CrossRef] [Green Version]
- Oliva-Lozano, J.M.; Maraver, E.F.; Fortes, V.; Muyor, J.M. Kinematic Analysis of the Postural Demands in Professional Soccer Match Play Using Inertial Measurement Units. Sensors 2020, 20, 5971. [Google Scholar] [CrossRef]
- O’Reilly, M.; Whelan, D.F.; Ward, T.; Delahunt, E.; Caulfield, B. Technology in Strength and Conditioning: Assessing Bodyweight Squat Technique with Wearable Sensors. J. Strength Cond. Res. 2017, 31, 2303–2312. [Google Scholar] [CrossRef]
- Magalhães, F.; Vannozzi, G.; Gatta, G.; Fantozzi, S. Wearable inertial sensors in swimming motion analysis: A systematic review. J. Sports Sci. 2014, 33, 732–745. [Google Scholar] [CrossRef]
- Preatoni, E.; Nodari, S.; Lopomo, N.F. Supervised Machine Learning Applied to Wearable Sensor Data Can Accurately Classify Functional Fitness Exercises Within a Continuous Workout. Front. Bioeng. Biotechnol. 2020, 8, 664. [Google Scholar] [CrossRef]
- Fasel, B.; Spörri, J.; Gilgien, M.; Boffi, G.; Chardonnens, J.; Müller, E.; Aminian, K. Three-dimensional body and centre of mass kinematics in alpine ski racing using differential GNSS and inertial sensors. Remote Sens. 2016, 8, 671. [Google Scholar] [CrossRef] [Green Version]
- Bonnet, V.; Mazzà, C.; Fraisse, P.; Cappozzo, A. Real-time estimate of body kinematics during a planar squat task using a single inertial measurement unit. IEEE Trans. Biomed. Eng. 2013, 60, 1920–1926. [Google Scholar] [CrossRef]
- Aasa, U.; Bengtsson, V.; Berglund, L.; Öhberg, F. Variability of lumbar spinal alignment among power- and weightlifters during the deadlift and barbell back squat. Sports Biomech. 2019, 00, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wellness Creative Co. Fitness Industry Market Research Report. Available online: https://www.wellnesscreatives.com/research-report/ (accessed on 12 July 2021).
- Tatsumi, R.L.; Hart, R.A. cervical, thoracic, and lumbar fractures. In Current Therapy of Trauma and Surgical Critical Care; Asensio, J.A., Trunkey, D.D., Eds.; Elsevier: Philadelphia, PA, USA, 2008; pp. 513–519. [Google Scholar]
- Elgueta-Cancino, E.; Schabrun, S.; Danneels, L.; Hodges, P. A clinical test of lumbopelvic control: Development and reliability of a clinical test of dissociation of lumbopelvic and thoracolumbar motion. Man. Ther. 2014, 19, 418–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hay, O.; Dar, G.; Abbas, J.; Stein, D.; May, H.; Masharawi, Y.; Peled, N.; Hershkovitz, I. The Lumbar Lordosis in Males and Females, Revisited. PLoS ONE 2015, 10, e0133685. [Google Scholar] [CrossRef] [Green Version]
- Tannenbaum, E.; Kopydlowski, N.; Smith, M.; Bedi, A.; Sekiya, J.K. Gender and Racial Differences in Focal and Global Acetabular Version. J. Arthroplast. 2014, 29, 373–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roetenberg, D.; Luinge, H.J.; Veltink, P.H. Inertial and magnetic sensing of human movement near ferromagnetic materials. In Proceedings of the Second IEEE and ACM International Symposium on Mixed and Augmented Reality, Tokyo, Japan, 10 October 2003; pp. 268–269. [Google Scholar] [CrossRef] [Green Version]
- Cuadrado, J.; Michaud, F.; Lugrís, U.; Soto, M.P. Using Accelerometer Data to Tune the Parameters of an Extended Kalman Filter for Optical Motion Capture: Preliminary Application to Gait Analysis. Sensors 2021, 21, 427. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, J.B. Quaternions and rotation sequences. In Proceedings of the International Conference on Geometry, Integrability and Quantization, Sofia, Bulgaria, 1–10 September 1999; pp. 127–143. [Google Scholar]
- Scannell, J.P.; McGill, S.M. Lumbar posture—Should it, and can it, be modified? A study of passive tissue stiffness and lumbar position during activities of daily living. Phys. Ther. 2003, 83, 907–917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navidi, W. Statistics for Engineers and Scientists, 3rd ed.; McGraw-Hill Higher Education: New York, NY, USA, 2010. [Google Scholar]
- Callaghan, J.P.; McGill, S.M. Intervertebral disc herniation: Studies on a porcine model exposed to highly repetitive flexion/extension motion with compressive force. Clin. Biomech. 2001, 16, 28–37. [Google Scholar] [CrossRef]
- Czuppon, S.; Prather, H.; Hunt, D.M.; Ma, K.S.; Bloom, N.J.; Clohisy, J.C.; Larsen, R.; Harris-Hayes, M. Gender-Dependent Differences in Hip Range of Motion and Impingement Testing in Asymptomatic College Freshman Athletes. PM R 2017, 9, 660–667. [Google Scholar] [CrossRef]
- Nepple, J.J.; Riggs, C.N.; Ross, J.R.; Clohisy, J.C. Clinical Presentation and Disease Characteristics of Femoroacetabular Impingement Are Sex-Dependent. J. Bone Jt. Surg.-Am. Vol. 2014, 96, 1683–1689. [Google Scholar] [CrossRef] [Green Version]
- Klasan, A.; Neri, T.; Sommer, C.; Leie, M.A.; Dworschak, P.; Schofer, M.D.; Heyse, T.J. Analysis of acetabular version: Retroversion prevalence, age, side and gender correlations. J. Orthop. Transl. 2019, 18, 7–12. [Google Scholar] [CrossRef]
- Marras, W.; Fathallah, F.; Miller, R.; Davis, S.; Mirka, G. Accuracy of a three-dimensional lumbar motion monitor for recording dynamic trunk motion characteristics. Int. J. Ind. Ergon. 1992, 9, 75–87. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| American Kettlebell Swing | ||||||
|---|---|---|---|---|---|---|
| Max. Lower Back Flexion (°) | Max. Pelvic Tilt (°) | Max. Leg Rotation (°) | ||||
| Experience | OPT | IMU | OPT | IMU | OPT | |
| Women | A | 20.48 | 17.21 | 54.01 | 57.66 | 34.49 |
| A | 31.47 | 36.12 | 57.03 | 56.65 | 82.36 | |
| A | 24.33 | 27.29 | 36.80 | 34.36 | 76.03 | |
| B | 32.19 | 30.48 | 50.99 | 44.34 | 26.90 | |
| B | 22.13 | 27.64 | 46.12 | 46.08 | 22.18 | |
| B | 26.00 | 31.11 | 52.66 | 52.84 | 33.01 | |
| B | 33.37 | 36.21 | 26.27 | 27.44 | 39.70 | |
| B | 20.81 | 26.25 | 54.34 | 54.02 | 16.17 | |
| B | 13.13 | 13.84 | 27.51 | 28.14 | 39.72 | |
| B | 19.26 | 19.08 | 58.08 | 61.74 | 34.82 | |
| B | 36.88 | 39.81 | 46.59 | 47.94 | 35.33 | |
| B | 3.25 | 5.68 | 54.89 | 56.68 | 27.80 | |
| B | 19.78 | 23.91 | 63.39 | 66.07 | 21.76 | |
| C | 28.85 | 32.64 | 47.73 | 47.15 | 26.13 | |
| C | 33.91 | 33.51 | 50.66 | 55.39 | 41.14 | |
| C | 28.36 | 28.47 | 44.26 | 46.02 | 47.34 | |
| C | 21.98 | 24.65 | 74.45 | 76.13 | 34.38 | |
| C | 22.96 | 25.97 | 38.16 | 41.16 | 29.37 | |
| Men | A | 60.90 | 60.59 | 46.20 | 47.51 | 55.24 |
| A | 20.70 | 19.14 | 58.88 | 60.81 | 73.50 | |
| A | 27.95 | 29.15 | 52.63 | 53.49 | 41.98 | |
| A | 45.39 | 49.12 | 37.28 | 37.65 | 46.06 | |
| A | 21.74 | 26.78 | 66.53 | 64.45 | 40.75 | |
| A | 32.29 | 33.84 | 18.93 | 20.70 | 51.17 | |
| B | 25.07 | 26.93 | 60.45 | 61.07 | 38.07 | |
| B | 17.41 | 20.04 | 40.69 | 43.81 | 38.58 | |
| B | 24.34 | 29.68 | 56.35 | 55.01 | 16.47 | |
| C | 47.78 | 42.99 | 58.44 | 59.60 | 40.24 | |
| C | 26.69 | 31.13 | 54.58 | 54.56 | 87.64 | |
| C | 21.38 | 17.37 | 57.39 | 51.84 | 42.64 | |
| C | 16.91 | 19.46 | 43.98 | 45.12 | 36.31 | |
| C | 16.99 | 19.37 | 57.41 | 57.61 | 22.30 | |
| C | 22.80 | 26.55 | 51.18 | 52.13 | 33.49 | |
| C | 25.82 | 29.35 | 33.42 | 36.85 | 40.63 | |
| C | 23.57 | 27.80 | 39.71 | 39.40 | 46.56 | |
| C | 39.24 | 40.65 | 18.14 | 18.32 | 34.23 | |
| C | 36.04 | 35.76 | 35.87 | 40.81 | 47.60 | |
| C | 24.17 | 22.42 | 48.42 | 50.57 | 30.44 | |
| C | 27.20 | 32.07 | 39.55 | 41.20 | 29.59 | |
| Mean | 26.76 | 28.72 | 47.69 | 48.52 | 40.05 | |
| RMSE | 2.71 | 2.44 | ||||
| Deadlift | ||||||
|---|---|---|---|---|---|---|
| Max. Spine Deviation (°) | Max. Pelvic Tilt (°) | Max. Leg Rotation (°) | ||||
| Experience | OPT | IMU | OPT | IMU | OPT | |
| Women | A | 25.03 | 22.84 | 58.30 | 64.18 | 58.46 |
| A | 33.79 | 33.92 | 47.87 | 51.21 | 99.78 | |
| A | 22.37 | 21.51 | 52.06 | 50.51 | 67.83 | |
| B | 21.49 | 21.32 | 66.65 | 64.91 | 35.88 | |
| B | 20.78 | 24.05 | 68.40 | 67.06 | 15.10 | |
| B | 33.43 | 36.16 | 32.91 | 32.72 | 58.11 | |
| B | 24.06 | 26.47 | 37.02 | 38.07 | 47.34 | |
| B | 13.38 | 14.70 | 70.23 | 70.30 | 26.75 | |
| B | 33.38 | 36.04 | 33.65 | 32.92 | 36.56 | |
| B | 12.96 | 14.10 | 53.82 | 55.77 | 43.05 | |
| B | 21.93 | 23.50 | 73.82 | 74.94 | 32.30 | |
| B | 14.86 | 15.86 | 67.85 | 69.40 | 33.08 | |
| B | 21.58 | 26.81 | 70.01 | 70.12 | 20.86 | |
| C | 23.22 | 26.72 | 60.68 | 59.91 | 20.21 | |
| C | 4.19 | 9.32 | 65.38 | 64.15 | 30.85 | |
| C | 30.33 | 32.72 | 39.41 | 39.90 | 41.41 | |
| C | 18.60 | 18.51 | 83.06 | 86.39 | 27.44 | |
| C | 20.79 | 23.07 | 84.35 | 84.98 | 23.80 | |
| Men | A | 56.41 | 61.77 | 29.13 | 29.08 | 106.06 |
| A | 18.29 | 18.72 | 67.34 | 67.77 | 35.89 | |
| A | 10.71 | 9.32 | 58.06 | 57.10 | 70.87 | |
| A | 33.83 | 36.57 | 57.05 | 56.43 | 50.78 | |
| A | 18.70 | 22.52 | 49.82 | 50.47 | 53.73 | |
| A | 27.28 | 28.21 | 51.82 | 52.97 | 41.08 | |
| B | 19.88 | 22.71 | 62.48 | 61.59 | 32.86 | |
| B | 34.71 | 41.54 | 50.77 | 49.27 | 33.53 | |
| B | 44.29 | 48.77 | 55.22 | 55.75 | 21.83 | |
| C | 34.51 | 39.05 | 62.18 | 61.54 | 41.36 | |
| C | 19.26 | 25.20 | 38.74 | 34.81 | 78.90 | |
| C | 15.50 | 17.36 | 61.48 | 64.12 | 26.97 | |
| C | 36.27 | 38.65 | 40.07 | 41.93 | 38.74 | |
| C | 15.83 | 19.76 | 55.26 | 54.67 | 28.71 | |
| C | 26.90 | 29.86 | 61.27 | 60.54 | 38.33 | |
| C | 19.85 | 22.20 | 57.05 | 58.27 | 30.23 | |
| C | 33.39 | 35.54 | 46.32 | 47.66 | 61.66 | |
| C | 52.39 | 52.80 | 27.58 | 28.12 | 35.65 | |
| C | 29.44 | 30.53 | 60.13 | 62.11 | 37.85 | |
| C | 27.25 | 26.50 | 41.48 | 45.42 | 67.70 | |
| C | 33.59 | 35.44 | 62.75 | 63.13 | 33.04 | |
| Mean | 25.76 | 27.97 | 55.42 | 55.90 | 43.19 | |
| RMSE | 3.01 | 1.85 | ||||
| Swing KB (OPT) | Deadlift (OPT) | ||||||
|---|---|---|---|---|---|---|---|
| A | B | C | A | B | C | ||
| Mean Spine Deviation (º) | 31.69 | 22.59 | 27.33 | 27.38 | 24.36 | 25.96 | |
| Mean Max. Pelvic Tilt (º) | 47.59 | 49.10 | 46.67 | 52.38 | 57.14 | 55.72 | |
| Mean Max. Leg Rotation (º) | 55.73 | 30.04 | 39.41 | 64.94 | 33.64 | 38.99 | |
| p-Value | ||||||
|---|---|---|---|---|---|---|
| American Kettlebell Swing | Deadlift | |||||
| H0 | Max. Spine Deviation | Max. Pelvic Tilt | Max. Leg Rotation | Max. Spine Deviation | Max. Pelvic Tilt | Max. Leg Rotation |
| W=M | 0.000392 | 0.032860 | 0.000681 | 0.000002 | 0.000018 | 0.000676 |
| A=B | 0.000293 | 0.351078 | 0.000000 | 0.079142 | 0.011574 | 0.000000 |
| B=C | 0.001229 | 0.069403 | 0.000028 | 0.207485 | 0.320128 | 0.002534 |
| A=C | 0.014508 | 0.565281 | 0.000011 | 0.356411 | 0.048909 | 0.000001 |
| OPT=IMU | 0.01206 | 0.34031 | / | 0.005563 | 0.574423 | / |
| Swing KB (OPT) | Deadlift (OPT) | ||||
|---|---|---|---|---|---|
| W | M | W | M | ||
| Mean Spine Deviation (º) | 24.40 | 28.78 | 22.01 | 28.97 | |
| Mean Max. Pelvic Tilt (º) | 49.11 | 46.48 | 59.19 | 52.19 | |
| Mean Max. Leg Rotation (º) | 37.15 | 42.55 | 39.93 | 45.99 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michaud, F.; Pérez Soto, M.; Lugrís, U.; Cuadrado, J. Lower Back Injury Prevention and Sensitization of Hip Hinge with Neutral Spine Using Wearable Sensors during Lifting Exercises. Sensors 2021, 21, 5487. https://doi.org/10.3390/s21165487
Michaud F, Pérez Soto M, Lugrís U, Cuadrado J. Lower Back Injury Prevention and Sensitization of Hip Hinge with Neutral Spine Using Wearable Sensors during Lifting Exercises. Sensors. 2021; 21(16):5487. https://doi.org/10.3390/s21165487
Chicago/Turabian StyleMichaud, Florian, Manuel Pérez Soto, Urbano Lugrís, and Javier Cuadrado. 2021. "Lower Back Injury Prevention and Sensitization of Hip Hinge with Neutral Spine Using Wearable Sensors during Lifting Exercises" Sensors 21, no. 16: 5487. https://doi.org/10.3390/s21165487
APA StyleMichaud, F., Pérez Soto, M., Lugrís, U., & Cuadrado, J. (2021). Lower Back Injury Prevention and Sensitization of Hip Hinge with Neutral Spine Using Wearable Sensors during Lifting Exercises. Sensors, 21(16), 5487. https://doi.org/10.3390/s21165487