Design and Evaluation of a Surface Electromyography-Controlled Steering Assistance Interface

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
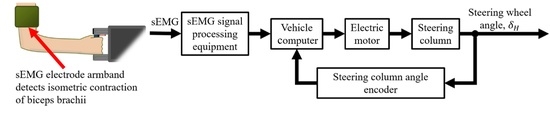
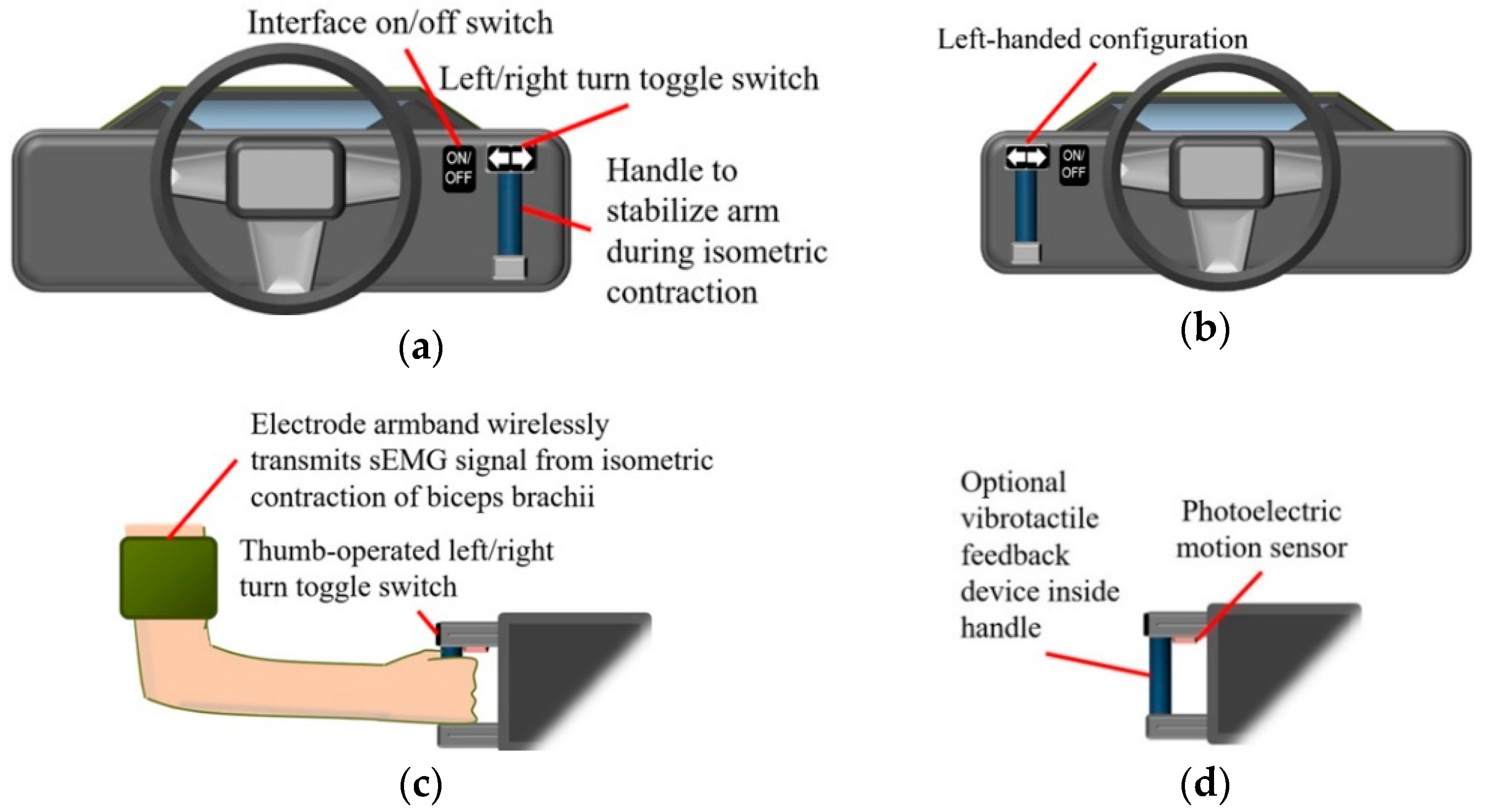
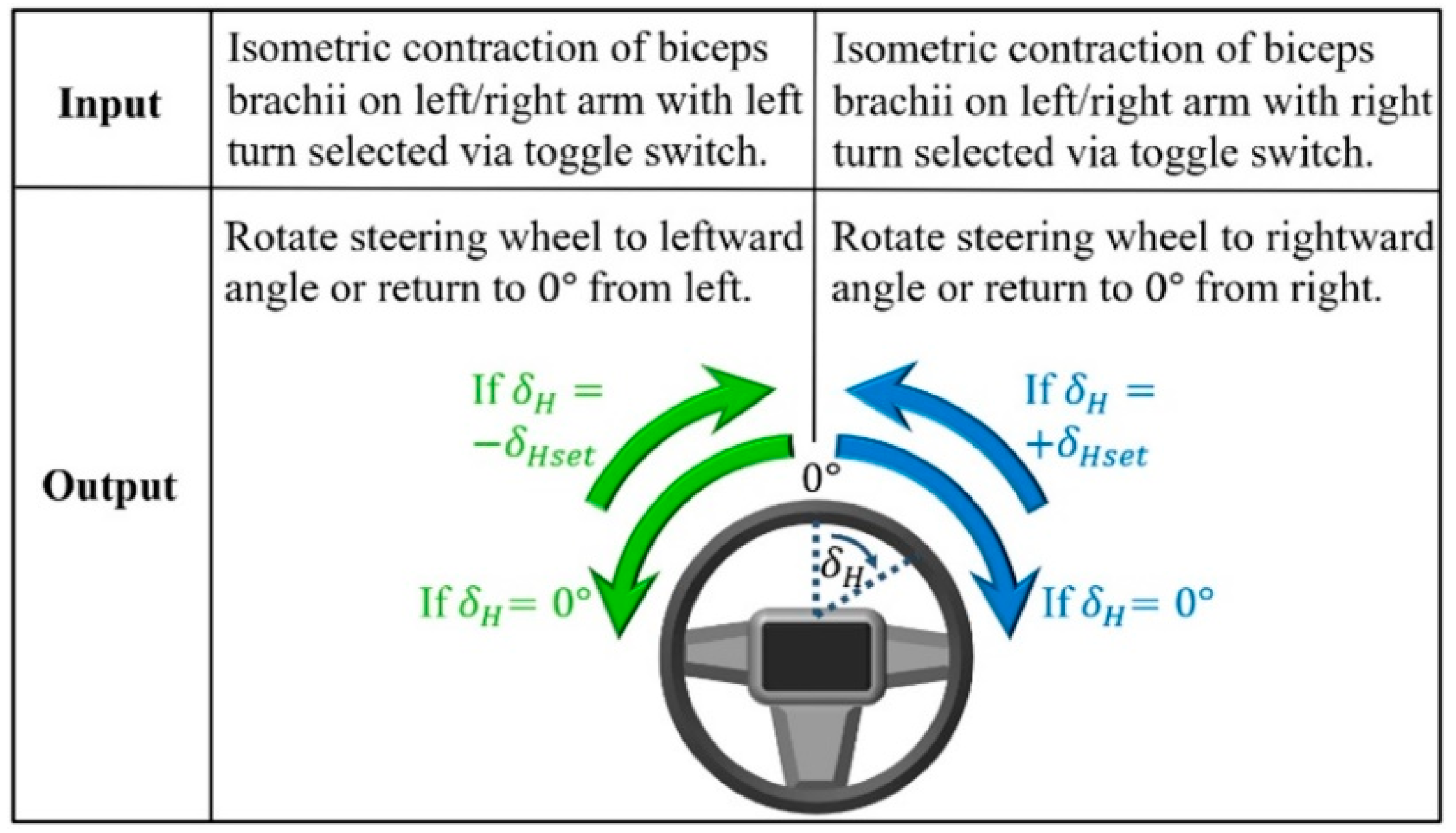
2.1. Steering Assistance Interface
2.2. Selection and Configuration of Surface Electromyography (sEMG) Equipment
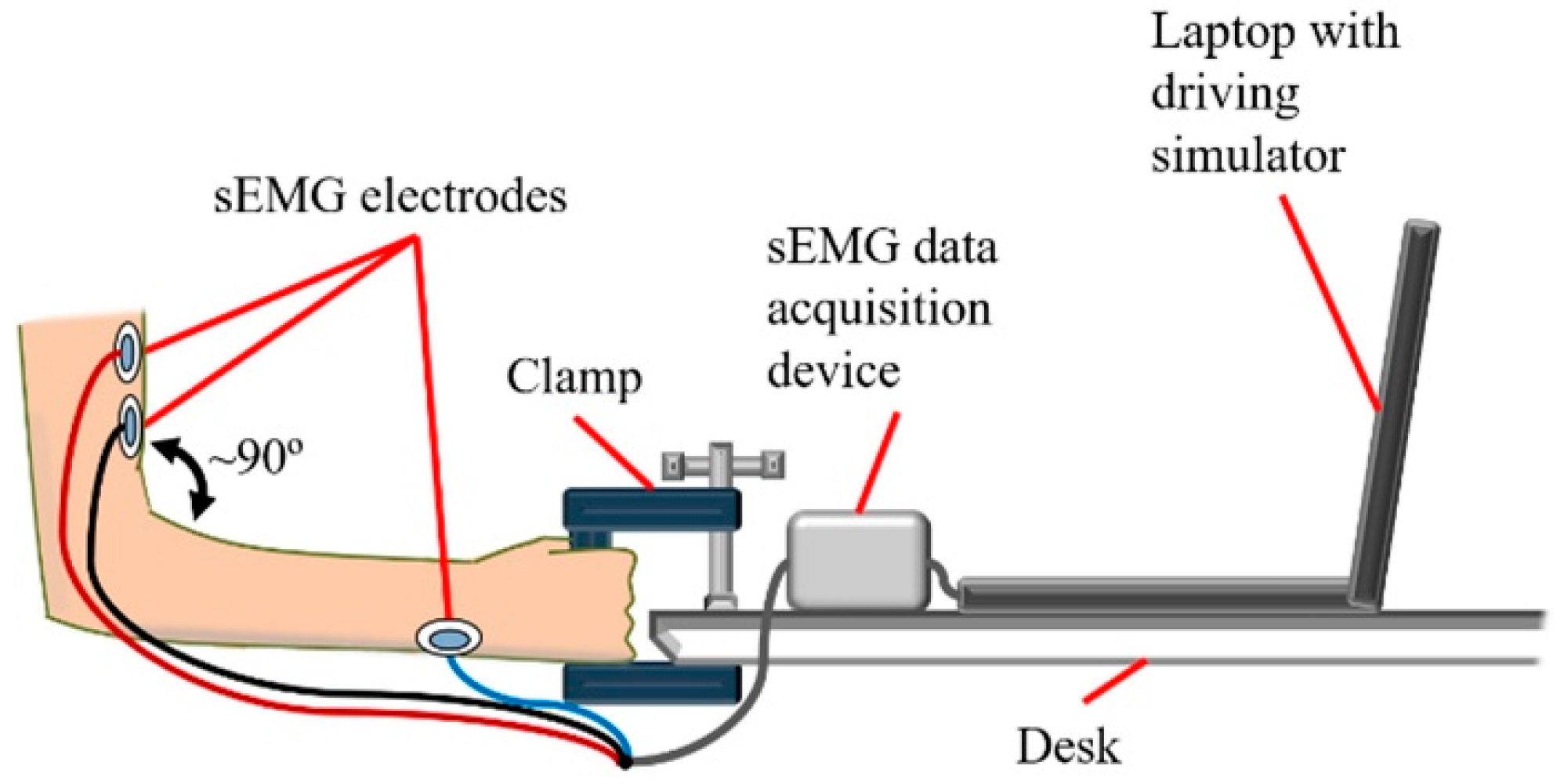
2.3. Experimental Setup
2.4. Driving Scenarios
2.5. Lateral Vehicle Dynamics
2.6. Experimental Trials
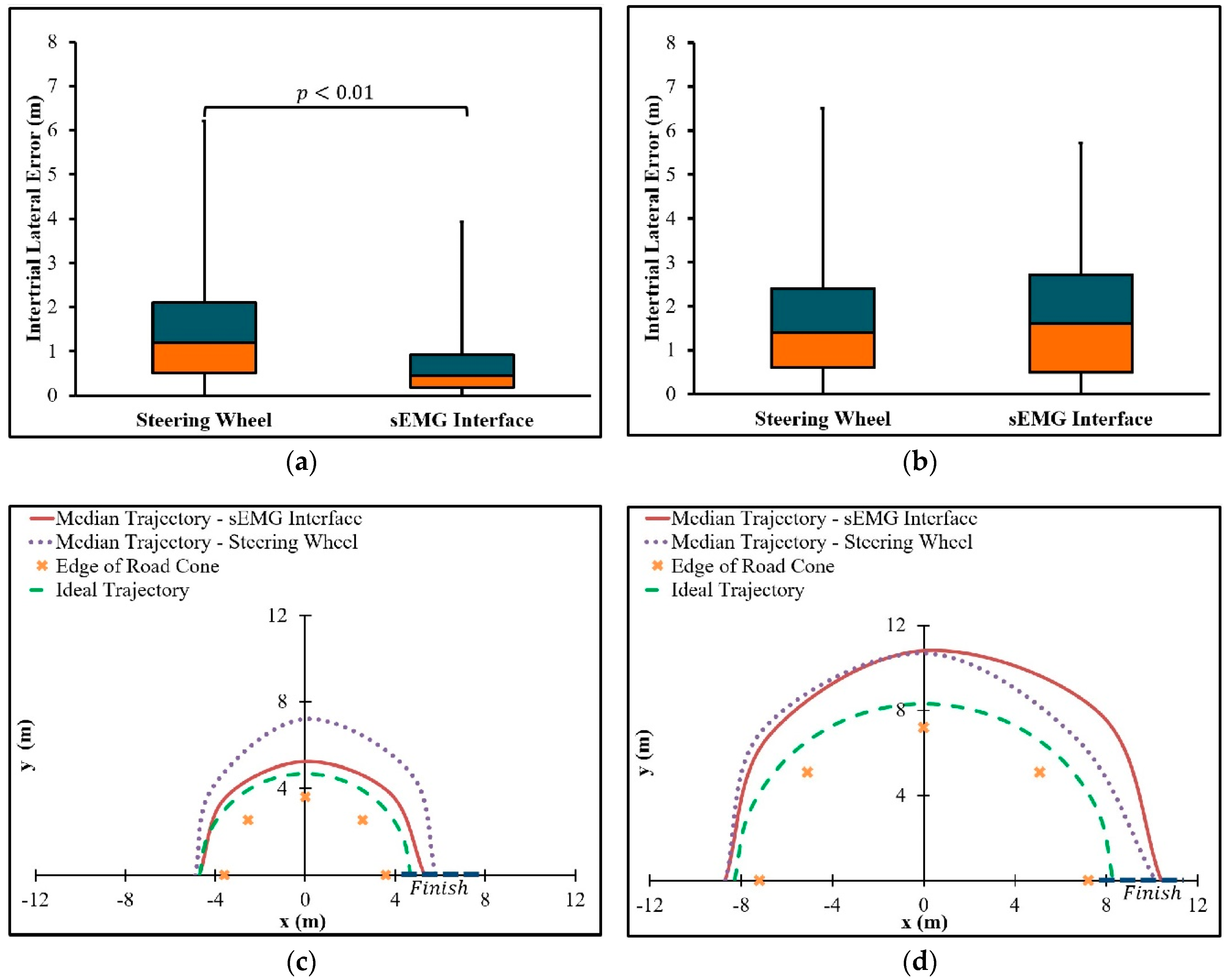
- For the U-turn with a radius of curvature equal to 3.6 m, the steering assistance interface is comparable or greater in path-following accuracy to the game steering wheel.
- For the U-turn with a radius of curvature equal to 7.2 m, the steering assistance interface is comparable or greater in path following accuracy to the game steering wheel, even if the sEMG interface is used without steering wheel correction.
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Meschtscherjakov, A. The Steering Wheel: A Design Space Exploration BT—Automotive User Interfaces: Creating Interactive Experiences in the Car; Meixner, G., Müller, C., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 349–373. [Google Scholar]
- Takada, Y.; Boer, E.R.; Sawaragi, T. Driving assist system: Shared haptic human system interaction. In Proceedings of the 12th IFAC Symposium on Analysis, Design, and Evaluation of Human-Machine Systems, Las Vegas, NV, USA, 11–14 August 2013; Narayanan, S., Ed.; International Federation of Automatic Control (IFAC): Las Vegas, NV, USA, 2013; pp. 203–210. [Google Scholar]
- Dinh, D.D.; Kubota, H. Profile-speed data-based models to estimate operating speeds for urban residential streets with a 30km/h speed limit. IATSS Res. 2013, 36, 115–122. [Google Scholar] [CrossRef]
- Pandis, P.; Prinold, J.A.I.; Bull, A.M.J. Shoulder muscle forces during driving: Sudden steering can load the rotator cuff beyond its repair limit. Clin. Biomech. 2015, 30, 839–846. [Google Scholar] [CrossRef]
- Bergmann, G.; Graichen, F.; Bender, A.; Kääb, M.; Rohlmann, A.; Westerhoff, P. In vivo glenohumeral contact forces-Measurements in the first patient 7 months postoperatively. J. Biomech. 2007, 40, 2139–2149. [Google Scholar] [CrossRef] [PubMed]
- ISO 4138:2012(E): Passenger Cars–Steady-State Circular Driving Behavior―Open-Loop Test Methods; International Standards Office: Geneva, Switzerland, 2012.
- Sharp, R.S.; Granger, R. On car steering torques at parking speeds. Proc. Inst. Mech. Eng. Part D J. Automob. Eng. 2003, 217, 87–96. [Google Scholar] [CrossRef]
- Ma, B.; Yang, Y.; Liu, Y.; Ji, X.; Zheng, H. Analysis of vehicle static steering torque based on tire-road contact patch sliding model and variable transmission ratio. Adv. Mech. Eng. 2016, 8, 1–11. [Google Scholar] [CrossRef]
- Hitosugi, M.; Takehara, I.; Watanabe, S.; Hayashi, Y.; Tokudome, S. Support for stroke patients in resumption of driving: Patient survey and driving simulator trial. Int. J. Gen. Med. 2011, 4, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Jung, N.; Kim, H.; Chang, M. Muscle activation of drivers with hemiplegia caused by stroke while driving using a steering wheel or knob. J. Phys. Ther. Sci. 2015, 27, 1009–1011. [Google Scholar] [CrossRef] [PubMed]
- Davidson, J. A survey of the satisfaction of upper limb amputees with their prostheses, their lifestyles, and their abilities. J. Hand Ther. 2002, 15, 62–70. [Google Scholar] [CrossRef]
- Jang, C.H.; Yang, H.S.; Yang, H.E.; Lee, S.Y.; Kwon, J.W.; Yun, B.D.; Choi, J.Y.; Kim, S.N.; Jeong, H.W. A survey on activities of daily living and occupations of upper extremity amputees. Ann. Rehabil. Med. 2011, 35, 907–921. [Google Scholar] [CrossRef]
- Basmajian, J.V.; De Luca, C.J. Muscles Alive: Their Functions Revealed by Electromyography, 5th ed.; Butler, J., Ed.; Williams and Wilkins: Baltimore, MD, USA, 1985. [Google Scholar]
- Nacpil, E.J.; Zheng, R.; Kaizuka, T.; Nakano, K. Implementation of a sEMG-machine interface for steering a virtual car in a driving simulator. In Proceedings of the AHFE 2017 International Conference on Human Factors in Simulation and Modeling, Los Angeles, CA, USA, 17–21 July 2017; Cassenti, D.N., Ed.; Springer International Publishing AG: Los Angeles, CA, USA, 2018; pp. 274–282. [Google Scholar]
- Kwak, J.; Jeon, T.W.; Park, H.; Kim, S.; An, K. Development of an EMG-Based Car Interface Using Artificial Neural Networks for the Physically Handicapped. Korea IT Serv. J. 2008, 7, 149–164. [Google Scholar]
- Iqbal, N.V.; Subramaniam, K.; Asmi, P.S. A Review on Upper-Limb Myoelectric Prosthetic Control. IETE J. Res. 2018, 64, 740–752. [Google Scholar] [CrossRef]
- Atzori, M.; Müller, H. Control Capabilities of Myoelectric Robotic Prostheses by Hand Amputees: A Scientific Research and Market Overview. Front. Syst. Neurosci. 2015, 9, 162. [Google Scholar] [CrossRef] [PubMed]
- Geethanjali, P. Myoelectric control of prosthetic hands: State-of-the-art review. Med. Devices Evid. Res. 2016, 9, 247–255. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, Q.; Lv, C.; Zheng, M.; Ji, X. A study on objective evaluation of vehicle steering comfort based on driver’s electromyogram and movement trajectory. IEEE Trans. Hum.-Machine Syst. 2018, 48, 41–49. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, Q.; Ji, X.; Hayama, R.; Mizuno, T.; Nakano, S. A New Objective Evaluation Method for Vehicle Steering Comfort. J. Dyn. Syst. Meas. Control 2017, 139, 91010–91013. [Google Scholar] [CrossRef]
- Liu, Y.; Ji, X.; Hayama, R.; Mizuno, T.; Nakano, S. Method for measuring a driver’s steering efficiency using electromyography. Proc. Inst. Mech. Eng. Part D J. Automob. Eng. 2014, 228, 1170–1184. [Google Scholar] [CrossRef]
- Dong, W.; Zhu, C.; Wang, Y.; Xiao, L.; Ye, D.; Huang, Y. Stretchable sEMG Electrodes Conformally Laminated on Skin for Continuous Electrophysiological Monitoring. In Intelligent Robotics and Applications; Huang, Y., Wu, H., Liu, H., Yin, Z., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 77–86. [Google Scholar]
- Hurwitz, D.S.; Pradhan, A.; Fisher, D.L.; Knodler, M.A.; Muttart, J.W.; Menon, R.; Meissner, U. Backing collisions: A study of drivers’ eye and backing behaviour using combined rear-view camera and sensor systems. Inj. Prev. 2010, 16, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Uchino, D.; Ikeda, K.; Endo, A.; Peeie, M.H.B.; Narita, T.; Kato, H. Driving Assist System for Ultra-Compact EVs―Fundamental Consideration of Muscle Burden Owing to Differences in the Drivers’ Physiques. Actuators 2018, 7, 44. [Google Scholar] [CrossRef]
- Minato, T.; Murata, Y.; Suzuki, A. Proposal of Automobile Driving Interface Using Strain Sensor for the Disabled People. In Proceedings of the 2015 Tohoku-Section Joint Convention of Institutes of Electrical and Information Engineers, Takizawa, Japan, 27–28 August 2015. [Google Scholar]
- Murata, Y.; Yoshida, K.; Suzuki, K.; Takahashi, D. Proposal of an Automobile Driving Interface Using Gesture Operation for Disabled People. In Proceedings of the ACHI 2013, The Sixth International Conference on Advances in Computer-Human Interactions, Nice, France, 24 February–1 March 2013; Miller, L., Ed.; 2013; pp. 472–478. [Google Scholar]
- Murata, Y.; Yoshida, K. Automobile Driving Interface Using Gesture Operations for Disabled People. Int. J. Adv. Intell. Syst. 2012, 6, 329–341. [Google Scholar]
- Wada, M.; Kameda, F. A joystick car drive system with seating in a wheelchair. In Proceedings of the 2009 35th Annual Conference of IEEE Industrial Electronics, Porto, Portugal, 3–5 November 2009; pp. 2163–2168. [Google Scholar]
- Wada, M.; Kimura, Y. Stability analysis of car driving with a joystick interface. In Proceedings of the 2013 IEEE 4th International Conference on Cognitive Infocommunications (CogInfoCom), Budapest, Hungary, 2–5 December 2013; pp. 493–496. [Google Scholar]
- Hakonen, M.; Piitulainen, H.; Visala, A. Current state of digital signal processing in myoelectric interfaces and related applications. Biomed. Signal Process. Control 2015, 18, 334–359. [Google Scholar] [CrossRef]
- Cheesborough, J.E.; Smith, L.H.; Kuiken, T.A.; Dumanian, G.A. Targeted muscle reinnervation and advanced prosthetic arms. Semin. Plast. Surg. 2015, 29, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Felzer, T.; Freisleben, B. HaWCoS: The “Hands-free” Wheelchair Control System. In Proceedings of the ASSETS ’02 The 5th ACM SIGCAPH Conference on Assistive Technologies, Edinburgh, UK, 8–10 July 2002; pp. 127–134. [Google Scholar]
- Ackermann, J. Robust control prevents car skidding. IEEE Control Syst. Mag. 1997, 17, 23–31. [Google Scholar] [CrossRef]
- Tandy, D.F.; Colborn, J.; Bae, J.C.; Coleman, C.; Pascarella, R. The True Definition and Measurement of Oversteer and Understeer. SAE Int. J. Commer. Veh. 2015, 8, 160–181. [Google Scholar] [CrossRef]
- Yamazaki, Y.; Suzuki, M.; Mano, T. Pulse control during rapid isometric contractions of the elbow joint. Brain Res. Bull. 1994, 34, 519–531. [Google Scholar] [CrossRef]
- Juds, S. Photoelectric Sensors and Controls: Selection and Application; Marcel Dekker, Inc.: New York, NY, USA, 1988. [Google Scholar]
- Whiting, W.; Rugg, S. Dynatomy with Web Resource: Dynamic Human Anatomy; Human Kinetics: Champaign, IL, USA, 2006. [Google Scholar]
- Forkenbrock, D.; Elsasser, D. An Assessment of Human Driver Steering Capability; National Highway Traffic Safety Administration: Liberty, NJ, USA, 2005.
- Cipriani, C.; Zaccone, F.; Micera, S.; Carrozza, M.C. On the shared control of an EMG-controlled prosthetic hand: Analysis of user-prosthesis interaction. IEEE Trans. Robot. 2008, 24, 170–184. [Google Scholar] [CrossRef]
- Kaczmarek, K.A.; Webster, J.G.; Bach-y-Rita, P.; Tompkins, W.J. Electrotactile and vibrotactile displays for sensory substitution systems. IEEE Trans. Biomed. Eng. 1991, 38, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Nissan ProPILOT Assist Technology Reduces the Hassle of Stop-And-Go Highway Driving, Ready for U.S. Launch. Available online: http://nissannews.com/en-US/nissan/usa/releases/nissan-propilot-assist-technology-reduces-the-hassle-of-stop-and-go-highway-driving-ready-for-u-s-launch?la=1&la=1 (accessed on 27 August 2018).
- J3016: Taxonomy and Definitions for Terms Related to On-Road Motor Vehicle Automated Driving Systems; SAE International: Warrendale, PA, USA, 2014.
- Dang, T.; Desens, J.; Franke, U.; Gavrila, D.; Schäfers, L.; Ziegler, W. Steering and Evasion Assist. In Handbook of Intelligent Vehicles; Eskandarian, A., Ed.; Springer-Verlag: London, UK, 2012; pp. 760–782. [Google Scholar]
- Kukkala, V.K.; Tunnell, J.; Pasricha, S.; Bradley, T. Advanced Driver-Assistance Systems: A Path Toward Autonomous Vehicles. IEEE Consum. Electron. Mag. 2018, 7, 18–25. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, Y.; Fujimoto, H.; Hori, Y. Vision-Based Lateral State Estimation for Integrated Control of Automated Vehicles Considering Multirate and Unevenly Delayed Measurements. IEEE/ASME Trans. Mechatron. 2018, 23, 2619–2627. [Google Scholar] [CrossRef]
- Gil, J.J.; Díaz, I.; Ciáurriz, P.; Echeverría, M. New driving control system with haptic feedback: Design and preliminary validation tests. Transp. Res. Part C Emerg. Technol. 2013, 33, 22–36. [Google Scholar] [CrossRef]
- Chen, R.; Gabler, H.C. Risk of thoracic injury from direct steering wheel impact in frontal crashes. J. Trauma Acute Care Surg. 2014, 76, 1441–1446. [Google Scholar] [CrossRef]
- Östlund, J. Joystick-Controlled Cars for Drivers with Severe Disabilities; Swedish National Road Administration, The Vehicle Standards Division: Linköping, Sweden, 1999.
- Pradko, F.; Lee, R.A. Theory of Human Vibration Response and its Application to Vehicle Design. In Biomechanics; Bootzin, D., Muffley, H.C., Eds.; Springer: New York, NY, USA, 1969; pp. 105–118. [Google Scholar]
- Belter, J.T.; Reynolds, B.C.; Dollar, A.M. Grasp and force based taxonomy of split-hook prosthetic terminal devices. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014. [Google Scholar]
- Sullivan, R.A.; Celikyol, F. Post Hospital Follow-Up of Three Bilateral Upper-Limb Amputees. Orthot. Prosthet. 1974, 28, 33–40. [Google Scholar]
- Lotte, F.; Larrue, F.; Mühl, C. Flaws in current human training protocols for spontaneous Brain-Computer Interfaces: Lessons learned from instructional design. Front. Hum. Neurosci. 2013, 7, 568. [Google Scholar] [CrossRef]
- Minguillon, J.; Lopez-Gordo, M.A.; Pelayo, F. Trends in EEG-BCI for daily-life: Requirements for artifact removal. Biomed. Signal Process. Control 2017, 31, 407–418. [Google Scholar] [CrossRef]
- Göhring, D.; Latotzky, D.; Wang, M.; Rojas, R. Semi-Autonomous Car Control Using Brain Computer Interfaces BT—Intelligent Autonomous Systems 12; Lee, S., Cho, H., Yoon, K.-J., Lee, J., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 393–408. [Google Scholar]
- Gomez-Gil, J.; San-Jose-Gonzalez, I.; Nicolas-Alonso, L.F.; Alonso-Garcia, S. Steering a tractor by means of an EMG-based human-machine interface. Sensors 2011, 11, 7110–7126. [Google Scholar] [CrossRef]
- Kar, A.; Corcoran, P. A review and analysis of eye-gaze estimation systems, algorithms and performance evaluation methods in consumer platforms. IEEE Access 2017, 5, 16495–16519. [Google Scholar] [CrossRef]
- Tuisku, O.; Rantanen, V.; Špakov, O.; Surakka, V.; Lekkala, J. Pointing and Selecting with Facial Activity. Interact. Comput. 2016, 28, 1–12. [Google Scholar] [CrossRef]
- Jiang, N.; Muceli, S.; Graimann, B.; Farina, D. Effect of arm position on the prediction of kinematics from EMG in amputees. Med. Biol. Eng. Comput. 2013, 51, 143–151. [Google Scholar] [CrossRef]
- Childress, D.S. Upper-Limb Prosthetics: Control of Limb Prostheses. In Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles; Bowker, H.K., Michael, J.W., Eds.; American Academy of Orthopedic Surgeons: Rosemont, IL, USA, 2002. [Google Scholar]
- Verrall, T.; Kulkarni, J.R. Driving appliances for upper limb amputees. Prosthet. Orthot. Int. 1995, 19, 124–127. [Google Scholar] [CrossRef]
- Raez, M.B.I.; Hussain, M.S.; Mohd-Yasin, F. Techniques of EMG signal analysis: Detection, processing, classification and applications. Biol. Proced. Online 2006, 8, 11–35. [Google Scholar] [CrossRef]
- Fukuoka, Y.; Miyazawa, K.; Mori, H.; Miyagi, M.; Nishida, M.; Horiuchi, Y.; Ichikawa, A.; Hoshino, H.; Noshiro, M.; Ueno, A. Development of a Compact Wireless Laplacian Electrode Module for Electromyograms and Its Human Interface Applications. Sensors 2013, 13, 2368–2383. [Google Scholar] [CrossRef]
- Vehkaoja, A.T.; Verho, J.A.; Puurtinen, M.M.; Nojd, N.M.; Lekkala, J.O.; Hyttinen, J.A. Wireless Head Cap for EOG and Facial EMG Measurements. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2005; pp. 5865–5868. [Google Scholar]
- Ding, I.-J.; Lin, R.-Z.; Lin, Z.-Y. Service robot system with integration of wearable Myo armband for specialized hand gesture human–computer interfaces for people with disabilities with mobility problems. Comput. Electr. Eng. 2018, 69, 815–827. [Google Scholar] [CrossRef]
- Mendez, I.G.; Pálsdóttir, Á.A.; Eiriksdóttir, D.H.; Faulkner, M.; Sriranjan, N.; Waris, A.; Kamavuako, E.N. Evaluation of classifiers performance using the Myo armband. In Proceedings of the Myoelectric Controls and Upper Limb Prosthetics Symposium, MEC17, Fredericton, NB, Canada, 15–18 August 2017. [Google Scholar]
- Roland, T.; Amsüss, S.; Russold, M.F.; Wolf, C.; Baumgartner, W. Capacitive Sensing of Surface EMG for Upper Limb Prostheses Control. Procedia Eng. 2016, 168, 155–158. [Google Scholar] [CrossRef]
- Searle, A.; Kirkup, L. A direct comparison of wet, dry and insulating bioelectric recording electrodes. Physiol. Meas. 2000, 21, 271–283. [Google Scholar] [CrossRef]
- Hermens, H.; Freriks, B. The State of the Art on Sensors and Sensor Placement Procedures for Surface ElectroMyoGraphy: A Proposal for Sensor Placement Procedures; SENIAM: Enschede, The Netherlands, 1997. [Google Scholar]
- Ahamed, N.U.; Sundaraj, K.; Ahmad, R.B.; Rahman, M.; Islam, M.A. Analysis of right arm biceps brachii muscle activity with varying the electrode placement on three male age groups during isometric contractions using a wireless EMG sensor. Procedia Eng. 2012, 41, 61–67. [Google Scholar] [CrossRef]
- Neilson, P.D. Frequency-response characteristics of the tonic stretch reflexes of biceps brachii muscle in intact man. Med. Biol. Eng. 1972, 10, 460–472. [Google Scholar] [CrossRef]
- Pulliam, C.L.; Lambrecht, J.M.; Kirsch, R.F. Electromyogram-based neural network control of transhumeral prostheses. J. Rehabil. Res. Dev. 2011, 48, 739–754. [Google Scholar] [CrossRef]
- Merad, M.; De Montalivet, É.; Touillet, A.; Martinet, N.; Roby-Brami, A.; Jarrassé, N. Can we achieve intuitive prosthetic elbow control based on healthy upper limb motor strategies? Front. Neurorobot. 2018, 12. [Google Scholar] [CrossRef]
- Abayasiri, R.A.M.; Madusanka, D.G.K.; Arachchige, N.M.P.; Silva, A.T.S.; Gopura, R.A.R.C. MoBio: A 5 DOF trans-humeral robotic prosthesis. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 1627–1632. [Google Scholar]
- Alshammary, N.A.; Dalley, S.A.; Goldfarb, M. Assessment of a multigrasp myoelectric control approach for use by transhumeral amputees. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 968–971. [Google Scholar] [CrossRef]
- Ruhunage, I.; Perera, C.J.; Nisal, K.; Subodha, J.; Lalitharatne, T.D. EMG signal controlled transhumerai prosthetic with EEG-SSVEP based approch for hand open/close. In Proceedings of the 2017 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Banff, AB, Canada, 5–8 October 2017; pp. 3169–3174. [Google Scholar]
- Dasanayake, W.D.I.G.; Gopura, R.A.R.C.; Dassanayake, V.P.C.; Mann, G.K.I. Surface EMG signals based elbow joint torque prediction. In Proceedings of the 2013 IEEE 8th International Conference on Industrial and Information Systems, Peradeniya, Sri Lanka, 17–20 December 2013; pp. 110–115. [Google Scholar]
- Scheme, E.J.; Englehart, K.B. Electromyogram pattern recognition for control of powered upper-limb prostheses: State of the art and challenges for clinical use. J. Rehabil. Res. Dev. 2011, 48, 643–659. [Google Scholar] [CrossRef]
- Bekey, G.A.; Chang, C.-W.; Perry, J.; Hoffer, M.M. Pattern recognition of multiple EMG signals applied to the description of human gait. Proc. IEEE 1977, 65, 674–681. [Google Scholar] [CrossRef]
- De Luca, C.J. The Use of Surface Electromyography in Biomechanics. J. Appl. Biomech. 1997, 13, 135–163. [Google Scholar] [CrossRef]
- DiCicco, M.; Lucas, L.; Matsuoka, Y. Comparison of control strategies for an EMG controlled orthotic exoskeleton for the hand. In Proceedings of the IEEE International Conference on Robotics and Automation, New Orleans, LA, USA, 26 April–1 May 2004; Volume 2, pp. 1622–1627. [Google Scholar]
- Chatham, A.; Walmink, W.; Mueller, F. UnoJoy! A Library for Rapid Video Game Prototyping Using Arduino. In Proceedings of the CHI ’13 Extended Abstracts on Human Factors in Computing Systems, Paris, France, 27 April–2 May 2013; pp. 2787–2788. [Google Scholar]
- JoyToKey Website. Available online: https://joytokey.net/en/ (accessed on 20 December 2018).
- Westerhoff, P.; Graichen, F.; Bender, A.; Halder, A.; Beier, A.; Rohlmann, A.; Bergmann, G. In vivo measurement of shoulder joint loads during activities of daily living. J. Biomech. 2009, 42, 1840–1849. [Google Scholar] [CrossRef] [PubMed]
- Rajamani, R. Lateral Vehicle Dynamics BT—Vehicle Dynamics and Control; Rajamani, R., Ed.; Springer: Boston, MA, USA, 2012; pp. 15–46. [Google Scholar]
- Benderius, O.; Markkula, G. Evidence for a fundamental property of steering. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2014, 58, 884–888. [Google Scholar] [CrossRef]
- Bernardi, M.; Felici, F.; Marchetti, M.; Montellanico, F.; Piacentini, M.; Solomonow, M. Force generation performance and motor unit recruitment strategy in muscles of contralateral limbs. J. Electromyogr. Kinesiol. 1999, 9, 121–130. [Google Scholar] [CrossRef]
- Ahamed, N.U.; Yusof, Z.B.M.; Alqahtani, M.; Altwijri, O.; Rahman, S.A.M.M.; Sundaraj, K. Gender Effects in Surface Electromyographic Activity of the Biceps Brachii Muscle During Prolonged Isometric Contraction. Procedia Comput. Sci. 2015, 61, 448–453. [Google Scholar] [CrossRef]
- Shuttleworth, M. Counterbalanced Measures Design. Available online: https://explorable.com/counterbalanced-measures-design (accessed on 12 October 2018).
- Upton, G.; Cook, I. Understanding Statistics; Oxford University Press: Oxford, UK, 1996. [Google Scholar]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samples). Biometrika 1965, 52, 591–611. [Google Scholar] [CrossRef]
- Whitley, E.; Ball, J. Statistics review 6: Nonparametric methods. Crit. Care 2002, 6, 509–513. [Google Scholar] [CrossRef]
- Pauwelussen, J.P. Essentials of Vehicle Dynamics; Elsevier, Ltd.: Oxford, UK, 2015. [Google Scholar]
- Plos, O.; Buisine, S.; Aoussat, A.; Mantelet, F.; Dumas, C. A Universalist strategy for the design of Assistive Technology. Int. J. Ind. Ergon. 2012, 42. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Conditions | Interface Type | Radius of Curvature of U-Turn (m) |
|---|---|---|
| 1 | sEMG | 3.6 |
| 2 | Game steering wheel | 3.6 |
| 3 | sEMG | 7.2 |
| 4 | Game steering wheel | 7.2 |
| Conditions | Interface Type | Radius of Curvature of U-Turn (m) | Intertrial Median Error (m) | Interquartile Range (IQR) (m) |
|---|---|---|---|---|
| 1 | sEMG | 3.6 | 0.5 | 0.8 |
| 2 | Game steering wheel | 3.6 | 1.2 | 1.6 |
| 3 | sEMG | 7.2 | 1.6 | 2.2 |
| 4 | Game steering wheel | 7.2 | 1.4 | 1.8 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nacpil, E.J.C.; Wang, Z.; Zheng, R.; Kaizuka, T.; Nakano, K. Design and Evaluation of a Surface Electromyography-Controlled Steering Assistance Interface. Sensors 2019, 19, 1308. https://doi.org/10.3390/s19061308
Nacpil EJC, Wang Z, Zheng R, Kaizuka T, Nakano K. Design and Evaluation of a Surface Electromyography-Controlled Steering Assistance Interface. Sensors. 2019; 19(6):1308. https://doi.org/10.3390/s19061308
Chicago/Turabian StyleNacpil, Edric John Cruz, Zheng Wang, Rencheng Zheng, Tsutomu Kaizuka, and Kimihiko Nakano. 2019. "Design and Evaluation of a Surface Electromyography-Controlled Steering Assistance Interface" Sensors 19, no. 6: 1308. https://doi.org/10.3390/s19061308
APA StyleNacpil, E. J. C., Wang, Z., Zheng, R., Kaizuka, T., & Nakano, K. (2019). Design and Evaluation of a Surface Electromyography-Controlled Steering Assistance Interface. Sensors, 19(6), 1308. https://doi.org/10.3390/s19061308