Using New Camera-Based Technologies for Gait Analysis in Older Adults in Comparison to the Established GAITRite System

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Apparatus
- (1)
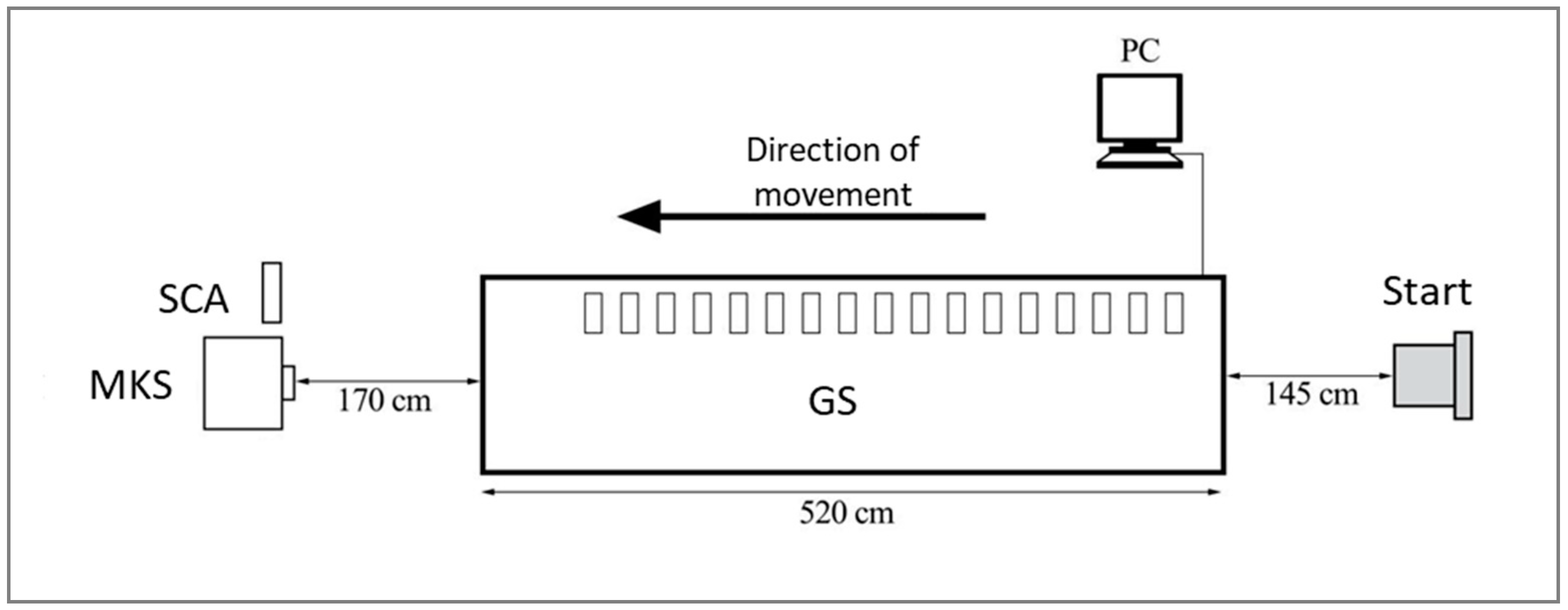
- GS: GAITRite is a 5.2 m long (active length 4.27 m) and 90 cm wide (active wide 61 cm) carpet with 16,128 embedded sensors in a grid. The sensors are placed at a distance of 1.27 cm and are activated by mechanical pressure. GS allows the measurement of different temporal (e.g., step time, velocity, single/double support) and spatial (e.g., step length, stride length, distance) parameters. The carpet is connected to a computer via an interface cable. Prior to the gait analysis, the participant’s age, weight, height, and leg length (right and left) had to be entered manually. The validity of GS was previously investigated in several studies [7,12,13] and used as gold standard in the presented study.
- (2)
- MKS: Motognosis Labs is software developed for the motor assessment of patients with neurodegenerative diseases [14] using a consumer 3D camera (Microsoft Kinect V2) to collect depth silhouettes of individuals (visual perceptive computing). The Software Development Kit of Microsoft (SDK V14.09) uses artificial intelligence to locate 25 different anatomical landmarks [15], which are then used by the software to calculate movement kinematics similar to GS. The system was placed at the end of GS with 1.7 m distance to the edge of the carpet. The measurement range of the system is up to 4.5 m, limiting the area covered by GS and MKS to approximately 3 m.
- (3)
- SCA: The smartphone application conducts gait analysis by recording a video of the subject with a 2D smartphone camera and an underlying algorithm. Within the smartphone application participants’ age, sex, height, and weight must be entered. SCA applies the recent advances of artificial intelligence to the problem of human pose estimation. Using a 2D smartphone camera and a deep convolutional neural net, the application estimates a 3D skeletal model based on a video of a person walking. The underlying algorithm was developed using the VNect algorithm (3D joint and skeleton detection). The VNect algorithm is a real-time method, which captures the full global 3D skeletal pose of human using a single RGB camera [16]. SCA was installed on a Nexus 5 smartphone (Android).
2.2. Procedure
2.3. Data Analysis
3. Results
3.1. Subjects
3.2. Concurrent Validity
3.3. Intertrial Repeatability
4. Discussion
5. Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (Ed.) WHO Global Report on Falls Prevention in Older Age; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Rapp, K.; Freiberger, E.; Todd, C.; Klenk, J.; Becker, C.; Denkinger, M.; Scheidt-Nave, C.; Fuchs, J. Fall incidence in Germany: Results of two population-based studies, and comparison of retrospective and prospective falls data collection methods. BMC Geriatr. 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Pericie, I. Sturzprävention im Krankenhaus und Pflegeheim. Trauma Berufskrankh. 2012, 14, 222–223. [Google Scholar] [CrossRef]
- Springer, S.; Seligmann, G.Y. Validity of the Kinect for Gait Assessment: A Focused Review. Sensors 2016, 16, 194. [Google Scholar] [CrossRef] [PubMed]
- Aboutorabi, A.; Arazpour, M.; Bahramizadeh, M.; Hutchins, S.W.; Fadayevatan, R. The effect of aging on gait parameters in able-bodied older subjects: A literature review. Aging Clin. Exp. Res. 2016, 28, 393–405. [Google Scholar] [CrossRef] [PubMed]
- Verghese, J.; Holtzer, R.; Lipton, R.B.; Wang, C. Quantitative Gait Markers and Incident Fall Risk in Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Bilney, B.; Morris, M.; Webster, K. Concurrent related validity of the GAITRite walkway system for quantification of the spatial and temporal parameters of gait. Gait Posture 2003, 17, 68–74. [Google Scholar] [CrossRef]
- Auvinet, E.; Multon, F.; Aubin, C.E.; Meunier, J.; Raison, M. Detection of gait cycles in treadmill walking using a Kinect. Gait Posture 2015, 41, 722–725. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; McGorry, R.W.; Chou, L.S.; Lin, J.H.; Chang, C.C. Accuracy of the Microsoft Kinect for measuring gait parameters during treadmill walking. Gait Posture 2015, 42, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Baldewijns, G.; Verheyden, G.; Vanrumste, B.; Croonenborghs, T. Validation of the kinect for gait analysis using the GAITRite walkway. In Proceedings of the 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 5920–5923. [Google Scholar] [CrossRef]
- Clark, R.A.; Bower, K.J.; Mentiplay, B.F.; Paterson, K.; Pua, Y.H. Concurrent validity of the Microsoft Kinect for assessment of spatiotemporal gait variables. J. Biomech. 2013, 46, 2722–2725. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Wittwer, J.E.; Feller, J.A. Validity of the GAITRite® walkway system for the measurement of averaged and individual step parameters of gait. Gait Posture 2005, 22, 317–321. [Google Scholar] [CrossRef] [PubMed]
- McDonough, A.L.; Batavia, M.; Chen, F.C.; Kwon, S.; Ziai, J. The validity and reliability of the GAITRite system’s measurements: A preliminary evaluation. Arch. Phys. Med. Rehabil. 2001, 82, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Behrens, J.R.; Mertens, S.; Krüger, T.; Grobelny, A.; Otte, K.; Mansow-Model, S.; Gusho, E.; Paul, F.; Brandt, A.U.; Schmitz-Hübsch, T. Validity of visual perceptive computing for static posturography in patients with multiple sclerosis. Mult. Scler. J. 2016, 22, 1596–1606. [Google Scholar] [CrossRef] [PubMed]
- Otte, K.; Kayser, B.; Mansow-Model, S.; Verrel, J.; Paul, F.; Brandt, A.U.; Schmitz-Hübsch, T. Accuracy and Reliability of the Kinect Version 2 for Clinical Measurement of Motor Function. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Mehta, D.; Sridhar, S.; Sotnychenko, O.; Rhodin, H.; Shafiei, M.; Seidel, H.P.; Xu, W.; Casas, D.; Theobalt, C. VNect. ACM Trans. Graph. 2017, 36, 1–14. [Google Scholar] [CrossRef]
- Finkbiner, M.J.; Gaina, K.M.; McRandall, M.C.; Wolf, M.M.; Pardo, V.M.; Reid, K.; Adams, B.; Galen, S.S. Video Movement Analysis Using Smartphones (ViMAS): A Pilot Study. J. Vis. Exp. 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- Manor, B.; Yu, W.; Zhu, H.; Harrison, R.; Lo, O.Y.; Lipsitz, L.; Travison, T.; Pascual-Leone, A.; Zhou, J. Smartphone App–Based Assessment of Gait During Normal and Dual-Task Walking: Demonstration of Validity and Reliability. JMIR Mhealth Uhealth 2018, 6, e36. [Google Scholar] [CrossRef] [PubMed]
- Niijima, A.; Mizuno, O.; Tanaka, T. A study of gait analysis with a smartphone for measurement of hip joint angle. In Proceedings of the Signal and Information Processing Association Annual Summit and Conference (APSIPA), 2014 Asia-Pacific, Siem Reap, Cambodia, 9–12 December 2014; pp. 1–4. [Google Scholar] [CrossRef]


{kind=link}
| Total | Female | Male | |
|---|---|---|---|
| N | 44 | 22 | 22 |
| Age [Mean ± SD, years] | 73.9 ± 6.1 | 74.1 ± 6.1 | 73.7 ± 6.2 |
| Height [Mean ± SD, cm] | 168.8 ± 8.9 | 162.4 ± 6.2 | 175.1 ± 6.2 |
| Weight [Mean ± SD, kg] | 76.2 ± 15.5 | 68.3 ± 14.0 | 84.1 ± 12.8 |
| Leg length right [Mean ± SD, cm] | 90.1 ± 5.4 | 87.4 ± 4.9 | 92.8 ± 4.6 |
| Leg length left [Mean ± SD, cm] | 89.9 ± 5.5 | 87.1 ± 5.2 | 92.7 ± 4.5 |
| GS | MKS | SCA | GS-MKS | GS-SCA | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Diff [95% CI] | t-Test p-Value | Pearson Corr. | ICC(2,k) | Diff [95% CI] | t-Test p-Value | Pearson Corr. | ICC(2,k) | ||
| Preferred speed | Gait speed [cm/s] | 120.69 (19.90) | 116.69 (19.04) | 122.05 (24.81) | 4.01 [3.14; 4.88] | 0.000 | 0.988 | 0.981 | −0.44 [−7.89; 7.02] | 0.906 | 0.275 | 0.434 |
| Cadence [steps/min] | 111.90 (8.72) | 111.75 (12.23) | 155.51 (23.86) | −1.16 [−2.81; 0.49] | 0.162 | 0.876 | 0.925 | −42.23 [−48.25; −36.21] | 0.000 | 0.078 | 0.020 | |
| Step length, left [cm] | 64.73 (7.78) | 62.45 (8.00) | 51.94 (25.04) | 1.99 [1.16; 2.82] | 0.000 | 0.952 | 0.958 | 14.79 [10.15; 19.43] | 0.000 | 0.316 | 0.233 | |
| Step length, right [cm] | 65.04 (7.92) | 62.38 (8.94) | 60.10 (41.84) | 2.59 [1.67; 3.51] | 0.000 | 0.946 | 0.941 | 8.35 [2.77; 13.93] | 0.004 | 0.413 | 0.394 | |
| Step time, left [s] | 0.54 (0.05) | 0.55 (0.08) | 0.62 (0.24) | −0.01 [−0.02; 0.01] | 0.307 | 0.887 | 0.921 | −0.08 [−0.13; −0.03] | 0.004 | 0.295 | 0.222 | |
| Step time, right [s] | 0.54 (0.04) | 0.53 (0.06) | 0.67 (0.39) | 0.01 [0.01; 0.02] | 0.003 | 0.857 | 0.903 | −0.10 [−0.17; −0.03] | 0.004 | 0.158 | 0.090 | |
| Fast speed | Gait speed [cm/s] | 164.80 (23.40) | 158.70 (22.20) | 143.60 (37.00) | 5.76 [2.59; 8.93] | 0.001 | 0.904 | 0.922 | 19.31 [9.86; 28.77] | 0.000 | 0.424 | 0.494 |
| Cadence [steps/min] | 132.70 (10.20) | 129.60 (14.80) | 177.50 (28.60) | −2.16 [−4.77; 0.45] | 0.097 | 0.876 | 0.904 | −46.09 [−52.43; −39.74] | 0.000 | 0.409 | 0.119 | |
| Step length, left [cm] | 74.50 (9.30) | 72.30 (10.40) | 79.60 (52.50) | 1.42 [−0.28; 3.12] | 0.095 | 0.910 | 0.947 | −2.72 [−12.10; 6.65] | 0.560 | 0.466 | 0.389 | |
| Step length, right [cm] | 74.10 (8.60) | 70.00 (10.20) | 68.20 (30.30) | 1.43 [0.30; 2.56] | 0.016 | 0.958 | 0.971 | 2.31 [−3.73; 8.35] | 0.442 | 0.342 | 0.415 | |
| Step time, left [s] | 0.45 (0.03) | 0.47 (0.05) | 0.54 (0.22) | 0.01 [0.00; 0.03] | 0.101 | 0.845 | 0.811 | −0.06 [−0.10; −0.01] | 0.013 | 0.267 | 0.176 | |
| Step time, right [s] | 0.45 (0.03) | 0.46 (0.06) | 0.61 (0.45) | 0.00 [−0.02; 0.02] | 0.873 | 0.884 | 0.864 | −0.09 [−0.15; −0.03] | 0.006 | −0.137 | −0.077 | |
| GS | MKS | SCA | |||||
|---|---|---|---|---|---|---|---|
| SEM | ICC(1,1) | SEM | ICC(1,1) | SEM | ICC(1,1) | ||
| Preferred speed | Gait speed [cm/s] | 1.739 | 0.816 | 1.664 | 0.823 | 2.219 | 0.535 |
| Cadence [steps/min] | 0.768 | 0.834 | 1.136 | 0.574 | 2.134 | 0.298 | |
| Step length, left [cm] | 0.685 | 0.854 | 0.749 | 0.843 | 2.258 | 0.125 | |
| Step length, right [cm] | 0.697 | 0.860 | 0.849 | 0.646 | 3.758 | 0.225 | |
| Step time, left [s] | 0.004 | 0.826 | 0.008 | 0.453 | 0.022 | 0.142 | |
| Step time, right [s] | 0.004 | 0.786 | 0.006 | 0.426 | 0.036 | 0.100 | |
| Fast speed | Gait speed [cm/s] | 2.076 | 0.502 | 3.285 | 0.944 | 1.980 | 0.526 |
| Cadence [steps/min] | 0.909 | 0.349 | 2.539 | 0.901 | 1.663 | 0.368 | |
| Step length, left [cm] | 0.814 | 0.508 | 4.692 | 0.962 | 1.108 | 0.136 | |
| Step length, right [cm] | 0.757 | 0.721 | 2.750 | 0.893 | 1.103 | 0.177 | |
| Step time, left [s] | 0.003 | 0.508 | 0.020 | 0.835 | 0.007 | 0.160 | |
| Step time, right [s] | 0.003 | 0.488 | 0.042 | 0.809 | 0.008 | 0.148 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steinert, A.; Sattler, I.; Otte, K.; Röhling, H.; Mansow-Model, S.; Müller-Werdan, U. Using New Camera-Based Technologies for Gait Analysis in Older Adults in Comparison to the Established GAITRite System. Sensors 2020, 20, 125. https://doi.org/10.3390/s20010125
Steinert A, Sattler I, Otte K, Röhling H, Mansow-Model S, Müller-Werdan U. Using New Camera-Based Technologies for Gait Analysis in Older Adults in Comparison to the Established GAITRite System. Sensors. 2020; 20(1):125. https://doi.org/10.3390/s20010125
Chicago/Turabian StyleSteinert, Anika, Igor Sattler, Karen Otte, Hanna Röhling, Sebastian Mansow-Model, and Ursula Müller-Werdan. 2020. "Using New Camera-Based Technologies for Gait Analysis in Older Adults in Comparison to the Established GAITRite System" Sensors 20, no. 1: 125. https://doi.org/10.3390/s20010125
APA StyleSteinert, A., Sattler, I., Otte, K., Röhling, H., Mansow-Model, S., & Müller-Werdan, U. (2020). Using New Camera-Based Technologies for Gait Analysis in Older Adults in Comparison to the Established GAITRite System. Sensors, 20(1), 125. https://doi.org/10.3390/s20010125