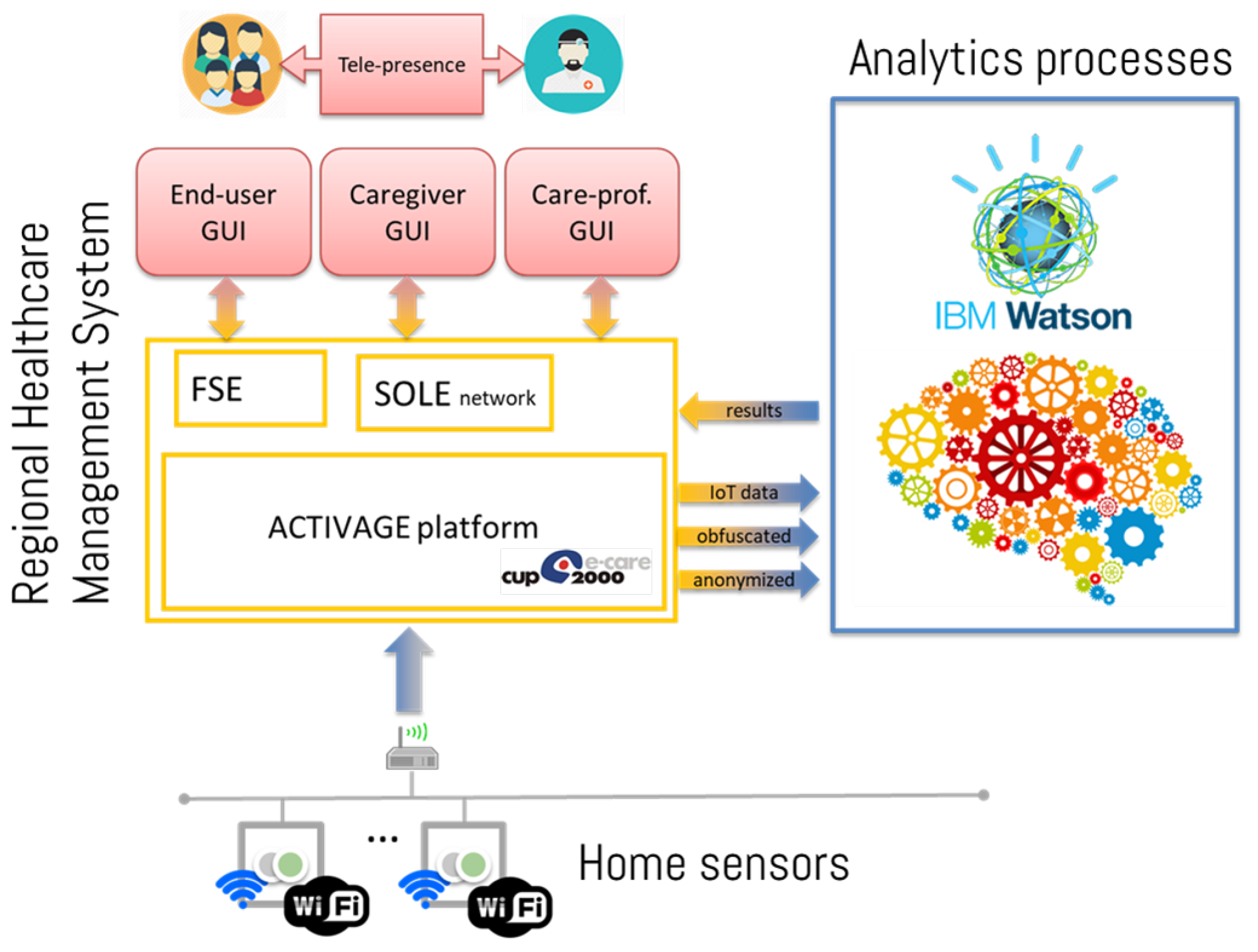
As mentioned, the main concept of the ACTIVAGE DS-RER project consists of enhancing current care management practice by providing insights from user-specific “behavioral” analysis: the approach aims at creating a multi-dimensional vision of care, allowing for a more sensible personalization. To this purpose, a comprehensive framework has been devised and implemented, consisting of:
Besides technical functionality, it is relevant to assess the actual benefit brought to both the end-user and the care provider. This depends on the effective integration of the proposed solution into the care ecosystem, which involves a large number of different stakeholders. Hence, the framework strictly needs to be validated against real-world use cases: within the scope of the ACTIVAGE DS-RER project, a comprehensive trial procedure has been designed. This section therefore deals with the framework architecture and its components, as well as with the trial design. All technical design has been completed, and the trial is currently under way. Functional validation results are available already, based on data streams coming from pilots. Assessing evidence of clinically-relevant outcomes (based on healthcare system feedback) is among the long-term goals of the current trial and is expected at a later stage.
2.1. IoT Wireless Sensor Kit
The IoT wireless sensor kit is composed of several different elements, which are used to continuously monitor and extract relevant behavioral information. In order to minimize the installation burden, sensors exploit the standard Wi-Fi (IEEE 802.11 b/g/n) communication infrastructure. While most diffused home sensing networks use dedicated networks (e.g., ZigBee, Bluetooth, Z-wave, etc.), the Wi-Fi option allows for easily connected devices to the main home network (i.e., sharing common infrastructure), with no need of a dedicated home sensor hub. This makes installation straightforward and reliable. In addition, the resulting approach is highly flexible and expandable, with no need for reconfiguring the network while adding or removing devices. The ACTIVAGE DS-RER sensor kit currently includes:
Passive InfraRed (PIR) sensors for motion detection, suitable for tracing room occupancy. Such sensors are deployed in users home by fixing them to a wall in the environment where motion needs to be captured
Magnetic contact sensors, useful for monitoring open/close states of different objects. For example, interactions with doors, drawers and medical cabinets can be easily detected with such sensors.
Bed occupancy sensor, useful in tracing sleeping patterns; detection of presence is achieved by a pressure-sensitive resistive pad, usually placed under the mattress. Such signal is read by the sensor module, attached to the bed frame.
Chair occupancy sensor, to gather information on how much time and when a user sits on a chair/armchair/sofa; physical sensing technology is the same as for the bed occupancy sensor.
Toilet presence sensor, specifically developed to keep track of daily toilet use. The sensing element is an active IR sensor with an IR illuminator and a photo-detector: this setup guarantees ranging capability and can be much more selective for close interactions detection, with respect to a PIR. Indeed, the sensor is fixed in close proximity to the toilet.
The whole sensor family was designed from scratch, taking care of both hardware and firmware design. This was necessary since no commercial WiFi sensor kit was available, providing such specific functions. In addition, interoperability and data security constraints were taken into consideration: since the ACTIVAGE project deals with information related to personal health, regulations require that the full data journey is known and the information is stored in national servers, hosted by authorized operators. The home devices kit is completed by a pill dispenser, suitable for reminding the user at medicine-taking time and for assessing the user’s compliance to the prescribed therapy. The pill dispenser was based on available hardware, and its software was updated to fit the project environment (Wi-Fi networking, cloud access).
The home infrastructure thus follows a genuine IoT approach, with sensors directly connected to the cloud, without any intermediate gateway. At any time, any element of the IoT wireless sensor kit can join the WiFi network by means of standard Wireless Protected Setup (WPS) procedure, which simplifies the device deployment. All devices are built around the same microcontroller and network processor unit, namely the CC3220 SoC (System on Chip) by Texas Instruments (Dallas, TX, USA): it is a Wi-Fi certified product, featuring IoT networking security, device identity and keys, optimized for low power management. The certified stack implements both IPv4 and IPv6 protocols, with industry-standard, optimized BSD sockets (both TCP and UDP), secured by SSL/TLS.
Data transmission towards the cloud is performed using the MQTT (
Message Queue Telemetry Transport) communication protocol. MQTT is a lightweight, data-agnostic protocol, particularly suitable for IoT applications, since it it relies on a broker for exchanging data between publishers and subscribers, and it supports various levels of
Quality of Service (QoS). In this project, all messages are sent with a QoS of 2, i.e., they are sent exactly once, with a unique reception confirmation. The Mosquitto [
18] MQTT broker was chosen to receive and handle all device communications, since it is a mature technology, widely-adopted, and has an active, open-source community. After reaching the MQTT broker, a Fiware IoT agent [
19] parses the messages, determines the sensor-person association, and stores the payload data into the appropriate Data Base (DB) table.
In order to guarantee data security, all traffic towards the cloud is encrypted by means of SSL/TLS protocol: certificates signed by a public Certification Authority guarantee the identification and proper authorization of devices.
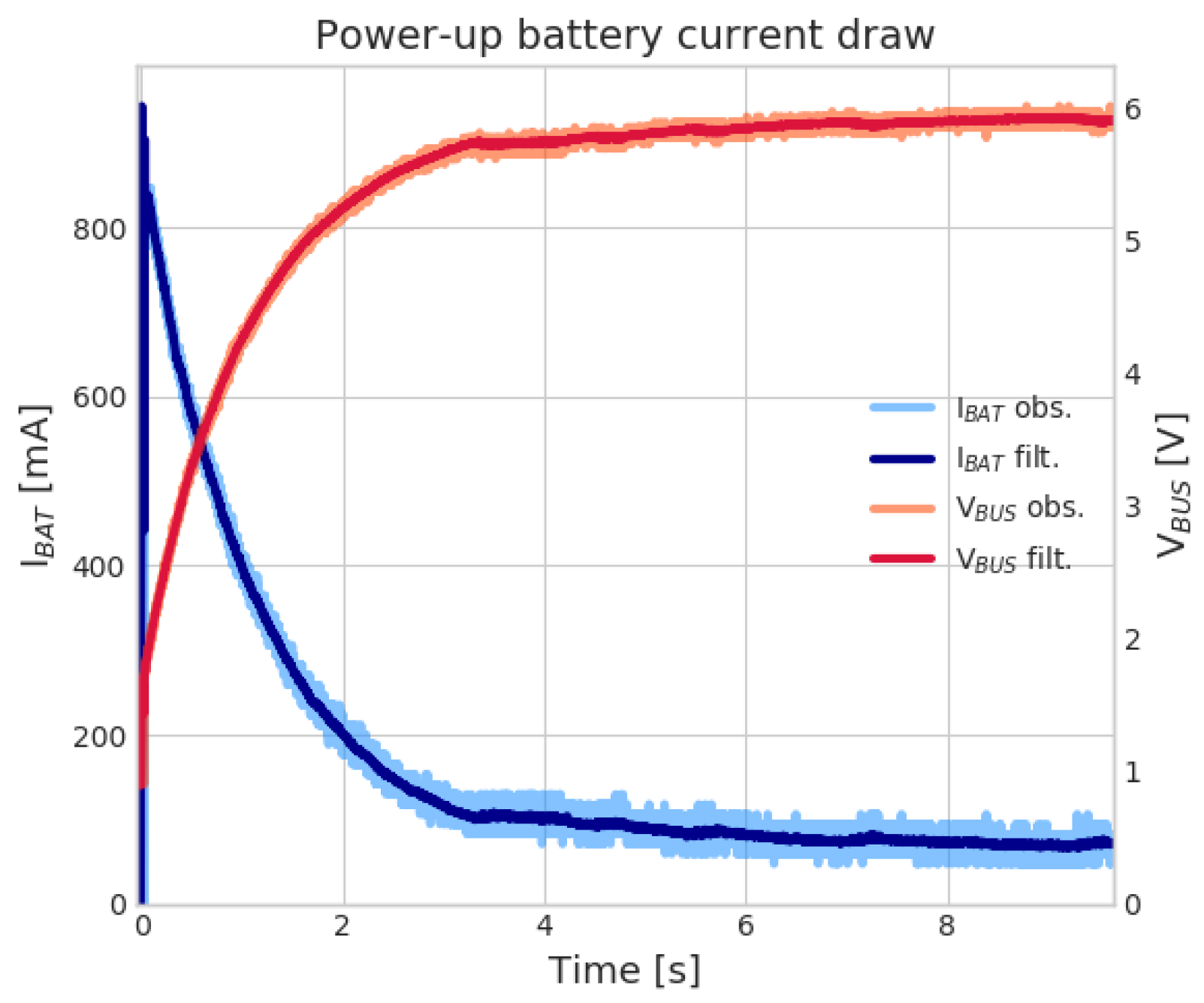
To keep the installation in users’ homes less intrusive as possible, all devices are battery-powered: besides being safer in terms of electrical hazard, the absence of power cords allows unconstrained placement of sensors in the home environment. Nonetheless, battery operation comes with its own disadvantages, mainly related to the limited energy budget, the reduced capability in terms of surge current sourcing and the rate of self discharge. All these factors have a great impact on the device operating time and pose constraints on devices’ WiFi communications, which are, by far, the most power-intensive activities. In order to compensate for reduced battery current sourcing capability, the IoT wireless sensor kit relies on super-capacitors in the power section, which makes it possible to use primary alkaline cells, this reducing maintenance costs. Alkaline batteries, in fact, tend to exhibit higher ESR (Equivalent Series Resistance) and generally feature a more rapid performance degradation, compared to Lithium-based ones. At the very end of their discharge curve, the alkaline battery’s ESR is so high that it prevents high output current sourcing: this can seriously hinder device operation and reliability (faulty connections). The adoption of super-capacitors is common in this field and allows for offloading batteries from supplying high peaks; during normal operation, batteries will approximately supply the average current that the sensor draws, due to the higher source impedance with respect to super-capacitors: such current is relatively low, given that the sensor duty-cycle is minimal. Batteries are required to supply high currents just at the very beginning of their operation (i.e., to charge the super-capacitor up to rated voltage), when the ESR is at its minimum. This architectural pattern effectively exploits the full battery discharge curve (even in the final, high-ESR region). In the present design, two 470 mF, 4.2 V rated super-capacitor units are stacked in series, to accommodate a 4xAA alkaline battery input. This provides a low-impedance path to supply the buck regulator high amounts of transient current, required during the transmission phase. Finally, power saving capability is achieved mainly through two factors:
Careful selection of low-power and low-quiescent current devices. For instance, FRAM (Ferroelectric Random Access Memory) memory is leveraged for non-volatile storage, due to their lower power consumption (compared to flash memories); low quiescent current switching regulator and analog signal conditioning ICs are selected as well, to keep sleep-mode currents as low as possible.
Efficient scheduling of messages: instead of streaming data (e.g., movement detected by a PIR) as soon as an event occur, such information is temporarily committed to on-board non-volatile storage and sent at regular intervals (e.g., hourly). This prevents multiple WiFi connection and disconnections, effectively lowering average radio usage.
By means of such design strategy, battery lifetime well in the practical range can be achieved, in the order of several months, as detailed in
Section 3.1 below.
2.3. Data Analysis
Although suitable for unobtrusive and continuous acquisition, behavioral data produced by home sensors lacks a straightforward and absolute interpretation, especially in terms of correlation with health and wellness status: human behaviors are inherently variable, from person to person and from time to time. Hence, it is not possible to define an absolute reference to detect behavioral anomalies and features: a personalized interpretation scheme is needed. Apart from gross anomalies, relevant trends and patterns have to be evaluated in a relative fashion, i.e., by checking behavioral changes with respect to individually personalized profiles. This calls for learning capabilities in the data analytics section.
Recently, artificial intelligence techniques have been applied to smart home data, aiming at predicting user’s behavior or activity [
12]. For example, the CASAS system [
21] was specifically designed to perform activity of daily living (ADL) recognition from a network of home sensors: good results were achieved with Support Vector Machine (SVM) classifiers. Recognized ADLs can also represent the input to higher-level models that aim at assessing the regularity of a user’s pattern. For example, in [
22], a sensor data clustering approach is adopted to obtain insights into patterns and, at the same time, to detect deviant ones. Moreover, the authors in [
23] demonstrate that the extracted daily living patterns and their relative changes can be good predictors of cognitive and mobility tests performed by clinicians. In the literature, ADL discovery and classification typically rely on two factors: (i) a large number of sensors (especially PIR motion detectors), (ii) a significant corpus of user-annotated data. Both such conditions, however, are hardly compatible with real-life scenarios, due to obtrusiveness constraints.
A less demanding approach could be to use very specific sensors [
24], more expressive from a semantic point of view. For example, electric appliance monitors, pressure pads, etc. can be more straightforwardly linked to specific behavioral features. Although having a narrower scope, they allow a more precise and fine-grained targeting of specific actions. Within the ACTIVAGE project environment, most IoT sensors (introduced in
Section 2.1) provide action- and subject-specific information indeed. Such approach is particularly suited for persons living alone (for which continuous monitoring is especially attractive). When multiple persons populate the monitoring scene, some sensors (PIR and toilet presence sensors, most notably) cannot distinguish between different persons. Trends and anomalies can be considered anyway, but care in the interpretation is needed, since anomalies may be triggered by other users. Nonetheless, detecting such conditions in aggregated sense is still important, triggering further investigations by involved care managers. Moreover, it is worth remarking that the analyses which can be practically carried out are necessarily unsupervised: any user feedback or annotation is unfeasible or unpractical. Therefore, all analysis methodologies are focused on data interpretation (in the long term), rather than future data prediction: this is, indeed, particularly useful for care managers, who need to analyze current behaviors and detect meaningful deviations within them.
As mentioned, the DS-RER approach is applicable to many different target behaviors; however, for clearer presentation purposes, the following subsections focus on two aspects: toilet usage and bed/rest routines, which were suggested by stakeholders interviewed in co-creation sessions as important factors to be quantitatively and qualitatively monitored in post-stroke treatment.
Monitoring sleep habits of individuals after the stroke event is relevant indeed: sleep disorders, such as hypersomnia, excessive daytime sleepiness and insomnia are observed in up to 40% of individuals with chronic stroke (defined as more than six months following stroke) and 70% of those with acute stroke [
25]. Proper resting is key to physical and mental health indeed [
26,
27,
28]: sleep disturbances can lead to short-term and long-term negative patient outcomes [
29], may reduce the ability to learn new motor skills [
30] and increase the risk of a stroke relapse [
31].
Detailed studies on sleep quality analysis are available in the literature, based on complex polysomnography setups [
32,
33] radio-frequency imaging [
34] or video analysis [
35]. Such approaches, however, do not fit well in the DS-RER approach, which focuses on low-cost, low-intrusive and self-manageable solutions instead. Similarly, monitoring of toilet usage patterns is relevant for the population at hand. Many studies in literature [
36] confirm that up to 25% of acute post-stroke patients experience urinary incontinence problems even one year after the adverse event. This condition was also found positively linked with of increased morbidity, disability, and institutionalization rates in the post-stroke patient [
37].
It is worth underlining that such indicators do not automatically trigger any action or therapy adjustment, but they just provide the GP or the care-manager with deeper insights about changes and anomalies in patient’s lifestyle, drawing their attention towards details which might remain unnoticed otherwise. Evaluating such information into the general framework of patient’s health is the responsibility of skilled professionals, who can assess their relevance in a personalized picture.
The DS-RER approach is general, and the methodologies detailed in the next sections can be easily adapted to many different use cases behavior; however, for conciseness’ sake, the rest of the paper will focus on bed/rest routines and toilet usage, which will serve as application examples for analytics methods explanation
2.3.1. Regression Framework and Applications
It was considered that the number of daily and, possibly, nightly toilet visits should be counted and monitored, looking for meaningful behavioral changes, possibly correlated to health issues. Given the nature of the problem at hand, the natural framework for carrying out such explanatory analysis is Generalized Linear Models (GLM). In particular, the special case of Poisson regression is used, since it accounts for discrete-valued observations. Poisson Regression assume that the count data
can be modeled as independently Poisson distributed random variables, under the effect of
k covariates
:
where
is a vector of
parameters (for the
k covariates, plus a bias term) fitted on observed data. In particular, it is known that the conditional mean count, given the vector of covariates
is:
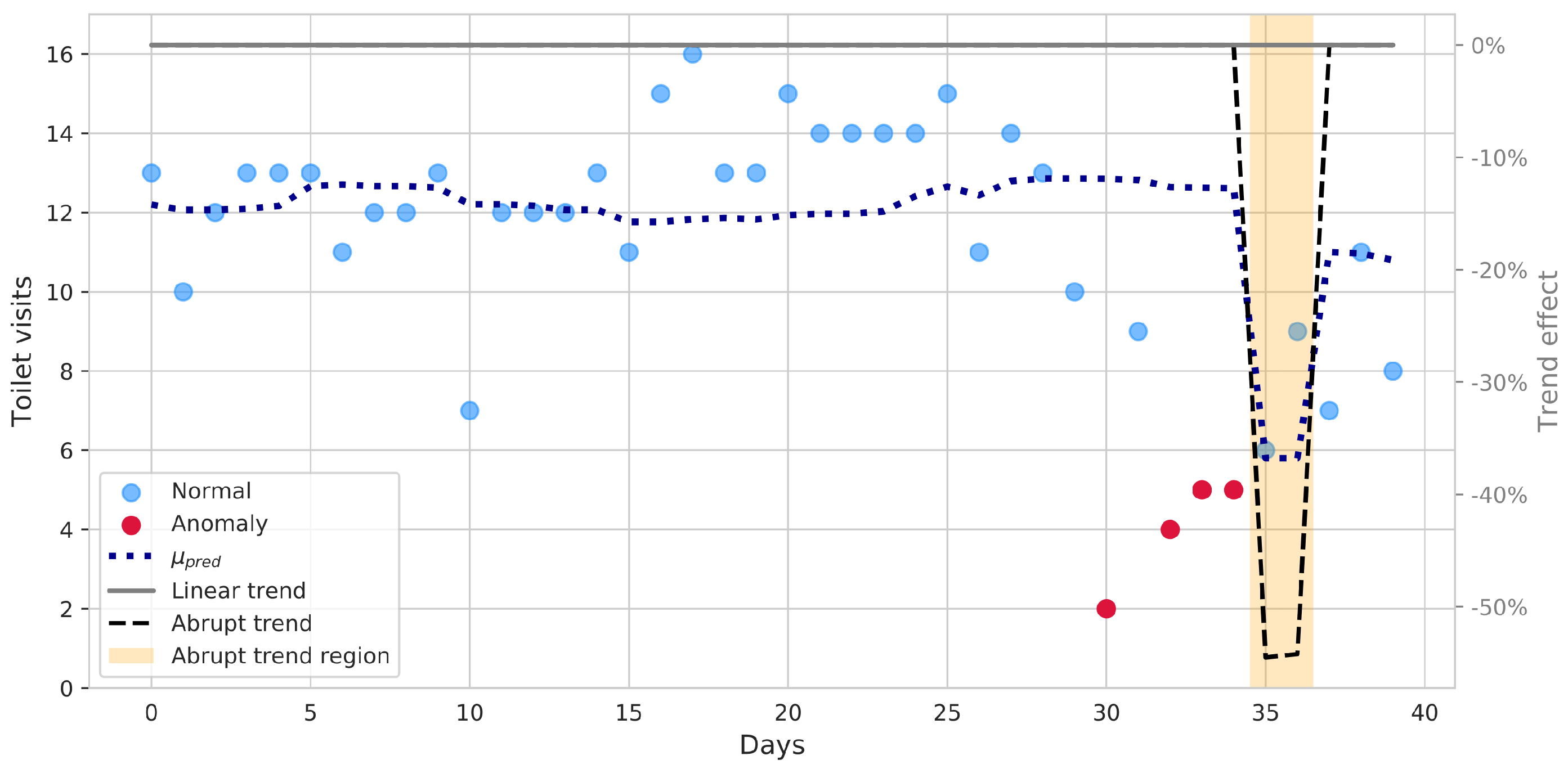
It is also known that the marginal effect of a single factor is multiplicative, i.e., a unit increment of a given covariate j results in a multiplication of the expected counts by a factor equal to the given parameter . In the case at hand, at each point in time , the last 30 daily counts are modeled using the Poisson regression framework, under the effect of a bias term (baseline) and three covariates:
an abrupt trend, focusing on the most recent days (e.g., the last 5).
an intermediate period, before the abrupt trend that allows for accounting for a past abrupt trend, without raising the baseline too much.
a linear trend, to model long-term trends over the whole window.
This model is useful to reliably detect the presence of statistically significant factors, such as recent, abrupt behavior changes. For the analysis, only statistically significant factors are retained (i.e., with a p-value < 0.05) and used for model fitting, ensuring proper explanatory power. If, for example, a significant abrupt or linear trend is detected by the model, an alert can be triggered to automatically notify care professionals. At the same time, data points that fall too far from the predicted mean counts (e.g., outside the region that contains 95% of the distribution at that time point) can be labeled and reported as unexplained, possibly worthy of further analysis.
Of course, such regression frameworks can be easily adapted to real-valued values. For example, the Rests Analysis Service (RAS) aims at providing personalized periodic reports on bed usage, in order to identify significant individual changes in the short and long term. The service analyzes data collected by bed occupancy sensors and, if available, it combines them with information from other sensors, in order to confirm user movements or absence from bed, therefore reducing errors. Short bed presences, unrelated to sleep activity (as it frequently happens in real-life data), are filtered out. On the other hand, data fusion from other sensors is leveraged to confirm the end of a rest period.
Furthermore, the extracted information about factor strengths and intercepts may act as descriptive statistics in higher-level models. For example, it is possible to cluster different subjects into groups based on their features extracted with the help of such models: this can deliver further insights to care managers, which may detect similarities between care cases. Comparison between time series of different periods or different subjects is also supported by means of cosine similarity scores.
2.3.2. Sensor Profiles and Applications
Another important aspect in the analysis of users’ behavior is the monitoring of temporal patterns, i.e., habits or routines. Actually, users may exhibit different habits, variable from person to person and, for the same person, from time to time. Even though explained in the following by means of the rest analysis example, this is a general topic, applicable to all data streams from the IoT sensor kit. With reference to resting habits, the necessity of modeling day-long patterns arises from the following considerations: for instance, in some cases, people rest in bed only overnight, whereas in some others daytime naps may be taken. Such routines might also shift temporally or dilate/shrink in duration. Thus, it is not possible to account for all these variabilities with just a single indicator (e.g., amount of time in bed). In order to process such information within a unified framework,
Sensor Profiles (SP) are introduced. By breaking up a day into a suitable number of time bins (e.g., 15, 30 or 60 min intervals), SP model the expected probability of having a sensor active within each bin. It is worth remarking that the main purpose of SP analysis is to capture temporal habits rather than computing precise events’ duration. Indeed, each time bin carries the information whether the given sensor was seen sufficiently active in that time frame (either a minimum number of activations or minimum continuous active time): this allows for discarding short or non-meaningful interactions. The choice of the SP bin size plays an important role: setting bins that are too long may lead to a suppression of relevant behavioral information, whereas bins that are too short may yield noisy estimates. A bin width of 30 min was selected as good trade-off for sleep-pattern analysis. SP are then constructed as follows: for each bin, for each day, if the bed sensor is seen active for at least
min, it is marked as a positive realization for that day (i.e., a value of 1 is associated with the bin); otherwise, it is marked as a negative realization (i.e., a value of 0). Thus, each time bin can be represented as a random variable
, whose realizations are drawn according to the following rule:
where
is the
i-th realization, corresponding to day
i, of the
j-th time bin,
is the time the bed sensor was active (i.e., person laying in bed) on day
i in time bin
j. It is then straightforward to model the time bin
as a
random variable: the probability parameter
p can then be interpreted as the expected probability of finding the subject in bed during the considered time bin. Applying the principle of Maximum Likelihood Estimation (MLE), it is well known that
, where
is the estimated probability parameter,
are the number of positive realizations (i.e., days with the sensor seen active, during the considered time bin), and
N is the total number of realizations (i.e., days). Of course, the underlying simplifying assumption is that each day is independent of the others. Confidence intervals can also be estimated, in order to quantify the
parameter uncertainty. The procedure can be repeated for each time bin
, with
, therefore modeling the probability of bed presence throughout the day.
The SP framework also lends itself well to detect behavioral pattern changes. In fact, two periods may be compared to detect statistically significant deviations in time bin estimated probabilities. For each couple of time bins , with associated probabilities , it is possible to compare them by applying the binomial proportion statistical hypothesis testing framework. This can take the form of analytic tests, such as chi-square, or other Bayesian methods using MCMC (Markov Chain Monte Carlo) simulations, which can be more robust (i.e., less extreme) in reduced sample size problems. The resulting p-values can adjusted using the Holm–Bonferroni procedure, in order to account for multiple comparisons of all time bins.
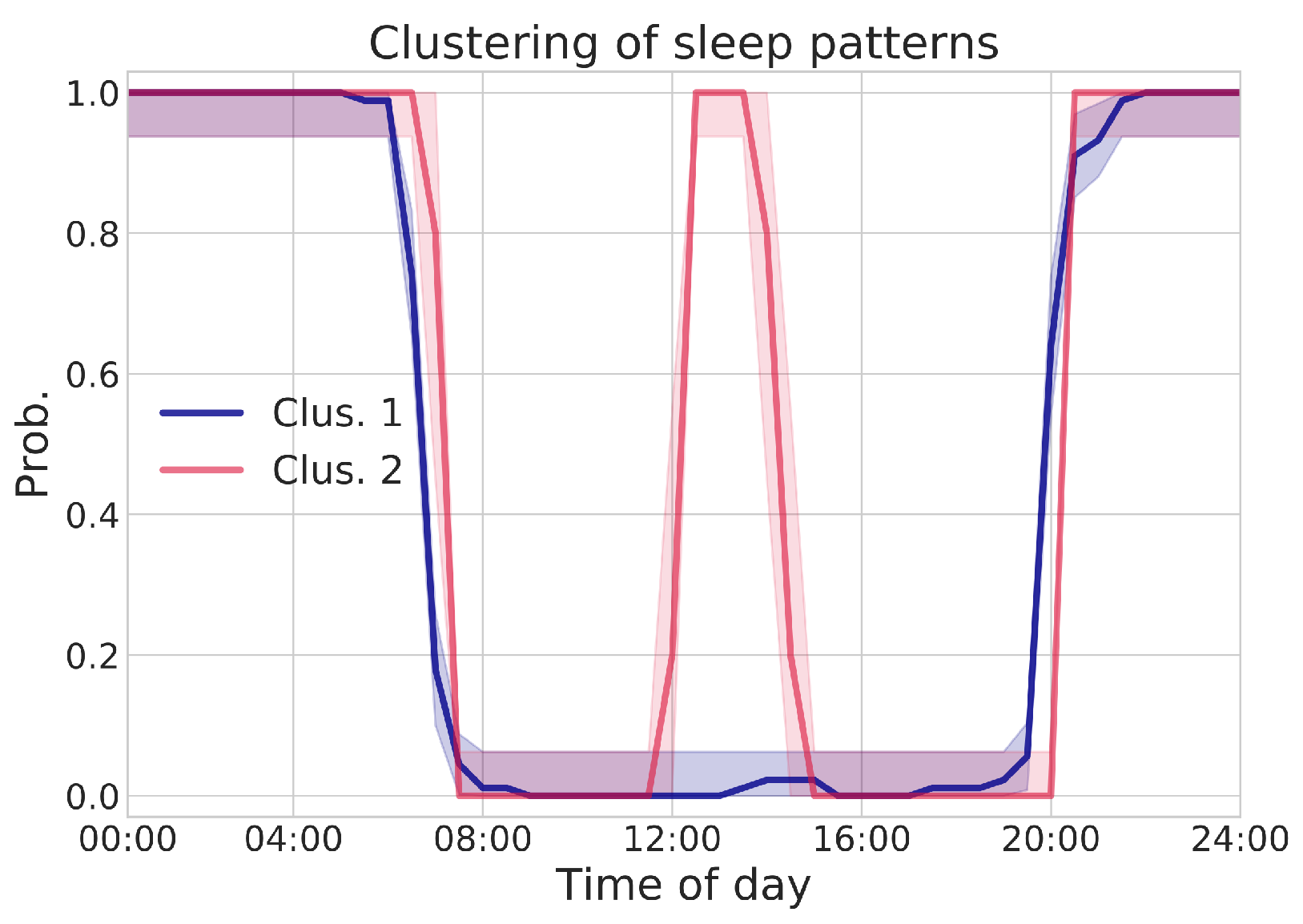
The SP framework also allows for performing daily pattern clustering. As previously mentioned, considering a feature vector composed of daily time bins’ realizations (where superscript i is referred to a single day), it is possible to perform pattern clustering by means, for example, of Agglomerative Clustering. This procedure allows for relaxing the assumption about the existence of a unique, average behavior: a person may exhibit more than one pattern. For example, a user may spend more time in bed during weekends, or may want to take a short rest in bed after lunch. This analysis may provide further insights on subjects’ habits.
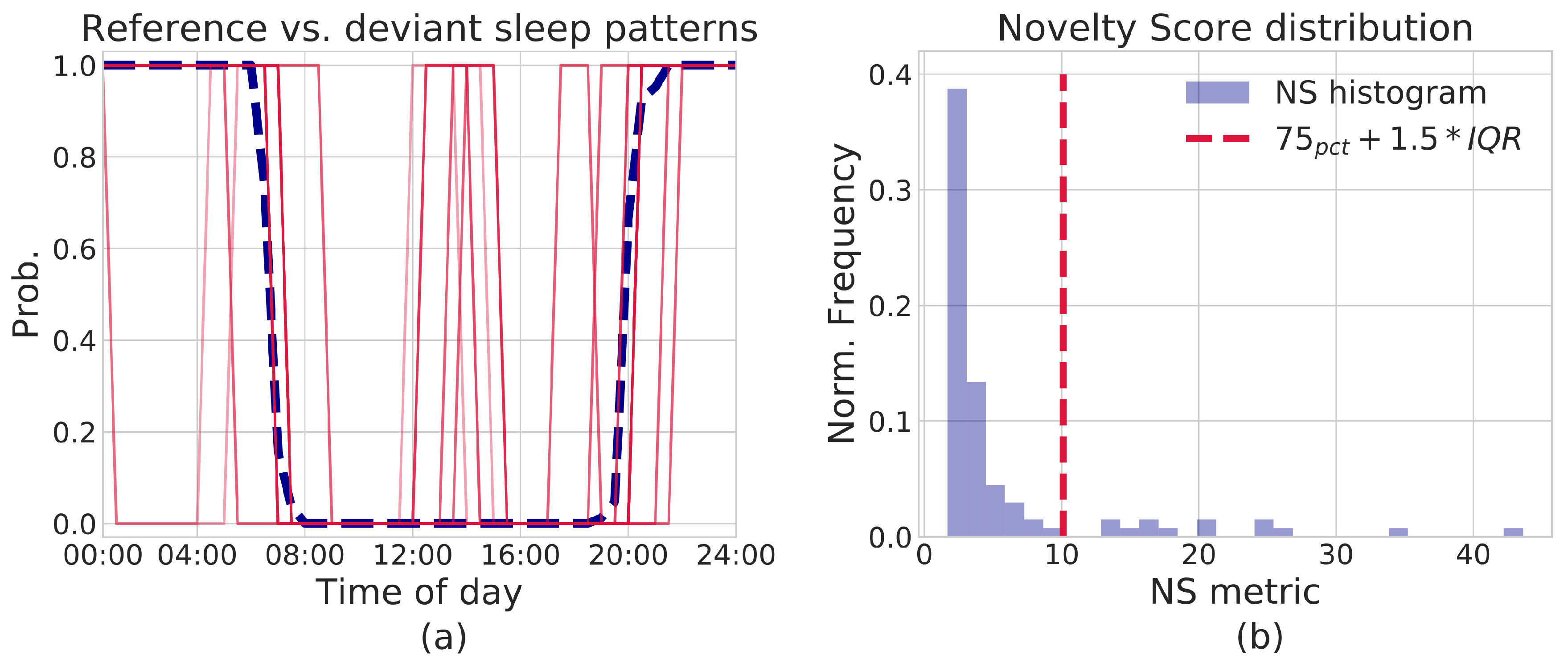
Finally, within the SP framework, it is also possible to derive a
Novelty Score (NS), to detect changes of a single day with respect to a reference period. In particular, let us suppose to have extracted a prototype pattern from said reference period, represented by a vector
(each
is the MLE estimate
of the time bin’s probability parameter). As mentioned above, for a given day
i, let us then consider its vector of realizations
; by assuming conditional independence between time bins
j, it is possible to compute the log-likelihood of a day
, with respect to the model
, as the sum of the log-likelihoods of each time bin realization
. The negative log-likelihood can then be taken as the NS indicator:
The greater the difference of the day-vector with respect to the reference prototype , the higher the NS score is. This allows for flagging deviant days as those with a sufficiently high NS score.
2.4. Trial Design
As previously mentioned, the ACTIVAGE DS-RER project was designed to eventually evaluate IoT-based behavioral monitoring as a mean for improving care continuity of persons undergoing stroke recovery.
Besides technological innovation, chances of practical success of the approach strictly depend on the effective integration into current care practices. This involves acceptance from care professionals and seamless cooperation with existing care-supporting tools (e.g., Electronic Health Record management): a user-centric service design methodology was strictly followed in devising service features, directly involving General Practitioners (GP), neurologists, formal caregivers, physiotherapists and actual patients. Actual impact of ACTIVAGE service in improving care effectiveness, instead, needs to be verified through a posteriori rigorous evaluation of trial outcomes. Thus, the proposed approach was formally designed as a clinical study, adopting a strict Randomized Controlled Trial (RCT) protocol. All methodologies and evaluation procedures were submitted to the Local Health Authority’s (LHA) Ethical Committee, receiving full approval (Resolution nr. 0002775, dated 16/01/2018). Up to 200 stroke-recovery patients are being recruited, consisting of over-65 years old persons with an assessed vulnerability index from vulnerable up to moderately frail (levels 4–6 over a full range of 9). As of RCT protocol, recruited subjects are split into active and control groups, following a blind randomization process (to eliminate any selection bias). Both populations will undergo the standard protocols for stroke recovery; in addition, for the active group, such standard care practices are integrated with behavioral analysis components.
Data management is compliant with EU regulations, with details about organizational and legal issues going beyond the scope of this paper. In order to assess the impact of the ACTIVAGE solution, several performance indexes are compared among two groups, including, for instance, the re-hospitalization rate, days spent at the hospital, and complications related to co-morbidities. In addition, periodic assessment of the patient condition are carried out by means of clinically-validated questionnaires, including: Barthel index [
38] for Activities of Daily Living (ADL) performance scoring, the Lawton Instrumental Activities of Daily Living Scale (IADL) [
39] for assessing ability to perform task using common appliances, the Kane scale for social interaction assessment [
40] and the UCLA Loneliness Scale [
41]. A detailed discussion of such indicators falls beyond the scope of this technical paper: they are mentioned here to highlight that the outcome evaluation is carried out on a multi-dimensional perspective, including evaluation tools commonly used in the application context. Conforming to familiar work environment and tools should foster acceptance by the care professional indeed.

 ,
, 







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}