Spectral Reflectance Can Differentiate Tracheal and Esophageal Tissue in the Presence of Bodily Fluids and Soot

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Collection and Spectra Collection
2.2. Experimental Group 1
2.3. Experimental Group 2
2.4. Spectral Reflectance Processing
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
DOD Disclaimer
Animal Statement
References
- Goto, T.; Watase, H.; Morita, H.; Nagai, H.; A Brown, C.; Brown, D.F.; Hasegawa, K. Repeated attempts at tracheal intubation by a single intubator associated with decreased success rates in emergency departments: An analysis of a multicentre prospective observational study. Emerg. Med. J. 2015, 32, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Sakles, J.C.; Chiu, S.; Mosier, J.; Walker, C.; Stolz, U. The importance of first pass success when performing orotracheal intubation in the emergency department. Acad. Emerg. Med. 2013, 20, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Combes, X.; Jabre, P.; Jbeili, C.; Leroux, B.; Bastuji-Garin, S.; Margenet, A.; Adnet, F.; Dhonneur, G. Prehospital standardization of medical airway management: Incidence and risk factors of difficult airway. Acad. Emerg. Med. 2006, 13, 828–834. [Google Scholar] [CrossRef] [PubMed]
- Rudraraju, P.; Eisen, L.A. Analytic Review: Confirmation of Endotracheal Tube Position: A Narrative Review. J. Intensive Care Med. 2009, 24, 283–292. [Google Scholar] [CrossRef]
- Hasegawa, K.; Shigemitsu, K.; Hagiwara, Y.; Chiba, T.; Watase, H.; Brown, C.A.; Brown, D.F. Association between repeated intubation attempts and adverse events in emergency departments: An analysis of a multicenter prospective observational study. Ann. Emerg. Med. 2012, 60, 749–754.e2. [Google Scholar] [CrossRef]
- Habib, N.; Harris, K.; Chalhoub, M.; Maroun, R.; Ciccone, R.; Elsayegh, D. Prolonged Esophageal Intubation: Is it Still Possible? Clin. Pulm. Med. 2012, 19, 44–46. [Google Scholar] [CrossRef]
- Neumar, R.W.; Otto, C.W.; Link, M.S.; Kronick, S.L.; Shuster, M.; Callaway, C.W.; Kudenchuk, P.J.; Ornato, J.P.; McNally, B.; Silvers, S.M.; et al. Part 8: Adult Advanced Cardiovascular Life Support. Circulation 2010, 122, S729–S767. [Google Scholar] [CrossRef]
- Sahyoun, C.; Siliciano, C.; Kessler, D. Use of Capnography and Cardiopulmonary Resuscitation Feedback Devices Among Prehospital Advanced Life Support Providers. Pediatr. Emerg. Care 2018. [Google Scholar] [CrossRef]
- Cook, T.M.; Woodall, N.; Harper, J.; Benger, J. Major complications of airway management in the UK: Results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 2: Intensive care and emergency departments†. BJA Br. J. Anaesth. 2011, 106, 632–642. [Google Scholar] [CrossRef]
- Nawn, C.D.; Blackburn, M.B.; De Lorenzo, R.A.; Ryan, K.L. Using spectral reflectance to distinguish between tracheal and oesophageal tissue: Applications for airway management. Anaesthesia 2019, 74, 340–347. [Google Scholar] [CrossRef]
- Nawn, C.D.; Souhan, B.E.; Carter, R.; Kneapler, C.; Fell, N.; Ye, J.Y. Distinguishing tracheal and esophageal tissues with hyperspectral imaging and fiber-optic sensing. J. Biomed. Opt. 2016, 21, 117004. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, M.B.; Nawn, C.D.; Ryan, K.L. Testing of novel spectral device sensor in swine model of airway obstruction. Physiol. Rep. 2019, 7, e14246. [Google Scholar] [CrossRef] [PubMed]
- Nawn, C.D.; Souhan, B.B.; Carter, R.; Kneapler, C.; Fell, N.F.; Ye, J.Y. Spectral characterization of tracheal and esophageal tissues using a hyperspectral camera and fiber optic sensors. In Proceedings of the Optical Fibers and Sensors for Medical Diagnostics and Treatment Applications XVI, San Francisco, CA, USA, 7 March 2016. [Google Scholar]
- Souhan, B.E.; Nawn, C.D.; Shmel, R.; Watts, K.L.; Ingold, K.A. Fiber optic tracheal detection device. In Proceedings of the Optical Fibers and Sensors for Medical Diagnostics and Treatment Applications XVII, San Francisco, CA, USA, 28 February 2017. [Google Scholar]
- Racine, J.; Li, Q. Nonparametric estimation of regression functions with both categorical and continuous data. J. Econom. 2004, 119, 99–130. [Google Scholar] [CrossRef]
- Tristen, H.; Racine, J. Nonparametric Econometrics: The Np Package. J. Stat. Softw. 2008, 27, 1–32. [Google Scholar]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.; Murphy, M.P.; Dickson, R.L.; Somerville, G.G.; Brizendine, E.J. Emergency Physician-Verified Out-of-hospital Intubation: Miss Rates by Paramedics. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2004, 11, 707–709. [Google Scholar]
- Silvestri, S.; Ralls, G.A.; Krauss, B.; Thundiyil, J.; Rothrock, S.G.; Senn, A.; Carter, E.; Falk, J. The effectiveness of out-of-hospital use of continuous end-tidal carbon dioxide monitoring on the rate of unrecognized misplaced intubation within a regional emergency medical services system. Ann. Emerg. Med. 2005, 45, 497–503. [Google Scholar] [CrossRef]
- Rabitsch, W.; Nikolic, A.; Schellongowski, P.; Kofler, J.; Kraft, P.; Krenn, C.G.; Staudinger, T.; Locker, G.J.; Knöbl, P.; Hofbauer, R.; et al. Evaluation of an end-tidal portable ETCO2 colorimetric breath indicator (COLIBRI). Am. J. Emerg. Med. 2004, 22, 4–9. [Google Scholar] [CrossRef]
- Berlac, P.; Hyldmo, P.K.; Kongstad, P.; Kurola, J.; Nakstad, A.R.; Sandberg, M. Pre-hospital airway management: Guidelines from a task force from the Scandinavian Society for Anaesthesiology and Intensive Care Medicine. Acta Anaesthesiol. Scand. 2008, 52, 897–907. [Google Scholar] [CrossRef]
- Kodali, B.S.; Urman, R.D. Capnography during cardiopulmonary resuscitation: Current evidence and future directions. J. Emerg. Trauma Shock. 2014, 7, 332–340. [Google Scholar]
- Paal, P.; Herff, H.; Mitterlechner, T.; Von Goedecke, A.; Brugger, H.; Lindner, K.H.; Wenzel, V. Anaesthesia in prehospital emergencies and in the emergency room. Resuscitation 2010, 81, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Nitzan, M.; Romem, A.; Koppel, R. Pulse oximetry: Fundamentals and technology update. Med. Devices 2014, 7, 231–239. [Google Scholar] [CrossRef]
- MacKenzie, L.E.; Harvey, A.R. Oximetry using multispectral imaging: Theory and application. J. Opt. 2018, 20, 063501. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Substance | Ratio | |
|---|---|---|
| B | Y | |
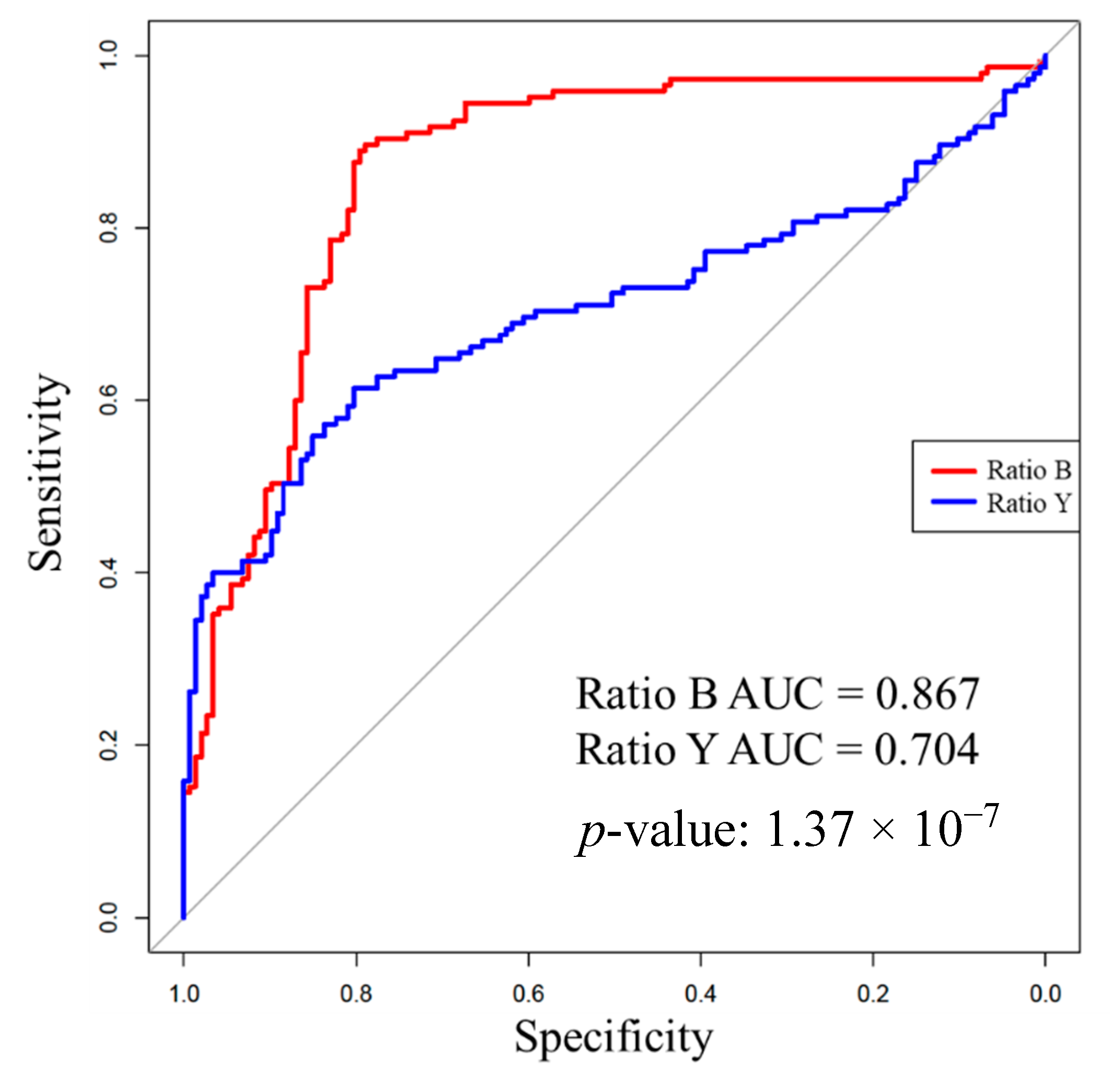
| Overall | 0.867 | 0.704 |
| Baseline | 0.891 | 0.871 |
| Saline | 0.947 | 0.878 |
| Blood | 0.763 | 0.364 |
| “Vomit” | 0.873 | 0.801 |
| Soot | 0.847 | 0.557 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berard, D.; Sen, C.; Nawn, C.D.; Blackburn, A.N.; Ryan, K.L.; Blackburn, M.B. Spectral Reflectance Can Differentiate Tracheal and Esophageal Tissue in the Presence of Bodily Fluids and Soot. Sensors 2020, 20, 6138. https://doi.org/10.3390/s20216138
Berard D, Sen C, Nawn CD, Blackburn AN, Ryan KL, Blackburn MB. Spectral Reflectance Can Differentiate Tracheal and Esophageal Tissue in the Presence of Bodily Fluids and Soot. Sensors. 2020; 20(21):6138. https://doi.org/10.3390/s20216138
Chicago/Turabian StyleBerard, David, Chirantan Sen, Corinne D. Nawn, August N. Blackburn, Kathy L. Ryan, and Megan B. Blackburn. 2020. "Spectral Reflectance Can Differentiate Tracheal and Esophageal Tissue in the Presence of Bodily Fluids and Soot" Sensors 20, no. 21: 6138. https://doi.org/10.3390/s20216138
APA StyleBerard, D., Sen, C., Nawn, C. D., Blackburn, A. N., Ryan, K. L., & Blackburn, M. B. (2020). Spectral Reflectance Can Differentiate Tracheal and Esophageal Tissue in the Presence of Bodily Fluids and Soot. Sensors, 20(21), 6138. https://doi.org/10.3390/s20216138