
Visualization of Venous Compliance of Superficial Veins Using Non-Contact Plethysmography Based on Digital Red-Green-Blue Images

Abstract
:1. Introduction
2. Materials and Methods
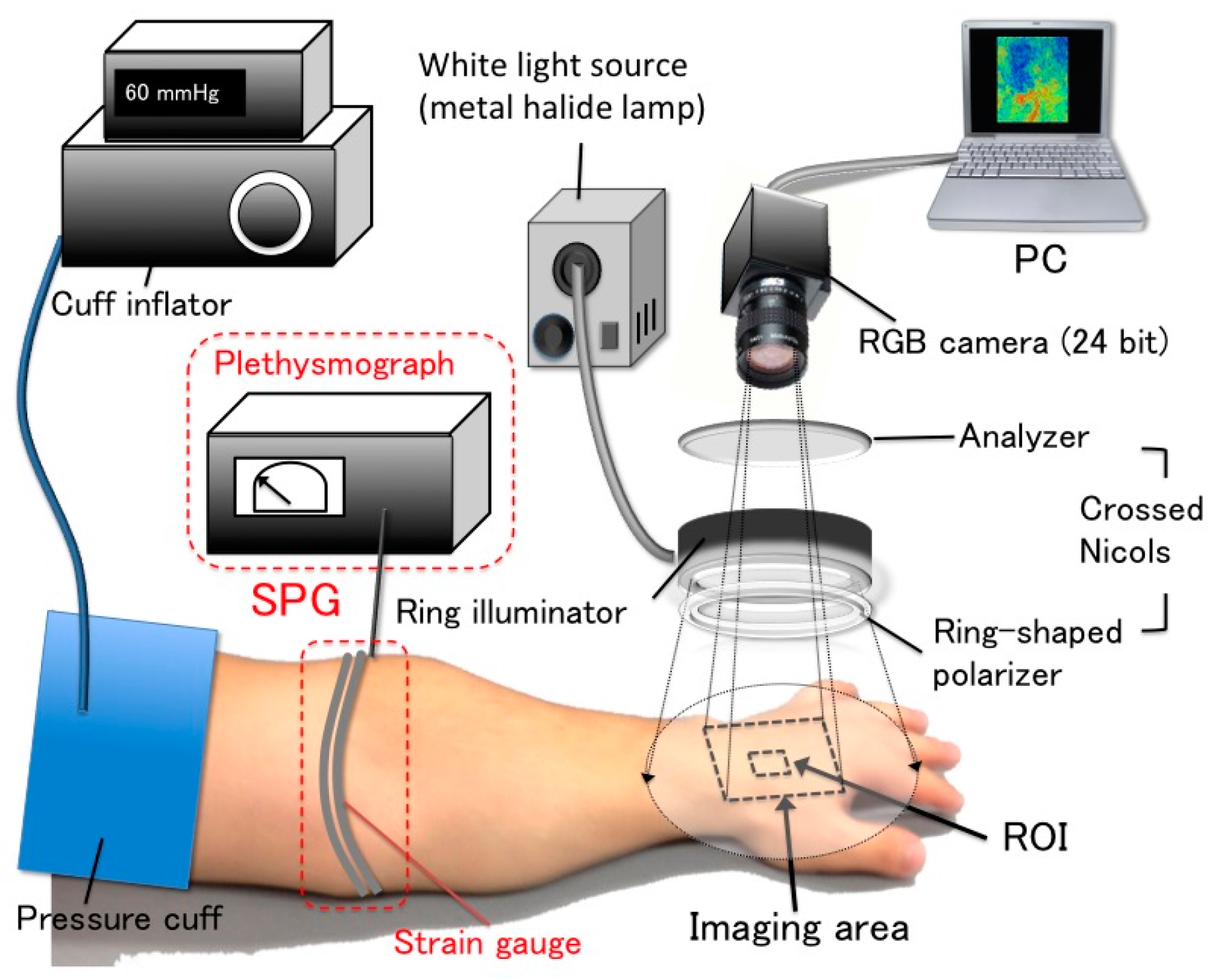
2.1. NCPG for VC Using an RGB Camera Combined with SPG
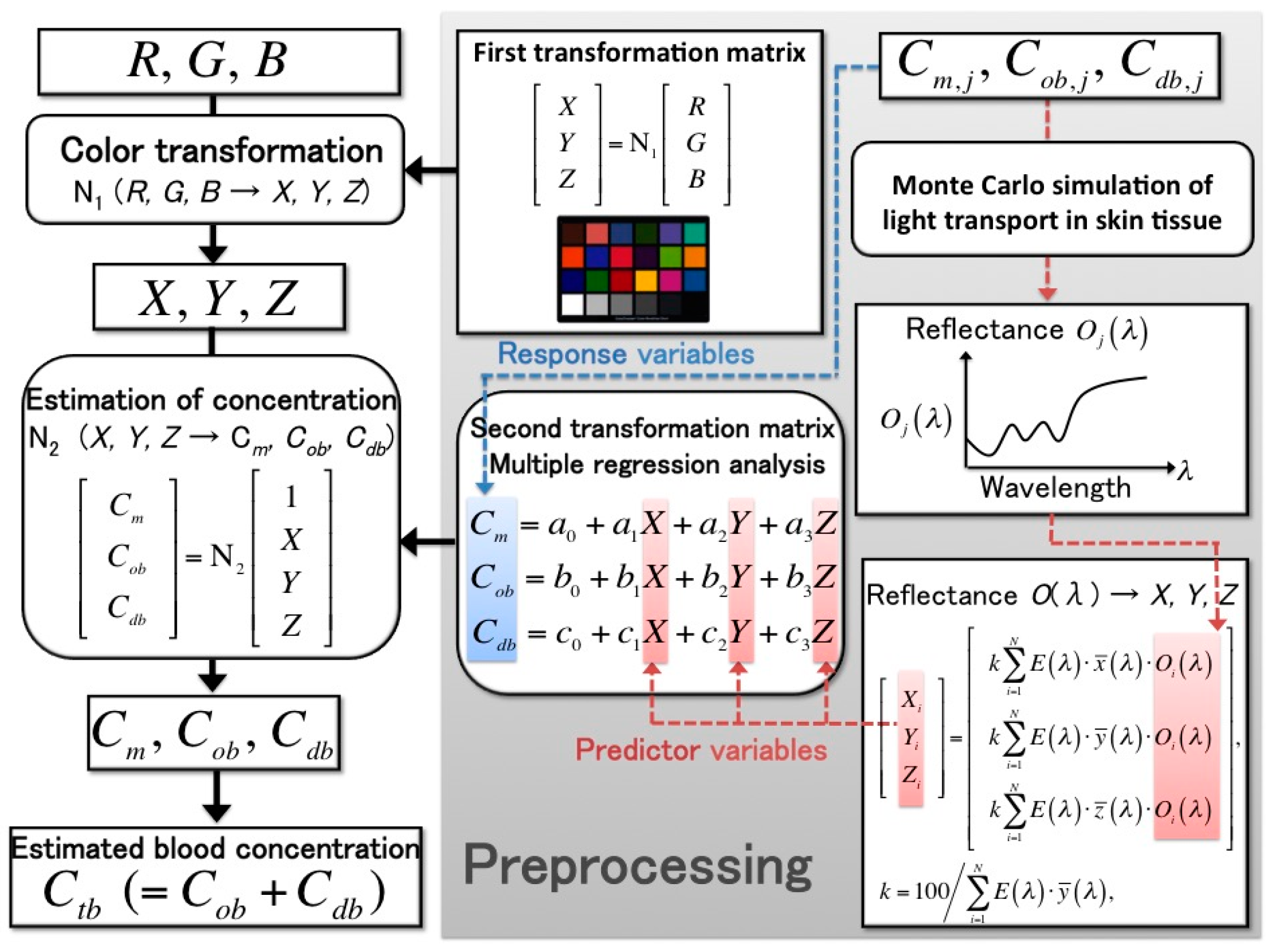
2.2. Estimation Method of Skin Chromophore Concentration from RGB Values
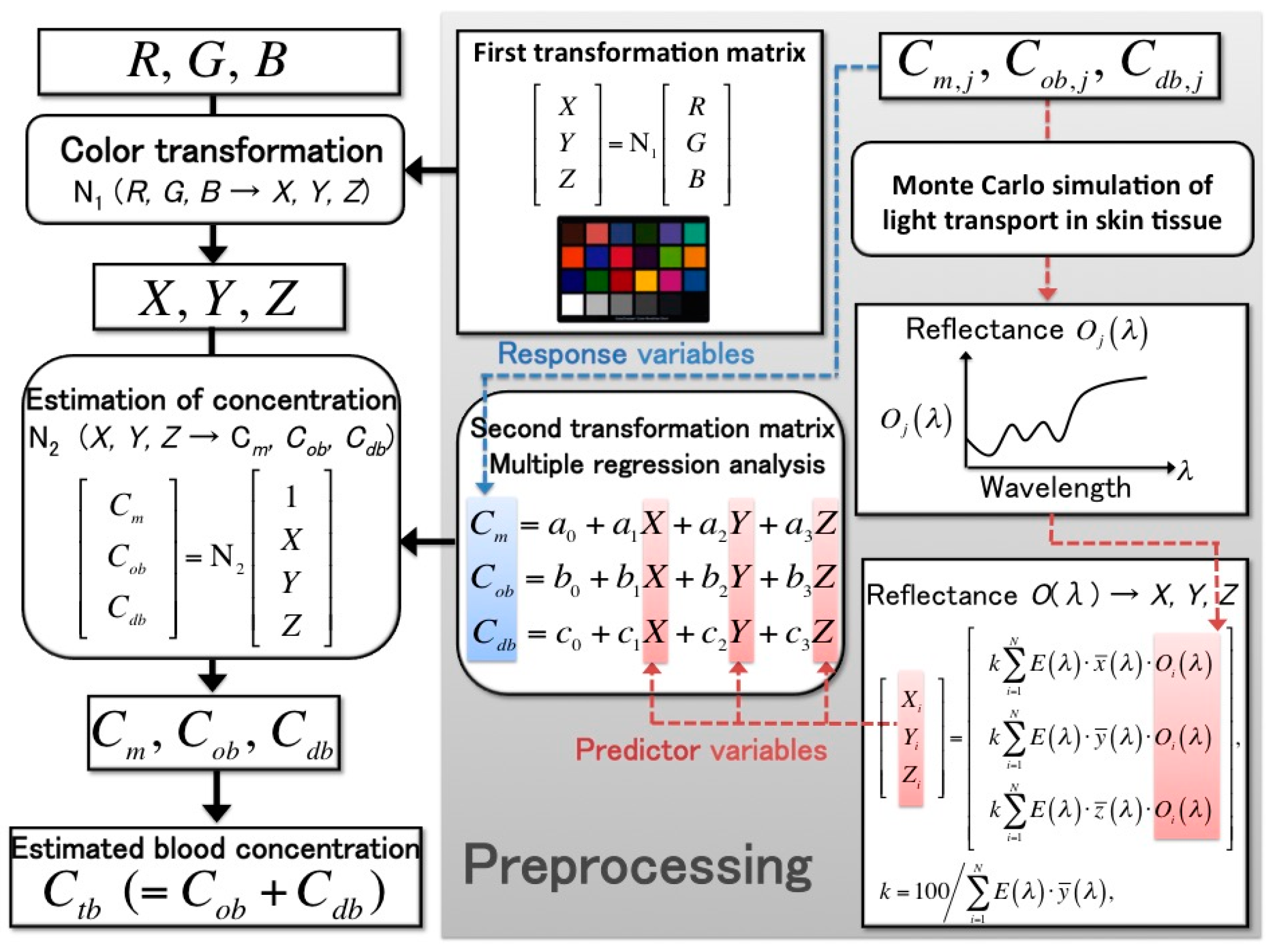
- Step 1:
- We calculated the color transformation matrix N1 that can transform RGB values into Commission Internationale de l’Éclairage XYZ (CIEXYZ) tristimulus values. The matrix N1 was determined in advance using a standard color chart. We measured the RGB values of a standard color chart (ColorChecker®, X-Rite Incorporated, Grand Rapids, MI, USA) consisting of 24 color chips. The diffuse reflectance spectra O(λ) for each chip were supplied with the chart. The CIEXYZ values for the specific illuminant E(λ) were calculated as follows:where Xi, Yi, and Zi are the CIEXYZ values; , , and are color-matching functions in the CIEXYZ color system; N is the total number of diffuse reflectance spectra; k is a constant whose value results in Y = 100 for a perfect diffuser. In this step, the XYZ value was calculated from each reflectance spectrum for 24 color chips (N = 24). Next, the transformation matrix N1 was determined using multiple regression analysis (MRA), in which the calculated XYZ values were the response variables and the measured RGB values were the predictor variables. The resulting regression coefficients were the elements of N1. If the RGB values of the color chips change by replacing the camera or the light source in the imaging system, the matrix N1 must be recalculated:
- Step 2:
- The second transformation matrix N2, which was used to transform the XYZ values into blood concentration values, was determined next. The skin chromophore concentrations—i.e., the melanin concentration Cm, the oxygenated blood concentration Cob, and the deoxygenated blood concentration Cdb—represent the light absorption coefficients of the skin tissue. Using various combinations of these three concentrations, we employed a Monte Carlo simulation (MCS) model of the transit of light in human skin to calculate the diffuse reflectance spectra of the skin surface O(λ). The parameters of the MCS used in this study—such as the absorption coefficient, the scattering coefficient, the refractive index, and the layer thickness of skin tissue—were those employed in an earlier study [20]. Moreover, to determine matrix N2, we used the simulation to calculate 300 diffuse reflectance spectra in the wavelength range 400–700 nm at intervals of 10 nm [20]. After the XYZ values were calculated by integrating the diffuse reflectance spectra from Equation (1), which were obtained using MCS, the transformation matrix N2 was determined using MRA:
- Step 3:
- The XYZ values, which were transformed from the measured RGB values using the first matrix, N1, were transformed into the skin chromophore concentrations Cm, Cob, and Cdb using matrix N2. Thus, the total blood concentration was calculated as Ctb = Cob + Cdb. The absorption coefficients of blood for the case of Ctb = 100% were set to those of blood with a 44% hematocrit and 150 g/L of hemoglobin.
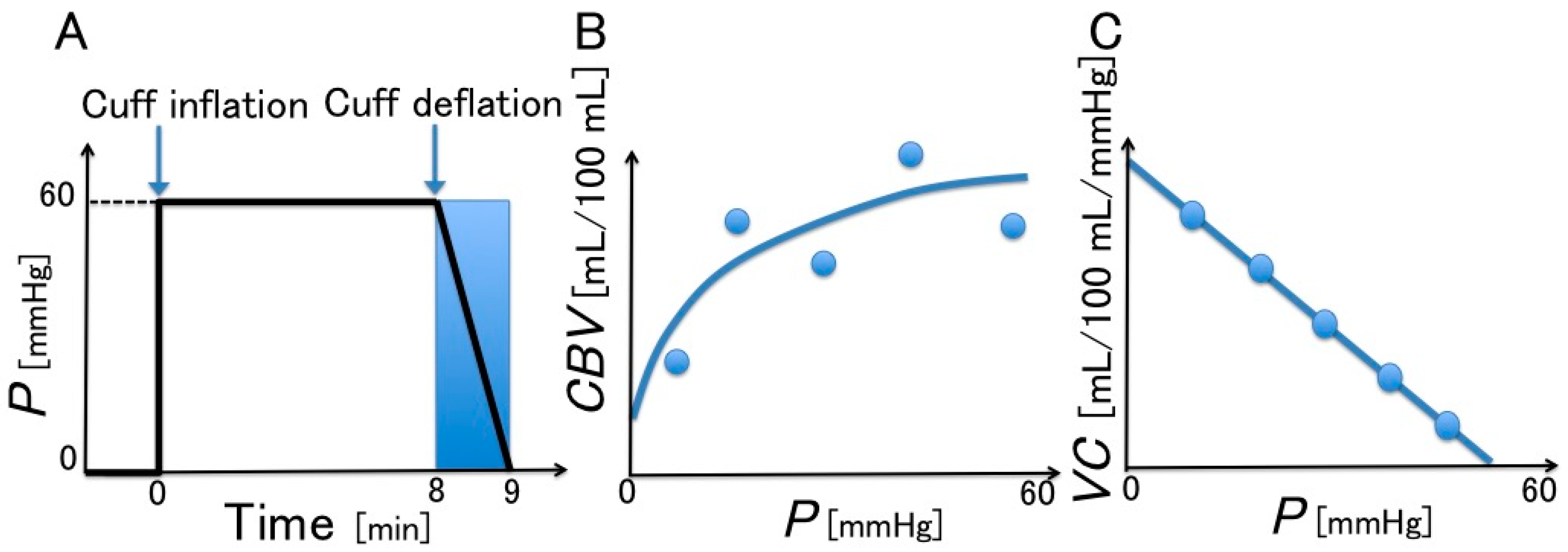
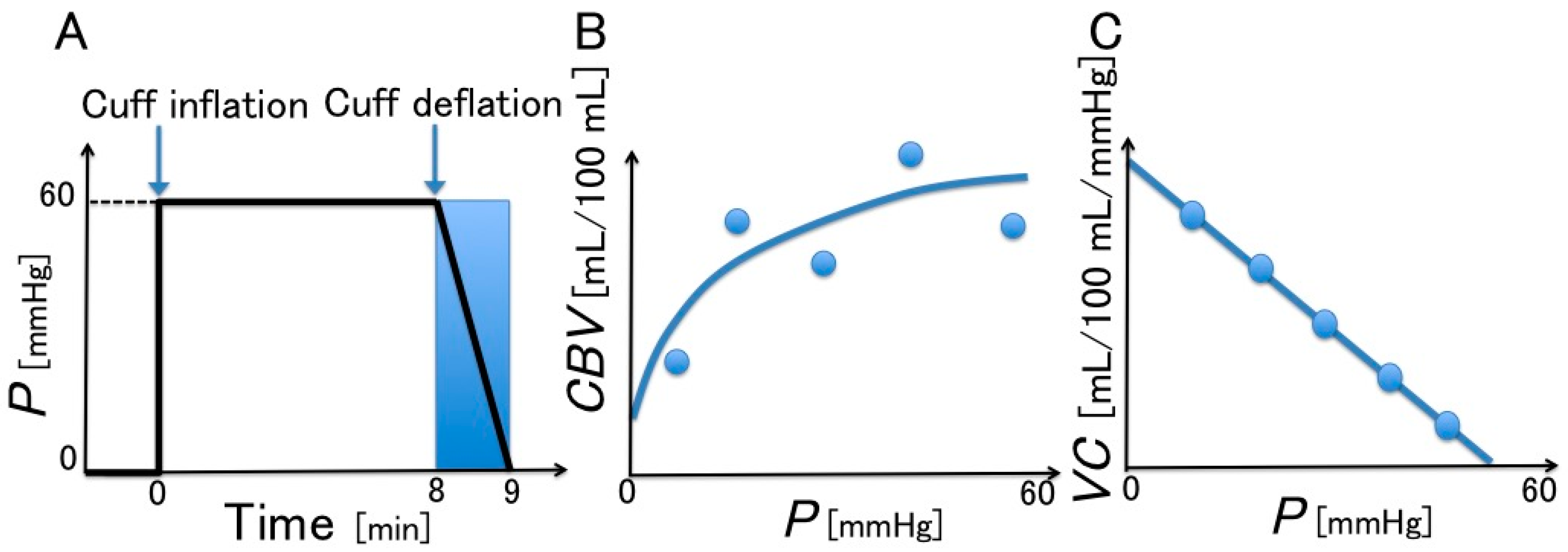
2.3. Evaluation of VC
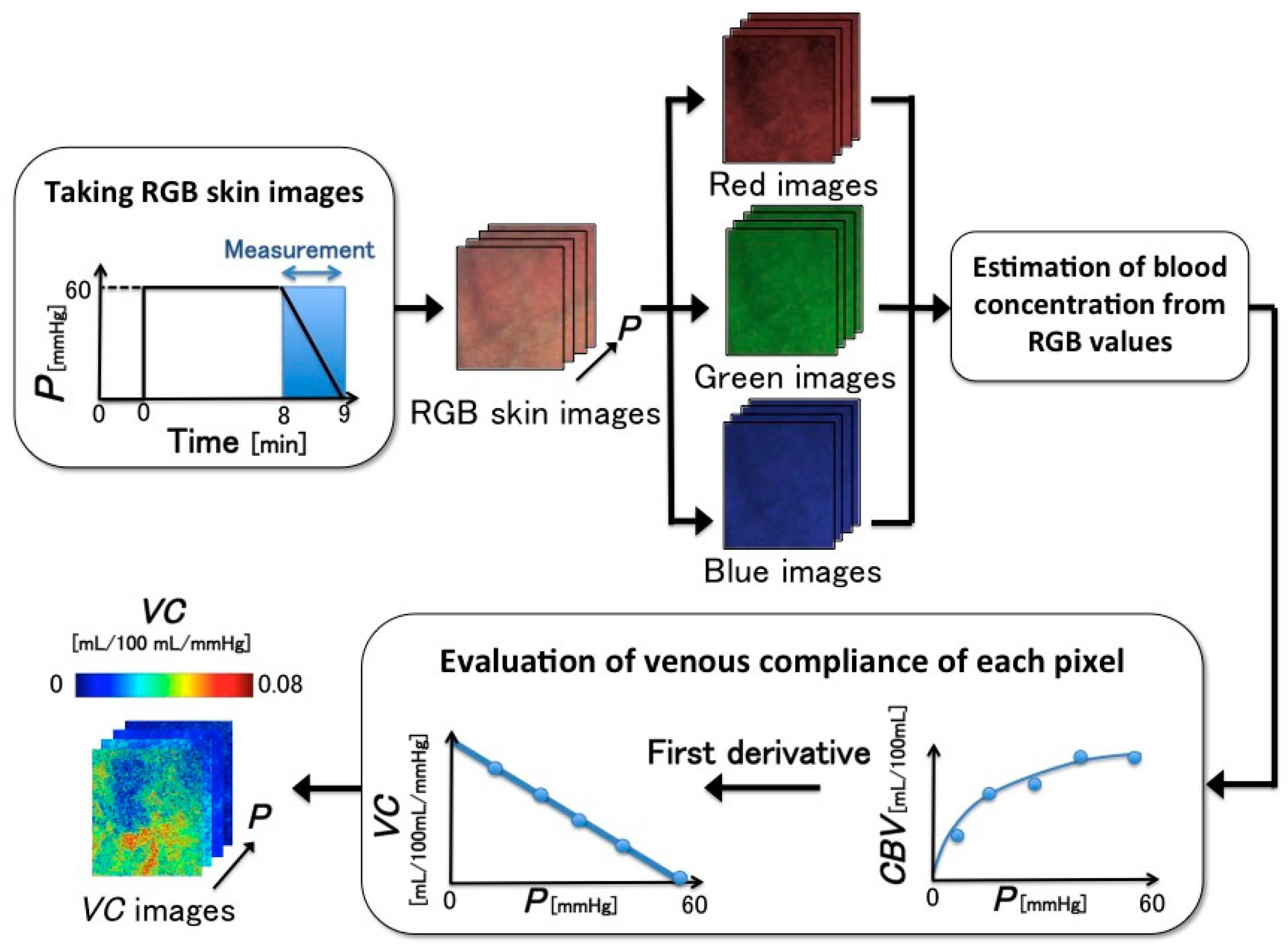
2.4. VC Imaging
2.5. Differences between the Two Measurement Systems
2.6. Experimental Conditions
- Q1 (Past habits): Did you perform any physical activity on a daily basis within the past year?
- Q2 (Current habits): Do you perform any physical activity more than two hours per week?
3. Results and Discussion
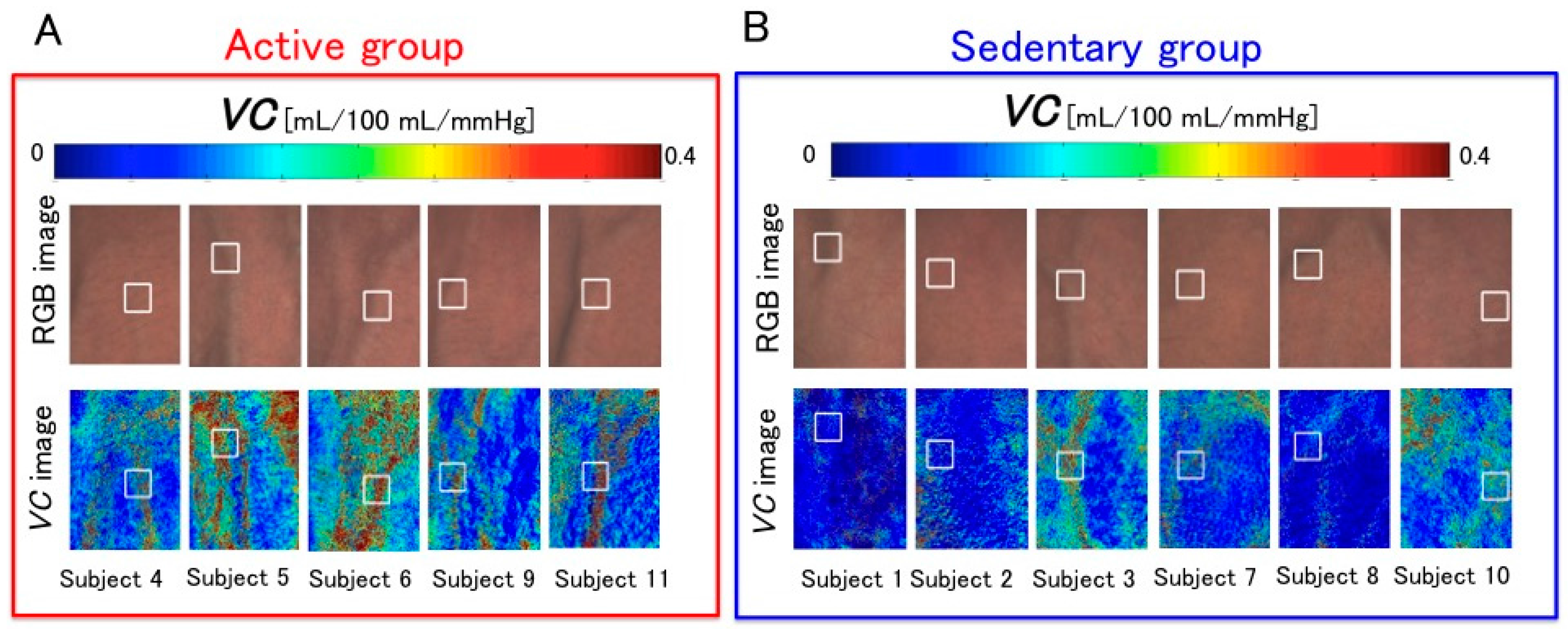
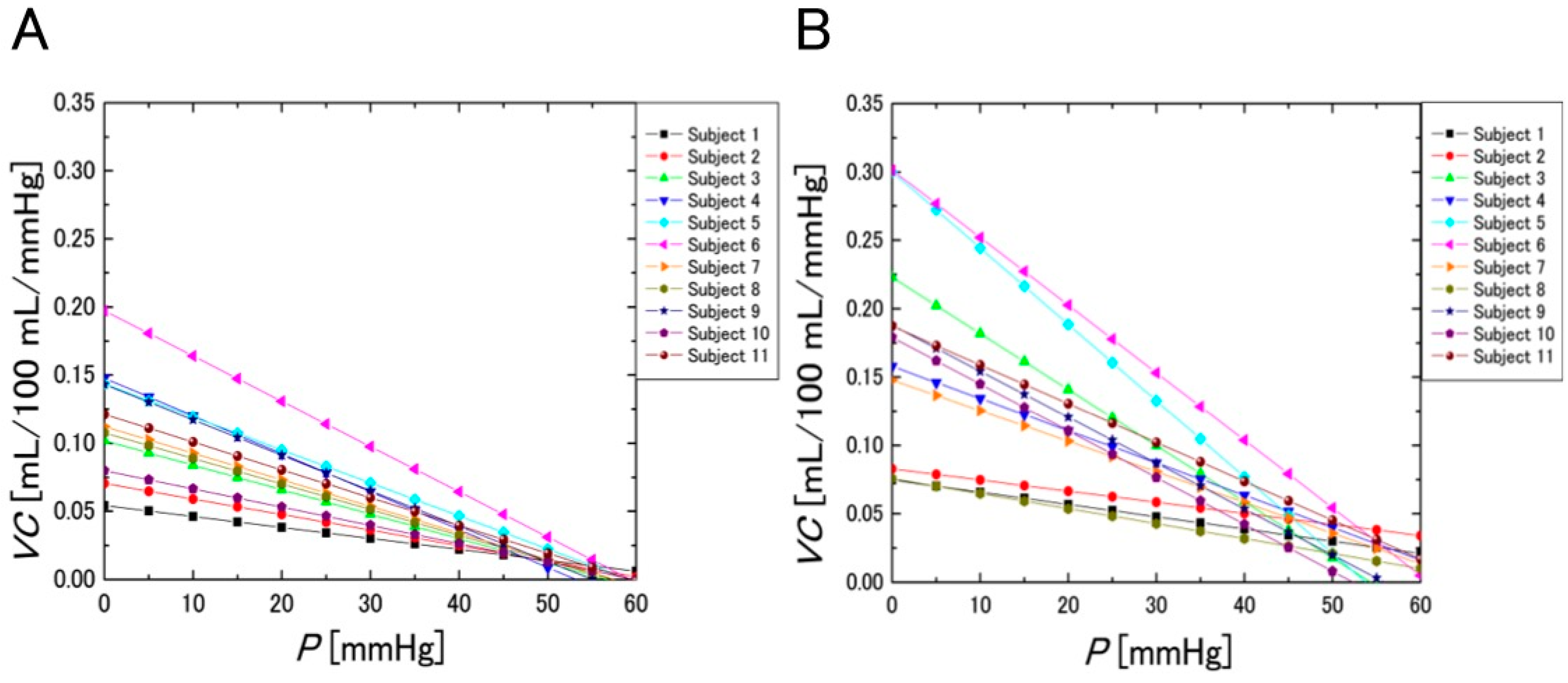
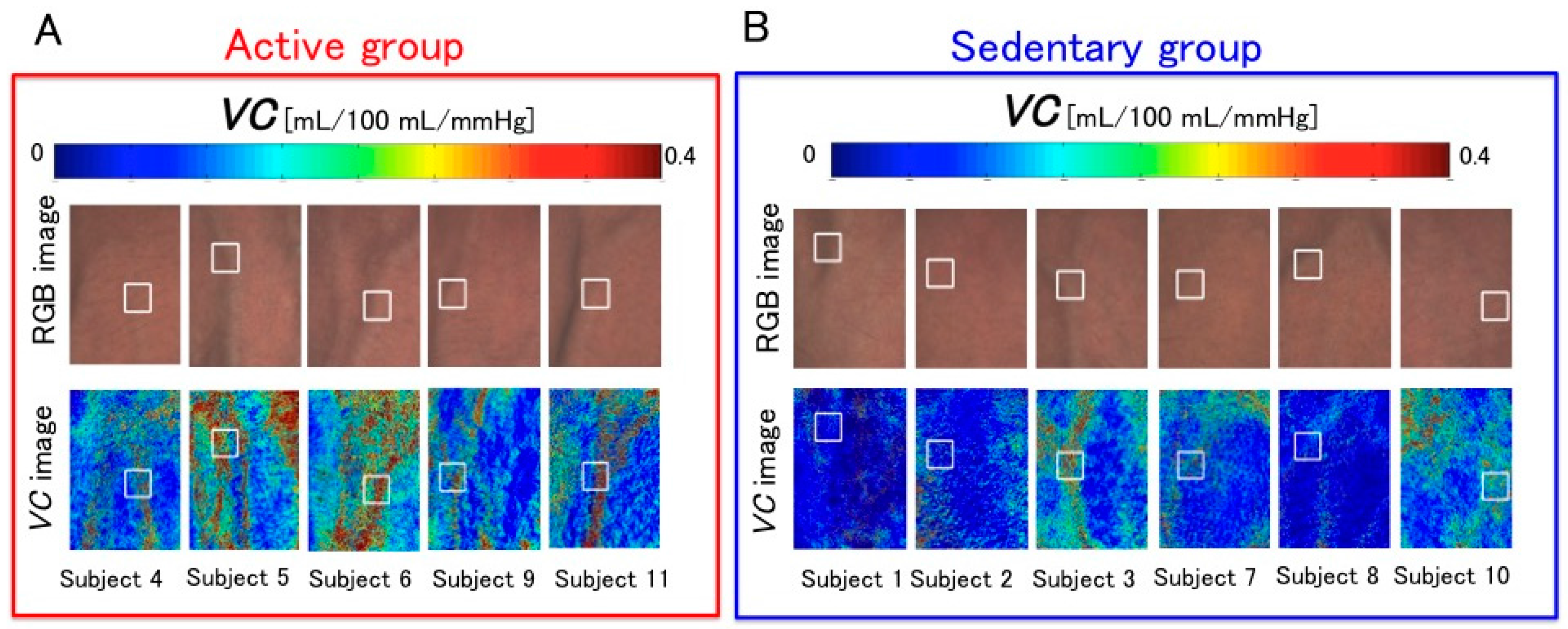
3.1. Images of Venous Compliances
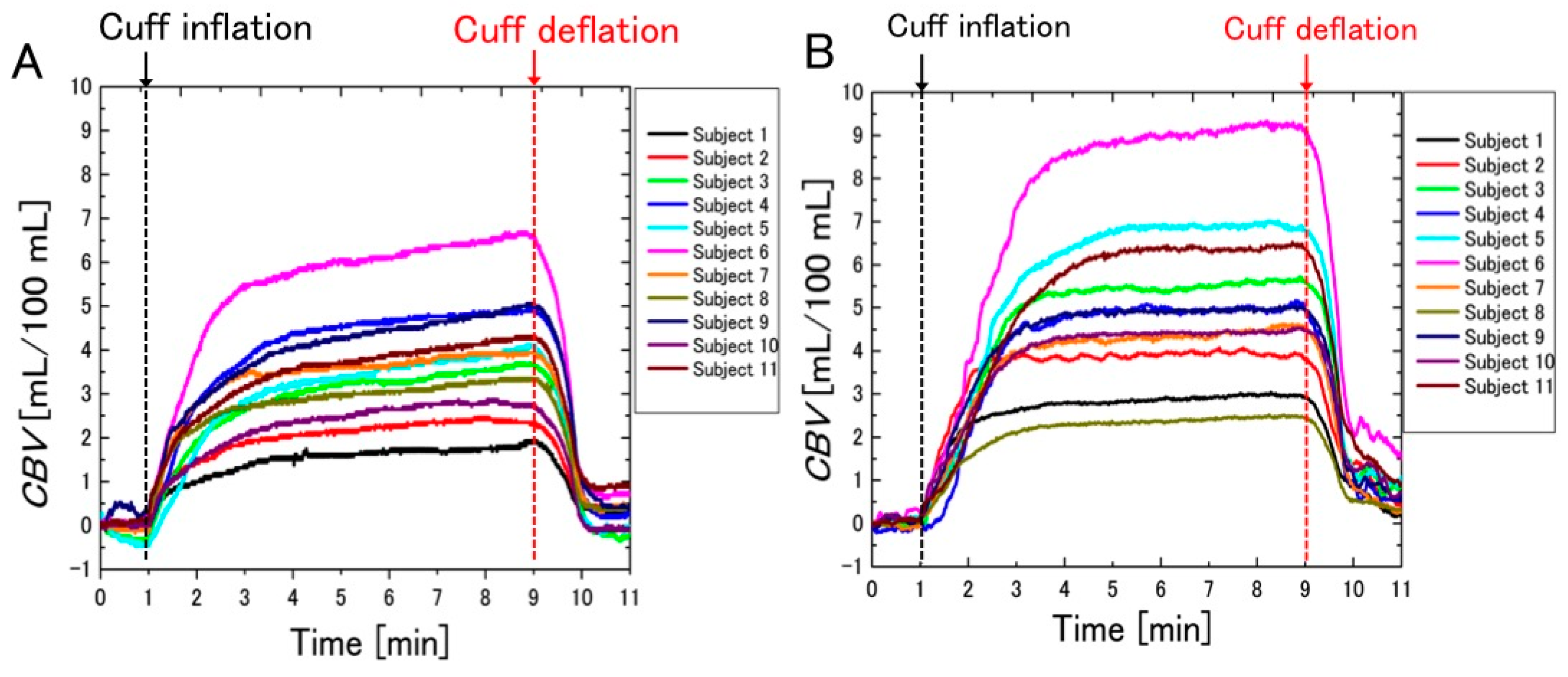
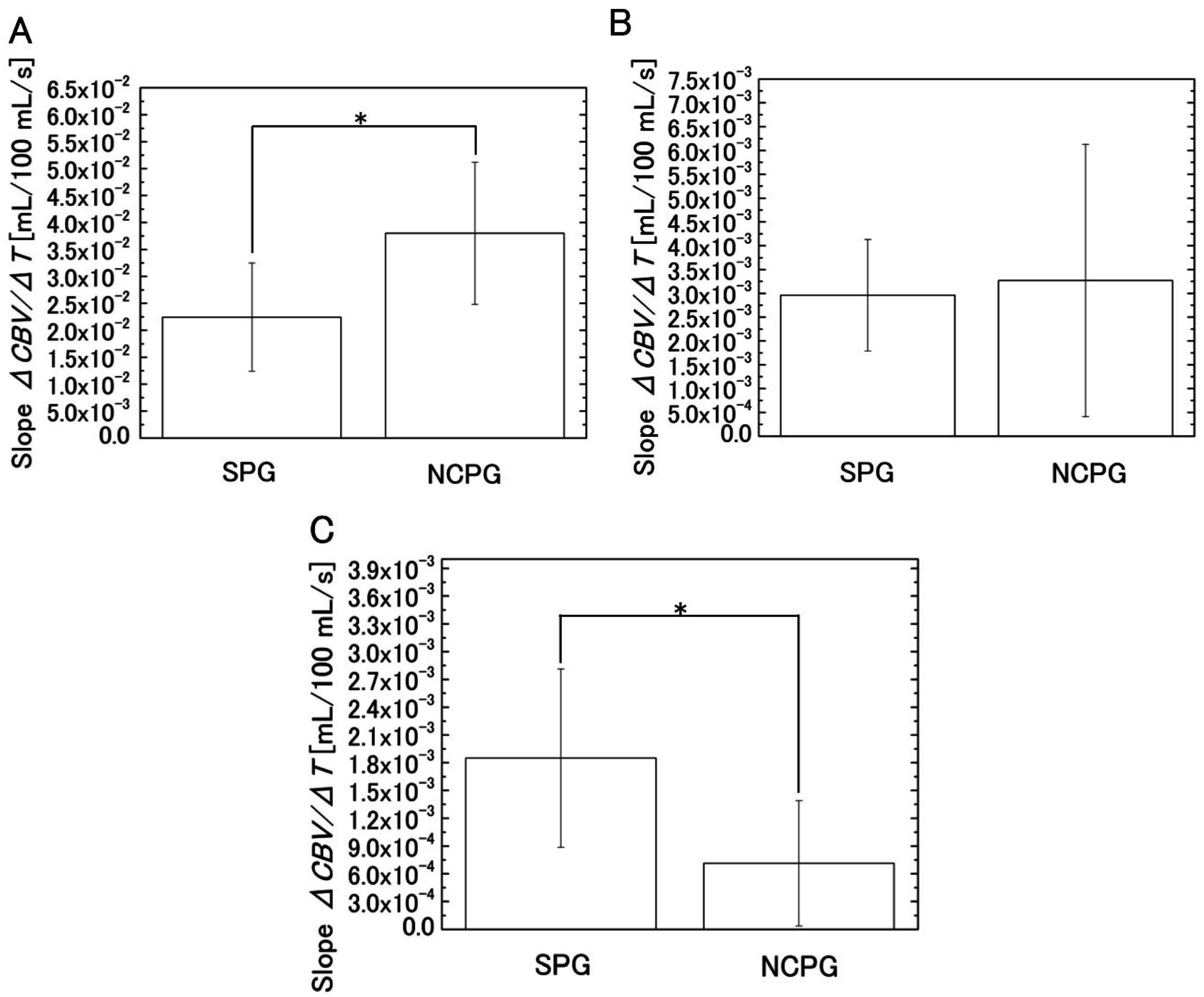
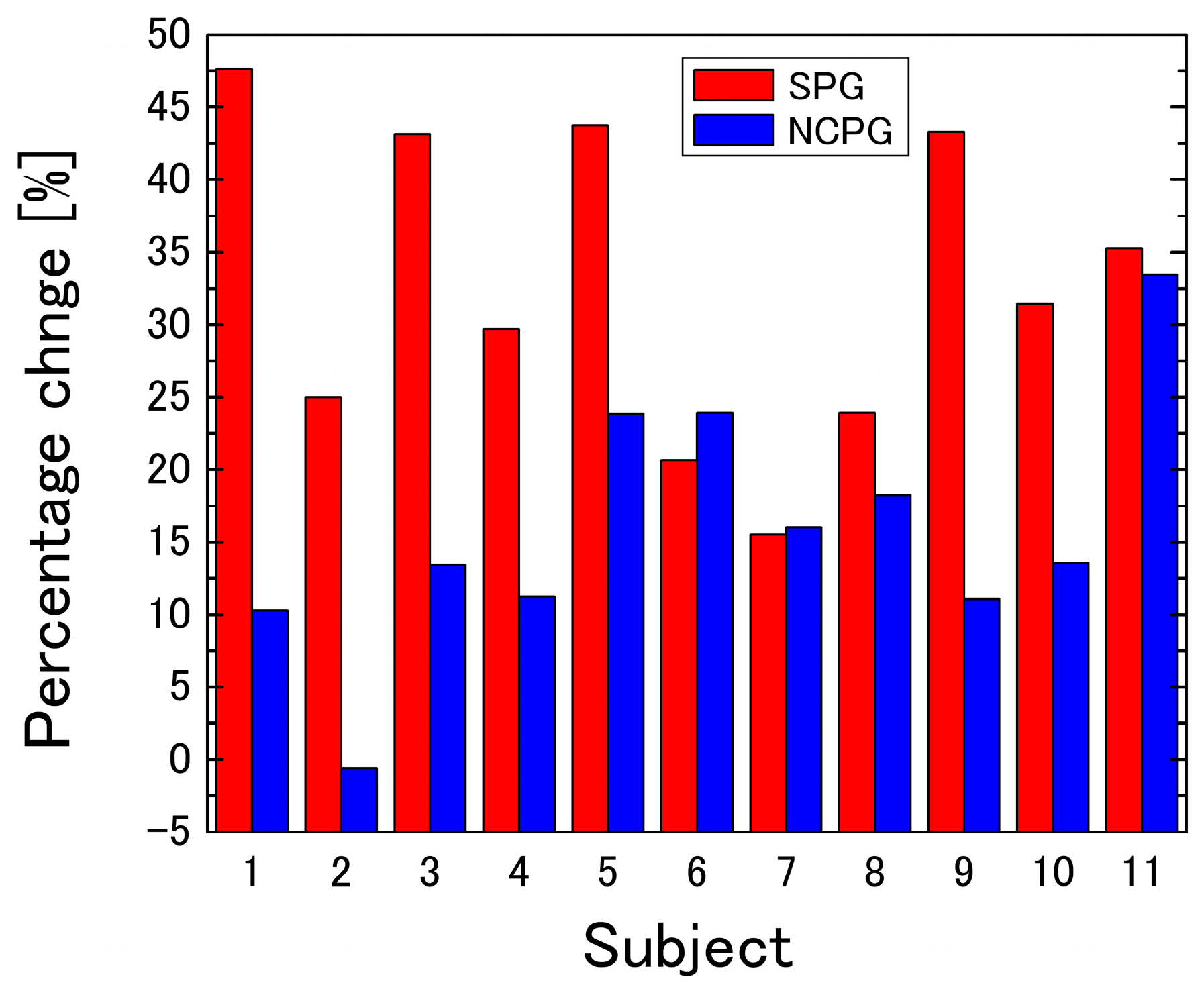
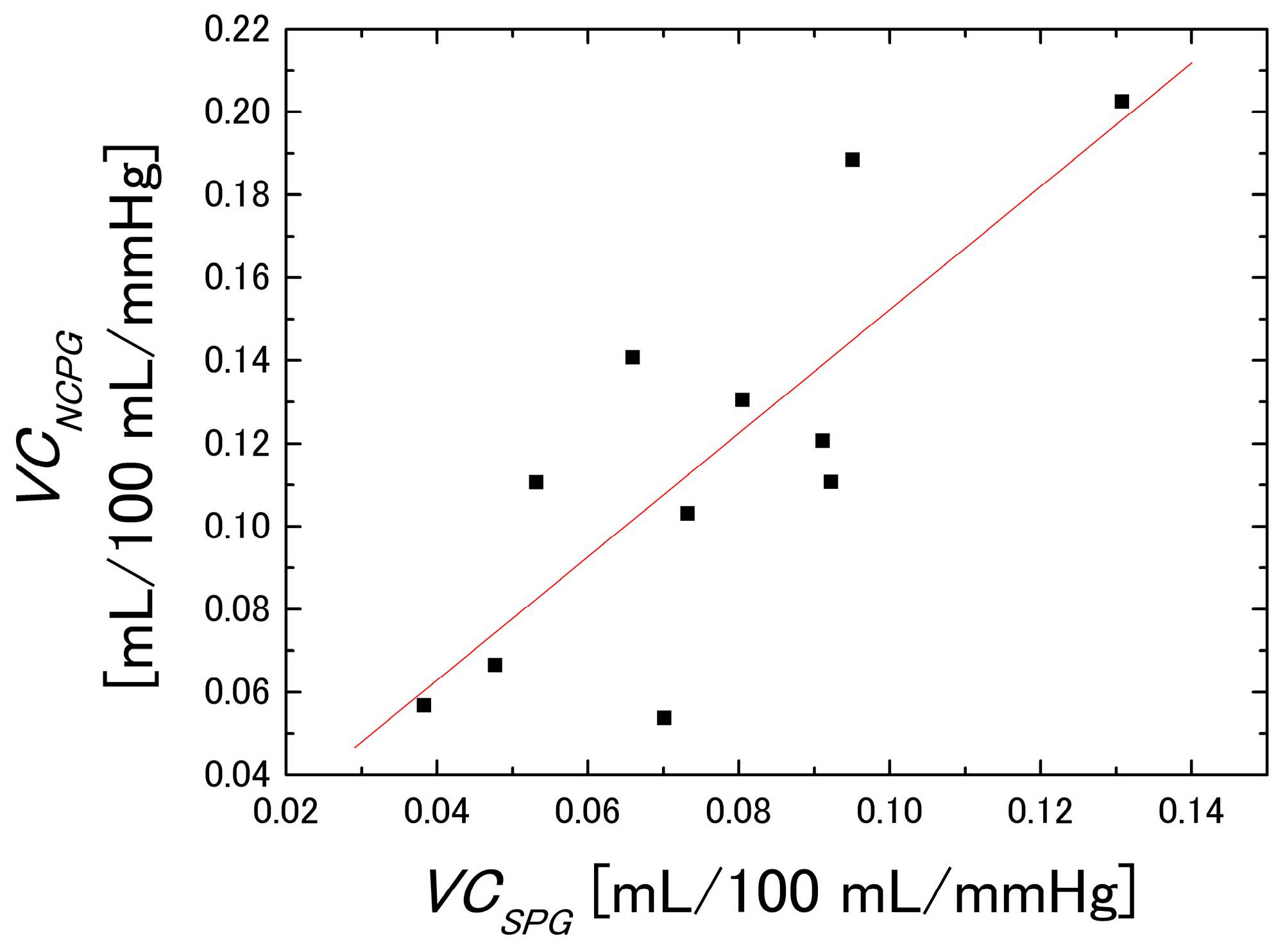
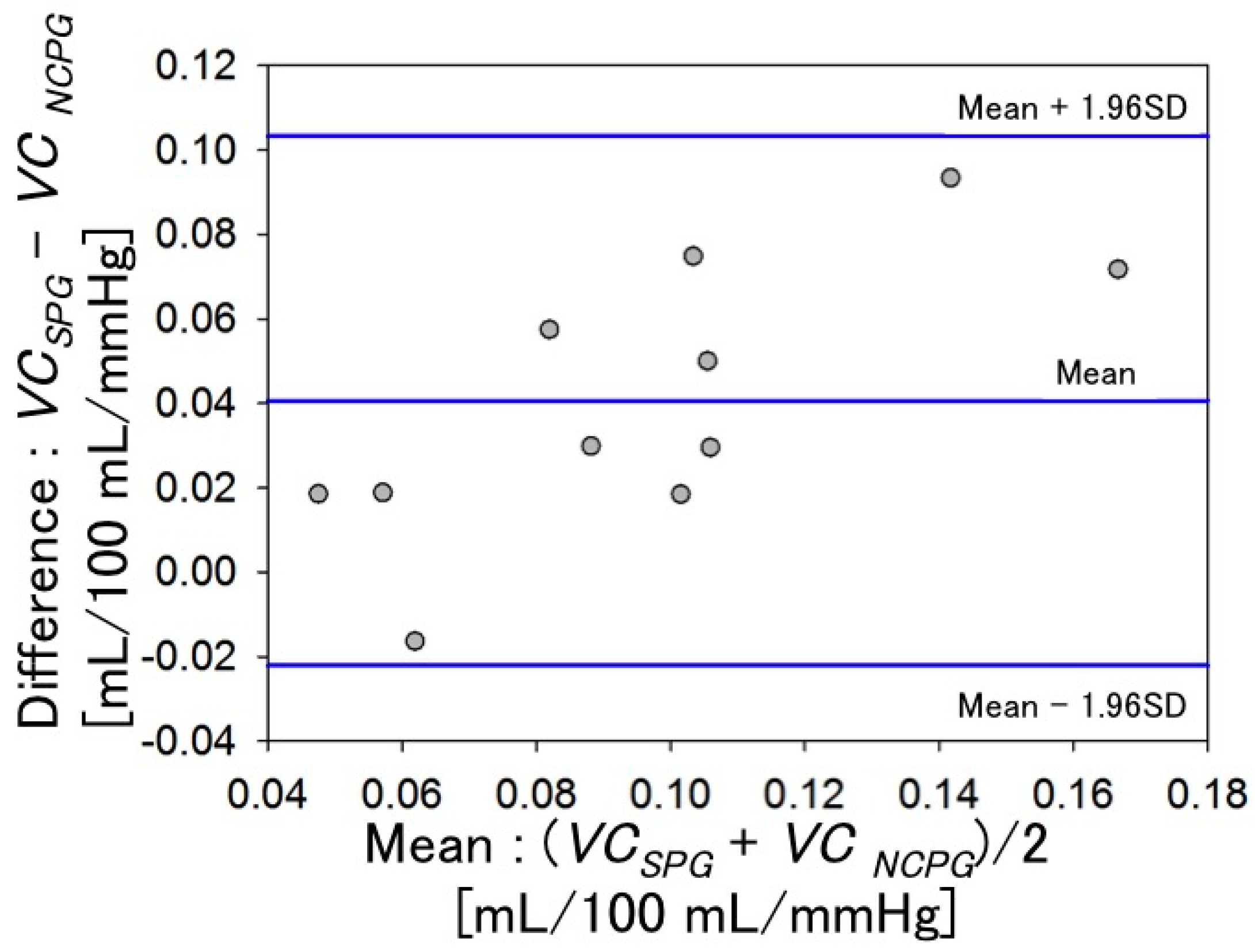
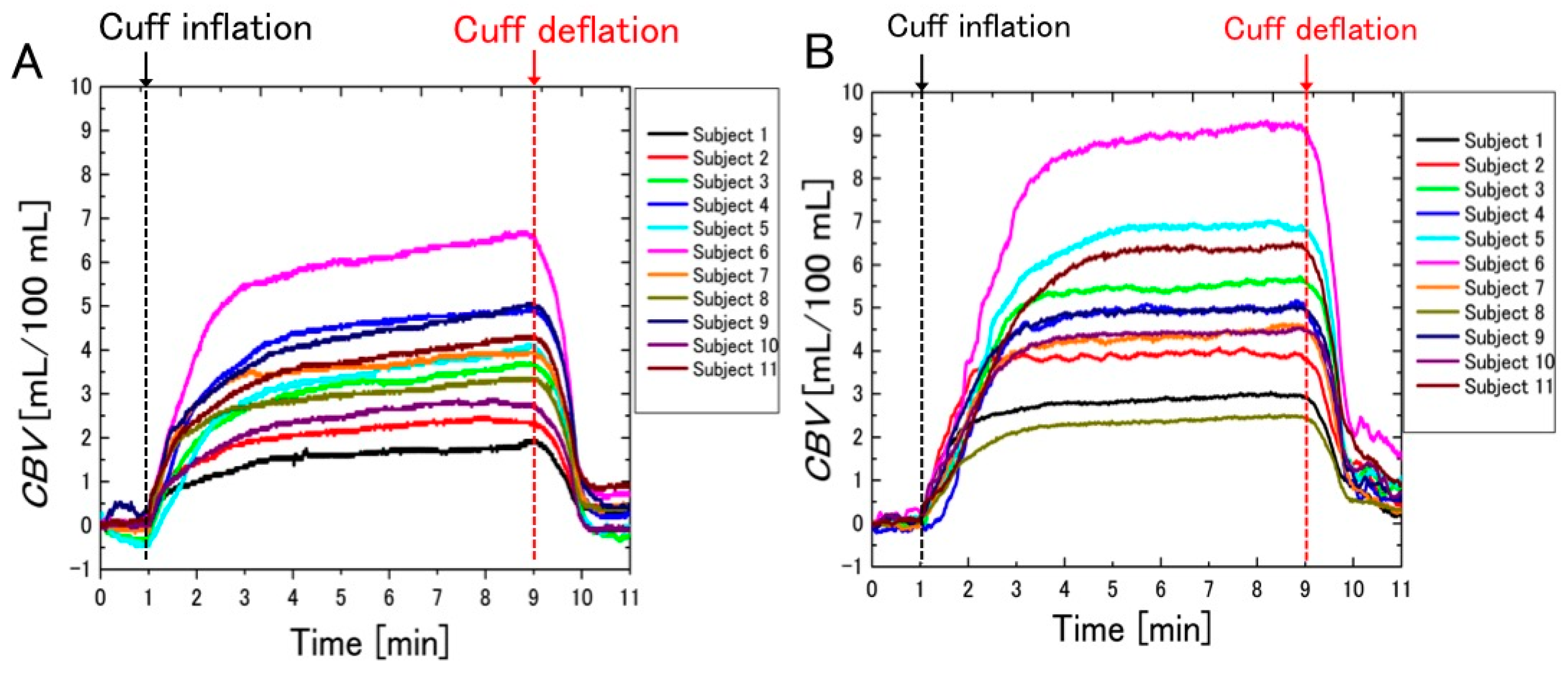
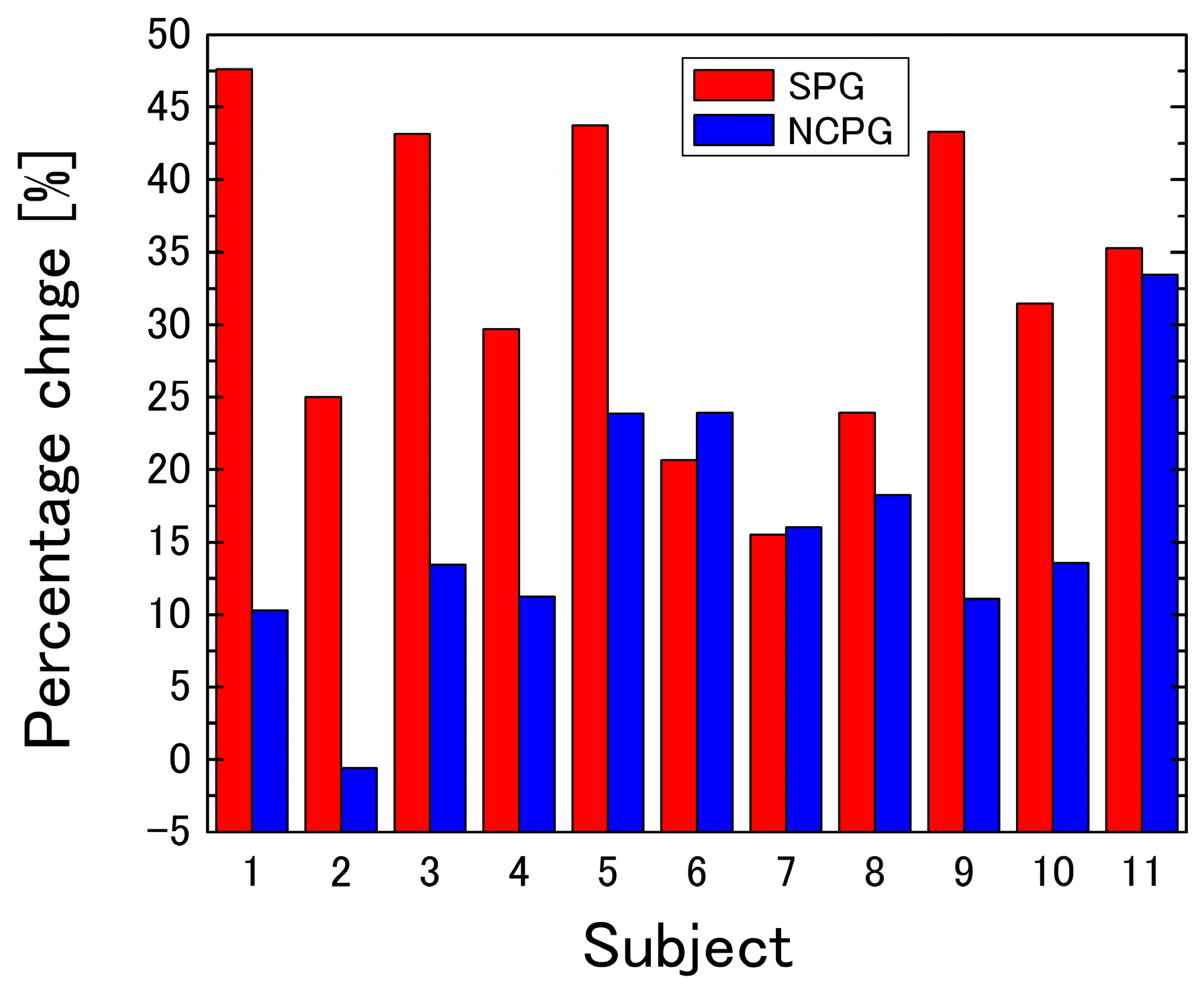
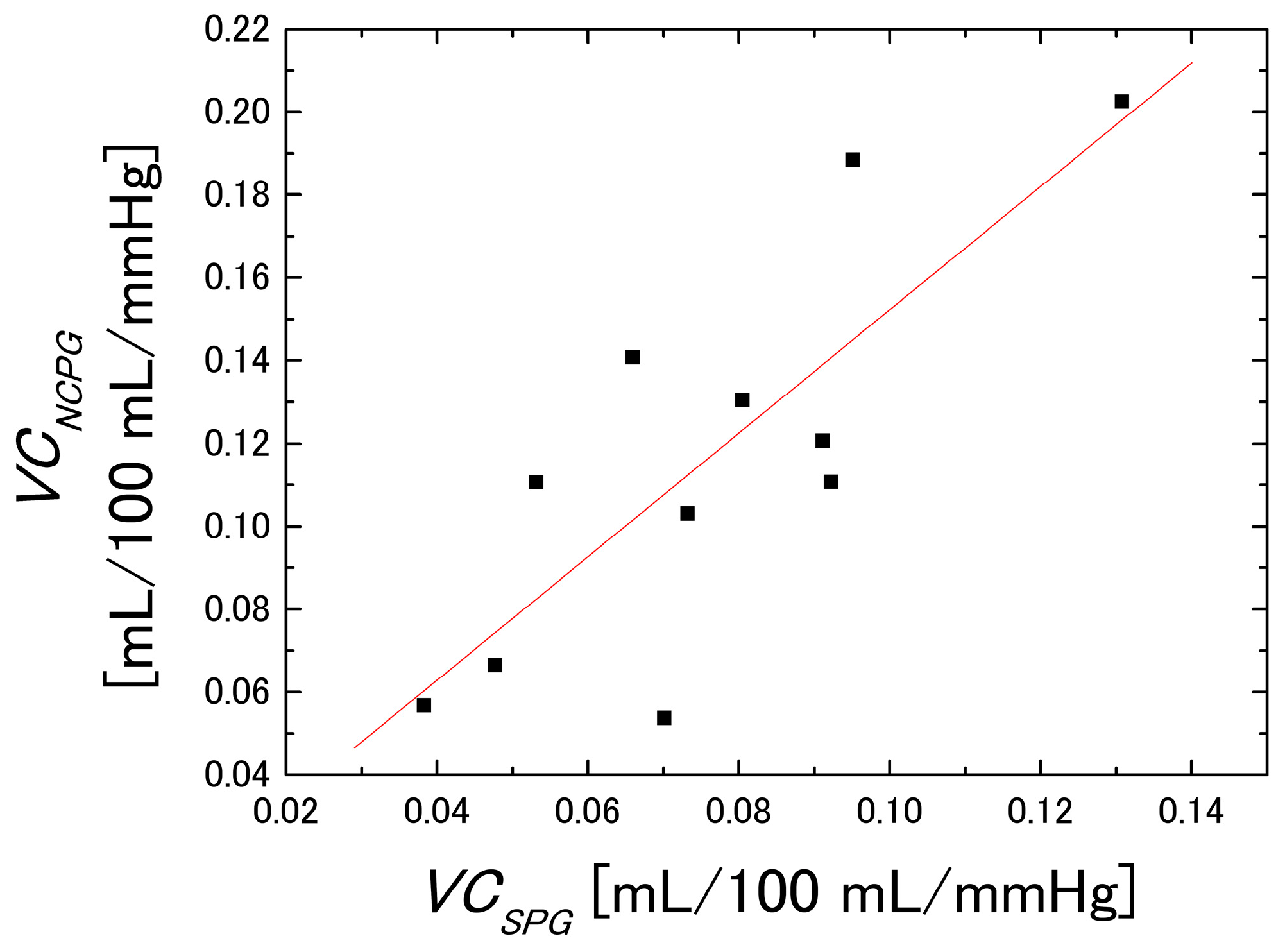
3.2. Difference between the Measurement Results of the Two Systems
3.3. Relationship between Physical Activity and VC
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| VC | Venous compliance |
| SPG | Strain gauge plethysmography |
| NCPG | Non-contact plethysmography |
| RGB | Red-green-blue |
| CBV | Change in blood volume |
| CCD | Charge-coupled device |
| CIEXYZ | Commission Internationale de l’Éclairage XYZ |
| MRA | Multiple regression analysis |
| MCS | Monte Carlo simulation |
| ROI | Region of interest |
References
- Wieringa, F.P.; Mastik, F.; van der Steen, A.F. Contactless multiple wavelength photoplethysmographic imaging: A first step toward “SpO2 camera” technology. Ann. Biomed. Eng. 2005, 33, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- McCombie, D.B.; Shaltis, P.A.; Reisner, A.T.; Asada, H.H. Adaptive hydrostatic blood pressure calibration: Development of a wearable, autonomous pulse wave velocity blood pressure monitor. In Proceedings of the 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 23–26 August 2007; pp. 370–373.
- Humphreys, K.; Ward, T.; Markham, C. Noncontact simultaneous dual wavelength photoplethysmography: A further step toward noncontact pulse oximetry. Rev. Sci. Instrum. 2007, 78, 044304. [Google Scholar] [CrossRef] [PubMed]
- Takano, C.; Ohta, Y. Heart rate measurement based on a time-lapse image. Med. Eng. Phys. 2007, 29, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Verkruysse, W.; Svaasand, L.O.; Nelson, J.S. Remote plethysmographic imaging using ambient light. Opt. Express 2008, 16, 21434–21445. [Google Scholar] [CrossRef] [PubMed]
- Lopez, G.; Shuzo, M.; Ushida, H.; Hidaka, K. Continuous blood pressure monitoring in daily life. JAMDSM 2010, 3, 179–186. [Google Scholar] [CrossRef]
- Poh, M.Z.; McDuff, D.J.; Picard, R.W. Non-contact, automated cardiac pulse measurements using video imaging and blind source separation. Opt. Express 2010, 18, 10762–10774. [Google Scholar] [CrossRef] [PubMed]
- Monahan, K.D.; Dikenno, F.A.; Seals, D.R.; Halliwill, J.R. Smaller age-associated reductions in leg venous compliance in endurance exercise-trained men. Am. J. Physiol. Heart Circ. Physiol. 2001, 281, 1267–1273. [Google Scholar]
- Hernandez, J.P.; Franke, W.D. Age- and fitness-related differences in limbs venous compliance do not affect tolerance to maximal lower body negative pressure in men and women. J. Appl. Physiol. 2004, 97, 925–929. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, J.P.; Franke, W.D. Effect of a 6-mo endurance training program on venous compliance and maximal lower body negative pressure in older men and women. J. Appl. Physiol. 2005, 99, 1070–1077. [Google Scholar] [CrossRef] [PubMed]
- Kawano, H.; Tanimoto, M.; Yamamoto, K.; Gando, Y.; Sanada, K.; Tabata, I.; Higuchi, M.; Miyachi, M. Greater forearm venous compliance in resistance-trained men. Eur. J. Appl. Physiol. 2010, 110, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Avolio, A.P.; Chen, S.G.; Wang, R.P.; Zhang, C.L.; Li, M.F.; O’Rourke, M.F. Effects of aging on changing arterial compliance and left ventricular load in a northern Chinese urban community. Circulation 1983, 68, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Young, C.N.; Stillabower, M.E.; DiSabatino, A.; Farquhar, W.B. Venous smooth muscle tone and responsiveness in older adults. J. Appl. Physiol. 2006, 101, 1362–1367. [Google Scholar] [CrossRef] [PubMed]
- Monahan, K.D.; Ray, C.A. Gender affects calf venous compliance at rest and during baroreceptor unloading in humans. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Hokanson, D.E.; Sumner, D.S.; Strandness, D.E. An electrically calibrated plethysmograph for direct measurement of limb blood flow. IEEE Trans. Biomed. Eng. 1975, 22, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, T.; Hokanson, D.; Barnes, R. Automatic quantitation of venous hemodynamics with an electrically calibrated strain gauge plethysmograph. Med. Instrum. 1977, 11, 240–243. [Google Scholar] [PubMed]
- Nakano, K.; Satoh, R.; Hoshi, A.; Matsuda, R.; Suzuki, H.; Nishidate, I. Non-contact imaging of venous compliance in humans using an RGB camera. Opt. Rev. 2015, 22, 335–341. [Google Scholar] [CrossRef]
- Nishidate, I.; Sasaoka, K.; Yuasa, T.; Niizeki, K.; Maeda, T.; Aizu, Y. Visualizing of skin chromophore concentrations by use of RGB images. Opt. Lett. 2008, 33, 2263–2265. [Google Scholar] [CrossRef] [PubMed]
- Nishidate, I.; Tanaka, N.; Kawase, T.; Maeda, T.; Yuasa, T.; Aizu, Y.; Yuasa, T.; Niizeki, K. Noninvasive imaging of human skin hemodynamics using a digital red-green-blue camera. J. Biomed. Opt. 2011, 16, 086012. [Google Scholar] [CrossRef] [PubMed]
- Nishidate, I.; Tanaka, N.; Kawase, T.; Maeda, T.; Yuasa, T.; Aizu, Y.; Yuasa, T.; Niizeki, K. Visualization of peripheral vasodilative indices in human skin by use of red, green, blue images. J. Biomed. Opt. 2013, 18, 061220. [Google Scholar] [CrossRef] [PubMed]
- Halliwill, J.R.; Minton, C.T.; Joyner, M.J. Measurement of limb venous compliance in humans: Technical considerations and physiological findings. J. Appl. Physiol. 1999, 87, 1555–1563. [Google Scholar] [PubMed]
- Hall, J.E. Guyton and Hall Textbook of Medical Physiology, 11th ed.; Elsevier Japan: Tokyo, Japan, 2010; pp. 189–198. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
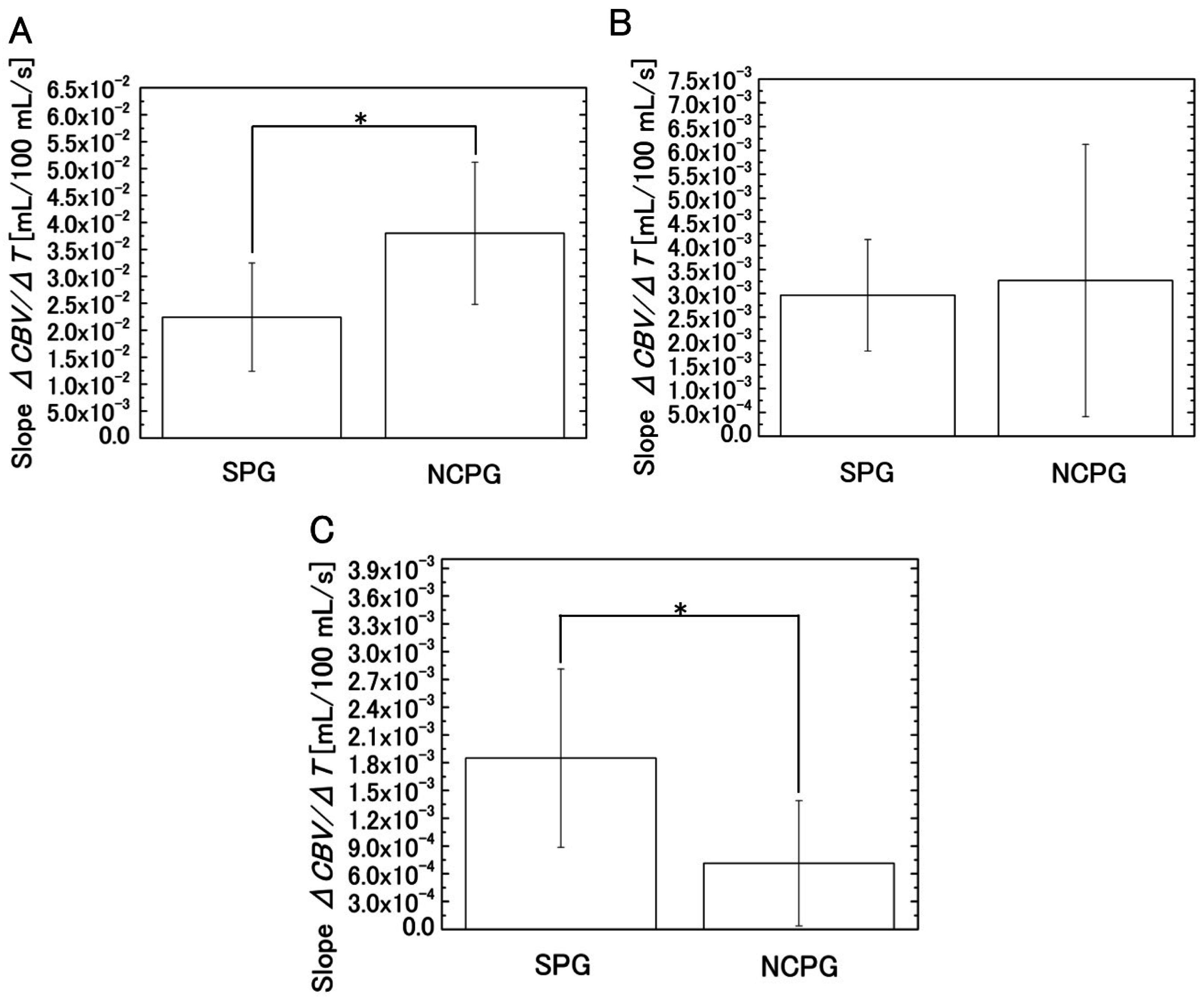
| Segment | System | Mean of Slope | SD of Slope | t-Value | p-Value |
|---|---|---|---|---|---|
| Segment 1 | SPG | 2.24 × 10−2 | 1.01 × 10−2 | −3.11 | 5.47 × 10−3 |
| NCPG | 3.80 × 10−2 | 1.32 × 10−2 | |||
| Segment 3 | SPG | 1.85 × 10−3 | 9.63 × 10−4 | 3.21 | 4.38 × 10−3 |
| NCPG | 7.14 × 10−4 | 6.76 × 10−4 |
| System | Mean of Percentage Change | SD of Percentage Change | t-Value | p-Value |
|---|---|---|---|---|
| SPG | 32.7 | 10.8 | 3.98 | 7.38 × 10−4 |
| NCPG | 15.9 | 8.95 |
| Group | Number of Subjects | Mean of VC at 20 mmHg | SD of VC at 20 mmHg | t-Value | p-Value |
|---|---|---|---|---|---|
| Active group | 5 | 0.151 | 0.042 | 2.68 | 0.025 |
| Sedentary group | 6 | 0.089 | 0.035 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakano, K.; Aoki, Y.; Satoh, R.; Suzuki, H.; Nishidate, I. Visualization of Venous Compliance of Superficial Veins Using Non-Contact Plethysmography Based on Digital Red-Green-Blue Images. Sensors 2016, 16, 1996. https://doi.org/10.3390/s16121996
Nakano K, Aoki Y, Satoh R, Suzuki H, Nishidate I. Visualization of Venous Compliance of Superficial Veins Using Non-Contact Plethysmography Based on Digital Red-Green-Blue Images. Sensors. 2016; 16(12):1996. https://doi.org/10.3390/s16121996
Chicago/Turabian StyleNakano, Kazuya, Yuta Aoki, Ryota Satoh, Hiroyuki Suzuki, and Izumi Nishidate. 2016. "Visualization of Venous Compliance of Superficial Veins Using Non-Contact Plethysmography Based on Digital Red-Green-Blue Images" Sensors 16, no. 12: 1996. https://doi.org/10.3390/s16121996
APA StyleNakano, K., Aoki, Y., Satoh, R., Suzuki, H., & Nishidate, I. (2016). Visualization of Venous Compliance of Superficial Veins Using Non-Contact Plethysmography Based on Digital Red-Green-Blue Images. Sensors, 16(12), 1996. https://doi.org/10.3390/s16121996