Computer-Aided Diagnosis of Multiple Sclerosis Using a Support Vector Machine and Optical Coherence Tomography Features


 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
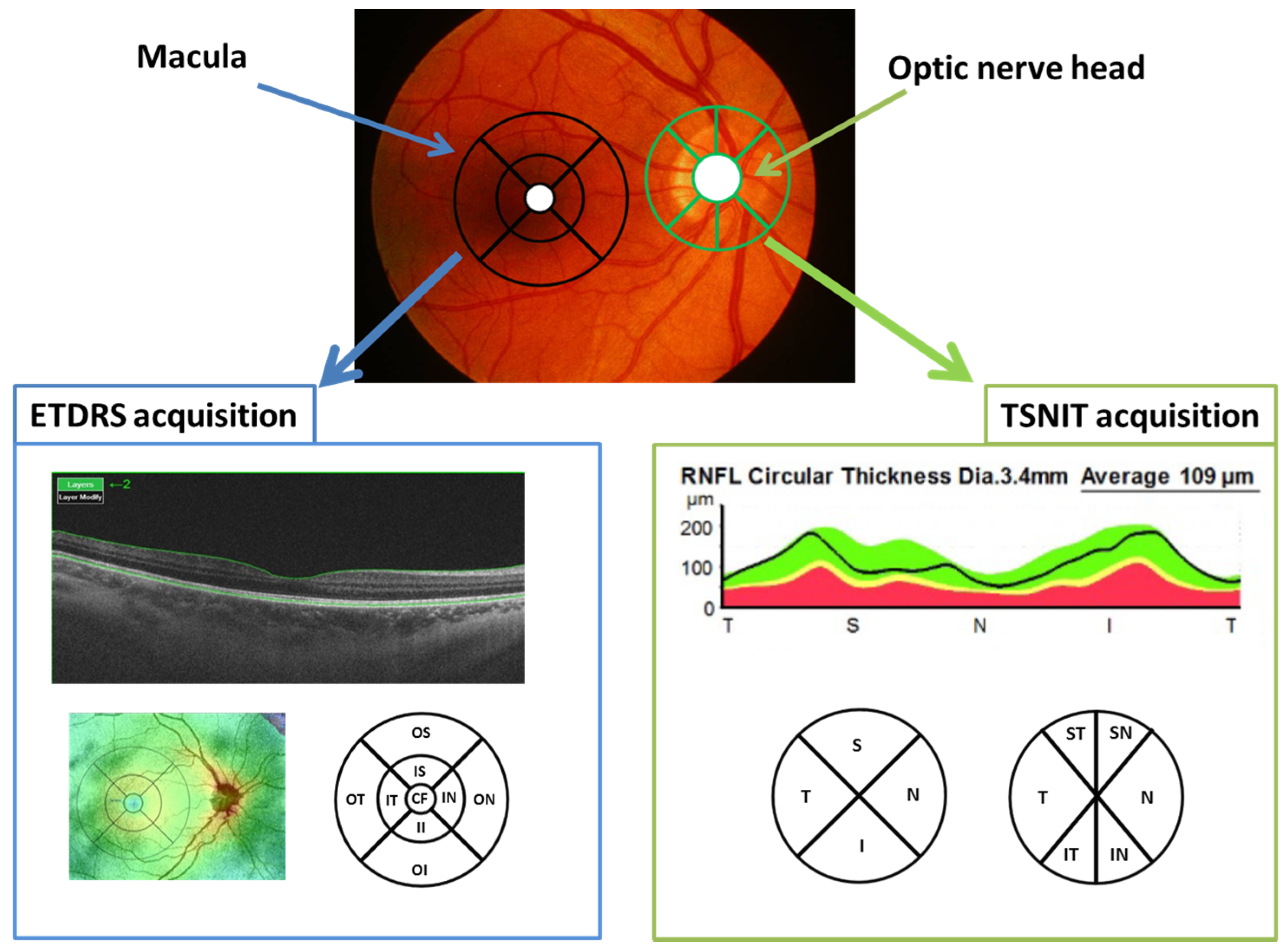
2.1. OCT Method
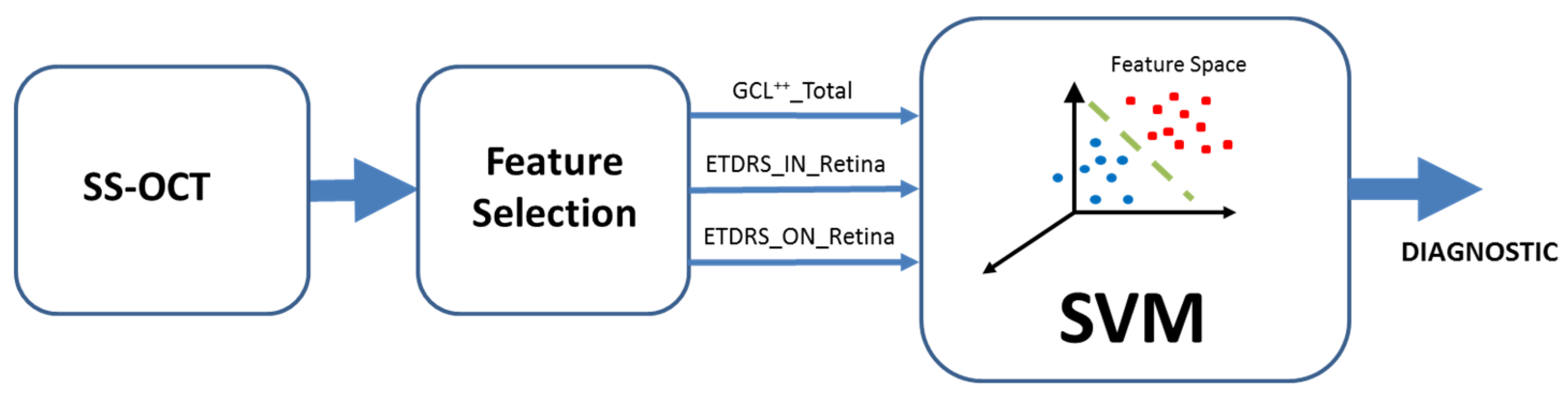
2.2. Support Vector Machine
2.3. Statistical Methods and Classification Assessment
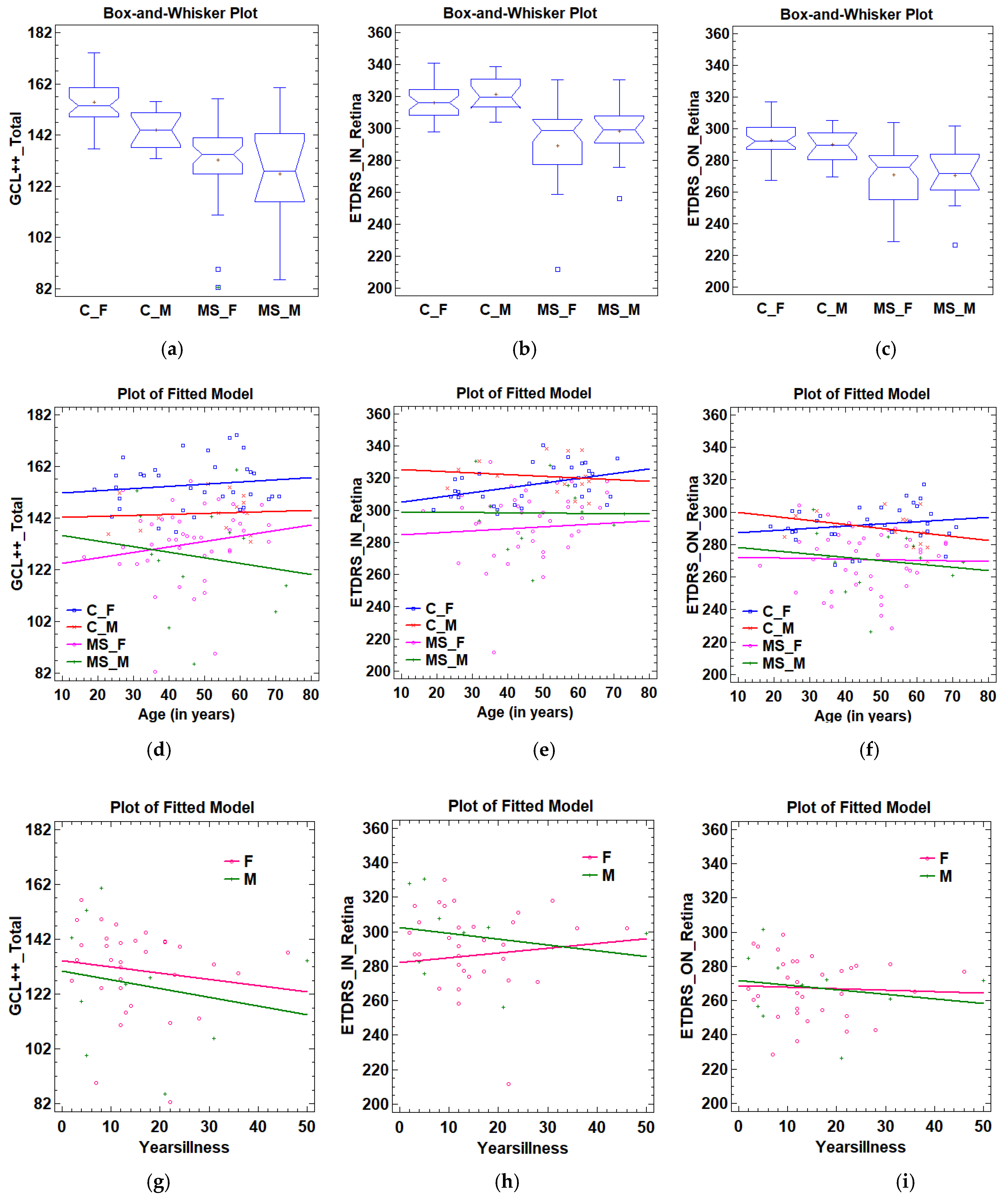
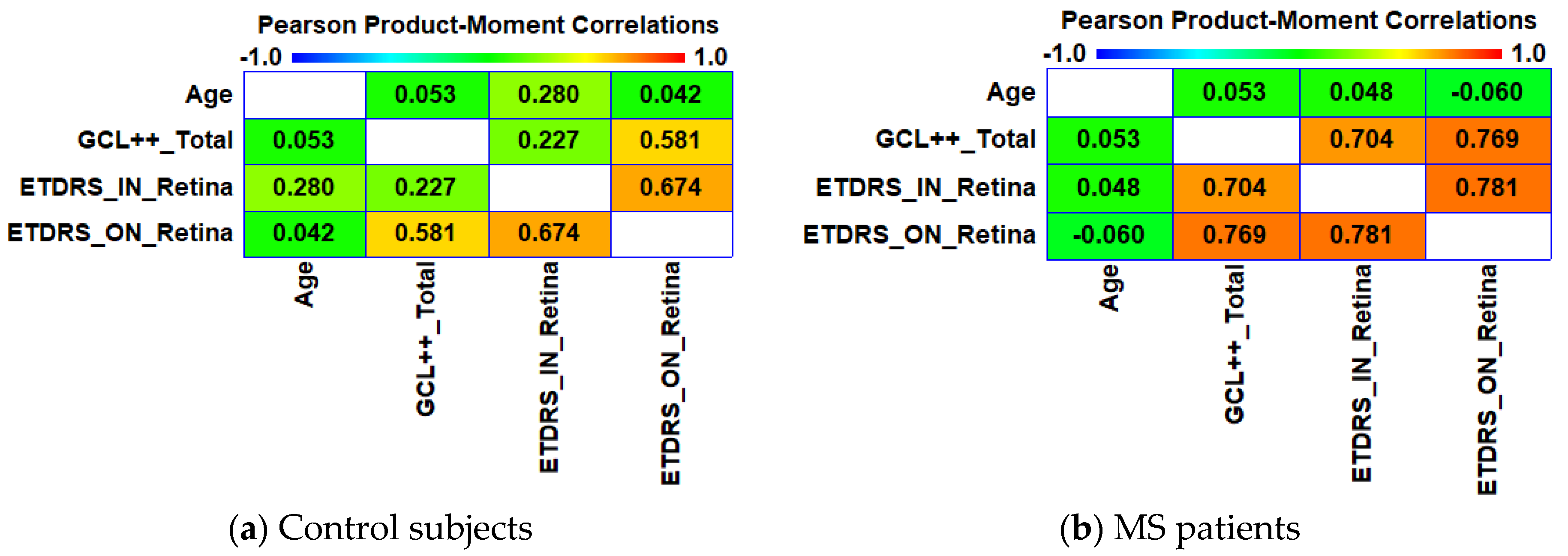
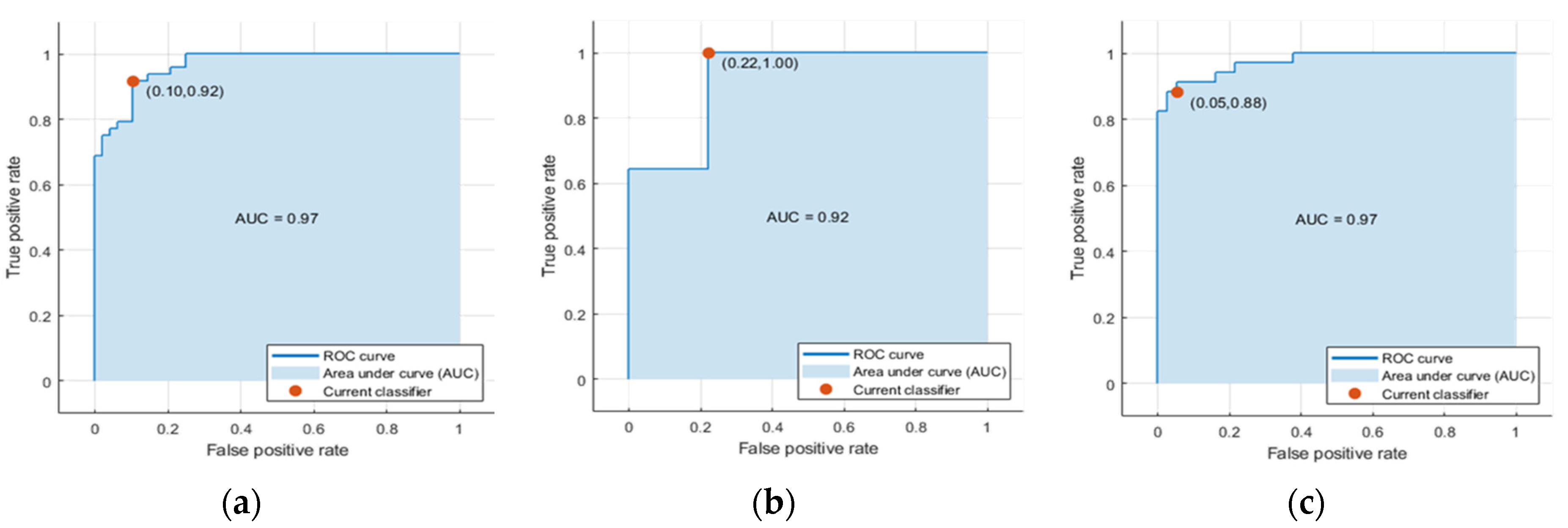
3. Results
Automatic Classifier
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Yamout, B.; Sahraian, M.; Bohlega, S.; Al-Jumah, M.; Goueider, R.; Dahdaleh, M.; Inshasi, J.; Hashem, S.; Alsharoqi, I.; Khoury, S.; et al. Consensus recommendations for the diagnosis and treatment of multiple sclerosis: 2019 revisions to the MENACTRIMS guidelines. Mult. Scler. Relat. Disord. 2020, 37, 101459. [Google Scholar] [CrossRef] [PubMed]
- Kaunzner, U.W.; Gauthier, S.A. MRI in the assessment and monitoring of multiple sclerosis: An update on best practice. Ther. Adv. Neurol. Disord. 2017, 10, 247–261. [Google Scholar] [CrossRef] [PubMed]
- Sakai, R.E.; Feller, D.J.; Galetta, K.M.; Galetta, S.L.; Balcer, L.J. Vision in multiple sclerosis: The story, structure-function correlations, and models for neuroprotection. J. Neuroophthalmol. 2011, 31, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef]
- Pérez Del Palomar, A.; Cegoñino, J.; Montolío, A.; Orduna, E.; Vilades, E.; Sebastián, B.; Pablo, L.E.; Garcia-Martin, E. Swept source optical coherence tomography to early detect multiple sclerosis disease. The use of machine learning techniques. PLoS ONE 2019, 14, e0216410. [Google Scholar] [CrossRef]
- de Boer, J.F.; Leitgeb, R.; Wojtkowski, M. Twenty-five years of optical coherence tomography: The paradigm shift in sensitivity and speed provided by Fourier domain OCT [Invited]. Biomed. Opt. Express 2017, 8, 3248. [Google Scholar] [CrossRef]
- Potsaid, B.; Baumann, B.; Huang, D.; Barry, S.; Cable, A.E.; Schuman, J.S.; Duker, J.S.; Fujimoto, J.G. Ultrahigh speed 1050nm swept source/Fourier domain OCT retinal and anterior segment imaging at 100,000 to 400,000 axial scans per second. Opt. Express 2010, 18, 20029–20048. [Google Scholar] [CrossRef]
- Yasin Alibhai, A.; Or, C.; Witkin, A.J. Swept Source Optical Coherence Tomography: A Review. Curr. Ophthalmol. Rep. 2018, 6, 7–16. [Google Scholar] [CrossRef]
- Hirata, M.; Tsujikawa, A.; Matsumoto, A.; Hangai, M.; Ooto, S.; Yamashiro, K.; Akiba, M.; Yoshimura, N. Macular choroidal thickness and volume in normal subjects measured by swept-source optical coherence tomography. Invest. Ophthalmol. Vis. Sci. 2011, 52, 4971–4978. [Google Scholar] [CrossRef]
- Copete, S.; Flores-Moreno, I.; Montero, J.A.; Duker, J.S.; Ruiz-Moreno, J.M. Direct comparison of spectral-domain and swept-source OCT in the measurement of choroidal thickness in normal eyes. Br. J. Ophthalmol. 2014, 98, 334–338. [Google Scholar] [CrossRef]
- Cogliati, A.; Canavesi, C.; Hayes, A.; Tankam, P.; Duma, V.-F.; Santhanam, A.; Thompson, K.P.; Rolland, J.P. MEMS-based handheld scanning probe with pre-shaped input signals for distortion-free images in Gabor-domain optical coherence microscopy. Opt. Express 2016, 24, 13365. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Martin, E.; Pueyo, V.; Pinilla, I.; Ara, J.-R.; Martin, J.; Fernandez, J. Fourier-domain OCT in multiple sclerosis patients: Reproducibility and ability to detect retinal nerve fiber layer atrophy. Investig. Ophthalmol. Vis. Sci. 2011, 52, 4124–4131. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wicki, C.A.; Hanson, J.V.M.; Schippling, S. Optical coherence tomography as a means to characterize visual pathway involvement in multiple sclerosis. Curr. Opin. Neurol. 2018, 31, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Lapiscina, E.H.; Arnow, S.; Wilson, J.A.; Saidha, S.; Preiningerova, J.L.; Oberwahrenbrock, T.; Brandt, A.U.; Pablo, L.E.; Guerrieri, S.; Gonzalez, I.; et al. Retinal thickness measured with optical coherence tomography and risk of disability worsening in multiple sclerosis: A cohort study. Lancet Neurol. 2016, 15, 574–584. [Google Scholar] [CrossRef]
- Parisi, V.; Manni, G.; Spadaro, M.; Colacino, G.; Restuccia, R.; Marchi, S.; Bucci, M.G.; Pierelli, F. Correlation between morphological and functional retinal impairment in multiple sclerosis patients. Invest. Ophthalmol. Vis. Sci. 1999, 40, 2520–2527. [Google Scholar]
- Alonso, R.; Gonzalez-Moron, D.; Garcea, O. Optical coherence tomography as a biomarker of neurodegeneration in multiple sclerosis: A review. Mult. Scler. Relat. Disord. 2018, 22, 77–82. [Google Scholar] [CrossRef]
- Satue, M.; Obis, J.; Rodrigo, M.J.; Otin, S.; Fuertes, M.I.; Vilades, E.; Gracia, H.; Ara, J.R.; Alarcia, R.; Polo, V.; et al. Optical Coherence Tomography as a Biomarker for Diagnosis, Progression, and Prognosis of Neurodegenerative Diseases. J. Ophthalmol. 2016, 2016, 8503859. [Google Scholar] [CrossRef]
- Kucharczuk, J.; Maciejek, Z.; Sikorski, B.L. Optical coherence tomography in diagnosis and monitoring multiple sclerosis. Neurol. Neurochir. Pol. 2018, 52, 140–149. [Google Scholar] [CrossRef]
- Petzold, A.; Balcer, L.J.; Calabresi, P.A.; Costello, F.; Frohman, T.C.; Frohman, E.M.; Martinez-Lapiscina, E.H.; Green, A.J.; Kardon, R.; Outteryck, O.; et al. Retinal layer segmentation in multiple sclerosis: A systematic review and meta-analysis. Lancet. Neurol. 2017, 16, 797–812. [Google Scholar] [CrossRef]
- Fisher, J.B.; Jacobs, D.A.; Markowitz, C.E.; Galetta, S.L.; Volpe, N.J.; Nano-Schiavi, M.L.; Baier, M.L.; Frohman, E.M.; Winslow, H.; Frohman, T.C.; et al. Relation of visual function to retinal nerve fiber layer thickness in multiple sclerosis. Ophthalmology 2006, 113, 324–332. [Google Scholar] [CrossRef]
- Britze, J.; Pihl-Jensen, G.; Frederiksen, J.L. Retinal ganglion cell analysis in multiple sclerosis and optic neuritis: A systematic review and meta-analysis. J. Neurol. 2017, 264, 1837–1853. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Martin, E.; Jarauta, L.; Vilades, E.; Ara, J.R.; Martin, J.; Polo, V.; Larrosa, J.M.; Pablo, L.E.; Satue, M. Ability of Swept-Source Optical Coherence Tomography to Detect Retinal and Choroidal Changes in Patients with Multiple Sclerosis. J. Ophthalmol. 2018, 2018, 7361212. [Google Scholar] [CrossRef] [PubMed]
- Zurita, M.; Montalba, C.; Labbé, T.; Cruz, J.P.; Dalboni da Rocha, J.; Tejos, C.; Ciampi, E.; Cárcamo, C.; Sitaram, R.; Uribe, S. Characterization of relapsing-remitting multiple sclerosis patients using support vector machine classifications of functional and diffusion MRI data. NeuroImage Clin. 2018, 20, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Healy, B.C.; Rotstein, D.; Guttmann, C.R.G.; Bakshi, R.; Weiner, H.L.; Brodley, C.E.; Chitnis, T. Exploration of machine learning techniques in predicting multiple sclerosis disease course. PLoS ONE 2017, 12, e0174866. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lu, S.; Zhou, X.; Yang, M.; Wu, L.; Liu, B.; Phillips, P.; Wang, S. Comparison of machine learning methods for stationary wavelet entropy-based multiple sclerosis detection: Decision tree, k -nearest neighbors, and support vector machine. Simulation 2016, 92, 861–871. [Google Scholar] [CrossRef]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef]
- Vapnik, V.N. An overview of statistical learning theory. IEEE Trans. Neural Netw. 1999, 10, 988–999. [Google Scholar] [CrossRef]
- Bamber, D. The area above the ordinal dominance graph and the area below the receiver operating characteristic graph. J. Math. Psychol. 1975, 12, 387–415. [Google Scholar] [CrossRef]
- Matthews, B.W. Comparison of the predicted and observed secondary structure of T4 phage lysozyme. Biochim. Biophys. Acta-Protein Struct. 1975, 405, 442–451. [Google Scholar] [CrossRef]
- Chicco, D. Ten quick tips for machine learning in computational biology. BioData Min. 2017, 10, 35. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Oertel, F.C.; Zimmermann, H.G.; Brandt, A.U.; Paul, F. Novel uses of retinal imaging with optical coherence tomography in multiple sclerosis. Expert Rev. Neurother. 2019, 19, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Richiardi, J.; Gschwind, M.; Simioni, S.; Annoni, J.-M.; Greco, B.; Hagmann, P.; Schluep, M.; Vuilleumier, P.; Van De Ville, D. Classifying minimally disabled multiple sclerosis patients from resting state functional connectivity. Neuroimage 2012, 62, 2021–2033. [Google Scholar] [CrossRef] [PubMed]
- Costello, F.; Burton, J.M. Retinal imaging with optical coherence tomography: A biomarker in multiple sclerosis? Eye Brain 2018, 10, 47–63. [Google Scholar] [CrossRef]
- Srinivasan, S.; Efron, N. Optical coherence tomography in the investigation of systemic neurologic disease. Clin. Exp. Optom. 2019, 102, 309–319. [Google Scholar] [CrossRef]
- Britze, J.; Frederiksen, J.L. Optical coherence tomography in multiple sclerosis. Eye 2018, 32, 884–888. [Google Scholar] [CrossRef]
- Garcia-Martin, E.; Pablo, L.E.; Herrero, R.; Ara, J.R.; Martin, J.; Larrosa, J.M.; Polo, V.; Garcia-Feijoo, J.; Fernandez, J. Neural networks to identify multiple sclerosis with optical coherence tomography. Acta Ophthalmol. 2013, 91, e628–e634. [Google Scholar] [CrossRef]
- Rudnicka, A.R.; Jarrar, Z.; Wormald, R.; Cook, D.G.; Fletcher, A.; Owen, C.G. Age and gender variations in age-related macular degeneration prevalence in populations of European ancestry: A meta-analysis. Ophthalmology 2012, 119, 571–580. [Google Scholar] [CrossRef]
- Harbo, H.F.; Gold, R.; Tintoré, M. Sex and gender issues in multiple sclerosis. Ther. Adv. Neurol. Disord. 2013, 6, 237–248. [Google Scholar] [CrossRef]
- Ribbons, K.A.; McElduff, P.; Boz, C.; Trojano, M.; Izquierdo, G.; Duquette, P.; Girard, M.; Grand’Maison, F.; Hupperts, R.; Grammond, P.; et al. Male Sex Is Independently Associated with Faster Disability Accumulation in Relapse-Onset MS but Not in Primary Progressive MS. PLoS ONE 2015, 10, e0122686. [Google Scholar] [CrossRef]
- MacKenzie-Graham, A.J.; Rinek, G.A.; Avedisian, A.; Morales, L.B.; Umeda, E.; Boulat, B.; Jacobs, R.E.; Toga, A.W.; Voskuhl, R.R. Estrogen treatment prevents gray matter atrophy in experimental autoimmune encephalomyelitis. J. Neurosci. Res. 2012, 90, 1310–1323. [Google Scholar] [CrossRef] [PubMed]
- González, H.; Elgueta, D.; Montoya, A.; Pacheco, R. Neuroimmune regulation of microglial activity involved in neuroinflammation and neurodegenerative diseases. J. Neuroimmunol. 2014, 274, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Desai, M.K.; Brinton, R.D. Autoimmune Disease in Women: Endocrine Transition and Risk Across the Lifespan. Front. Endocrinol. 2019, 10, 265. [Google Scholar] [CrossRef] [PubMed]
- Herting, M.M.; Sowell, E.R. Puberty and structural brain development in humans. Front. Neuroendocrinol. 2017, 44, 122–137. [Google Scholar] [CrossRef]
- Guo, L.; Normando, E.M.; Nizari, S.; Lara, D.; Cordeiro, M.F. Tracking longitudinal retinal changes in experimental ocular hypertension using the cSLO and spectral domain-OCT. Investig. Ophthalmol. Vis. Sci. 2010, 51, 6504–6513. [Google Scholar] [CrossRef]
- Fjeldstad, C.; Bemben, M.; Pardo, G. Reduced retinal nerve fiber layer and macular thickness in patients with multiple sclerosis with no history of optic neuritis identified by the use of spectral domain high-definition optical coherence tomography. J. Clin. Neurosci. 2011, 18, 1469–1472. [Google Scholar] [CrossRef]
- Garcia-Martin, E.; Polo, V.; Larrosa, J.M.; Marques, M.L.; Herrero, R.; Martin, J.; Ara, J.R.; Fernandez, J.; Pablo, L.E. Retinal layer segmentation in patients with multiple sclerosis using spectral domain optical coherence tomography. Ophthalmology 2014, 121, 573–579. [Google Scholar] [CrossRef]
- Sull, A.C.; Vuong, L.N.; Price, L.L.; Srinivasan, V.J.; Gorczynska, I.; Fujimoto, J.G.; Schuman, J.S.; Duker, J.S. Comparison of spectral/Fourier domain optical coherence tomography instruments for assessment of normal macular thickness. Retina 2010, 30, 235–245. [Google Scholar] [CrossRef]
- Miller, A.R.; Roisman, L.; Zhang, Q.; Zheng, F.; Rafael de Oliveira Dias, J.; Yehoshua, Z.; Schaal, K.B.; Feuer, W.; Gregori, G.; Chu, Z.; et al. Comparison Between Spectral-Domain and Swept-Source Optical Coherence Tomography Angiographic Imaging of Choroidal Neovascularization. Investig. Ophthalmol. Vis. Sci. 2017, 58, 1499–1505. [Google Scholar] [CrossRef]
- Del Castillo, M.O.; Cordón, B.; Sánchez Morla, E.M.; Vilades, E.; Rodrigo, M.J.; Cavaliere, C.; Boquete, L.; Garcia-Martin, E. Identification of clusters in multifocal electrophysiology recordings to maximize discriminant capacity (patients vs. control subjects). Doc. Ophthalmol. 2019. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Controls (n = 48) | MS (n = 48) | Test to Compare Distributions | Test to Compare Variances | Test to Compare Means | Test to Compare Medians | AUC (n = 96) | AUCM (n = 24) | AUCF (n = 72) | |
|---|---|---|---|---|---|---|---|---|---|
| GCL++_Total (µm) | 151.65 (10.28) | 130.91 (16.63) | K-S = 3.162, p = 0.000 | F = 0.381, p = 0.0009 | t = 7.759, p = 4.43 × 10−7 not assuming equal variances | W = 326.0, p = 3.27 × 10−11 | 0.879 | 0.750 | 0.934 |
| ETDRS_IN_Retina (µm) | 317.52 (11.35) | 291.28 (30.71) | K-S = 3.102, p = 8.801 × 10−9 | F = 0.136, p = 1.29 × 10−10 | t = 5.937, p = 6.93 × 10−7 not assuming equal variances | W = 379.0, p = 3.20 × 10−10 | 0.859 | 0.845 | 0.853 |
| ETDRS_ON_Retina (µm) | 291.72 (11.28) | 270.62 (17.96) | K-S = 3.101, p = 8.795 × 10−9 | F = 0.394, p = 0.001 | t = 7.272, p = 0.000 not assuming equal variances | W = 406.5, p = 1.00 × 10−9 | 0.849 | 0.821 | 0.859 |
| Area | Retina | Choroid | RNFL | GCL+ | GCL++ | ||
|---|---|---|---|---|---|---|---|
| ETDRS | Inner superior (IS) | 0.818 | 0.570 | -- | -- | -- | |
| Inner nasal (IN) | 0.859 | 0.520 | -- | -- | -- | ||
| Inner inferior (II) | 0.836 | 0.509 | -- | -- | -- | ||
| Inner temporal (IT) | 0.812 | 0.512 | -- | -- | -- | ||
| Outer superior (OS) | 0.755 | 0.541 | -- | -- | -- | ||
| Outer nasal (ON) | 0.849 | 0.501 | -- | -- | -- | ||
| Outer inferior (OI) | 0.751 | 0.512 | -- | -- | -- | ||
| Outer temporal (OT) | 0.712 | 0.520 | -- | -- | -- | ||
| TSNIT | Quadrants | Temporal (T) | 0.805 | 0.515 | 0.656 | 0.82 | 0.772 |
| Superior (S) | 0.831 | 0.516 | 0.832 | 0.626 | 0.805 | ||
| Nasal (N) | 0.733 | 0.507 | 0.68 | 0.685 | 0.724 | ||
| Inferior (I) | 0.823 | 0.52 | 0.766 | 0.668 | 0.805 | ||
| Sectors | Temporal (T) | 0.805 | 0.515 | 0.656 | 0.82 | 0.772 | |
| Superotemporal (ST) | 0.762 | 0.511 | 0.742 | 0.624 | 0.768 | ||
| Superonasal (SN) | 0.829 | 0.502 | 0.82 | 0.605 | 0.829 | ||
| Nasal (N) | 0.753 | 0.501 | 0.704 | 0.685 | 0.745 | ||
| Inferonasal (IN) | 0.769 | 0.509 | 0.692 | 0.679 | 0.737 | ||
| Inferotemporal (IT) | 0.770 | 0.523 | 0.738 | 0.596 | 0.764 | ||
| Total | 0.835 | 0.517 | 0.809 | 0.76 | 0.879 | ||
| Controls (n = 48) | MS (n = 48) | Test to Compare Distributions | Test to Compare Variances | Test to Compare Means | Test to Compare Medians | AUC (n = 96) | AUCM (n = 24) | AUCF (n = 72) | |
|---|---|---|---|---|---|---|---|---|---|
| GCL++_Total (µm) | 151.65 (10.28) | 130.91 (16.63) | K-S = 3.162, p = 0.000 | F = 0.381, p = 0.0009 | T = 7.759, p = 4.43 × 10−7 not assuming equal variances | W = 326.0, p = 3.27 × 10−11 | 0.879 | 0.750 | 0.934 |
| ETDRS_IN_Retina (µm) | 317.52 (11.35) | 291.28 (30.71) | K-S = 3.102, p = 8.801 × 10−9 | F = 0.136, p = 1.29 × 10−10 | t = 5.937, p = 6.93 × 10−7 not assuming equal variances | W = 379.0, p = 3.20 × 10−10 | 0.859 | 0.845 | 0.853 |
| ETDRS_ON_Retina (µm) | 291.72 (11.28) | 270.62 (17.96) | K-S = 3.101, p = 8.795 × 10−9 | F = 0.394, p = 0.001 | t = 7.272, p = 0.000 not assuming equal variances | W = 406.5, p = 1.00 × 10−9 | 0.849 | 0.821 | 0.859 |
| Predicted Class (Males and Females) | Predicted Class (Males) | Predicted Class (Females) | |||||
|---|---|---|---|---|---|---|---|
| Controls | MS | Controls | MS | Controls | MS | ||
| True Class | Controls | 44 | 4 | 14 | 0 | 30 | 4 |
| MS | 5 | 43 | 3 | 7 | 3 | 35 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavaliere, C.; Vilades, E.; Alonso-Rodríguez, M.C.; Rodrigo, M.J.; Pablo, L.E.; Miguel, J.M.; López-Guillén, E.; Morla, E.M.S.; Boquete, L.; Garcia-Martin, E. Computer-Aided Diagnosis of Multiple Sclerosis Using a Support Vector Machine and Optical Coherence Tomography Features. Sensors 2019, 19, 5323. https://doi.org/10.3390/s19235323
Cavaliere C, Vilades E, Alonso-Rodríguez MC, Rodrigo MJ, Pablo LE, Miguel JM, López-Guillén E, Morla EMS, Boquete L, Garcia-Martin E. Computer-Aided Diagnosis of Multiple Sclerosis Using a Support Vector Machine and Optical Coherence Tomography Features. Sensors. 2019; 19(23):5323. https://doi.org/10.3390/s19235323
Chicago/Turabian StyleCavaliere, Carlo, Elisa Vilades, Mª C. Alonso-Rodríguez, María Jesús Rodrigo, Luis Emilio Pablo, Juan Manuel Miguel, Elena López-Guillén, Eva Mª Sánchez Morla, Luciano Boquete, and Elena Garcia-Martin. 2019. "Computer-Aided Diagnosis of Multiple Sclerosis Using a Support Vector Machine and Optical Coherence Tomography Features" Sensors 19, no. 23: 5323. https://doi.org/10.3390/s19235323
APA StyleCavaliere, C., Vilades, E., Alonso-Rodríguez, M. C., Rodrigo, M. J., Pablo, L. E., Miguel, J. M., López-Guillén, E., Morla, E. M. S., Boquete, L., & Garcia-Martin, E. (2019). Computer-Aided Diagnosis of Multiple Sclerosis Using a Support Vector Machine and Optical Coherence Tomography Features. Sensors, 19(23), 5323. https://doi.org/10.3390/s19235323