
Miniaturized Real-Time PCR on a Q3 System for Rapid KRAS Genotyping

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Primers and Probes Design
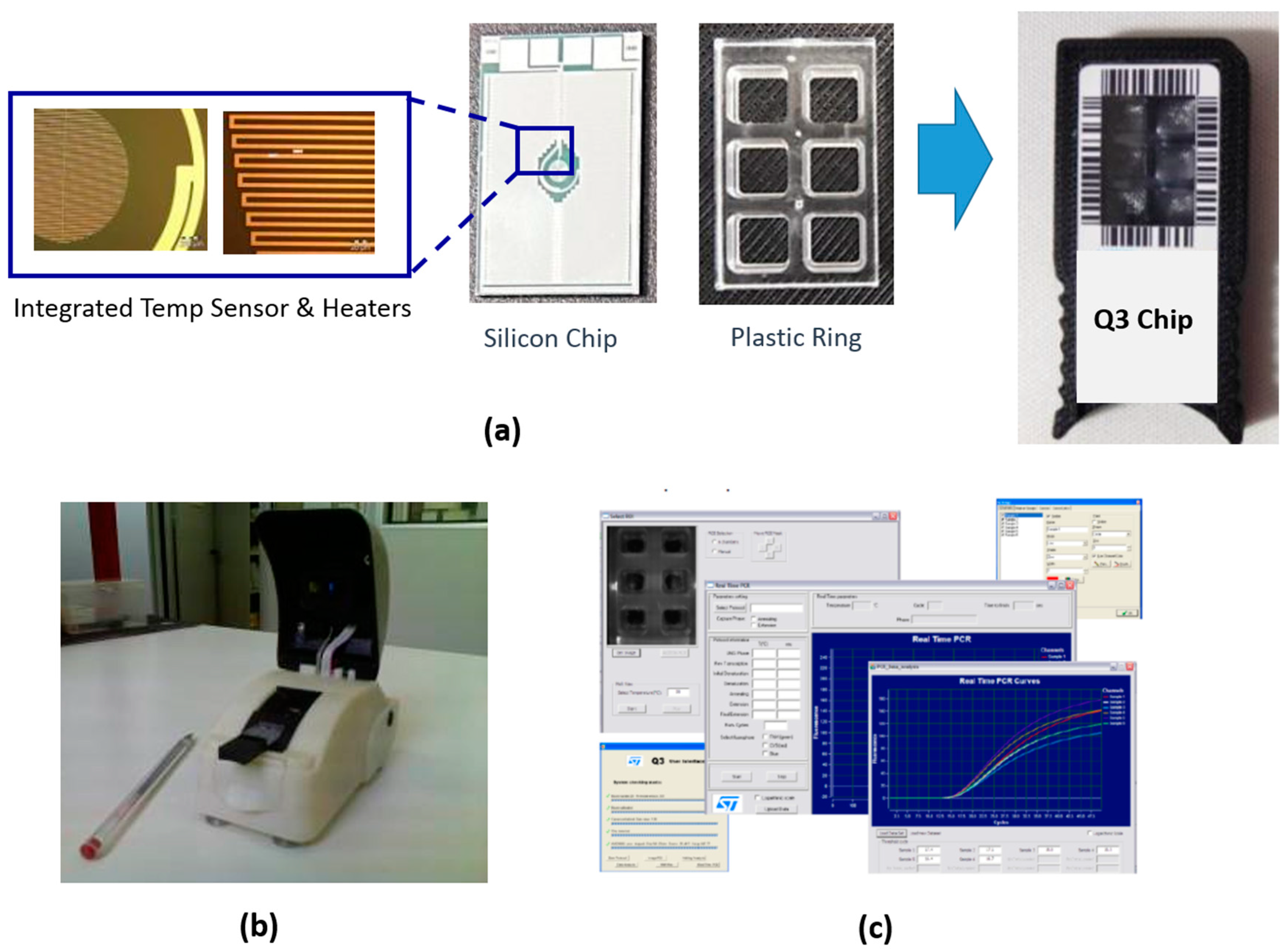
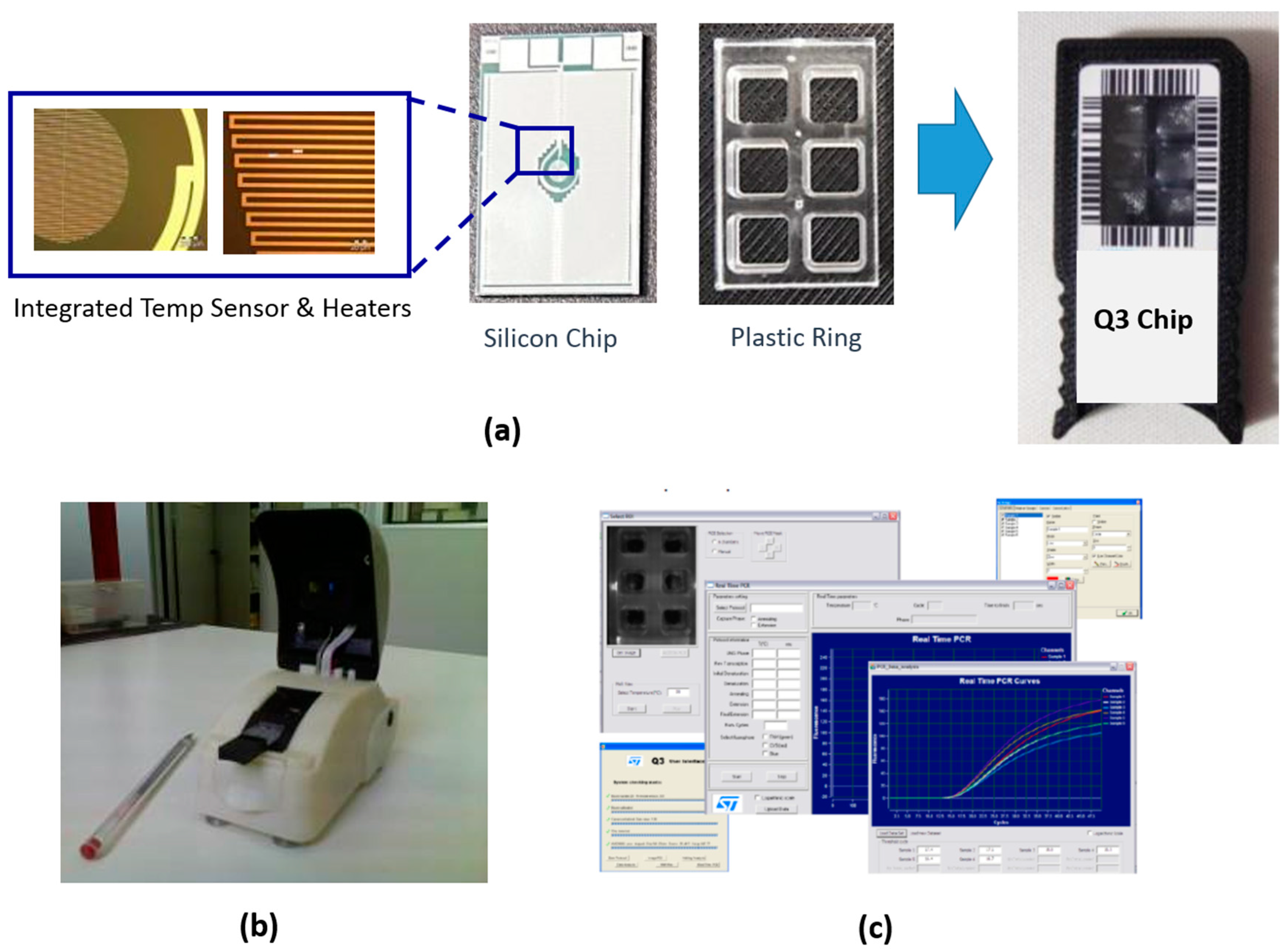
2.2. Real-Time PCR Q3 Platform
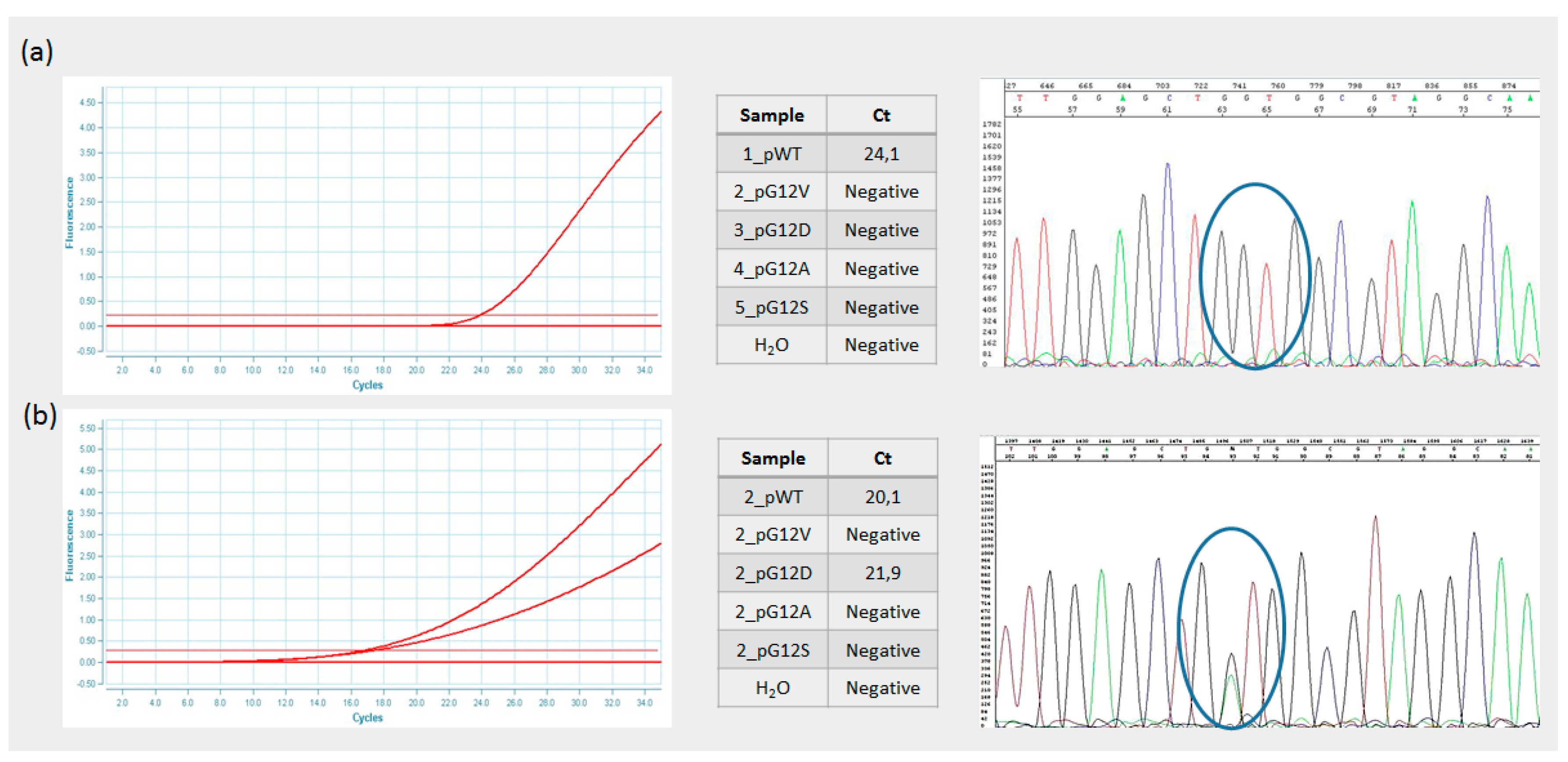
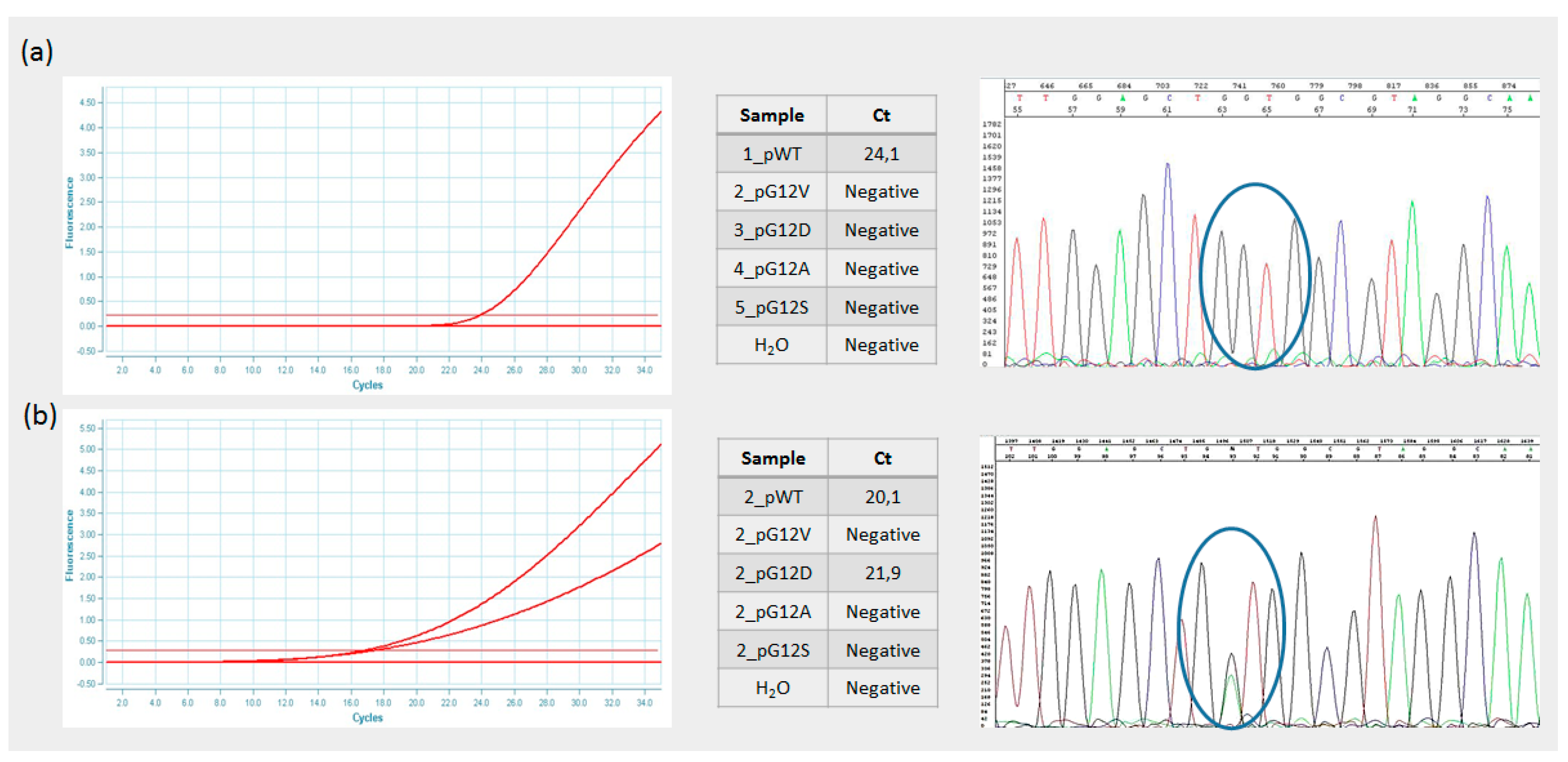
2.3. KRAS Genotyping on Real-Time PCR Q3 Platform
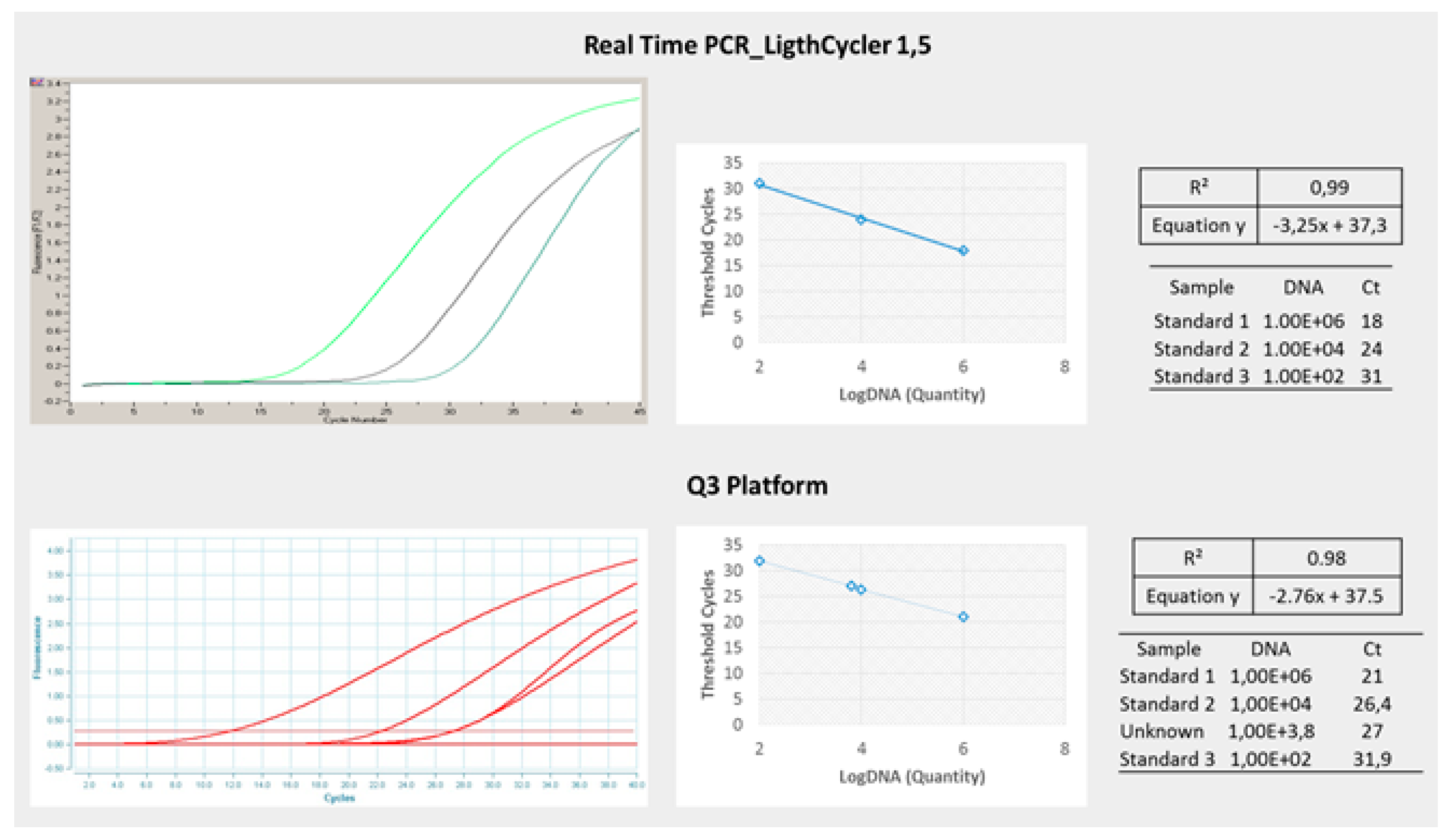
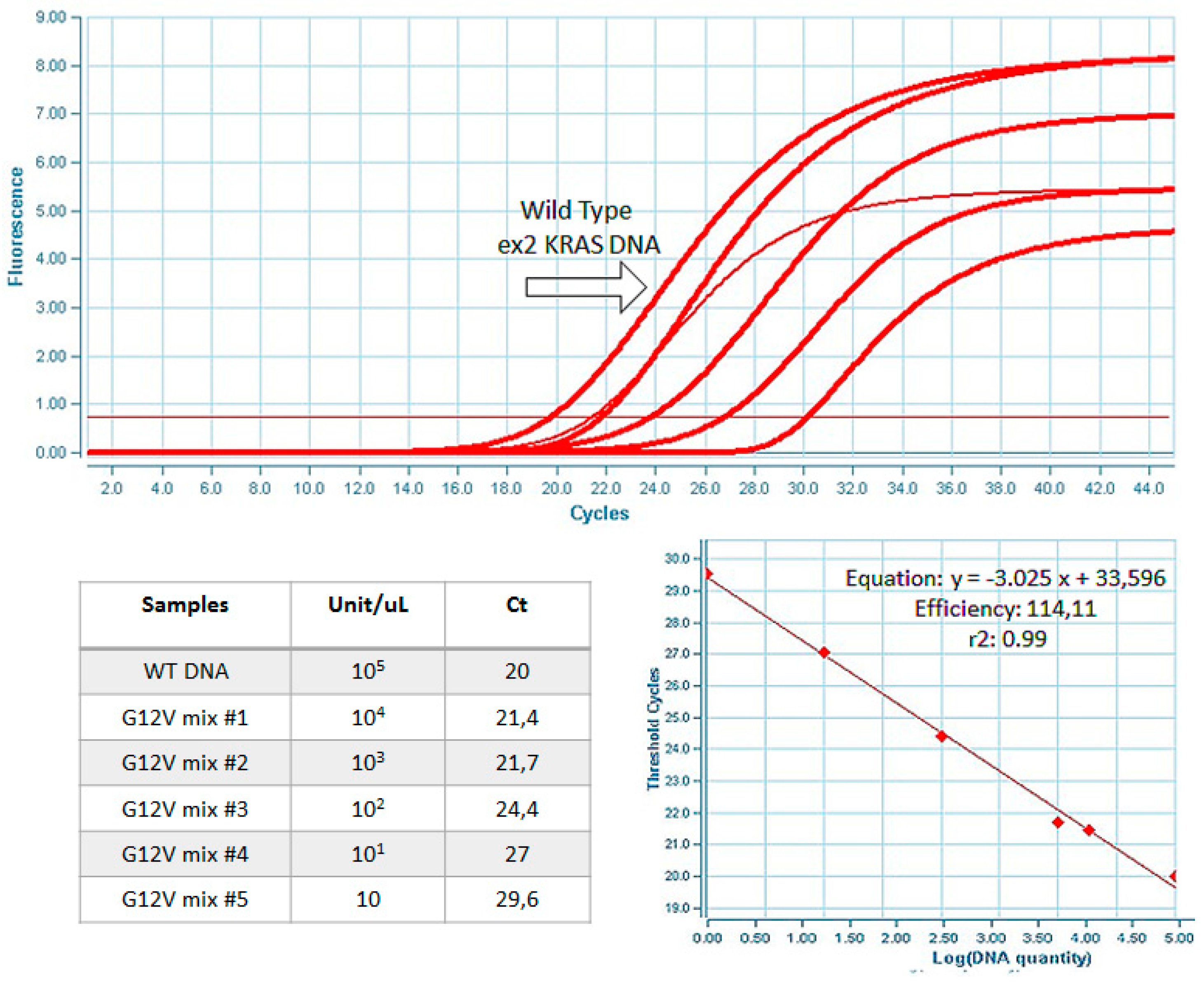
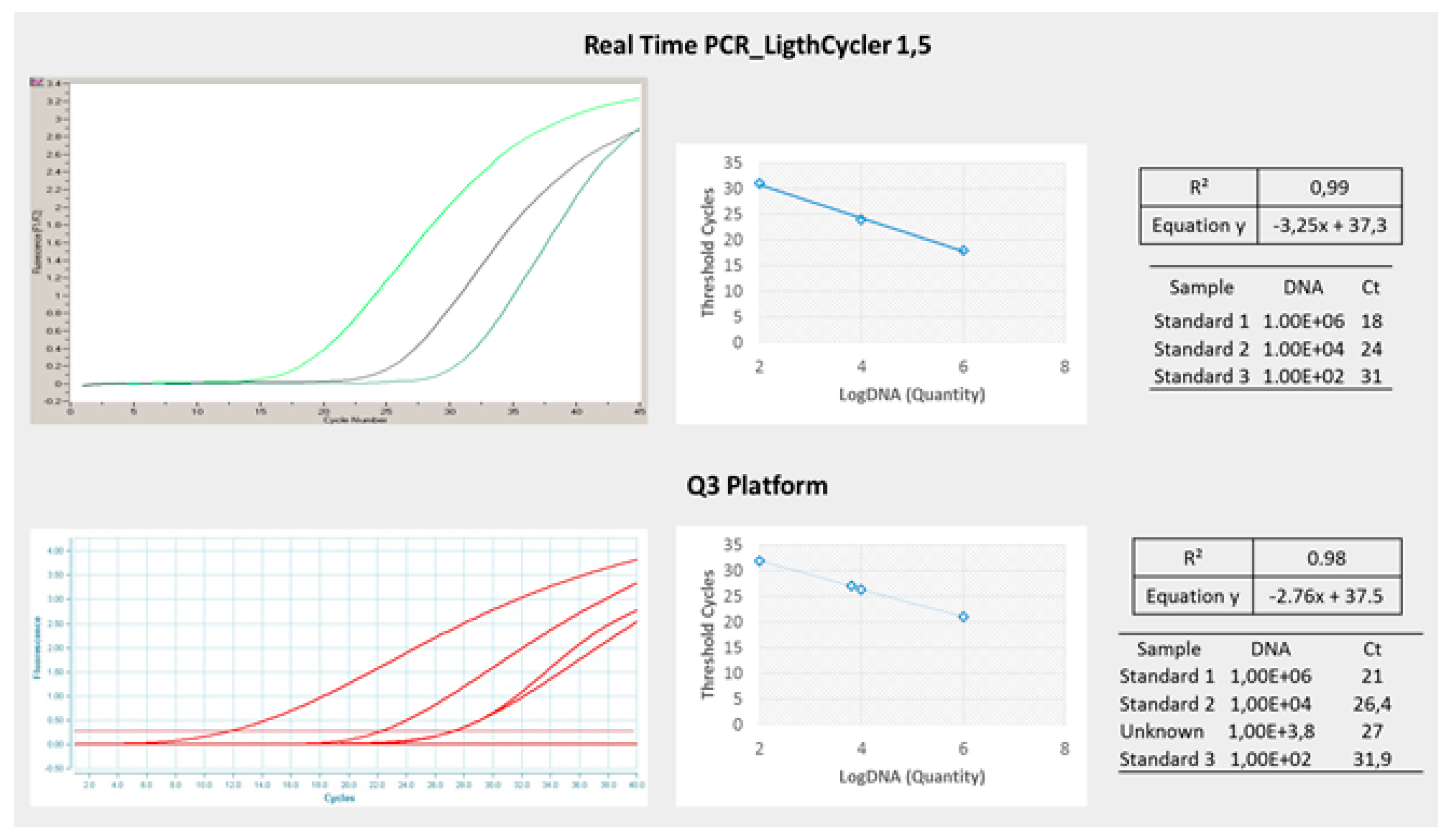
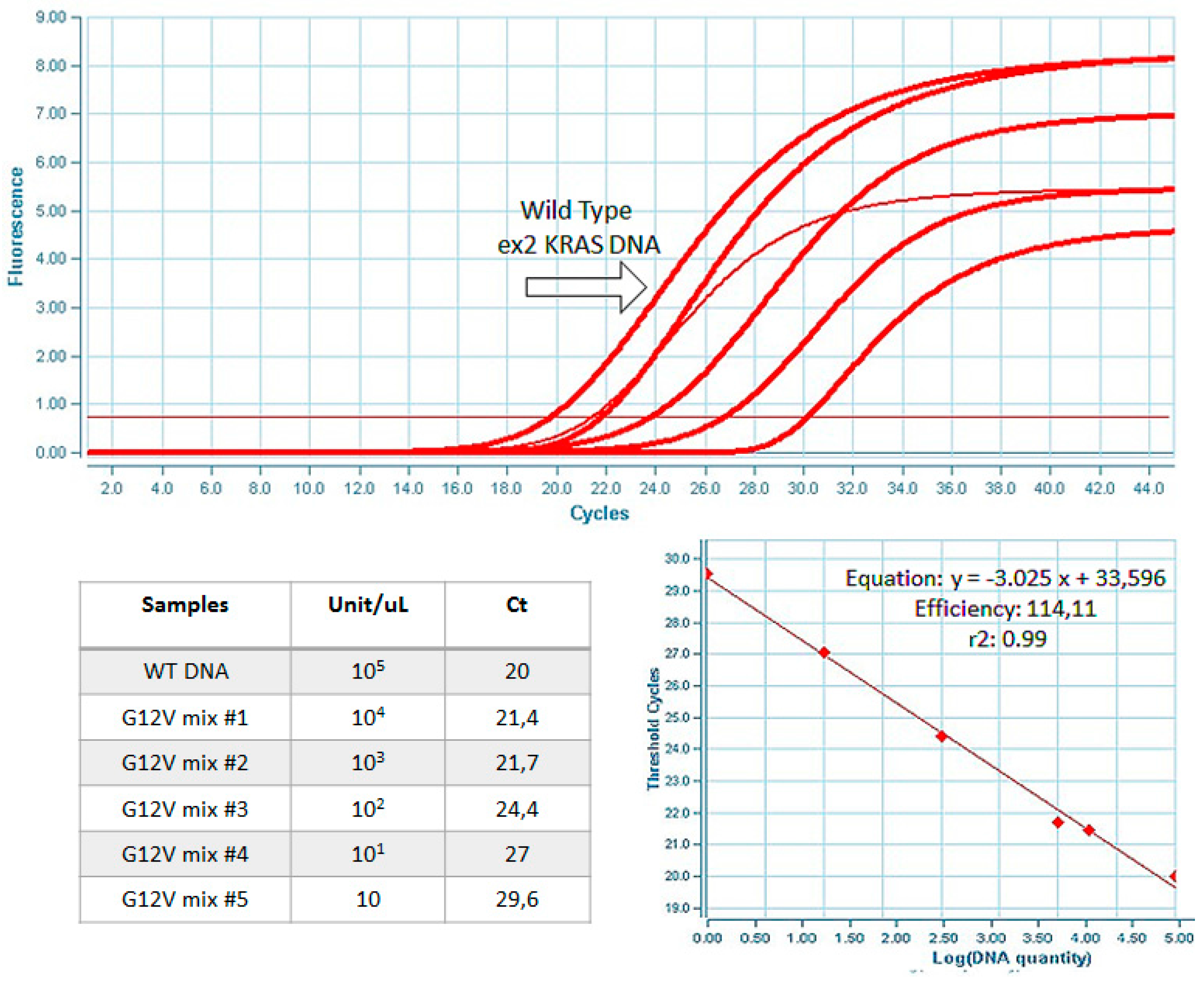
2.4. Assay Validation
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Tan, C.; Du, X. Kras mutation testing in metastatic colorectal cancer. World J. Gastroenterol. 2012, 18, 5171–5180. [Google Scholar] [PubMed]
- Cox, A.D.; Fesik, S.W.; Kimmelman, A.C.; Luo, J.; Der, C.J. Drugging the undruggable ras: Mission possible? Nat. Rev. Drug Discov. 2014, 13, 828–851. [Google Scholar] [CrossRef] [PubMed]
- Nandan, M.O.; Yang, V.W. An update on the biology of ras/raf mutations in colorectal cancer. Curr. Colorectal Cancer Rep. 2011, 7, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Zenonos, K.; Kyprianou, K. Ras signaling pathways, mutations and their role in colorectal cancer. World J. Gastrointest. Oncol. 2013, 5, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zheng, J.; Yang, Y.; Lu, J.; Gao, J.; Lu, T.; Sun, J.; Jiang, H.; Zhu, Y.; Zheng, Y.; et al. Molecular spectrum of kras, nras, braf and pik3ca mutations in chinese colorectal cancer patients: Analysis of 1110 cases. Sci. Rep. 2015, 5, 18678. [Google Scholar] [CrossRef] [PubMed]
- Jancik, S.; Drabek, J.; Radzioch, D.; Hajduch, M. Clinical relevance of kras in human cancers. J. Biomed. Biotechnol. 2010, 2010, 150960. [Google Scholar] [CrossRef] [PubMed]
- Peeters, M.; Kafatos, G.; Taylor, A.; Gastanaga, V.M.; Oliner, K.S.; Hechmati, G.; Terwey, J.H.; van Krieken, J.H. Prevalence of ras mutations and individual variation patterns among patients with metastatic colorectal cancer: A pooled analysis of randomised controlled trials. Eur. J. Cancer 2015, 51, 1704–1713. [Google Scholar] [CrossRef] [PubMed]
- Shackelford, R.E.; Whitling, N.A.; McNab, P.; Japa, S.; Coppola, D. Kras testing: A tool for the implementation of personalized medicine. Genes Cancer 2012, 3, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Eser, S.; Schnieke, A.; Schneider, G.; Saur, D. Oncogenic kras signalling in pancreatic cancer. Br. J. Cancer 2014, 111, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Margonis, G.A.; Kim, Y.; Spolverato, G.; Ejaz, A.; Gupta, R.; Cosgrove, D.; Anders, R.; Karagkounis, G.; Choti, M.A.; Pawlik, T.M. Association between specific mutations in kras codon 12 and colorectal liver metastasis. JAMA Surg. 2015, 150, 722–729. [Google Scholar] [CrossRef] [PubMed]
- Janakiraman, M.; Vakiani, E.; Zeng, Z.; Pratilas, C.A.; Taylor, B.S.; Chitale, D.; Halilovic, E.; Wilson, M.; Huberman, K.; Ricarte Filho, J.C.; et al. Genomic and biological characterization of exon 4 kras mutations in human cancer. Cancer Res. 2010, 70, 5901–5911. [Google Scholar] [CrossRef] [PubMed]
- Atreya, C.E.; Corcoran, R.B.; Kopetz, S. Expanded ras: Refining the patient population. J. Clin. Oncol. 2015, 33, 682–685. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Robb, K.; Vernon, S.; Waller, J. Screening for prevention and early diagnosis of cancer. Am. Psychol. 2015, 70, 119–133. [Google Scholar] [CrossRef] [PubMed]
- Kekelidze, M.; D'Errico, L.; Pansini, M.; Tyndall, A.; Hohmann, J. Colorectal cancer: Current imaging methods and future perspectives for the diagnosis, staging and therapeutic response evaluation. World J. Gastroenterol. 2013, 19, 8502–8514. [Google Scholar] [CrossRef] [PubMed]
- Tsang, A.H.; Cheng, K.H.; Wong, A.S.; Ng, S.S.; Ma, B.B.; Chan, C.M.; Tsui, N.B.; Chan, L.W.; Yung, B.Y.; Wong, S.C. Current and future molecular diagnostics in colorectal cancer and colorectal adenoma. World J. Gastroenterol. 2014, 20, 3847–3857. [Google Scholar] [CrossRef] [PubMed]
- Young, P.E.; Womeldorph, C.M. Colonoscopy for colorectal cancer screening. J. Cancer 2013, 4, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Lech, G.; Slotwinski, R.; Slodkowski, M.; Krasnodebski, I.W. Colorectal cancer tumour markers and biomarkers: Recent therapeutic advances. World J. Gastroenterol. 2016, 22, 1745–1755. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Tanaka, M.; Tanaka, T.; Ishigamori, R. Biomarkers for colorectal cancer. Int. J. Mol. Sci. 2010, 11, 3209–3225. [Google Scholar] [CrossRef] [PubMed]
- Seekhuntod, S.; Thavarungkul, P.; Chaichanawongsaroj, N. Validation of a multiplex allele-specific polymerase chain reaction assay for detection of kras gene mutations in formalin-fixed, paraffin-embedded tissues from colorectal cancer patients. PLoS ONE 2016, 11, e0147672. [Google Scholar] [CrossRef] [PubMed]
- Knickelbein, K.; Zhang, L. Mutant kras as a critical determinant of the therapeutic response of colorectal cancer. Genes Dis. 2015, 2, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Hocking, C.M.; Price, T.J. Panitumumab in the management of patients with kras wild-type metastatic colorectal cancer. Ther. Adv. Gastroenterol. 2014, 7, 20–37. [Google Scholar] [CrossRef] [PubMed]
- Geiger, T.M.; Ricciardi, R. Screening options and recommendations for colorectal cancer. Clin. Colon Rectal Surg. 2009, 22, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Vigneshvar, S.; Sudhakumari, C.C.; Senthilkumaran, B.; Prakash, H. Recent advances in biosensor technology for potential applications—An overview. Front. Bioeng. Biotechnol. 2016, 4, 11. [Google Scholar] [CrossRef] [PubMed]
- Gruhl, F.J.; Rapp, B.E.; Länge, K. Biosensors for diagnostic applications. In Molecular Diagnostics; Seitz, H., Schumacher, S., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 115–148. [Google Scholar]
- Gu, L.Q.; Shim, J.W. Single molecule sensing by nanopores and nanopore devices. Analyst 2010, 135, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Petralia, S.; Sciuto, E.L.; Conoci, S. A novel miniaturized biofilter based on silicon micropillars for nucleic acid extraction. Analyst 2017, 142, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Spata, M.O.; Castagna, M.E.; Conoci, S. Image data analysis in qpcr: A method for smart analysis of DNA amplification. Sens. Bio-Sens. Res. 2015, 6, 79–84. [Google Scholar] [CrossRef]
- Misale, S.; Yaeger, R.; Hobor, S.; Scala, E.; Janakiraman, M.; Liska, D.; Valtorta, E.; Schiavo, R.; Buscarino, M.; Siravegna, G.; et al. Emergence of kras mutations and acquired resistance to anti-egfr therapy in colorectal cancer. Nature 2012, 486, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Kerr, E.M.; Gaude, E.; Turrell, F.K.; Frezza, C.; Martins, C.P. Mutant kras copy number defines metabolic reprogramming and therapeutic susceptibilities. Nature 2016, 531, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Ogino, S.; Nishihara, R.; VanderWeele, T.J.; Wang, M.; Nishi, A.; Lochhead, P.; Qian, Z.R.; Zhang, X.; Wu, K.; Nan, H.; et al. Review article: The role of molecular pathological epidemiology in the study of neoplastic and non-neoplastic diseases in the era of precision medicine. Epidemiology 2016, 27, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Hamada, T.; Keum, N.; Nishihara, R.; Ogino, S. Molecular pathological epidemiology: New developing frontiers of big data science to study etiologies and pathogenesis. J. Gastroenterol. 2017, 52, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Ben Amar, A.; Kouki, A.B.; Cao, H. Power approaches for implantable medical devices. Sensors 2015, 15, 28889–28914. [Google Scholar] [CrossRef] [PubMed]
- Song, H.O.; Kim, J.H.; Ryu, H.S.; Lee, D.H.; Kim, S.J.; Kim, D.J.; Suh, I.B.; Choi du, Y.; In, K.H.; Kim, S.W.; et al. Polymeric labchip real-time pcr as a point-of-care-potential diagnostic tool for rapid detection of influenza a/h1n1 virus in human clinical specimens. PLoS ONE 2012, 7, e53325. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primer | Sequence | Product Length (bp) |
|---|---|---|
| KRAS-F | 5’-GACTGAATATAAACTTGTGGTAGTTGGA-3’ | 98 |
| KRAS-R | 5’-CATATTCGTCCACAAAATGATTCTGA-3’ | |
| G12S | 5’-AATATAAACTTGTGGTAGTTGGAGCTA-3’ | 90 |
| G12R | 5’-AATATAAACTTGTGGTAGTTGGAGCTC-3’ | 90 |
| G12C | 5’-AATATAAACTTGTGGTAGTTGGAGCTT-3’ | 90 |
| G12D | 5’-AACTTGTGGTAGTTGGAGCTGA-3’ | 84 |
| G12A | 5’-CTTGTGGTAGTTGGAGCTGC-3’ | 82 |
| G12V | 5’-ACTTGTGGTAGTTGGAGCTGT-3’ | 83 |
| G13D | 5’-GTGGTAGTTGGAGCTGGTGA-3’ | 79 |
| Probe | Sequence | |
| KRAS | 5’-FAM-CTGTATCGTCAAGGCACTCT-MGB-3’ |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guarnaccia, M.; Iemmolo, R.; Petralia, S.; Conoci, S.; Cavallaro, S. Miniaturized Real-Time PCR on a Q3 System for Rapid KRAS Genotyping. Sensors 2017, 17, 831. https://doi.org/10.3390/s17040831
Guarnaccia M, Iemmolo R, Petralia S, Conoci S, Cavallaro S. Miniaturized Real-Time PCR on a Q3 System for Rapid KRAS Genotyping. Sensors. 2017; 17(4):831. https://doi.org/10.3390/s17040831
Chicago/Turabian StyleGuarnaccia, Maria, Rosario Iemmolo, Salvatore Petralia, Sabrina Conoci, and Sebastiano Cavallaro. 2017. "Miniaturized Real-Time PCR on a Q3 System for Rapid KRAS Genotyping" Sensors 17, no. 4: 831. https://doi.org/10.3390/s17040831
APA StyleGuarnaccia, M., Iemmolo, R., Petralia, S., Conoci, S., & Cavallaro, S. (2017). Miniaturized Real-Time PCR on a Q3 System for Rapid KRAS Genotyping. Sensors, 17(4), 831. https://doi.org/10.3390/s17040831