A Novel Smart Assistance System for Blood Vessel Approaching: A Technical Report Based on Oximetry


Abstract
1. Introduction
2. Materials and Methods
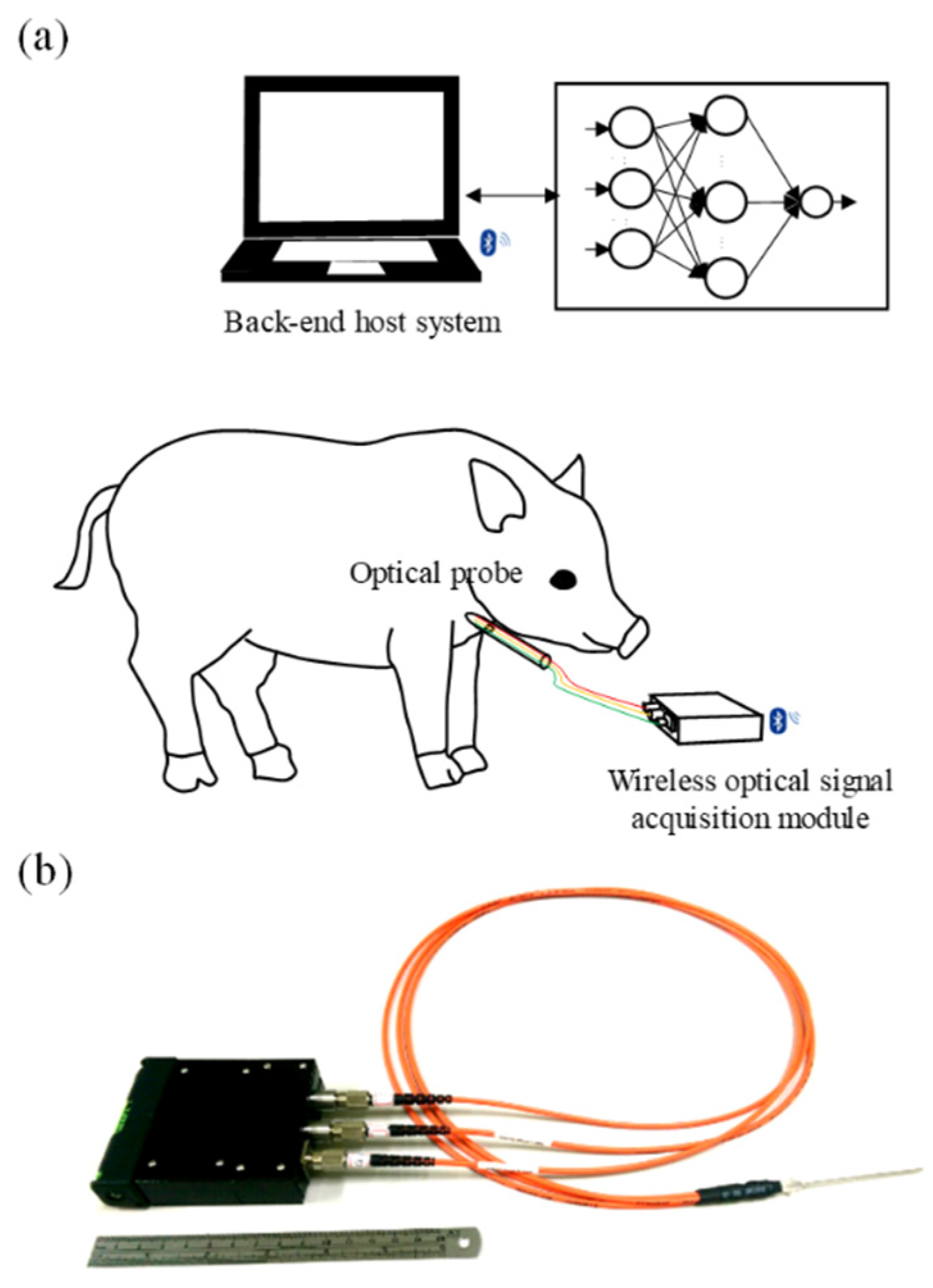
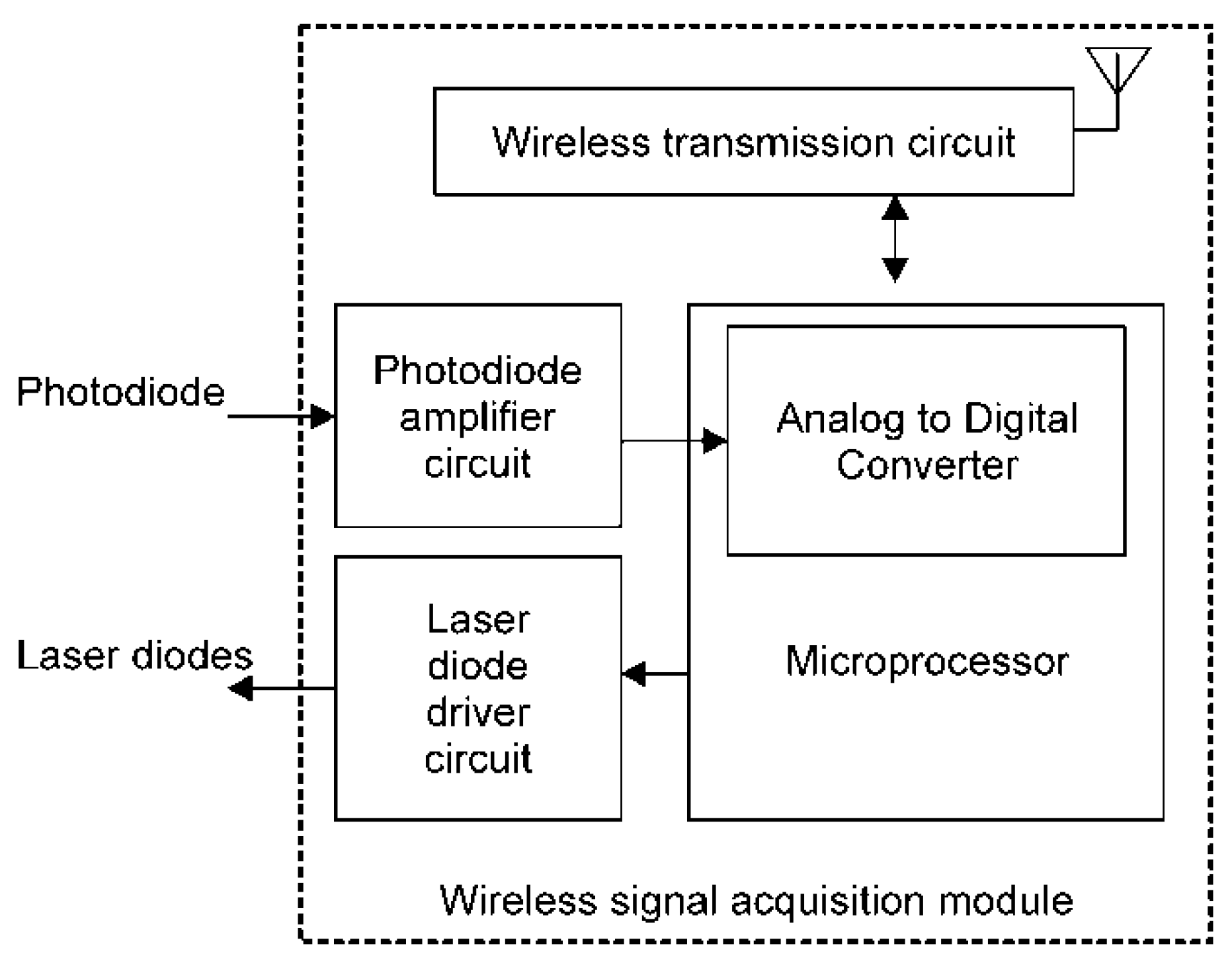
2.1. Design of the Smart Assistance System for Blood Vessel Catheter Placement
2.2. Fundamental Principle of the Modified Beer–Lambert Law
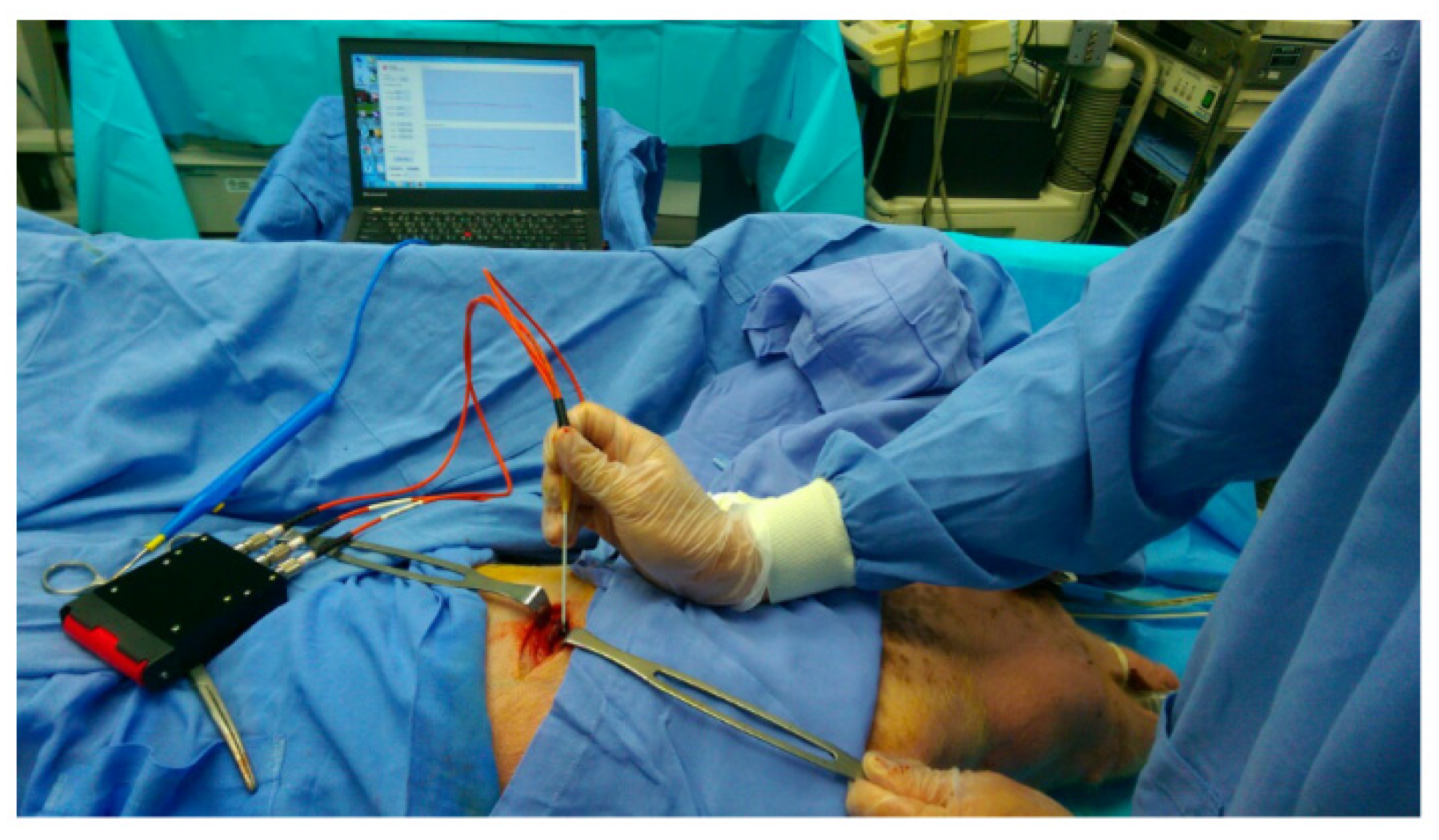
2.3. Experimental Design
3. Results
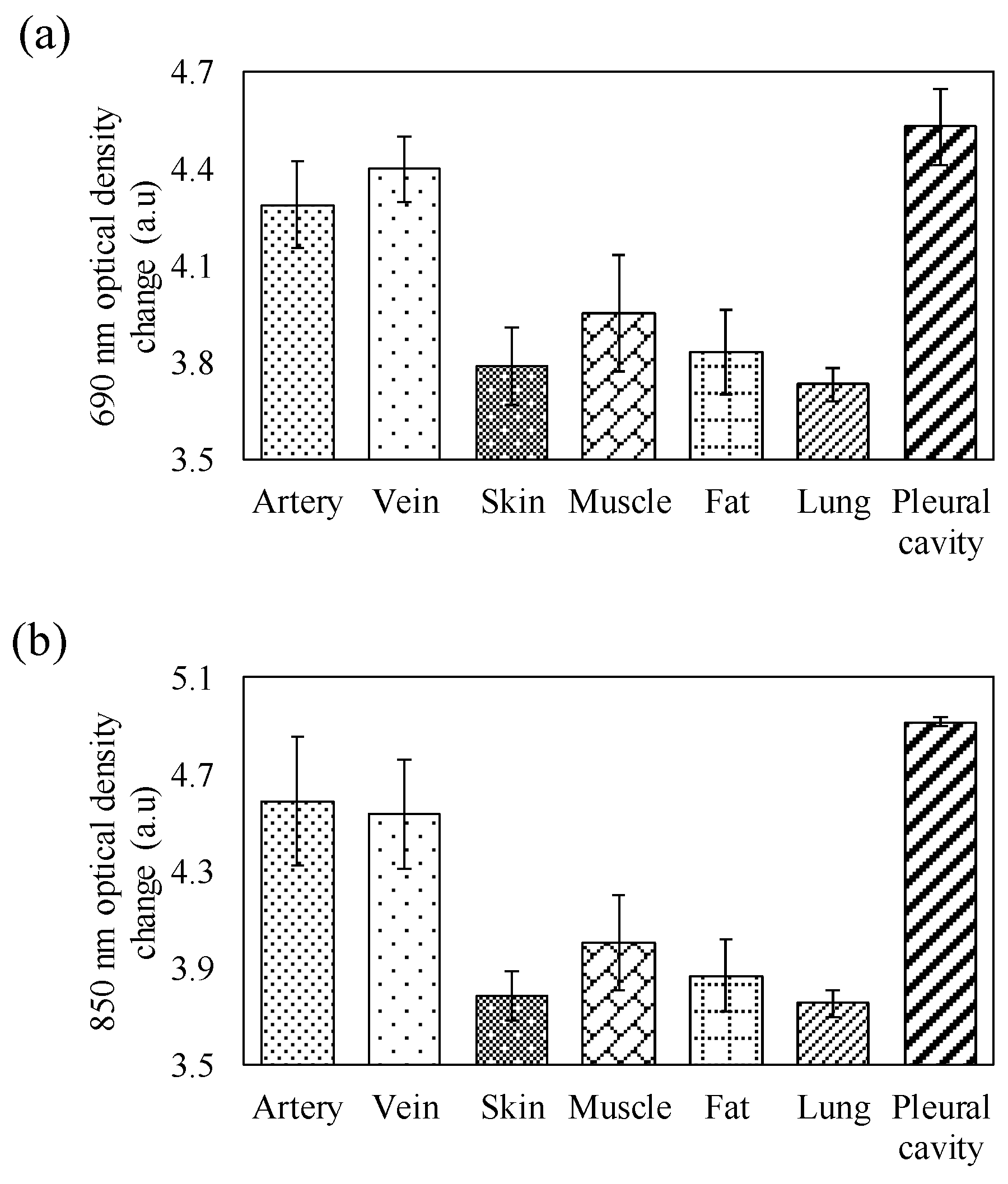
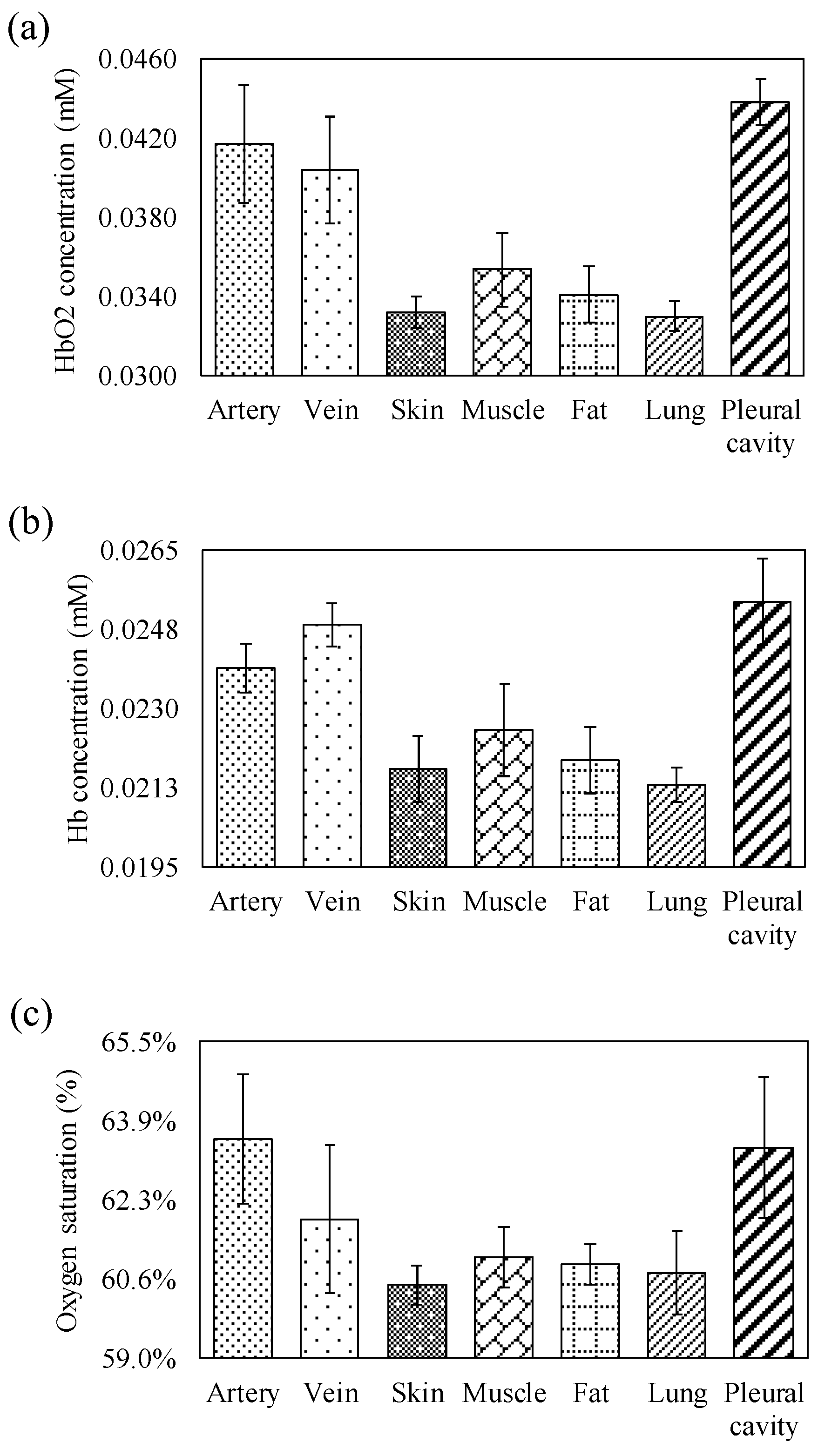
3.1. Hemoglobin Parameter of Different Tissue Components
3.2. Performance of RBFNN in Recognizing Human Tissue Components
3.3. Comparison to the Commercial Products
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Denys, B.G.; Uretsky, B.F.; Reddy, P.S. Ultrasound-assisted cannulation of the internal jugular vein. A prospective comparison to the external landmark-guided technique. Circulation 1993, 87, 1557–1562. [Google Scholar] [CrossRef]
- Ortega, R.; Song, M.; Hansen, C.J.; Barash, P. Ultrasound-Guided Internal Jugular Vein Cannulation. N. Engl. J. Med. 2010, 362, e57. [Google Scholar] [CrossRef] [PubMed]
- Randolph, A.G.; Cook, D.J.; Gonzales, C.A.; Pribble, C.G. Ultrasound guidance for placement of central venous catheters: A meta-analysis of the literature. Crit. Care Med. 1996, 24, 2053–2058. [Google Scholar] [CrossRef] [PubMed]
- Maslove, D.; Mihm, F.; Movahed, M.R. Ultrasound-guided internal jugular vein cannulation. N. Engl. J. Med. 2010, 363, 796–797. [Google Scholar] [PubMed]
- Rufes, T.D.; Mayoral, V.; Casals, M.; Serrano, A.; Miguel, M.; Sabaté, A. [Ultrasound-guided puncture: Applications in a chronic pain clinic]. Revista Española de Anestesiología y Reanimación 2010, 57, 493–507. [Google Scholar]
- Xia, W.; Mari, J.M.; West, S.J.; Ginsberg, Y.; David, A.L.; Ourselin, S.; Desjardins, A.E. In-plane ultrasonic needle tracking using a fiber-optic hydrophone. Med. Phys. 2015, 42, 5983–5991. [Google Scholar] [CrossRef]
- Xia, W.; Ginsberg, Y.; West, S.J.; Nikitichev, D.; Ourselin, S.; David, A.L.; Desjardins, A.E. Coded excitation ultrasonic needle tracking: An in vivo study. Med. Phys. 2016, 43, 4065. [Google Scholar] [CrossRef]
- Hebard, S.; Hocking, G. Echogenic technology can improve needle visibility during ultrasound-guided regional anesthesia. Reg. Anesth. Pain Med. 2011, 36, 185–189. [Google Scholar] [CrossRef]
- Klein, S.M.; Fronheiser, M.P.; Reach, J.; Nielsen, K.C.; Smith, S.W. Piezoelectric Vibrating Needle and Catheter for Enhancing Ultrasound-Guided Peripheral Nerve Blocks. Anesth. Analg. 2007, 105, 1858–1860. [Google Scholar] [CrossRef]
- Rothbart, A.; Yu, P.; Müller-Lobeck, L.; Spies, C.; Wernecke, K.-D.; Nachtigall, I. Peripheral intravenous cannulation with support of infrared laser vein viewing system in a pre-operation setting in pediatric patients. BMC Res. Notes 2015, 8, 463. [Google Scholar] [CrossRef]
- Cuper, N.J.; De Graaff, J.C.; Hartman, B.J.; Verdaasdonk, R.M.; Kalkman, C.J. Difficult arterial cannulation in children: Is a near-infrared vascular imaging system the answer? Br. J. Anaesth. 2012, 109, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Perry, A.M.; Caviness, A.C.; Hsu, D.C. Efficacy of a Near-Infrared Light Device in Pediatric Intravenous Cannulation. Pediatr. Emerg. Care 2011, 27, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Aulagnier, J.; Hoc, C.; Mathieu, E.; Dreyfus, J.F.; Fischler, M.; Le Guen, M. Efficacy of AccuVein to Facilitate Peripheral Intravenous Placement in Adults Presenting to an Emergency Department: A Randomized Clinical Trial. Acad. Emerg. Med. 2014, 21, 858–863. [Google Scholar] [CrossRef] [PubMed]
- Seiyama, A.; Higaki, K.; Takeuchi, N.; Uehara, M.; Takayama, N. Oxygen Transport to Tissue XXXVII. In Estimation of Skin Blood Flow Artefacts in NIRS Signals during a Verbal Fluency Task; Springer: New York, NY, USA, 2016; pp. 327–340. [Google Scholar]
- Preuss, L.E.; Profio, A.E. Optical properties of mammalian tissue: Introduction by the feature editors. Appl. Opt. 1989, 28, 2207. [Google Scholar] [CrossRef]
- Akay, M. Nonlinear Biomedical Signal Processing, Fuzzy Logic, Neural Networks, and New Algorithms; Institute of Electrical and Electronics Engineers (IEEE): Hanover, MN, USA, 2000. [Google Scholar]
- Lin, B.-S.; Chong, F.-C.; Lai, F. Higher-Order-Statistics-Based Radial Basis Function Networks for Signal Enhancement. IEEE Trans. Neural Netw. 2007, 18, 823–832. [Google Scholar] [CrossRef]
- Lin, B.-S.; Lin, B.-S.; Chong, F.-C.; Lai, F. Higher Order Statistics-Based Radial Basis Function Network for Evoked Potentials. IEEE Trans. Biomed. Eng. 2008, 56, 93–100. [Google Scholar]
- Lin, B.-S.; Sheu, M.-J.; Chuang, C.-C.; Tseng, K.-C.; Chen, J.-Y. Enhancing bowel sounds by using a higher order statistics-based radial basis function network. IEEE J. Biomed. Health Inform. 2013, 17, 675–680. [Google Scholar] [CrossRef]
- Huang, Y.-K.; Chang, C.-C.; Lin, P.-X.; Lin, B.-S. Quantitative Evaluation of Rehabilitation Effect on Peripheral Circulation of Diabetic Foot. IEEE J. Biomed. Health Inform. 2018, 22, 1019–1025. [Google Scholar] [CrossRef]
- Lin, B.-S.; Wu, P.-J.; Chen, C.-Y. 2D/3D-Display Auto-Adjustment Switch System. IEEE J. Biomed. Health Inform. 2018, 22, 799–805. [Google Scholar] [CrossRef]
- Haykin, S. Adaptive Filter Theory, 2nd ed.; Prentice-Hall: Englewood Cliffs, NJ, USA, 1991. [Google Scholar]
- Chen, S.; Mulgrew, B.; Grant, P.M. A clustering technique for digital communications channel equalization using radial basis function networks. IEEE Trans. Neural Netw. 1993, 4, 570–590. [Google Scholar] [CrossRef]
- Boas, D.A.; Gaudette, T.; Strangman, G.; Cheng, X.; Marota, J.J.; Mandeville, J.B. The Accuracy of Near Infrared Spectroscopy and Imaging during Focal Changes in Cerebral Hemodynamics. NeuroImage 2001, 13, 76–90. [Google Scholar] [CrossRef] [PubMed]
- Cope, M.; Delpy, D.T. System for long-term measurement of cerebral blood and tissue oxygenation on newborn infants by near infra-red transillumination. Med. Boil. Eng. 1988, 26, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Kaspers, O.P.; Sterenborg, H.J.C.M.; Amelink, A. Controlling the optical path length in turbid media using differential path-length spectroscopy: Fiber diameter dependence. Appl. Opt. 2008, 47, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Varma, R.; Sahane, S.D.; Thakre, S.S. Infrared VeinViewer. Int. J. Eng. Educ. 2014, 2, 1–6. [Google Scholar]
- Wynd, K.P.; Smith, H.M.; Jacob, A.K.; Torsher, L.C.; Kopp, S.; Hebl, J.R. Ultrasound Machine Comparison. Reg. Anesth. Pain Med. 2009, 34, 349–356. [Google Scholar] [CrossRef]
- Kashani, A.H.; Lee, S.Y.; Moshfeghi, A.; Durbin, M.K.; Puliafito, C.A. Optical coherence tomography angiography of retinal venous occlusion. Retina 2015, 35, 2323–2331. [Google Scholar] [CrossRef]
- Garcia, J.V.; Zhang, F.; Ford, P.C. Multi-photon excitation in uncaging the small molecule bioregulator nitric oxide. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2013, 371, 20120129. [Google Scholar] [CrossRef]
- Lin, L.; Shiga, T.; Niwayama, M.; Kudo, N.; Takahashi, M.; Yamamoto, K. Influence of a fat on muscle oxygenation measurement using near-IR spectroscopy: Quantitative analysis based on two-layered phantom experiments and Monte Carlo simulation. Front. Med. Boil. Eng. 2000, 10, 43–58. [Google Scholar]
- Pump, K.K. Distribution of Bronchial Arteries in the Human Lung. Chest 1972, 62, 447–451. [Google Scholar] [CrossRef]
- Mittal, M.K.; Mittal, A.; Sinha, M.; Sureka, B.; Thukral, B.B. Radiological review of pleural tumors. Indian J. Radiol. Imaging 2013, 23, 313–320. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vein Viewer [27] | HD11 XE [28] | SD-OCT 5000 [29] | Proposed System | |
|---|---|---|---|---|
| Sensing technique | Near-infrared spectroscopy | Ultrasound | Optical coherence tomography | Near-infrared spectroscopy |
| Sensor type | CCD camera | Ultrasound Probe | OCT probe | Optical probe |
| Channels | 1 | 1 | 1 | 1 |
| Transmission mode | - | USB | USB | Bluetooth |
| System size (cm3) | 4.8 × 6 × 19.8 | 53 × 110 × 151 | 65 × 46 × 53 | 11 × 7.5 × 2.5 |
| Wavelength (nm) | 740 | - | 840 | 690, 850 |
| Physiological parameters | 2-D image | 2-D image | 3-D image | , hemoglobin concentration |
| System complexity | Low | High | High | Low |
| Advantages | Distinguishability of vessel types | Imaging capability of soft tissue structure | Imaging capability of tissue structure; higher image resolution | Distinguishability of vessel types in deeper tissue |
| Limitations | Depth limitation | Bone; air; needle tip recognition | Depth limitation | Low image resolution |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, C.-C.; Chuang, C.-C.; Lai, B.-C.; Huang, Y.-C.; Chen, J.-Y.; Lin, B.-S. A Novel Smart Assistance System for Blood Vessel Approaching: A Technical Report Based on Oximetry. Sensors 2020, 20, 1891. https://doi.org/10.3390/s20071891
Lee C-C, Chuang C-C, Lai B-C, Huang Y-C, Chen J-Y, Lin B-S. A Novel Smart Assistance System for Blood Vessel Approaching: A Technical Report Based on Oximetry. Sensors. 2020; 20(7):1891. https://doi.org/10.3390/s20071891
Chicago/Turabian StyleLee, Chien-Ching, Chia-Chun Chuang, Bo-Cheng Lai, Yi-Chia Huang, Jen-Yin Chen, and Bor-Shyh Lin. 2020. "A Novel Smart Assistance System for Blood Vessel Approaching: A Technical Report Based on Oximetry" Sensors 20, no. 7: 1891. https://doi.org/10.3390/s20071891
APA StyleLee, C.-C., Chuang, C.-C., Lai, B.-C., Huang, Y.-C., Chen, J.-Y., & Lin, B.-S. (2020). A Novel Smart Assistance System for Blood Vessel Approaching: A Technical Report Based on Oximetry. Sensors, 20(7), 1891. https://doi.org/10.3390/s20071891