Semi-Automatic Calibration Method for a Bed-Monitoring System Using Infrared Image Depth Sensors

 , and
, and
Abstract
1. Introduction
- Installation of the depth sensor in any position and attitude without installation on the ceiling, such as on a tripod or on a bed fence. However, both the bed and floor need to be captured and their total area needs to be larger than the wall area.
- Automatic calculation of the bed and floor regions, sensor position and attitude, and spatial domain.
- Reconfiguration of the spatial domain considering occlusion by the head or foot of the bed.
- Reconfiguration of the spatial domain considering the gravity center of the patient.
2. Calibration Methods
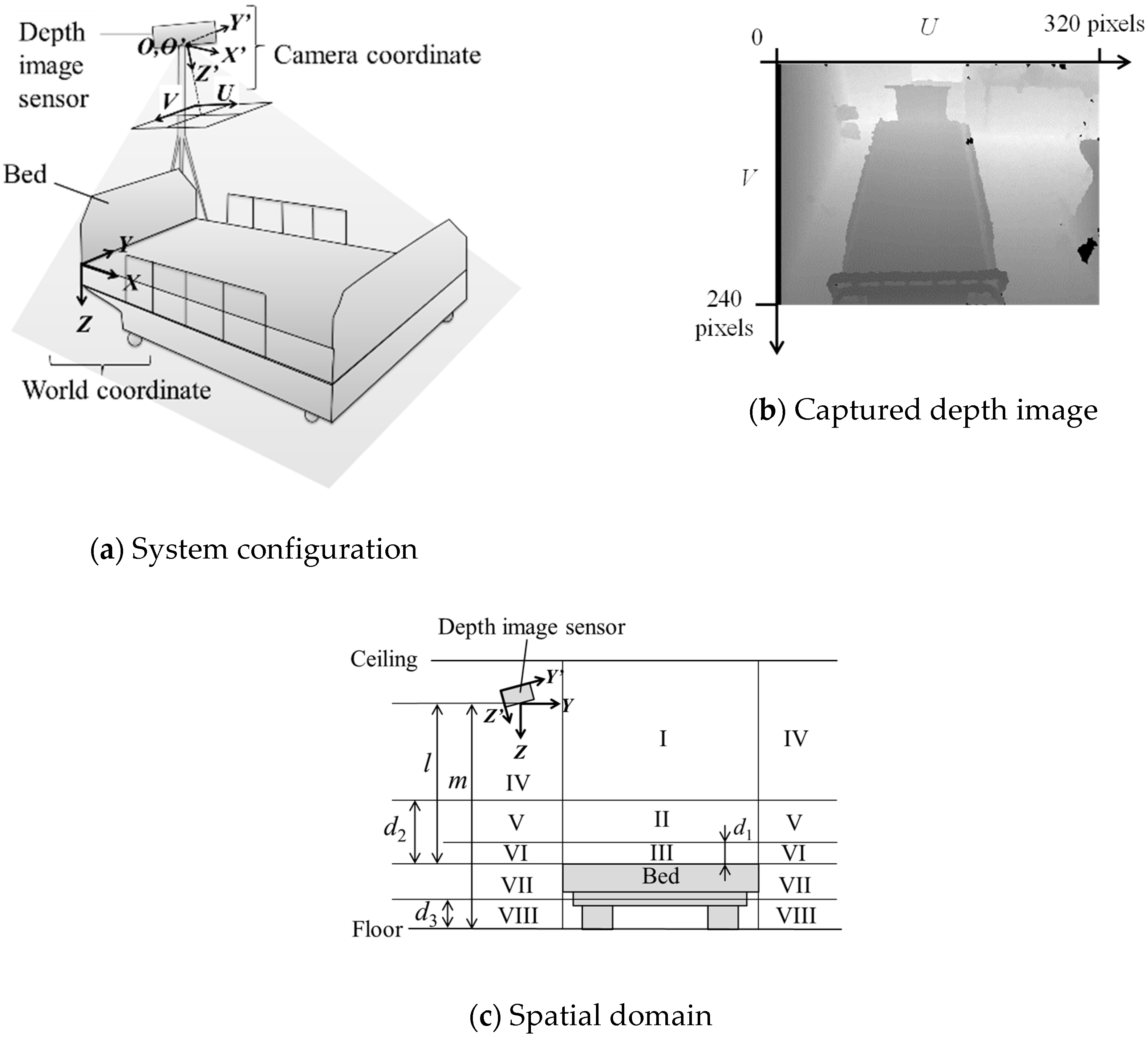
2.1. System Configuration
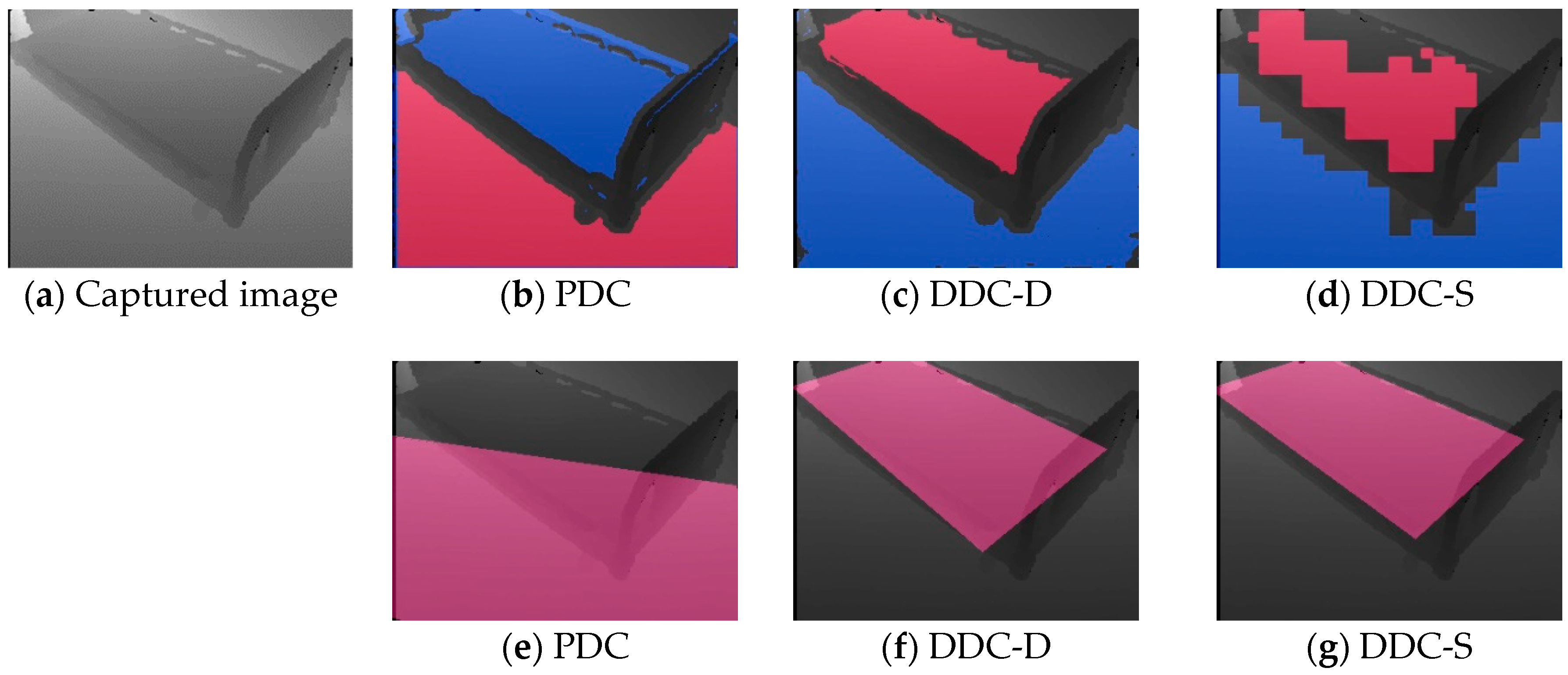
2.2. PCA-Based Depth Sensor-Calibration (PDC) Method
2.3. D-KHT Based Depth-Sensor Calibration (DDC) Method
2.3.1. Step 1: Calculation of Horizontal-Plane Polar Coordinates and
2.3.2. Step 2: Calculation of the Distance between the Sensor and Floor
2.3.3. Step 3: Calculation of Distance between the Sensor and the Bed
2.3.4. Step 4: Calculation of the Floor Surface Φ and Bed-Region Candidate
Alternative 1: DDC Method with High Density (DDC-D)
Alternative 2: DDC Method at High Speed (DDC-S)
2.3.5. Step 5: Calculation of the Bed-Region
2.3.6. Step 6: Automatic Calculation of the Sensor Attitude R and Distances l and m
2.4. Reconfiguration of the Bed Region
2.5. Recognition of the Spatial Domain
3. Experimental Results and Discussions
3.1. Experimental Methods
3.1.1. Experiment 1
3.1.2. Experiment 2
3.1.3. Experiment 3
- 3 points when K correctly indicates the actual corner points using default parameters.
- 2 points when K correctly indicates the actual corner points after changing the parameters.
- 1 point when K deviates from the actual corner points even if any parameter is used.
- 0 point when K does not indicate the actual corner points.
3.1.4. Experiment 4
- PC: Desktop computer, MDV-GX9200B made by Mouse Computer Co., LTD. equipped with Windows 8.1.
- CPU: Intel Core i7-4820K 3.70 GHz
- RAM: 32.0 GB
- Development environment: Microsoft Visual C++ 2010
- Library: OpenCV 2.4.2 and OpenNI
3.1.5. Experiment 5
3.1.6. Experiment 6
3.1.7. Experiment 7
- Install and take an image so that the floor area is larger than the bed area.
- Install and take an image so that the wall area is larger than the sum of the bed and floor areas.
3.2. Results of Pre-Experiment
- .
- , where .
- .
3.3. Results and Discussion of Calibration Experiments (Experiments 1–4)
3.4. Results and Discussion of Bed-Region and Spatial-Domain Experiments (Experiments 5–6)
3.5. Results and Discussion of Two Specific Condition Experiments (Experiment 7)
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). WHO Global Report on Falls Prevention in Older Age; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Vu, M.Q.; Weintraub, N.; Rubenstein, L.Z. Falls in the Nursing Home: Are They Preventable? J. Am. Med. Dir. Assoc. 2004, 5, 401–406. [Google Scholar] [CrossRef]
- Japan Council for Quality Health Care. Project to Collect Medical Near-Miss/Adverse Event Information 2014 Annual Report; Japan Council for Quality Health Care: Tokyo, Japan, 2015. [Google Scholar]
- Berry, S.; Schmader, K.E.; Sokol, H.N. Falls: Prevention in Nursing Care Facilities and the Hospital Setting; UpToDate: Waltham, MA, USA, 2018. [Google Scholar]
- Lapierre, N.; Neubauer, N.; Miguel-Cruz, A.; Rincon, A.R.; Liu, L.; Rousseau, J. The state of knowledge on technologies and their use for fall detection: A scoping review. Int. J. Med. Inform. 2018, 111, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, S.; Thompson, H.; Demiris, G. Fall Detection Devices and their Use with Older Adults: A Systematic Review. J. Geriatr. Phys. Ther. 2014, 37, 178–196. [Google Scholar] [CrossRef] [PubMed]
- Vallabh, P.; Malekian, R. Fall detection monitoring systems: A comprehensive review. J. Ambient. Intell. Humaniz. Comput. 2017, 9, 1809–1833. [Google Scholar] [CrossRef]
- Bian, Z.P.; Chau, L.P.; Thalmann, N.M. A Depth Video Approach for Fall Detection Based on Human Joins Height and Falling Velocity. In Proceedings of the International Conference on Computer Animation and Social Agents, Singapore, 9–11 May 2012. [Google Scholar]
- Mazurek, P.; Wagner, J.; Morawski, R.Z. Use of kinematic and mel-cepstrum-related features for fall detection based on data from infrared depth sensors. Biomed. Signal Process. Control 2018, 40, 102–110. [Google Scholar] [CrossRef]
- Pannurat, N.; Thiemjarus, S.; Nantajeewarawat, E. Automatic Fall Monitoring: A Review. Sensors 2014, 14, 12900–12936. [Google Scholar] [CrossRef]
- Stone, E.E.; Skubic, M. Fall detection in homes of older adults using the Microsoft Kinect. IEEE J. Biomed. Health Inform. 2015, 19, 290–301. [Google Scholar] [CrossRef]
- Banerjee, T.; Enayati, M.; Keller, J.M.; Skubic, M.; Popescu, M.; Rantz, M. Monitoring patients in hospital beds using unobtrusive depth sensors. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 5904–5907. [Google Scholar]
- Perell, K.L.; Nelson, A.; Goldman, R.L.; Luther, S.L.; Prieto-Lewis, N.; Rubenstein, L.Z. Fall Risk Assessment Measures: An Analytic Review. J. Gerontol. 2001, 56, M761–M766. [Google Scholar] [CrossRef]
- Nunan, S.; Wilson, C.B.; Henwood, T.; Parker, D. Fall risk assessment tools for use among older adults in long-term care settings: A systematic review of the literature. Australas. J. Ageing 2018, 37, 23–33. [Google Scholar] [CrossRef]
- Hubbartt, B.; Davis, S.G.; Kautz, D.D. Nurses’ experiences with bed exit alarms may lead to ambivalence about their effectiveness. Rehabil. Nurs. 2011, 36, 196–199. [Google Scholar] [CrossRef]
- Miskelly, F.G. Assistive technology in elderly care. Age Ageing 2001, 30, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Capezuti, E.; Brush, B.L.; Lane, S.; Rabinowitz, H.U.; Secic, M. Bed-exit alarm effectiveness. Arch. Gerontol. Geriatr. 2009, 49, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Madokoro, H.; Shimoi, N. Predication of Bed-leaving Behaviors using piezoelectric non-restraining sensors. J. Sens. Sens. Syst. 2013, 2, 27–34. [Google Scholar] [CrossRef]
- Bruyneel, M.; Libert, W.; Ninane, V. Detection of bed-exit events using a new wireless bed monitoring assistance. Int. J. Med. Inform. 2011, 80, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, M.; Toba, S.; Fukuda, K.; Hori, S.; Abe, Y.; Ozaki, K. Application of Deep Learning to Develop a Safety Confirmation System for the Elderly in a Nursing Home. J. Robot. Mechatron. 2017, 29, 338–345. [Google Scholar] [CrossRef]
- Hori, T.; Nishida, Y.; Aizawa, H.; Murakami, S.; Mizoguchi, H. Sensor network for supporting elderly care home. In Proceedings of the IEEE Sensors, Vienna, Austria, 24–27 October 2004. [Google Scholar]
- Hirabayashi, Y. Monitoring system around bed and indoor [Translated from Japanese]. Japan Patent JP2011-86286A, 28 April 2011. (In Japanese). [Google Scholar]
- Asano, H.; Suzuki, T.; Okamoto, J.; Muragaki, Y.; Iseki, H. Bed Exit Detection Using Depth Image Sensor. J. Tokyo Women Med. Univ. 2014, 84, 45–53. (In Japanese) [Google Scholar]
- Ogura, M.; Koga, M.; Uda, S.; Tanoue, A.; Nakao, N. The development of a bed-exit sensor using a three-dimensional range image. Jpn. J. Med. Instrum. 2015, 85, 487–493. [Google Scholar]
- Gasparrini, S.; Cippitelli, E.; Spinsante, S.; Gambi, E. A Depth-Based Fall Detection System Using a Kinect® Sensor. Sensors 2014, 14, 2756–2775. [Google Scholar] [CrossRef]
- Ni, B.; Nguyen, C.D.; Moulin, P. RGBD-camera based get-up event detection for hospital fall prevention. In Proceedings of the 2012 IEEE International Conference on Acoustics, Speech and Signal Processing (ICASSP), Kyoto, Japan, 25–30 March 2012; pp. 1405–1408. [Google Scholar]
- Liu, C.; Yuen, J.; Torralba, A. SIFT Flow: Dense Correspondence across Scenes and its Applications. IEEE Trans. Pattern Anal. Mach. Intell. 2011, 33, 978–994. [Google Scholar] [CrossRef]
- Fischer, M.A.; Bolles, R.C. Randam sample consensus: A paradigm for model fitting with applications to image analysis and automated cartography. Commun. ACM 1981, 24, 381–395. [Google Scholar] [CrossRef]
- Nurunnabi, A.; Belton, D.; West, G. Robust statistical approaches for local planar surface fitting in 3D laser scanning data. ISPRS J. Photogramm. Remote Sens. 2014, 96, 106–122. [Google Scholar] [CrossRef]
- Limberger, F.A.; Oliveira, M.M. Real-time detection of planar regions in unorganized point clouds. Pattern Recognit. 2015, 48, 2043–2053. [Google Scholar] [CrossRef]
- Vera, E.; Lucio, D.; Fernandes, L.A.; Velho, L. Hough Transform for real-time plane detection in depth images. Pattern Recognit. Lett. 2018, 103, 8–15. [Google Scholar] [CrossRef]
- Arthur, D.; Vassilvitskii, S. k-means++: The advantages of careful seeding. In Proceedings of the Eighteenth Annual ACM-SIAM Symposium on Discrete Algorithms, New Orleans, LA, USA, 7–9 January 2007; Society for Industrial and Applied Mathematics: Philadelphia, PA, USA, 2007; pp. 1027–1035. [Google Scholar]
- Canny, J. A Computational Approach to Edge Detection. IEEE Trans. Pattern Anal. Mach. Intell. 1986, 8, 679–698. [Google Scholar] [CrossRef]
- Kumar, M.; Saxena, R. Algorithm and Technique on Various Edge Detection: A Survey. Signal Image Process. Int. J. 2013, 4, 65–75. [Google Scholar]
- Komagata, H.; Onotsuka, N.; Nakano, M.; Kase, H.; Murayama, D.; Ishikawa, M.; Shinoda, K.; Kobayashi, N. Proposal of Space Recognition Method for Bed Fall Prevention Using Depth Image Sensor. Forum Inf. Technol. 2017, 16, 211–213. (In Japanese) [Google Scholar]
- Lam, W.C.; Lam, L.T.; Yuen, K.S.; Leung, D.N.; Yuen, S.Y.K. An analysis on quantizing the hough space. Pattern Recognit. Lett. 1994, 15, 1127–1135. [Google Scholar] [CrossRef]
- Ratcliff, R. Methods for dealing with reaction time outliers. Psychol. Bull. 1993, 114, 510–532. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PDC | DDC-D | DDC-S | ||
|---|---|---|---|---|
| 1. Height of bed (cm) | Average | 46.09 | 45.94 | 45.96 |
| Standard deviation | 0.93 | 0.92 | 1.05 | |
| 2. Width of bed (cm) | Average | 94.25 | 96.29 | 93.72 |
| Standard deviation | 4.64 | 5.15 | 5.39 | |
| 3. Visual observation (point) | Average | 3.00 | 2.94 | 2.06 |
| 4. Calibration time (ms) | Average | 1400 | 964 | 243 |
| Standard deviation | 110 | 71 | 65 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komagata, H.; Kakinuma, E.; Ishikawa, M.; Shinoda, K.; Kobayashi, N. Semi-Automatic Calibration Method for a Bed-Monitoring System Using Infrared Image Depth Sensors. Sensors 2019, 19, 4581. https://doi.org/10.3390/s19204581
Komagata H, Kakinuma E, Ishikawa M, Shinoda K, Kobayashi N. Semi-Automatic Calibration Method for a Bed-Monitoring System Using Infrared Image Depth Sensors. Sensors. 2019; 19(20):4581. https://doi.org/10.3390/s19204581
Chicago/Turabian StyleKomagata, Hideki, Erika Kakinuma, Masahiro Ishikawa, Kazuma Shinoda, and Naoki Kobayashi. 2019. "Semi-Automatic Calibration Method for a Bed-Monitoring System Using Infrared Image Depth Sensors" Sensors 19, no. 20: 4581. https://doi.org/10.3390/s19204581
APA StyleKomagata, H., Kakinuma, E., Ishikawa, M., Shinoda, K., & Kobayashi, N. (2019). Semi-Automatic Calibration Method for a Bed-Monitoring System Using Infrared Image Depth Sensors. Sensors, 19(20), 4581. https://doi.org/10.3390/s19204581