
Machine Learning Prediction of Fall Risk in Older Adults Using Timed Up and Go Test Kinematics



Abstract
1. Introduction
- The geriatrician’s fall-risk assessment is facilitated by combining an affordable and convenient way of measuring patients’ gait and balance. This inexpensive method can provide performance comparable to the human clinician’s assessment.
- This is the first paper to compare a prediction model with a geriatrician’s assessment of fall risk, which synthesizes information on fall risk factors (medical health status, gait impairments, and fall history), rather than only relying on the fall incidents, which can increase the error of false negatives.
- Sensor location was navigated to guarantee data acquisition from three important body points that we consider relevant to fall-risk prediction. Comparison of kinematics data from three sensor locations is conducted to investigate the most effective measurement of risk factors.
2. Materials and Methods
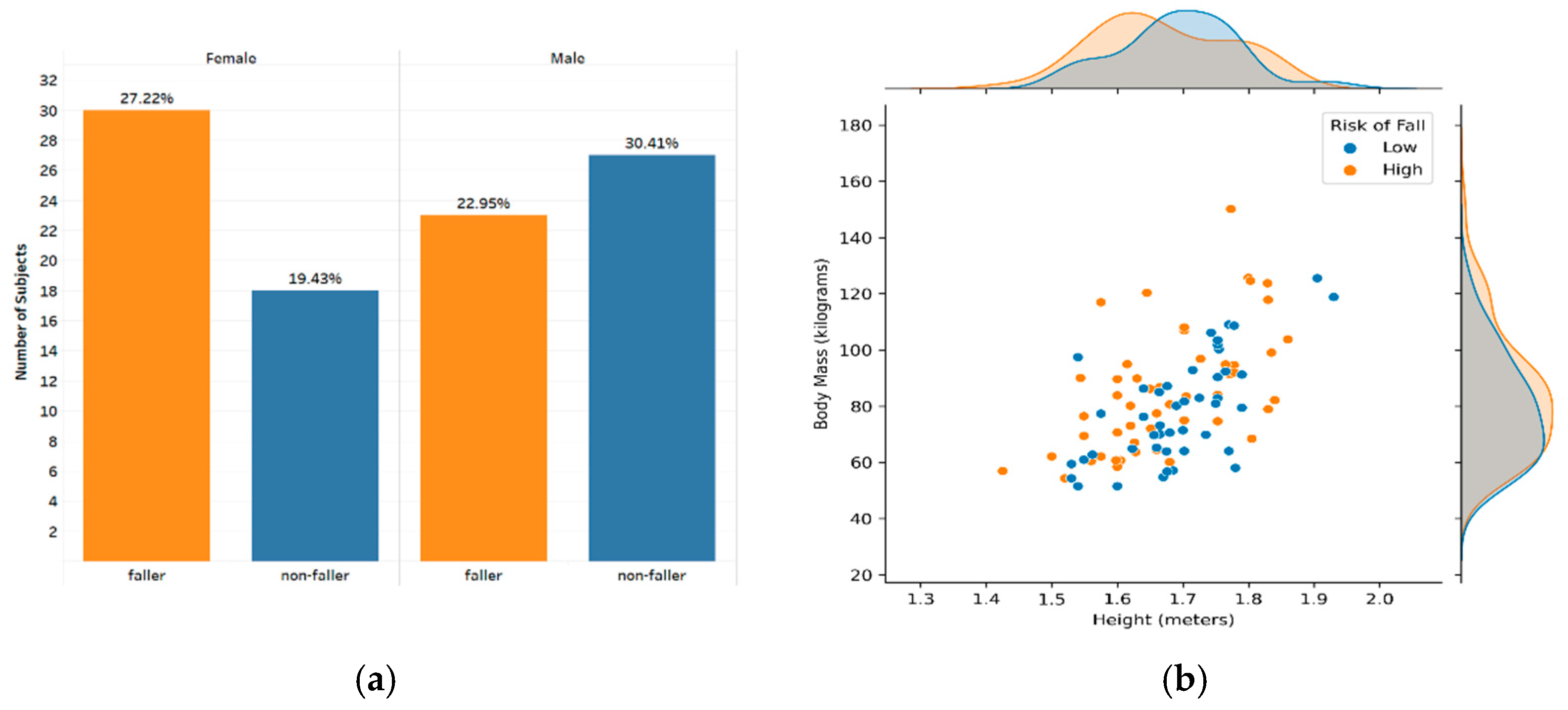
2.1. Population
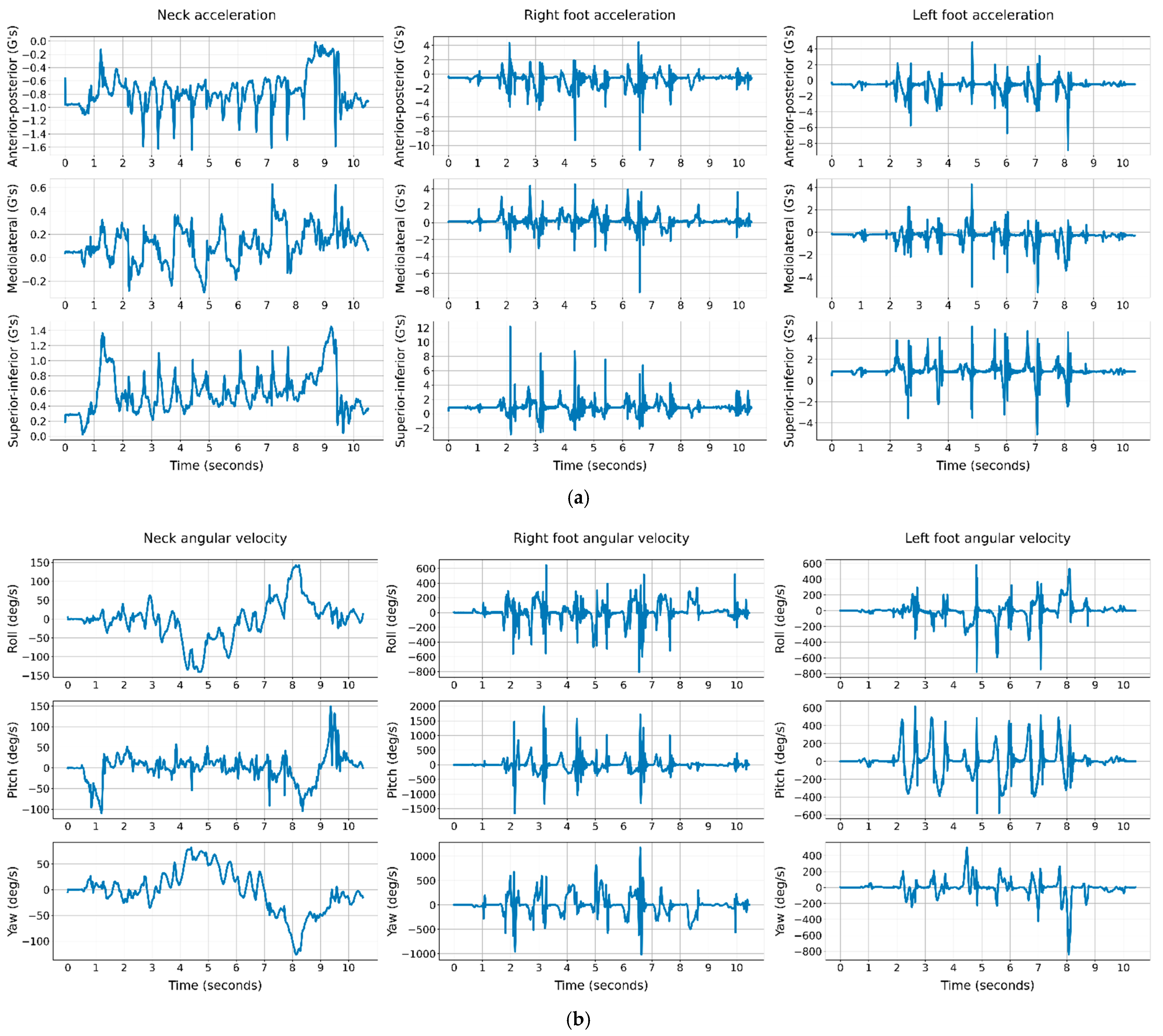
2.2. Data Acquisition
2.3. CNN Model with the Segmented Raw Signals of the TUG Test
3. Results
3.1. The Clinical Scoring Tests in Predicting Geriatrician’s Fall Classification
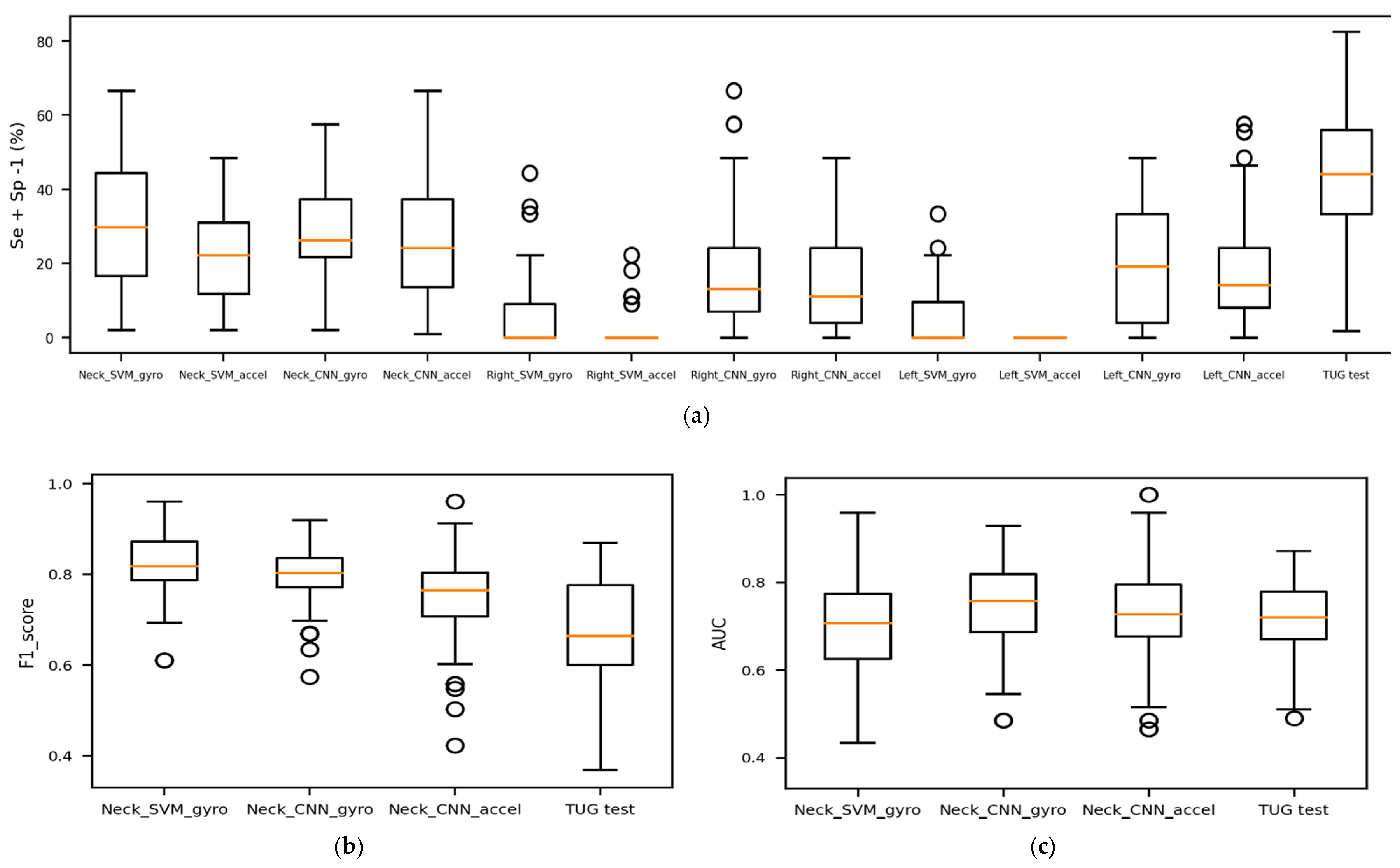
3.2. The CNN Prediction of Geriatrician’s Fall Classification
3.3. The CNN Prediction of the Follow-Up Falls Report
3.4. The Geriatrician’s Classification of the Follow-Up Falls Report
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tests | Function | Measurement | Assessment | Average Completion Time |
|---|---|---|---|---|
| FSST | Stepping over multiple low objects in different directions. | completion time | dynamic standing stability | <5 m |
| TUG test | Standing up from a chair, walking for three meters, turning, walking back to the chair, and sitting down. | completion time | gait and balance | <2 m |
| FRT | Measures the maximum forward reach without moving the feet (while standing in a fixed position). | maximum forward reach | stability and balance | <2 m |
| Step test | Stepping on the same foot on a stair without moving the other foot for 15 s. | number of steps | dynamic standing stability | <1 m |
| BBS | Performing 14 static and dynamic balance-related tasks, including standing, sitting, turning, reaching forward. | a total score of all the tasks | stability and balance | >15 m |
| 4-stage balance | Standing in 4 different foot positions, in each stage, not moving the feet while keeping the balance. | total time of keeping the balance | stability and balance | <2 m |
| 30 sec stand | Standing up from a chair and sitting back, repeating this move for 30 s. | number of stands, age- and gender-dependent | functional lower extremity strength | <2 m |
References
- Falls Prevention Conversation Guide for Caregivers. Available online: https://www.ncoa.org/article/falls-prevention-conversation-guide-for-caregivers (accessed on 10 March 2021).
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/ (accessed on 15 December 2020).
- Stay Independent: Prevent Falls. Available online: https://www.cdc.gov/steadi/pdf/STEADI_OlderAdultFactSheet-a.pdf (accessed on 10 March 2021).
- Medina, L.; Sabo, S.; Vespa, J. Living Longer: Historical and Projected Life Expectancy in the United States, 1960 to 2060; US Department of Commerce, US Census Bureau: Suitland, MD, USA, 2020.
- Hayes, W.C.; Myers, E.R.; Morris, J.N.; Gerhart, T.N.; Yett, H.S.; Lipsitz, L.A. Impact near the hip dominates fracture risk in elderly nursing home residents who fall. Calcif. Tissue Int. 1993, 52, 192–198. [Google Scholar] [CrossRef]
- Sterling, D.A.; O’connor, J.A.; Bonadies, J. Geriatric falls: Injury severity is high and disproportionate to mechanism. J. Trauma Acute Care Surg. 2001, 50, 116–119. [Google Scholar] [CrossRef]
- Jager, T.E.; Weiss, H.B.; Coben, J.H.; Pepe, P.E. Traumatic brain injuries evaluated in U.S. emergency departments, 1992–1994. Acad. Emerg. Med. 2000, 7, 134–140. [Google Scholar] [CrossRef]
- Alexander, B.H.; Rivara, F.P.; Wolf, M.E. The cost and frequency of hospitalization for fall-related injuries in older adults. Am. J. Public Health 1992, 82, 1020–1023. [Google Scholar] [CrossRef]
- Kuzuya, M.; Masuda, Y.; Hirakawa, Y.; Iwata, M.; Enoki, H.; Hasegawa, J.; Izawa, S.; Iguchi, A. Falls of the elderly are associated with burden of caregivers in the community. Int. J. Geriatr. Psychiatry 2006, 21, 740–745. [Google Scholar] [CrossRef] [PubMed]
- Dow, B.; Meyer, C.; Moore, K.J.; Hill, K.D. The impact of care recipient falls on caregivers. Aust. Health Rev 2013, 37, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Important Facts about Falls. Available online: https://www.cdc.gov/homeandrecreationalsafety/falls/adultfalls.html (accessed on 10 March 2021).
- Berg, R.L.; Cassells, J.S. Falls in older persons: Risk factors and prevention. In The Second Fifty Years: Promoting Health and Preventing Disability; National Academies Press: Washington, DC, USA, 1992. [Google Scholar]
- Environmental Causes of Falls—#81. Available online: https://www.geriatricfastfacts.com/fast-facts/environmental-causes-falls (accessed on 15 December 2020).
- Dite, W.; Temple, V.A. A clinical test of stepping and change of direction to identify multiple falling older adults. Arch. Phys. Med. Rehabil. 2002, 83, 1566–1571. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- Duncan, P.W.; Weiner, D.K.; Chandler, J.; Studenski, S. Functional reach: A new clinical measure of balance. J. Gerontol. 1990, 45, M192–M197. [Google Scholar] [CrossRef]
- Hill, K.D.; Bernhardt, J.; McGann, A.M.; Maltese, D.; Berkovits, D. A new test of dynamic standing balance for stroke patients: Reliability, validity and comparison with healthy elderly. Physiother. Can. 1996, 48, 257–262. [Google Scholar] [CrossRef]
- Berg, K.; Wood-Dauphine, S.; Williams, J.I.; Gayton, D. Measuring balance in the elderly: Preliminary development of an instrument. Physiother. Can. 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Stevens, J.A.; Phelan, E.A. Development of STEADI: A fall prevention resource for health care providers. Health Promot. Pract. 2013, 14, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Algorithm for Fall Risk Screening, Assessment, and Intervention. Available online: https://www.cdc.gov/steadi/pdf/STEADI-Algorithm-508.pdf (accessed on 10 August 2020).
- Materials for Healthcare Providers. Available online: https://www.cdc.gov/steadi/materials.html (accessed on 10 August 2020).
- Functional Assessments. Available online: https://www.cdc.gov/steadi/materials.html (accessed on 10 August 2020).
- Checklist—Fall Risk Factors. Available online: https://www.cdc.gov/steadi/pdf/STEADI-Form-RiskFactorsCk-508.pdf (accessed on 10 August 2020).
- Arnold, C.M.; Faulkner, R.A. The history of falls and the association of the timed up and go test to falls and near-falls in older adults with hip osteoarthritis. BMC Geriatr. 2007, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Reference values for the timed up and go test: A descriptive meta-analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef]
- Greene, B.R.; O’Donovan, A.; Romero-Ortuno, R.; Cogan, L.; Scanaill, C.N.; Kenny, R.A. Quantitative falls risk assessment using the timed up and go test. IEEE Trans. Biomed. Eng. 2010, 57, 2918–2926. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Herman, T.; Plotnik, M.; Brozgol, M.; Giladi, N.; Hausdorff, J.M. An instrumented timed up and go: The added value of an accelerometer for identifying fall risk in idiopathic fallers. Physiol. Meas. 2011, 32, 2003. [Google Scholar] [CrossRef]
- Buisseret, F.; Catinus, L.; Grenard, R.; Jojczyk, L.; Fievez, D.; Barvaux, V.; Dierick, F. Timed Up and Go and Six-Minute Walking Tests with Wearable Inertial Sensor: One Step Further for the Prediction of the Risk of Fall in Elderly Nursing Home People. Sensors 2020, 20, 3207. [Google Scholar] [CrossRef]
- The RunScribe System. Available online: https://runscribe.com/ (accessed on 15 December 2020).
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the timed up and go test. Phys. Ther. 2001, 18, 889–914. [Google Scholar] [CrossRef]
- Someshwar, H.P.; Kunde, C.; Ganvir, S.S. Predicting the probability of falls in geriatrics using traditional timed up and go test and dual-task constraint timed up and go test: An observational study. Int. J. Health Allied Sci. 2017, 6, 88–92. [Google Scholar]
- Goetzinger, K.R.; Odibo, A.O. Statistical analysis and interpretation of prenatal diagnostic imaging studies, Part 1: Evaluating the efficiency of screening and diagnostic tests. J. Ultrasound Med. 2011, 30, 1121–1127. [Google Scholar] [CrossRef]
- Maxim, L.D.; Niebo, R.; Utell, M.J. Screening tests: A review with examples. Inhal. Toxicol. 2014, 26, 811–828. [Google Scholar] [CrossRef] [PubMed]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the 2017 IEEE international conference on computer vision (ICCV), Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- Zakaria, N.A.; Kuwae, Y.; Tamura, T.; Minato, K.; Kanaya, S. Quantitative analysis of fall risk using TUG test. Comput. Methods Biomech. Biomed. Eng. 2015, 18, 426–437. [Google Scholar] [CrossRef] [PubMed]
- Misu, S.; Asai, T.; Ono, R.; Sawa, R.; Tsutsumimoto, K.; Ando, H.; Doi, T. Development and validity of methods for the estimation of temporal gait parameters from heel-attached inertial sensors in younger and older adults. Gait Posture 2017, 57, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Dadashi, F.; Mariani, B.; Rochat, S.; Büla, C.J.; Santos-Eggimann, B.; Aminian, K. Gait and foot clearance parameters obtained using shoe-worn inertial sensors in a large-population sample of older adults. Sensors 2014, 14, 443–457. [Google Scholar] [CrossRef]
- Kim, J.; Bae, M.N.; Lee, K.B.; Hong, S.G. Gait event detection algorithm based on smart insoles. ETRI J. 2020, 42, 46–53. [Google Scholar] [CrossRef]
- Tschopp, F.; Riner, M.; Fehr, M.; Bernreiter, L.; Furrer, F.; Novkovic, T.; Pfrunder, A.; Cadena, C.; Siegwart, R.; Nieto, J. VersaVIS—An Open Versatile Multi-Camera Visual-Inertial Sensor Suite. Sensors 2020, 20, 1439. [Google Scholar] [CrossRef]
- Sessa, S.; Zecca, M.; Lin, Z.; Bartolomeo, L.; Ishii, H.; Takanishi, A. A methodology for the performance evaluation of inertial measurement units. J. Intell. Robot. Syst. 2013, 71, 143–157. [Google Scholar] [CrossRef]




| Features | Clinical Tools | ||||||
|---|---|---|---|---|---|---|---|
| FSST | Step Test | TUG | FRT | BBS | 4-Stage Balance | 30 Sec Stand | |
| Time required <a couple of minutes | + | + | + | + | − | + | + |
| Ease of performing | − | − | + | + | − | − | − |
| Measures static stability | − | − | + | + | + | + | − |
| Measures dynamic stability | + | + | + | − | + | − | + |
| Gait motion | − | − | + | − | − | − | − |
| Turning motion | − | − | + | − | + | − | − |
| Sitting and Standing motions | − | − | + | − | + | − | + |
| Reaching forward | − | − | − | + | + | − | − |
| Stepping | + | + | + | − | − | − | − |
| Total | 3 | 3 | 8 | 4 | 5 | 2 | 3 |
| Summary Statistics | Age (Years) | Gender (Female vs. Male) | BMI (kg/m2) | # of Diagnoses | # of Movement Disorders | # of Medications | # of Psychoactive Medications | TUG (14 s or > vs. <14 s) | 4-Stage Balance (30 s or < vs. >30 s) | 30 Sec Stand (8 or < vs. >8 Stands) | SIB Score (4 or > vs. 0–3) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (range) | 75.41 (65–96) | 49% | 28.8 (18.30–47.74) | 8.43 (1–19) | 0.47 (0–4) | 7.70 (0–21) | 0.91 (0–5) | 14.1 (7–98) | 31.4 (4–40) | 10.55 (0–23) | 3.24 (0–12) |
| Odds ratio of being a faller (95% CI) | 1.09 (1.03–1.16) | 2.10 (0.94–4.67) | 1.08 (1.00–1.16) | 1.44 (1.23–1.69) | 2.56 (1.21–5.39) | 1.34 (1.17–1.55) | 1.66 (1.13–2.44) | 10.25 (3.51–29.96) | 28.66 (7.81–105.71) | 14.33 (3.96–51.87) | 44.00 (9.57–202.35) |
| p-value | 0.004 | 0.070 | 0.042 | <0.001 | 0.014 | <0.001 | 0.009 | <0.001 | <0.001 | <0.001 | <0.001 |
| Fall-Risk Assessment Tools (Fallers vs. Non-Fallers) | Acc (%) | Se (%) | Sp (%) | AUC | J Index | Optimal Cut-Off |
|---|---|---|---|---|---|---|
| TUG (14 s or > vs. <14 s) | 71.00 | 55.55 | 89.13 | 0.72 | 0.45 | 14 |
| 4-stage balance (30 s or < vs. >30 s) | 81.00 | 70.37 | 93.48 | 0.82 | 0.64 | 32 |
| 30 sec stand (8 or < vs. >8 stands) | 70.00 | 50.00 | 93.47 | 0.71 | 0.43 | 10 |
| Sensor | Classification Method | Acc (%) | Se (%) | Sp (%) | J Index | F1-Score | AUC | C-Statistic (95% CI) | C-Statistic p-Value |
|---|---|---|---|---|---|---|---|---|---|
| - | Clinical TUG test | 70.65 (53.80, 85.78) | 56.02 (27.48, 81.64) | 88.53 (67.70, 100) | 0.44 (0.10, 0.73) | 0.67 (0.41, 0.85) | 0.72 (0.55, 0.87) | 25.70 (0.71, 0.74) | <0.001 |
| Neck | SVM_gyro | 67.13 (50.00, 80.00) | 92.51 (72.72, 100) | 36.11 (11.11, 66.67) | 0.29 (0.04, 0.57) | 0.81 (0.69, 0.92) | 0.70 (0.51, 0.90) | 18.57 (0.68, 0.73) | <0.001 |
| SVM_accel | 62.39 (46.87, 75.00) | 83.14 (54.54, 100) | 36.57 (4.17, 66.67) | 0.21 (0.02, 0.46) | 0.77 (0.62, 0.88) | 0.71 (0.51, 0.87) | 23.05 (0.69, 0.73) | <0.001 | |
| CNN_gyro | 66.21 (50.00, 80.00) | 86.51 (56.82, 100) | 41.27 (11.11, 66.67) | 0.28 (0.05, 0.57) | 0.80 (0.67, 0.92) | 0.75 (0.54, 0.92) | 25.20 (0.73, 0.77) | <0.001 | |
| CNN_accel | 63.08 (50.00, 75.00) | 75.47 (45.45, 100) | 47.93 (22.22, 66.67) | 0.25 (0.01, 0.48) | 0.75 (0.55, 0.88) | 0.73 (0.49, 0.89) | 20.32 (0.71, 0.75) | <0.001 | |
| Right | SVM_gyro | 56.06 (50.00, 67.87) | 98.00 (81.82, 100) | 4.89 (0.00, 33.33) | 0.05 (0.00, 0.33) | 0.76 (0.71, 0.84) | 0.52 (0.41, 0.71) | 3.33 (0.51, 0.53) | <0.001 |
| SVM_accel | 55.35 (55.00, 60.00) | 99.64 (95.22, 100) | 1.22 (0.00, 11.11) | 0.01 (0.00, 0.11) | 0.76 (0.73, 0.79) | 0.50 (0.43, 0.55) | 1.55 (0.49, 0.51) | 0.061 | |
| CNN_gyro | 59.77 (45.00, 79.50) | 83.18 (46.82, 100) | 31.04 (0.00, 66.67) | 0.17 (0.00, 0.56) | 0.75 (0.59, 0.91) | 0.66 (0.47, 0.84) | 14.82 (0.64, 0.68) | <0.001 | |
| CNN_accel | 58.33 (45.00, 75.00) | 79.57 (36.36, 100) | 32.37 (0.00, 66.67) | 0.16 (0.00, 0.44) | 0.72 (0.50, 0.86) | 0.61 (0.38, 0.81) | 9.92 (0.58, 0.63) | <0.001 | |
| Left | SVM_gyro | 56.65 (55.00, 65.00) | 99.36 (90.91, 100) | 4.55 (0.00, 22.22) | 0.04 (0.00, 0.22) | 0.77 (0.73, 0.82) | 0.53 (0.43, 0.66) | 4.77 (0.52, 0.54) | <0.001 |
| SVM_accel | 55.00 (55.00, 55.00) | 100 (100, 100) | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.76 (0.76, 0.76) | 0.50 (0.50, 0.50) | −1.00 (0.49, 0.50) | 0.841 | |
| CNN_gyro | 60.91 (45.00, 73.50) | 81.13 (39.09, 100) | 36.20 (0.00, 66.67) | 0.19 (0.00, 0.45) | 0.75 (0.51, 0.86) | 0.68 (0.48, 0.88) | 15.71 (0.65, 0.70) | <0.001 | |
| CNN_accel | 59.41 (40.00, 78.50) | 82.89 (36.36, 100) | 30.70 (0.00, 66.67) | 0.18 (0.00, 0.53) | 0.71 (0.00, 0.90) | 0.63 (0.37, 0.84) | 10.45 (0.61, 0.65) | <0.001 |
| Sensor | Classification Method | Acc (%) | Se (%) | Sp (%) | J Index | F1-Score | AUC | C-Statistic (95% CI) | C-Statistic p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Neck | SVM_gyro | 70.00 (58.19, 72.22) | 2.20 (0.00, 20.00) | 96.08 (76.92, 100.00) | −0.02 | 0.16 (0.00, 0.43) | 0.50 (0.36, 0.69) | 0.34 (0.49, 0.52) | 0.367 |
| SVM_accel | 69.00 (47.08, 72.22) | 1.20 (0.00, 20.00) | 95.08 (65.19, 100) | −0.04 | 0.04 (0.00, 0.26) | 0.53 (0.36, 0.68) | 2.92 (0.51, 0.54) | 0.002 | |
| CNN_gyro | 60.46 (44.44, 72.16) | 42.35 (0.00, 83.5) | 67.42 (37.11, 100) | 0.07 (−0.37, 0.42) | 0.41 (0.00, 0.69) | 0.56 (0.33, 0.74) | 4.27 (0.54, 0.58) | <0.001 | |
| CNN_accel | 54.71 (27.78, 72.22) | 28.61 (0.00, 100) | 64.74 (19.61, 84.61) | −0.06 1 | 0.26 (0.00, 0.63) | 0.46 (0.16, 0.81) | −2.13 (0.43, 0.49) | 0.983 | |
| Right | SVM_gyro | 71.78 (66.67, 72.22) | 1.40 (0.00, 20.00) | 98.77 (88.27, 100) | 0.00 (−0.08, 0.12) | 0.11 (0.00, 0.31) | 0.49 (0.37, 0.60) | −0.25 (0.49, 0.51) | 0.599 |
| SVM_accel | 70.50 (61.11, 72.22) | 0.60 (0.00, 10.50) | 97.38 (84.61, 100) | −0.02 1 | 0.12 (0.00, 0.29) | 0.49 (0.31, 0.66) | −0.12 (0.48, 0.51) | 0.548 | |
| CNN_gyro | 50.38 (26.11, 72.22) | 44.00 (0.00, 100) | 54.10 (0.00, 88.84) | −0.12 1 | 0.52 (0.00, 1) | 0.48 (0.26, 0.68) | −1.83 (0.45, 0.50) | 0.966 | |
| CNN_accel | 49.72 (27.78, 72.22) | 43.05 (0.00, 100) | 52.11 (0.00, 84.61) | −0.14 1 | 0.32 (0.00, 0.53) | 0.46 (0.18, 0.68) | −2.48 (0.43, 0.49) | 0.993 | |
| Left | SVM_gyro | 71.61 (66.67, 72.22) | 0.00 (0.00, 0.00) | 99.15 (92.31, 100) | −0.01 1 | 0.00 (0.00, 0.00) | 0.49 (0.34, 0.66) | −0.82 (0.48, 0.51) | 0.794 |
| SVM_accel | 71.06 (61.11, 72.22) | 1.00 (0.00, 20.00) | 98.00 (84.62, 100.00) | −0.01 1 | 0.21 (0.00, 0.33) | 0.51 (0.37, 0.62) | 1.37 (0.49, 0.51) | 0.085 | |
| CNN_gyro | 47.15 (27.78, 77.78) | 64.32 (0.00, 100) | 40.54 (0.00, 84.61) | 0.05 (−0.27, 0.45) | 0.54 (0.32, 0.81) | 0.41 (0, 0.70) | 3.06 (0.51, 0.57) | <0.001 | |
| CNN_accel | 49.91 (27.78, 72.22) | 38.02 (0.00, 100) | 54.48 (3.84, 84.61) | −0.08 1 | 0.28 (0.00, 0.62) | 0.44 (0.19, 0.70) | −3.95 (0.41, 0.46) | >0.999 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roshdibenam, V.; Jogerst, G.J.; Butler, N.R.; Baek, S. Machine Learning Prediction of Fall Risk in Older Adults Using Timed Up and Go Test Kinematics. Sensors 2021, 21, 3481. https://doi.org/10.3390/s21103481
Roshdibenam V, Jogerst GJ, Butler NR, Baek S. Machine Learning Prediction of Fall Risk in Older Adults Using Timed Up and Go Test Kinematics. Sensors. 2021; 21(10):3481. https://doi.org/10.3390/s21103481
Chicago/Turabian StyleRoshdibenam, Venous, Gerald J. Jogerst, Nicholas R. Butler, and Stephen Baek. 2021. "Machine Learning Prediction of Fall Risk in Older Adults Using Timed Up and Go Test Kinematics" Sensors 21, no. 10: 3481. https://doi.org/10.3390/s21103481
APA StyleRoshdibenam, V., Jogerst, G. J., Butler, N. R., & Baek, S. (2021). Machine Learning Prediction of Fall Risk in Older Adults Using Timed Up and Go Test Kinematics. Sensors, 21(10), 3481. https://doi.org/10.3390/s21103481