Study of Three Interface Pressure Measurement Systems Used in the Treatment of Venous Disease



Abstract
1. Introduction
2. Materials and Methods
2.1. Sensors
2.2. Calibration of the Sensors
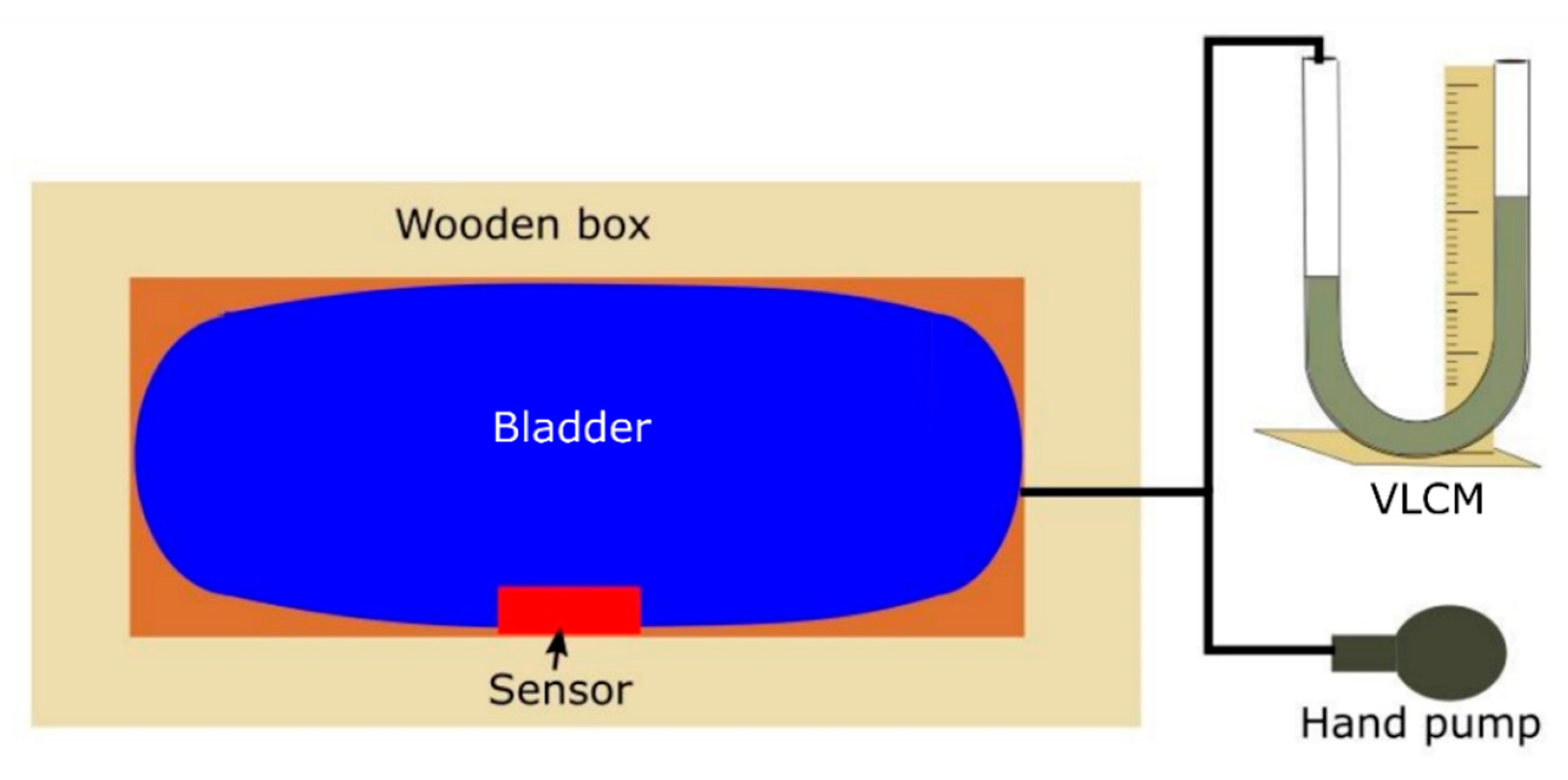
2.3. Validation against the Manometer
2.4. Evaluation of Sensor Performance
3. Results and Discussion
3.1. FlexiForce® Sensor Evaluation
3.2. AMI Air-Pack Sensor Evaluation
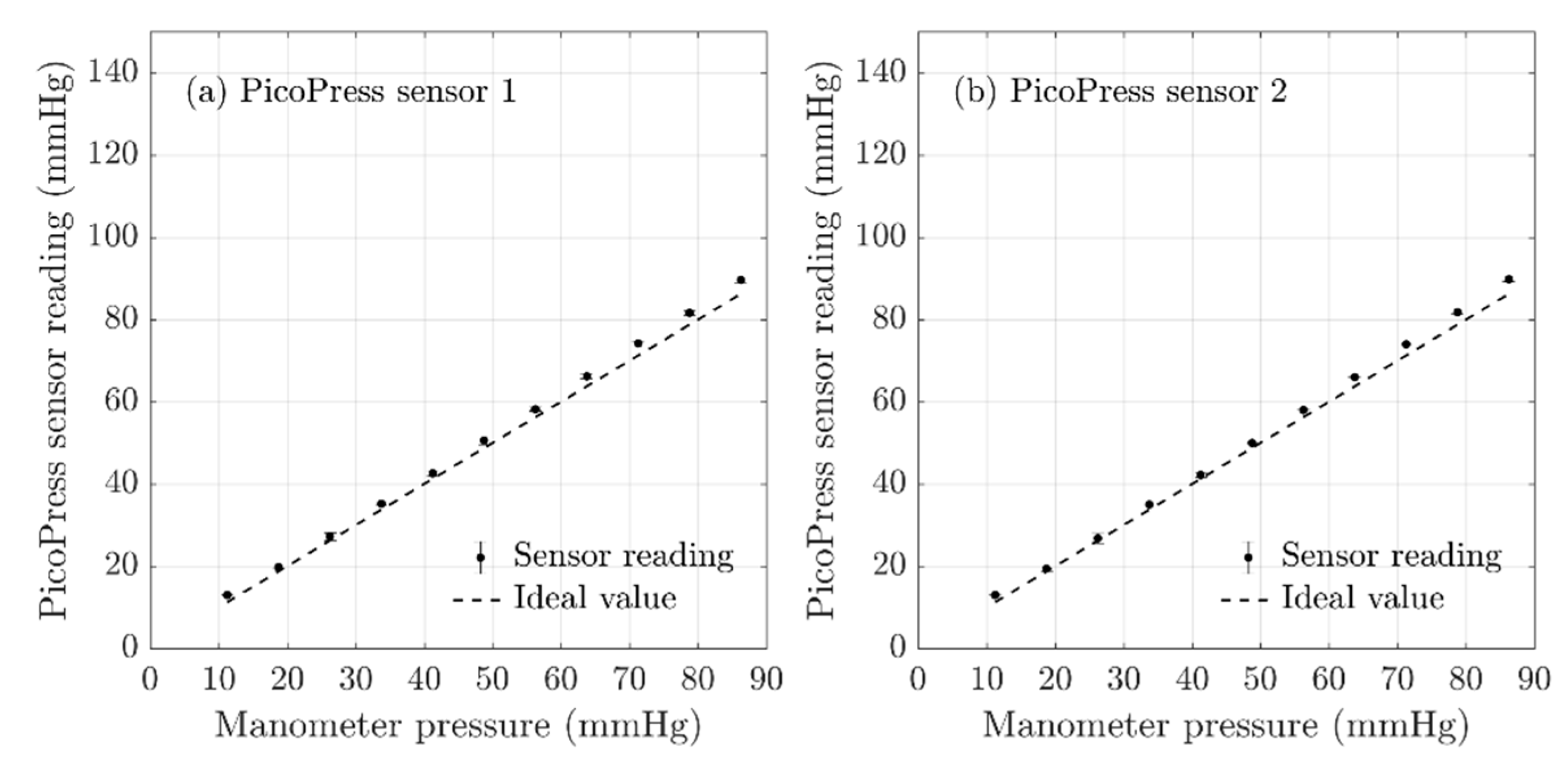
3.3. PicoPress® Sensor Evaluation
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nandasiri, G.K.; Ianakiev, A.; Dias, T. Hyperelastic Properties of Platinum Cured Silicones and its Applications in Active Compression. Polymers 2020, 12, 148. [Google Scholar] [CrossRef] [PubMed]
- Kakkos, S.K.; Timpilis, M.; Patrinos, P.; Nikolakopoulos, K.M.; Papageorgopoulou, C.P.; Kouri, A.K.; Ntouvas, I.; Papadoulas, S.I.; Lampropoulos, G.C.; Tsolakis, I.A. Acute Effects of Graduated Elastic Compression Stockings in Patients with Symptomatic Varicose Veins: A Randomised Double Blind Placebo Controlled Trial. J. Vasc. Surg. 2018, 67, 679. [Google Scholar] [CrossRef][Green Version]
- Attaran, R.R.; Chaar, C.I.O. Compression Therapy in Venous Disease. Curr. Manag. Venous Dis. 2017, 32, 65–74. [Google Scholar] [CrossRef] [PubMed]
- DePopas, E.; Brown, M. Varicose Veins and Lower Extremity Venous Insufficiency. Semin. Interv. Radiol. 2018, 35, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Yamany, A.; Hamdy, B. Effect of sequential pneumatic compression therapy on venous blood velocity, refilling time, pain and quality of life in women with varicose veins: A randomized control study. J. Phys. Ther. Sci. 2016, 28, 1981–1987. [Google Scholar] [CrossRef]
- Zhao, S.; Liu, R.; Fei, C.; Guan, D. Dynamic Interface Pressure Monitoring System for the Morphological Pressure Mapping of Intermittent Pneumatic Compression Therapy. Sensors 2019, 19, 2881. [Google Scholar] [CrossRef]
- Flaud, P.; Bassez, S.; Counord, J.-L. Comparative In Vitro Study of Three Interface Pressure Sensors Used to Evaluate Medical Compression Hosiery. Dermatol. Surg. 2010, 36, 1930–1940. [Google Scholar] [CrossRef]
- Partsch, B.; Partsch, H. Calf compression pressure required to achieve venous closure from supine to standing positions. J. Vasc. Surg. 2005, 42, 734–738. [Google Scholar] [CrossRef]
- Milic, D.J.; Zivic, S.S.; Bogdanovic, D.C.; Jovanovic, M.M.; Jankovic, R.J.; Milosevic, Z.D.; Stamenkovic, D.M.; Trenkic, M.S. The influence of different sub-bandage pressure values on venous leg ulcers healing when treated with compression therapy. J. Vasc. Surg. 2010, 51, 655–661. [Google Scholar] [CrossRef]
- Ferguson-Pell, M.; Hagisawa, S.; Bain, D. Evaluation of a sensor for low interface pressure applications. Med. Eng. Phys. 2000, 22, 657–663. [Google Scholar] [CrossRef]
- Brophy-Williams, N.; Driller, M.; Halson, S.L.; Fell, J.; Shing, C.M. Evaluating the Kikuhime pressure monitor for use with sports compression clothing. Sports Eng. 2013, 17, 55–60. [Google Scholar] [CrossRef]
- Mosti, G.; Rossari, S. The importance of measuring sub bandage pressure and presentation of new measuring device. Acta Vulnol 2008, 6, 31–36. [Google Scholar]
- Damstra, R.J.; Partsch, H. Prospective, randomized, controlled trial comparing the effectiveness of adjustable compression Velcro wraps versus inelastic multicomponent compression bandages in the initial treatment of leg lymphedema. J. Vasc. Surg. Venous Lymphat. Disord. 2013, 1, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Luo, S.; Wang, J.; Shi, H.; Yao, X. A novel approach to characterize dynamic pressure on lower limb wearing compression cycling shorts. J. Text. Inst. 2015, 107, 1–10. [Google Scholar] [CrossRef]
- Liu, R.; Kwok, Y.L.; Li, Y.; Lao, T.T.H.; Zhang, X.; Dai, X.Q. Objective Evaluation of Skin Pressure Distribution of Graduated Elastic Compression Stockings. Dermatol. Surg. 2005, 31, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Kwok, Y.L.; Li, J.-S.; Lao, T.T.; Zhang, X. Skin pressure profiles and variations with body postural changes beneath medical elastic compression stockings. Int. J. Dermatol. 2007, 46, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Dai, D.X. (Eds.) Biomechanical Engineering of Textiles and Clothing; Woodhead Publishing: Cambridge, UK, 2006. [Google Scholar]
- Lai, C.H.; Li-Tsang, C.W. Validation of the Pliance X System in measuring interface pressure generated by pressure garment. Burns 2009, 35, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Partsch, H.; Mosti, G. Comparison of three portable instruments to measure compression pressure. Int. Angiol. 2010, 29, 426. [Google Scholar] [PubMed]
- Al Khaburi, J.; Dehghani-Sanij, A.A.; Nelson, E.A.; Hutchinson, J. Pressure mapping bandage prototype: Development and testing. In Proceedings of the 2012 International Conference on Biomedical Engineering (ICoBE), Penang, Malaysia, 27–28 February 2012; pp. 430–435. [Google Scholar]
- Al Khaburi, J.; Nelson, E.A.; Hutchinson, J.; Dehghani-Sanij, A.A. Impact of multilayered compression bandages on sub-bandage interface pressure: A model. Phlebol. J. Venous Dis. 2011, 26, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Parmar, S.; Khodasevych, I.E.; Troynikov, O. Evaluation of Flexible Force Sensors for Pressure Monitoring in Treatment of Chronic Venous Disorders. Sensors 2017, 17, 1923. [Google Scholar] [CrossRef] [PubMed]
- Al Khaburi, J.; Dehghani-Sanij, A.A.; Nelson, E.A.; Hutchinson, J. Measurement of interface pressure applied by medical compression bandages. In Proceedings of the 2011 IEEE International Conference on Mechatronics and Automation, Beijing, China, 7–10 August 2011; pp. 289–294. [Google Scholar]
- Chi, Y.-W.; Tseng, K.-H.; Li, R.; Pan, T. Comparison of piezoresistive sensor to PicoPress® in in-vitro interface pressure measurement. Phlebol. J. Venous Dis. 2017, 33, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Al Khaburi, J.A.J. Pressure Mapping of Medical Compression Bandages Used for Venous Leg Ulcer Treatment; University of Leeds: Leeds, UK, 2010. [Google Scholar]
- Microlab Electronica. PicoPress® COMPRESSION Measurement System. Available online: http://www.microlabitalia.it/wfolder/filescasehistory/file/11.pdf (accessed on 10 August 2020).
- Hakala, T.T.M.; Puolakka, A.; Nousiainen, P.; Vuorela, T.; Vanhala, J. Application of air bladders for medical compression hosieries. Text. Res. J. 2017, 88, 2169–2181. [Google Scholar] [CrossRef]
- Bentley, J.P. Principles of Measurement Systems, 4th ed.; Pearson Education: Harlow, Essex, UK, 2005. [Google Scholar]
- Fraden, J. Handbook of Modern Sensors: Physics, Designs, and Applications, 3rd ed.; Springer: New York, NY, USA, 2004. [Google Scholar]
- Dunn, P.F.; Davis, M.P. Measurement and Data Analysis for Engineering and Science; CRC Press: Boca Raton, FL, USA, 2017. [Google Scholar]
- Niu, Z.; Zhao, T.; Zhao, Y.; Hu, Q.; Ding, S. Design and Analysis of the Measurement Characteristics of a Bidirectional-Decoupling Over-Constrained Six-Dimensional Parallel-Mechanism Force Sensor. Sensors 2017, 17, 1985. [Google Scholar] [CrossRef] [PubMed]
- Bolton, W. Measurement and Instrumentation Systems; Butterworth-Heinemann: Oxford, UK, 1996. [Google Scholar]
- Tekscan®. FlexiForceTM Standard Model A201. 2018. Available online: https://www.tekscan.com/products-solutions/force-sensors/a201 (accessed on 10 August 2020).
- AMI Techno. Air-Pack Type Contact Surface Pressure Measurement System. 2009. Available online: https://www.ami-tec.co.jp/pdf/e_20sessyoku_20siyou.pdf (accessed on 10 August 2020).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Constant (Peg and Perspex Sheet) Weight (g) | Standard Weight (g) | Total Weight (g) | Force (N) | Pressure (N/mm2) | Pressure (mmHg) |
|---|---|---|---|---|---|
| 3.463 | 20 | 23.463 | 0.2301 | 0.00324 | 24.31 |
| 3.463 | 40 | 43.463 | 0.4363 | 0.006 | 45.03 |
| 3.463 | 50 | 53.463 | 0.5343 | 0.00739 | 55.39 |
| 3.463 | 70 | 73.463 | 0.7205 | 0.01015 | 76.11 |
| 3.463 | 80 | 83.463 | 0.8185 | 0.01153 | 86.48 |
| 3.463 | 100 | 103.463 | 1.0147 | 0.01429 | 107.2 |
| Sensor | Nonlinearity Error (%) | Repeatability Error (%) |
|---|---|---|
| Batch 1 | ||
| Sensor 1 | 15.82 | 7.49 |
| Sensor 2 | 20.86 | 9.51 |
| Sensor 3 | 20.19 | 6.87 |
| Sensor 4 | 13.85 | 6.59 |
| Batch 2 | ||
| Sensor 1 | 2.92 | |
| Sensor 2 | 4.97 | |
| Sensor 3 | 4.98 | |
| Sensor 4 | 4.16 |
| Sensor | Nonlinearity Error (%) | Repeatability Error (%) | Hysteresis Error (%) | Accuracy (mmHg) |
|---|---|---|---|---|
| Batch 1 | ||||
| Sensor 1 | 1.22 | 3.62 | 2.37 | 2.67 |
| Sensor 2 | 0.52 | 1.48 | 1.60 | 1.41 |
| Sensor 3 | 0.64 | 2.60 | 3.39 | 2.65 |
| Sensor 4 | 0.31 | 2.00 | 3.18 | 2.35 |
| Batch 2 | ||||
| Sensor 1 | 1.17 | 2.08 | 2.69 | 2.18 |
| Sensor 2 | 0.97 | 2.08 | 0.91 | 1.53 |
| Sensor 3 | 0.88 | 3.07 | 1.39 | 2.19 |
| Sensor 4 | 1.27 | 2.67 | 1.91 | 2.19 |
| Sensor | Nonlinearity Error (%) | Repeatability Error (%) |
|---|---|---|
| Sensor 1 | 0.57 | 0.84 |
| Sensor 2 | 0.81 | 0.73 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nandasiri, G.K.; Shahidi, A.M.; Dias, T. Study of Three Interface Pressure Measurement Systems Used in the Treatment of Venous Disease. Sensors 2020, 20, 5777. https://doi.org/10.3390/s20205777
Nandasiri GK, Shahidi AM, Dias T. Study of Three Interface Pressure Measurement Systems Used in the Treatment of Venous Disease. Sensors. 2020; 20(20):5777. https://doi.org/10.3390/s20205777
Chicago/Turabian StyleNandasiri, Gayani K., Arash M. Shahidi, and Tilak Dias. 2020. "Study of Three Interface Pressure Measurement Systems Used in the Treatment of Venous Disease" Sensors 20, no. 20: 5777. https://doi.org/10.3390/s20205777
APA StyleNandasiri, G. K., Shahidi, A. M., & Dias, T. (2020). Study of Three Interface Pressure Measurement Systems Used in the Treatment of Venous Disease. Sensors, 20(20), 5777. https://doi.org/10.3390/s20205777