An Adaptive Median Filter Based on Sampling Rate for R-Peak Detection and Major-Arrhythmia Analysis


Abstract
1. Introduction
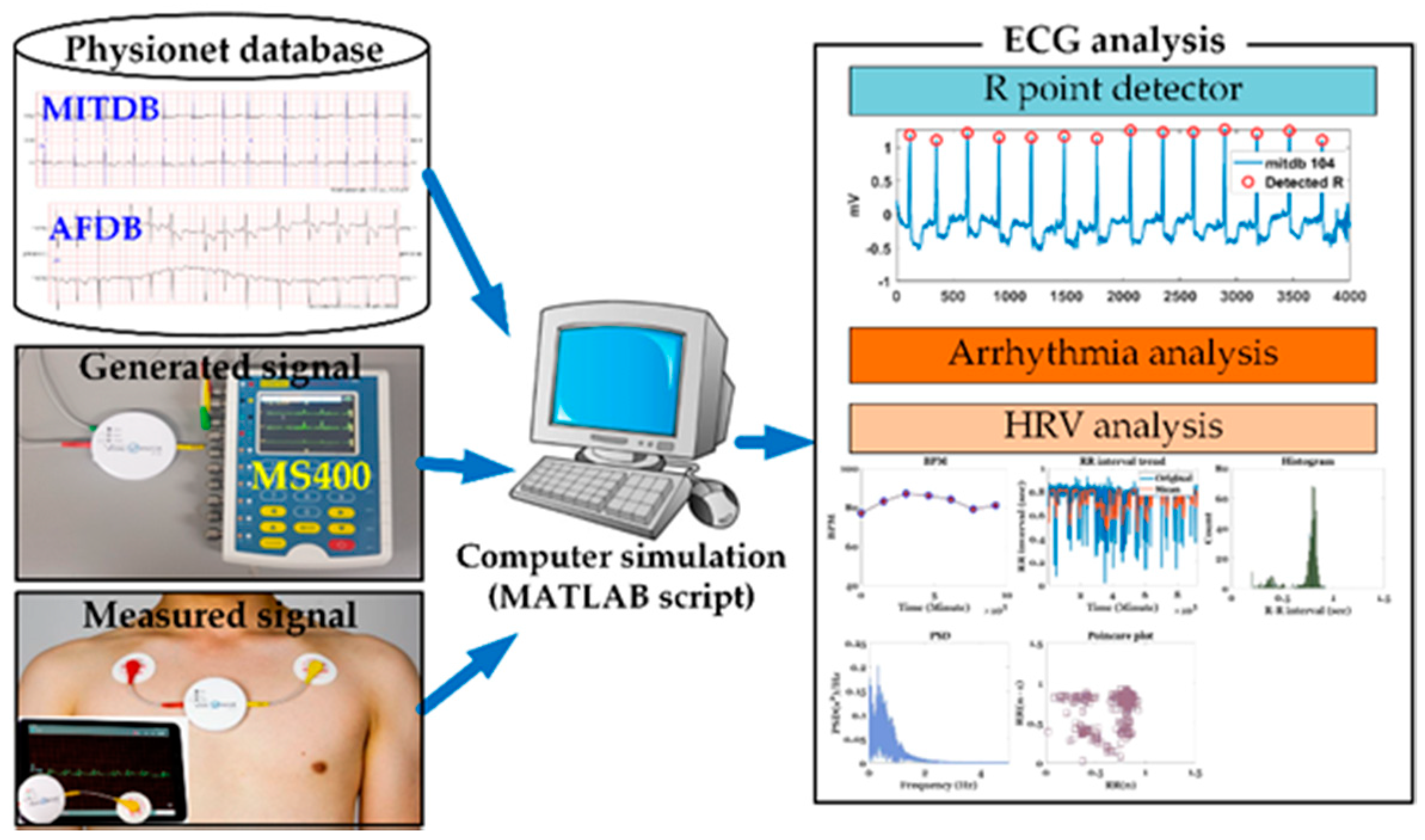
2. Materials and Methods
2.1. ECG Data Used
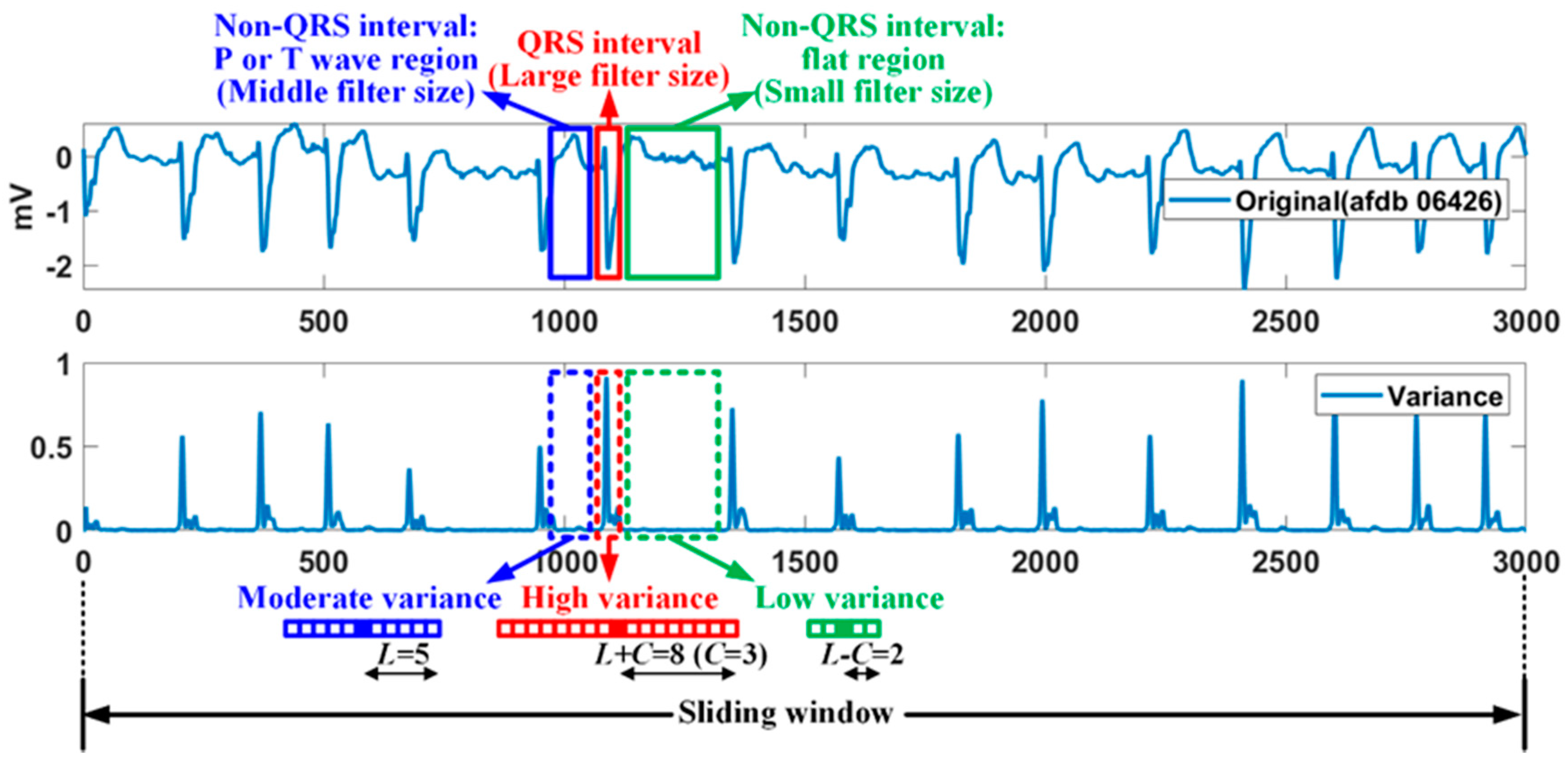
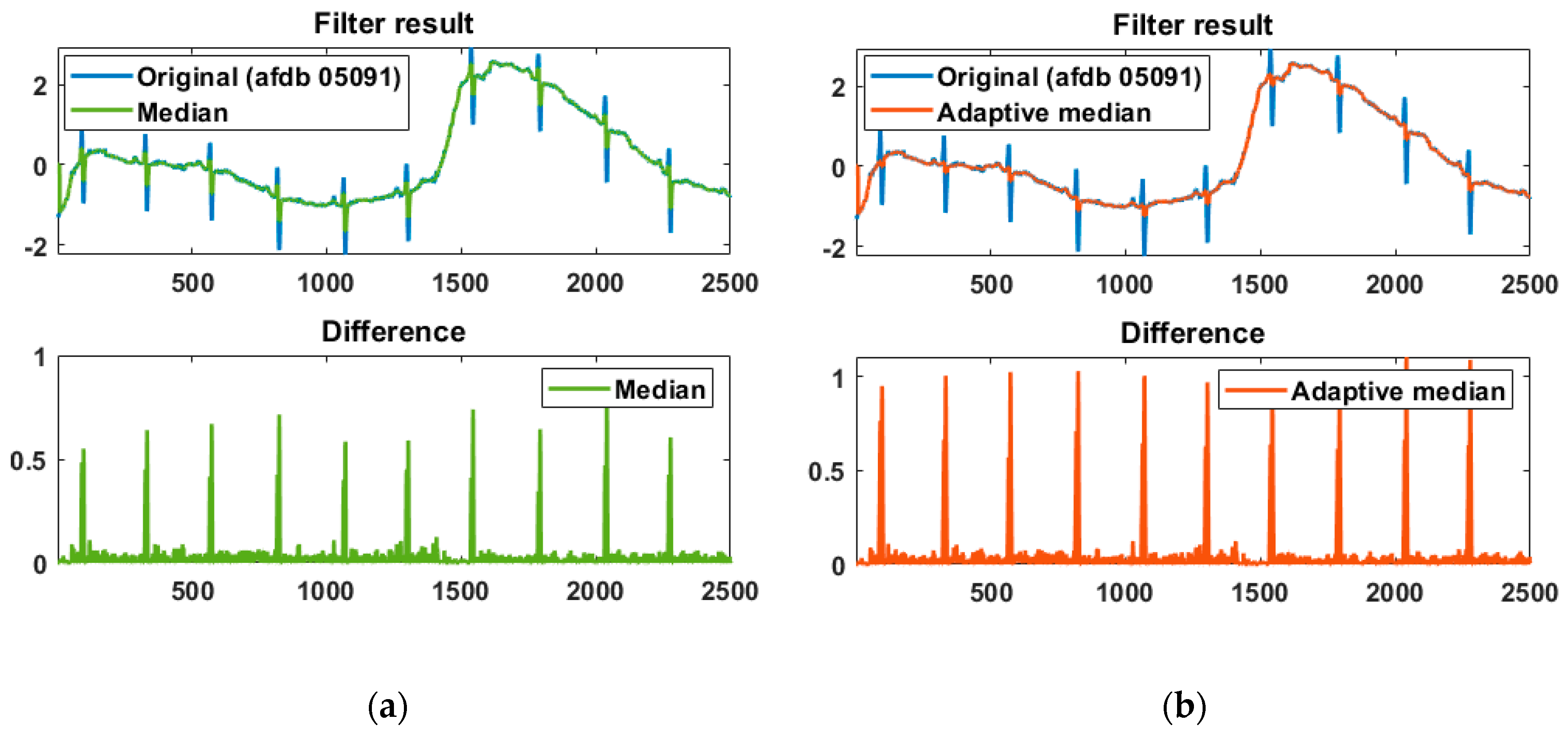
2.2. R-Peak Detection
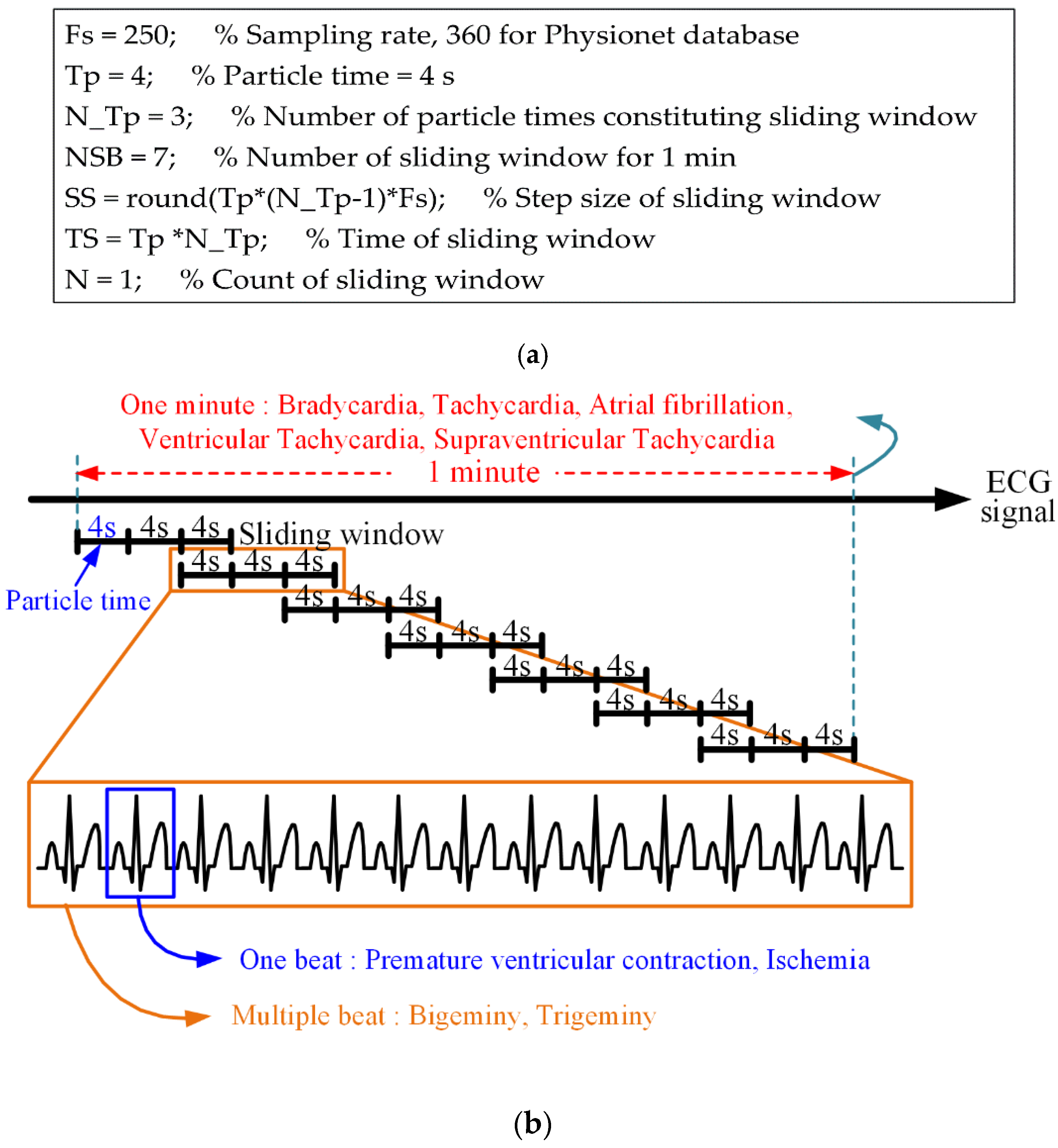
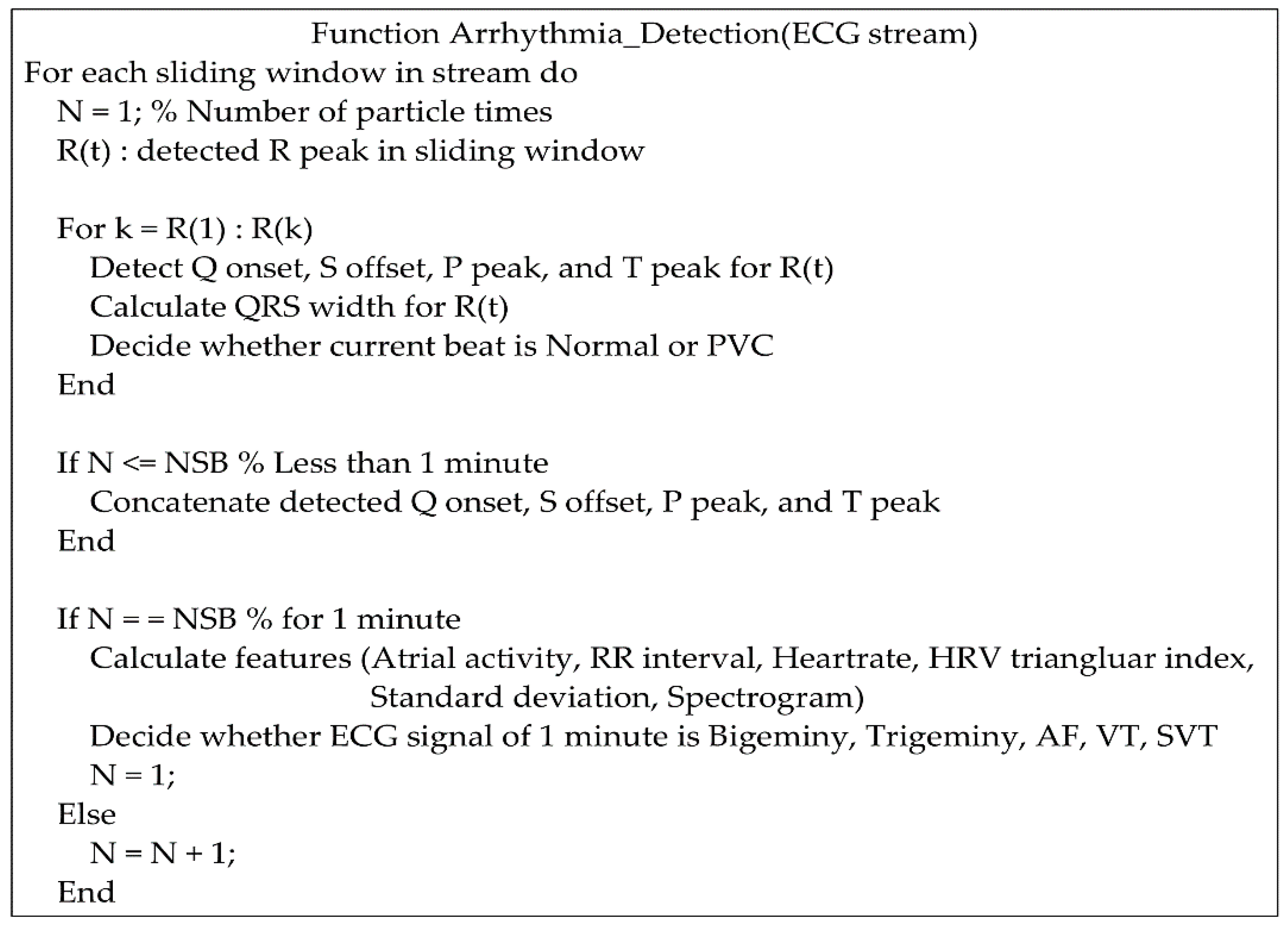
2.3. Detection of Important Arrhythmias
2.3.1. Bradycardia and Tachycardia
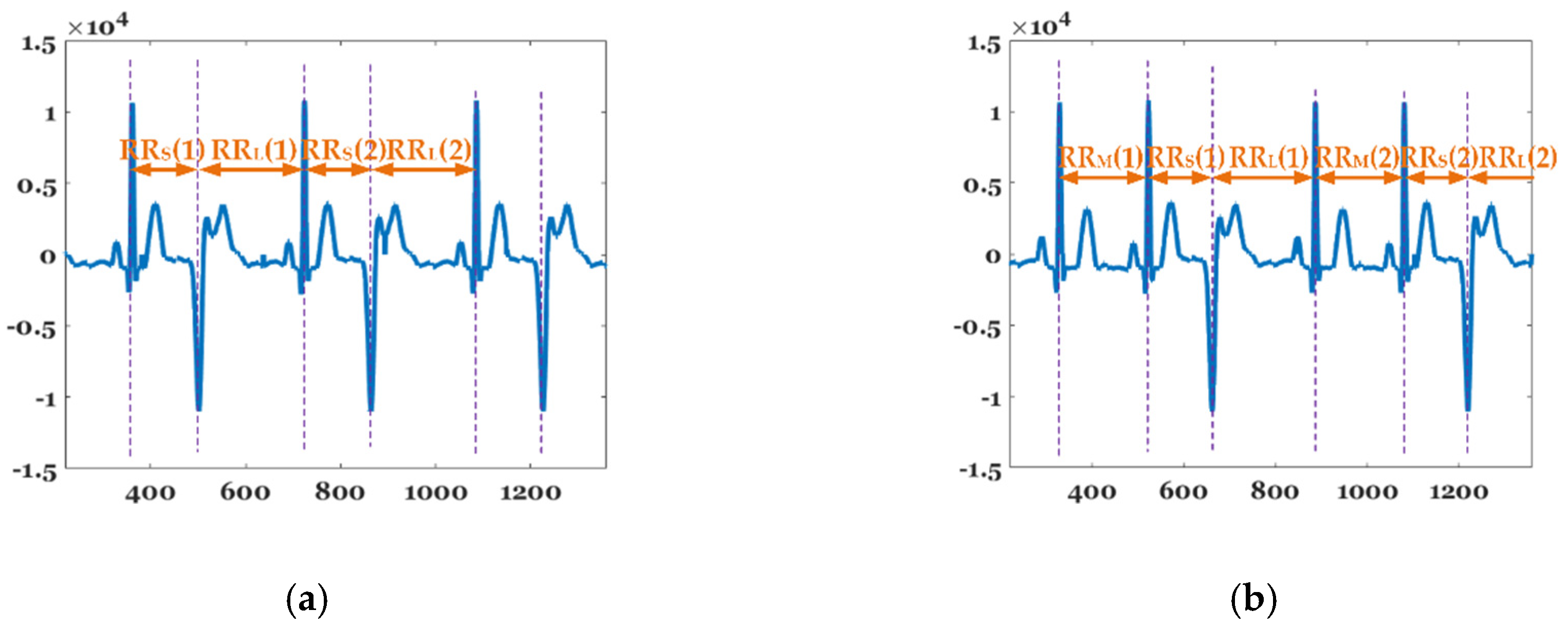
2.3.2. Bigeminy and Trigeminy
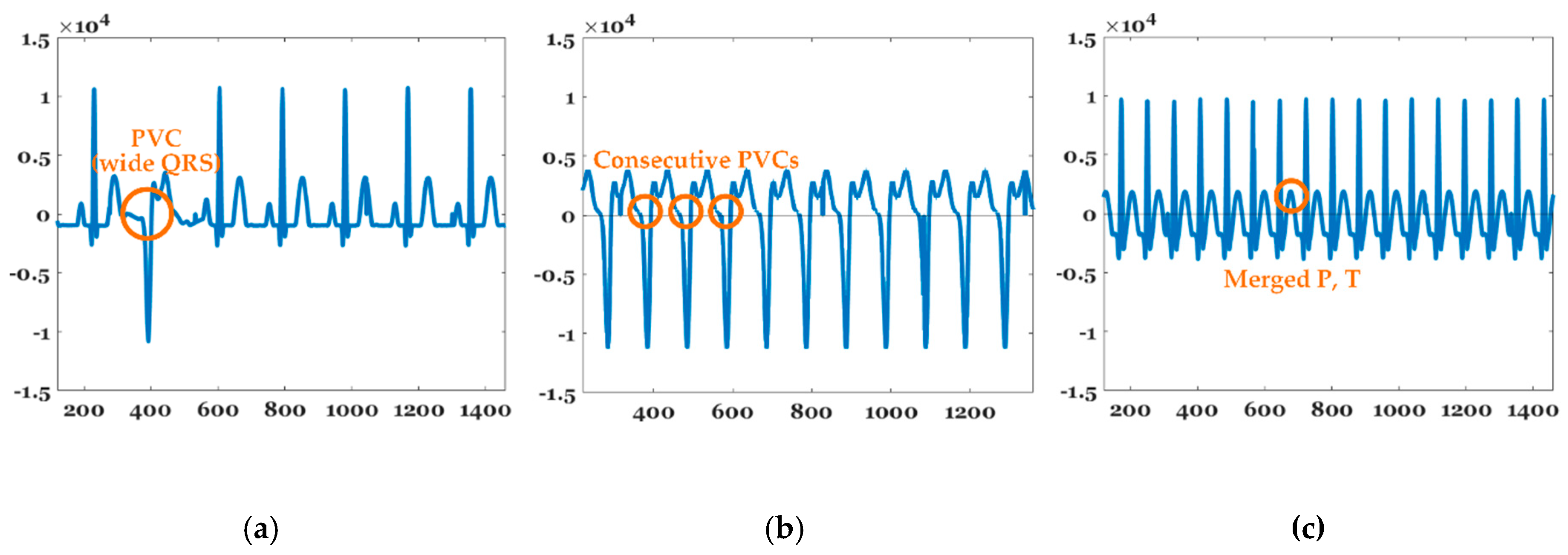
2.3.3. PVC, VT, and SVT
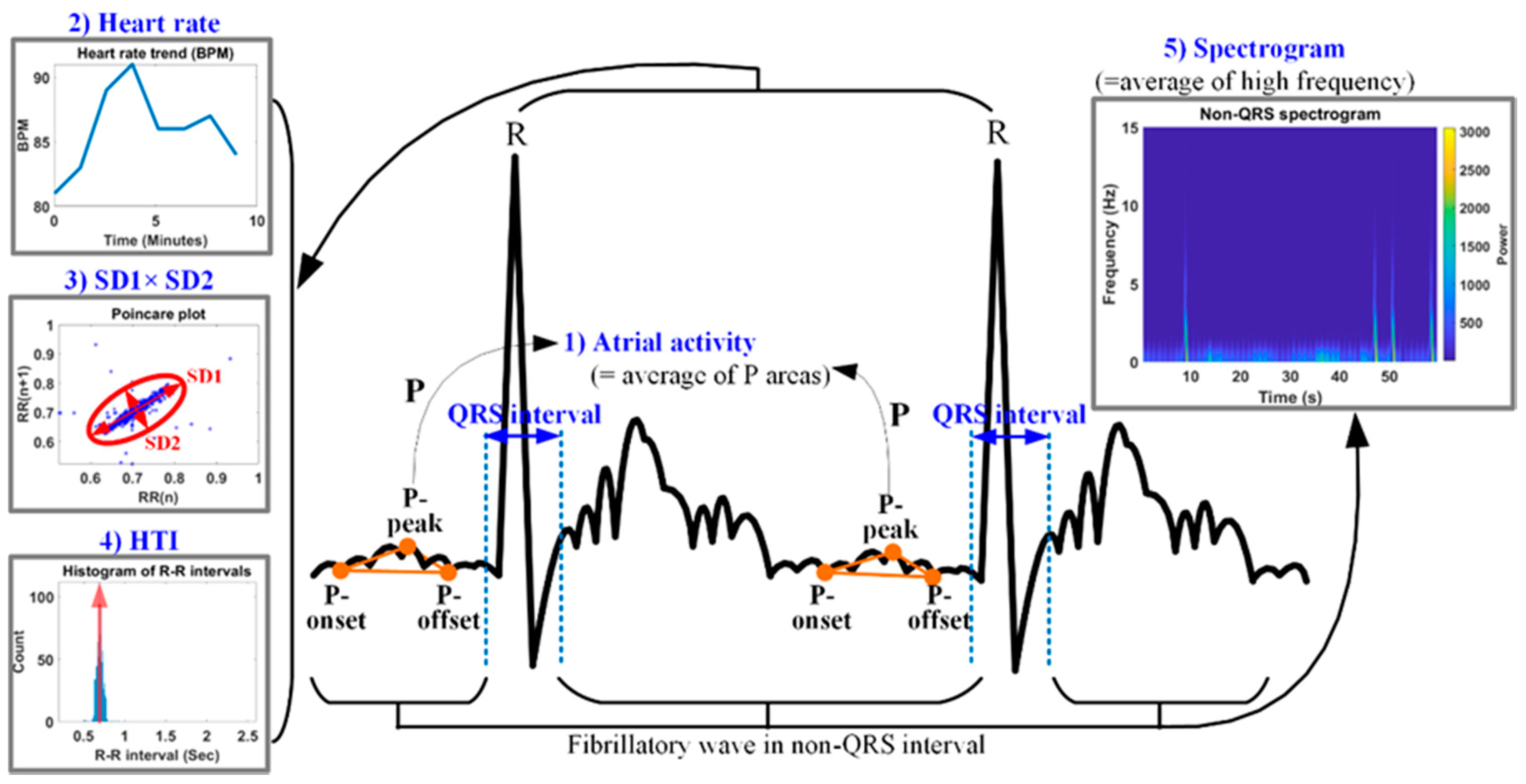
2.3.4. AF
3. Results
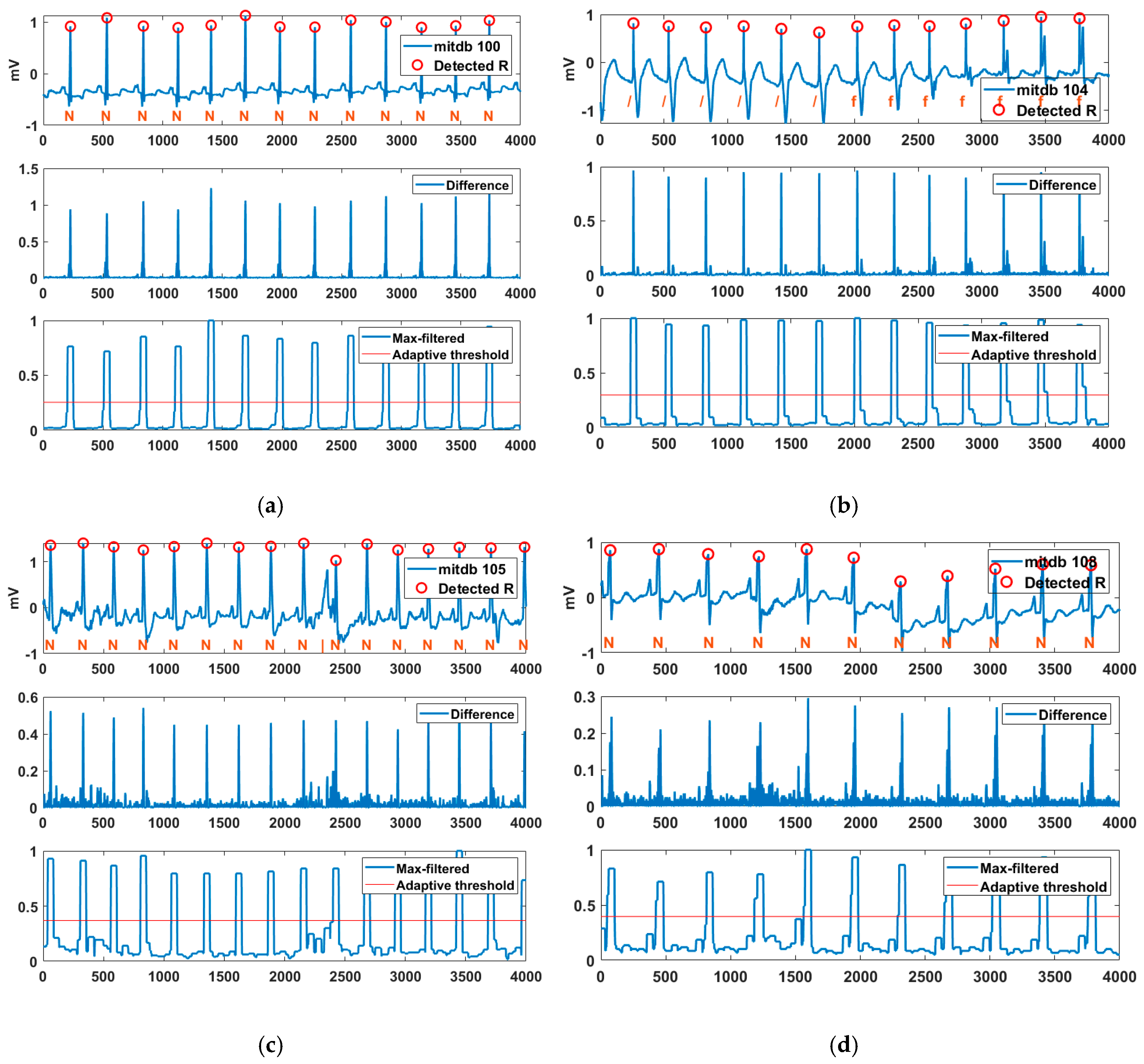
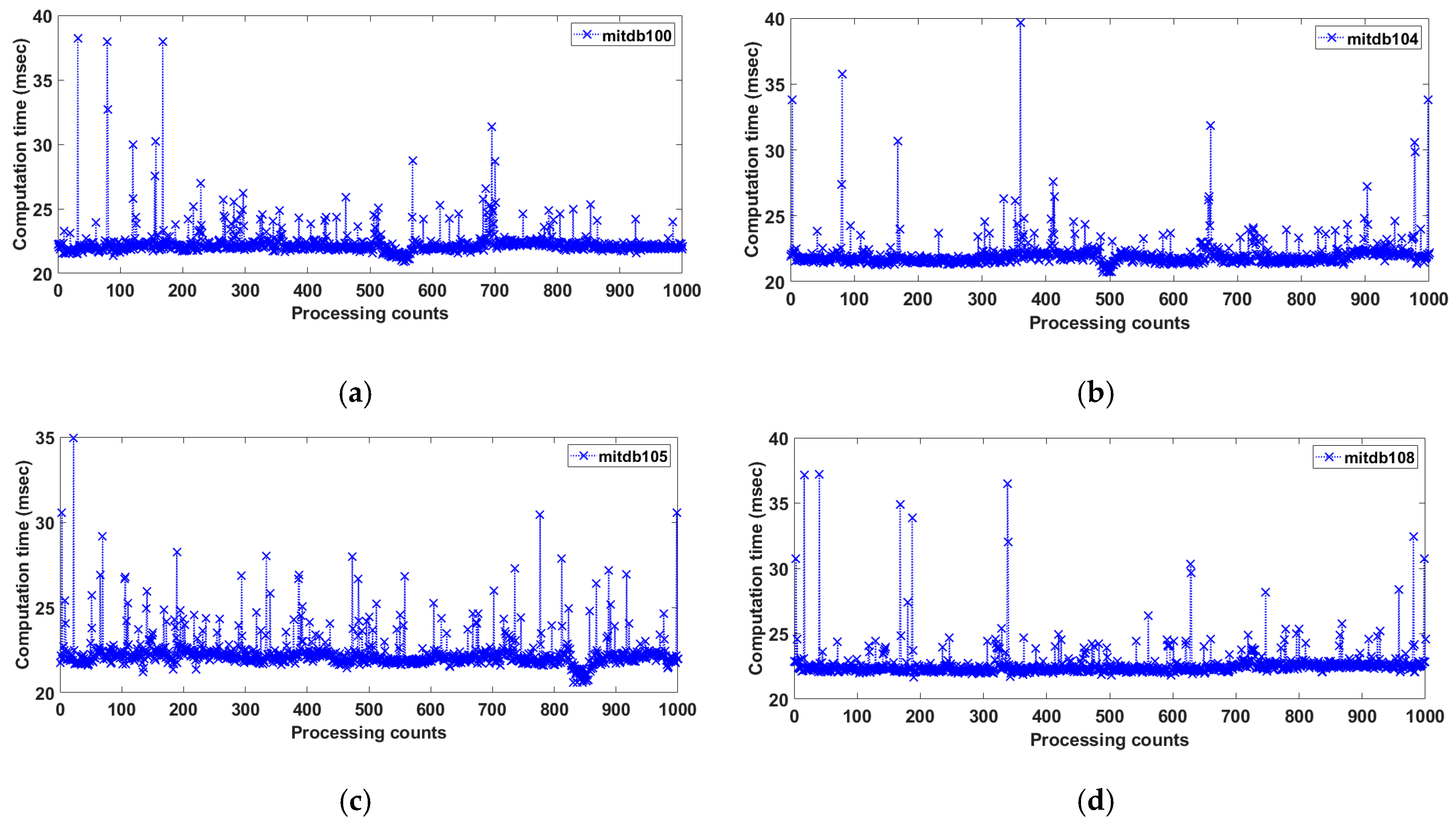
3.1. R-Peak Detection Performance Using MITDB
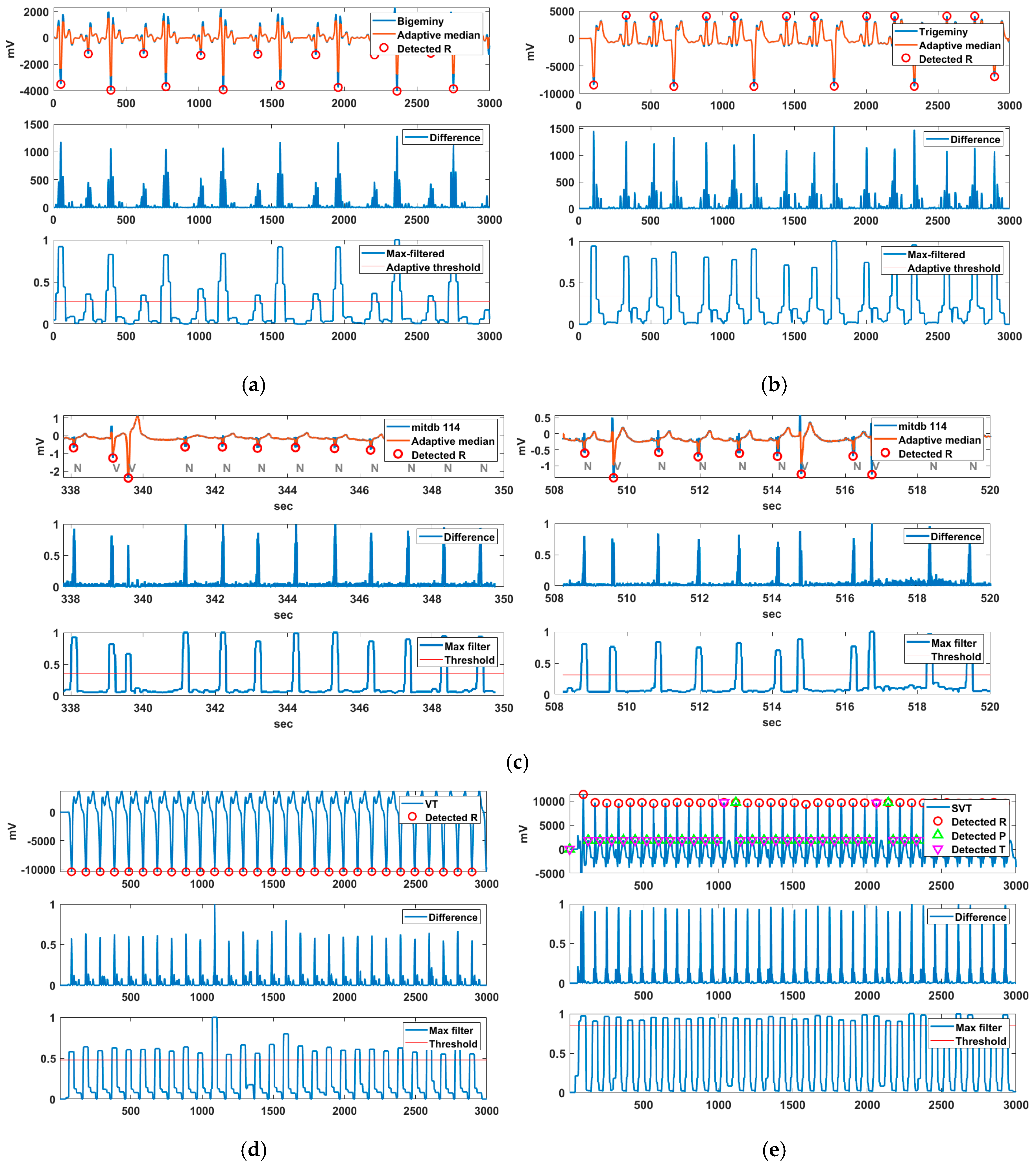
3.2. Arrhythmic Feature Detection Using Various ECG Data
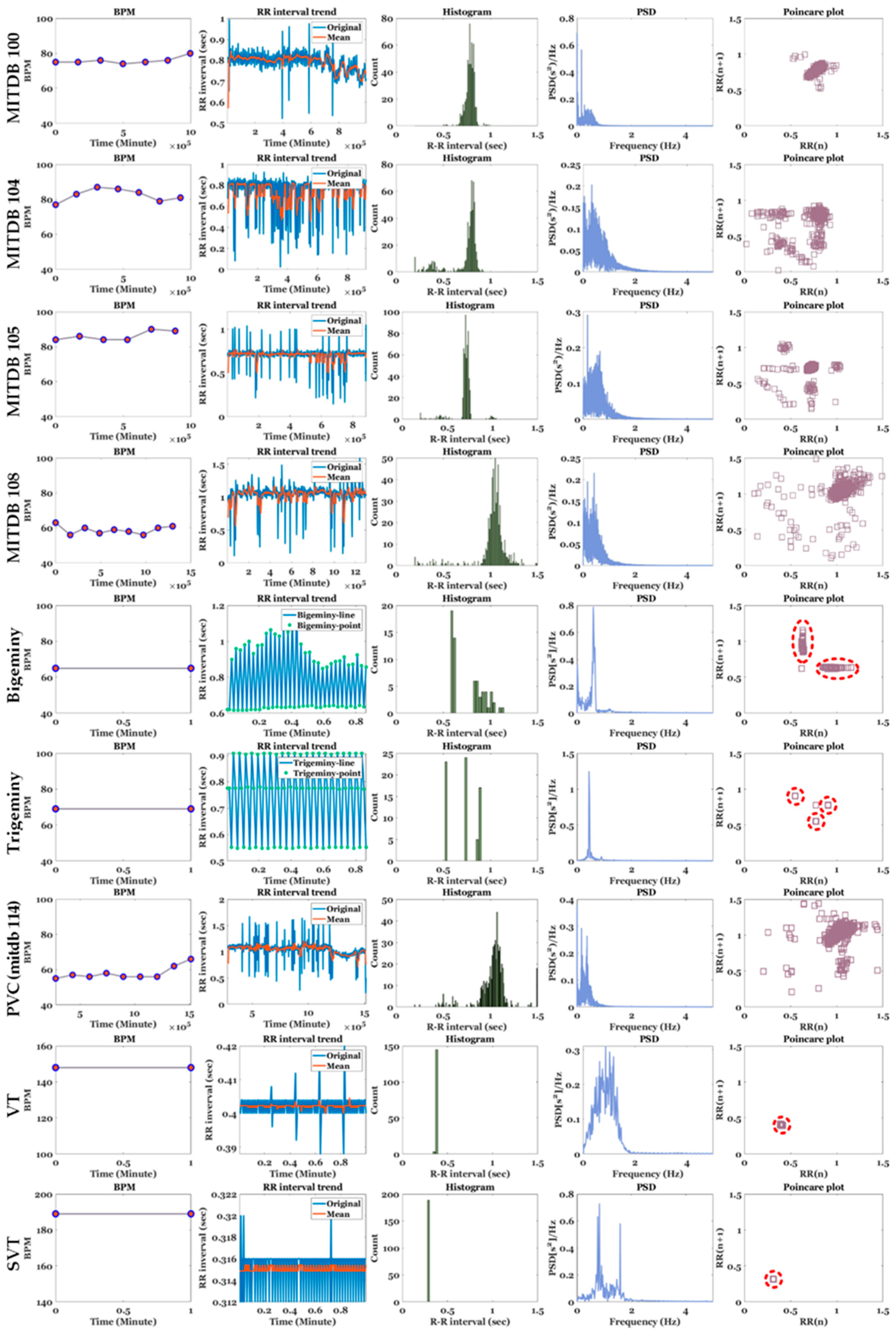
3.3. HRV Analysis of Various ECG Signals
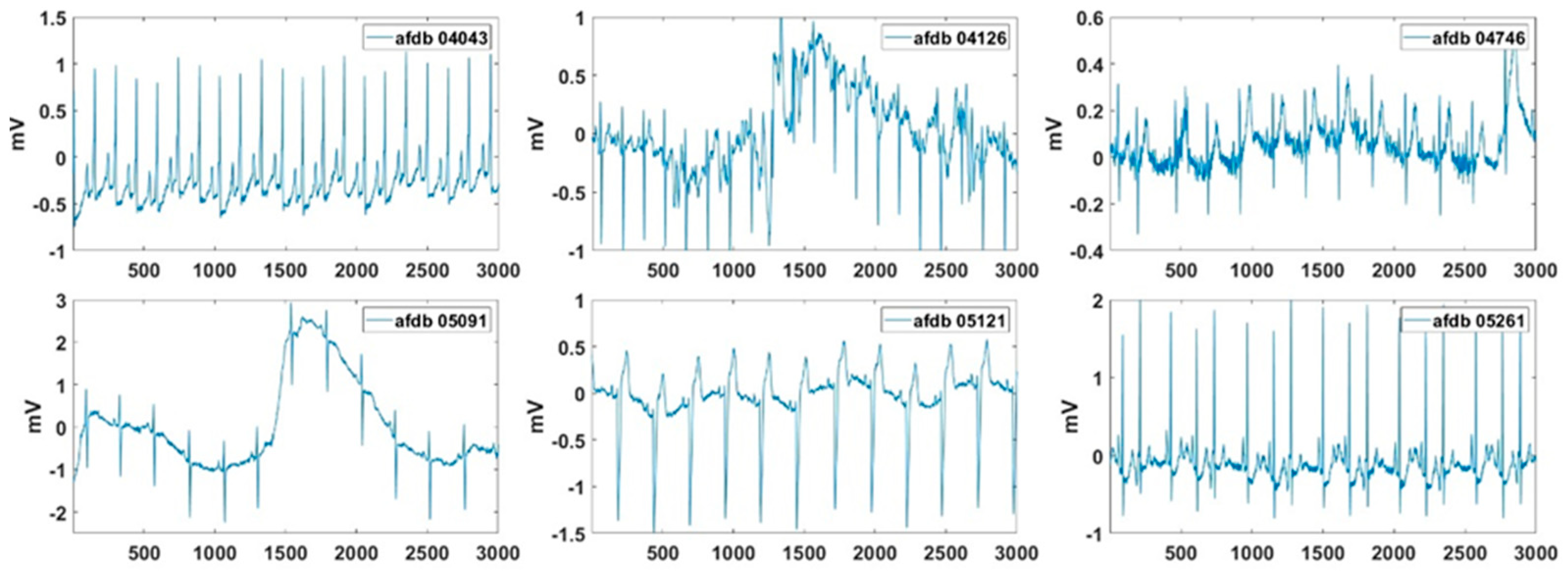
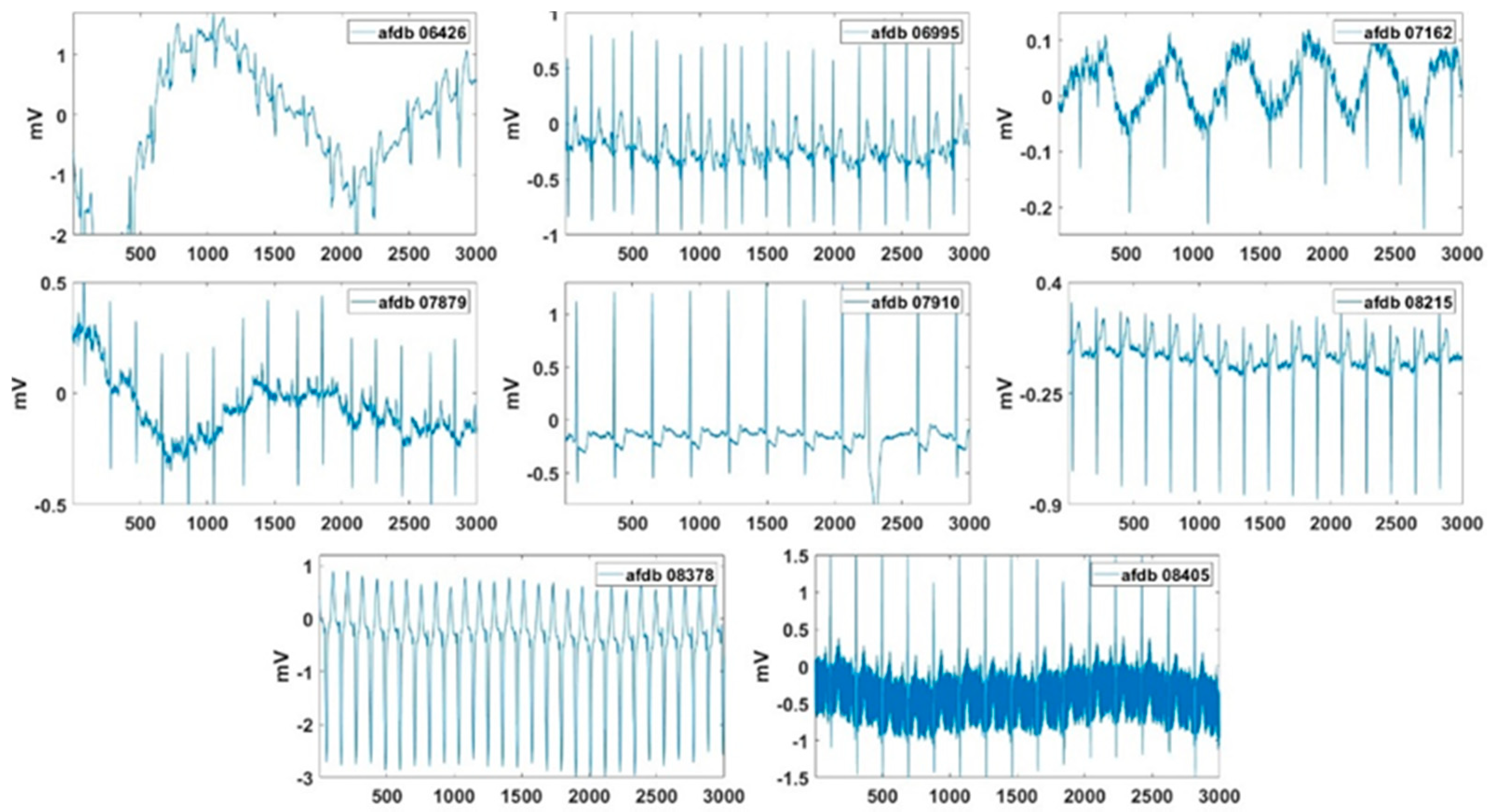
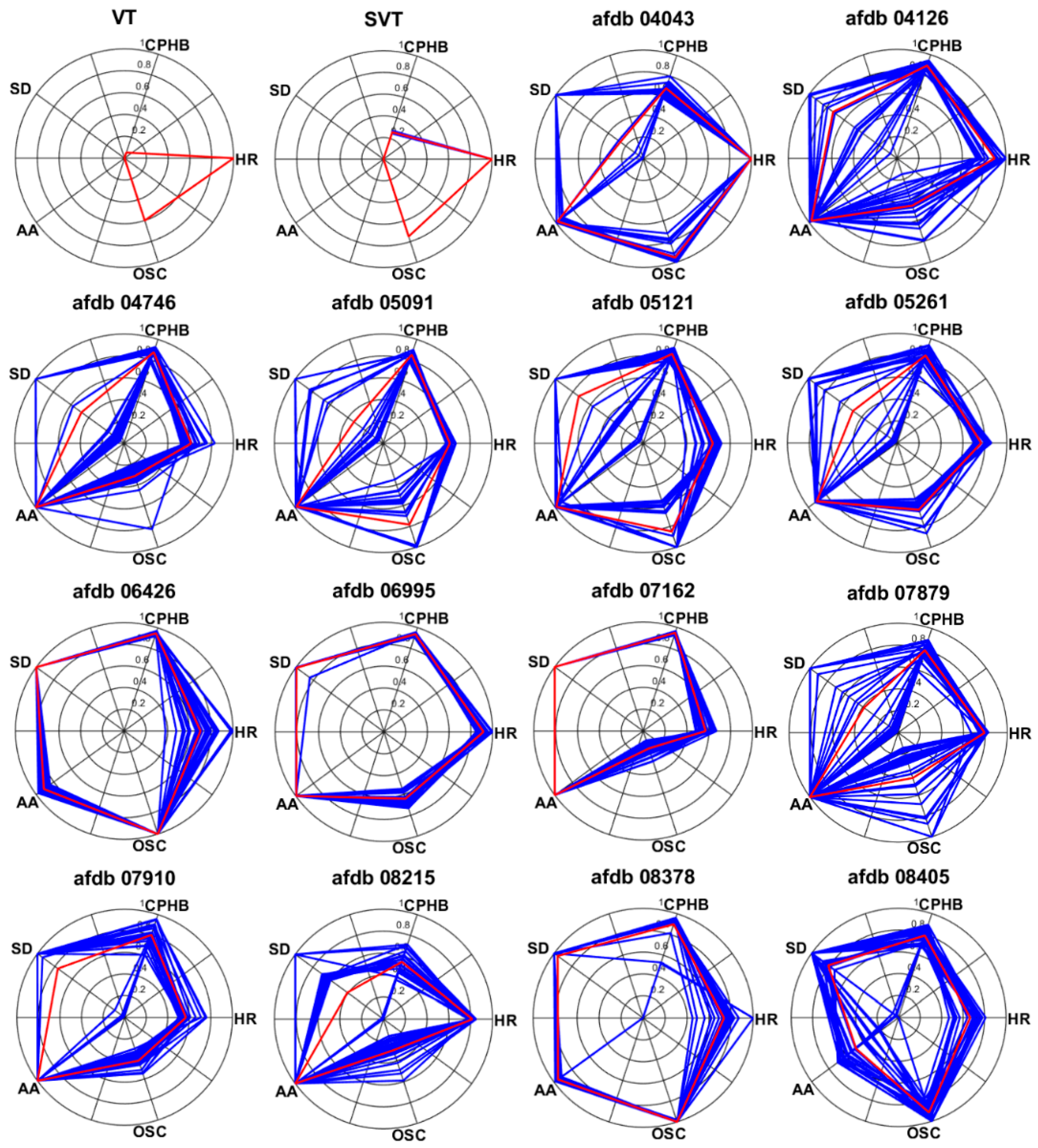
3.4. AF Detection
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Product Overview of Wearable Bio Patch MC100. Available online: https://www.seerstech.com/wearable-bio-patch (accessed on 23 September 2020).
- KardiaMobile. Available online: https://store.alivecor.com/products/kardiamobile (accessed on 23 September 2020).
- TLC5000 Dynamic ECG Systems. Available online: http://www.contecmed.com/index.php?page=shop.product_details&flypage=flypage.tpl&product_id=88&category_id=11&option=com_virtuemart&Itemid=605 (accessed on 23 September 2020).
- MIT-BIH Arrhythmia Database. Available online: https://physionet.org/content/mitdb/1.0.0 (accessed on 23 September 2020).
- MIT-BIH Atrial Fibrillation Database. Available online: https://physionet.org/content/afdb/1.0.0 (accessed on 23 September 2020).
- QT Database. Available online: https://physionet.org/content/qtdb/1.0.0 (accessed on 23 September 2020).
- Long Term AF Database. Available online: https://physionet.org/content/ltafdb/1.0.0 (accessed on 23 September 2020).
- MS400 Multiparameter Simulator. Available online: http://www.contecmed.com/index.php?page=shop.product_details&flypage=flypage.tpl&product_id=102&category_id=18&option=com_virtuemart&Itemid=601 (accessed on 23 September 2020).
- Benitez, D.S.; Gaydecki, P.A.; Zaidi, A.; Fitzpatrick, A.P. A new QRS detection algorithm based on the hilbert transform. In Proceedings of the Computers in Cardiology, Cambridge, MA, USA, 24–27 September 2000; pp. 379–382. [Google Scholar]
- Pan, J.; Tompkins, W.J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng. 1985, 32, 230–236. [Google Scholar] [CrossRef]
- Hamilton, P.S.; Tompkins, W.J. Quantitative investigation of QRS detection rules using the MIT/BIH arrhythmia database. IEEE Trans. Biomed. Eng. 1986, 33, 1157–1165. [Google Scholar] [CrossRef]
- Xue, Q.; Hu, Y.H.; Tompkins, W.J. Neural-network-based adaptive filtering for QRS detection. IEEE Trans. Biomed. Eng. 1992, 39, 315–329. [Google Scholar] [CrossRef]
- Arzeno, N.M.; Deng, Z.D.; Poon, C.S. Analysis of first-derivative based QRS detection algorithms. IEEE Trans. Biomed. Eng. 2008, 55, 478–484. [Google Scholar] [CrossRef]
- Zhang, F.; Tan, J.; Lian, Y. An effective QRS detection algorithm for wearable ECG in body area network. In Proceedings of the IEEE Biomedical Circuits and Systems Conference, Montreal, QC, Canada, 27–30 November 2007; pp. 195–198. [Google Scholar]
- Castells-Rufas, D.; Carrabina, J. Simple real-time QRS detector with the MaMeMi filter. Biomed. Signal Process. Control 2015, 21, 137–145. [Google Scholar] [CrossRef]
- Poli, R.; Cagnoni, S.; Valli, G. Genetic design of optimum linear and nonlinear QRS detectors. IEEE Trans. Biomed. Eng. 1995, 42, 1137–1141. [Google Scholar] [CrossRef]
- Alvarado, C.; Arregui, J.; Pallas-Areny, R. Automatic detection of ECG ventricular activity waves using continuous spline wavelet transform. In Proceedings of the 2nd International Conference on Electrical and Electronics Engineering 2005, Mexico City, Mexico, 9 September 2005; pp. 189–192. [Google Scholar]
- Chen, S.; Chen, H.; Chan, H. A real time QRS detection method based on moving-averaging incorporating with wavelet denosing. Comput. Methods Programs Biomed. 2006, 82, 187–195. [Google Scholar] [CrossRef]
- Zhang, F.; Lian, Y. QRS detection based on multi-scale mathematical morphology for wearable ECG device in body area networks. IEEE Trans. Biomed. Circuits Syst. 2009, 3, 220–228. [Google Scholar] [CrossRef]
- Bae, T.W.; Kwon, K.K. Efficient real-time R and QRS detection method using a pair of derivative filters and max filter for portable ECG device. Appl. Sci. 2019, 9, 4128. [Google Scholar] [CrossRef]
- Hossain, M.B.; Bashar, S.K.; Walkey, A.J.; McManus, D.D.; Chon, K.H. An accurate QRS complex and P wave detection in ECG signals using complete ensemble empirical mode decomposition with adaptive noise approach. IEEE Access 2019, 7, 128869–128880. [Google Scholar] [CrossRef]
- Rahul, J.; Sora, M. A novel adaptive window based technique for T wave detection and delineation in the ECG. Bio Algorithms Med. Syst. 2020, 16, 1–10. [Google Scholar] [CrossRef]
- Heartline ECG Monitoring. Available online: https://www.aerotel.com/index.php/en/products-and-solutions/heartline-ecg-monitoring (accessed on 9 October 2020).
- Serhani, M.A.; El Kassabi, H.T.; Ismail, H.; Nujum Navaz, A. ECG monitoring systems: Review, architecture, processes, and key challenges. Sensors 2020, 20, 1796. [Google Scholar] [CrossRef]
- Abo-Zahhad, M.; Ahmed, S.M.; Elnahas, O. A wireless emergency telemedicine system for patients monitoring and diagnosis. Int. J. Telemed. Appl. 2014, 2014, 1–11. [Google Scholar] [CrossRef]
- Tripathy, R.K.; Bhattacharyya, A.; Pachori, R.B. Localization of myocardial infarction from multi-lead ECG signals using multiscale analysis and convolutional neural network. IEEE Sens. 2019, 19, 11437–11448. [Google Scholar] [CrossRef]
- Mobile ECG with Web-Based Telemedicine Platform. Available online: https://www.who.int/medical_devices/innovation/compendium_med_dev2012_9.pdf?ua=1 (accessed on 9 October 2020).
- Fantoni, C.; Raffa, S.; Regoli, F.; Giraldi, F.; La Rovere, M.T.; Prentice, J.; Pastori, F.; Fratini, S.; Salerno-Uriarte, J.A.; Klein, H.U.; et al. Cardiac resynchronization therapy improves heart rate profile and heart rate variability of patients with moderate to severe heart failure. J. Am. Coll. Cardiol. 2005, 46, 1875–1882. [Google Scholar] [CrossRef]
- Stipdonk, A.; Wijers, S.; Meine, M.; Vernooy, K. ECG patterns in cardiac resynchronization therapy. J. Atr. Fibrillation 2015, 7, 1–6. [Google Scholar]
- Shelly, I.L. Algorithm for Premature Ventricular Contraction Detection from a Subcutaneous Electrocardiogram Signal. Master’s Thesis, Portland State University, Portland, OR, USA, 2016. [Google Scholar]
- Tropeano, F. Arrhythmia detection and classification through the analysis of human ECG signal. Master’s Thesis, Sapienza—University of Rome, Rome, Italy, 2019. [Google Scholar]
- Malek, A.S.; Elnahrawy, A.; Anwar, H.; Naeem, M. Automated detection of premature ventricular contraction in ECG signals using enhanced template matching algorithm. Biomed. Phys. Eng. Express 2020, 6, 015024. [Google Scholar] [CrossRef]
- Zarei, R.; He, J.; Huang, G.; Zhang, Y. Effective and efficient detection of premature ventricular contractions based on variation of principal directions. Digit. Signal Process. 2016, 50, 93–102. [Google Scholar] [CrossRef]
- Thachil, A.; Chennapragada, S.; Calambur, N. Inappropriate detection of a supraventricular tachycardia as dual tachycardia by the PR logic algorithm. Indian Pacing Electrophysiol. J. 2014, 14, 161–164. [Google Scholar] [CrossRef]
- Li, Z.; Derksen, H.; Gryak, J.; Hooshmand, M.; Wood, A. Supraventricular tachycardia detection via machine learning algorithms. In Proceedings of the IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Madrid, Spain, 3–6 December 2018; pp. 2419–2422. [Google Scholar]
- VP-100. Available online: http://www.tribell-lab.com/product/view.html?pid=17&cate1=53&cate2=81&no=81 (accessed on 23 September 2020).
- Verma, K.; Singh, B.K.; Thoke, A.S. An enhancement in adaptive median filter for edge preservation. Procedia Comput. Sci. 2015, 48, 29–36. [Google Scholar] [CrossRef]
- Lin, H.M.; Willson, A.N. Median filters with adaptive length. IEEE Trans. Circuits Syst. 1988, 35, 675–690. [Google Scholar] [CrossRef]
- Suoranta, R.; Estola, K.-P. Robust median filter with adaptive window length. In Proceedings of the IEEE International Symposium on Circuits and Systems, Singapore, 11–14 June 1991; pp. 108–111. [Google Scholar]
- Categories of Arrhythmias. Available online: https://www.texasheart.org/heart-health/heart-information-center/topics/categories-of-arrhythmias/#:~:text=Ventricular%20arrhythmias%20occur%20in%20the,or%20too%20fast%20(tachycardia) (accessed on 23 September 2020).
- What Is Bigeminy? Available online: https://www.webmd.com/heart-disease/atrial-fibrillation/bigeminy-arrhythmia (accessed on 23 September 2020).
- What Is Trigeminy and How Is It Treated? Available online: https://www.healthline.com/health/trigeminy (accessed on 23 September 2020).
- Premature Ventricular Complex. Available online: https://litfl.com/premature-ventricular-complex-pvc-ecg-library (accessed on 23 September 2020).
- Premature Ventricular Contractions. Available online: https://www.mayoclinic.org/diseases-conditions/premature-ventricular-contractions/symptoms-causes/syc-20376757#:~:text=Premature%20ventricular%20contractions%20(PVCs)%20are,skipped%20beat%20in%20your%20chest (accessed on 23 September 2020).
- Supraventricular Tachycardia. Available online: https://www.mayoclinic.org/diseases-conditions/supraventricular-tachycardia/symptoms-causes/syc-20355243#:~:text=Overview,the%20atria%20or%20AV%20node (accessed on 23 September 2020).
- What is Atrial Fibrillation? Available online: https://www.healthline.com/health/living-with-atrial-fibrillation (accessed on 23 September 2020).
- Mechanism of Atrial Fibrillation. Available online: https://litfl.com/atrial-fibrillation-ecg-library (accessed on 23 September 2020).
- The P Wave. Available online: http://platosnous.com/main-blog/2015/11/2/the-p-wave#:~:text=Figure%2013.,mm%20and%20a%20pointed%20tip (accessed on 23 September 2020).
- Atrial Fibrillation. Available online: https://ecgwaves.com/topic/atrial-fibrillation-ecg-ekg-causes-classification-management (accessed on 14 October 2020).
- Gertsch, M. Atrial fibrillation. In The ECG Manual; Springer: London, UK, 2009; pp. 223–224. [Google Scholar]
- Shaffer, F.; Ginsberg, J.P. An overview of heart rate variability metrics and norms. Front. Public Health 2017, 5, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Heart Rate Variability. Available online: https://www.firstbeat.com/en/science-and-physiology/heart-rate-variability (accessed on 23 September 2020).
- Heart Rate Variability: A New Way to Track Well-Being. Available online: https://www.health.harvard.edu/blog/heart-rate-variability-new-way-track-well-2017112212789 (accessed on 23 September 2020).
- Records in the MIT-BIH Arrhythmia Database. Available online: https://archive.physionet.org/physiobank/database/html/mitdbdir/records.htm#114 (accessed on 23 September 2020).
- Elgendi, M.; Mohamed, A.; Ward, R. Efficient ECG compression and QRS detection for E-Health applications. Sci. Rep. 2017, 7, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Rebollo-Neira, L. Effective high compression of ECG signals at low level distortion. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Elena, M.M.; Quero, J.M.; Borrego, I. Optimal selection of wavelet coefficients for electrocardiograph compression. ETRI J. 2007, 29, 530–532. [Google Scholar] [CrossRef]
- Xiao, N.; Yu, W.; Han, X. Wearable heart rate monitoring intelligent sports bracelet based on Internet of things. Measurement 2020, 164, 108102. [Google Scholar] [CrossRef]
- Lazazzera, R.; Belhaj, Y.; Carrault, G. A new wearable device for blood pressure estimation using photoplethysmogram. Sensors 2019, 19, 2557. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Processing Unit (per) | Kinds of Arrhythmia |
|---|---|
| One beat | Premature ventricular contraction (PVC) |
| Multiple beat (or one minute) | Bigeminy, trigeminy |
| At least one minute | Bradycardia, tachycardia, ventricular tachycardia (VT), supraventricular tachycardia (SVT), atrial fibrillation (AF) |
| Tape | Total | FN | FP | Se [%] | +P [%] | DER [%] | Tape | Total | FN | FP | Se [%] | +P [%] | DER [%] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 100 | 2273 | 0 | 0 | 100 | 100 | 0 | 201 | 1963 | 7 | 3 | 99.64 | 99.85 | 0.51 |
| 101 | 1865 | 2 | 5 | 99.89 | 99.73 | 0.38 | 202 | 2136 | 4 | 5 | 99.81 | 99.77 | 0.42 |
| 102 | 2187 | 1 | 1 | 99.95 | 99.95 | 0.09 | 203 | 2980 | 18 | 21 | 99.40 | 99.30 | 1.31 |
| 103 | 2084 | 0 | 1 | 100 | 99.95 | 0.05 | 205 | 2656 | 7 | 3 | 99.74 | 99.89 | 0.38 |
| 104 | 2229 | 3 | 12 | 99.87 | 99.46 | 0.67 | 207 | 1862 | 9 | 7 | 99.52 | 99.62 | 0.86 |
| 105 | 2572 | 11 | 18 | 99.57 | 99.30 | 1.13 | 208 | 2955 | 13 | 5 | 99.56 | 99.83 | 0.61 |
| 106 | 2027 | 5 | 6 | 99.75 | 99.70 | 0.54 | 209 | 3004 | 4 | 5 | 99.87 | 99.83 | 0.30 |
| 107 | 2137 | 2 | 5 | 99.91 | 99.77 | 0.33 | 210 | 2650 | 14 | 6 | 99.47 | 99.77 | 0.75 |
| 108 | 1774 | 7 | 27 | 99.61 | 98.49 | 1.92 | 212 | 2748 | 3 | 5 | 99.89 | 99.82 | 0.29 |
| 109 | 2532 | 3 | 4 | 99.88 | 99.84 | 0.28 | 213 | 3251 | 2 | 5 | 99.94 | 99.85 | 0.22 |
| 111 | 2124 | 4 | 3 | 99.81 | 99.86 | 0.33 | 214 | 2265 | 2 | 2 | 99.91 | 99.91 | 0.18 |
| 112 | 2539 | 0 | 1 | 100 | 99.96 | 0.04 | 215 | 3363 | 1 | 3 | 99.97 | 99.91 | 0.12 |
| 113 | 1795 | 2 | 4 | 99.89 | 99.78 | 0.33 | 217 | 2209 | 5 | 2 | 99.77 | 99.91 | 0.32 |
| 114 | 1879 | 2 | 5 | 99.89 | 99.73 | 0.37 | 219 | 2154 | 2 | 5 | 99.91 | 99.77 | 0.32 |
| 115 | 1953 | 0 | 1 | 100 | 99.95 | 0.05 | 220 | 2048 | 1 | 1 | 99.95 | 99.95 | 0.10 |
| 116 | 2412 | 9 | 5 | 99.63 | 99.79 | 0.58 | 221 | 2427 | 5 | 2 | 99.79 | 99.92 | 0.29 |
| 117 | 1535 | 2 | 3 | 99.87 | 99.80 | 0.33 | 222 | 2483 | 7 | 2 | 99.72 | 99.92 | 0.36 |
| 118 | 2278 | 0 | 1 | 100 | 99.96 | 0.04 | 223 | 2605 | 5 | 1 | 99.81 | 99.96 | 0.23 |
| 119 | 1987 | 1 | 3 | 99.95 | 99.85 | 0.20 | 228 | 2053 | 6 | 8 | 99.71 | 99.61 | 0.68 |
| 121 | 1863 | 4 | 2 | 99.79 | 99.89 | 0.32 | 230 | 2256 | 3 | 2 | 99.87 | 99.91 | 0.22 |
| 122 | 2476 | 0 | 1 | 100 | 99.96 | 0.04 | 231 | 1571 | 1 | 2 | 99.94 | 99.87 | 0.19 |
| 123 | 1518 | 3 | 1 | 99.80 | 99.93 | 0.26 | 232 | 1780 | 3 | 4 | 99.83 | 99.78 | 0.39 |
| 124 | 1619 | 2 | 1 | 99.88 | 99.94 | 0.19 | 233 | 3079 | 5 | 1 | 99.84 | 99.97 | 0.19 |
| 200 | 2601 | 1 | 7 | 99.96 | 99.73 | 0.31 | 234 | 2753 | 3 | 2 | 99.89 | 99.93 | 0.18 |
| Total | 109510 | 194 | 219 | 99.82 | 99.80 | 0.38 |
| Method | FP | FN | DER (%) | Ref |
|---|---|---|---|---|
| Linear adaptive filter | 40 | 22 | 2.41 | [12] |
| Bandpass filter | 67 | 22 | 3.46 | [10] |
| Generic algorithm | 86 | 5 | 3.54 | [16] |
| Wavelet transform | 31 | 13 | 1.17 | [17] |
| Wavelet denoising | 5 | 78 | 3 | [18] |
| 3M method | 19 | 7 | 1.01 | [19] |
| Derivative-max filter | 20 | 13 | 1.28 | [20] |
| Proposed method | 18 | 11 | 1.13 |
| Arrhythmias | Length | No. of Beats | FN | FP | Se(%) | +P(%) | DER(%) |
|---|---|---|---|---|---|---|---|
| Bigeminy | 56 sec | 72 | 7 | 0 | 90.28 | 100 | 9.72 |
| Trigeminy | 56 sec | 79 | 10 | 0 | 87.34 | 100 | 12.66 |
| VT | 59 sec | 149 | 1 | 0 | 99.33 | 100 | 0.67 |
| SVT | 59 sec | 191 | 2 | 0 | 98.95 | 100 | 1.05 |
| Variables | Units | Meaning | |
|---|---|---|---|
| Time domain | Mean HR | [s] | - |
| HR std. | [s] | - | |
| RR mean | [s] | Average RR interval in the window of measurement | |
| NN50 | [count] | Number of adjacent RR intervals that varied by more than 50 ms | |
| pNN50 | [%] | Percentage of adjacent RR intervals that varied by more than 50 ms | |
| RMSSD | [s] | Root mean square of difference between coupling intervals of adjacent RR intervals | |
| HTI | - | Reciprocal of probability of the highest bin of histogram of RR intervals | |
| TINN | - | The baseline width of the distribution measured as a base of a triangle | |
| Frequency domain | VLF power | [ms2] | Power from very low frequency (0 Hz~0.04 Hz) |
| LF power | [ms2] | Power from low frequency (0.04 Hz~0.15 Hz) | |
| HF power | [ms2] | Power from high frequency (0.15 Hz~0.40 Hz) | |
| VLF | [%] | (VLF Power/Total Power) × 100 | |
| LF | [%] | (LF Power/Total Power) × 100 | |
| HF | [%] | (HF Power/Total Power) × 100 | |
| LF/HF | - | Sympathovagal balance |
| HRV | MITDB | Arrhythmias | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 100 | 104 | 105 | 108 | Bigeminy | Trigeminy (gen.*) | PVC (mitdb114) | VT (gen. *) | SVT (gen. *) | |
| RR mean | 0.79 | 0.73 | 0.70 | 1.03 | 0.79 | 0.74 | 1.04 | 0.40 | 0.32 |
| RR std. | 0.05 | 0.17 | 0.11 | 0.17 | 0.17 | 0.15 | 0.18 | - | - |
| Heart rate mean | 75.86 | 82.43 | 86.17 | 58.89 | 65 | 69 | 58 | 148 | 189 |
| Heart rate std. | 1.95 | 3.65 | 2.71 | 2.37 | - | - | 3.64 | - | - |
| RMSSD | 0.05 | 0.19 | 0.15 | 0.20 | 0.33 | 0.25 | 0.25 | 0.01 | 0.00 |
| NN50 | 23 | 118 | 49 | 142 | 31 | 45 | 144 | - | - |
| pNN50 | 3.96 | 20.31 | 8.43 | 24.44 | 48.44 | 66.18 | 26.23 | - | - |
| HTI | 7.66 | 8.56 | 6 | 11.64 | 3.42 | 2.88 | 12.50 | 1.02 | 1 |
| TINN | 0.21 | 0.25 | 0.11 | 0.39 | 0.06 | 0.03 | 0.31 | 0.06 | 0.03 |
| LF power | 22.91 | 29.33 | 25.08 | 32.41 | 37.12 | 10.39 | 16.25 | 15.43 | 27.34 |
| HF power | 77.09 | 70.67 | 74.92 | 67.59 | 62.88 | 89.61 | 83.73 | 84.57 | 72.66 |
| LF | 2.93 | 5.18 | 4.12 | 5.34 | 0.61 | 0.08 | 2.91 | 0.25 | 0.20 |
| HF | 9.84 | 12.48 | 12.29 | 11.13 | 1.03 | 0.66 | 14.98 | 1.35 | 0.52 |
| LF/HF | 0.30 | 0.42 | 0.33 | 0.48 | 0.59 | 0.12 | 0.19 | 0.18 | 0.38 |
| Records | HR | CPHB | SD | AA | OSC | Average |
|---|---|---|---|---|---|---|
| 04043 | 1 | 0.68 | 0.26 | 0.98 | 0.96 | 0.78 |
| 04126 | 0.90 | 0.90 | 0.73 | 0.97 | 0.46 | 0.79 |
| 04746 | 0.61 | 0.88 | 0.48 | 1 | 0.32 | 0.66 |
| 05091 | 0.61 | 0.85 | 0.33 | 0.99 | 0.78 | 0.71 |
| 05121 | 0.64 | 0.86 | 0.73 | 0.99 | 0.85 | 0.81 |
| 05261 | 0.77 | 0.84 | 0.50 | 0.91 | 0.64 | 0.73 |
| 06426 | 0.70 | 0.95 | 1 | 0.91 | 1 | 0.91 |
| 06995 | 0.92 | 0.94 | 0.99 | 1 | 0.64 | 0.90 |
| 07162 | 0.57 | 0.95 | 1 | 1 | 0.17 | 0.74 |
| 07879 | 0.79 | 0.79 | 0.34 | 0.99 | 0.43 | 0.67 |
| 07910 | 0.57 | 0.80 | 0.77 | 1 | 0.42 | 0.71 |
| 08215 | 0.82 | 0.55 | 0.41 | 1 | 0.30 | 0.61 |
| 08378 | 0.74 | 0.90 | 0.96 | 0.96 | 1 | 0.91 |
| 08405 | 0.67 | 0.79 | 0.81 | 0.49 | 0.92 | 0.73 |
| Average | 0.74 | 0.83 | 0.67 | 0.94 | 0.63 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, T.W.; Lee, S.H.; Kwon, K.K. An Adaptive Median Filter Based on Sampling Rate for R-Peak Detection and Major-Arrhythmia Analysis. Sensors 2020, 20, 6144. https://doi.org/10.3390/s20216144
Bae TW, Lee SH, Kwon KK. An Adaptive Median Filter Based on Sampling Rate for R-Peak Detection and Major-Arrhythmia Analysis. Sensors. 2020; 20(21):6144. https://doi.org/10.3390/s20216144
Chicago/Turabian StyleBae, Tae Wuk, Sang Hag Lee, and Kee Koo Kwon. 2020. "An Adaptive Median Filter Based on Sampling Rate for R-Peak Detection and Major-Arrhythmia Analysis" Sensors 20, no. 21: 6144. https://doi.org/10.3390/s20216144
APA StyleBae, T. W., Lee, S. H., & Kwon, K. K. (2020). An Adaptive Median Filter Based on Sampling Rate for R-Peak Detection and Major-Arrhythmia Analysis. Sensors, 20(21), 6144. https://doi.org/10.3390/s20216144