
Beacon-Based Remote Measurement of Social Behavior in ASD Clinical Trials: A Technical Feasibility Assessment

 , ,
, ,
Abstract
:1. Introduction
2. Methods
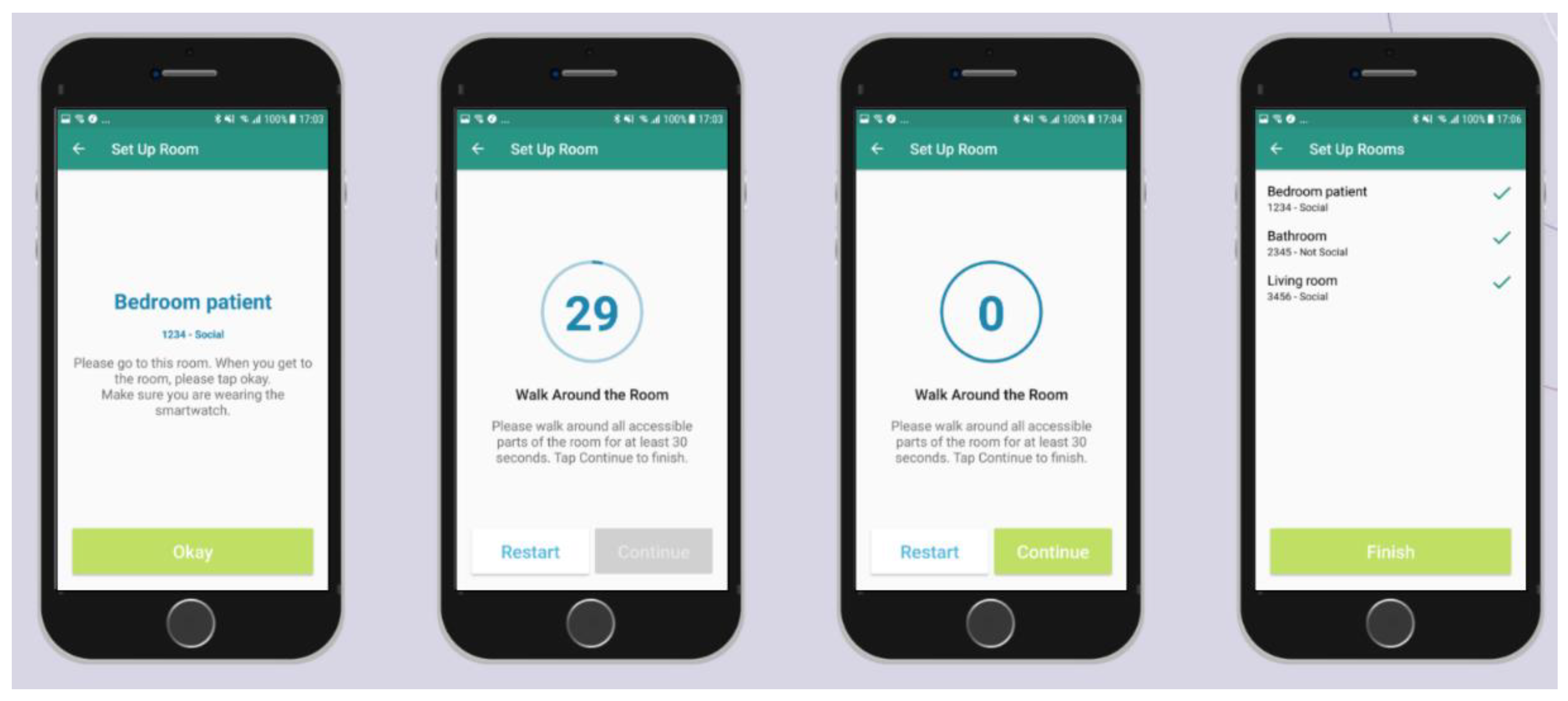
2.1. Technology and Instructions
2.2. Studies Where Data Was Collected
2.2.1. Clinical Trial
2.2.2. Internal Study with Healthy Volunteers
2.3. Algorithm
- Obtain the raw beacon signal per iBeacon from the smartwatch recording app;
- Resample the beacon signal with frequency of 1 Hz to account for any missing values due to interference/collisions (i.e., when two or more devices attempt to transmit data over a network at the same time);
- Perform linear interpolation per beacon on missing signal gaps below 5 min;
- Fill in any remaining missing data (i.e., for longer intervals than 5 min) with −100 dBm to indicate out of range/missing signal [7];
- Smooth signal per iBeacon using a Gaussian filter with window size of 90 s;
- Rescale signal to the range of [−100, −20] dBm per iBeacon;
- Normalize signal by dividing each iBeacon signal by its mean over the whole day;
- Compute the weight of each iBeacon (range of [0, 1]). The weight of each beacon is its normalized values per time point divided by the sum of the normalized values across all day. If we have in total N iBeacons and this weight is higher than pN = 1/N then the person could actually be in the room with this specific iBeacon;
- Compute and smooth signal derivatives per iBeacon using a Gaussian filter and a window of 90 s.
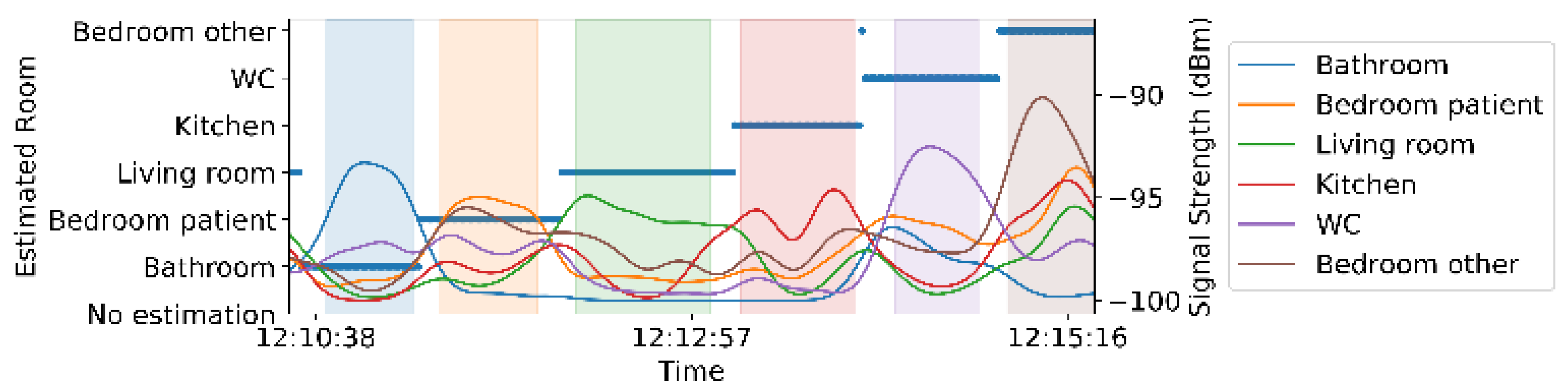
- Once we have all this information, we use it to estimate the room location for each second in the time range that we have iBeacon data for, as follows:
- Find the iBeacon (bi) with the maximum weight, and the maximum filtered beacon signal strength;
- If the weight of iBeacon bi is greater than threshold pN, and the derivative is not zero, then the estimated room location is set to the room with bi. The non-zero derivative indicates that there is variation in the signal and therefore not missing and replaced by a static value of −100 as described earlier;
- Otherwise, the estimated room location could either be set to unknown (if we are interested only in locations with high confidence), or if we want to avoid having gaps in our location estimation with lower confidence, then the estimated room location is set to the room with the iBeacon with maximum unscaled filtered signal. In our scenario, we are interested in having a continuous signal of room estimations, so we pick the latter approach;
- Once we have a continuous estimation of room locations, we filter out all time points and respective estimated locations while the participant was not wearing the watch. To estimate the spans that the participant was wearing the smartwatch, we were inspired by a previous publication [20]. We filtered out accelerometer data where the standard deviation of Euclidean norm was less than 0.04 m/s2 for more than 30 min, as during these spans smartwatches were likely not carried by the subjects. This threshold is higher than the threshold we used for smartphones [20], because the standard deviation of the background accelerometer signal is slightly higher than the smartphone.
2.4. Performance Metrics
3. Results
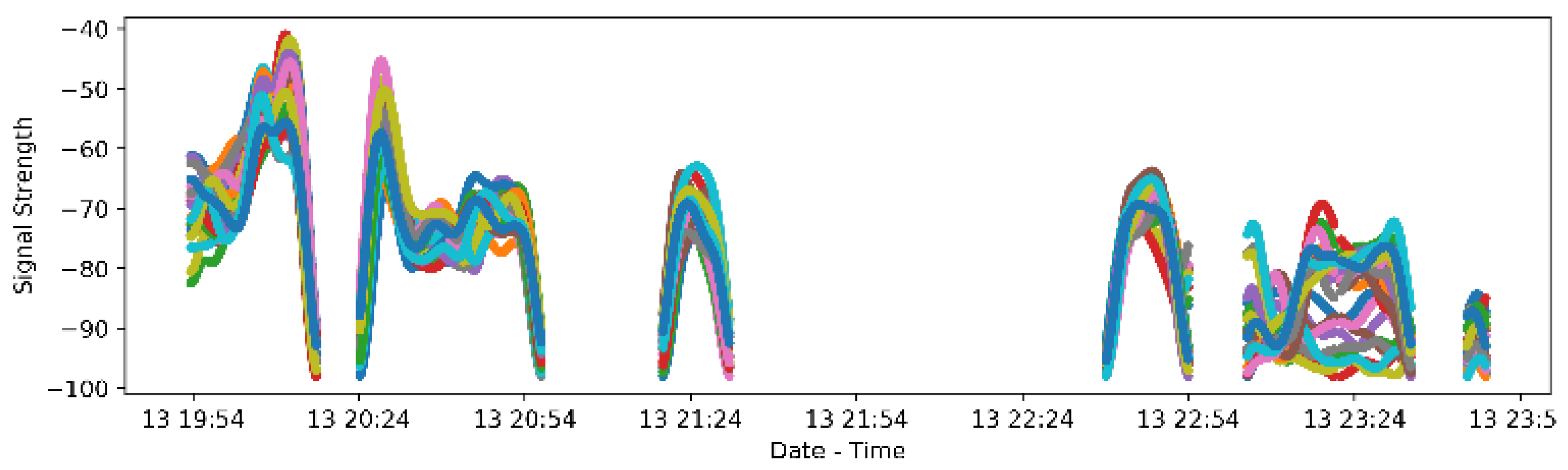
3.1. Signal Collection
3.2. Performance of the Approach in Healthy Volunteers
3.3. Feasibility of iBeacon Set Up in a Clinical Trial
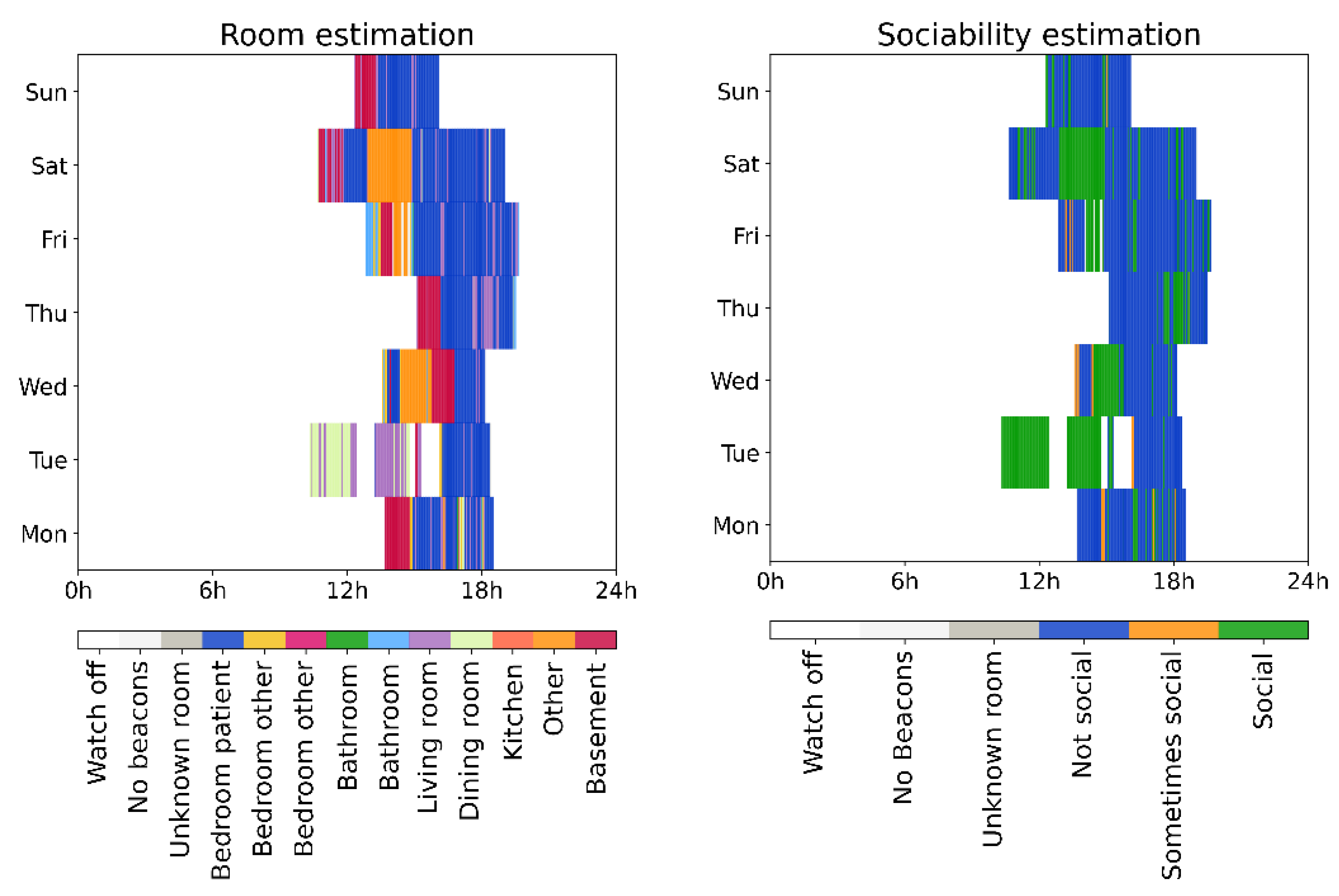
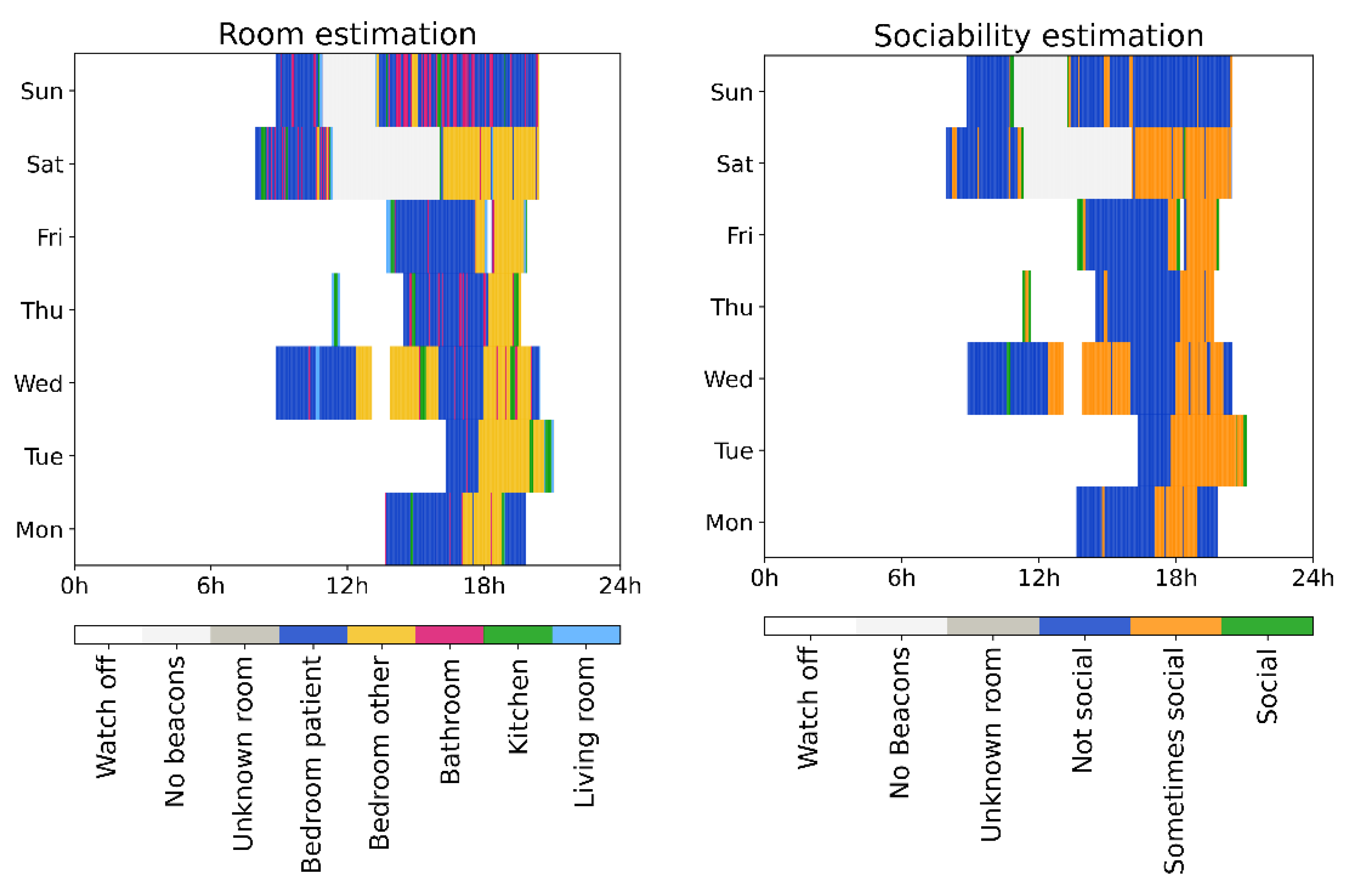
3.4. Examples from Individual Participants from the Clinical Trial
4. Discussion
4.1. Novelty and Principal Findings
4.2. Limitations
4.3. Sensor Setup Best Practices
4.4. Comparison with Prior Work
4.5. Learnings and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Autism and Autism and Developmental Disabilities Monitoring Network Surveillance Year 2008 Principal Investigators. Prevalence of Autism Spectrum Disorders—Autism and Developmental Disabilities Monitoring Network, 14 Sites, United States, 2008. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2012, 61, 1–19. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: Diagnostic and Statistical Manual of Mental Disorders (DSM-5®), 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Anagnostou, E.; Jones, N.; Huerta, M.; Halladay, A.K.; Wang, P.; Scahill, L.; Horrigan, J.P.; Kasari, C.; Lord, C.; Choi, D.; et al. Measuring Social Communication Behaviors as a Treatment Endpoint in Individuals with Autism Spectrum Disorder. Autism 2015, 19, 622–636. [Google Scholar] [CrossRef] [PubMed]
- Siafis, S.; Çıray, O.; Schneider-Thoma, J.; Bighelli, I.; Krause, M.; Rodolico, A.; Ceraso, A.; Deste, G.; Huhn, M.; Fraguas, D.; et al. Placebo response in pharmacological and dietary supplement trials of autism spectrum disorder (ASD): Systematic review and meta-regression analysis. Mol. Autism 2020, 11, 66. [Google Scholar] [CrossRef] [PubMed]
- Ware, S.; Yue, C.; Morillo, R.; Lu, J.; Shang, C.; Kamath, J.; Bamis, A.; Bi, J.; Russell, A.; Wang, B. Large-scale Automatic De-pression Screening Using Meta-data from WiFi Infrastructure. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2018, 2, 195. [Google Scholar] [CrossRef]
- Sun, S.; Folarin, A.A.; Ranjan, Y.; Rashid, Z.; Conde, P.; Stewart, C.; Cummins, N.; Matcham, F.; Dalla Costa, G.; Simblett, S.; et al. Using smartphones and wearable devices to monitor behavioural changes during COVID-19. J. Med Internet Res. 2020, 22, e19992. [Google Scholar] [CrossRef] [PubMed]
- Dong, K.; Ling, Z.; Xia, X.; Ye, H.; Wu, W.; Yang, M. Dealing with Insufficient Location Fingerprints in Wi-Fi Based In-door Location Fingerprinting. Wirel. Commun. Mob. Comput. 2017, 2017, 1268515. [Google Scholar] [CrossRef] [Green Version]
- Bagautdinov, T.; Alahi, A.; Fleuret, F.; Fua, P.; Savarese, S. Social Scene Understanding: End-to-End Multi-person Action Localization and Collective Activity Recognition. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 3425–3434. [Google Scholar]
- Allurwar, N.; Nawale, B.; Patel, S. Beacon for Proximity Target Marketing. Int. J. Eng. Comput. Sci. 2016, 5, 16359–16364. [Google Scholar] [CrossRef]
- Belka, R. An Indoor Tracking System and Pattern Recognition Algorithms as Key Components of IoT-based Entertainment Industry. In Photonics Applications in Astronomy, Communications, Industry, and HighEnergy Physics Experiments; International Society for Optics and Photonics: Bellingham, WA, USA, 2019; Volume 11176, pp. 1694–1703. [Google Scholar]
- Toledo-Castro, J.; Caballero-Gil, P.; Rodríguez-Pérez, N.; Santos-González, I.; Hernández-Goya, C. Beacon-Based Fuzzy Indoor Tracking at Airports. Proceedings 2018, 2, 1255. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Zhang, P.; Al Moubayed, S.; Patel, S.N.; Sample, A.P. ID-Match: A Hybrid Computer Vision and RFID System for Recognizing Individuals in Groups. In Proceedings of the Conference on Human Factors in Computing Systems, New York, NY, USA, 7–12 May 2016; ACM: New York, NY, USA, 2016; p. 7. [Google Scholar]
- Spachos, P.; Plataniotis, K.N. BLE Beacons for Indoor Positioning at an Interactive IoT-Based Smart Museum. IEEE Syst. J. 2020, 14, 3483–3493. [Google Scholar] [CrossRef] [Green Version]
- Shipkovenski, G.; Kalushkov, T.; Petkov, E.; Angelov, V. A Beacon-Based Indoor Positioning System for Location Track-ing of Patients in a Hospital. In Proceedings of the 2020 International Congress on Human-Computer Interaction, Optimization and Robotic Applications (HORA), Ankara, Turkey, 26–28 June 2020; pp. 1–6. [Google Scholar]
- Curran, K. Hybrid passive and active approach to tracking movement within indoor environments. IET Commun. 2018, 12, 1188–1194. [Google Scholar] [CrossRef] [Green Version]
- kontakt.io. Available online: https://store.kontakt.io/our-products/30-smart-beacon-sb16-2.html (accessed on 7 July 2021).
- Samsung Gear Sport Smartwatch. Available online: https://www.samsung.com/global/galaxy/gear-sport/specs/ (accessed on 7 July 2021).
- Iqbal, Z.; Luo, D.; Henry, P.; Kazemifar, S.; Rozario, T.; Yan, Y.; Westover, K.; Lu, W.; Nguyen, D.; Long, T.; et al. Accurate real time localization tracking in a clinical environment using Bluetooth Low Energy and deep learning. PLoS ONE 2018, 13, e0205392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniş, F.S.; Cemgil, A.T. Model-Based Localization and Tracking Using Bluetooth Low-Energy Beacons. Sensors 2017, 17, 2484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, W.-Y.; Lipsmeier, F.; Creigh, A.; Scotland, A.; Kilchenmann, T.; Jin, L.; Schjodt-Eriksen, J.; Wolf, D.; Zhang-Schaerer, Y.-P.; Garcia, I.F.; et al. Large-Scale Continuous Mobility Monitoring of Parkinson’s Disease Patients Using Smartphones; Wireless Mobile Communication and Healthcare; Springer Science and Business Media LLC: Cham, Switzerland, 2018; pp. 12–19. [Google Scholar]
- Rayanchu, S.; Mishra, A.; Agrawal, D.; Saha, S.; Banerjee, S. Diagnosing Wireless Packet Losses in 802.11: Separating Col-lision from Weak Signal. In Proceedings of the International Conference on Computer Communications, Phoenix, AZ, USA, 13–18 April 2008; pp. 735–743. [Google Scholar]
- Kyritsis, A.I.; Kostopoulos, P.; Deriaz, M.; Konstantas, D. A BLE-based probabilistic room-level localization method. In Proceedings of the 2016 International Conference on Localization and GNSS (ICL-GNSS), Barcelona, Spain, 28–30 June 2016; pp. 1–6. [Google Scholar]
- Li, X.; Deng, Z.; Rauchenstein, L.; Carlson, T. Contributed Review: Source-localization algorithms and applications us-ing time of arrival and time difference of arrival measurements. Rev. Sci. Instrum. 2016, 87, 041502. [Google Scholar] [CrossRef] [PubMed]
- Milioris, D.; Kriara, L.; Papakonstantinou, A.; Tzagkarakis, G.; Tsakalides, P.; Papadopouli, M. Empirical evaluation of signal-strength fingerprint positioning in wireless LANs. In Proceedings of the 13th ACM International Conference on Modeling, Analysis, and Simulation of Wireless and Mobile Systems; ACM: New York, NY, USA, 2016. [Google Scholar]
- Zwirello, L.; Schipper, T.; Harter, M.; Zwick, T. UWB Localization System for Indoor Applications: Concept, Realization and Analysis. J. Electr. Comput. Eng. 2012, 2012, 1–11. [Google Scholar] [CrossRef]
- Radu, V.; Kriara, L.; Marina, M.K. Pazl: A mobile crowdsensing based indoor WiFi monitoring system. In Proceedings of the 9th International Conference on Network and Service Management (CNSM 2013), Zurich, Switzerland, 14–18 October 2013; pp. 75–83. [Google Scholar]
- Kabelac, Z.; Tarolli, C.G.; Snyder, C.; Feldman, B.; Glidden, A.; Hsu, C.Y.; Hristov, R.; Dorsey, E.R.; Katabi, D. Passive Mon-itoring at Home: A Pilot Study in Parkinson Disease. Digit. Biomark. 2019, 3, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Urwyler, P.; Stucki, R.; Rampa, L.; Müri, R.; Mosimann, U.; Nef, T. Cognitive impairment categorized in communi-ty-dwelling older adults with and without dementia using in-home sensors that recognise activities of daily living. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surian, D.; Kim, V.; Menon, R.; Dunn, A.G.; Sintchenko, V.; Coiera, E. Tracking a moving user in indoor environments using Bluetooth low energy beacons. J. Biomed. Inform. 2019, 98, 103288. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Home Setup | Number of Rooms | Test Run | Test Run Accuracy (%) | Mean Setup Accuracy (%) | Wall Type | iBeacon Location in Room |
|---|---|---|---|---|---|---|
| 1 | 3 | 1–2 | 97.9, 100 | 98.9 | Concrete | By external walls |
| 2 | 5 | 3–4 | 97.7, 99 | 98.4 | Thin | Center |
| 3 | 7 | 5 | 92.8 | 92.8 | Thin | Center |
| 4 | 6 | 6–7 | 69.4, 70.3 | 69.8 | Thin | By shared walls |
| 5 | 5 | 8–9 | 93.9, 96.4 | 95.2 | Concrete | Center |
| 6 | 4 | 10 | 99.2 | 99.2 | Thin | By external walls |
| 7 | 4 | 11 | 91.4 | 91.4 | Thin | Center |
| 8 | 6 | 12–17 | 96.2, 100, 100, 100, 97.3, 100 | 98.9 | Concrete | Center |
| 9 | 4 | 18–38 | 97.7, 100, 100, 100, 97.7, 100, 100, 100, 100, 99.4, 100, 98.5, 99.4, 100, 97.7, 97.9, 100, 98, 100, 100, 100 | 99.3 | Concrete | Center |
| 10 | 5 | 39–45 | 95.2, 97.5, 99.4, 100, 98.3, 100, 97.6 | 98.3 | Concrete | Center |
| Wall Type | iBeacon Location in Room | Number of Home Setups | Mean Accuracy (%) |
|---|---|---|---|
| Concrete | - | 5 | 98.1 |
| Thin | - | 5 | 90.3 |
| - | Center | 7 | 96.3 |
| - | By external walls | 2 | 99.1 |
| - | By shared walls | 1 | 69.8 |
| Reason for Room Misclassification | Number of Occurrences | Percentage of Occurrences out of All Sources of Error | Median Error per Room Estimation |
|---|---|---|---|
| Previously visited as part of the test run | 13 | 33.3% | 2 s |
| Next visited as part of the test run | 11 | 28.2% | 2 s |
| Walk by/through room during room transition | 6 | 15.4% | 1 s |
| Neighboring rooms have very thin walls & iBeacons not in the center of each room | 4 | 10.3% | 11 s |
| Error with start/end ground truth recorder | 5 | 12.8% | 5 s |
| Technology | Calibration Needed | Sensor Exact Location in Room Needed | Centralized (Synchronization Needed) | Privacy Preserving | Off-the-Shelf Hardware |
|---|---|---|---|---|---|
| Wi-Fi | Yes | Maybe | Yes | Maybe | Maybe |
| Bluetooth/BLE | No | No | No | Yes | Yes |
| Cameras | Yes | Yes | Yes | No | Yes |
| UWB | No | Yes | Yes | Maybe | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kriara, L.; Hipp, J.; Chatham, C.; Nobbs, D.; Slater, D.; Lipsmeier, F.; Lindemann, M. Beacon-Based Remote Measurement of Social Behavior in ASD Clinical Trials: A Technical Feasibility Assessment. Sensors 2021, 21, 4664. https://doi.org/10.3390/s21144664
Kriara L, Hipp J, Chatham C, Nobbs D, Slater D, Lipsmeier F, Lindemann M. Beacon-Based Remote Measurement of Social Behavior in ASD Clinical Trials: A Technical Feasibility Assessment. Sensors. 2021; 21(14):4664. https://doi.org/10.3390/s21144664
Chicago/Turabian StyleKriara, Lito, Joerg Hipp, Christopher Chatham, David Nobbs, David Slater, Florian Lipsmeier, and Michael Lindemann. 2021. "Beacon-Based Remote Measurement of Social Behavior in ASD Clinical Trials: A Technical Feasibility Assessment" Sensors 21, no. 14: 4664. https://doi.org/10.3390/s21144664
APA StyleKriara, L., Hipp, J., Chatham, C., Nobbs, D., Slater, D., Lipsmeier, F., & Lindemann, M. (2021). Beacon-Based Remote Measurement of Social Behavior in ASD Clinical Trials: A Technical Feasibility Assessment. Sensors, 21(14), 4664. https://doi.org/10.3390/s21144664