Wireless Body Sensor Communication Systems Based on UWB and IBC Technologies: State-of-the-Art and Open Challenges




Abstract
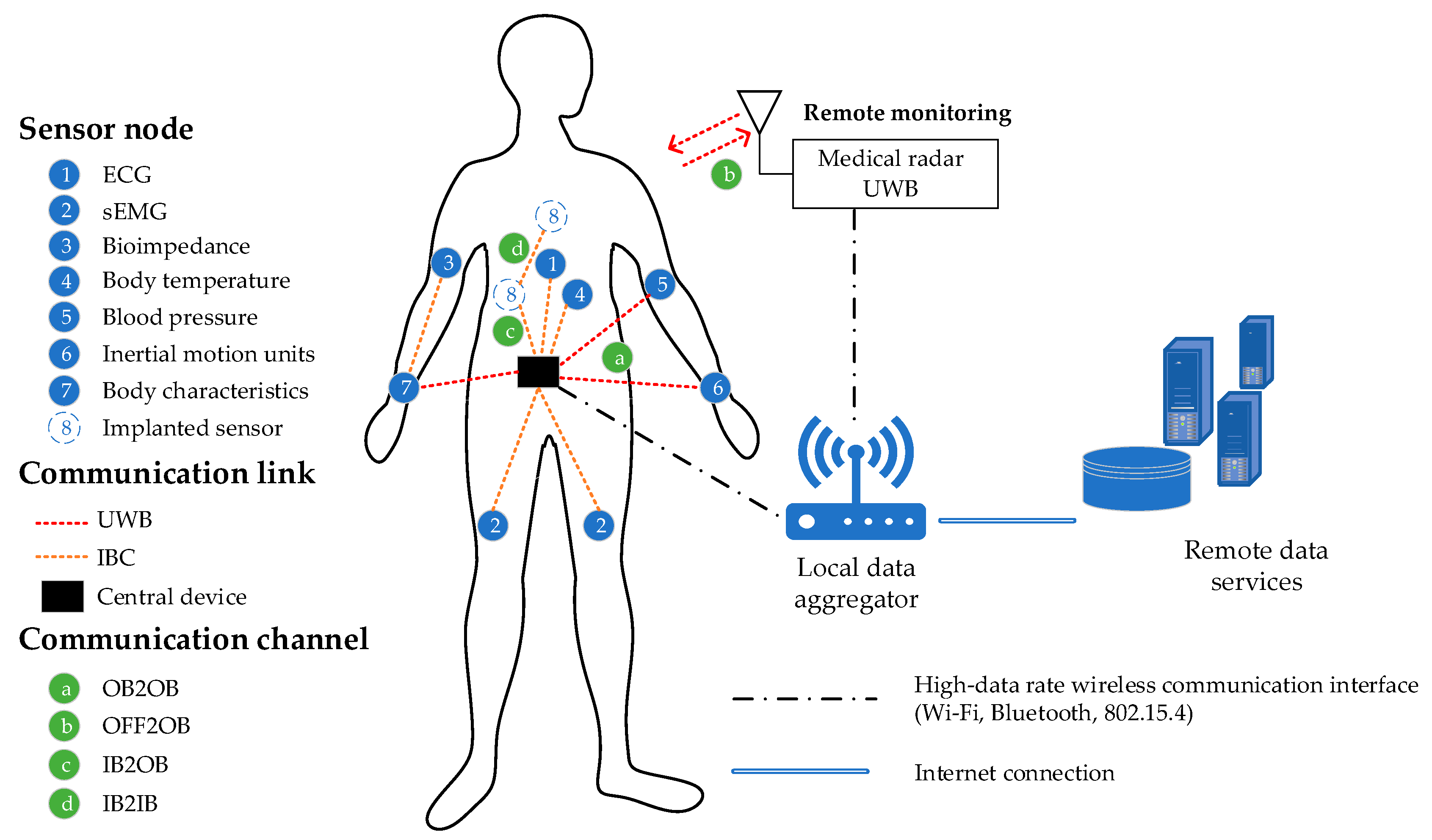
1. Introduction
2. State of the Art: WBAN Communication Systems
2.1. IEEE 802.15.4a Standard (UWB (PHY))
- Sub–GHz: 250–750 MHz
- Low-band: 3.244–4.742 GHz
- Hi-band: 5.944–10.234 GHz
2.2. IEEE 802.15.6 Standard
3. State of the Art: Emerging Technologies for the WBS Applications
3.1. State of the Art: Ultra-Wideband Communication Technology
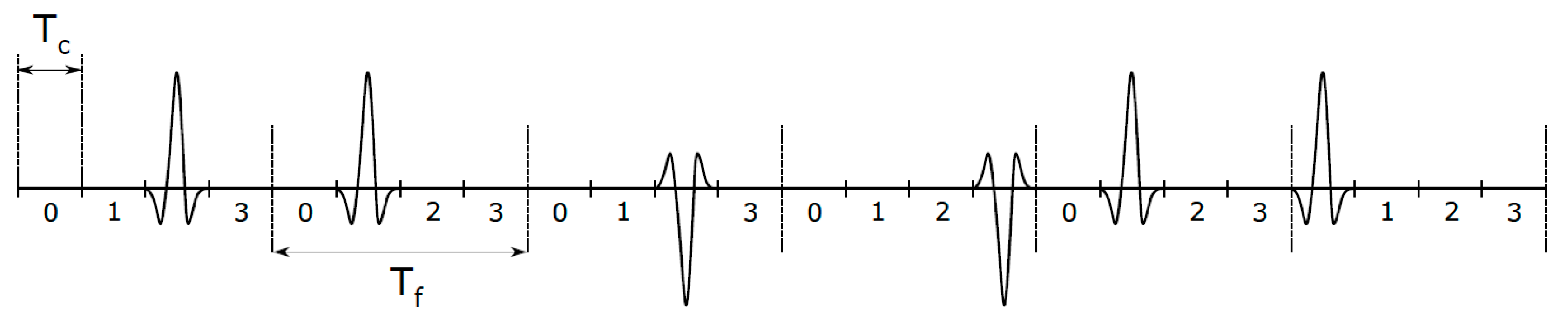
3.1.1. UWB Communication
- better signal penetration through various obstacles (e.g., walls in buildings, human tissues);
- the possibility of achieving high accuracy and precision of radiofrequency positioning due to communication using very narrow pulses in the time domain;
- high-speed data communication;
- low price and consumption.
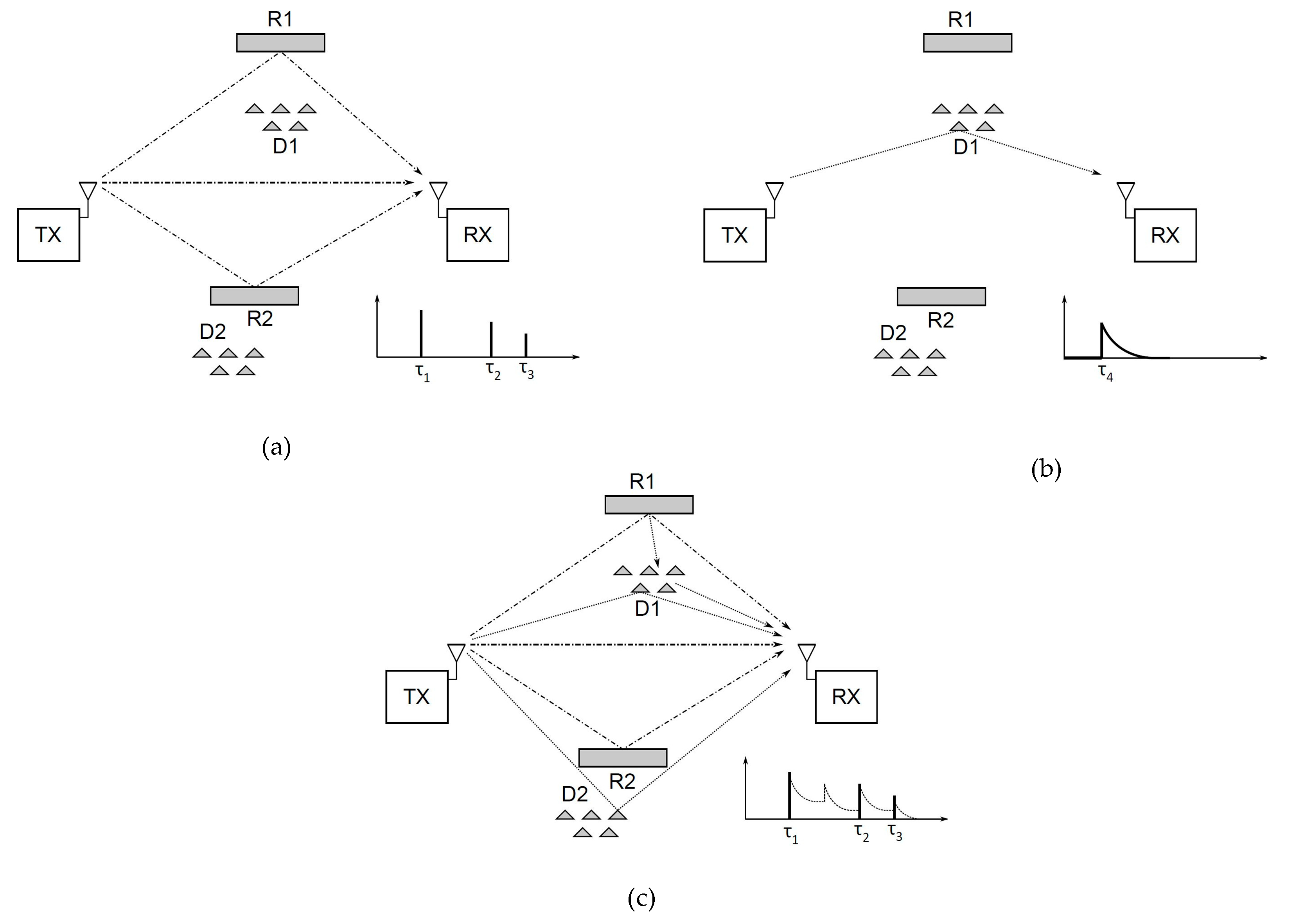
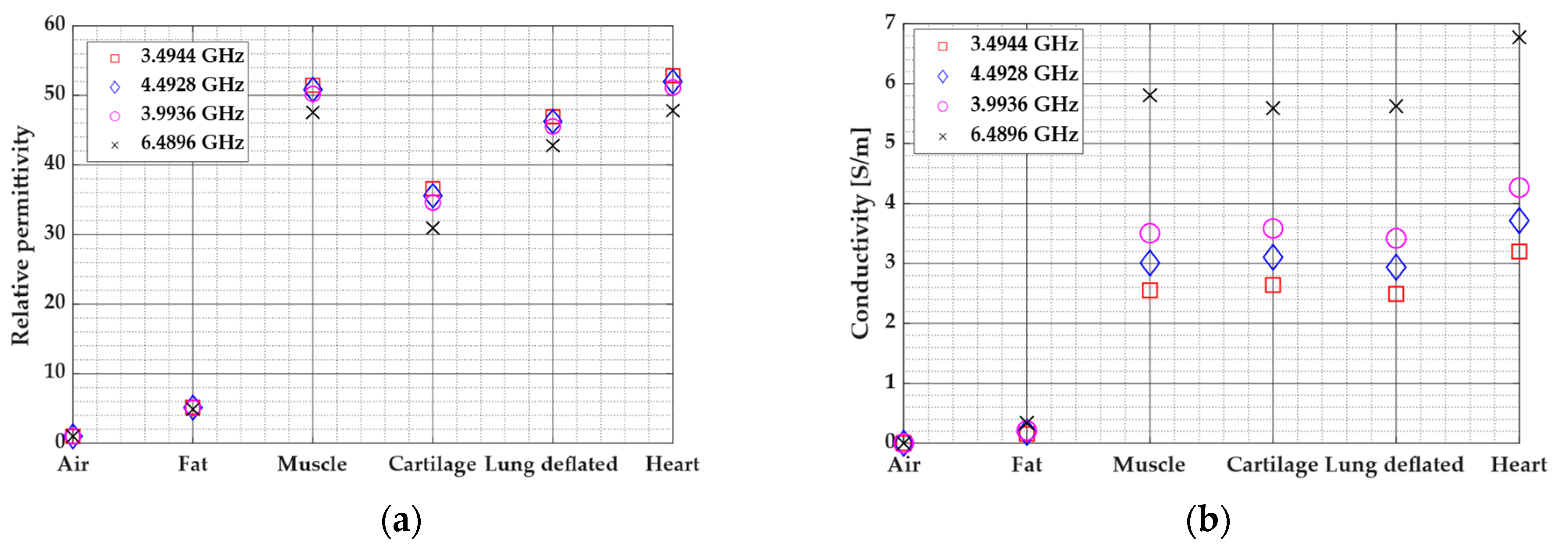
3.1.2. UWB Signal Propagation Modeling
3.1.3. UWB Applications and Systems
UWB Applications in Healthcare
Application of the UWB in Human Motion Tracking
3.2. State of the Art: Intrabody Communication Technology
3.2.1. Measurements of IBC Channel Transmission Characteristics
3.2.2. IBC Channel Modeling and Device Design
3.2.3. Capacitive IBC for Communication with In-Body Devices
4. Comparison, Discussion and Open Challenges: UWB and IBC Technologies
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| BCC | Body channel communication |
| BPM | Burst position modulation |
| BPSK | Binary phase shift keying |
| BS | Base station |
| BT | Bluetooth |
| CIR | Channel impulse response |
| CSS | Chirp spread spectrum |
| DS-CDMA | Direct-Sequence Code Division Multiple Access |
| DS-UWB | Direct-Sequence UWB |
| ECC | European Communication Committee |
| ECG | Electrocardiograph |
| EIRP | Equivalent isotropically radiated power |
| EPI | Electrode polarization impedance |
| EMC | Electromagnetic compatibility |
| EMG | Electromyography |
| FCC | Federal Communications Commission |
| FDTD | Finite difference time-domain |
| FEM | Finite element method |
| GI | Gastrointestinal |
| GPR | Ground penetrating radars |
| HBC | Human body communication |
| HMT | Human motion tracking |
| HR | Heart rate |
| IB2IB | In-body to in-body |
| IB2OB | In-body to on-body |
| IBC | Intrabody communication |
| IEEE | Institute of Electrical and Electronics Engineers |
| IMU | Inertial measurement unit |
| IR-UWB | Impulse radio UWB |
| LOS | Line of sight |
| MAC | Medium Access Control |
| MBOFDM | Multiband orthogonal frequency division multiplexing |
| MB-UWB | multiband UWB |
| MICS | Medical Implant Communication Service |
| MPC | Multipath components |
| NLOS | Non-line of sight |
| OB2OB | On-body to on-body |
| PDP | Power delay profile |
| PHY | Physical layer |
| PL | Path loss |
| PRF | Pulse repetition frequency |
| PSD | Power spectral density |
| QoS | Quality-of-Service |
| RBM | Random body movement |
| RF | Radio frequency |
| RR | Respiration rate |
| RX | Receiver |
| SV | Saleh-Valenzuela |
| TH | Time-hopping |
| TOA | Time of arrival |
| TX | Transmitter |
| UWB | Ultra-wideband |
| WBAN | Wireless body area network |
| WBS | Wireless body sensors |
| WLAN | Wireless LAN |
| WPAN | Wireless personal area networks |
| WSN | Wireless sensor network |
References
- Hall, P.S.; Hao, Y. (Eds.) Antennas and Propagation for Body-Centric Wireless Communications, 1st ed.; Artech House: Massachusetts, MA, USA, 2006. [Google Scholar]
- Arbia, D.B.; Alam, M.M.; Moullec, Y.L.; Hamida, E.B. Communication Challenges in on-Body and Body-to-Body Wearable Wireless Networks—A Connectivity Perspective. Technologies 2017, 5, 43. [Google Scholar] [CrossRef]
- Leelatien, P.; Ito, K.; Saito, K.; Sharma, M.; Alomainy, A. Channel Characteristics and Wireless Telemetry Performance of Transplanted Organ Monitoring System Using Ultrawideband Communication. IEEE J. Electromagn. RF Microw. Med. Biol. 2018, 2, 94–101. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiang, Y.; Zhang, L.Y.; Rong, Y.; Guo, S. Secure Wireless Communications Based on Compressive Sensing: A Survey. IEEE Commun. Surv. Tutor. 2019, 21, 1093–1111. [Google Scholar] [CrossRef]
- Otim, T.; Bahillo, A.; Diez, L.E.; Lopez-Iturri, P.; Falcone, F. Impact of Body Wearable Sensor Positions on UWB Ranging. IEEE Sens. J. 2019, 19, 11449–11457. [Google Scholar] [CrossRef]
- Samal, P.B.; Jack Soh, P.; Zakaria, Z. Compact and Wearable Microstrip-based Textile Antenna with Full Ground Plane Designed for WBAN-UWB 802.15.6 Application. In Proceedings of the 2019 13th European Conference on Antennas and Propagation (EuCAP), Krakow, Poland, 31 March–5 April 2019; pp. 1–4. [Google Scholar]
- Särestöniemi, M.; Kissi, C.; Raez, C.P.; Kumpuniemi, T.; Sonkki, M.; Myllymäki, S.; Hämäläinen, M.; Iinatti, J. Measurement and Simulation Based Study on UWB Channel Characteristics on the Abdomen Area. In Proceedings of the 2019 13th International Symposium on Medical Information and Communication Technology (ISMICT), Oslo, Norway, 8–10 May 2019; pp. 1–6. [Google Scholar]
- Bharadwaj, R.; Koul, S.K. Experimental Analysis of Ultra-Wideband Body-to-Body Communication Channel Characterization in an Indoor Environment. IEEE Trans. Antennas Propag. 2019, 67, 1779–1789. [Google Scholar] [CrossRef]
- Fang, X.; Ramzan, M.; Zhang, Q.; Pérez-Simbor, S.; Wang, Q.; Neumann, N.; Garcia-Pardo, C.; Cardona, N.; Plettemeier, D. Experimental In-Body to On-Body and In-Body to In-Body Path Loss Models of Planar Elliptical Ring Implanted Antenna in the Ultra-Wide Band. In Proceedings of the 2019 13th International Symposium on Medical Information and Communication Technology (ISMICT), Oslo, Norway, 8–10 May 2019; pp. 1–5. [Google Scholar]
- Amir, N.F.; Jusoh, M.; Isa, M.M.; Sabapathy, T.; Al-Bawri, S.S.; Rahim, H.A.; Osman, M.N.; Yasin, M.N. A Flexible UWB Antenna for Wearable Technologies Application. In Proceedings of the 2019 6th International Conference on Space Science and Communication (IconSpace), Johor, Malaysia, 28–30 July 2019; pp. 121–124. [Google Scholar]
- El-Bardan, R.; Malaviya, D.; Di Rienzo, A. On the estimation of respiration and heart rates via an IR-UWB radar: An algorithmic perspective. In Proceedings of the 2017 IEEE International Conference on Microwaves, Antennas, Communications and Electronic Systems (COMCAS), Tel-Aviv, Israel, 13–15 November 2017; IEEE: Tel-Aviv, Israel, 2017; pp. 1–5. [Google Scholar]
- Kjelgard, K.G.; Tommer, M.; Lande, T.S.; Wisland, D.T.; Stoa, S.; Kloboe, L.G.; Edvardsen, T. Heart wall velocity sensing using pulsed radar. In Proceedings of the 2017 IEEE Biomedical Circuits and Systems Conference (BioCAS), Turin, Italy, 19–21 October 2017; IEEE: Turin, Italy, 2017; pp. 1–4. [Google Scholar]
- Naranjo-Hernández, D.; Callejón-Leblic, M.A.; Lučev Vasić, Ž.; Seyedi, M.; Gao, Y.-M. Past Results, Present Trends, and Future Challenges in Intrabody Communication. Wirel. Commun. Mob. Comput. 2018, 2018, 1–39. [Google Scholar] [CrossRef]
- Lučev Vasić, Ž; Gao, Y.; Pun, S.; Mak, P.; Vai, M.; Krois, I.; Cifrek, M. Effect of transmitter and receiver electrodes configurations on the capacitive intrabody communication channel from 100 kHz to 100 MHz. In Proceedings of the 15th International Conference in Biomedical Engineering Proceedings, Singapore, 4–7 December 2013; Goh, J., Ed.; IFMBE Proceedings: Volume 43. Springer: Cham, Switzerland; pp. 613–616. [Google Scholar]
- Callejón, M.A.; Naranjo-Hernández, D.; Reina-Tosina, L.J.; Roa, L.M. A Comprehensive Study Into Intrabody Communication Measurements. Instrum. Meas. IEEE Trans. 2013, 62, 2446–2455. [Google Scholar] [CrossRef]
- Wu, L.-S.; Sakai, J.; Sun, H.-C.; Guo, Y.-X. Matching network to improve the transmission level of capacitive intra-body communication (IBC) channels. In Proceedings of the IEEE MTT-S International Microwave Workshop Series on RF and Wireless Technologies for Biomedical and Healthcare Applications (IMWS-BIO), Singapore, 9–11 December 2013; pp. 1–3. [Google Scholar]
- Gharpurey, R.; Kinget, P. Ultra Wideband: Circuits, Transceivers and Systems; Springer Science & Business Media: Berlin, Germany, 2008; ISBN 978-0-387-69278-4. [Google Scholar]
- Chávez-Santiago, R.; Balasingham, I.; Bergsland, J. Ultrawideband Technology in Medicine: A Survey. J. Electr. Comput. Eng. 2012, 2012, 1–9. [Google Scholar] [CrossRef]
- Kebe, M.; Gadhafi, R.; Mohammad, B.; Sanduleanu, M.; Saleh, H.; Al-Qutayri, M. Human Vital Signs Detection Methods and Potential Using Radars: A Review. Sensors 2020, 20, 1454. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Hong, H.; Zhao, H.; Li, Y.; Gu, C.; Zhu, X. Through-Wall Multiple Targets Vital Signs Tracking Based on VMD Algorithm. Sensors 2016, 16, 1293. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Cho, S.H. A Detailed Algorithm for Vital Sign Monitoring of a Stationary/Non-Stationary Human through IR-UWB Radar. Sensors 2017, 17, 290. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Xu, C.; Yang, Y.; Sun, L.; Cai, Z.; Bai, L.; Clancy, E.; Huang, X. Respiration and Heartbeat Rates Measurement Based on Autocorrelation Using IR-UWB Radar. IEEE Trans. Circuits Syst. II Express Briefs 2018, 65, 1470–1474. [Google Scholar] [CrossRef]
- Yang, Z.; Bocca, M.; Jain, V.; Mohapatra, P. Contactless Breathing Rate Monitoring in Vehicle Using UWB Radar. In Proceedings of the RealWSN’18, New York, NY, USA, 16–19 November 2018. [Google Scholar]
- Schires, E.; Georgiou, P.; Lande, T.S. Vital Sign Monitoring Through the Back Using an UWB Impulse Radar With Body Coupled Antennas. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 292–302. [Google Scholar] [CrossRef]
- Khan, F.; Ghaffar, A.; Khan, N.; Cho, S.H. An Overview of Signal Processing Techniques for Remote Health Monitoring Using Impulse Radio UWB Transceiver. Sensors 2020, 20, 2479. [Google Scholar] [CrossRef] [PubMed]
- Hilger, I.; Dahlke, K.; Rimkus, G.; Geyer, C.; Seifert, F.; Kosch, O.; Thiel, F.; Hein, M.; di Clemente, F.S.; Schwarz, U.; et al. ultraMEDIS—Ultra-Wideband Sensing in Medicine. Ultra-Wideband Radio Technol. Commun. Localization Sens. Appl. 2013. [Google Scholar] [CrossRef]
- Terashima, K.; Yamaguchi, S.; Nagayama, Y.; Hanashima, T.; Moriyama, T.; Tanaka, T.; Tsuchiya, H. Development of UWB Microwave Mammography with Multi-Polarization. In Proceedings of the 2018 Progress in Electromagnetics Research Symposium (PIERS-Toyama), Toyama, Japan, 1–4 August 2018; pp. 1081–1083. [Google Scholar]
- Song, H.; Sasada, S.; Masumoto, N.; Kadoya, T.; Shiroma, N.; Orita, M.; Arihiro, K.; Okada, M.; Kikkawa, T. Detectability of Breast Tumors in Excised Breast Tissues of Total Mastectomy by IR-UWB-Radar-Based Breast Cancer Detector. IEEE Trans. Biomed. Eng. 2019, 66, 2296–2305. [Google Scholar] [CrossRef]
- Ara, P.; Yu, K.; Cheng, S.; Dutkiewicz, E.; Heimlich, M.C. Human Abdomen Path-Loss Modeling and Location Estimation of Wireless Capsule Endoscope Using Round-Trip Propagation Loss. IEEE Sens. J. 2018, 18, 3266–3277. [Google Scholar] [CrossRef]
- Särestöniemi, M.; Pomalaza-Ráez, C.; Kissi, C.; Berg, M.; Hämäläinen, M.; Iinatti, J. WBAN Channel Characteristics Between Capsule Endoscope and Receiving Directive UWB On-Body Antennas. IEEE Access 2020, 8, 55953–55968. [Google Scholar] [CrossRef]
- Chávez-Santiago, R.; Wang, J.; Balasingham, I. The ultra wideband capsule endoscope. In Proceedings of the 2013 IEEE International Conference on Ultra-Wideband (ICUWB), Sydney, Australia, 15–18 September 2013; pp. 72–78. [Google Scholar]
- Cho, H.-S.; Lyu, H.-K.; Park, Y.-J. Noninvasive heartbeat extraction from IR UWB radar signals. In Proceedings of the 2015 International Conference on Information and Communication Technology Convergence (ICTC), Jeju Island, Korea, 28–30 October 2015; pp. 977–980. [Google Scholar]
- Liang, X.; Zhang, H.; Fang, G.; Ye, S.; Gulliver, T.A. An Improved Algorithm for Through-Wall Target Detection Using Ultra-Wideband Impulse Radar. IEEE Access 2017, 5, 22101–22118. [Google Scholar] [CrossRef]
- Lauteslager, T.; Tommer, M.; Lande, T.S.; Constandinou, T.G. Coherent UWB Radar-on-Chip for In-Body Measurement of Cardiovascular Dynamics. IEEE Trans. Biomed. Circuits Syst. 2019, 13, 814–824. [Google Scholar] [CrossRef]
- Jang, J.; Bae, J.; Yoo, H.-J. Understanding Body Channel Communication: A review: From history to the future applications. In Proceedings of the 2019 IEEE Custom Integrated Circuits Conference (CICC), Austin, TX, USA, 14–17 April 2019; pp. 1–8. [Google Scholar]
- Teshome, A.K.; Kibret, B.; Lai, D.T.H. A Review of Implant Communication Technology in WBAN: Progress and Challenges. IEEE Rev. Biomed. Eng. 2019, 12, 88–99. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Mao, J.; Zhao, J.; Yang, H.; Lian, Y. The Role and Challenges of Body Channel Communication in Wearable Flexible Electronics. IEEE Trans. Biomed. Circuits Syst. 2020, 14, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.F.; Chen, X.M.; Liang, B.D.; Chen, Q.X. A Review on Human Body Communication: Signal Propagation Model, Communication Performance, and Experimental Issues. Wirel. Commun. Mob. Comput. 2017, 2017, 1–15. [Google Scholar] [CrossRef]
- Das, D.; Maity, S.; Chatterjee, B.; Sen, S. Enabling Covert Body Area Network using Electro-Quasistatic Human Body Communication. Sci. Rep. 2019, 9, 1–14. [Google Scholar] [CrossRef] [PubMed]
- IEEE Standard for Local and Metropolitan Area Networks—Part 15.6: Wireless Body Area Networks; IEEE: Piscataway, NJ, USA, 2012.
- Lučev, Ž.; Krois, I.; Cifrek, M. A capacitive intrabody communication channel from 100 kHz to 100 MHz. IEEE Trans. Instrum. Meas. 2012, 61, 3280–3289. [Google Scholar] [CrossRef]
- Lučev Vasić, Ž.; Krois, I.; Cifrek, M. Effect of transformer symmetry on intrabody communication channel measurements using grounded instruments. Autom. J. Control Meas. Electron. Comput. Commun. 2016, 57, 15–26. [Google Scholar]
- Sangwan, A.; Bhattacharya, P.P. Wireless Body Sensor Networks: A Review. Int. J. Hybrid Inf. Technol. 2015, 8, 105–120. [Google Scholar] [CrossRef]
- Kiourti, A.; Nikita, K.S. A Review of In-Body Biotelemetry Devices: Implantables, Ingestibles, and Injectables. IEEE Trans. Biomed. Eng. 2017, 64, 1422–1430. [Google Scholar] [CrossRef]
- Hämäläinen, M.; Taparugssanagorn, A.; Tesi, R.; Iinatti, J. Wireless medical communications using UWB. In Proceedings of the 2009 IEEE International Conference on Ultra-Wideband, Vancouver, BC, Canada, 9–11 September 2009; IEEE: Vancouver, BC, Canada, 2009; pp. 485–489. [Google Scholar]
- Lazaro, A.; Girbau, D.; Villarino, R.; Ramos, A. Vital signs monitoring using impulse based UWB signal. In Proceedings of the 2011 41st European Microwave Conference, Manchester, UK, 12–14 October 2011; pp. 135–138. [Google Scholar]
- Yin, W.; Yang, X.; Zhang, L.; Oki, E. ECG Monitoring System Integrated With IR-UWB Radar Based on CNN. IEEE Access 2016, 4, 6344–6351. [Google Scholar] [CrossRef]
- Qi, Y.; Soh, C.B.; Gunawan, E.; Low, K.-S.; Maskooki, A. Using wearable UWB radios to measure foot clearance during walking. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 5199–5202. [Google Scholar]
- Bharadwaj, R.; Swaisaenyakorn, S.; Parini, C.G.; Batchelor, J.; Alomainy, A. Localization of Wearable Ultrawideband Antennas for Motion Capture Applications. IEEE Antennas Wirel. Propag. Lett. 2014, 13, 507–510. [Google Scholar] [CrossRef]
- Qi, Y.; Soh, C.B.; Gunawan, E.; Low, K.-S.; Maskooki, A. A novel approach to joint flexion/extension angles measurement based on wearable UWB radios. IEEE J. Biomed. Health Inform. 2014, 18, 300–308. [Google Scholar] [PubMed]
- Huang, R.; Nie, Z.; Duan, C.; Liu, Y.; Jia, L.; Wang, L. Analysis and Comparison of the IEEE 802.15.4 and 802.15.6 Wireless Standards Based on MAC Layer. In Health Information Science; Yin, X., Ho, K., Zeng, D., Aickelin, U., Zhou, R., Wang, H., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2015; Volume 9085, pp. 7–16. ISBN 978-3-319-19155-3. [Google Scholar]
- Niemelä, V.; Haapola, J.; Hämäläinen, M.; Iinatti, J. An Ultra Wideband Survey: Global Regulations and Impulse Radio Research Based on Standards. IEEE Commun. Surv. Tutor. 2017, 19, 874–890. [Google Scholar] [CrossRef]
- IEEE Standard for Local and Metropolitan Area Networks—Part 15.4: Low-Rate Wireless Personal Area Networks (LR-WPANs); IEEE: New Jersey, NJ, USA, 2011.
- 802154a-2007—IEEE Standard for Information technology—Local and metropolitan area networks—Specific requirements—Part 15.4: Wireless Medium Access Control (MAC) and Physical Layer (PHY) Specifications for Low-Rate Wireless Personal Area Networks (WPANs): Amendment 1: Add Alternate PHYs; IEEE: Piscataway, NJ, USA, 2007; pp. 1–210.
- Karapistoli, E.; Pavlidou, F.-N.; Gragopoulos, I.; Tsetsinas, I. An overview of the IEEE 802.15.4a Standard. IEEE Commun. Mag. 2010, 48, 47–53. [Google Scholar] [CrossRef]
- IEEE 802.15 WPAN Task Group 6 (BAN); IEEE 802.15.6 tutorial; IEEE: Piscataway, NJ, USA, November 2011.
- Joshi, V.; Knoefel, F.; Goubran, R.; El-Tanany, M. Measurement of spontaneous body sway during quiet stand using UWB sensor. In Proceedings of the 2017 IEEE EMBS International Conference on Biomedical Health Informatics (BHI), Orlando, FL, USA, 16–19 February 2017; pp. 281–284. [Google Scholar]
- Nakamura, R.; Hadama, H. Target localization using multi-static UWB sensor for indoor monitoring system. In Proceedings of the 2017 IEEE Topical Conference on Wireless Sensors and Sensor Networks (WiSNet), Phoenix, AZ, USA, 15–18 January 2017; pp. 37–40. [Google Scholar]
- Ghavami, M.; Michael, L.B.; Kohno, R. Ultra Wideband Signals and Systems in Communication Engineering; John Wiley & Sons: Hoboken, NJ, USA, 2007; ISBN 978-0-470-06049-0. [Google Scholar]
- Dai, X.; Zhou, Z.; Zhang, J.J.; Davidson, B. Ultra-wideband radar-based accurate motion measuring: Human body landmark detection and tracking with biomechanical constraints. Sonar Navig. IET Radar 2015, 9, 154–163. [Google Scholar] [CrossRef]
- Novák, D.; Kocur, D.; Demčák, J. Static person detection and localization with estimation of person’s breathing rate using single multistatic UWB radar. In Proceedings of the 2017 IEEE 15th International Symposium on Applied Machine Intelligence and Informatics (SAMI), Herl’any, Slovakia, 26–28 January 2017; pp. 143–148. [Google Scholar]
- Guvenc, I.; Gezici, S.; Sahinoglu, Z. Ultra-wideband range estimation: Theoretical limits and practical algorithms. In Proceedings of the 2008 IEEE International Conference on Ultra-Wideband, Hannover, Germany, 10–12 September 2008; Volume 3, pp. 93–96. [Google Scholar]
- Zekavat, S.; Buehrer, R.M. Handbook of Position Location: Theory, Practice, and Advances; Wiley: Hoboken, NJ, USA, 2011. [Google Scholar]
- Alemaryeen, A.; Noghanian, S.; Fazel-Rezai, R. Antenna Effects on Respiratory Rate Measurement Using a UWB Radar System. IEEE J. Electromagn. RF Microw. Med. Biol. 2018, 2, 87–93. [Google Scholar] [CrossRef]
- Bharadwaj, R.; Swaisaenyakorn, S.; Parini, C.; Batchelor, J.C.; Koul, S.K.; Alomainy, A. UWB Channel Characterization for Compact L-Shape Configurations for Body-Centric Positioning Applications. IEEE Antennas Wirel. Propag. Lett. 2020, 19, 29–33. [Google Scholar] [CrossRef]
- Yan, S.; Soh, P.J.; Vandenbosch, G.A.E. Wearable Ultrawideband Technology—A Review of Ultrawideband Antennas, Propagation Channels, and Applications in Wireless Body Area Networks. IEEE Access 2018, 6, 42177–42185. [Google Scholar] [CrossRef]
- Kumar, V.; Gupta, B. Design Aspects of Body-Worn UWB Antenna for Body-Centric Communication: A Review. Wirel. Pers. Commun. 2017, 97, 5865–5895. [Google Scholar] [CrossRef]
- Risset, T.; Goursaud, C.; Brun, X.; Marquet, K.; Meyer, F. UWB Ranging for Rapid Movement. In Proceedings of the 2018 International Conference on Indoor Positioning and Indoor Navigation (IPIN), Nantes, France, 24–27 September 2018; IEEE: Nantes, France, 2018; pp. 1–8. [Google Scholar]
- Ridolfi, M.; Vandermeeren, S.; Defraye, J.; Steendam, H.; Gerlo, J.; De Clercq, D.; Hoebeke, J.; De Poorter, E. Experimental Evaluation of UWB Indoor Positioning for Sport Postures. Sensors 2018, 18, 168. [Google Scholar] [CrossRef]
- Dove, I. Analysis of Radio Propagation Inside the HumanBody for in-Body Localization Purposes. Master’s Thesis, University of Twente, Enschede, The Netherlands, 2014. [Google Scholar]
- Gabriel, S.; Lau, R.W.; Gabriel, C. The dielectric properties of biological tissues: II. Measurements in the frequency range 10 Hz to 20 GHz. Phys. Med. Biol. 1996, 41, 2251–2269. [Google Scholar] [CrossRef]
- Staderini, E.M. UWB radars in medicine. IEEE Aerosp. Electron. Syst. Mag. 2002, 17, 13–18. [Google Scholar] [CrossRef]
- Lai, C.P.; Narayanan, R.M.; Ruan, Q.; Davydov, A. Hilbert-Huang transform analysis of human activities using through-wall noise and noise-like radar. Sonar Navig. IET Radar 2008, 2, 244–255. [Google Scholar] [CrossRef]
- Leib, M.; Menzel, W.; Schleicher, B.; Schumacher, H. Vital signs monitoring with a UWB radar based on a correlation receiver. In Proceedings of the Fourth European Conference on Antennas and Propagation, Barcelona, Spain, 12–16 April 2010; pp. 1–5. [Google Scholar]
- Baboli, M.; Boric-Lubecke, O.; Lubecke, V. A new algorithm for detection of heart and respiration rate with UWB signals. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 3947–3950. [Google Scholar]
- Nguyen, V.; Javaid, A.Q.; Weitnauer, M.A. Spectrum-averaged Harmonic Path (SHAPA) algorithm for non-contact vital sign monitoring with ultra-wideband (UWB) radar. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 2241–2244. [Google Scholar]
- Lazaro, A.; Girbau, D.; Villarino, R. Techniques for Clutter Suppression in the Presence of Body Movements during the Detection of Respiratory Activity through UWB Radars. Sensors 2014, 14, 2595–2618. [Google Scholar] [CrossRef] [PubMed]
- Brovoll, S.; Berger, T.; Paichard, Y.; Aardal, Ø.; Lande, T.; Hamran, S. Time-lapse imaging of human heart motion with switched array UWB radar. IEEE Trans. Biomed. Circuits Syst. 2014, 8, 704–715. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Jin, T. Short-Range Vital Signs Sensing Based on EEMD and CWT Using IR-UWB Radar. Sensors 2016, 16, 2025. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.; Wang, H.; Naishadham, K.; Kilic, O.; Fathy, A.E. Phase-Based Methods for Heart Rate Detection Using UWB Impulse Doppler Radar. IEEE Trans. Microw. Theory Tech. 2016, 64, 3319–3331. [Google Scholar] [CrossRef]
- Leem, S.K.; Khan, F.; Cho, S.H. Vital Sign Monitoring and Mobile Phone Usage Detection Using IR-UWB Radar for Intended Use in Car Crash Prevention. Sensors 2017, 17, 1240. [Google Scholar] [CrossRef]
- Shyu, K.-K.; Chiu, L.-J.; Lee, P.-L.; Tung, T.-H.; Yang, S.-H. Detection of Breathing and Heart Rates in UWB Radar Sensor Data Using FVPIEF-Based Two-Layer EEMD. IEEE Sens. J. 2019, 19, 774–784. [Google Scholar] [CrossRef]
- Yim, D.; Lee, W.; Kim, J.; Kim, K.; Ahn, D.; Lim, Y.-H.; Cho, S.; Park, H.-K.; Cho, S. Quantified Activity Measurement for Medical Use in Movement Disorders through IR-UWB Radar Sensor. Sensors 2019, 19, 688. [Google Scholar] [CrossRef]
- Kim, S.-H.; Geem, Z.W.; Han, G.-T. A Novel Human Respiration Pattern Recognition Using Signals of Ultra-Wideband Radar Sensor. Sensors 2019, 19, 3340. [Google Scholar] [CrossRef]
- Čuljak, I.; Mihaldinec, H.; Lučev Vasić, Ž; Friganović, K.; Džapo, H.; Cifrek, M. A Contactless Human Respiration Rate Measurement Using UWB Transversal Propagation Method. In Proceedings of the 2019 International Symposium on Antennas and Propagation (ISAP), Xi’an, China, 27–30 October 2019; pp. 1–3. [Google Scholar]
- Wang, G.R.; Han, H.G.; Kim, S.Y.; Kim, T.W. Wireless Vital Sign Monitoring Using Penetrating Impulses. IEEE Microw. Wirel. Compon. Lett. 2017, 27, 94–96. [Google Scholar] [CrossRef]
- Čuljak, I.; Mihaldinec, H.; Kovačić, Z.; Cifrek, M.; Džapo, H. UWB Platform for Vital Signs Detection and Monitoring. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering 2018, Prague, Czech, 3–8 June 2018; Lhotska, L., Sukupova, L., Lacković, I., Ibbott, G.S., Eds.; Springer: Singapore, 2019; pp. 33–37. [Google Scholar]
- Perez-Simbor, S.; Andreu, C.; Garcia-Pardo, C.; Frasson, M.; Cardona, N. UWB Path Loss Models for Ingestible Devices. IEEE Trans. Antennas Propag. 2019, 67, 5025–5034. [Google Scholar] [CrossRef]
- Kissi, C.; Särestöniemi, M.; Pomalaza-Raez, C.; Sonkki, M.; Srifi, M.N. Low-UWB Directive Antenna for Wireless Capsule Endoscopy Localization. In Proceedings of the 13th EAI International Conference on Body Area Networks, Tallinn, Estonia, 21–22 October 2020; Sugimoto, C., Farhadi, H., Hämäläinen, M., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 431–442. [Google Scholar]
- Park, J.; Cho, S.H. IR-UWB radar sensor for human gesture recognition by using machine learning. In Proceedings of the Proceedings—18th IEEE International Conference on High Performance Computing and Communications, 14th IEEE International Conference on Smart City and 2nd IEEE International Conference on Data Science and Systems, HPCC/SmartCity/DSS 2016, Sydney, Australia, 12–14 December 2016; Institute of Electrical and Electronics Engineers Inc.: New Jersey, NJ, USA, 2017; pp. 1246–1249. [Google Scholar]
- Dai, X.; Zhou, Z.; Zhang, J.J.; Davidson, B. Ultra-wideband radar based human body landmark detection and tracking with biomedical constraints for human motion measuring. In Proceedings of the 2014 48th Asilomar Conference on Signals, Systems and Computers, Pacific Grove, CA, USA, 2–5 November 2014; pp. 1752–1756. [Google Scholar]
- Li, J.; Zeng, Z.; Sun, J.; Liu, F. Through-Wall Detection of Human Being’s Movement by UWB Radar. IEEE Geosci. Remote Sens. Lett. 2012, 9, 1079–1083. [Google Scholar] [CrossRef]
- Sharma, M.; Parini, C.; Alomainy, A. UWB Sensor Nodes for Tracking of Human Motion in Medical and Rehabilitation Applications. In Proceedings of the 5th EAI International Conference on Wireless Mobile Communication and Healthcare—“Transforming Healthcare through Innovations in Mobile and Wireless Technologies”, London, UK, 14–16 October 2015; ICST: London, UK, 2015. [Google Scholar]
- Sharma, M.; Parini, C.G.; Alomainy, A. Experimental investigation of 3D localisation of an on-body UWB antenna using several base stations. In Proceedings of the 2014 Loughborough Antennas and Propagation Conference (LAPC), London, UK, 10–11 November 2014; pp. 173–177. [Google Scholar]
- Zihajehzadeh, S.; Yoon, P.K.; Kang, B.-S.; Park, E.J. UWB-Aided Inertial Motion Capture for Lower Body 3-D Dynamic Activity and Trajectory Tracking. IEEE Trans. Instrum. Meas. 2015, 64, 3577–3587. [Google Scholar] [CrossRef]
- Qiu, S.; Liu, L.; Wang, Z.; Li, S.; Zhao, H.; Wang, J.; Li, J.; Tang, K. Body Sensor Network-Based Gait Quality Assessment for Clinical Decision-Support via Multi-Sensor Fusion. IEEE Access 2019, 7, 59884–59894. [Google Scholar] [CrossRef]
- Ashhar, K.; Soh, C.B.; Kong, K.H. Wireless Ultrawideband Sensor Network for Gait Analysis in Rehabilitation Clinics. In Proceedings of the 2018 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Miyazaki, Japan, 7–10 October 2018; pp. 1524–1529. [Google Scholar]
- Mekonnen, Z.W.; Slottke, E.; Luecken, H.; Steiner, C.; Wittneben, A. Constrained maximum likelihood positioning for UWB based human motion tracking. In Proceedings of the 2010 International Conference on Indoor Positioning and Indoor Navigation, Campus Science City (Hoenggerberg), Switzerland, 15–17 September 2010; pp. 1–10. [Google Scholar]
- Yoon, P.K.; Zihajehzadeh, S.; Kang, B.-S.; Park, E.J. Robust Biomechanical Model-Based 3-D Indoor Localization and Tracking Method Using UWB and IMU. IEEE Sens. J. 2017, 17, 1084–1096. [Google Scholar] [CrossRef]
- Zeng, Z.; Liu, S.; Wang, W.; Wang, L. Infrastructure-free indoor pedestrian tracking based on foot mounted UWB/IMU sensor fusion. In Proceedings of the 2017 11th International Conference on Signal Processing and Communication Systems (ICSPCS), Gold Coast, Australia, 13–15 December 2017; pp. 1–7. [Google Scholar]
- Nahar, S.; Phan, T.; Quaiyum, F.; Ren, L.; Fathy, A.E.; Kilic, O. An Electromagnetic Model of Human Vital Signs Detection and Its Experimental Validation. IEEE J. Emerg. Sel. Top. Circuits Syst. 2018, 8, 338–349. [Google Scholar] [CrossRef]
- McEwan, T.E. Body Monitoring and Imaging Apparatus and Method 1996. U.S. Patent 5,573,012, 12 November 1996. [Google Scholar]
- McEwan, T.E. Body Monitoring and Imaging Apparatus and Method 1998. U.S. Patent 5,766,208, 16 June 1998. [Google Scholar]
- Park, J.-K.; Hong, Y.; Lee, H.; Jang, C.; Yun, G.-H.; Lee, H.-J.; Yook, J.-G. Noncontact RF Vital Sign Sensor for Continuous Monitoring of Driver Status. IEEE Trans. Biomed. Circuits Syst. 2019, 13, 493–502. [Google Scholar] [CrossRef]
- Särestöniemi, M.; Pomalaza-Ráez, C.; Berg, M.; Kissi, C.; Hämäläinen, M.; Iinatti, J. UWB-WBAN Radio Channel Characteristics between the Endoscope Capsule and On-body Antenna. In Proceedings of the EAI International Conference on Body Area Networks, Florence, Italy, 2–3 October 2019; Springer: Cham, Switzerland, 2019; pp. 360–373. [Google Scholar]
- Kissi, C.; Särestöniemi, M.; Kumpuniemi, T.; Myllymaki, S.; Sonkki, M.; Mäkelä, J.-P.; Srifi, M.; Jantunen, H.; Pomalaza-Ráez, C. Receiving Uwb Antenna for Wireless Capsule Endoscopy Communications. Prog. Electromagn. Res. 2020, 101, 53–69. [Google Scholar] [CrossRef]
- Han, F.; Liu, H.; Li, B.; Shi, J.; Wang, J. HBC-UWB Channel Modeling for In-body to On-body Communication Link. In Proceedings of the 2019 IEEE 19th International Conference on Communication Technology (ICCT), Xi’an, China, 16–19 October 2019; pp. 1458–1462. [Google Scholar]
- Kumpuniemi, T.; Mäkelä, J.-P.; Hämäläinen, M.; Yazdandoost, K.Y.; Iinatti, J. Measurements and Analysis on Dynamic Off-Body Radio Channels at UWB Frequencies. In Proceedings of the 2019 13th International Symposium on Medical Information and Communication Technology (ISMICT), Oslo, Norway, 8–10 May 2019; pp. 1–5. [Google Scholar]
- Chang, S.; Chu, T.-S.; Roderick, J.; Du, C.; Mercer, T.; Burdick, J.W.; Hashemi, H. UWB human detection radar system: A RF CMOS chip and algorithm integrated sensor. In Proceedings of the 2011 IEEE International Conference on Ultra-Wideband (ICUWB), Bologna, Italy, 14–16 September 2011; pp. 355–359. [Google Scholar]
- Chiang, Y.-Y.; Hsu, W.-H.; Yeh, S.-C.; Li, Y.-C.; Wu, J.-S. Fuzzy support vector machines for device-free localization. In Proceedings of the 2012 IEEE International Instrumentation and Measurement Technology Conference Proceedings, Graz, Austria, 13–16 May 2012; pp. 2169–2172. [Google Scholar]
- Chang, S.; Wolf, M.; Burdick, J.W. Human detection and tracking via Ultra-Wideband (UWB) radar. In Proceedings of the 2010 IEEE International Conference on Robotics and Automation, Anchorage, Alaska, 3–8 May 2010; pp. 452–457. [Google Scholar]
- Bryan, J.; Kim, Y. Classification of human activities on UWB radar using a support vector machine. In Proceedings of the 2010 IEEE Antennas and Propagation Society International Symposium, Toronto, Ontario, Canada, 11–17 July 2010; pp. 1–4. [Google Scholar]
- Bryan, J.D.; Kwon, J.; Lee, N.; Kim, Y. Application of ultra-wide band radar for classification of human activities. Sonar Navig. IET Radar 2012, 6, 172–179. [Google Scholar] [CrossRef]
- Hu, J.; Zhu, G.; Jin, T.; Zhou, Z. Adaptive Through-Wall Indication of Human Target with Different Motions. IEEE Geosci. Remote Sens. Lett. 2014, 11, 911–915. [Google Scholar] [CrossRef]
- Lu, Q.; Liu, C.; Zeng, Z.; Li, J.; Zhang, X. Detection of human’s motions through a wall using UWB radar. In Proceedings of the 2016 16th International Conference on Ground Penetrating Radar (GPR), Hong Kong, China, 13–16 June 2016; pp. 1–4. [Google Scholar]
- Catherwood, P.A.; Scanlon, W.G. Body-centric ultra-wideband multi-channel characterisation and spatial diversity in the indoor environment. Antennas Propag. IET Microw. 2013, 7, 61–70. [Google Scholar] [CrossRef]
- Mokhtari, G.; Zhang, Q.; Hargrave, C.; Ralston, J.C. Non-Wearable UWB Sensor for Human Identification in Smart Home. IEEE Sens. J. 2017, 17, 3332–3340. [Google Scholar] [CrossRef]
- Xu, C.; He, J.; Zhang, X.; Zhou, X.; Duan, S. Towards Human Motion Tracking: Multi-Sensory IMU/TOA Fusion Method and Fundamental Limits. Electronics 2019, 8, 142. [Google Scholar] [CrossRef]
- Kok, M.; Hol, J.D.; Schön, T.B. Using Inertial Sensors for Position and Orientation Estimation; Now: Toronto, ON, Canada, 2017; ISBN 978-1-68083-357-7. [Google Scholar]
- Bharadwaj, R.; Parini, C.; Alomainy, A. Indoor tracking of human movements using UWB technology for motion capture. In Proceedings of the 8th European Conference on Antennas and Propagation (EuCAP 2014), The Hague, The Netherlands, 6–11 April 2014; pp. 2097–2099. [Google Scholar]
- Kok, M.; Hol, J.D.; Schön, T.B. Indoor Positioning Using Ultrawideband and Inertial Measurements. IEEE Trans. Veh. Technol. 2015, 64, 1293–1303. [Google Scholar] [CrossRef]
- Persson, A. Platform Development of Body Area Network for Gait Symmetry Analysis Using IMU and UWB Technology. Master’s Thesis, Mälardalen University, Västerås, Sweden, 2018. [Google Scholar]
- Mekonnen, Z.W.; Wittneben, A. Localization via Taylor series approximation for UWB based human motion tracking. In Proceedings of the Navigation and Communication 2011 8th Workshop on Positioning, Dresden, Germany, 7–8 April 2011; pp. 77–82. [Google Scholar]
- Xu, C.; He, J.; Zhang, X.; Yao, C.; Tseng, P.-H. Geometrical kinematic modeling on human motion using method of multi-sensor fusion. Inf. Fusion 2018, 41, 243–254. [Google Scholar] [CrossRef]
- Xu, C.; He, J.; Zhang, X.; Duan, S.; Yao, C. 3D Localization Performance Evaluation using IMU/TOA Fusion Methods. Int. J. Wirel. Inf. Netw. 2019, 26, 67–79. [Google Scholar] [CrossRef]
- Decawave. Available online: https://www.decawave.com/ (accessed on 29 May 2020).
- Ubisense—Transforming Physical Space into SmartSpace. Available online: https://ubisense.com/ (accessed on 15 June 2020).
- Zihajehzadeh, S.; Park, E.J. A Novel Biomechanical Model-Aided IMU/UWB Fusion for Magnetometer-Free Lower Body Motion Capture. IEEE Trans. Syst. Man Cybern. Syst. 2017, 47, 927–938. [Google Scholar] [CrossRef]
- Humatics—Leading Microlocation Systems for the Industrial World. Available online: https://www.humatics.com/ (accessed on 15 June 2020).
- Blinksight—Accurate Indoor Positioning System. Available online: https://www.blinksight.com/ (accessed on 15 June 2020).
- BeSpoon—Inch-Level Indoor Location Based on Ultra-Wideband Technology. Available online: http://bespoon.com/ (accessed on 15 June 2020).
- Jiménez Ruiz, A.R.; Seco Granja, F. Comparing Ubisense, BeSpoon, and DecaWave UWB Location Systems: Indoor Performance Analysis. IEEE Trans. Instrum. Meas. 2017, 66, 2106–2117. [Google Scholar] [CrossRef]
- Home|Pozyx. Available online: https://www.pozyx.io/ (accessed on 15 June 2020).
- Tong, C.; Tailor, S.A.; Lane, N.D. Are Accelerometers for Activity Recognition a Dead-end? In Proceedings of the 21st International Workshop on Mobile Computing Systems and Applications, Austin, TX, USA, 30–31 March 2020. [Google Scholar]
- Ma, F.; He, J.; Zhang, X. Robust Kalman Filter Algorithm Based on Generalized Correntropy for Ultra-Wideband Ranging in Industrial Environment. IEEE Access 2019, 7, 27490–27500. [Google Scholar] [CrossRef]
- Zeng, Z.; Liu, S.; Wang, L. UWB/IMU integration approach with NLOS identification and mitigation. In Proceedings of the 2018 52nd Annual Conference on Information Sciences and Systems (CISS), Princeton, NJ, USA, 21 March 2018; pp. 1–6. [Google Scholar]
- Macoir, N.; Bauwens, J.; Jooris, B.; Van Herbruggen, B.; Rossey, J.; Hoebeke, J.; De Poorter, E. UWB Localization with Battery-Powered Wireless Backbone for Drone-Based Inventory Management. Sensors 2019, 19, 467. [Google Scholar] [CrossRef] [PubMed]
- Tiemann, J.; Elmasry, Y.; Koring, L.; Wietfeld, C. ATLAS FaST: Fast and Simple Scheduled TDOA for Reliable Ultra-Wideband Localization. In Proceedings of the 2019 International Conference on Robotics and Automation (ICRA), Montreal, QC, Canada, 20–24 May 2019; pp. 2554–2560. [Google Scholar]
- Lian Sang, C.; Adams, M.; Hörmann, T.; Hesse, M.; Porrmann, M.; Rückert, U. Numerical and Experimental Evaluation of Error Estimation for Two-Way Ranging Methods. Sensors 2019, 19, 616. [Google Scholar] [CrossRef] [PubMed]
- Sidorenko, J.; Schatz, V.; Scherer-Negenborn, N.; Arens, M.; Hugentobler, U. Decawave UWB Clock Drift Correction and Power Self-Calibration. Sensors 2019, 19, 2942. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pardo, C.; Fornes-Leal, A.; Cardona, N.; Chávez-Santiago, R.; Bergsland, J.; Balasingham, I.; Brovoll, S.; Aardal, Ø.; Hamran, S.-E.; Palomar, R. Experimental ultra wideband path loss models for implant communications. In Proceedings of the 2016 IEEE 27th Annual International Symposium on Personal, Indoor, and Mobile Radio Communications (PIMRC), Valencia, Spain, 4–7 September 2016; pp. 1–6. [Google Scholar]
- Zhang, Z.; Li, Y.; Mouthaan, K.; Lian, Y. A Miniature Mode Reconfigurable Inductorless IR-UWB Transmitter–Receiver for Wireless Short-Range Communication and Vital-Sign Sensing. IEEE J. Emerg. Sel. Top. Circuits Syst. 2018, 8, 294–305. [Google Scholar] [CrossRef]
- Särestöniemi, M.; Pomalaza-Raez, C.; Berg, M.; Kissi, C.; Hämäläinen, M.; Iinatti, J. In-Body Power Distribution for Abdominal Monitoring and Implant Communications Systems. In Proceedings of the 2019 16th International Symposium on Wireless Communication Systems (ISWCS), Oulu, Finland, 27–30 August 2019; pp. 457–462. [Google Scholar]
- Kissi, C.; Särestöniemi, M.; Kumpuniemi, T.; Sonkki, M.; Myllymäki, S.; Srifi, M.N.; Pomalaza Raez, C. Low-UWB Receiving Antenna for WCE Localization. In Proceedings of the 2019 13th International Symposium on Medical Information and Communication Technology (ISMICT), Oslo, Norway, 8–10 May 2019; pp. 1–6. [Google Scholar]
- Tomlinson, W.J.; Banou, S.; Yu, C.; Stojanovic, M.; Chowdhury, K.R. Comprehensive Survey of Galvanic Coupling and Alternative Intra-Body Communication Technologies. IEEE Commun. Surv. Tutor. 2019, 21, 1145–1164. [Google Scholar] [CrossRef]
- Zhang, K.; Hao, Q.; Song, Y.; Wang, J.; Huang, R.; Liu, Y. Modeling and Characterization of the Implant Intra-Body Communication Based on Capacitive Coupling Using a Transfer Function Method. Sensors 2014, 14, 1740–1756. [Google Scholar] [CrossRef]
- Li, M.; Song, Y.; Wang, G.; Hao, Q.; Zang, K. Characterization of the implantable intra-body communication based on capacitive coupling by transfer function. In Proceedings of the 2016 10th International Conference on Sensing Technology (ICST), Nanjing, China, 11–13 November 2016; pp. 1–5. [Google Scholar]
- Jang, J.; Yoo, H.-J. A Capsule Endoscope System for Wide Visualization Field and Location Tracking. In Proceedings of the 2018 IEEE Biomedical Circuits and Systems Conference (BioCAS), Cleveland, OH, USA, 17–19 October 2018; pp. 1–4. [Google Scholar]
- Jang, J.; Lee, J.; Lee, K.-R.; Lee, J.; Kim, M.; Lee, Y.; Bae, J.; Yoo, H.-J. A Four-Camera VGA-Resolution Capsule Endoscope System With 80-Mb/s Body Channel Communication Transceiver and Sub-Centimeter Range Capsule Localization. IEEE J. Solid-State Circuits 2019, 54, 538–549. [Google Scholar] [CrossRef]
- Li, M.; Song, Y.; Hou, Y.; Li, N.; Jiang, Y.; Sulaman, M.; Hao, Q. Comparable Investigation of Characteristics for Implant Intra-body Communication Based on Galvanic and Capacitive Coupling. IEEE Trans. Biomed. Circuits Syst. 2019, 13, 1747–1758. [Google Scholar] [CrossRef]
- Maity, S.; Nath, M.; Bhattacharya, G.; Chatterjee, B.; Sen, S. On the Safety of Human Body Communication. IEEE Trans. Biomed. Eng. 2020, 1–11. [Google Scholar] [CrossRef]
- Gao, Y.-M.; Zhang, H.; Lin, S.; Jiang, R.-X.; Chen, Z.-Y.; Lučev Vasić, Ž.; Vai, M.-I.; Du, M.; Cifrek, M.; Pun, S.-H. Electrical exposure analysis of galvanic-coupled intra-body communication based on the empirical arm models. Biomed. Eng. OnLine 2018, 17, 1–16. [Google Scholar] [CrossRef]
- Álvarez-Botero, G.A.; Hernández-Gómez, Y.K.; Telléz, C.E.; Coronel, J.F. Human body communication: Channel characterization issues. IEEE Instrum. Meas. Mag. 2019, 22, 48–53. [Google Scholar] [CrossRef]
- Callejón, M.A.; Naranjo-Hernández, D.; Reina-Tosina, L.J.; Roa, L.M. A First Approach to the Harmonization of Intrabody Communications Measurements. In Proceedings of the WC2012 World Congress on Medical Physics and Biomedical Engineering Proceedings, Beijing, China, 26–31 May 2012; Long, M., Ed.; Springer: Berlin/Heidelberg, Germany, 2012; Volume 39, pp. 704–707. [Google Scholar]
- Kibret, B.; Seyedi, M.; Lai, D.T.H.; Faulkner, M. Investigation of Galvanic-Coupled Intrabody Communication Using the Human Body Circuit Model. IEEE J. Biomed. Health Inform. 2014, 18, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Nath, M.; Maity, S.; Sen, S. Towards Understanding the Return Path Capacitance in Capacitive Human Body Communication. IEEE Trans. Circuits Syst. II Express Briefs 2019. [Google Scholar] [CrossRef]
- Zhao, J.; Mao, J.; Zhou, T.; Lai, L.; Yang, H.; Zhao, B. An Auto Loss Compensation System for Non-contact Capacitive Coupled Body Channel Communication. In Proceedings of the 2018 IEEE International Symposium on Circuits and Systems (ISCAS), Florence, Italy, 27–30 May 2018; pp. 1–5. [Google Scholar]
- Callejón, M.A.; Reina-Tosina, L.J.; Naranjo-Hernández, D.; Roa, L.M. Measurement Issues in Galvanic Intrabody Communication: Influence of Experimental Setup. IEEE Trans. Biomed. Eng. 2015, 62, 2724–2732. [Google Scholar] [CrossRef]
- Maity, S.; He, M.; Nath, M.; Das, D.; Chatterjee, B.; Sen, S. BioPhysical Modeling, Characterization and Optimization of Electro-Quasistatic Human Body Communication. IEEE Trans. Biomed. Eng. 2019, 66, 1791–1802. [Google Scholar] [CrossRef]
- Park, J.; Garudadri, H.; Mercier, P.P. Channel Modeling of Miniaturized Battery-Powered Capacitive Human Body Communication Systems. IEEE Trans. Biomed. Eng. 2017, 64, 452–462. [Google Scholar]
- Cho, N.; Yoo, J.; Song, S.-J.; Lee, J.; Jeon, S.; Yoo, H.-J. The human body characteristics as a signal transmission medium for intrabody communication. IEEE Trans. Microw. Theory Tech. 2007, 55, 1080–1086. [Google Scholar] [CrossRef]
- Lučev, Ž.; Krois, I.; Cifrek, M. A capacitive intrabody communication channel from 100 kHz to 100 MHz. In Proceedings of the IEEE Instrumentation and Measurement Technology Conference (I2MTC), Hangzhou, China, 10–12 May 2011; pp. 845–848. [Google Scholar]
- Pereira, M.D.; Álvarez-Botero, G.A.; De Sousa, F.R. Characterization and Modeling of the Capacitive HBC Channel. IEEE Trans. Instrum. Meas. 2015, 64, 2626–2635. [Google Scholar] [CrossRef]
- Wegmüller, M.S.; Oberle, M.; Felber, N.; Kuster, N.; Fichtner, W. Signal Transmission by Galvanic Coupling Through the Human Body. IEEE Trans. Instrum. Meas. 2010, 59, 963–969. [Google Scholar] [CrossRef]
- Lučev Vasić, Ž.; Krois, I.; Hrabar, S.; Cifrek, M. On the Transformer Effects in the Measurements of Capacitive Intrabody Communication Transmission Characteristics Using Grounded Instruments. In Proceedings of the 6th European Conference of the International Federation for Medical and Biological Engineering, Dubrovnik, Croatia, 7–11 September 2014; Lacković, I., Vasić, D., Eds.; Springer International Publishing: Cham, Switzerland, 2014; Volume 45, pp. 260–263. [Google Scholar]
- Sakai, J.; Wu, L.-S.; Sun, H.-C.; Guo, Y.-X. Balun’s effect on the measurement of transmission characteristics for intrabody communication channel. In Proceedings of the Microwave Workshop Series on RF and Wireless Technologies for Biomedical and Healthcare Applications (IMWS-BIO), 2013 IEEE MTT-S International, Singapore, 9–11 December 2013; pp. 1–3. [Google Scholar]
- Xu, R.; Zhu, H.; Yuan, J. Characterization and analysis of intra-body communication channel. In Proceedings of the Antennas and Propagation Society International Symposium (APSURSI ’09), Charleston, South Carolina, 1–5 June 2009; IEEE: Charleston, SC, USA, 2009; pp. 1–4. [Google Scholar]
- Ott, H.W. Noise Reduction Techniques in Electronic Systems, 2nd ed.; John Wiley & Sons: New York, NY, USA, 1988; ISBN 0-471-85068-3. [Google Scholar]
- Cho, H.; Kim, H.; Kim, M.; Jang, J.; Lee, Y.; Lee, K.J.; Bae, J.; Yoo, H.-J. A 79 pJ/b 80 Mb/s Full-Duplex Transceiver and a 42.5 µW 100 kb/s Super-Regenerative Transceiver for Body Channel Communication. IEEE J. Solid-State Circuits 2016, 51, 310–317. [Google Scholar]
- Benarrouch, R.; Thielens, A.; Cathelin, A.; Frappé, A.; Kaiser, A.; Rabaey, J. Capacitive Body-Coupled Communication in the 400–500MHz Frequency Band. In Proceedings of the Body Area Networks: Smart IoT and Big Data for Intelligent Health Management, Florence, Italy, 2–3 October 2019; Mucchi, L., Hämäläinen, M., Jayousi, S., Morosi, S., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 218–235. [Google Scholar]
- Krhač, K.; Sayrafian, K.; Noetscher, G.; Šimunić, D. A Simulation Platform to Study the Human Body Communication Channel. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 4040–4043. [Google Scholar]
- Zhu, X.-Q.; Guo, Y.-X.; Wu, W. Investigation and Modeling of Capacitive Human Body Communication. IEEE Trans. Biomed. Circuits Syst. 2017, 11, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.; Yang, H.; Zhao, B. An Investigation on Ground Electrodes of Capacitive Coupling Human Body Communication. IEEE Trans. Biomed. Circuits Syst. 2017, 11, 910–919. [Google Scholar] [CrossRef]
- Maity, S.; Mojabe, K.; Sen, S. Characterization of Human Body Forward Path Loss and Variability Effects in Voltage-Mode HBC. IEEE Microw. Wirel. Compon. Lett. 2018, 28, 266–268. [Google Scholar] [CrossRef]
- Aliau-Bonet, C.; Pallas-Areny, R. On the effect of body capacitance to ground in tetrapolar bioimpedance measurements. IEEE Trans. Biomed. Eng. 2012, 59, 3405–3411. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, A.-I.; Mizota, T.; Morimura, H.; Yabe, S.; Kikuchi, R.; Suzuki, S.; Matsumoto, R. Extended Noisy-Channel Models for Capacitively Coupled Personal Area Network Under Influence of a Wall. IEEE Trans. Antennas Propag. 2014, 62, 2802–2812. [Google Scholar]
- Zimmerman, T.G. Personal Area Networks (PAN): Near-Field Intra-Body Communication. Master’s Thesis, Massachusetts Institute of Technology, Cambridge, MA, USA, 1995. [Google Scholar]
- Serrano-Finetti, R.E.; Pallas-Areny, R. On the Use of Decoupling Capacitors in Autonomous Sensors. In Proceedings of the IEEE Instrumentation and Measurement Technology Conference (I2MTC) 2007, Warsaw, Poland, 1–3 May 2007; pp. 1–4. [Google Scholar]
- Xu, R.; Ng, W.C.; Zhu, H.; Yuan, J. Equation Environment Coupling and Interference on the Electric-Field Intrabody Communication Channel. IEEE Trans. Biomed. Eng. 2012, 59, 2051–2059. [Google Scholar] [CrossRef] [PubMed]
- Seyedi, M.; Lai, D.T.H. Effect of Limb Joints and Limb Movement on Intrabody Communications for Body Area Network Applications. J. Med. Biol. Eng. JMBE 2014, 34, 276–283. [Google Scholar] [CrossRef]
- Mao, J.; Yang, H.; Lian, Y.; Zhao, B. A Self-Adaptive Capacitive Compensation Technique for Body Channel Communication. IEEE Trans. Biomed. Circuits Syst. 2017, 11, 1001–1012. [Google Scholar] [CrossRef]
- Sasaki, K.; Arai, N.; Muramatsu, D.; Koshiji, F. Evaluation of Ground Loop Through the Floor in Human Body Communication. Int. J. Wirel. Inf. Netw. 2017, 24, 78–90. [Google Scholar] [CrossRef]
- Linnartz, J.-P.M.G. Rules of thumb for predicting path loss in body coupled communication channels. In Proceedings of the 2013 IEEE 20th Symposium on Communications and Vehicular Technology in the Benelux (SCVT), Namur, Belgium, 21 November 2013; pp. 1–6. [Google Scholar]
- Zhao, J.; Sun, W.; Mao, J.; Huang, Y.; Zhao, B.; Liu, Y.; Yang, H. An Auto Loss Compensation System for Capacitive-Coupled Body Channel Communication. IEEE Trans. Biomed. Circuits Syst. 2019, 13, 756–765. [Google Scholar] [CrossRef]
- Tang, T.; Yan, L.; Park, J.H.; Wu, H.; Zhang, L.; Lee, H.Y.B.; Yoo, J. 34.6 EEG Dust: A BCC-Based Wireless Concurrent Recording/Transmitting Concentric Electrode. In Proceedings of the 2020 IEEE International Solid- State Circuits Conference—(ISSCC), San Francisco, CA, USA, 2–6 February 2020; pp. 516–518. [Google Scholar]
- Lee, J.; Jang, J.; Lee, J.; Yoo, H. A battery-less 31 µW HBC receiver with RF energy harvester for implantable devices. In Proceedings of the 2019 IEEE Asian Solid-State Circuits Conference (A-SSCC), Macao, China, 4–6 November 2019; pp. 177–180. [Google Scholar]
- Yuk, B.; Kim, B.; Park, S.; Huh, Y.; Bae, J. An Implantable Body Channel Communication System With 3.7-pJ/b Reception and 34-pJ/b Transmission Efficiencies. IEEE Solid-State Circuits Lett. 2020, 3, 50–53. [Google Scholar] [CrossRef]
- Brumm, J.-C.; Bauch, G. On the Placement of On-Body Antennas for Ultra Wideband Capsule Endoscopy. IEEE Access 2017, 5, 10141–10149. [Google Scholar] [CrossRef]
- Floor, P.A.; Chávez-Santiago, R.; Kim, A.N.; Kansanen, K.; Ramstad, T.A.; Balasingham, I. Communication Aspects for a Measurement Based UWB In-Body to On-Body Channel. IEEE Access 2019, 7, 29425–29440. [Google Scholar] [CrossRef]
- Gao, Y.-M.; Ye, Y.-T.; Lin, S.; Lučev Vasić, Ž.; Vai, M.-I.; Du, M.; Cifrek, M.; Pun, S.-H. Investigation of implantable signal transmission characteristics based on visible data of the human leg. Biomed. Eng. OnLine 2017, 16, 1–14. [Google Scholar] [CrossRef]
- Park, M.J.; Kang, T.; Lim, I.G.; Oh, K.-I.; Kim, S.-E.; Lee, J.-J.; Park, H.-I. Low-Power, High Data-Rate Digital Capsule Endoscopy Using Human Body Communication. Appl. Sci. 2018, 8, 1414. [Google Scholar] [CrossRef]
- Peyman, A.; Gabriel, C. Development and characterisation of tissue equivalent materials for frequency range 30-300 MHz. Electron. Lett. 2007, 43, 19–20. [Google Scholar] [CrossRef]
- Castelló-Palacios, S.; Vallés-Lluch, A.; Garcia-Pardo, C.; Fornes-Leal, A.; Cardona, N. Formulas for easy-to-prepare tailored phantoms at 2.4 GHz ISM band. In Proceedings of the 2017 11th International Symposium on Medical Information and Communication Technology (ISMICT), Lisbon, Portugal, 6–8 February 2017; pp. 27–31. [Google Scholar]
- Chou, C.-K.; Chen, G.-W.; Guy, A.W.; Luk, K.H. Formulas for preparing phantom muscle tissue at various radiofrequencies. Bioelectromagnetics 1984, 5, 435–441. [Google Scholar] [CrossRef]
- Hagmann, M.J.; Levin, R.L.; Calloway, L.; Osborn, A.J.; Foster, K.R. Muscle-equivalent phantom materials for 10–100 MHz. IEEE Trans. Microw. Theory Tech. 1992, 40, 760–762. [Google Scholar] [CrossRef]
- Gabriel, S.; Lau, R.W.; Gabriel, C. The dielectric properties of biological tissues: III. Parametric models for the dielectric spectrum of tissues. Phys. Med. Biol. 1996, 41, 2271–2293. [Google Scholar] [CrossRef]
- Haynes, W.M. , Handbook of Chemistry and Physics, 97th ed.; CRC Press: Boca Raton, FL, USA, 2017; Volume I, ISBN 978-1-138-36729-6. [Google Scholar]
- Khorshid, A.E.; Alquaydheb, I.N.; Eltawil, A.M.; Kurdahi, F.J. Physical Multi-Layer Phantoms for Intra-Body Communications. IEEE Access 2018, 6, 42812–42821. [Google Scholar] [CrossRef]
- Maldari, M.; Albatat, M.; Bergsland, J.; Haddab, Y.; Jabbour, C.; Desgreys, P. Wide frequency characterization of Intra-Body Communication for Leadless Pacemakers. IEEE Trans. Biomed. Eng. 2020, 1–12. [Google Scholar] [CrossRef]
- Lučev Vasić, Ž; Cifrek, M.; Gao, Y.; Du, M. Preliminary Characterization of Capacitive Intrabody Communication Channel under Implantable-Like Conditions. In Proceedings of the IEEE Instrumentation and Measurement Technology Conference (I2MTC2020), Dubrovnik, Croatia, 25–28 May 2020; pp. 1–5. [Google Scholar]
- Gao, Y.M.; Ye, Y.T.; Vai, M.I.; Du, M.; Pun, S.H. Channel modeling and power consumption analysis for galvanic coupling intra-body communication. EURASIP J. Wirel. Commun. Netw. 2016, 2016, 106. [Google Scholar] [CrossRef]
- Filipe, L.; Fdez-Riverola, F.; Costa, N.; Pereira, A. Wireless Body Area Networks for Healthcare Applications: Protocol Stack Review. Int. J. Distrib. Sens. Netw. 2015, 11, 213705. [Google Scholar] [CrossRef]
- Yazdi, F.R.; Hosseinzadeh, M.; Jabbehdari, S. A Review of State-of-the-Art on Wireless Body Area Networks. Int. J. Adv. Comput. Sci. Appl. Ijacsa 2017, 11, 443–455. [Google Scholar]
- Al-Janabi, S.; Al-Shourbaji, I.; Shojafar, M.; Shamshirband, S. Survey of main challenges (security and privacy) in wireless body area networks for healthcare applications. Egypt. Inform. J. 2017, 18, 113–122. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Author Year | Ref | Parameter | Method | UWB System (Frequency) | Application Scenario | Accuracy (Limitation) |
|---|---|---|---|---|---|---|
| Nguyen, 2014 | [76] | HR, RR | SHAPA algorithm | IR-UWB radar Central freq. 4.1 GHz | Eight subjects, lying on the top of a mattress | Practical for a real-time system |
| Brovoll, 2014 | [78] | Human Heart Motion | Time-lapse imaging | Switched Array UWB r. 0.75–2.27 GHz | Antenna was aligned with the body | The subject was holding his breath |
| Hu, 2016 | [79] | HR, RR | EEMD;CWT | IR-UWB radar Central freq. 6.8 GHz | Sitting in a chair and breathing regularly | SNR of RR and HR improved by 7.59 dB and 4.82 dB |
| Ren, 2016 | [80] | HR | Phase-Based | UWB Impulse Doppler r. 1.5–4.5 GHz | Subject sat still in front of the radar system | CSD and AD heart rate deviation is 2.6% and operating rate is 0.8 m |
| Yin, 2016 | [47] | HR | Cascade CNN | NVA-R661 IR-UWB radar module | HR analysis by combination of the ECG and radar | Results accuracy of 88.89% in the slight motion state |
| Shy, 2018 | [82] | HR, RR | FVPIEF based 2-Layer EEMD | UWB radar Central freq. 4.3 GHz | Simultaneously analysis of RR and HR | Relatively accurately |
| Shen,2018 | [22] | HR, RR Subject location | Autocorr. VMD; FFT | PulsOn410 UWB radar Center freq. 4.3 GHz | Vital signs monitoring | Potential implemention in integrated circuits and embedded systems |
| Yim, 2019 | [83] | HR Subject position | CFAR algorithm | XK300-MVI radar 7.29–8.748 GHz | Clinical application | Quantified index to clinically record |
| Kim, 2019 | [84] | RR | 1D CNN model | UWB radar 3–4 GHz | Eupnea, bradypnea, tachypnea, apnea, and motion classification | Average recognition rate of respiration patterns 93.9% |
| 1st Author Year | Ref | Application | System | Frequency Band | Data Rate | Features |
|---|---|---|---|---|---|---|
| Garcia-Pardo, 2016 | [141] | UWB path loss models and channel measurements for IB2OB and IB2OFF communication scenarios | Two UWB omnidirectional patch antennas | 3.1–8.5 GHz | 20001 frequency points | Practical estimation of UWB transmissions path loss from wireless devices implanted in the abdominal cavity to an external unit Implantable application |
| Kjelgård, 2017 | [12] | Heart Wall Velocity Sensing | Body coupled antennas, RF-amplifiers, core radar processor (Novelda X2) | Center freq. 4 GHz | >35 GS/s | Good correlation with tissue doppler ultrasound and microwave radar |
| Leelatien, 2018 | [3] | Wireless monitoring of transplanted organs (liver) | A low-profile tapered UWB antenna with vertical polarization | 4.5–6.5 GHz | 10 Mb/s | Attenuation variation 30 dB (with respect to 40 mm largest organ movement distance) due to respiration-induced organ movement |
| Schires, 2018 | [24] | Through the back vital signs monitoring | UWB Novelda Xethru X2 chip with body coupled antennas | 3.8–9 GHz | 65 frames per second | High accuracy of back monitoring of vital sign using a pulsed radar mounted into a car seat |
| Zhang, 2018 | [142] | Vital signs radar sensing and short-range communication and | CMOS IR – UWB radar and communication interface | BW = 5.6 | 10 Mb/s | Power consumption 6.4 mW and sensitivity −64 dBm at 10 Mb/s |
| Perez-Simbor, 2019 | [88] | Wireless capsule endoscopy | Quasi-omnidirectional antenna | 3.1–8.5 GHz (phantom) 3.1–6 GHz (in-vivo) | Resolution point:3201 | Study of the path loss using simulations, phantoms, and in-vivo measurements |
| Han, 2019 | [107] | In-body to on-body links | HBC-UWB signals Simulation | 10–50 MHz | Combination of HBC and UWB band signal, better high data rate | |
| Lauteslager, 2019 | [34] | Measurement of Cardiovascular Dynamics | UWB Xethru X2 single-chip radar in combination with body coupled antennas | BW = 2.5 GHz | 64 frames per second | High accuracy |
| Särestöniemi, 2019 | [7] | Human abdomen area UWB on-body radio channel characteristics | UWB on body antenna (measurements conducted in an anechoic chamber) | 3.75–4.25 GHz | If the antenna separation distance is large on-body channel characteristics vary significantly depending on the body size and shape | |
| Fang, 2019 | [9] | Channel modeling inside a UWB liquid phantom for wireless capsule endoscopy | Planar elliptical ring implanted IB antenna Semicircle monopole OB antenna | 3.1–5.1 GHz | Frequency point 1601 | Proposed models confirm the agreement with the radiation performance of the designed in-body antenna |
| Song, 2019 | [28] | Breast tumors detection | CMOS-IC portable IR-UWB-radar | 0.5–20 GHz | 100 G Sample/s | Results: IR-UWB radar-based detector has a potential for early-stage breast cancers detection |
| Kumpuniemi, 2019 | [108] | Dynamic off-body on UWB frequencies radio channels measurements | Two planar prototype (dipole and double loop) antennas Six on-body antenna locations, one off-body site | 2–8 GHz | 1601 points in the band | Mean path losses varied between 47.6–69.4 dB (average distance of 2 m) |
| Särestöniemi, 2020 | [30] | UWB radio channel characteristics study between a capsule endoscope and a directive on-body antenna in different parts of the small intestine | In-body omnidirectional dipole antenna (capsule model) from [143] Two on-body directive low-band UWB antennas from [106,144] | In-body antenna 4 GHz On-body antennas 3.75–4.25 GHz | Radio channel characteristics varied significantly depending on the capsule model and on-body antennas location Investigation of the power flow: influence of the cavity sizes |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Čuljak, I.; Lučev Vasić, Ž.; Mihaldinec, H.; Džapo, H. Wireless Body Sensor Communication Systems Based on UWB and IBC Technologies: State-of-the-Art and Open Challenges. Sensors 2020, 20, 3587. https://doi.org/10.3390/s20123587
Čuljak I, Lučev Vasić Ž, Mihaldinec H, Džapo H. Wireless Body Sensor Communication Systems Based on UWB and IBC Technologies: State-of-the-Art and Open Challenges. Sensors. 2020; 20(12):3587. https://doi.org/10.3390/s20123587
Chicago/Turabian StyleČuljak, Ivana, Željka Lučev Vasić, Hrvoje Mihaldinec, and Hrvoje Džapo. 2020. "Wireless Body Sensor Communication Systems Based on UWB and IBC Technologies: State-of-the-Art and Open Challenges" Sensors 20, no. 12: 3587. https://doi.org/10.3390/s20123587
APA StyleČuljak, I., Lučev Vasić, Ž., Mihaldinec, H., & Džapo, H. (2020). Wireless Body Sensor Communication Systems Based on UWB and IBC Technologies: State-of-the-Art and Open Challenges. Sensors, 20(12), 3587. https://doi.org/10.3390/s20123587