
Frailty Level Classification of the Community Elderly Using Microsoft Kinect-Based Skeleton Pose: A Machine Learning Approach

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Acquisition and Description
2.1.1. Subjects
2.1.2. Experimental Test Procedure
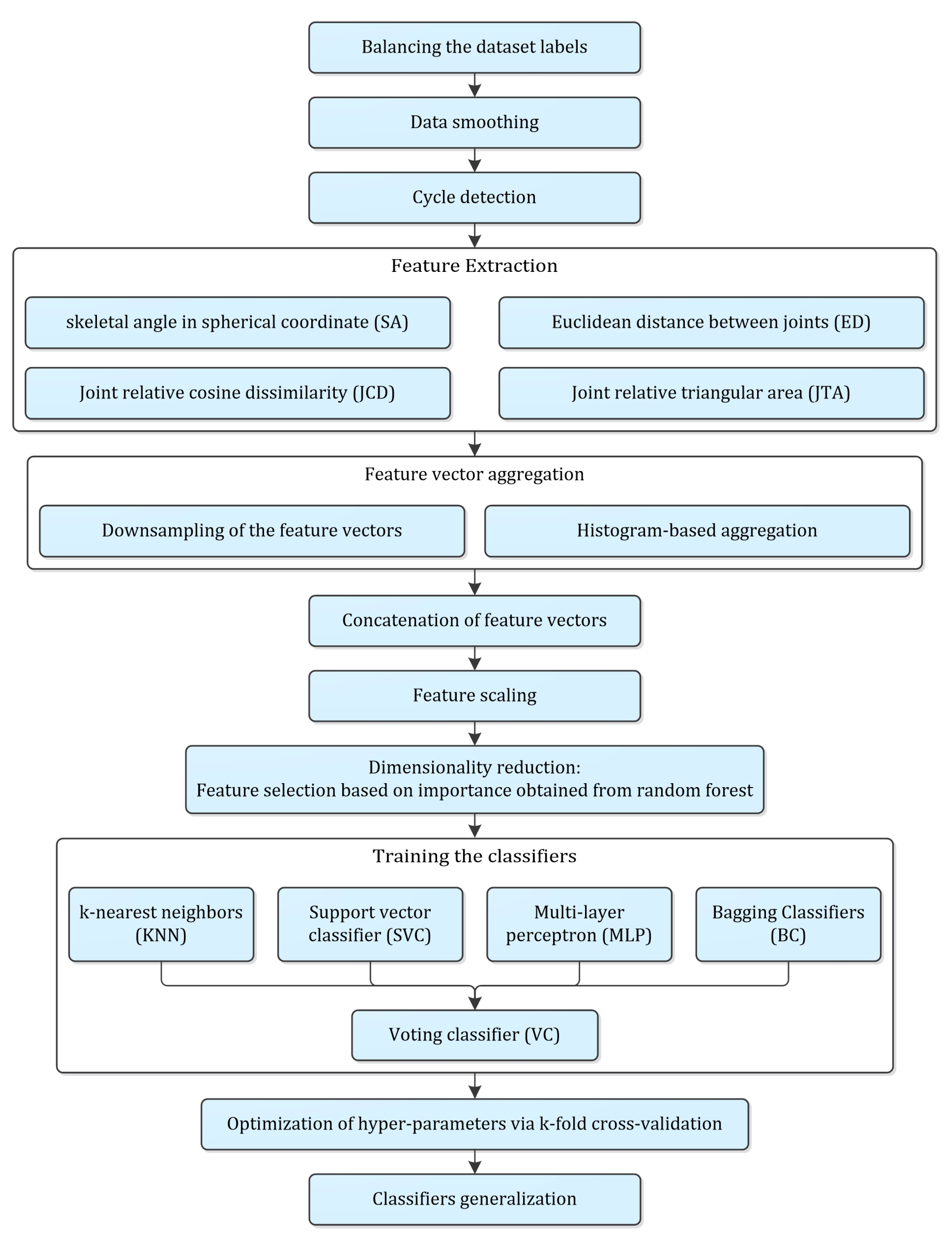
2.2. Proposed Methodology
2.2.1. Balancing the Dataset Labels
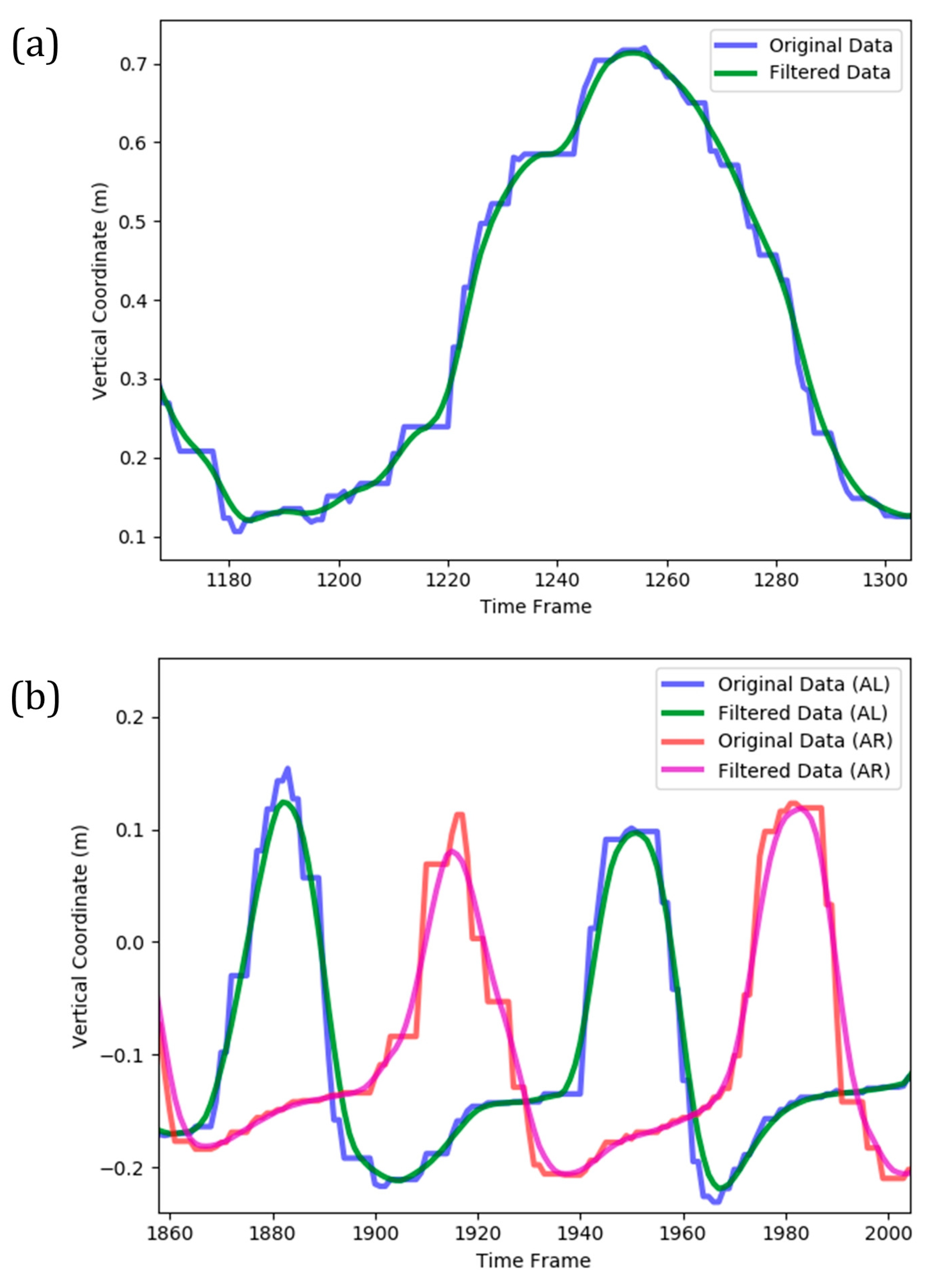
2.2.2. Data Smoothing
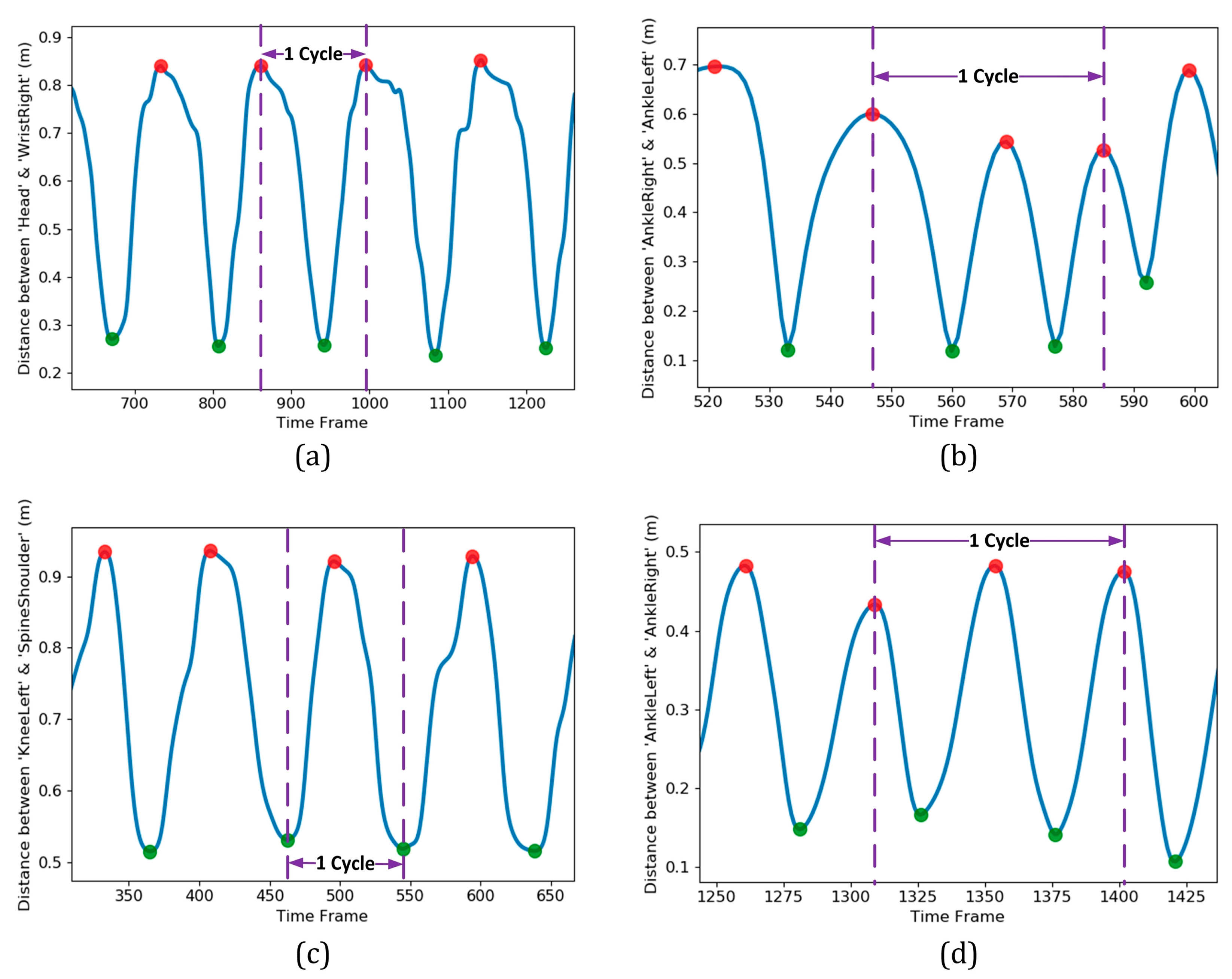
2.2.3. Cycle Detection
2.2.4. Feature Extraction
- The skeletal angle in spherical coordinate (SA): Two spherical coordinate angles (ϕ and θ) could be calculated for each pair of body joints with given Cartesian coordinates, namely and , as shown in Figure 6a [28]:where is the Euclidean distance between the two joints,Eight skeletal primitives, namely right- and left-side Humerus, Radius, Femur and Tibia were considered due to their dominant angular movements in different exercises. Based on this procedure, 16 feature vectors (8 vectors for each of angular components) were extracted, as well. They appeared as time-series with identical lengths as the original Kinect time series for each subject/exercise.
- Euclidean distance between joints (ED): The distance between each pair of body joints can be calculated instantaneously using Equation (4) [30]. This feature was useful in both cycle identification procedure (as summarized in Table 2) and classification stage. The number of feature vectors extracted by this approach is where was the number of active body joints, which was 21 by neglecting significance of the four body joints in the dynamics of the subject, namely left and right hand tip and thumb joints.
- Joint relative cosine dissimilarity (JCD): This feature represented the cosine distance between two arbitrary body joints in three-dimensional vector space. It was capable to reflect the directional motion of every body joint with respect to the others [23]. and were three-dimensional vectors between a common reference point with coordinate and two arbitrary body joints with coordinates and as illustrated in Figure 6b. The cosine dissimilarity () was defined as:where denotes the magnitude of each 3D vector. The spine body joint was considered as the reference point due to its stability in various skeletal movements. The cosine dissimilarity of each particular joint was calculated with respect to the remaining connected or non-connected body joints (except the spine joint, which is the reference point for all computations). The number of feature vectors obtained by this approach was .
- Joint relative triangular area (JTA): Relative position of three body joints could be considered concurrently by definition of joint relative triangular area. It calculated the area of the triangle constructed by the spine joint (as the most stable body joint) and two other arbitrary joints (Figure 6b). Let and have the same definition as those described for the cosine dissimilarity, then the joint relative triangular area () was calculated as:Since this feature was based on the geometry area, it was more stable than distance- or angle-based features and could be more robust for a noisy data set [23]. Every three-joint combination (including the spine as the reference joint) based on 21 active body joints were considered and joint relative triangular area was calculated accordingly. This lead to feature vectors for each subject/exercise.
2.2.5. Feature Vector Aggregation and Concatenation
- Resampling the data to a lower frame rate (downsampling of the feature vectors): After detection of a complete cycle, the segmented time series with different lengths for various subjects/exercises were resampled to a lower frame rate. Downsampling was performed by calculating the mean of data over each customized interval (bin) of the time series. Considering the number of bins to be , a vector with the same length was obtained for each feature type.
- Histogram-based aggregation: The histogram of each single- or multiple-cycle pattern in a predefined range was another way to downsample the original feature vector. The probability of data at each bin for a histogram with bins was then calculated to extract a vector with the same length as the aggregated vector for each feature type.After resampling each feature vector of a subject/exercise, all vectors should be concatenated into a unified feature vector for future stages. When all four feature types, namely SA, ED, JCD and JTA were implemented, the length of the concatenated feature vector was:where , , and are the number of feature vectors regarding each of the four feature types, respectively.
2.2.6. Scaling the Feature Space
2.2.7. Curse of Dimensionality and Necessity of Dimensionality Reduction
2.2.8. Training the Classifiers
- k-nearest neighbors (KNN): The frailty class in this instance-based model was determined from the majority vote among all neighbors identified based on the distance metric calculated in the feature space [54]. Simplicity of implementation and low computational cost on KNN inspire using this classifier in cases with comparable accuracies to more complicated classifiers.
- Support vector classifier (SVC): Using the so-called kernel trick approach to capture non-linear characteristics of the feature space, SVC provides a robust model that is suitable for classification of complex data sets with small to medium size [55]. This is particularly important for human skeleton data due to its inherent nonlinear characteristics that result in high-dimensional and multidisciplinary data [56]. SVC is robust to bias and variance of data, which are frequently observed in human gait or skeleton pose data, and results in accurate predictions for either binary or multiclass classifications [56]. The literature has also indicated that SVC is robust to overfitting and has a remarkable generalization capability [57].
- Multi-layer perceptron (MLP): Implementation of numerous layers in conjunction with applying non-linear activation functions in MLP introduce it as a powerful tool in classification of non-linear problems. Flexibility of MLP in the learning process regardless of network structure, particularly in higher dimensions of feature space, and its reasonable classification accuracy are the other supportive reasons for selection of this classifier. Based on the literature in human gait patterns recognition, the MLP classifier has resulted in satisfactory predictions by comparable or even higher accuracies with respect to the SVC [58,59,60].
- Ensemble classifiers: Aggregation of predictions performed by a group of classifiers could often enhance the accuracy compared to each individual classifier performance. Bagging and voting classifiers were two approaches among such ensemble learning methods, utilized in the present study.
- Bagging Classifier (BC) based on decision tree: The bagging classifier works based on this principle that a group of classifiers can be combined to form a more reliable classifier [55]. Individual decision tree classifiers as the weak learners were trained on multiple random subsets of the dataset while bagging aggregates them to extract the majority vote of all the predictors as the output class and possibly enhance the classifier accuracy [55]. Implementation of bagging classifier based on decision tree on the Kinect data was reported to be successful in accurate recognition of physical disorder [61].
- Voting classifier (VC): This ensemble approach aggregated the predictions made by multiple different classifiers (four previously mentioned classifiers) based on the predicted class probabilities to provide a more accurate classification. For instance, implementation of VC to predict freezing of gait in Parkinsonian patients using movement data from wearable sensors resulted in comparable accuracies to the SVM-based classifiers (as the most accurate estimators in that study) [62].
2.2.9. Optimization of Hyper-Parameters via k-Fold Cross-Validation and Generalization
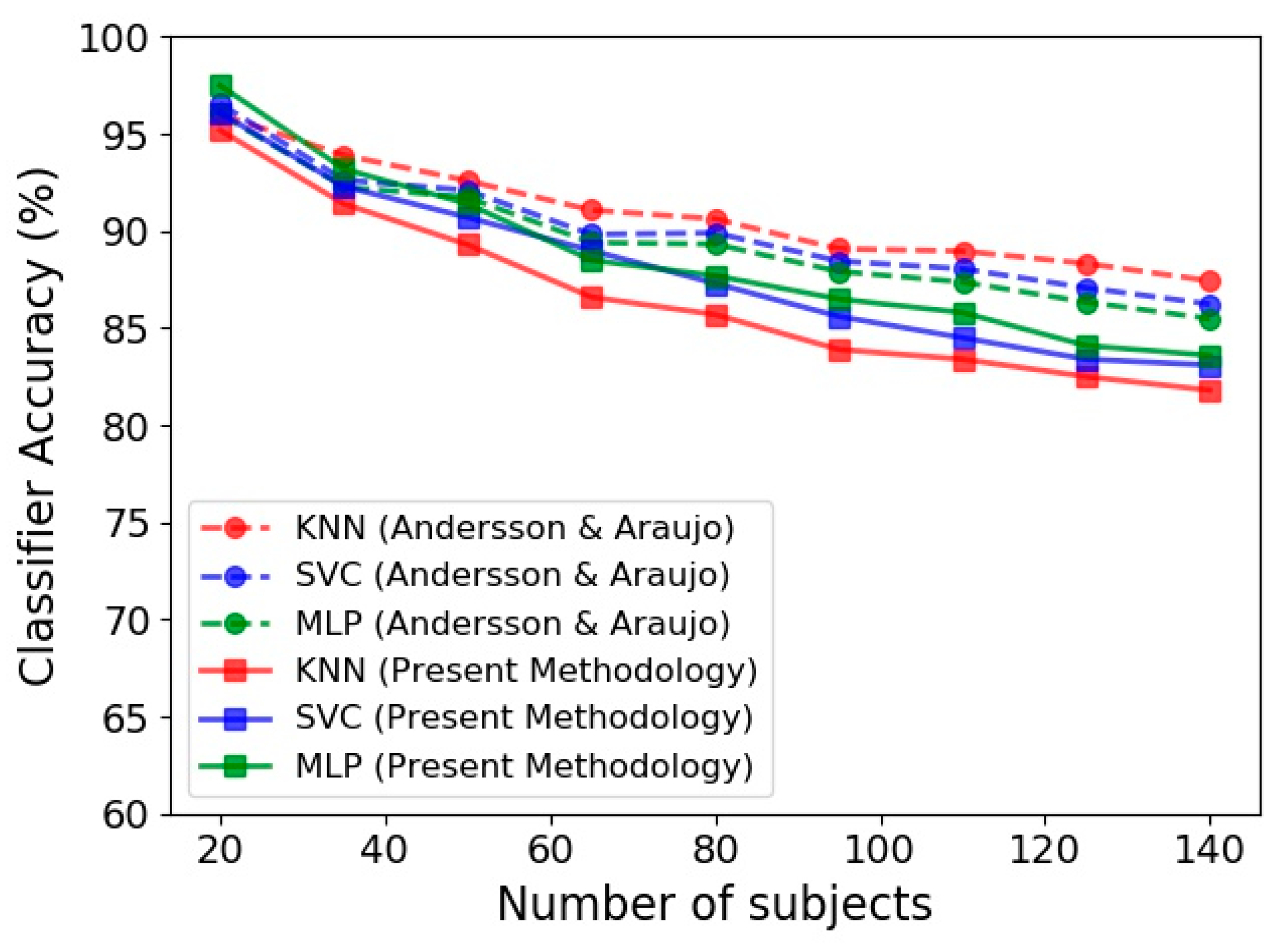
- The first was the data collected by Andersson and Araujo [29], known as Kinect gait biometry dataset, containing skeleton-based gait sequences of 140 subjects. Each walking time series has approximately 500–600 frames and 6–12 cycles.
- The second one was the dataset of the present study, in which the gender of subjects was considered as the classification target class. The gait analysis data of at most 140 individuals out of 787 subjects was used in the gender identification procedure.
3. Results
3.1. Validation of Classifiers
3.2. Frailty Level Classification Accuracy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xue, Q.-L. The frailty syndrome: Definition and natural history. Clin. Geriatr. Med. 2011, 27, 1–15. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Liu, C.K.; Fielding, R.A. Exercise as an Intervention for Frailty. Clin. Geriatr. Med. 2011, 27, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Parvaneh, S.; Mohler, J.; Toosizadeh, N.; Grewal, G.S.; Najafi, B. Postural Transitions during Activities of Daily Living Could Identify Frailty Status: Application of Wearable Technology to Identify Frailty during Unsupervised Condition. Gerontology 2017, 63, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Fugate Woods, N.; LaCroix, A.Z.; Gray, S.L.; Aragaki, A.; Cochrane, B.B.; Brunner, R.L.; Masaki, K.; Murray, A.; Newman, A.B. Frailty: Emergence and Consequences in Women Aged 65 and Older in the Women’s Health Initiative Observational Study. J. Am. Geriatr. Soc. 2005, 53, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, K.; Kivimaki, M.; Hamer, M.; Sabia, S.; Fransson, E.I.; Singh-Manoux, A.; Gale, C.R.; Batty, G.D. Measures of frailty in population-based studies: An overview. BMC Geriatr. 2013, 13. [Google Scholar] [CrossRef]
- Ibrahim, K.; Howson, F.F.A.; Culliford, D.J.; Sayer, A.A.; Roberts, H.C. The feasibility of assessing frailty and sarcopenia in hospitalised older people: A comparison of commonly used tools. BMC Geriatr. 2019, 19. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K. A global clinical measure of fitness and frailty in elderly people. Can. Med. Assoc. J. 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Rothman, M.D.; Leo-Summers, L.; Gill, T.M. Prognostic Significance of Potential Frailty Criteria. J. Am. Geriatr. Soc. 2008, 56, 2211–2216. [Google Scholar] [CrossRef]
- Pannurat, N.; Thiemjarus, S.; Nantajeewarawat, E. Automatic Fall Monitoring: A Review. Sensors 2014, 14, 12900–12936. [Google Scholar] [CrossRef]
- Ezeugwu, V.; Klaren, R.E.; Hubbard, E.A.; Manns, P.; Motl, R.W. Mobility disability and the pattern of accelerometer-derived sedentary and physical activity behaviors in people with multiple sclerosis. Prev. Med. Rep. 2015, 2, 241–246. [Google Scholar] [CrossRef]
- Elmannai, W.; Elleithy, K. Sensor-Based Assistive Devices for Visually-Impaired People: Current Status, Challenges, and Future Directions. Sensors 2017, 17, 565. [Google Scholar] [CrossRef]
- Almeida, O.; Zhang, M.; Liu, J.-C. Dynamic Fall Detection and Pace Measurement in Walking Sticks. In Proceedings of the Joint Workshop on High Confidence Medical Devices, Software, and Systems and Medical Device Plug-and-Play Interoperability, Boston, MA, USA, 25–27 June 2007; pp. 204–206. [Google Scholar] [CrossRef]
- Nikkhoo, M.; Niu, C.-C.; Fu, C.-J.; Lu, M.-L.; Chen, W.-C.; Lin, Y.-H.; Cheng, C.-H. Reliability and Validity of a Mobile Device for Assessing Head Control Ability. J. Med. Biol. Eng. 2020. [Google Scholar] [CrossRef]
- Delahoz, Y.; Labrador, M. Survey on Fall Detection and Fall Prevention Using Wearable and External Sensors. Sensors 2014, 14, 19806–19842. [Google Scholar] [CrossRef]
- Aurand, A.M.; Dufour, J.S.; Marras, W.S. Accuracy map of an optical motion capture system with 42 or 21 cameras in a large measurement volume. J. Biomech. 2017, 58, 237–240. [Google Scholar] [CrossRef]
- Colyer, S.L.; Evans, M.; Cosker, D.P.; Salo, A.I.T. A Review of the Evolution of Vision-Based Motion Analysis and the Integration of Advanced Computer Vision Methods Towards Developing a Markerless System. Sports Med. Open 2018, 4. [Google Scholar] [CrossRef]
- Mundher, Z.A.; Jiaofei, Z. A Real-Time Fall Detection System in Elderly Care Using Mobile Robot and Kinect Sensor. Int. J. Mater. Mech. Manuf. 2014, 2, 133–138. [Google Scholar] [CrossRef]
- Guerra, B.M.V.; Ramat, S.; Gandolfi, R.; Beltrami, G.; Schmid, M. Skeleton data pre-processing for human pose recognition using Neural Network. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 4265–4268. [Google Scholar] [CrossRef]
- Choppin, S.; Wheat, J. The potential of the Microsoft Kinect in sports analysis and biomechanics. Sports Technol. 2013, 6, 78–85. [Google Scholar] [CrossRef]
- Stamm, O.; Heimann-Steinert, A. Accuracy of Monocular Two-Dimensional Pose Estimation Compared With a Reference Standard for Kinematic Multiview Analysis: Validation Study. JMIR Mhealth Uhealth 2020, 8, e19608. [Google Scholar] [CrossRef]
- Baeza-Barragán, M.R.; Labajos Manzanares, M.T.; Ruiz Vergara, C.; Casuso-Holgado, M.J.; Martín-Valero, R. The Use of Virtual Reality Technologies in the Treatment of Duchenne Muscular Dystrophy: Systematic Review. JMIR Mhealth Uhealth 2020, 8, e21576. [Google Scholar] [CrossRef]
- Bari, A.S.M.H.; Gavrilova, M.L. Artificial Neural Network Based Gait Recognition Using Kinect Sensor. IEEE Access 2019, 7, 162708–162722. [Google Scholar] [CrossRef]
- Halilaj, E.; Rajagopal, A.; Fiterau, M.; Hicks, J.L.; Hastie, T.J.; Delp, S.L. Machine learning in human movement biomechanics: Best practices, common pitfalls, and new opportunities. J. Biomech. 2018, 81, 1–11. [Google Scholar] [CrossRef]
- Kidziński, Ł.; Yang, B.; Hicks, J.L.; Rajagopal, A.; Delp, S.L.; Schwartz, M.H. Deep neural networks enable quantitative movement analysis using single-camera videos. Nat. Commun. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Kastaniotis, D.; Theodorakopoulos, I.; Economou, G.; Fotopoulos, S. Gait based recognition via fusing information from Euclidean and Riemannian manifolds. Pattern Recognit. Lett. 2016, 84, 245–251. [Google Scholar] [CrossRef]
- Kastaniotis, D.; Theodorakopoulos, I.; Theoharatos, C.; Economou, G.; Fotopoulos, S. A framework for gait-based recognition using Kinect. Pattern Recognit. Lett. 2015, 68, 327–335. [Google Scholar] [CrossRef]
- Kastaniotis, D.; Theodorakopoulos, I.; Economou, G.; Fotopoulos, S. Gait-based gender recognition using pose information for real time applications. In Proceedings of the 2013 18th International Conference on Digital Signal Processing (DSP), Fira, Greece, 1–3 July 2013; pp. 1–6. [Google Scholar]
- Andersson, V.; Araujo, R. Person identification using anthropometric and gait data from kinect sensor. In Proceedings of the AAAI Conference on Artificial Intelligence, Austin, TX, USA, 25–30 January 2015; Available online: https://ojs.aaai.org/index.php/AAAI/article/view/9212 (accessed on 25 January 2015).
- Rahman, M.W.; Gavrilova, M.L. Kinect gait skeletal joint feature-based person identification. In Proceedings of the 2017 IEEE 16th International Conference on Cognitive Informatics & Cognitive Computing (ICCI* CC), Oxford, UK, 26–28 July 2017; pp. 423–430. [Google Scholar]
- Chen, K.; Vervoort, D.; Vuillerme, N.; Kosse, N.; Hortobágyi, T.; Lamoth, C.J.C. Multivariate Analyses and Classification of Inertial Sensor Data to Identify Aging Effects on the Timed-Up-and-Go Test. PLoS ONE 2016, 11, e0155984. [Google Scholar] [CrossRef]
- Greene, B.R.; Doheny, E.P.; O’Halloran, A.; Anne Kenny, R. Frailty status can be accurately assessed using inertial sensors and the TUG test. Age Ageing 2013, 43, 406–411. [Google Scholar] [CrossRef]
- Collado-Villaverde, A.; R-Moreno, M.D.; Barrero, D.F.; Rodriguez, D. Machine Learning Approach to Detect Falls on Elderly People Using Sound. In Advances in Artificial Intelligence: From Theory to Practice; Springer International Publishing: Cham, Switzerland, 2017; Volume 10350, pp. 149–159. [Google Scholar] [CrossRef]
- Lovis, C.; Albert, M.V.; Kording, K.; Herrmann, M.; Jayaraman, A. Fall Classification by Machine Learning Using Mobile Phones. PLoS ONE 2012, 7, e36556. [Google Scholar] [CrossRef]
- Tarekegn, A.; Ricceri, F.; Costa, G.; Ferracin, E.; Giacobini, M. Predictive Modeling for Frailty Conditions in Elderly People: Machine Learning Approaches. JMIR Med. Inform. 2020, 8, e16678. [Google Scholar] [CrossRef]
- Ambagtsheer, R.C.; Shafiabady, N.; Dent, E.; Seiboth, C.; Beilby, J. The application of artificial intelligence (AI) techniques to identify frailty within a residential aged care administrative data set. Int. J. Med. Inform. 2020, 136, 104094. [Google Scholar] [CrossRef]
- Peng, L.-N.; Hsiao, F.-Y.; Lee, W.-J.; Huang, S.-T.; Chen, L.-K. Comparisons Between Hypothesis- and Data-Driven Approaches for Multimorbidity Frailty Index: A Machine Learning Approach. J. Med. Internet Res. 2020, 22, e16213. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Schwenk, M.; Mohler, J.; Wendel, C.; D’Huyvetter, K.; Fain, M.; Taylor-Piliae, R.; Najafi, B. Wearable Sensor-Based In-Home Assessment of Gait, Balance, and Physical Activity for Discrimination of Frailty Status: Baseline Results of the Arizona Frailty Cohort Study. Gerontology 2015, 61, 258–267. [Google Scholar] [CrossRef]
- Alcazar, J.; Losa-Reyna, J.; Rodriguez-Lopez, C.; Alfaro-Acha, A.; Rodriguez-Mañas, L.; Ara, I.; García-García, F.J.; Alegre, L.M. The sit-to-stand muscle power test: An easy, inexpensive and portable procedure to assess muscle power in older people. Exp. Gerontol. 2018, 112, 38–43. [Google Scholar] [CrossRef]
- Baltasar-Fernandez, I.; Alcazar, J.; Rodriguez-Lopez, C.; Losa-Reyna, J.; Alonso-Seco, M.; Ara, I.; Alegre, L.M. Sit-to-stand muscle power test: Comparison between estimated and force plate-derived mechanical power and their association with physical function in older adults. Exp. Gerontol. 2021, 145, 111213. [Google Scholar] [CrossRef] [PubMed]
- Scholkmann, F.; Boss, J.; Wolf, M. An efficient algorithm for automatic peak detection in noisy periodic and quasi-periodic signals. Algorithms 2012, 5, 588–603. [Google Scholar] [CrossRef]
- Wu, Y.; Zhang, A. Feature selection for classifying high-dimensional numerical data. In Proceedings of the 2004 IEEE Computer Society Conference on Computer Vision and Pattern Recognition, Washington, DC, USA, 27 June–2 July 2004. [Google Scholar]
- Menze, B.H.; Kelm, B.M.; Masuch, R.; Himmelreich, U.; Bachert, P.; Petrich, W.; Hamprecht, F.A. A comparison of random forest and its Gini importance with standard chemometric methods for the feature selection and classification of spectral data. BMC Bioinform. 2009, 10, 1–16. [Google Scholar] [CrossRef]
- Chen, R.-C.; Dewi, C.; Huang, S.-W.; Caraka, R.E. Selecting critical features for data classification based on machine learning methods. J. Big Data 2020, 7, 1–26. [Google Scholar] [CrossRef]
- Kawakubo, H.; Yoshida, H. Rapid feature selection based on random forests for high-dimensional data. Expert Syst. Appl. 2012, 40, 6241–6252. [Google Scholar]
- Archer, K.J.; Kimes, R.V. Empirical characterization of random forest variable importance measures. Comput. Stat. Data Anal. 2008, 52, 2249–2260. [Google Scholar] [CrossRef]
- Saeys, Y.; Inza, I.; Larranaga, P. A review of feature selection techniques in bioinformatics. Bioinformatics 2007, 23, 2507–2517. [Google Scholar] [CrossRef]
- Dindorf, C.; Konradi, J.; Wolf, C.; Taetz, B.; Bleser, G.; Huthwelker, J.; Drees, P.; Fröhlich, M.; Betz, U. General method for automated feature extraction and selection and its application for gender classification and biomechanical knowledge discovery of sex differences in spinal posture during stance and gait. Comput. Methods Biomech. Biomed. Eng. 2020, 1–9. [Google Scholar] [CrossRef]
- Ebina, T.; Toh, H.; Kuroda, Y. DROP: An SVM domain linker predictor trained with optimal features selected by random forest. Bioinformatics 2011, 27, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Wang, Y.; Chen, C.; Ricanek, K. Improved image-based automatic gender classification by feature selection. J. Artif. Intell. Soft Comput. Res. 2011, 1, 241–253. [Google Scholar]
- Chen, Y.-W.; Lin, C.-J. Combining SVMs with various feature selection strategies. In Feature Extraction; Springer: Cham, Switzerland, 2006; pp. 315–324. [Google Scholar]
- Rahman, M.S.; Rahman, M.K.; Kaykobad, M.; Rahman, M.S. isGPT: An optimized model to identify sub-Golgi protein types using SVM and Random Forest based feature selection. Artif. Intell. Med. 2018, 84, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, M.; Khan, M.B.; Bashier, E.B.M. Machine Learning: Algorithms and Applications; CRC Press: Boca Raton, FL, USA, 2016. [Google Scholar]
- Marsland, S. Machine Learning: An Algorithmic Perspective; CRC Press: Boca Raton, FL, USA, 2015. [Google Scholar]
- Figueiredo, J.; Santos, C.P.; Moreno, J.C. Automatic recognition of gait patterns in human motor disorders using machine learning: A review. Med. Eng. Phys. 2018, 53, 1–12. [Google Scholar] [CrossRef]
- Khera, P.; Kumar, N. Role of machine learning in gait analysis: A review. J. Med. Eng. Technol. 2020, 44, 441–467. [Google Scholar] [CrossRef]
- Zhang, Y.; Ma, Y. Application of supervised machine learning algorithms in the classification of sagittal gait patterns of cerebral palsy children with spastic diplegia. Comput. Biol. Med. 2019, 106, 33–39. [Google Scholar] [CrossRef]
- Chan, H.; Yang, M.; Wang, H.; Zheng, H.; McClean, S.; Sterritt, R.; Mayagoitia, R.E. Assessing gait patterns of healthy adults climbing stairs employing machine learning techniques. Int. J. Intell. Syst. 2013, 28, 257–270. [Google Scholar] [CrossRef]
- Pogorelc, B.; Bosnić, Z.; Gams, M. Automatic recognition of gait-related health problems in the elderly using machine learning. Multimed. Tools Appl. 2012, 58, 333–354. [Google Scholar] [CrossRef]
- Saha, S.; Pal, M.; Konar, A.; Roy, J. Ensemble Classifier-Based Physical Disorder Recognition System Using Kinect Sensor. In Computational Advancement in Communication Circuits and Systems; Springer: Cham, Switzerland, 2015; pp. 169–175. [Google Scholar]
- Arami, A.; Poulakakis-Daktylidis, A.; Tai, Y.F.; Burdet, E. Prediction of gait freezing in Parkinsonian patients: A binary classification augmented with time series prediction. IEEE Trans. Neural. Syst. Rehabil. Eng. 2019, 27, 1909–1919. [Google Scholar] [CrossRef] [PubMed]
- Bergstra, J.; Bengio, Y. Random search for hyper-parameter optimization. J. Mach. Learn. Res. 2012, 13, 281–305. [Google Scholar]
- Panhwar, Y.N.; Naghdy, F.; Naghdy, G.; Stirling, D.; Potter, J. Assessment of frailty: A survey of quantitative and clinical methods. BMC Biomed. Eng. 2019, 1. [Google Scholar] [CrossRef] [PubMed]
- Barreira, C.C.; Forner-Cordero, A.; Grangeiro, P.M.; Moura, R.T. Kinect v2 based system for gait assessment of children with cerebral palsy in rehabilitation settings. J. Med. Eng. Technol. 2020, 44, 198–202. [Google Scholar] [CrossRef]
- Yeung, L.F.; Cheng, K.C.; Fong, C.H.; Lee, W.C.C.; Tong, K.-Y. Evaluation of the Microsoft Kinect as a clinical assessment tool of body sway. Gait Posture 2014, 40, 532–538. [Google Scholar] [CrossRef] [PubMed]
- Eltoukhy, M.A.; Kuenze, C.; Oh, J.; Signorile, J.F. Validation of Static and Dynamic Balance Assessment Using Microsoft Kinect for Young and Elderly Populations. IEEE J. Biomed. Health Inform. 2018, 22, 147–153. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Cardiovascular Health Study (CHS) Measure | Value/Criteria |
|---|---|---|
| Characterizing Parameters | ||
| Weight Loss (WL) | Weight loss (unintentional loss greater than 10 lbs. in the past year) | 0: No 1: Yes |
| Weakness (WK) | Grip strength: lowest 20% by gender and BMI (Based on the appendix of Fried et al. [2]) | 0: No 1: Yes |
| Poor Endurance (PE) | “Exhaustion” (self-report) | 0: No 1: Yes |
| Slowness (SL) | Walking time speed/15 feet: slowest 20% by gender and height (Based on the appendix of Fried et al. [2]) | 0: No 1: Yes |
| Low Physical Activity (LA) | Kcals/week: lowest 20% Males: <383 Kcals/week Females: <270 Kcals/week | 0: No 1: Yes |
| Frailty score definition and criteria | ||
| Frailty score (FS) | Calculated based on the Fried definition (Equation (1)) | 0: healthy 1–2: Pre-frail 3–5: frail |
| Type of Exercise | Distance Metric Utilized to Identify the Cycle(s) | Portion of Time Series That Could Be Considered as a Complete Cycle | Additional Comments |
|---|---|---|---|
| Arm curled | 3D distance between ‘Head’ and ‘WristRight’ or ‘WristLeft’, depending on the dominant hand | Starting from a global maximum and reaching the subsequent global maximum after passing a global minimum | The ‘Head’ position was utilized as fairly fixed reference coordinates that successfully help in detection of the cycle’s extremum points |
| Gait analysis | 3D distance between left and right ankles coordinate | Starting from a global maximum and ending at its second subsequent global maximum | A maximum of distance metric corresponded to the farthest positions of the left and right ankles, while the minimum occurred when the ankles had the nearest positions |
| Repeatedly sit and stand | 3D distance between ‘KneeLeft’ and ‘SpineShoulder’ coordinates | Starting from a global minimum and reaching the subsequent global minimum after passing a global maximum | The maximum of the distance metric corresponded to the standing position while the minimum occurred when the subject was sat on the bench |
| Two-minute step | 3D distance between left and right ankles coordinate | Starting from a global maximum and ending at its second subsequent global maximum | Each maximum of distance metric corresponded to the highest vertical level of the lifting foot, while the minimum occurred in the standing position with both feet on the floor |
| Classifier | Dataset of Andersson and Araujo [29] | The Present Dataset | |
|---|---|---|---|
| Present Methodology | Andersson and Araujo Methodology [29] | ||
| KNN | 81.82 | 87.43 | 90.73 |
| SVC | 83.09 | 86.24 | 91.67 |
| MLP | 83.64 | 85.48 | 91.14 |
| BAG | 82.62 | NA | 92.03 |
| VC | 83.22 | NA | 90.85 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akbari, G.; Nikkhoo, M.; Wang, L.; Chen, C.P.C.; Han, D.-S.; Lin, Y.-H.; Chen, H.-B.; Cheng, C.-H. Frailty Level Classification of the Community Elderly Using Microsoft Kinect-Based Skeleton Pose: A Machine Learning Approach. Sensors 2021, 21, 4017. https://doi.org/10.3390/s21124017
Akbari G, Nikkhoo M, Wang L, Chen CPC, Han D-S, Lin Y-H, Chen H-B, Cheng C-H. Frailty Level Classification of the Community Elderly Using Microsoft Kinect-Based Skeleton Pose: A Machine Learning Approach. Sensors. 2021; 21(12):4017. https://doi.org/10.3390/s21124017
Chicago/Turabian StyleAkbari, Ghasem, Mohammad Nikkhoo, Lizhen Wang, Carl P. C. Chen, Der-Sheng Han, Yang-Hua Lin, Hung-Bin Chen, and Chih-Hsiu Cheng. 2021. "Frailty Level Classification of the Community Elderly Using Microsoft Kinect-Based Skeleton Pose: A Machine Learning Approach" Sensors 21, no. 12: 4017. https://doi.org/10.3390/s21124017
APA StyleAkbari, G., Nikkhoo, M., Wang, L., Chen, C. P. C., Han, D.-S., Lin, Y.-H., Chen, H.-B., & Cheng, C.-H. (2021). Frailty Level Classification of the Community Elderly Using Microsoft Kinect-Based Skeleton Pose: A Machine Learning Approach. Sensors, 21(12), 4017. https://doi.org/10.3390/s21124017