Use of Multiple EEG Features and Artificial Neural Network to Monitor the Depth of Anesthesia


Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects and EEG Recordings
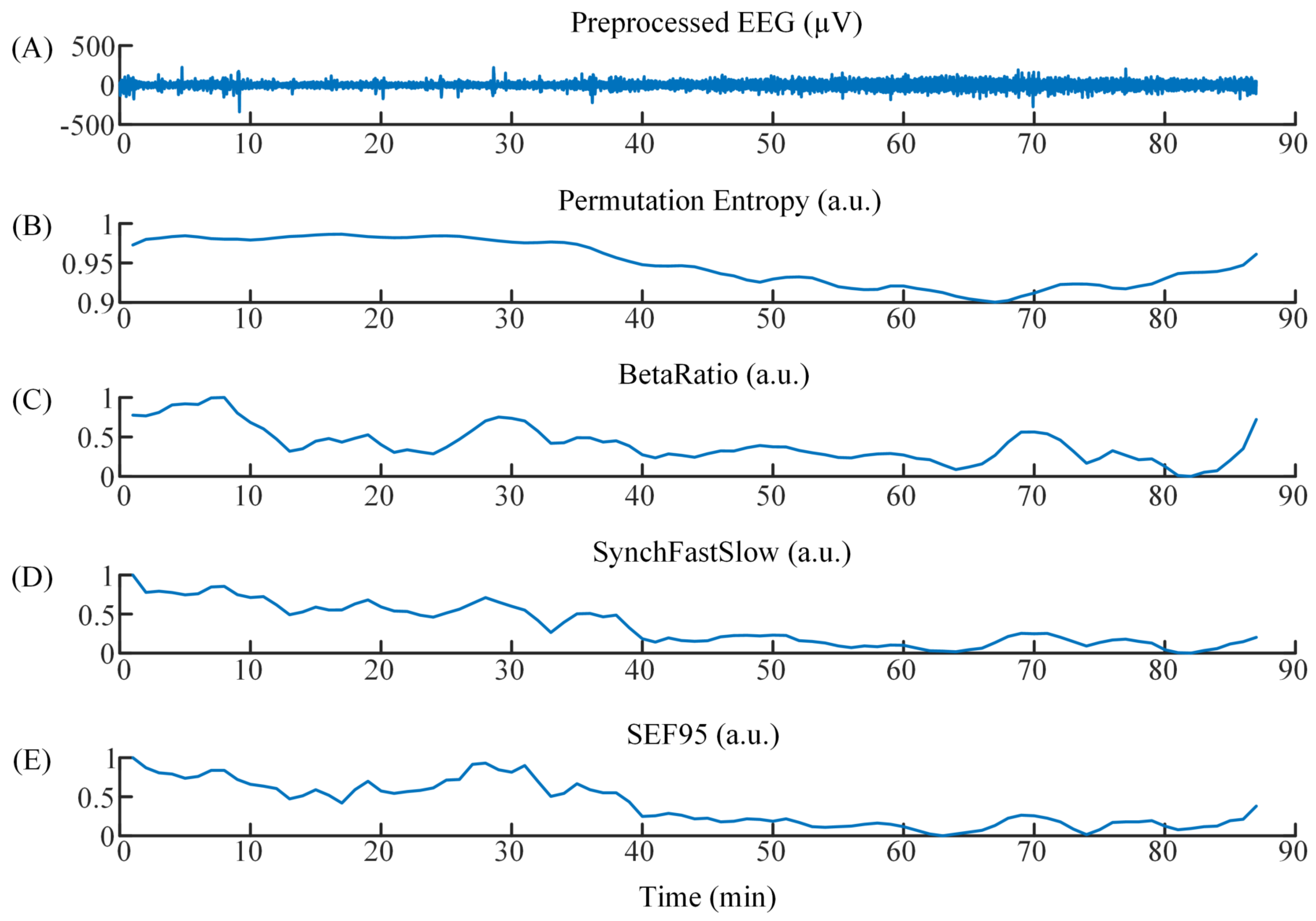
2.2. EEG Processing
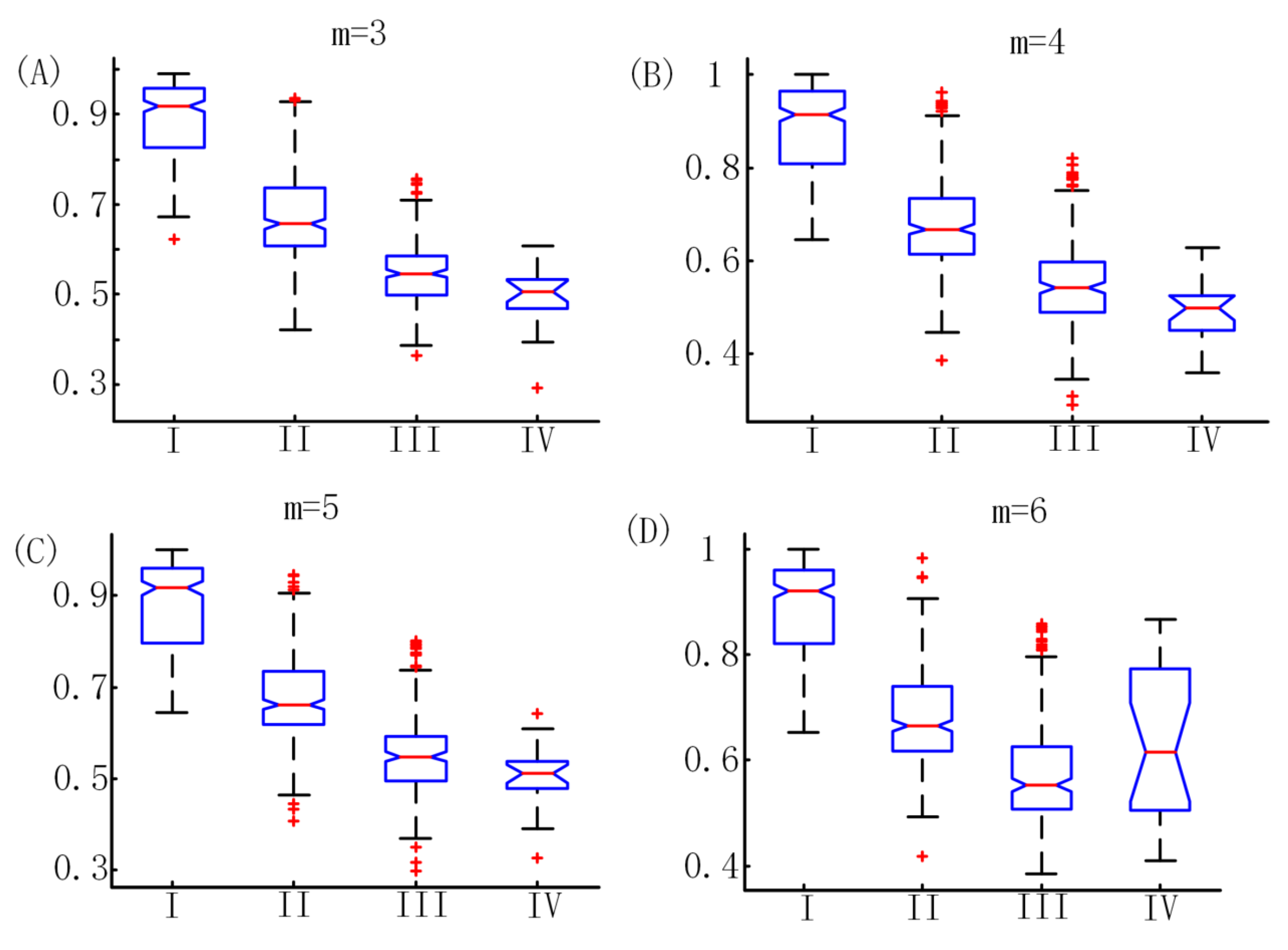
2.3. Permutation Entropy Algorithm
2.4. Frequency-Domain Algorithm
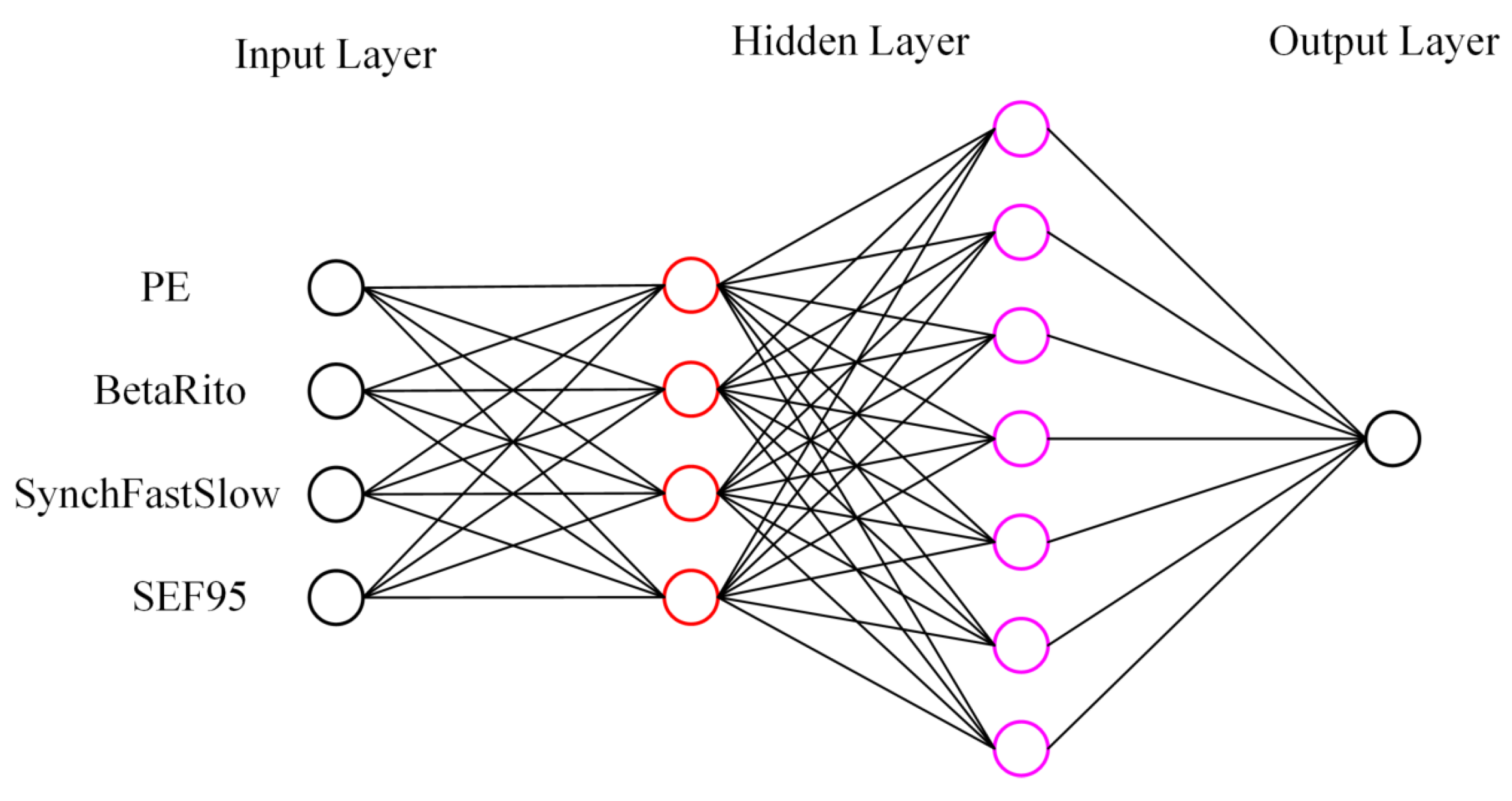
2.5. Artificial Neural Network
2.6. Support Vector Machine
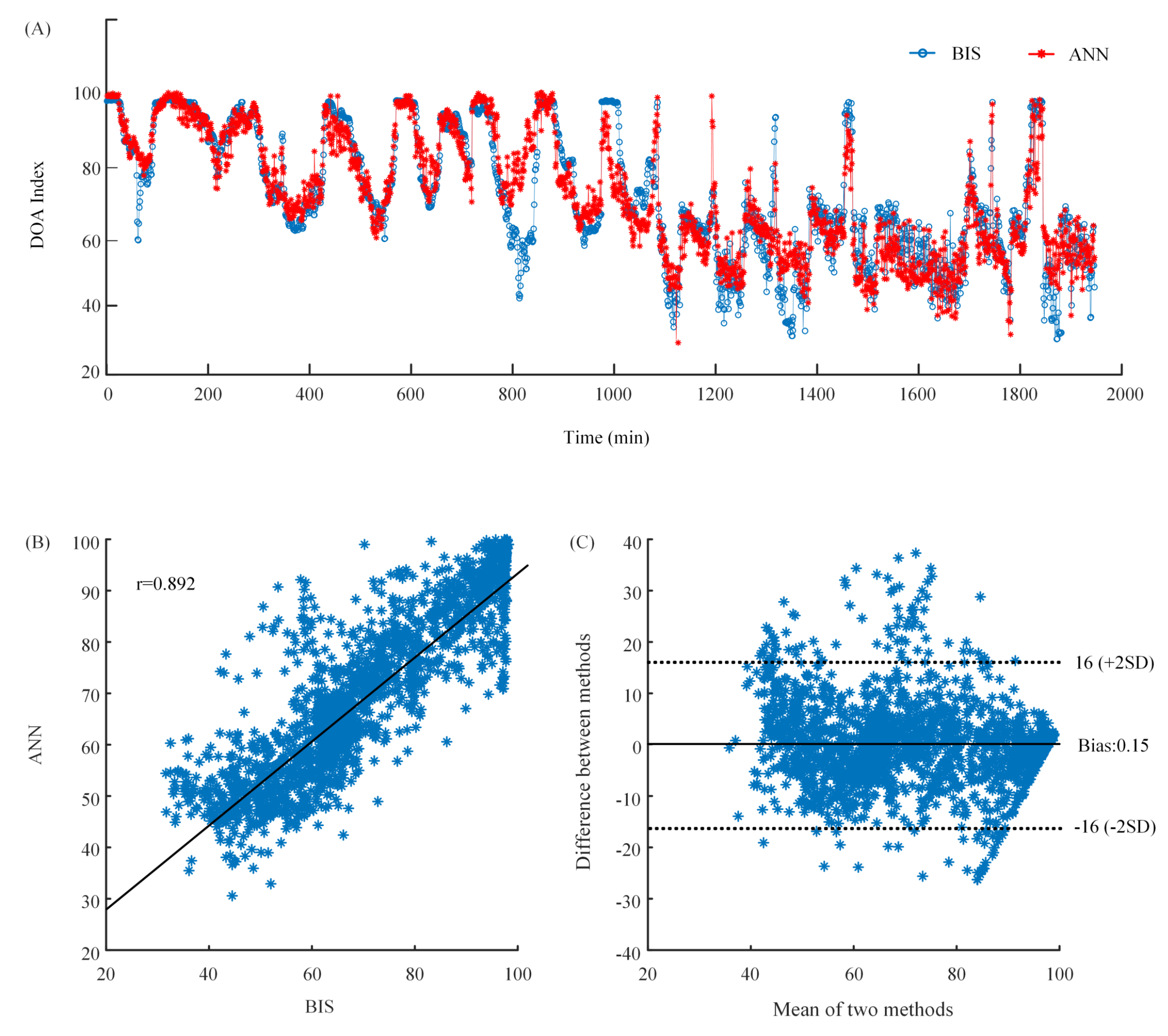
2.7. Performance Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensitivity of | Sensitivity of | Sensitivity of | Sensitivity of | Classification | |
|---|---|---|---|---|---|
| Awake | Light Anesthesia | General Anesthesia | Deep Anesthesia | Accuracy | |
| ANN | 36.2% | 51.4% | 39.7% | 6% | 42.2% |
References
- Sebel, P.S.; Bowdle, T.A.; Ghoneim, M.M.; Rampil, I.J.; Padilla, R.E.; Gan, T.J.; Domino, K.B. The incidence of awareness during anesthesia: A multicenter United States study. Anesth. Analg. 2004, 99, 833–839. [Google Scholar] [CrossRef]
- Jiang, G.J.; Fan, S.Z.; Abbod, M.F.; Huang, H.H.; Lan, J.Y.; Tsai, F.F.; Chang, H.C.; Yang, Y.W.; Chuang, F.L.; Chiu, Y.F.; et al. Sample Entropy Analysis of EEG Signals via Artificial Neural Networks to Model Patients’ Consciousness Level Based on Anesthesiologists Experience. Biomed. Res. Int. 2015, 2015, 343478. [Google Scholar] [CrossRef]
- Monk, T.G.; Saini, V.; Weldon, B.C.; Sigl, J.C. Anesthetic management and one-year mortality after noncardiac surgery. Anesth. Analg. 2005, 100, 4–10. [Google Scholar] [CrossRef]
- Shalbaf, R.; Behnam, H.; Sleigh, J.W.; Steyn-Ross, A.; Voss, L.J. Monitoring the depth of anesthesia using entropy features and an artificial neural network. J. Neurosci. Methods 2013, 218, 17–24. [Google Scholar] [CrossRef]
- Shalbaf, R.; Behnam, H.; Sleigh, J.W.; Voss, L.J. Using the Hilbert-Huang transform to measure the electroencephalographic effect of propofol. Physiol. Meas. 2012, 33, 271–285. [Google Scholar] [CrossRef]
- Li, D.; Li, X.; Liang, Z.; Voss, L.J.; Sleigh, J.W. Multiscale permutation entropy analysis of EEG recordings during sevoflurane anesthesia. J. Neural. Eng. 2010, 7, 046010. [Google Scholar] [CrossRef]
- Liang, Z.; Wang, Y.; Sun, X.; Li, D.; Voss, L.J.; Sleigh, J.W.; Hagihira, S.; Li, X. EEG entropy measures in anesthesia. Front. Comput. Neurosci. 2015, 9, 16. [Google Scholar] [CrossRef]
- Al-Kadi, M.I.; Reaz, M.B.I.; Ali, M.A.M. Evolution of Electroencephalogram Signal Analysis Techniques during Anesthesia. Sensors 2013, 13, 6605–6635. [Google Scholar] [CrossRef]
- Schwender, D.; Daunderer, M.; Klasing, S.; Finsterer, U.; Peter, K. Power spectral analysis of the electroencephalogram during increasing end-expiratory concentrations of isoflurane, desflurane and sevoflurane. Anaesthesia 1998, 53, 335–342. [Google Scholar] [CrossRef]
- Otto, K.A.; Cebotari, S.; Hoffler, H.K.; Tudorache, I. Electroencephalographic Narcotrend index, spectral edge frequency and median power frequency as guide to anaesthetic depth for cardiac surgery in laboratory sheep. Vet. J. 2012, 191, 354–359. [Google Scholar] [CrossRef]
- Schultz, A.; Siedenberg, M.; Grouven, U.; Kneif, T.; Schultz, B. Comparison of Narcotrend Index, Bispectral Index, Spectral and Entropy Parameters during Induction of Propofol-Remifentanil Anaesthesia. J. Clin. Monit. Comput. 2008, 22, 103–111. [Google Scholar] [CrossRef]
- Ellerkmann, R.K.; Soehle, M.; Riese, G.; Zinserling, J.; Wirz, S.; Hoeft, A.; Bruhn, J. The Entropy Module (R) and Bispectral Index (R) as guidance for propofol-remifentanil anaesthesia in combination with regional anaesthesia compared with a standard clinical practice group. Anaesth. Intensive Care 2010, 38, 159–166. [Google Scholar] [CrossRef]
- Revuelta, M.; Paniagua, P.; Campos, J.M.; Fernandez, J.A.; Martinez, A.; Jospin, M.; Litvan, H. Validation of the index of consciousness during sevoflurane and remifentanil anaesthesia: A comparison with the bispectral index and the cerebral state index. Br. J. Anaesthesia 2008, 101, 653–658. [Google Scholar] [CrossRef]
- Viertio-Oja, H.; Maja, V.; Sarkela, M.; Talja, P.; Tenkanen, N.; Tolvanen-Laakso, H.; Paloheimo, M.; Vakkuri, A.; Yli-Hankala, A.; Merilainen, P. Description of the Entropy (TM) algorithm as applied in the Datex-Ohmeda S/5 (TM) Entropy Module. Acta Anaesthesiol. Scand. 2004, 48, 154–161. [Google Scholar] [CrossRef]
- Casteleiro-Roca, J.L.; Calvo-Rolle, J.L.; Méndez Pérez, J.A.; Roqueñí Gutiérrez, N.; De Cos Juez, F.J. Hybrid Intelligent System to Perform Fault Detection on BIS Sensor during Surgeries. Sensors 2017, 17. [Google Scholar] [CrossRef]
- Rampil, I.J. A primer for EEG signal processing in anesthesia. Anesthesiology 1998, 89, 980–1002. [Google Scholar] [CrossRef]
- Morimoto, Y.; Hagihira, S.; Koizumi, Y.; Ishida, K.; Matsumoto, M.; Sakabe, T. The relationship between bispectral index and electroencephalographic parameters during isoflurane anesthesia. Anesth. Analg. 2004, 98, 1336–1340. [Google Scholar] [CrossRef]
- Elbert, T.; Ray, W.J.; Kowalik, Z.J.; Skinner, J.E.; Graf, K.E.; Birbaumer, N. Chaos and physiology: Deterministic chaos in excitable cell assemblies. Physiol. Rev. 1994, 74, 1–47. [Google Scholar] [CrossRef]
- Fell, J.; Kaplan, A.; Darkhovsky, B.; Roschke, J. EEG analysis with nonlinear deterministic and stochastic methods: A combined strategy. Acta Neurobiol. Exp. 2000, 60, 87–108. [Google Scholar]
- Stam, C.J. Nonlinear dynamical analysis of EEG and MEG: Review of an emerging field. Clin. Neurophysiol. 2005, 116, 2266–2301. [Google Scholar] [CrossRef]
- Bai, Y.; Liang, Z.; Li, X.; Voss, L.J.; Sleigh, J.W. Permutation Lempel-Ziv complexity measure of electroencephalogram in GABAergic anaesthetics. Physiol. Meas. 2015, 36, 2483. [Google Scholar] [CrossRef]
- Olofsen, E.; Sleigh, J.W.; Dahan, A. Permutation entropy of the electroencephalogram: A measure of anaesthetic drug effect. Br. J. Anaesth. 2008, 101, 810–821. [Google Scholar] [CrossRef]
- Li, X.L.; Cui, S.Y.; Voss, L.J. Using permutation entropy to measure the electroencephalographic effects of sevoflurane. Anesthesiology 2008, 109, 448–456. [Google Scholar] [CrossRef]
- Li, D.; Liang, Z.; Wang, Y.; Hagihira, S.; Sleigh, J.W.; Li, X. Parameter selection in permutation entropy for an electroencephalographic measure of isoflurane anesthetic drug effect. J. Clin. Monit. Comput. 2013, 27, 113–123. [Google Scholar] [CrossRef]
- Zhu, L.; Cui, G.; Cao, J.; Cichocki, A.; Zhang, J.; Zhou, C. A Hybrid System for Distinguishing between Brain Death and Coma Using Diverse EEG Features. Sensors 2019, 19, 1342. [Google Scholar] [CrossRef]
- Bandt, C.; Pompe, B. Permutation entropy: A natural complexity measure for time series. Phys. Rev. Lett. 2002, 88, 174102. [Google Scholar] [CrossRef]
- Huang, J.R.; Fan, S.Z.; Abbod, M.F.; Jen, K.K.; Wu, J.F.; Shieh, J.S. Application of Multivariate Empirical Mode Decomposition and Sample Entropy in EEG Signals via Artificial Neural Networks for Interpreting Depth of Anesthesia. Entropy 2013, 15, 3325–3339. [Google Scholar] [CrossRef]
- Kortelainen, J.; Vayrynen, E.; Seppanen, T. Isomap Approach to EEG-Based Assessment of Neurophysiological Changes during Anesthesia. IEEE Trans. Neural Syst. Rehabilit. Eng. 2011, 19, 113–120. [Google Scholar] [CrossRef]
- Ortolani, O.; Conti, A.; Di Filippo, A.; Adembri, C.; Moraldi, E.; Evangelisti, A.; Maggini, M.; Roberts, S.J. EEG signal processing in anaesthesia. Use of a neural network technique for monitoring depth of anaesthesia. Br. J. Anaesth. 2002, 88, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Yu, J.; Wu, L.; Liu, Y.; Jia, C.; Xie, Y. Analysis and Feature Extraction of EEG Signals Induced by Anesthesia Monitoring Based on Wavelet Transform. IEEE Access 2019, 7, 41565–41575. [Google Scholar] [CrossRef]
- Liu, Q.; Ma, L.; Fan, S.Z.; Abbod, M.F.; Shieh, J.S. Sample entropy analysis for the estimating depth of anaesthesia through human EEG signal at different levels of unconsciousness during surgeries. PeerJ 2018, 6, e4817. [Google Scholar] [CrossRef]
- Shalbaf, A.; Saffar, M.; Sleigh, J.W.; Shalbaf, R. Monitoring the Depth of Anesthesia Using a New Adaptive Neurofuzzy System. IEEE J. Biomed. Health Inform. 2018, 22, 671–677. [Google Scholar] [CrossRef]
- Shalbaf, A.; Shalbaf, R.; Saffar, M.; Sleigh, J. Monitoring the level of hypnosis using a hierarchical SVM system. J. Clin. Monitor. Comput. 2019, 1–8. [Google Scholar] [CrossRef]
- Li, X.L.; Li, D.; Liang, Z.H.; Voss, L.J.; Sleigh, J.W. Analysis of depth of anesthesia with Hilbert-Huang spectral entropy. Clin. Neurophysiol. 2008, 119, 2465–2475. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Wang, Y.; Ouyang, G.; Voss, L.J.; Sleigh, J.W.; Li, X. Permutation auto-mutual information of electroencephalogram in anesthesia. J. Neural Eng. 2013, 10, 026004. [Google Scholar] [CrossRef]
- Schwender, D.; Daunderer, M.; Mulzer, S.; Klasing, S.; Finsterer, U.; Peter, K. Spectral edge frequency of the electroencephalogram to monitor "depth" of anaesthesia with isoflurane or propofol. Br. J. Anaesth. 1996, 77, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Bose, N.K.; Liang, P. Neural Network Fundamentals with Graphs, Algorithms, and Applications (McGraw-Hill Series in Electrical and Computer Engineering); McGraw-Hill: New York, NY, USA, 1996. [Google Scholar]
- Zhang, G.Q.; Hu, M.Y.; Patuwo, B.E.; Indro, D.C. Artificial neural networks in bankruptcy prediction: General framework and cross-validation analysis. Eur. J. Op. Res. 1999, 116, 16–32. [Google Scholar] [CrossRef]
- Boser, B.E.; Guyon, I.M.; Vapnik, V.N. A training algorithm for optimal margin classifiers. In Proceedings of the Fifth Annual Workshop on Computational Learning Theory, Pittsburgh, PA, USA, 27–29 July 1992; pp. 144–152. [Google Scholar]
- Vapnik, V. The Nature of Statistical Learning Theory; Springer-Verlag: New York, NY, USA, 1995. [Google Scholar]
- Gunn, S.R. Support Vector Machines for Classification and Regression; ISIS Technical Report; University of Southampton: Southampton, UK, 1998; p. 14. [Google Scholar]
- Chang, C.C.; Lin, C.J. LIBSVM: A library for support vector machines. ACM Trans. Intell. Syst. Technol. 2011, 2, 27. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]





| Subject | Raw EEG Length (min) | Preprocessed EEG Length (min) | Number of Samples |
|---|---|---|---|
| Patient 1 | 139 | 130 | 130 |
| Patient 2 | 139 | 138 | 138 |
| Patient 3 | 170 | 168 | 168 |
| Patient 4 | 135 | 134 | 134 |
| Patient 5 | 88 | 87 | 87 |
| Patient 6 | 68 | 63 | 63 |
| Patient 7 | 134 | 129 | 129 |
| Patient 8 | 129 | 126 | 126 |
| Patient 9 | 110 | 109 | 109 |
| Patient 10 | 108 | 108 | 108 |
| Patient 11 | 126 | 125 | 125 |
| Patient 12 | 138 | 137 | 137 |
| Patient 13 | 168 | 168 | 168 |
| Patient 14 | 124 | 124 | 124 |
| Patient 15 | 88 | 80 | 80 |
| Patient 16 | 124 | 121 | 121 |
| Sensitivity of | Sensitivity of | Sensitivity of | Sensitivity of | Classification | |
|---|---|---|---|---|---|
| Awake | Light Anesthesia | General Anesthesia | Deep Anesthesia | Accuracy | |
| 82.8% | 65.5% | 81.3% | 8% | 73.7% | |
| 81.5% | 64.2% | 80.3% | 4% | 72.4% | |
| 80.7% | 63.6% | 79.4% | 6% | 71.8% | |
| 79.8% | 60.6% | 81.5% | 2% | 70.7% |
| Single | Classification | Two | Classification | Three | Classification | Four | Classification |
|---|---|---|---|---|---|---|---|
| Feature | Accuracy | Features | Accuracy | Features | Accuracy | Features | Accuracy |
| PE | 73.7% | PE-SFS | 75.7% | PE-SFS-BR | 76.2% | PE-SFS-BR-SEF95 | 79.1% |
| SFS | 63.6% | PE-BR | 76.0% | PE-SFS-SEF95 | 76.8% | ||
| BR | 60.4% | PE-SEF95 | 75.5% | PE-BR-SEF95 | 75.8% | ||
| SEF95 | 66.7% | SFS-BR | 64.6% | SFS-BR-SEF95 | 71.8% | ||
| SFS-SEF95 | 69.1% | ||||||
| BR-SEF95 | 64.4% |
| Sensitivity of | Sensitivity of | Sensitivity of | Sensitivity of | Classification | |
|---|---|---|---|---|---|
| Awake | Light Anesthesia | General Anesthesia | Deep Anesthesia | Accuracy | |
| ANN | 86.4% | 73.6% | 84.4% | 14% | 79.1% |
| SVM | 84.8% | 71.1% | 82.1% | 2% | 76.7% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gu, Y.; Liang, Z.; Hagihira, S. Use of Multiple EEG Features and Artificial Neural Network to Monitor the Depth of Anesthesia. Sensors 2019, 19, 2499. https://doi.org/10.3390/s19112499
Gu Y, Liang Z, Hagihira S. Use of Multiple EEG Features and Artificial Neural Network to Monitor the Depth of Anesthesia. Sensors. 2019; 19(11):2499. https://doi.org/10.3390/s19112499
Chicago/Turabian StyleGu, Yue, Zhenhu Liang, and Satoshi Hagihira. 2019. "Use of Multiple EEG Features and Artificial Neural Network to Monitor the Depth of Anesthesia" Sensors 19, no. 11: 2499. https://doi.org/10.3390/s19112499
APA StyleGu, Y., Liang, Z., & Hagihira, S. (2019). Use of Multiple EEG Features and Artificial Neural Network to Monitor the Depth of Anesthesia. Sensors, 19(11), 2499. https://doi.org/10.3390/s19112499