1. Introduction
Computer-aided design and computer-aided manufacturing (CAD/CAM) technology has drastically changed the face of dentistry since it was introduced to the field in the 1980s [
1]. In the early stages of the application of CAD/CAM to dentistry, desktop scanners were used in dental laboratories to digitize gypsum models before the milling and manufacturing of dental prosthetics [
2]. Most recently, the advancement of chairside CAD/CAM systems has provided a more efficient digital workflow in the clinical setting [
3]. In the last two decades, many commercially available intraoral scanners (IOS) have been developed [
4], and both in vivo and in vitro studies have examined the accuracy and precision of various intraoral scanners compared to conventional impression materials and techniques [
5]. The use of intraoral scanners as an alternative to conventional impression reduces patient discomfort, is more environmentally friendly, and is easier for clinicians to manipulate without the risk of damage or distortion [
6]. Other advantages of intraoral scanning include real-time visualization and magnification, automatic color-scanning for esthetic shade selection, and better patient compliance. Along with improved reliability and reproducibility in the technology, these advantages have increased the acceptance and popularity of digital impression [
7].
The success of any dental restoration in the long term depends on its marginal adaptation to the existing tooth structure. Complications such as caries may arise around the margins as a result of bacterial penetration into leaking open margins and biofilm accumulation on marginal discrepancies. Therefore, obtaining an accurate impression from the tooth is critical in the fabrication process of a dental restoration [
8].
Given that intraoral scanning is the first and therefore foundational step in chairside digital workflow, the accuracy of intraoral scanners must be evaluated critically. To this end, we examined the 3Shape TRIOS 3 intraoral scanner (3Shape, Copenhagen, Denmark) because it is one of the major intraoral scanning systems currently on the market and has gained widespread use in restorative dentistry. In addition, several recent studies have shown that the TRIOS 3 is one of the most accurate intraoral scanners, in comparison to other intraoral scanning systems [
9,
10,
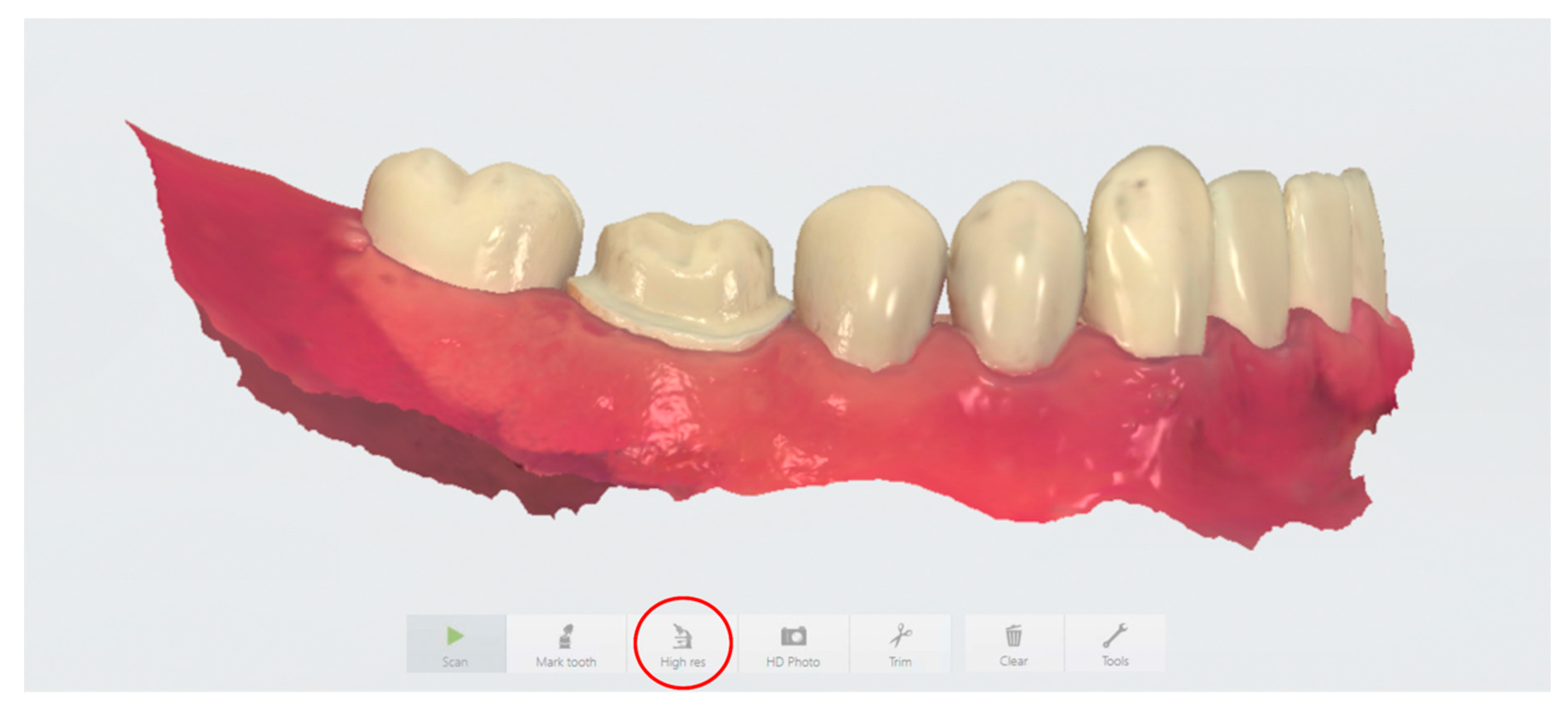
11]. However, different scan settings have been suggested by the manufacturer and a variety of scanning techniques have been applied depending on operator preferences. More specifically, the 3Shape TRIOS 3 user manual (ver. 2017) recommends the use of High Resolution (High res; also known as Zoom in some software versions) when scanning critical surfaces such as crown preparation margins in order to “capture areas that are difficult to scan with higher amounts of details” (
Figure 1). Data on the accuracy of digital impressions made under different scanning resolution settings are insufficient, however. Theoretically, the High res function would allow for superior finish line accuracy to minimize marginal discrepancy between the preparation and the restoration. Clinically, however, using the High res function requires additional chair-time and can be disruptive to the provider’s workflow.
The purpose of this study was to investigate the difference in accuracy between digital impressions obtained using various scan resolution settings on the 3Shape TRIOS 3 scanner. These data allowed evaluation of the necessity of the TRIOS 3 scanner High res function as an essential step in taking digital impressions for single unit fixed dental prostheses. Furthermore, we were most interested in the accuracy of the scans at the cavosurface finish line on the prepared tooth, where restoration margin integrity is critical to the success and longevity of the restoration. The null hypothesis was that no significant difference in discrepancy was expected among different intraoral scanning resolutions.
3. Results
On average, the scan times for the SHR group and the HR group were 34.2 s and 46.5 s longer compared to the SR group, respectively. The mean number of images captured per scan was 1124 for the SR group, 1584 for the SHR group, and 1692 for the HR group (
Table 1). Scanning in high resolution in both the SHR and HR groups took significantly longer (
p < 0.05) and required that more images be taken to complete the scan than for scanning in standard resolution alone (
Figure 4C,E). No correlation was observed between total discrepancy and scan time or number of images captured (
Figure 4B,D). Scan time and number of images captured showed a strong linear correlation (
Figure 4F).
In total, 60 scans from three experimental groups were evaluated. Their accuracy was defined by measuring the discrepancy between the master scan and the IOS scans for the three scan groups. Discrepancy at the preparation finish line was calculated as the average distance between the master scan and the IOS scan at each of 100 points. For total discrepancy along the finish line, the HR group showed the lowest discrepancy value of 31.5 ± 5.5 μm, followed by the SHR group (33.2 ± 3.7 μm) and the SR group (33.6 ± 3.1 μm) (
Table 2). These scanning discrepancies along the finish line were not significantly different among the three groups (
p > 0.05;
Figure 4A).
Additional statistical analysis by two-way repeated-measures ANOVA suggested that while scan resolution was not a significant factor (
p > 0.05), significant differences were observed in discrepancy among tooth surfaces (
p < 0.05) (
Figure 5). Digital scanning of the distal surface was significantly less accurate when compared to that for the other three tooth surfaces in all three groups, with the discrepancy ranging from 56.1 ± 16.8 μm (SR group) to 68.2 ± 11.3 μm (SHR group) (
Table 3).
4. Discussion
In this study, the accuracies of different scanning strategies using the 3Shape TRIOS 3 intraoral scanner were compared using an all-ceramic crown preparation of a mandibular first molar on a typodont. Differences in scanning accuracy at the preparation finish line between scan resolutions were examined to evaluate the necessity of including the additional step of scanning in High res mode to achieve optimal marginal integrity on the digital impression.
The null hypothesis that no significant difference would be observed among different intraoral scanning resolutions was not rejected by the results, suggesting that digitally trimming the preparation finish line and re-scanning in High res mode, which would increase the duration of a digital workflow, is not warranted. The additional time needed to digitally trim away the preparation margin and set up for High res mode in the software as well as the increased amount of computer data required (i.e., higher number of images taken) make this step in the scanning process undesirable. It is important to note that the scan time measured in this study was strictly based on the amount of time required to complete scanning as recorded by the software and did not take into account processing time in between scanning modes as well as the time needed to trim the margin, which would have further increased the total amount of time required for scanning when using the combination resolution technique.
Our results also revealed that the tooth surface plays a significant role in the accuracy of intraoral scans at the finish line. The lower accuracy observed for the distal surface suggests that interproximal regions where distances between adjacent teeth are small may be challenging for the current scanner, regardless of the scanning mode. A similar pattern was not observed for the mesial surface, however. The distance between the cavosurface margin of the prepared tooth and the adjacent tooth might impact the scanning accuracy. The absolute value of this distance on both mesial and distal surfaces should be measured in the future to evaluate the role that the distance between adjacent teeth surfaces plays in scanning accuracy. Another study reported that the crown preparation quality as measured by the tooth surface smoothness had a profound effect on the marginal fit of CAD/CAM-fabricated crowns, while the scanner type itself did not [
13]. Furthermore, a previous in vivo study found that digital impression systems in general displayed increased distortion towards the distal end when full-arch impressions were taken [
12]. This distortion pattern is consistent with the findings in this study.
Moreover, the occlusal plane slope and anatomy of the dental arch at the molar region could affect the distance of the scanner from the scanned margin, and therefore the focus of the obtained images. Additional studies should be conducted to examine the difference in scanning accuracy between surfaces of a single tooth at various positions in a dental arch.
The longevity and success of fixed dental prostheses depend heavily on marginal integrity between the preparation and the restoration. A systematic review conducted by Ahlholm et al. concluded that in their current state, digital impression techniques are clinically acceptable and comparable to conventional impression techniques in terms of accuracy for single crowns and short-span fixed partial dentures, but that their accuracy for complete dental arch treatment is lower [
14]. The clinically acceptable value for marginal discrepancy of CAD/CAM-generated restorations has been described as between 50 and 100 μm [
2,
15]. This means that the accuracy of digital impression as the first step in any digital workflow should fall below that range in terms of marginal discrepancy. The results of this study showed that the accuracy of the 3Shape TRIOS 3 scanner, regardless of scanning resolution, falls within clinically accepted limits and is comparable to previously published data that showed a discrepancy that ranged from 6.9 ± 0.9 µm to 119 ± 48 μm [
4,
9,
16,
17,
18,
19,
20]. The variation in observed discrepancy values could be due to differences in software and hardware versions, different materials scanned, operator discrepancies, differences in scanning strategies, or the span length of the scan.
Although numerous studies have compared the differences in scanning accuracy between various IOS, fewer studies have investigated the discrepancy in accuracy as a result of different scanning strategies. A common comparison between scanning protocols involves evaluating the difference in accuracy between strategies that differ in directional sequence. In an in vitro study, Müller et al. found that changing the directional sequence of scanning did not impact the accuracy of a full-arch digital impression using the 3Shape TRIOS Pod scanner [
21]. Furthermore, Medina-Sotomayor et al. explored how differences in scanning direction affected the accuracy of digital impressions using four different IOS and found no significant difference among scanning systems [
16]. It is important to note, however, that scanning strategies based on the sequence in which a tooth surface is scanned could be utilized by other intraoral scanning systems, thus allowing for a comparison between scanners to be made. Conversely, it is to the best of the authors’ knowledge that the high-resolution scanning tool investigated in this study is a unique feature of the 3Shape TRIOS scanning interface, and a scanning protocol combining different optical resolutions has not been recommended by other manufacturers.
In addition, 3Shape has recently released a new scanner model, the TRIOS 4 scanner, with a Zoom function that appears to be similar in functionality to the TRIOS 3 High res/Zoom setting. As intraoral scanners and associated software are developed, it is possible that the accuracy and precision of impressions can improve substantially. Further studies are needed to fairly evaluate the TRIOS 4 scanner and its optical resolution. The authors plan to utilize the methodology developed in the current study to further examine the TRIOS 4 scanner, as well as scanning parameters recommended by other major intraoral scanners comprehensively in the near future.
Previous studies have been performed to examine the difference in accuracy according to multiple scan strategies within a single scanning system. Motel et al. compared the difference in accuracy between two strategies for implant impression using the TRIOS 3 scanner in an in vitro study [
22]. The first strategy involved a one-step approach by scanning both the scan bodies and surrounding structures together, whereas the second strategy combined an initial scan without the scan bodies and a final scan with the scan bodies in place. These authors concluded that the one-step scanning strategy achieved significantly higher accuracy compared to the two-step approach. This finding is consistent with our recommendation of a one-step scanning approach for optimal scanning efficiency.
The 3Shape TRIOS 3 intraoral scanner was selected for this study due to its popularity and proven superior accuracy. Accordingly, a limitation of our study is that it was designed specifically for the TRIOS 3 scanner and other IOS were not included for comparison. Therefore, our conclusion of no significant difference in digital impression accuracy between default resolution and high resolution using TRIOS 3 should not be considered applicable for other IOS without further evaluation. While the scope of this study limits its direct application to users of TRIOS 3, the results of this study highlight the importance of evaluating different parameters within a single scanning system when making digital impressions for the fabrication of dental prostheses.
Given that this was an in vitro study, factors that could influence the scanning accuracy when digital impressions are taken in vivo, such as the presence of saliva and blood, soft tissue movement, and the limited space that the oral cavity allows for maneuvering of the camera, were not considered. The notion that the High res function could yield superior accuracy when such in vivo artifacts are present is plausible. Further study goals include the investigation of the impact of intraoral variables and margin design on scanning accuracy under different optical resolutions in clinical settings.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}