Assessment of Dry Epidermal Electrodes for Long-Term Electromyography Measurements

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
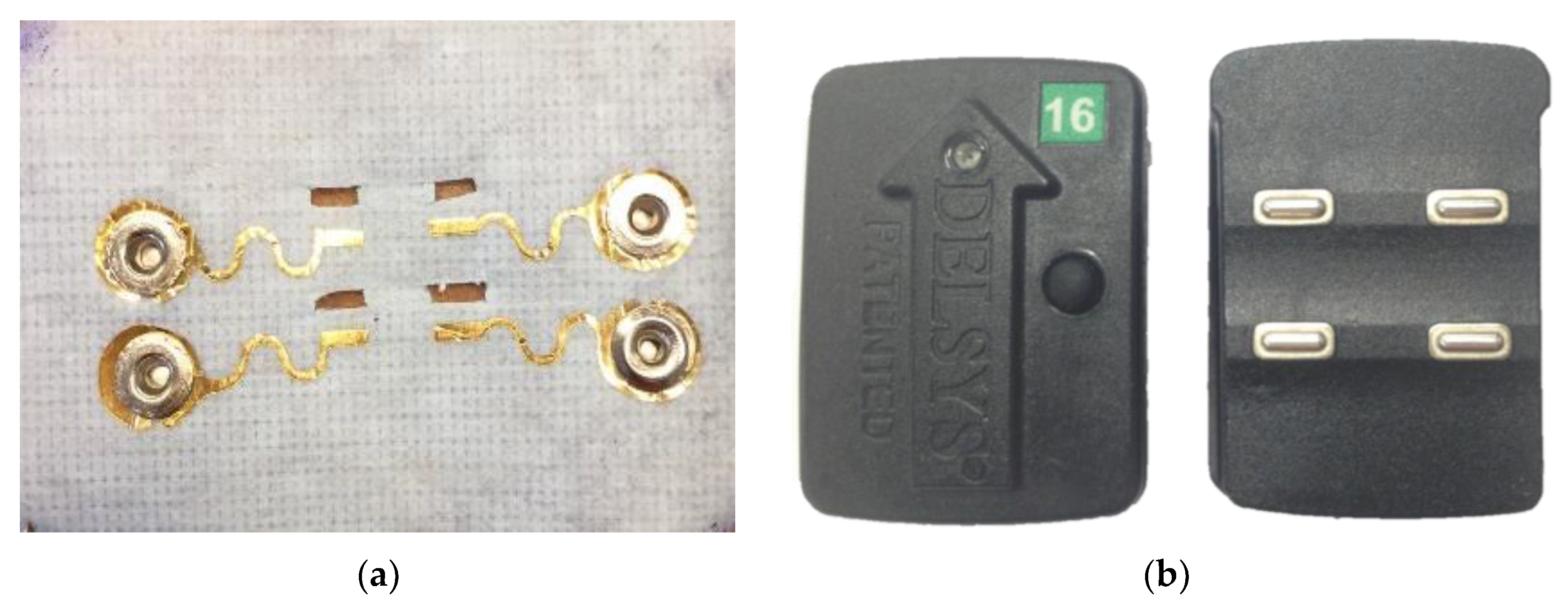
2.1. Electrodes
2.2. sEMG Data Collection Over Six Hours
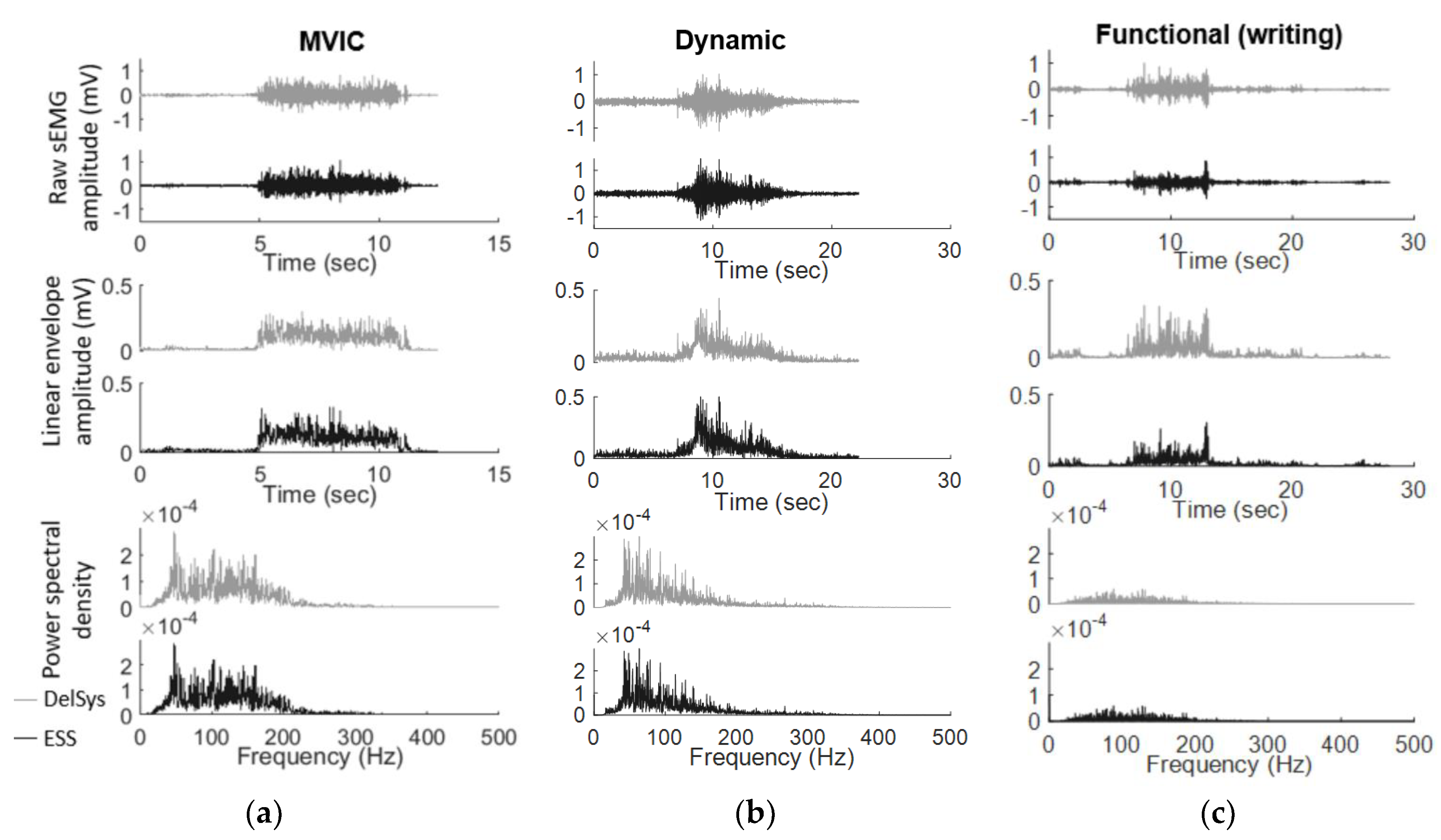
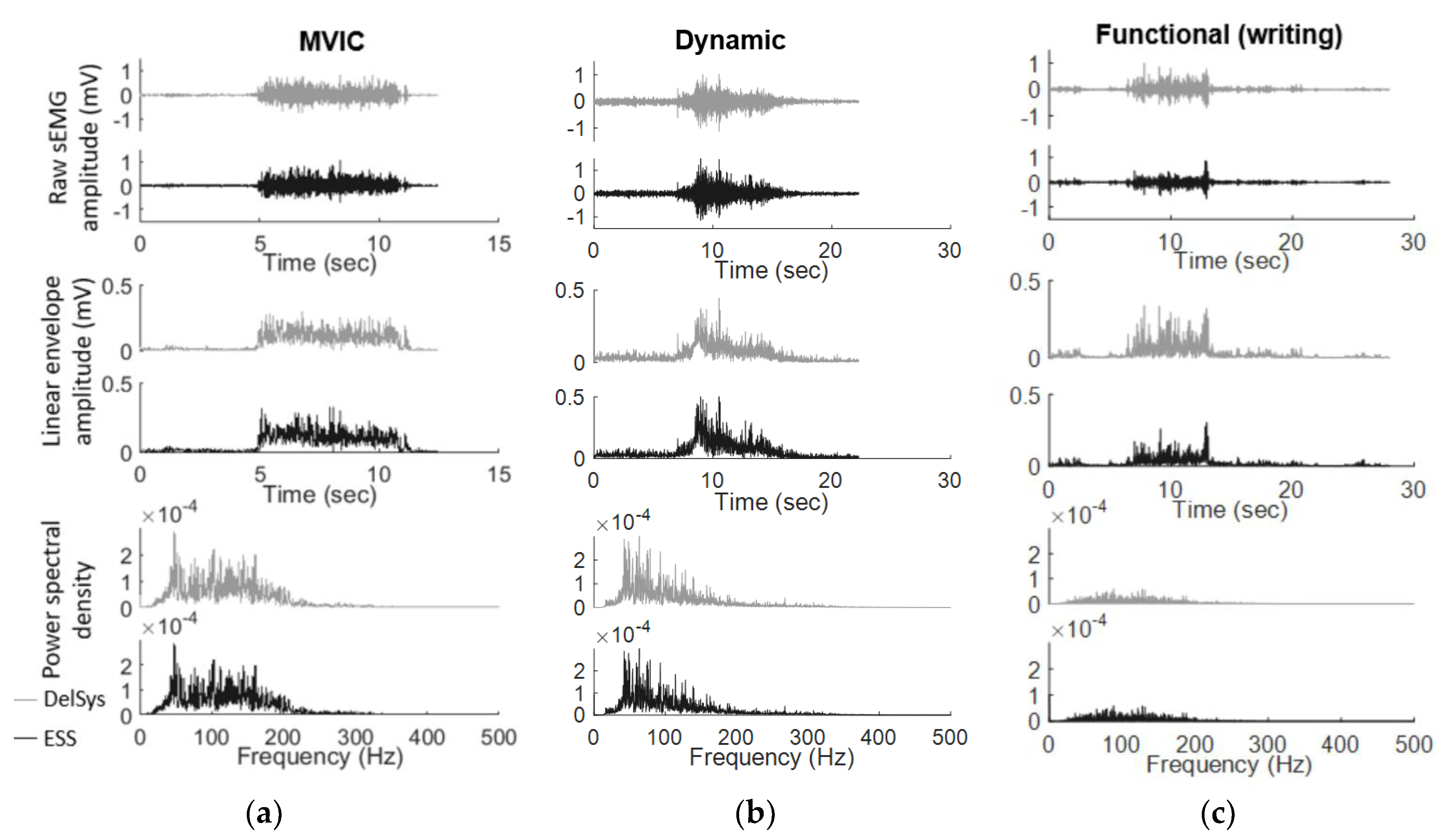
- Maximum voluntary isometric contractions (MVICs): While seated, the subject was asked to perform MVICs, contracting against a static support for each muscle. For the ECR and FCU, subjects were stabilized by the experimenter with their wrist at a 45° angle, and for the TRI and BIC, subjects were stabilized with their elbow at a 90° angle. Subjects were asked to rest for 5 s, contract against a support for 5 s, then rest for 5 s. Subjects were given loud verbal encouragement during contraction to ensure maximal effort.
- Dynamic range of motion test (Dynamic): Subjects were asked to choose between a 2, 3, and 5 lb weight and perform a dynamic range of motion test with verbal and visual cues. For ECR and FCU, subjects held the weight 45° below a horizontal plane with their forearms parallel to the ground for 5 s, then over 2 s lifted the weight to a 45° angle above the horizontal plane and held the weight at this angle for 6 s, concluding by slowly releasing the weight over 2 s back to 45° below horizontal (ECR: forearm pronated; FCU: forearm supinated). For TRI, subjects held the weight in a lunge position with their upper arm parallel to the ground for 5 s, then over 2 s extended their forearm without moving their upper arm and held the extension for 6 s and concluded by lowering the weight over 2 s. For BIC, subjects were asked to stand and hold the weight with their arm relaxed for 5 s, then with their elbow tucked into their side and forearm supinated to lift the weight to a 90° angle (parallel to the ground) over two s, hold the weight for 6 s, and to conclude by slowly lowering the weight back down over 2 s.
- Functional tests (Functional): For the Jebsen Taylor Hand Function Test [38], subjects were asked to complete the seven Jebsen Taylor tasks (writing, card flipping, small objects, simulated feeding, checkers, light objects, heavy objects) as quickly as possible with their dominant hand. The time taken to fully complete each task was recorded. For the Box & Block Test [39], subjects were asked to move wooden cubes (2.5 cm), one cube at a time from their dominant to non-dominant side over a 19 cm high partition as quickly as possible. Subjects were given a 15 s practice session, followed by a one-minute test moving the cubes. The number of cubes moved over the minute-long test was recorded. The sEMG signals taken from each trial were concatenated for analysis to provide an evaluation of the functional tests as a whole, instead of evaluating individual tasks (i.e., seven separate Jebsen Taylor tasks).
2.3. sEMG Analysis
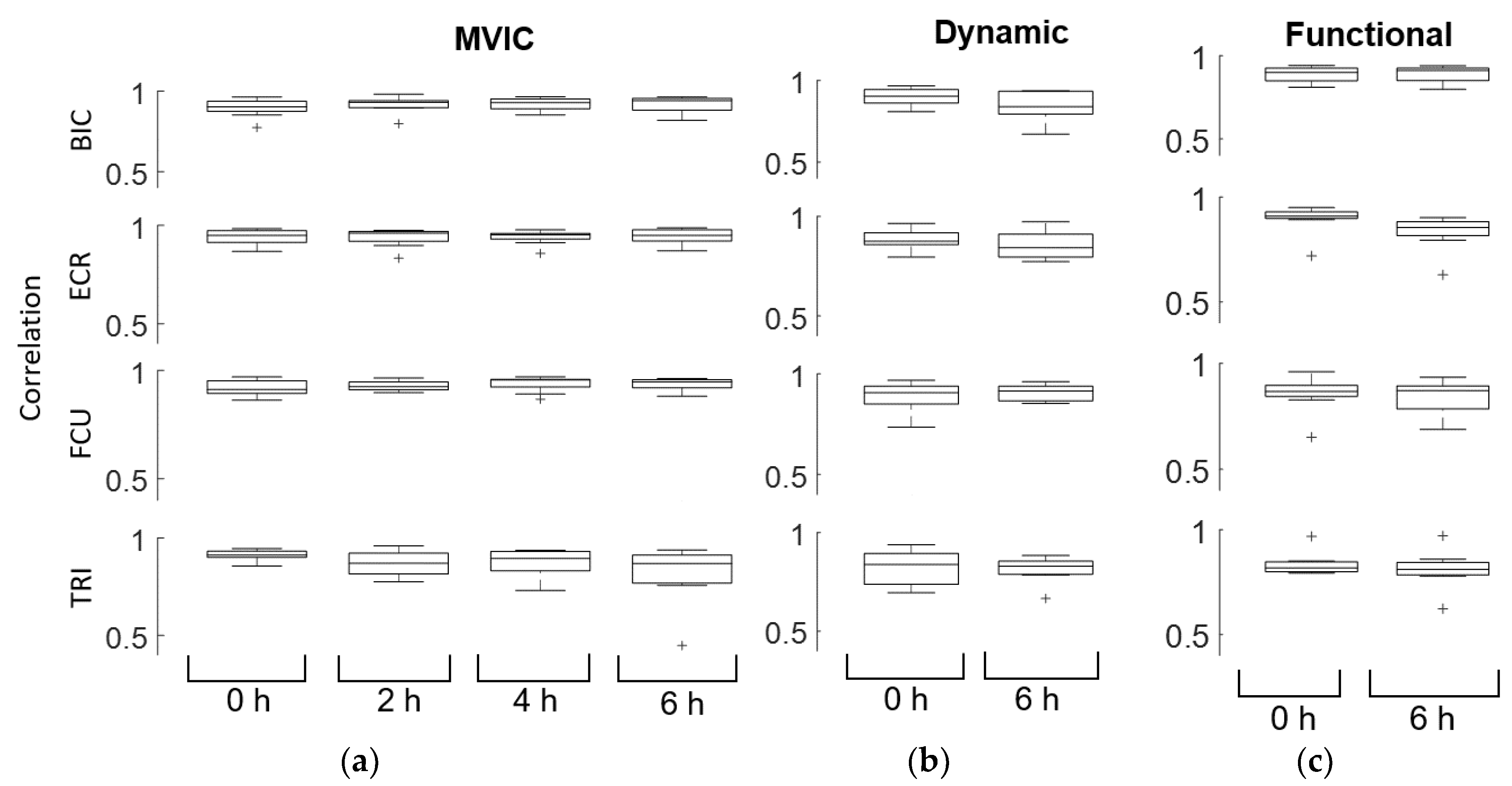
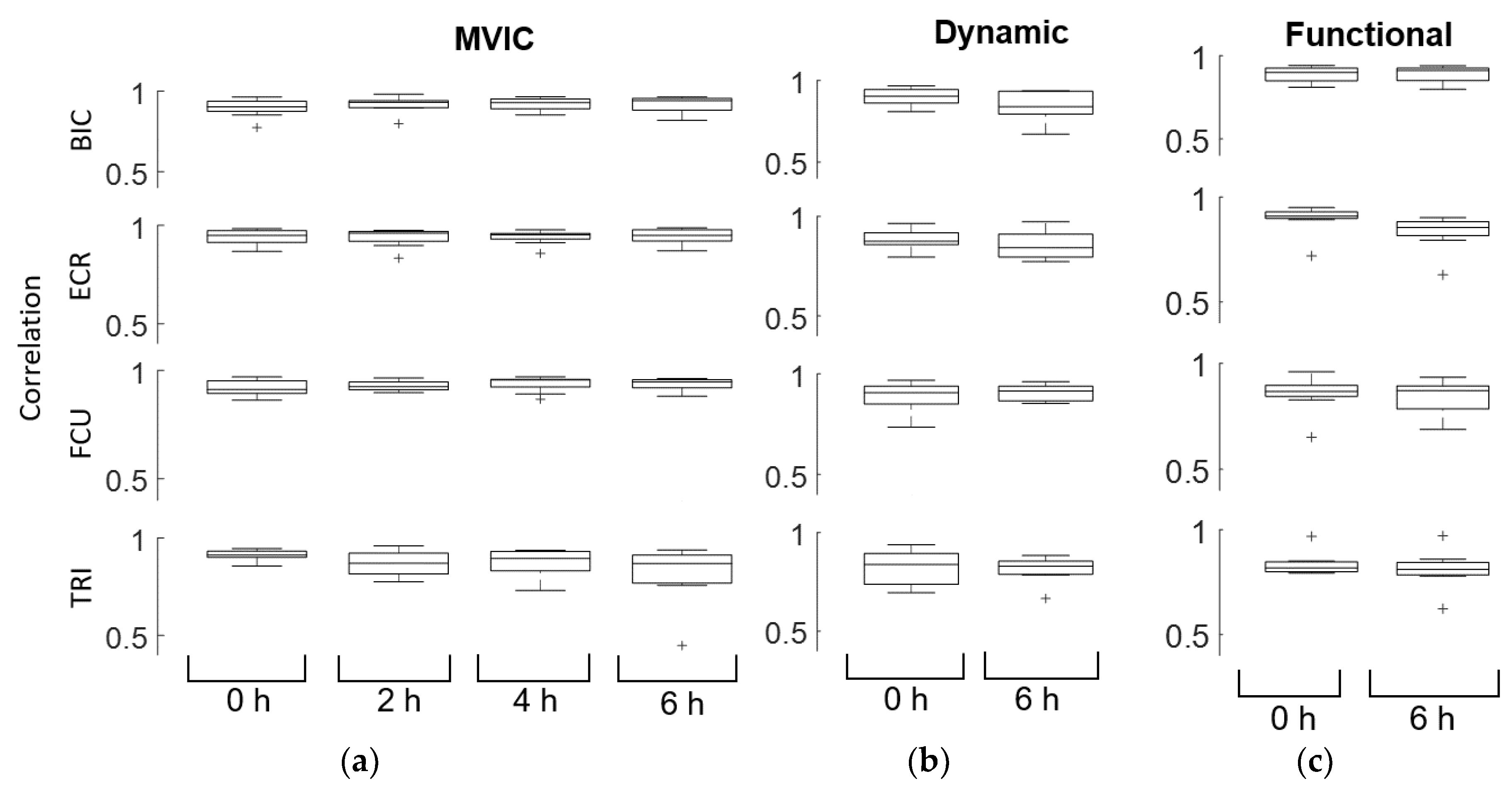
- Pearson’s correlations: Correlations were calculated by taking the Pearson’s correlation for the linear envelope of the Delsys and ESS electrode. Correlation coefficients values between 0.7 and 1.0 were interpreted as a strong positive linear relationship. We defined a moderate correlation as values between 0.3 and 0.7, and low correlation as between 0.0 and 0.3.
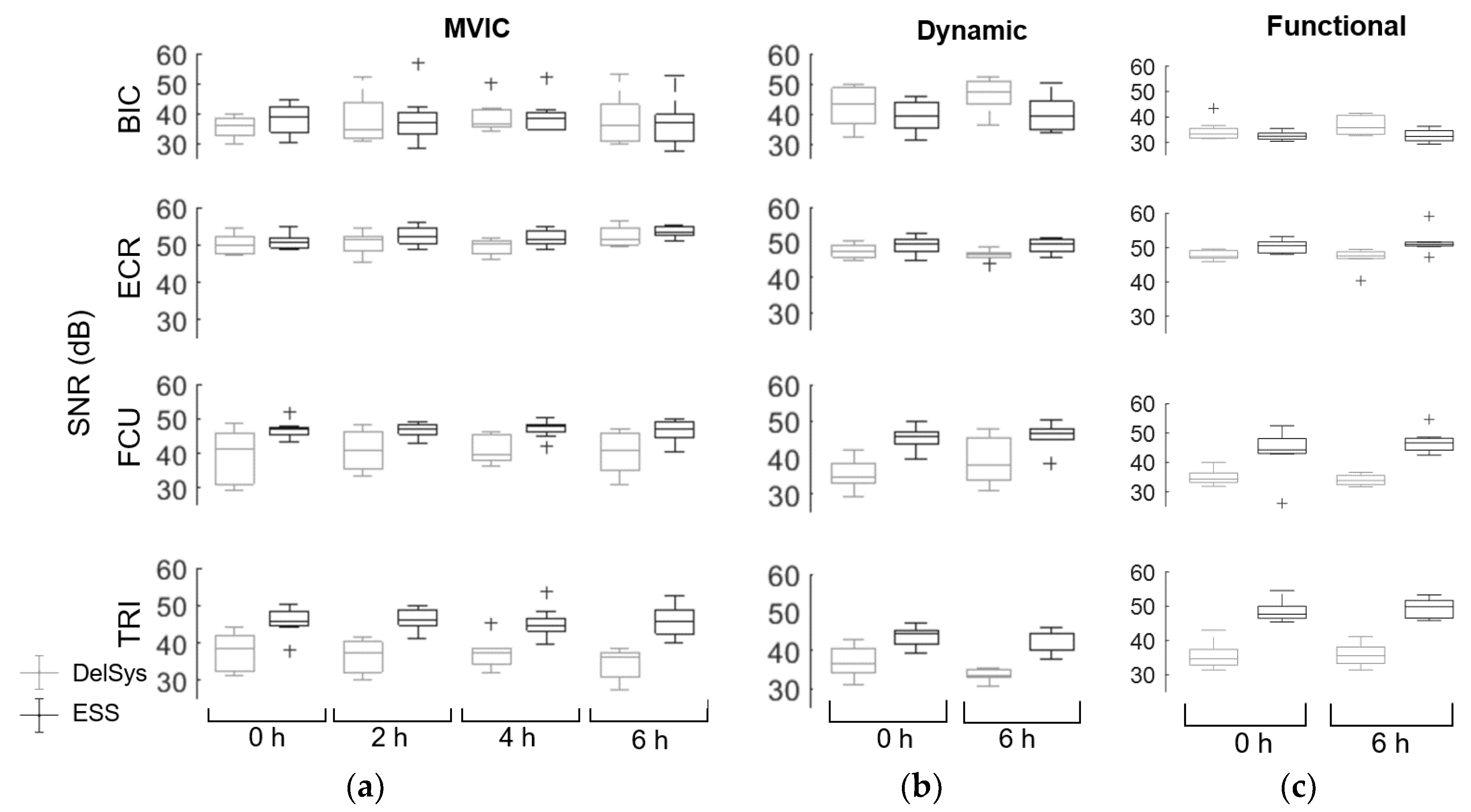
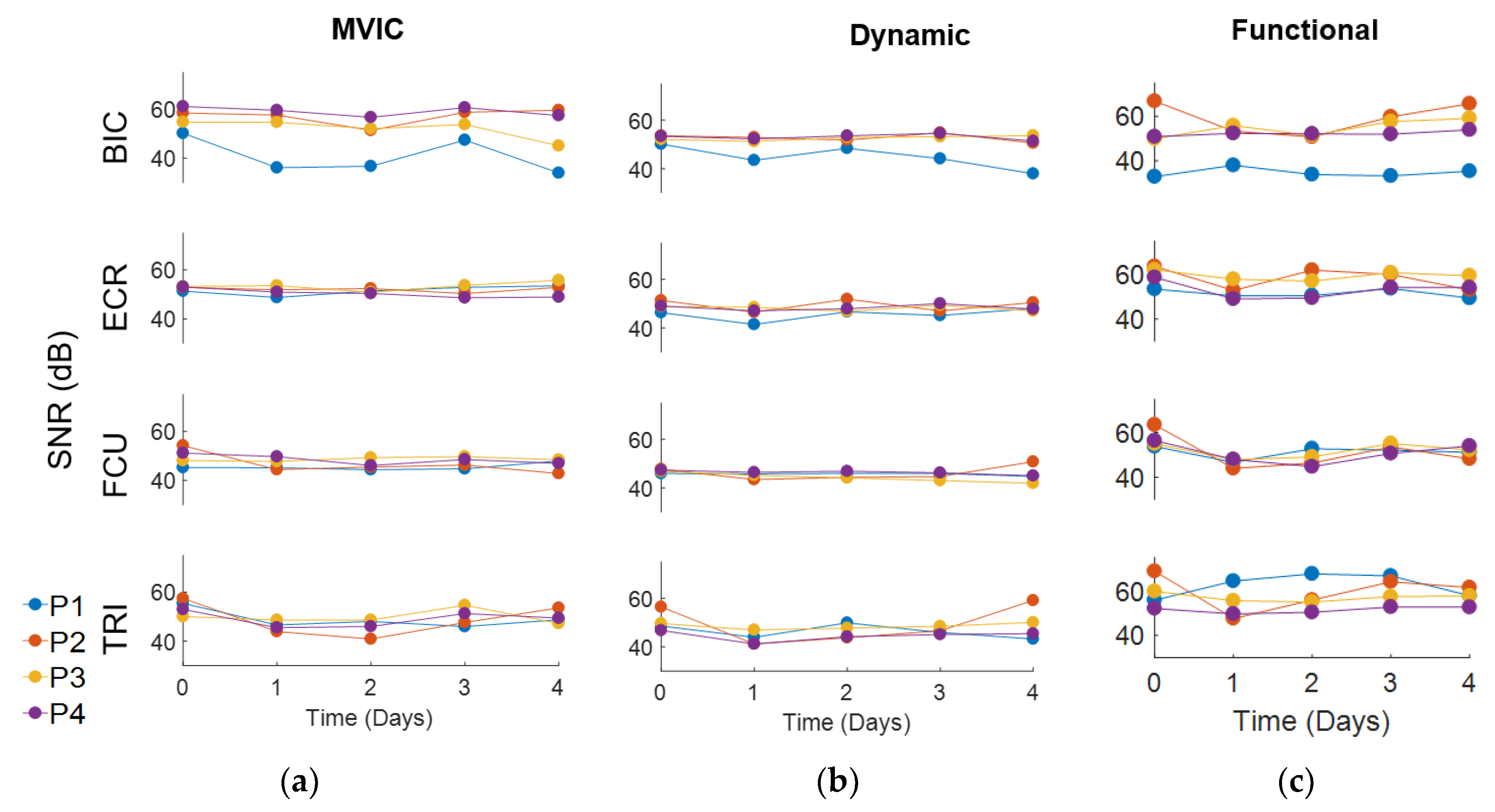
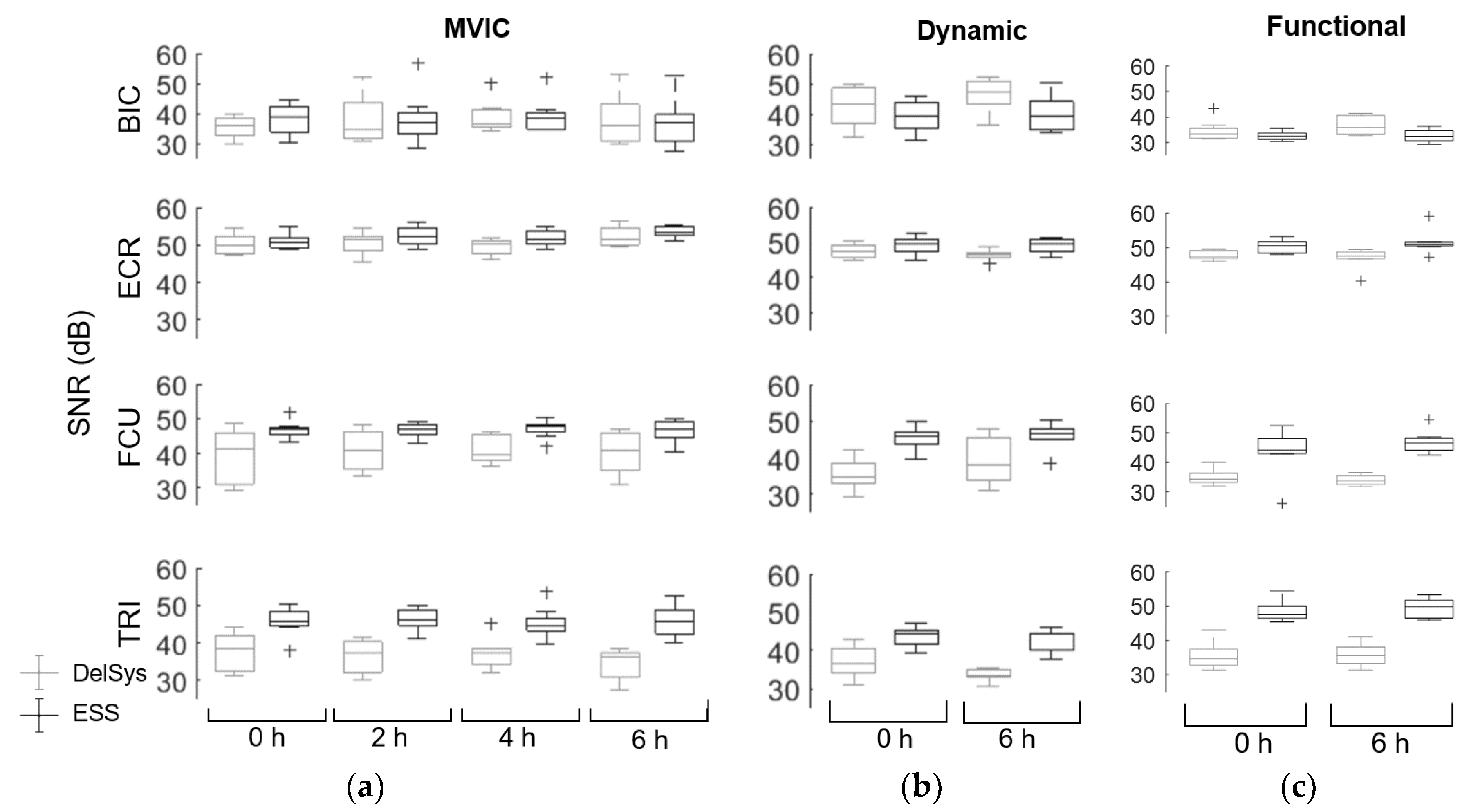
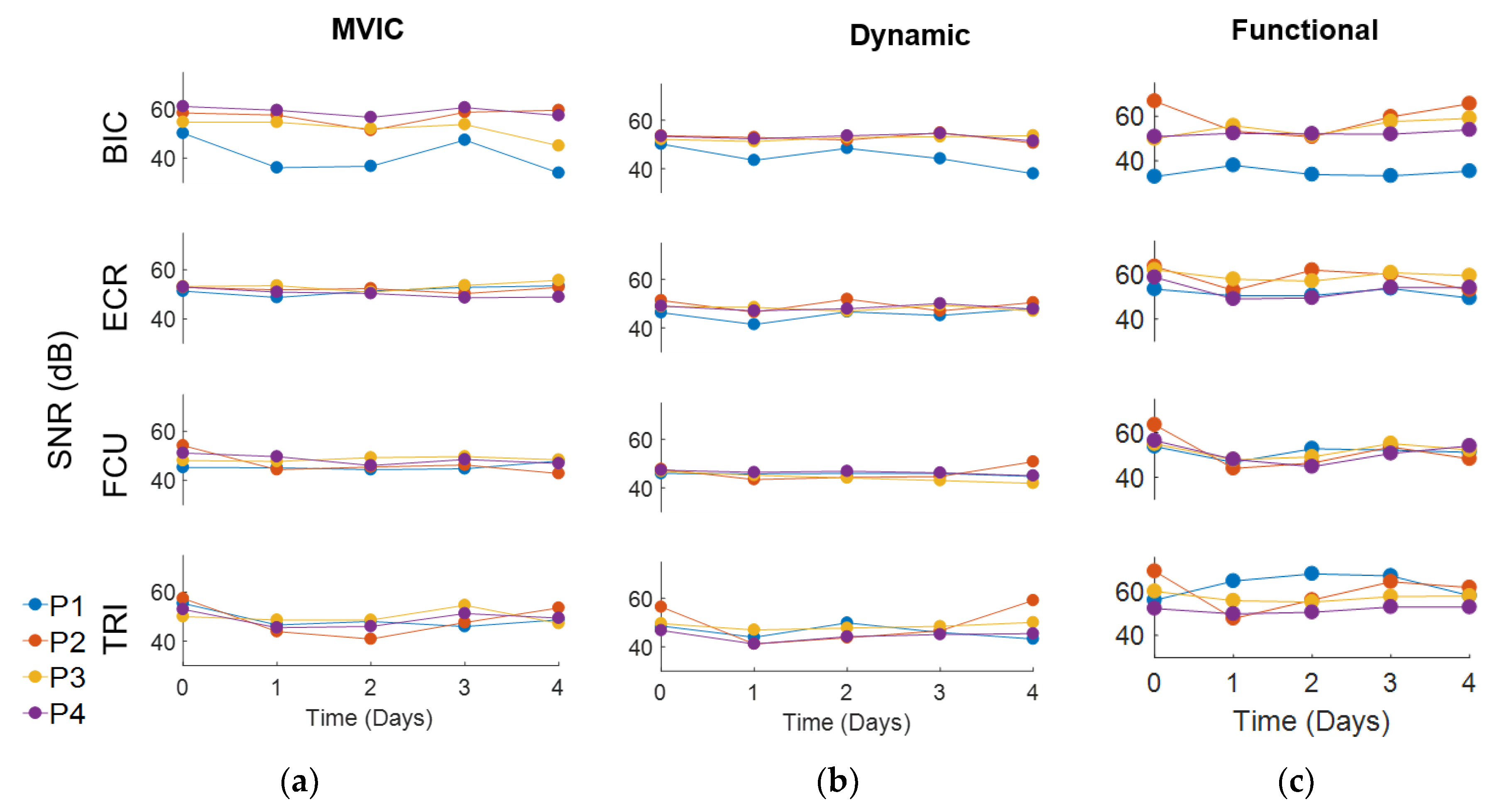
- Signal-to-noise ratio (SNR): Noise was assumed to be any signal present in the upper 20% of the frequency range (above 400 Hz) [31]. The total power across all frequencies was divided by the power of the frequency range above 400 Hz to obtain the SNR. An sEMG signal simulated under ideal conditions with minimum influence of motion and noise artifacts would have an SNR of at least 50 dB, while the sEMG signal influenced by noise would have an SNR of 15 dB or below [31]. A linear regression model was constructed to examine the effect of time, type of muscle, and test on SNR for the Delsys and ESS electrodes. For this calculation, line noise was assumed to be filtered out by the Delsys amplifier for both electrodes.
- Signal-to-motion ratio (SMR): Two assumptions were made to calculate SMR: (1) that all motion noise is under 20 Hz, and (2) that the sEMG signal under 20 Hz is approximately linear [31]. As such, motion noise can be calculated by drawing a line drawn between 0 dB and the peak power between 50 Hz and 150 Hz, and calculating the power above the line from 0 to 20 Hz. The SMR is calculated by dividing the total power across all frequencies by the motion noise. A higher SMR indicates that the sEMG data are less affected by motion artifacts. A linear regression model was also constructed to examine the effect of time and type of muscle on SMR for the Delsys and ESS electrodes.
- Linear regression models: MATLAB was used to run forward stepwise multiple linear regressions (stepwiselm) to determine which variables (time, muscles, tests, and electrodes) were associated with Pearson’s correlation, SNR, and SMR measurements. Fisher transformations were performed on the correlation measurements to obtain normal distributions for analysis. We used the MATLAB function stepwiselm to determine which predictors were important in predicting the output variables to find an optimal linear regression model. Next, the data was fit to the chosen linear regression model using the MATLAB function fitlm to evaluate the magnitude of significant changes with time, muscles, tests, and/or electrodes. While overfitting is a concern to a small sample size of eight participants, the robustops option was used when fitting the linear regression model to make the model less sensitive to outliers that may arise with a small sample. In addition, assumptions of normality were evaluated by plotting and assessing residuals.
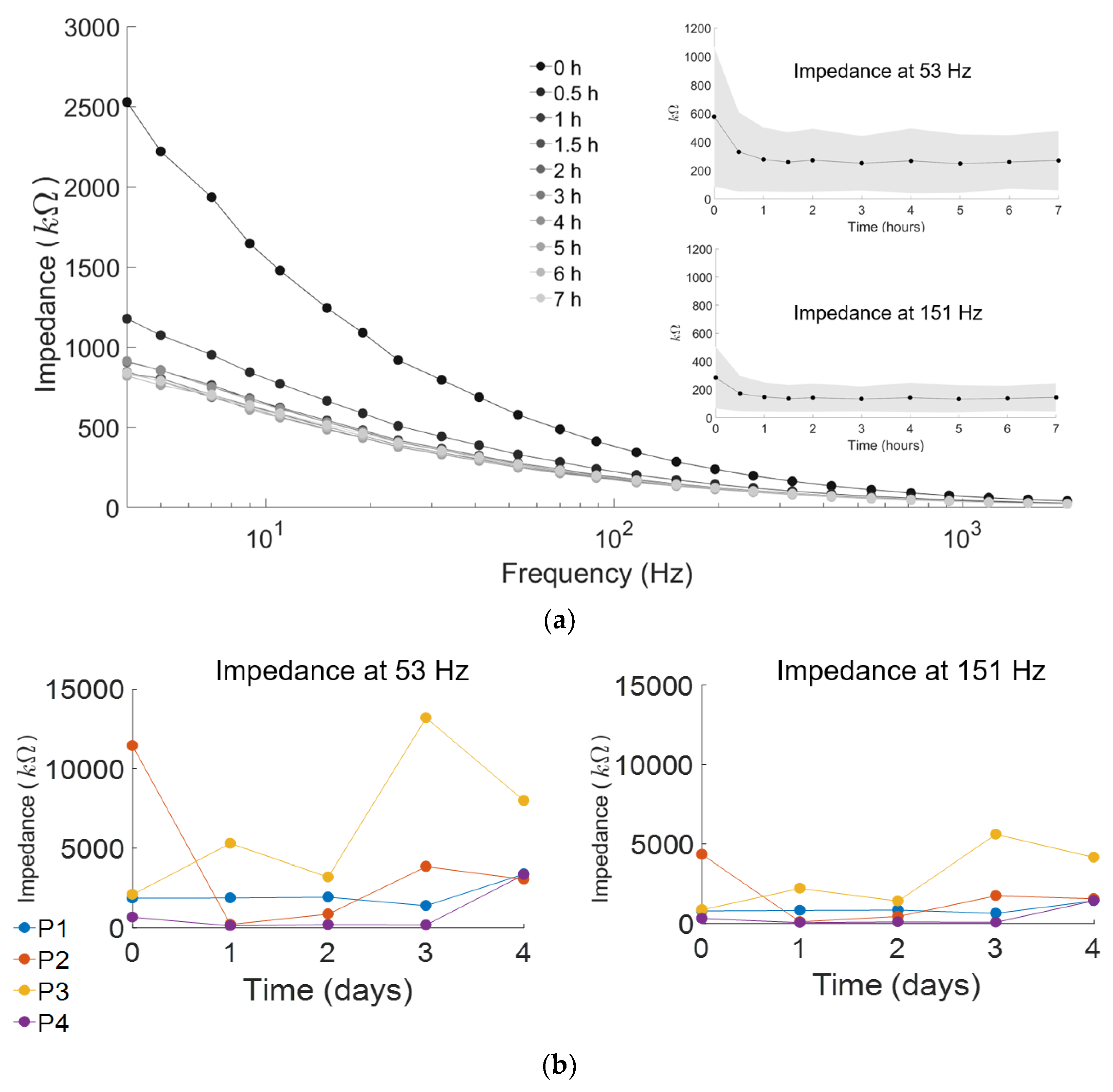
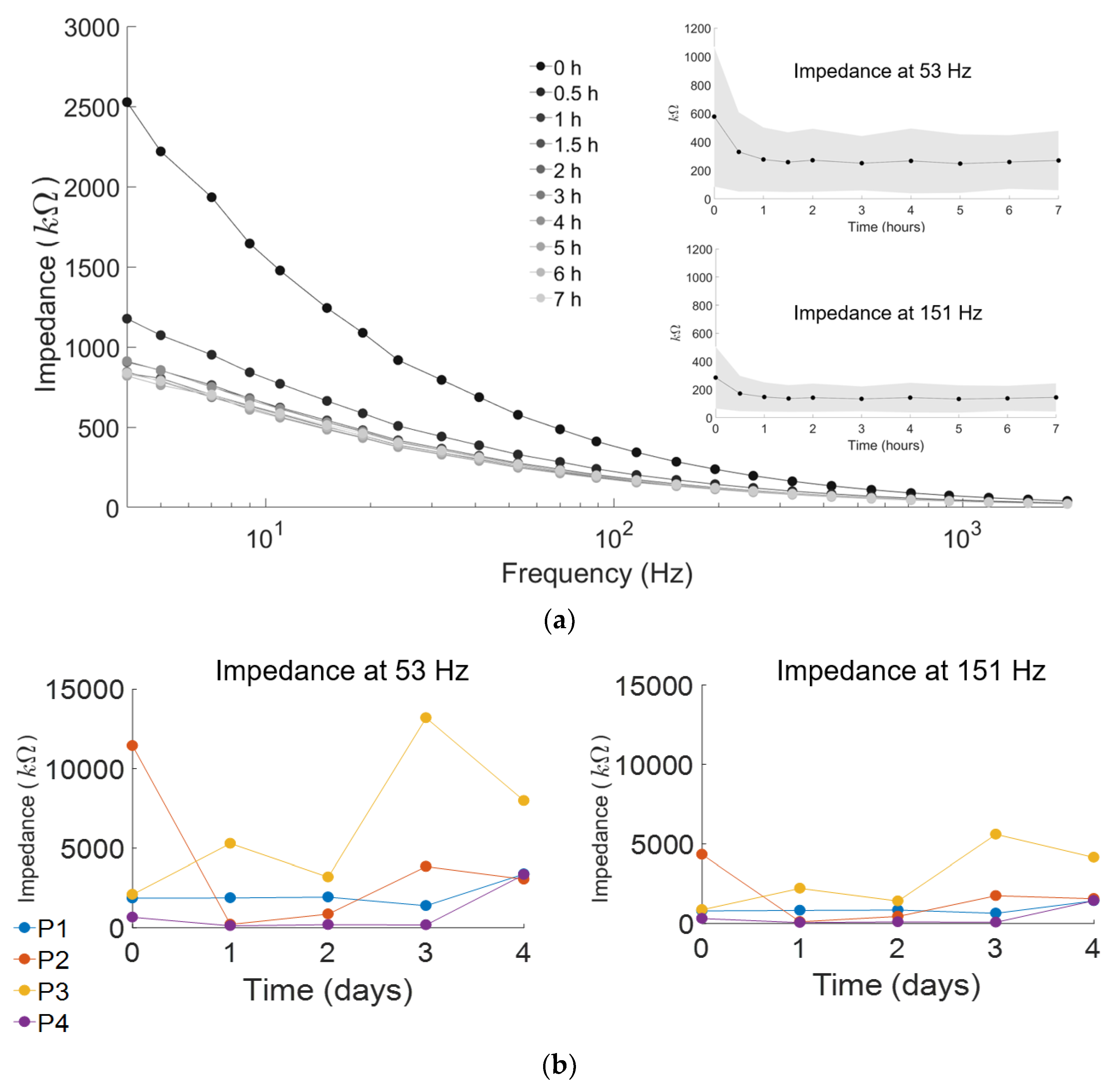
2.4. Stability Testing of ESS Electrode over Seven Hours
2.5. Stability Testing of ESS Electrode over Four Days
3. Results
3.1. Comparison of ESS and Delsys Electrodes
3.2. Signal Consistency of ESS Electrodes
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Enoka, R.M.; Duchateau, J. Physiology of muscle activation and force generation. In Surface Electromyography: Physiology, Engineering and Applications; Merletti, R., Farina, D., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2016; pp. 1–30. ISBN 978-1-118-98702-5. [Google Scholar]
- Saponas, T.S.; Tan, D.S.; Morris, D.; Balakrishnan, R. Demonstrating the feasibility of using forearm electromyography for muscle-computer interfaces. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Florence, Italy, 5–10 April 2008; ACM: Florence, Italy, 2008; pp. 515–524. [Google Scholar]
- Laferriere, P.; Lemaire, E.D.; Chan, A.D. Surface electromyographic signals using dry electrodes. IEEE Trans. Instrum. Meas. 2011, 60, 3259–3268. [Google Scholar] [CrossRef]
- De Luca, C.J. The use of surface electromyography in biomechanics. J. Appl. Biomech. 1997, 13, 135–163. [Google Scholar] [CrossRef]
- Basmajian, J.V.; De Luca, C. Muscles Alive: Their Functions Revealed by Electromyography, Subsequent, Ed. ed; Williams & Wilkins: Philadelphia, PA, USA, 1985; Volume 278, ISBN 978-0683004144. [Google Scholar]
- Crow, J.; Lincoln, N.; Nouri, F.; De Weerdt, W. The effectiveness of EMG biofeedback in the treatment of arm function after stroke. Int. Disabil. Stud. 1989, 11, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Searle, A.; Kirkup, L. A direct comparison of wet, dry and insulating bioelectric recording electrodes. Physiol. Meas. 2000, 21, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Siu, H.C.; Arenas, A.M.; Sun, T.; Stirling, L.A. Implementation of a surface electromyography-based upper extremity exoskeleton controller using learning from demonstration. Sensors 2018, 18, 467. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Liu, Y.; Lv, C.; Sun, D. Hand motion classification using a multi-channel surface electromyography sensor. Sensors 2012, 12, 1130–1147. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.Y.; An, J.-H.; Choi, J.M.; Park, K.S.; Lee, S.H. Flexible polymeric dry electrodes for the long-term monitoring of ECG. Sens. Actuators A Phys. 2008, 143, 423–429. [Google Scholar] [CrossRef]
- Haque, F.; Nancel, M.; Vogel, D. Myopoint: Pointing and clicking using forearm mounted electromyography and inertial motion sensors. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems, Seoul, Korea, 18–23 April 2015; ACM: Seoul, Korea, 2015; pp. 3653–3656. [Google Scholar]
- Qamar, A.; Murad, A.; Rahman, M.M.; Rehman, F.U.; Ahmad, A.; Sadiq, B.; Basalamah, S. A multi-sensory gesture-based login environment. In Proceedings of the 23rd ACM International Conference on Multimedia, Brisbane, Australia, 26–30 October 2015; ACM: Brisbane, Australia, 2015; pp. 763–764. [Google Scholar]
- Nymoen, K.; Haugen, M.R.; Jensenius, A.R. Mumyo–evaluating and exploring the myo armband for musical interaction. In Proceedings of the International Conference on New Interfaces for Musical Expression, Baton Rouge, LA, USA, 31 May–3 June 2015; ACM: Baton Rouge, LA, USA, 2015. [Google Scholar]
- Amatanon, V.; Chanhang, S.; Naiyanetr, P.; Thongpang, S. Sign language-thai alphabet conversion based on electromyogram (EMG). In Proceedings of the 7th Biomedical Engineering International Conference (BMEiCON), Fukuoka, Japan, 26–28 November 2014; IEEE: Fukuoka, Japan, 2014; pp. 1–4. [Google Scholar]
- Abreu, J.G.; Teixeira, J.M.; Figueiredo, L.S.; Teichrieb, V. In Evaluating sign language recognition using the myo armband. In Proceedings of the 2016 XVIII Symposium on Virtual and Augmented Reality (SVR), Gramado, Brazil, 21–24 June 2016; IEEE: Gramado, Brazil, 2016; pp. 64–70. [Google Scholar]
- Adams, J.L.; Dinesh, K.; Xiong, M.; Tarolli, C.G.; Sharma, S.; Sheth, N.; Aranyosi, A.; Zhu, W.; Goldenthal, S.; Biglan, K.M.; et al. Multiple wearable sensors in parkinson and huntington disease individuals: A pilot study in clinic and at home. Digit. Biomark. 2017, 1, 52–63. [Google Scholar] [CrossRef]
- Dinesh, K.; Xiong, M.; Adams, J.; Dorsey, R.; Sharma, G. Signal analysis for detecting motor symptoms in Parkinson’s and Huntington’s disease using multiple body-affixed sensors: A pilot study. In Proceedings of the 2016 IEEE Western New York Image and Signal Processing Workshop (WNYISPW), Rochester, NY, USA, 18 November 2016; IEEE: Rochester, NY, USA, 2016; pp. 1–5. [Google Scholar]
- Bareket, L.; Inzelberg, L.; Rand, D.; David-Pur, M.; Rabinovich, D.; Brandes, B.; Hanein, Y. Temporary-tattoo for long-term high fidelity biopotential recordings. Sci. Rep. 2016, 6, 25727. [Google Scholar] [CrossRef] [PubMed]
- Scalisi, R.; Paleari, M.; Favetto, A.; Stoppa, M.; Ariano, P.; Pandolfi, P.; Chiolerio, A. Inkjet printed flexible electrodes for surface electromyography. Org. Electron. 2015, 18, 89–94. [Google Scholar] [CrossRef]
- Xu, B.; Akhtar, A.; Liu, Y.; Chen, H.; Yeo, W.H.; Park, S.I.; Boyce, B.; Kim, H.; Yu, J.; Lai, H.Y.; et al. An epidermal stimulation and sensing platform for sensorimotor prosthetic control, management of lower back exertion, and electrical muscle activation. Adv. Mater. 2016, 28, 4462–4471. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Lu, N.; Ma, R.; Kim, Y.-S.; Kim, R.H.; Wang, S.; Wu, J.; Won, S.M.; Tao, H.; Islam, A.; et al. Epidermal electronics. Science 2011, 333, 838–843. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.W.; Yeo, W.H.; Akhtar, A.; Norton, J.J.; Kwack, Y.J.; Li, S.; Jung, S.Y.; Su, Y.; Lee, W.; Xia, J.; et al. Materials and optimized designs for human-machine interfaces via epidermal electronics. Adv. Mater. 2013, 25, 6839–6846. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Chen, Y.C.; Nicolini, L.; Pasupathy, P.; Sacks, J.; Su, B.; Yang, R.; Sanchez, D.; Chang, Y.F.; Wang, P.; et al. “Cut-and-paste” manufacture of multiparametric epidermal sensor systems. Adv. Mater. 2015, 27, 6423–6430. [Google Scholar] [CrossRef] [PubMed]
- Posada-Quintero, H.F.; Rood, R.T.; Burnham, K.; Pennace, J.; Chon, K.H. Assessment of carbon/salt/adhesive electrodes for surface electromyography measurements. IEEE J. Transl. Eng. Health Med. 2016, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Marozas, V.; Petrenas, A.; Daukantas, S.; Lukosevicius, A. A comparison of conductive textile-based and silver/silver chloride gel electrodes in exercise electrocardiogram recordings. J. Electrocardiol. 2011, 44, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Kabiri Ameri, S.; Ho, R.; Jang, H.; Tao, L.; Wang, Y.; Wang, L.; Schnyer, D.M.; Akinwande, D.; Lu, N. Graphene electronic tattoo sensors. ACS Nano 2017, 11, 7634–7641. [Google Scholar] [CrossRef] [PubMed]
- Gruetzmann, A.; Hansen, S.; Müller, J. Novel dry electrodes for ECG monitoring. Physiol. Meas. 2007, 28, 1375–1390. [Google Scholar] [CrossRef] [PubMed]
- Konrad, P. The ABC of EMG: A Practical Introduction to Kinesiological Electromyography; Noraxon: Scottsdale, AZ, USA, 2005; Volume 1, pp. 30–35. [Google Scholar]
- Wright, Z.A.; Rymer, W.Z.; Slutzky, M.W. Reducing abnormal muscle coactivation after stroke using a myoelectric-computer interface: A pilot study. Neurorehabilit. Neural Repair 2014, 28, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Piervirgili, G.; Petracca, F.; Merletti, R. A new method to assess skin treatments for lowering the impedance and noise of individual gelled Ag–AgCl electrodes. Physiol. Meas. 2014, 35, 2101–2118. [Google Scholar] [CrossRef] [PubMed]
- Sinderby, C.; Lindstrom, L.; Grassino, A. Automatic assessment of electromyogram quality. J. Appl. Physiol. 1995, 79, 1803–1815. [Google Scholar] [CrossRef] [PubMed]
- Lou, C.; Li, R.; Li, Z.; Liang, T.; Wei, Z.; Run, M.; Yan, X.; Liu, X. Flexible graphene electrodes for prolonged dynamic ECG monitoring. Sensors 2016, 16, 1833. [Google Scholar] [CrossRef] [PubMed]
- Zaino, C.A.; McCoy, S.W. Reliability and comparison of electromyographic and kinetic measurements during a standing reach task in children with and without cerebral palsy. Gait Posture 2008, 27, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Yang, D.; Jiang, L.; Zhang, H.; Liu, H.; Kotani, K. A novel unsupervised adaptive learning method for long-term electromyography (EMG) pattern recognition. Sensors 2017, 17, 1370. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Chen, X.; Liu, A.; Peng, H. A novel phonology-and radical-coded chinese sign language recognition framework using accelerometer and surface electromyography sensors. Sensors 2015, 15, 23303–23324. [Google Scholar] [CrossRef] [PubMed]
- Neuman, M.R.; Chung, C.; Yitzak, M.; Richard, P. 48. Biopotential electrodes. In The Biomedical Engineering Handbook, 2nd ed.; Bronzino, J.D., Ed.; CRC Press: Boca Raton, FL, USA, 2000; ISBN 978-0849385940. [Google Scholar]
- Albulbul, A. Evaluating major electrode types for idle biological signal measurements for modern medical technology. Bioengineering 2016, 3, 20. [Google Scholar] [CrossRef] [PubMed]
- Jebsen, R.H. An objective and standardized test of hand function. Arch. Phys. Med. Rehabil. 1969, 50, 311–319. [Google Scholar] [PubMed]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult norms for the box and block test of manual dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Peters, K.M.; Kelly, V.E.; Chang, T.; Weismann, M.C.; McCoy, S.W.; Steele, K.M. Muscle recruitment and coordination during upper-extremity functional tests. J. Electromyogr. Kinesiol. 2018, 28, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Can Delsys EMG Sensors Measure Skin Impedance? Available online: http://www.Delsys.com/faq-items/can-Delsys-emg-sensors-measure-skin-impedance/ (accessed on 10 February 2018).
- What Factors Affect EMG Signal Quality? Available online: http://www.delsys.com/products/software/emgworks/sqm/factors/ (accessed on 10 February 2018).
- Chvatal, S.A.; Ting, L.H. Common muscle synergies for balance and walking. Front. Comput. Neurosci. 2013, 7, 48. [Google Scholar] [CrossRef]
- Merletti, R.; Di Torino, P. Standards for reporting EMG data. J. Electromyogr. Kinesiol. 1999, 9, 3–4. [Google Scholar]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MVIC | Dynamic | Functional | ||||||
|---|---|---|---|---|---|---|---|---|
| 0 h | 2 h | 4 h | 6 h | 0 h | 6 h | 0 h | 6 h | |
| BIC | 0.90 | 0.93 | 0.93 | 0.94 | 0.90 | 0.84 | 0.90 | 0.91 |
| ECR | 0.95 | 0.96 | 0.95 | 0.95 | 0.88 | 0.84 | 0.90 | 0.85 |
| FCU | 0.91 | 0.93 | 0.96 | 0.95 | 0.91 | 0.91 | 0.87 | 0.87 |
| TRI | 0.91 | 0.87 | 0.89 | 0.87 | 0.84 | 0.83 | 0.82 | 0.81 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamagami, M.; Peters, K.M.; Milovanovic, I.; Kuang, I.; Yang, Z.; Lu, N.; Steele, K.M. Assessment of Dry Epidermal Electrodes for Long-Term Electromyography Measurements. Sensors 2018, 18, 1269. https://doi.org/10.3390/s18041269
Yamagami M, Peters KM, Milovanovic I, Kuang I, Yang Z, Lu N, Steele KM. Assessment of Dry Epidermal Electrodes for Long-Term Electromyography Measurements. Sensors. 2018; 18(4):1269. https://doi.org/10.3390/s18041269
Chicago/Turabian StyleYamagami, Momona, Keshia M. Peters, Ivana Milovanovic, Irene Kuang, Zeyu Yang, Nanshu Lu, and Katherine M. Steele. 2018. "Assessment of Dry Epidermal Electrodes for Long-Term Electromyography Measurements" Sensors 18, no. 4: 1269. https://doi.org/10.3390/s18041269
APA StyleYamagami, M., Peters, K. M., Milovanovic, I., Kuang, I., Yang, Z., Lu, N., & Steele, K. M. (2018). Assessment of Dry Epidermal Electrodes for Long-Term Electromyography Measurements. Sensors, 18(4), 1269. https://doi.org/10.3390/s18041269