HemoKinect: A Microsoft Kinect V2 Based Exergaming Software to Supervise Physical Exercise of Patients with Hemophilia

 ,
,  ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Hardware and Software Description
2.2. Measurement and Methodology
| Algorithm 1: Joint flexion (elbow and knee) count algorithm. The detection is a two-step procedure that firstly checks that a flexed status has been reached, and then, an extension is observed to count the exercise as completed. |
 |
| Algorithm 2: Step count algorithm. The step detection is based on (a) the general rise of the body, taking the hip center as a reference and (b) the sequential flexion and extension of the knees. The ankle angle history is recorded throughout the duration of the exercise for medical evaluation purposes, but is not used to detect the step climb due to its inaccuracy. |
 |
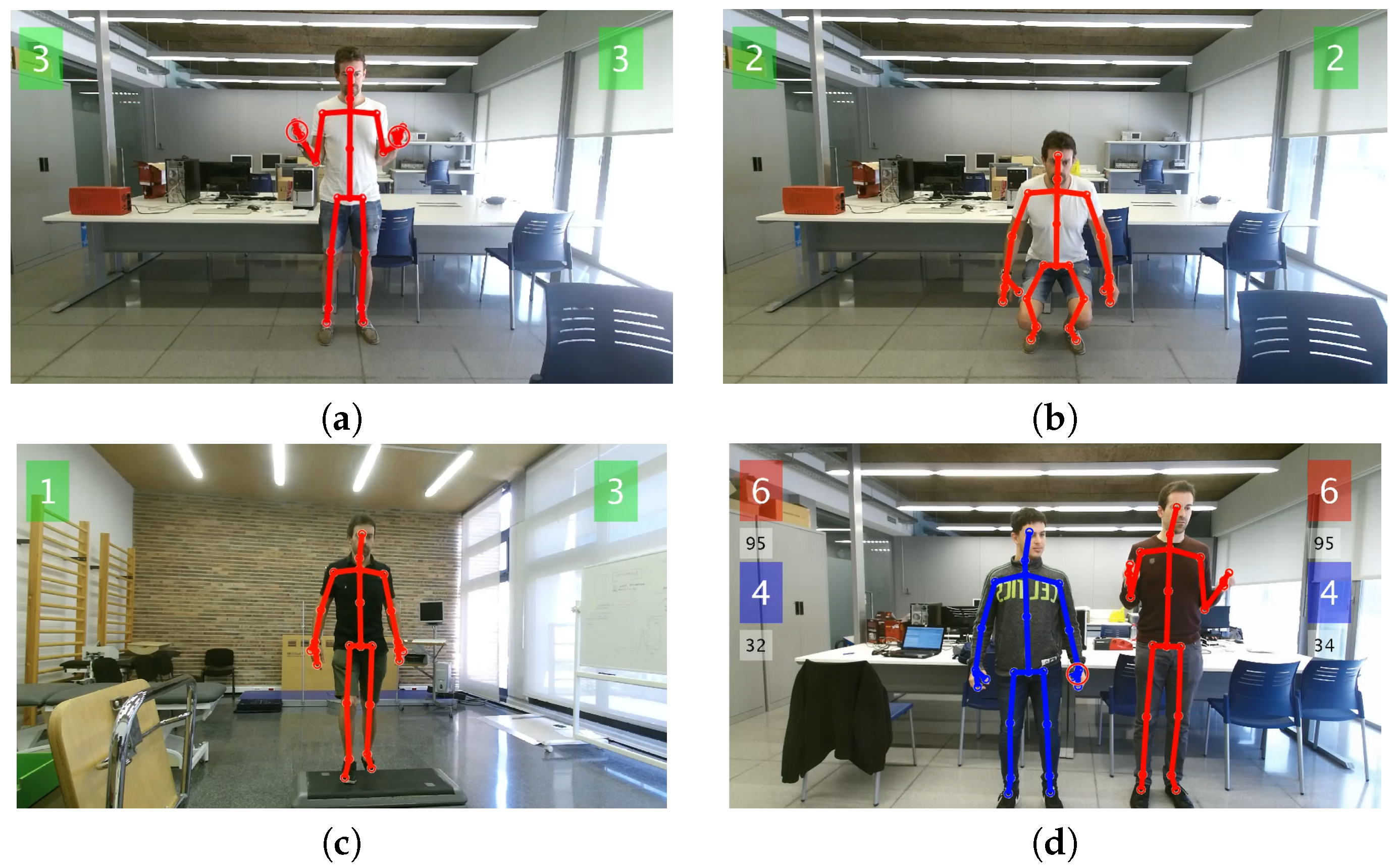
| Algorithm 3: Balance exercise algorithm. Balance is evaluated in 8 directions in the plane, targeted sequentially in clockwise order: north (N), northeast (NE), east (E), southeast (SE), south (S), southwest (SW), west (W) and northwest (NW), where N corresponds to the player’s front-facing direction. The player must swing back to the starting position () before each change of direction. The scores’ array contains the percentages of time spent by the subject in each of the target balance spots. |
 |
2.3. Population
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mannucci, P.M.; Tuddenham, E.G. The hemophilias—From royal genes to gene therapy. N. Engl. J. Med. 2001, 344, 1773–1779. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, A.; Brewer, A.K.; Mauser-Bunschoten, E.P.; Key, N.S.; Kitchen, S.; Llinas, A.; Ludlam, C.A.; Mahlangu, J.N.; Mulder, K.; Poon, M.C.; et al. Guidelines for the management of hemophilia. Haemophilia 2013, 19, e1–e47. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, J.; Hughes, D.; Camp, C.; Burke, T.; Carroll, L.; Diego, D.A.G. The cost of severe haemophilia in Europe: The CHESS study. Orphanet J. Rare Dis. 2017, 12, 106. [Google Scholar] [CrossRef] [PubMed]
- Raffini, L.; Manno, C. Modern management of haemophilic arthropathy. Br. J. Haematol. 2007, 136, 777–787. [Google Scholar] [PubMed]
- Van Vulpen, L.F.D.; Mastbergen, S.C.; Lafeber, F.P.J.G.; Schutgens, R.E.G. Differential effects of bleeds on the development of arthropathy-basic and applied issues. Haemophilia 2017, 23, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Forsyth, A.L.; Rivard, G.E.; Valentino, L.A.; Zourikian, N.; Hoffman, M.; Monahan, P.E.; Van Meegeren, M.E.R.; Forriol, F. Consequences of intra-articular bleeding in haemophilia: Science to clinical practice and beyond. Haemophilia 2012, 4, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Mulder, K. Exercise for People with Hemophilia; Technical Report; World Federation of Hemophilia: Montreal, QC, Canada, 2006. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health (WHO); World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Negrier, C.; Seuser, A.; Forsyth, A.; Lobet, S.; Llinas, A.; Rosas, M.; Heijnen, L. The benefits of exercise for patients with haemophilia and recommendations for safe and effective physical activity. Haemophilia 2013, 19, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Strike, K.; Mulder, K.; Michael, R. Exercise for haemophilia. In Cochrane Database of Systematic Reviews; The Cochrane Collaboration, Ed.; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2016. [Google Scholar]
- Taylor, M.J.; McCormick, D.; Impson, R.; Shawis, T.; Griffin, M. Activity Promoting Gaming Systems in Exercise and Rehabilitation. J. Rehabil. Res. Dev. 2011, 48, 1171–1186. [Google Scholar] [CrossRef] [PubMed]
- Smith, K. Chapter 6. Playing for Health. In Digital Outcasts: Moving Technology Forward without Leaving People Behind; Morgan Kaufmann: Boston, MA, USA, 2013; pp. 125–155. [Google Scholar]
- Moreno, F.A.; Merchán-Baeza, J.A.; González-Sánchez, M.; González-Jiménez, J.; Cuesta-Vargas, A.I. Experimental Validation of Depth Cameras for the Parameterization of Functional Balance of Patients in Clinical Tests. Sensors 2017, 17, 424. [Google Scholar] [CrossRef] [PubMed]
- Hondori, H.M.; Khademi, M. A Review on Technical and Clinical Impact of Microsoft Kinect on Physical Therapy and Rehabilitation. J. Med. Eng. 2014, 2014. [Google Scholar] [CrossRef]
- Webster, D.; Celik, O. Systematic review of Kinect applications in elderly care and stroke rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 108. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hui, X.; Andong, L. Kinect-based rehabilitation exercises system: Therapist involved approach. Bio-Med. Mater. Eng. 2014, 24, 2611–2618. [Google Scholar]
- Chang, Y.J.; Chen, S.F.; Huang, J.D. A Kinect-based system for physical rehabilitation: A pilot study for young adults with motor disabilities. Res. Dev. Dis. 2011, 32, 2566–2570. [Google Scholar] [CrossRef] [PubMed]
- Su, C.J.; Chiang, C.Y.; Huang, J.Y. Kinect-enabled home-based rehabilitation system using Dynamic Time Warping and fuzzy logic. Appl. Soft Comput. 2014, 22, 652–666. [Google Scholar] [CrossRef]
- Rantz, M.J.; Skubic, M.; Abbott, C.; Galambos, C.; Pak, Y.; Ho, D.K.; Stone, E.E.; Rui, L.; Back, J.; Miller, S.J.; et al. In-home fall risk assessment and detection sensor system. J. Gerontol. Nurs. 2013, 39, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Yoon, C.; Chung, S.G.; Kim, H.C.; Kwak, Y.; Park, H.W.; Kim, K. Measurement of Shoulder Range of Motion in Patients with Adhesive Capsulitis Using a Kinect. PLoS ONE 2015, 10, e0129398. [Google Scholar] [CrossRef] [PubMed]
- Lim, D.; Kim, C.; Jung, H.; Jung, D.; Chun, K.J. Use of the Microsoft Kinect system to characterize balance ability during balance training. Clin. Interv. Aging 2015, 10, 1077–1083. [Google Scholar] [PubMed]
- Clark, R.A.; Pua, Y.H.; Fortin, K.; Ritchie, C.; Webster, K.E.; Denehy, L.; Bryant, A.L. Validity of the Microsoft Kinect for assessment of postural control. Gait Posture 2012, 36, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Cassola, F.; Morgado, L.; de Carvalho, F.; Paredes, H.; Fonseca, B.; Martins, P. Online-Gym: A 3D Virtual Gymnasium Using Kinect Interaction. Procedia Technol. 2014, 13, 130–138. [Google Scholar] [CrossRef]
- Fernández-Baena, A.; Susín, A.; Lligadas, X. Biomechanical validation of upper-body and lower-body joint movements of kinect motion capture data for rehabilitation treatments. In Proceedings of the 2012 4th International Conference on Intelligent Networking and Collaborative Systems (INCoS), Bucharest, Romania, 19–21 September 2012; pp. 656–661. [Google Scholar]
- Pedro, L.M.; de Paula Caurin, G.A. Kinect evaluation for human body movement analysis. In Proceedings of the 2012 4th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Rome, Italy, 24–27 June 2012; pp. 1856–1861. [Google Scholar]
- Hawi, N.; Liodakis, E.; Musolli, D.; Suero, E.M.; Stuebig, T.; Claassen, L.; Kleiner, C.; Krettek, C.; Ahlers, V.; Citak, M. Range of motion assessment of the shoulder and elbow joints using a motion sensing input device: A pilot study. Technol. Health Care 2014, 22, 289–295. [Google Scholar] [PubMed]
- Huber, M.; Seitz, A.; Leeser, M.; Sternad, D. Validity and reliability of Kinect skeleton for measuring shoulder joint angles: A feasibility study. Physiotherapy 2015, 101, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Otte, K.; Kayser, B.; Mansow-Model, S.; Verrel, J.; Paul, F.; Brandt, A.U.; Schmitz-Hübsch, T. Accuracy and reliability of the Kinect version 2 for clinical measurement of motor function. PLoS ONE 2016, 11, e0166532. [Google Scholar] [CrossRef] [PubMed]
- Wasenmüller, O.; Stricker, D. Comparison of Kinect V1 and V2 Depth Images in Terms of Accuracy and Precision. In Proceedings of the Computer Vision—ACCV 2016 Workshops, Taipei, Taiwan, 20–24 November 2016; Chen, C.S., Lu, J., Ma, K.K., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 34–45. [Google Scholar]
- Wang, Q.; Kurillo, G.; Ofli, F.; Bajcsy, R. Evaluation of Pose Tracking Accuracy in the First and Second Generations of Microsoft Kinect. In Proceedings of the 2015 International Conference on Healthcare Informatics (ICHI), Dallas, TX, USA, 21–23 October 2015; pp. 380–389. [Google Scholar]
- Capecci, M.; Ceravolo, M.G.; Ferracuti, F.; Grugnetti, M.; Iarlori, S.; Longhi, S.; Romeo, L.; Verdini, F. An instrumental approach for monitoring physical exercises in a visual markerless scenario: A proof of concept. J. Biomech. 2018, 69, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Daponte, P.; De Vito, L.; Riccio, M.; Sementa, C. Design and validation of a motion-tracking system for ROM measurements in home rehabilitation. Measurement 2014, 55, 82–96. [Google Scholar] [CrossRef]
- Dolatabadi, E.; Taati, B.; Mihailidis, A. Concurrent validity of the Microsoft Kinect for Windows v2 for measuring spatiotemporal gait parameters. Med. Eng. Phys. 2016, 38, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.; Fagnani, R.; Silva, E.; Matta, M.; Ozelo, M. Use of the exergaming (Nintendo Wii) in the rehabilitation of patients with hemophilia. Haemophilia 2012, 18, 154. [Google Scholar]
- Pérez-Alenda, S.; Carrasco, J.J.; Aguilar-Rodríguez, M.; Martínez-Gómez, L.; Querol-Giner, M.; Cuesta-Barriuso, R.; Torres-Ortuño, A.; Querol, F. Balance evaluation in haemophilic preadolescent patients using Nintendo Wii Balance Board®. Haemophilia 2017, 23, e18–e24. [Google Scholar] [CrossRef] [PubMed]
- Microsoft Corporation. Kinect for Windows SDK 2.0. Available online: http://www.microsoft.com/en-us/download/details.aspx?id=44561 (accessed on 13 July 2018).
- Zennaro, S.; Munaro, M.; Milani, S.; Zanuttigh, P.; Bernardi, A.; Ghidoni, S.; Menegatti, E. Performance evaluation of the 1st and 2nd generation Kinect for multimedia applications. In Proceedings of the 2015 IEEE International Conference on Multimedia and Expo (ICME), Turin, Italy, 29 June–3 July 2015; pp. 1–6. [Google Scholar]
- Shotton, J.; Fitzgibbon, A.; Cook, M.; Sharp, T.; Finocchio, M.; Moore, R.; Kipman, A.; Blake, A. Real-time human pose recognition in parts from single depth images. In Proceedings of the 2011 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Springs, CO, USA, 20–25 June 2011; pp. 1297–1304. [Google Scholar]
- MATLAB. R2016a; The MathWorks Inc.: Natick, MA, USA, 2016. [Google Scholar]
- Xu, X.; McGorry, R.W. The validity of the first and second generation Microsoft KinectTM for identifying joint center locations during static postures. Appl. Ergon. 2015, 49, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Plagenhoef, S.; Evans, F.; Abdelnour, T. Anatomical data for analyzing human motion. Res. Q. Exerc. Sport 1983, 54, 169–178. [Google Scholar] [CrossRef]
- Tantisuwat, A.; Chamonchant, D.; Boonyong, S. Multi-directional Reach Test: An Investigation of the Limits of Stability of People Aged between 20–79 Years. J. Phys. Ther. Sci. 2014, 26, 877–880. [Google Scholar] [CrossRef] [PubMed]
- Newton, R.A. Validity of the Multi-Directional Reach TestA Practical Measure for Limits of Stability in Older Adults. J. Gerontol. 2001, 56, M248–M252. [Google Scholar] [CrossRef]
- Microsoft. Kinect for Windows. Available online: https://developer.microsoft.com/en-us/windows/kinect (accessed on 13 July 2018).
- Intel. Intel Real Sense. Available online: https://software.intel.com/realsense (accessed on 13 July 2018).
- VicoVr. Available online: https://vicovr.com/ (accessed on 13 July 2018).
- Orbbec. Available online: https://orbbec3d.com/products/ (accessed on 13 July 2018).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Body Segment | Percent of Total Body Mass |
|---|---|
| Head | 8.26% |
| Thorax | 20.10% |
| Abdomen | 13.06% |
| Pelvis | 13.66% |
| Upper Arm | 3.25% |
| Forearm | 1.87% |
| Hand | 0.65% |
| Thigh | 10.50% |
| Leg | 4.75% |
| Foot | 1.43% |
| Control | Right Step | Left Step |
|---|---|---|
| 1 | 80 ± 20 | 72 ± 11 |
| 2 | 88 ± 18 | 80 ± 14 |
| 3 | 84 ± 16 | 80 ± 20 |
| 4 | 76 ± 26 | 84 ± 22 |
| 5 | 80 ± 28 | 72 ± 11 |
| 6 | 72 ± 11 | 64 ± 17 |
| 7 | 72 ± 23 | 68 ± 18 |
| 8 | 80 ± 25 | 76 ± 22 |
| 9 | 68 ± 22 | 76 ± 26 |
| 10 | 80 ± 14 | 84 ± 26 |
| Mean | 78 ± 20 | 75 ± 19 |
| Patient | Right Knee | Left Knee | Right Step | Left Step |
|---|---|---|---|---|
| 1 | 100 | 100 | 64 ± 22 | 56 ± 17 |
| 2 | 92 ± 11 | 96 ± 9 | 52 ± 18 | 60 ± 20 |
| 3 | 100 | 100 | 80 ± 20 | 76 ± 26 |
| 4 | 72 ± 11 | 76 ± 9 | 68 ± 22 | 64 ± 29 |
| 5 | 100 | 100 | 64 ± 22 | 56 ± 26 |
| 6 | 60 ± 14 | 52 ± 11 | 52 ± 18 | 56 ± 17 |
| 7 | 64 ± 9 | 60 ± 14 | 68 ± 11 | 72 ± 11 |
| 8 | 100 | 100 | 80 ± 28 | 76 ± 17 |
| Mean | 86 ± 5 | 85 ± 5 | 66 ± 20 | 64 ± 20 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mateo, F.; Soria-Olivas, E.; Carrasco, J.J.; Bonanad, S.; Querol, F.; Pérez-Alenda, S. HemoKinect: A Microsoft Kinect V2 Based Exergaming Software to Supervise Physical Exercise of Patients with Hemophilia. Sensors 2018, 18, 2439. https://doi.org/10.3390/s18082439
Mateo F, Soria-Olivas E, Carrasco JJ, Bonanad S, Querol F, Pérez-Alenda S. HemoKinect: A Microsoft Kinect V2 Based Exergaming Software to Supervise Physical Exercise of Patients with Hemophilia. Sensors. 2018; 18(8):2439. https://doi.org/10.3390/s18082439
Chicago/Turabian StyleMateo, Fernando, Emilio Soria-Olivas, Juan J. Carrasco, Santiago Bonanad, Felipe Querol, and Sofía Pérez-Alenda. 2018. "HemoKinect: A Microsoft Kinect V2 Based Exergaming Software to Supervise Physical Exercise of Patients with Hemophilia" Sensors 18, no. 8: 2439. https://doi.org/10.3390/s18082439
APA StyleMateo, F., Soria-Olivas, E., Carrasco, J. J., Bonanad, S., Querol, F., & Pérez-Alenda, S. (2018). HemoKinect: A Microsoft Kinect V2 Based Exergaming Software to Supervise Physical Exercise of Patients with Hemophilia. Sensors, 18(8), 2439. https://doi.org/10.3390/s18082439