
Smart Sensing Strip Using Monolithically Integrated Flexible Flow Sensor for Noninvasively Monitoring Respiratory Flow

Abstract
:
1. Introduction
2. System Design
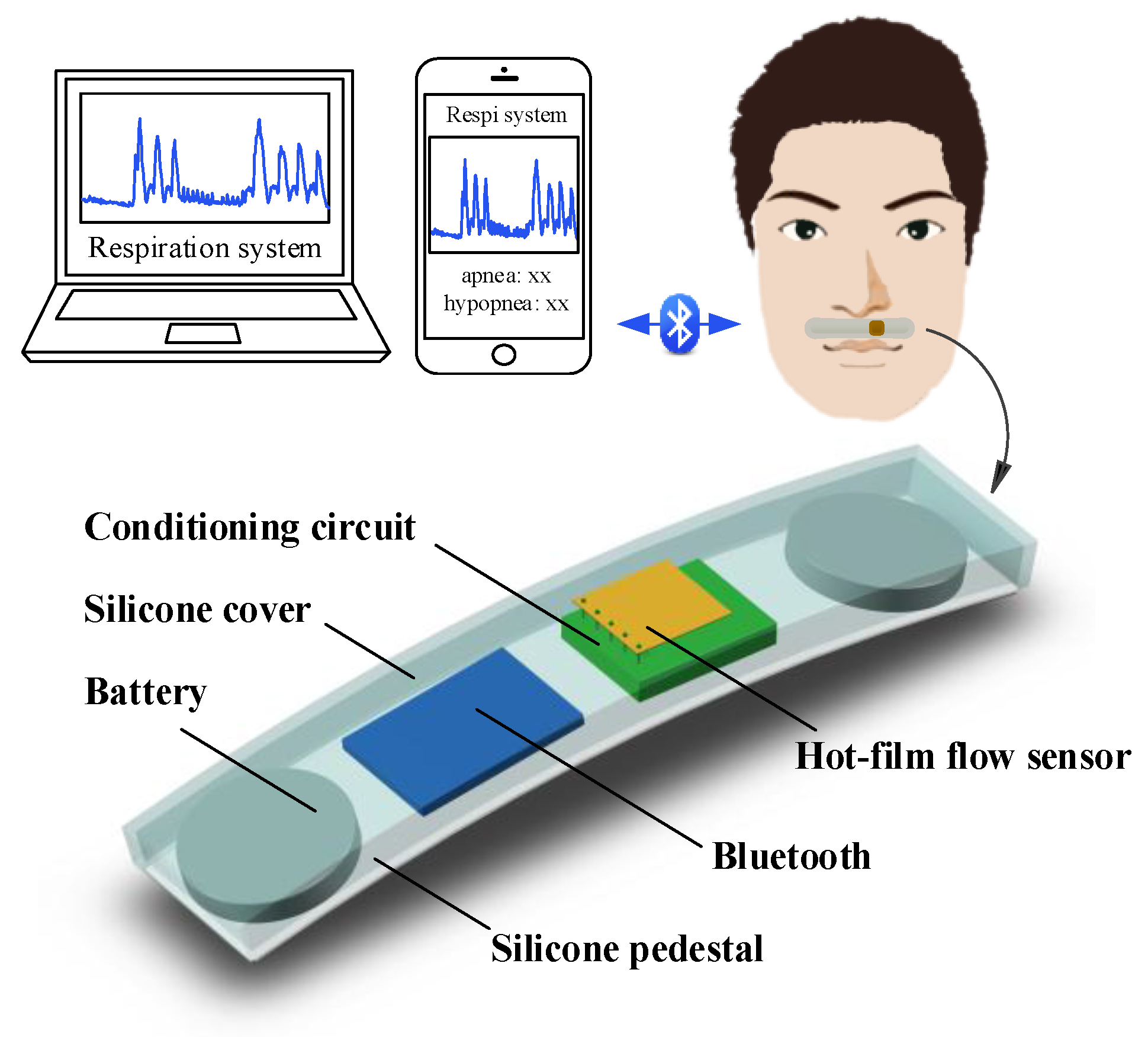
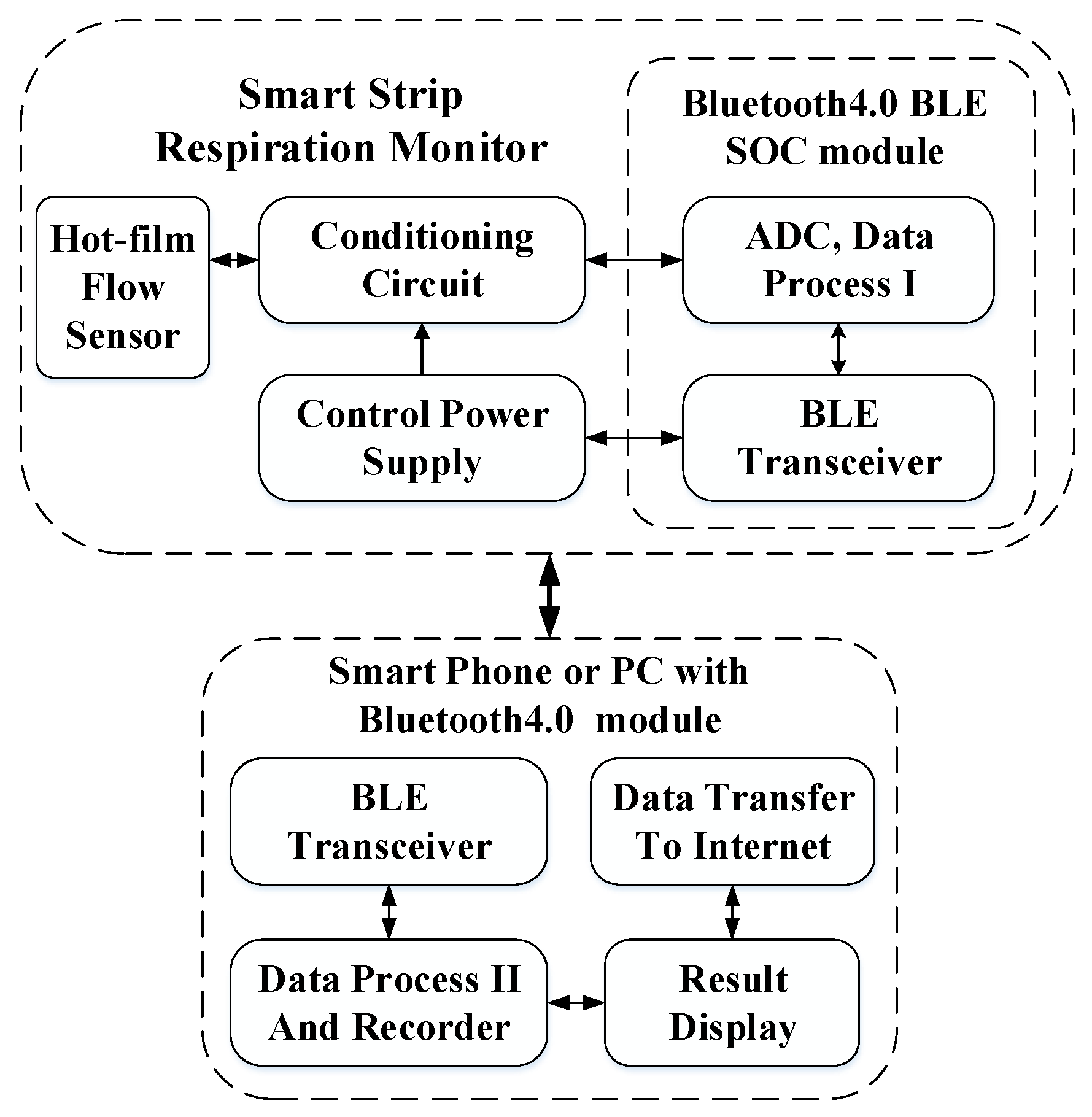
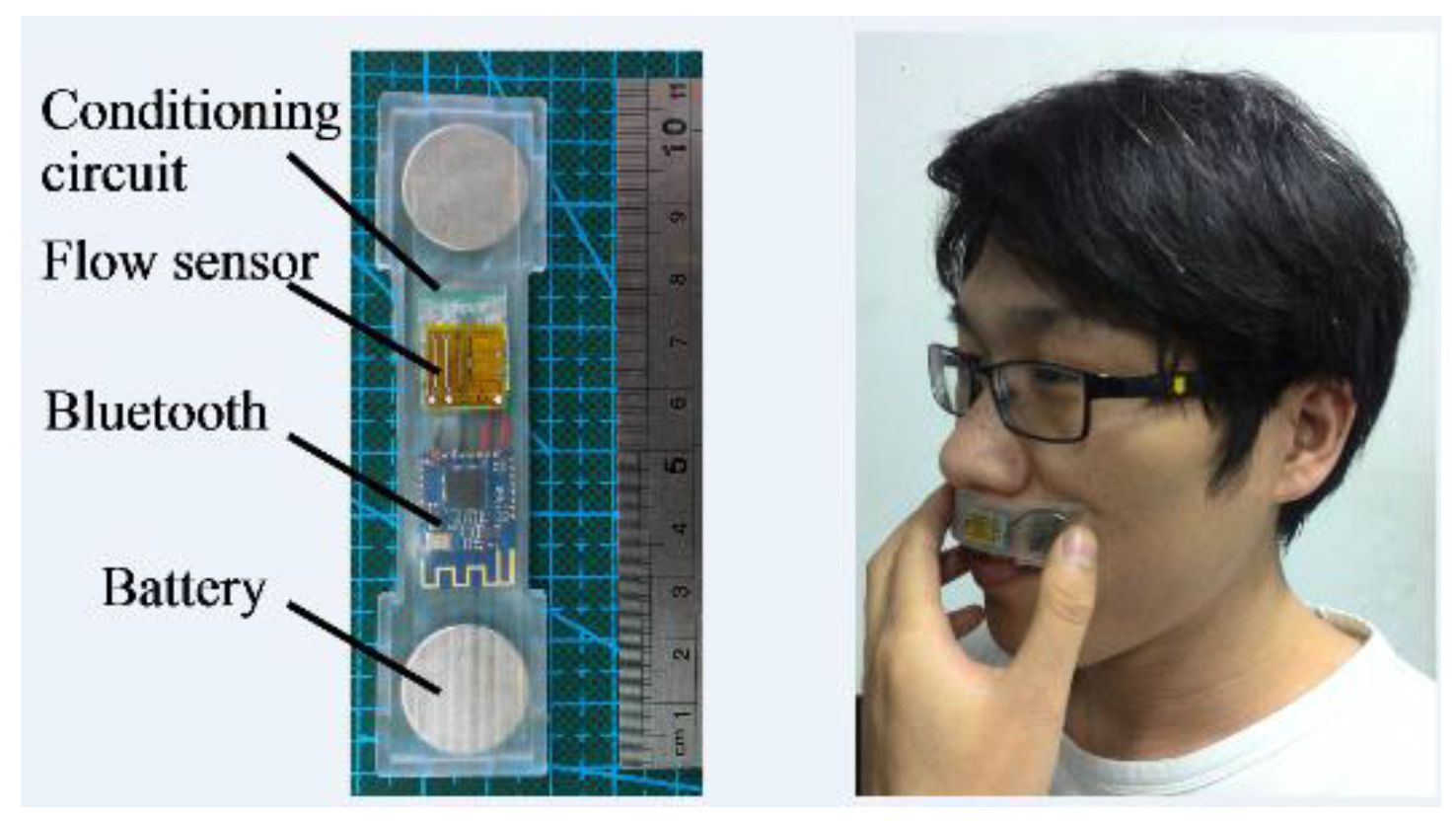
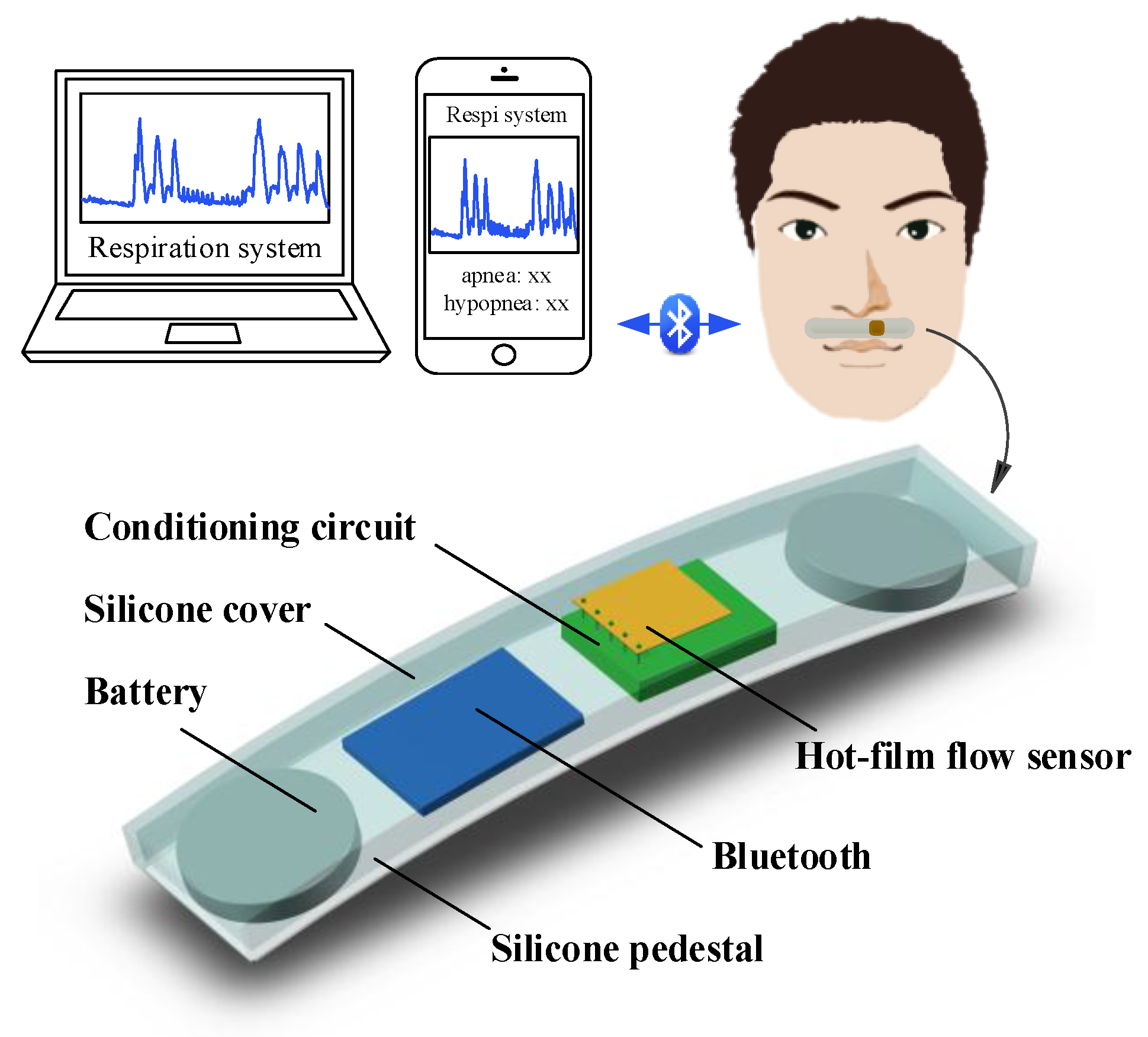
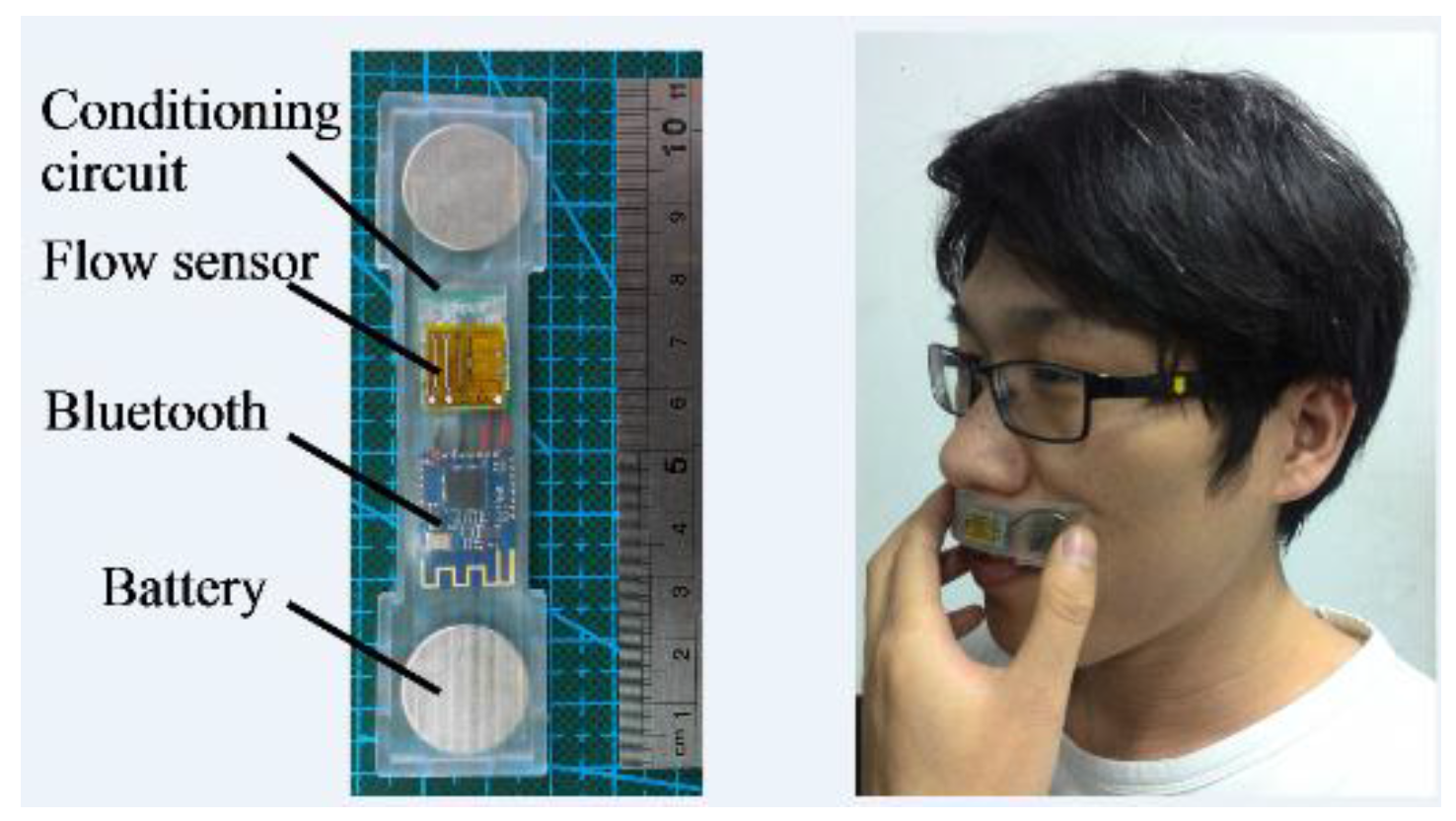
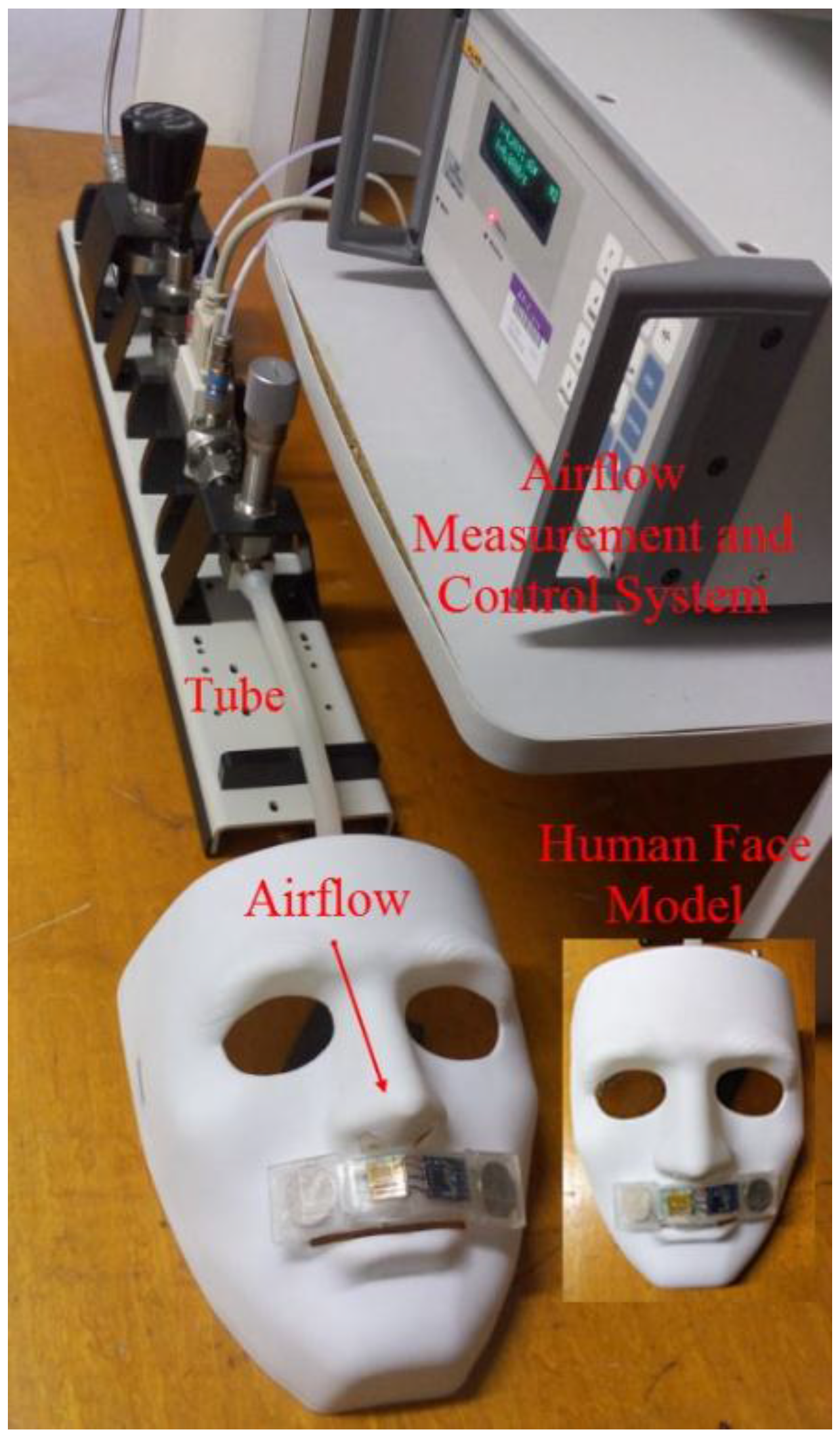
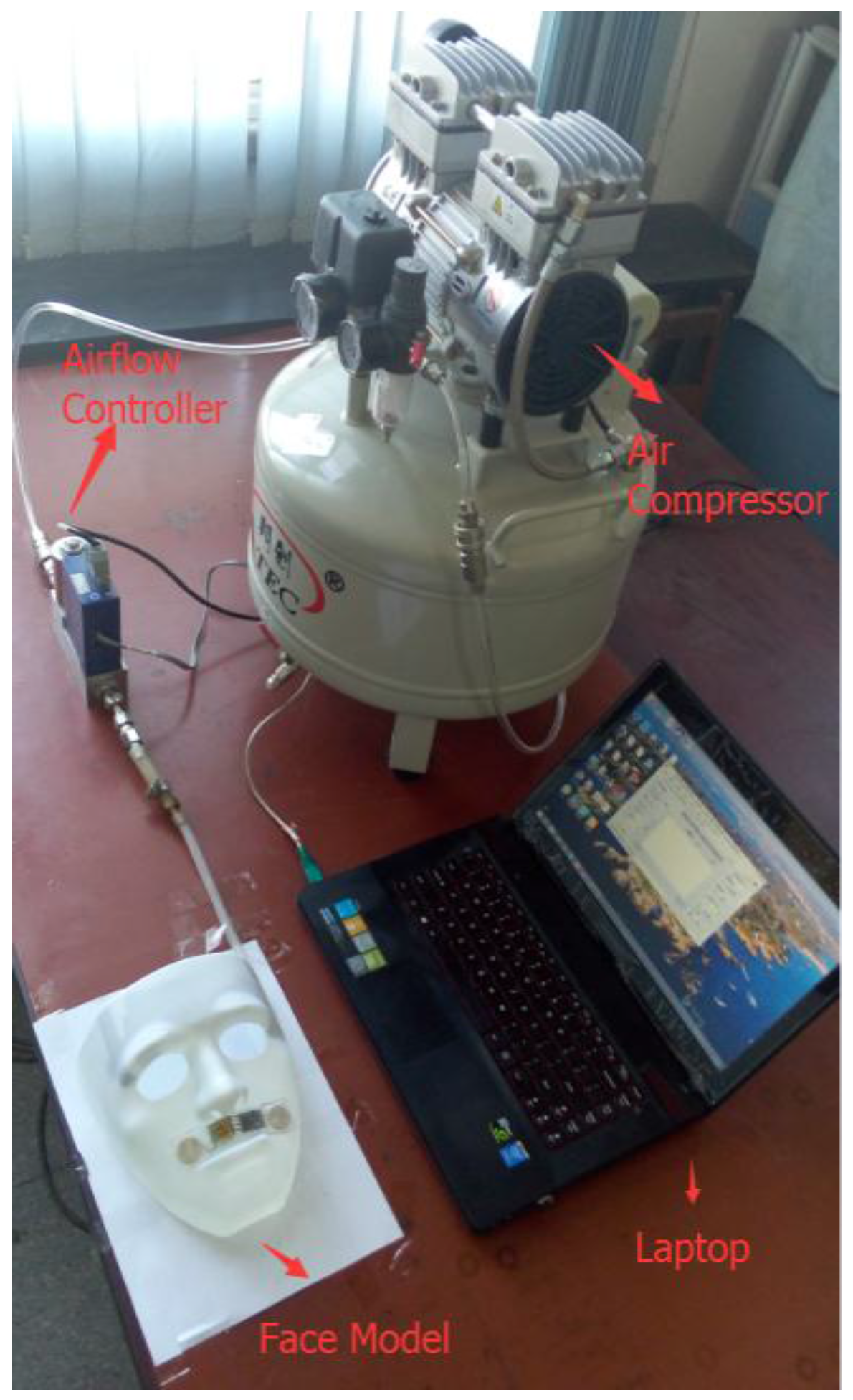
2.1. System Overview
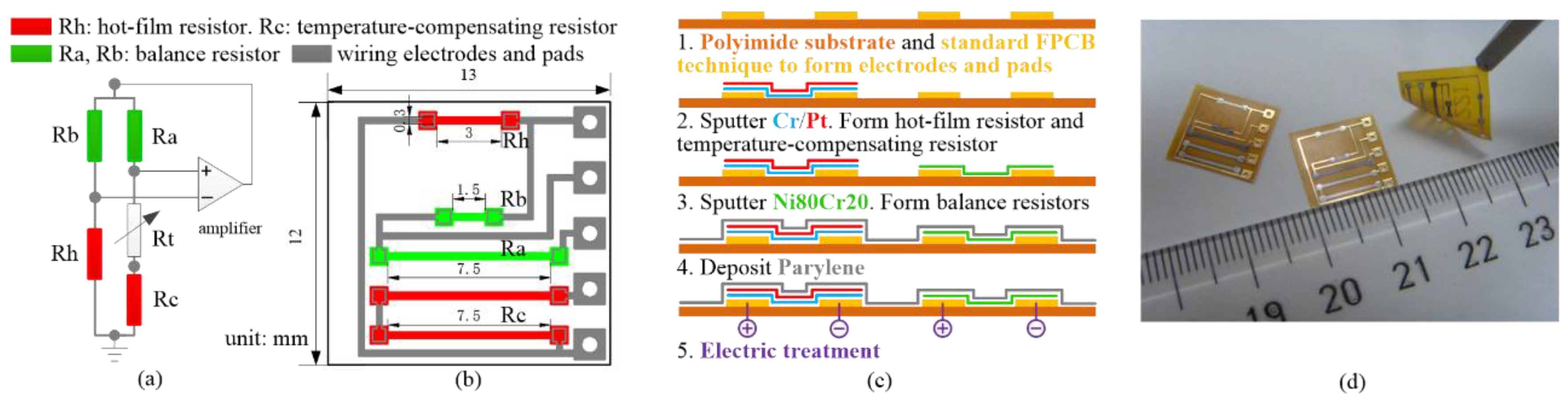
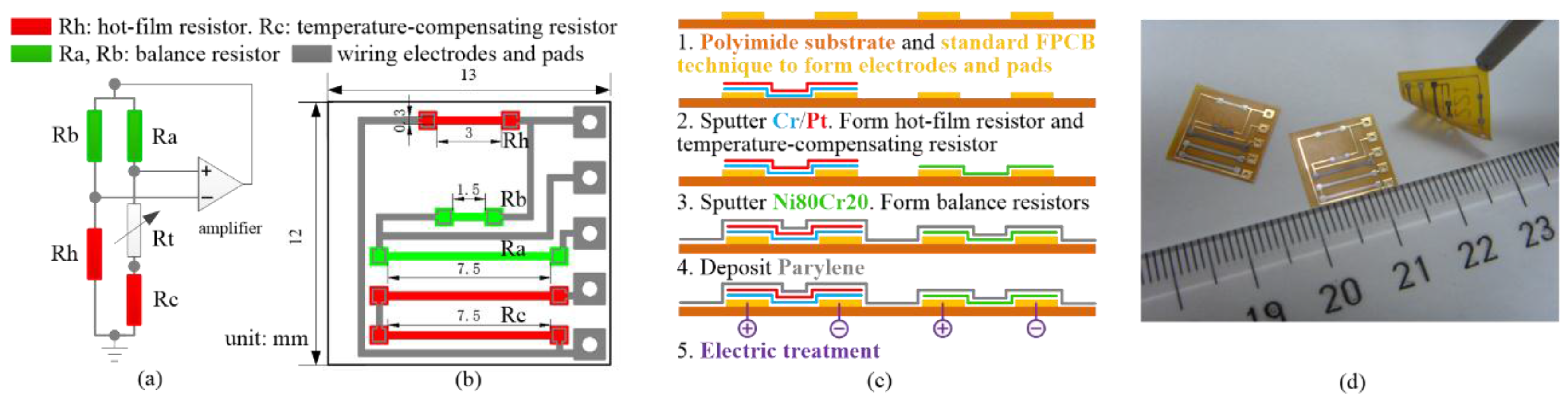
2.2. Design and Fabrication of Monolithically Integrated Flexible Hot-Film Flow Sensor
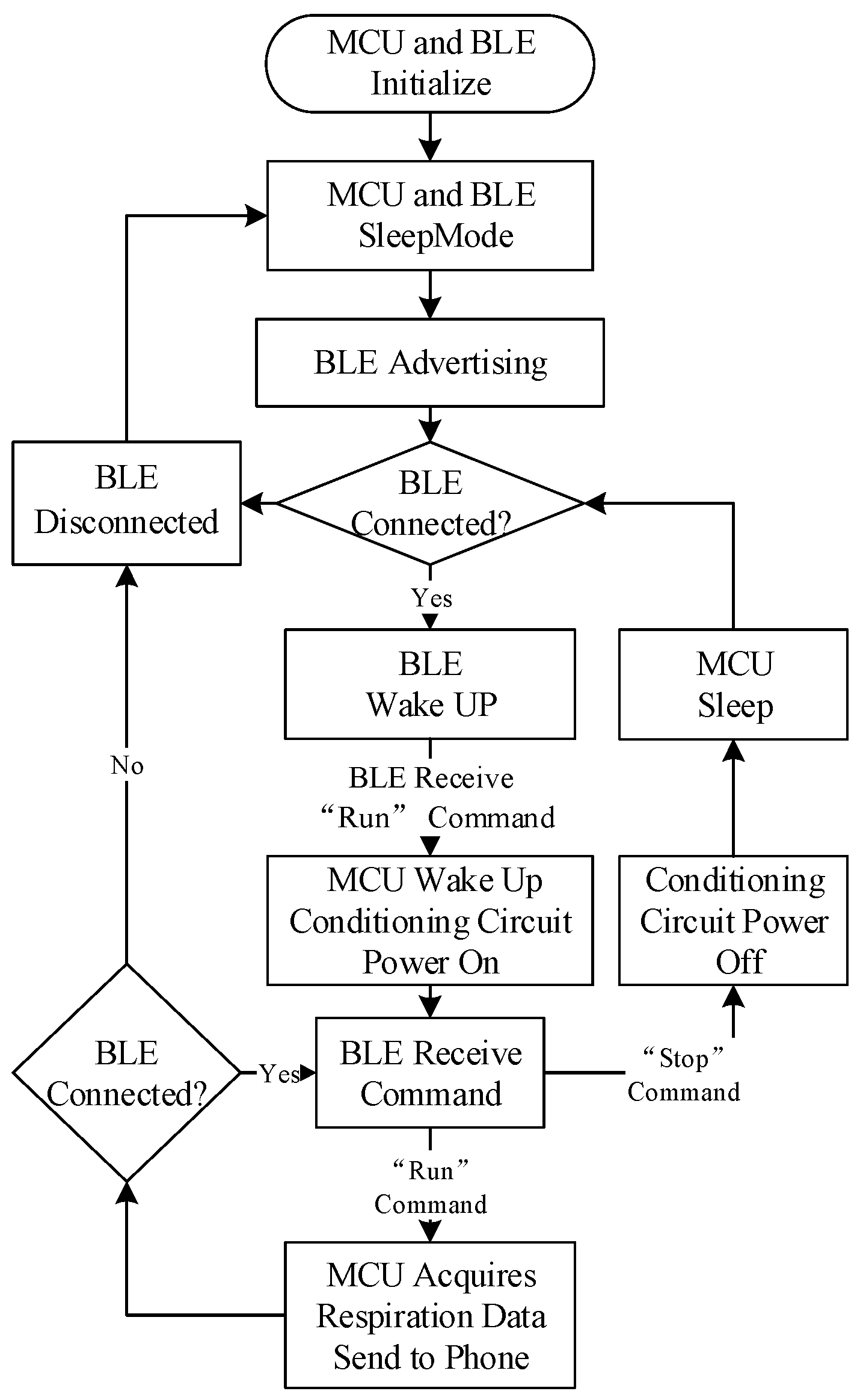
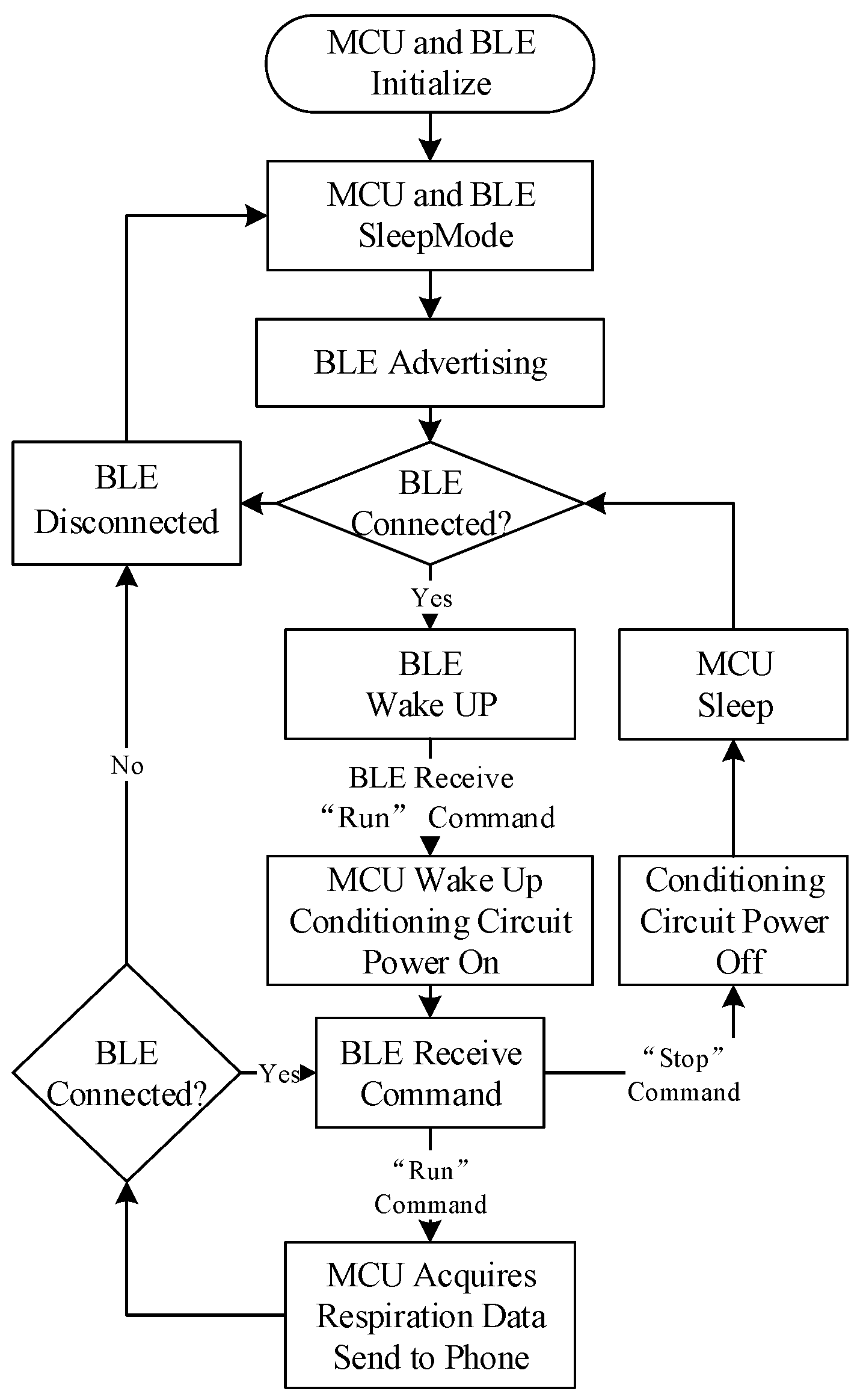
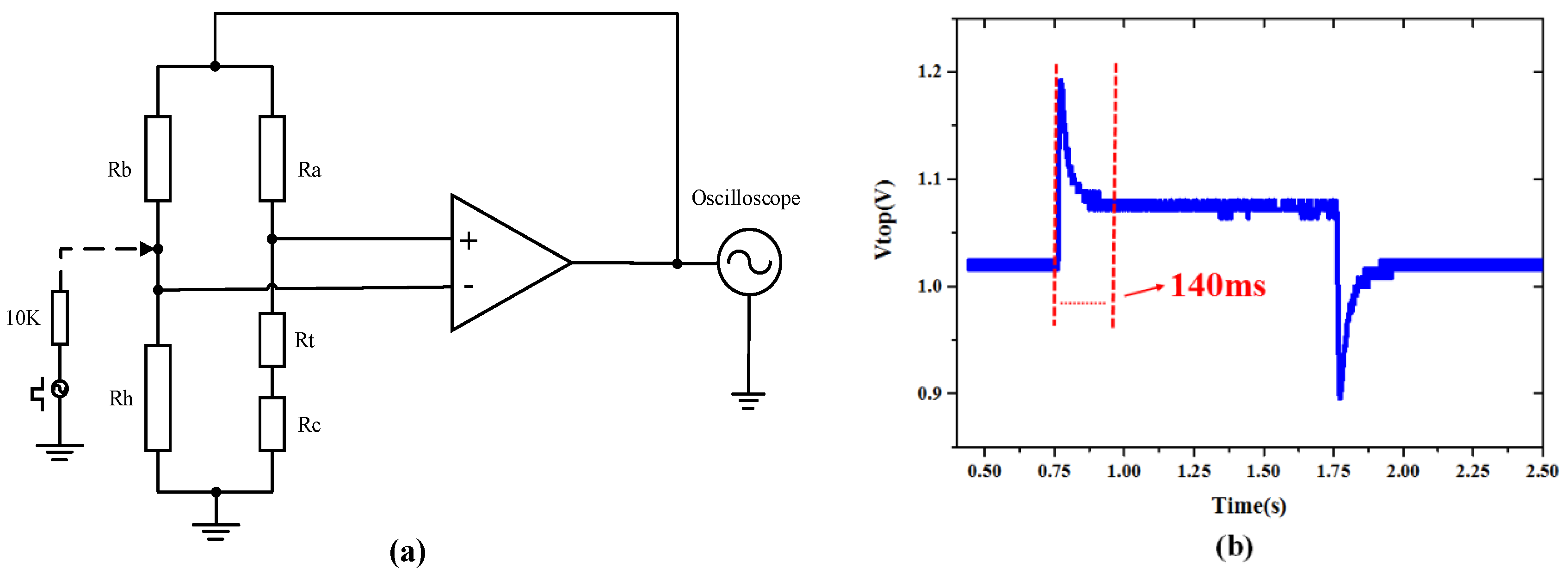
2.3. Low Power Consumption Design
2.4. Algorithm for Extracting Respiratory Parameters

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | MV (L) | TV (L) | PIF (L/min) | RR (min−1) |
|---|---|---|---|---|
| Tested Value | 6.1 | 0.3 | 21 | 20 |
| Normal Value | 6–8 | 0.3–0.8 | N/A | 12–24 |
3. Experimental Results and Discussions
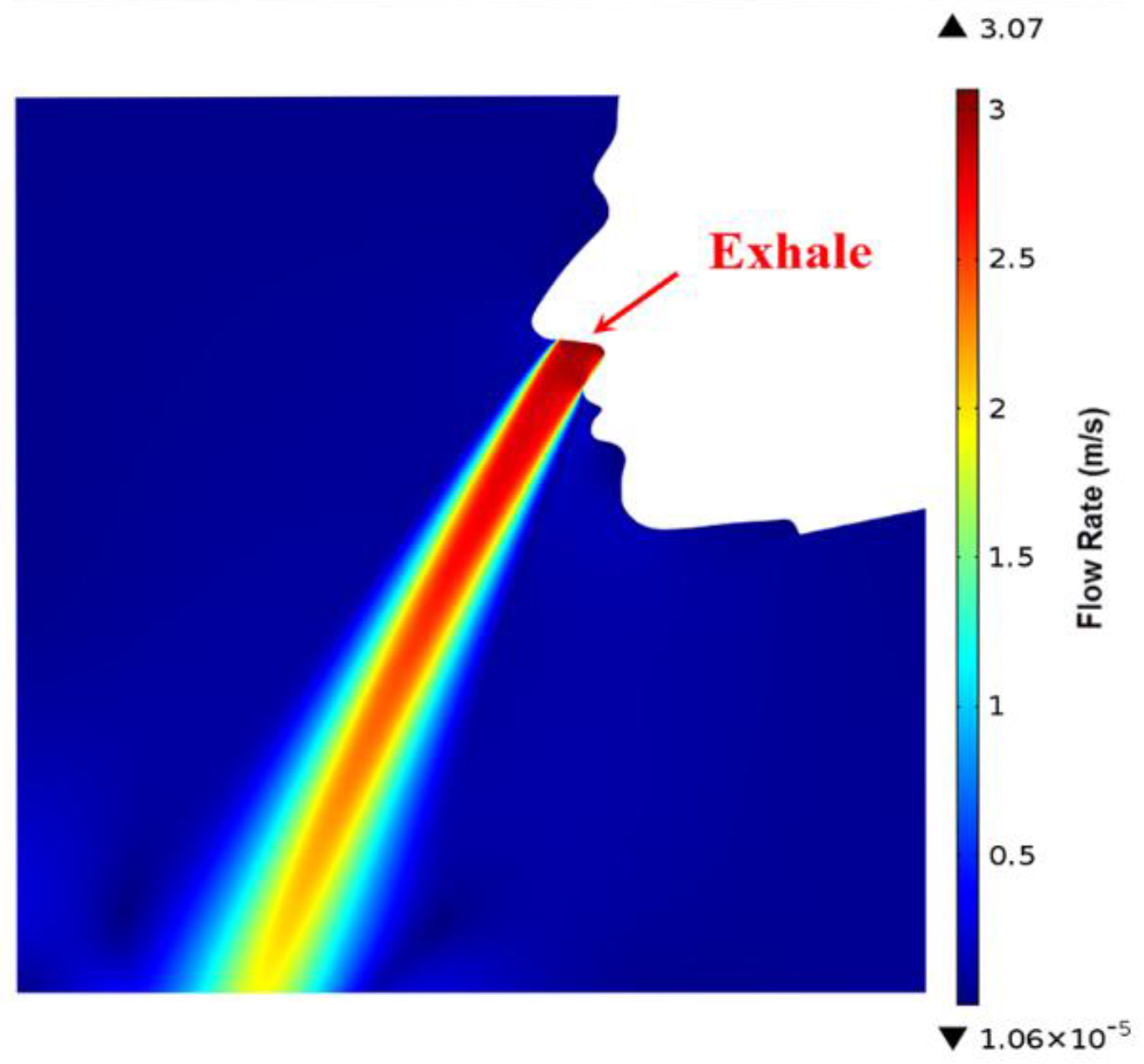
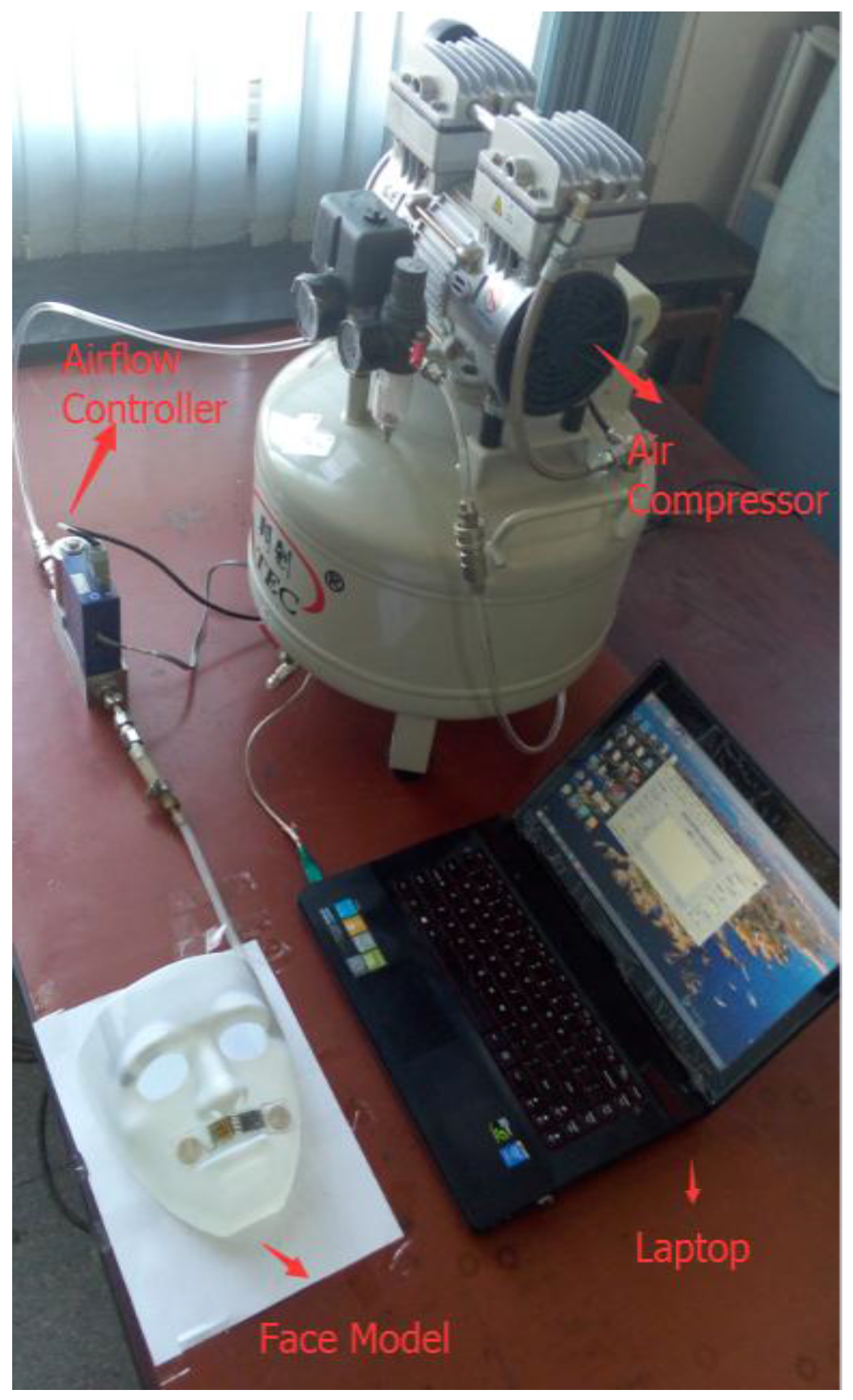
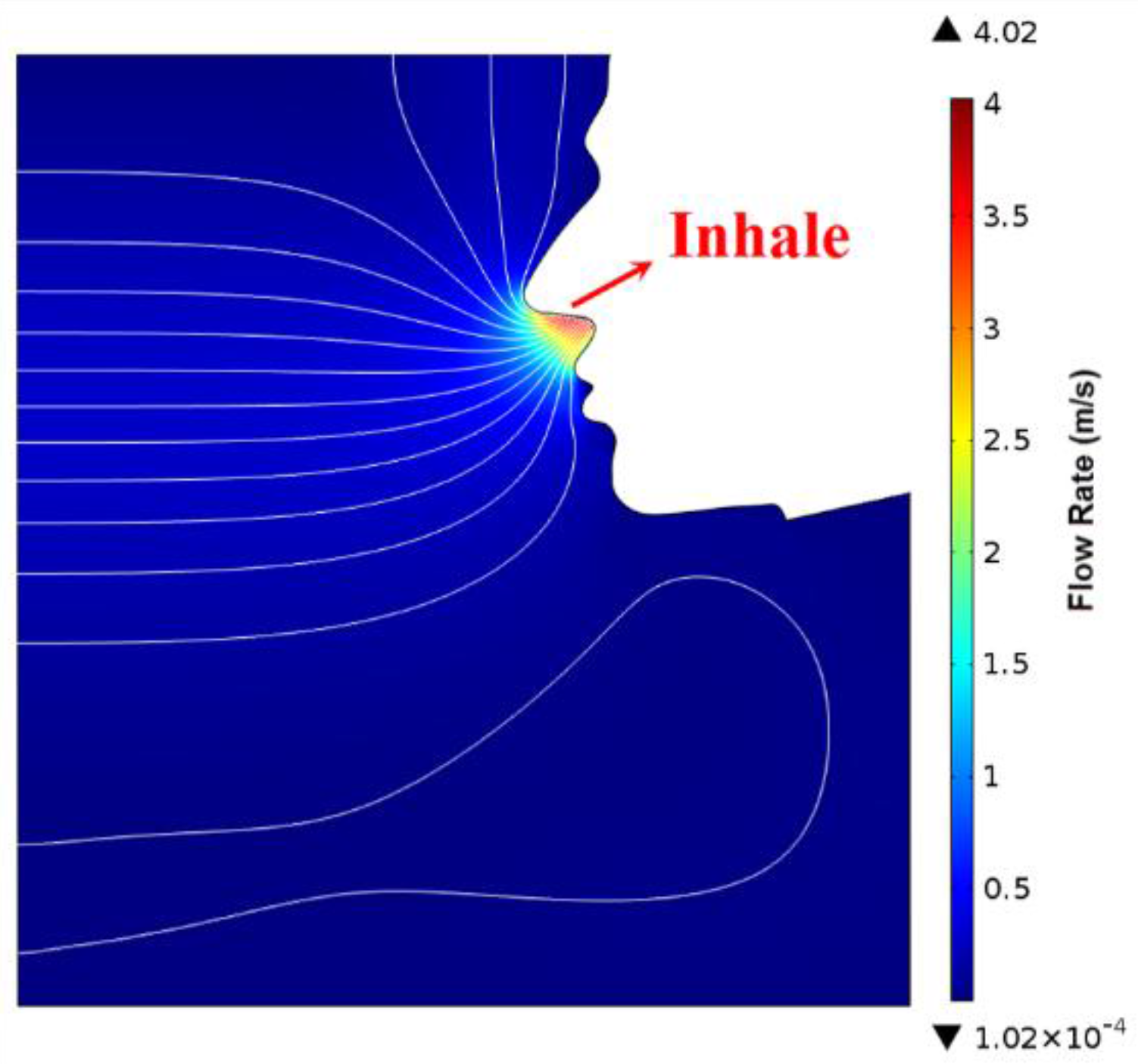
3.1. Simulation of Human Exhalation and Inhalation Flow Field

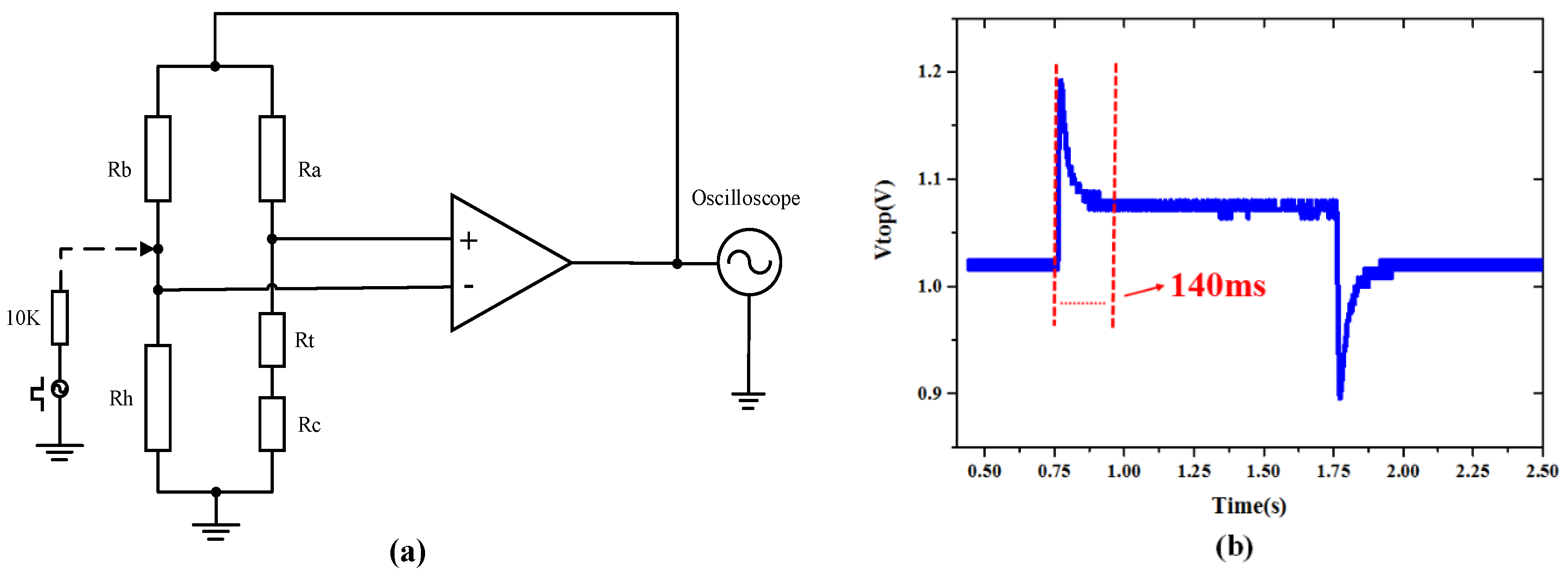
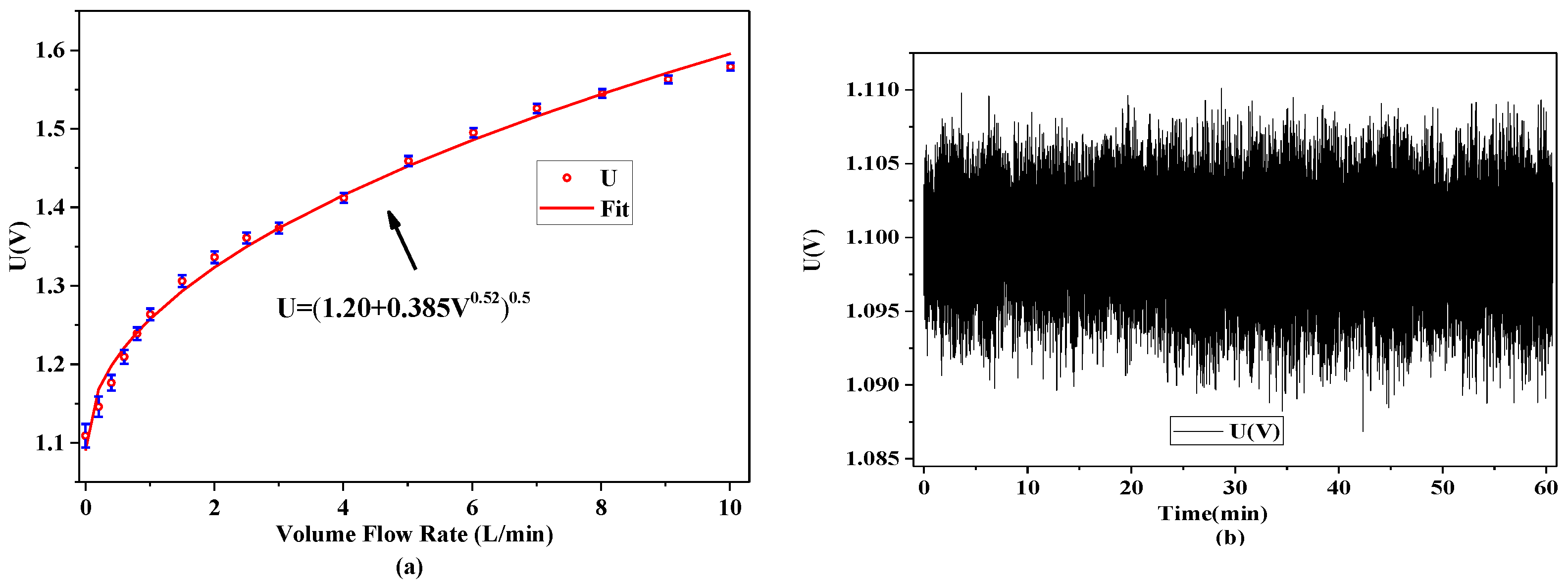
3.2. Calibration and Dynamic Response of the Airflow Sensor
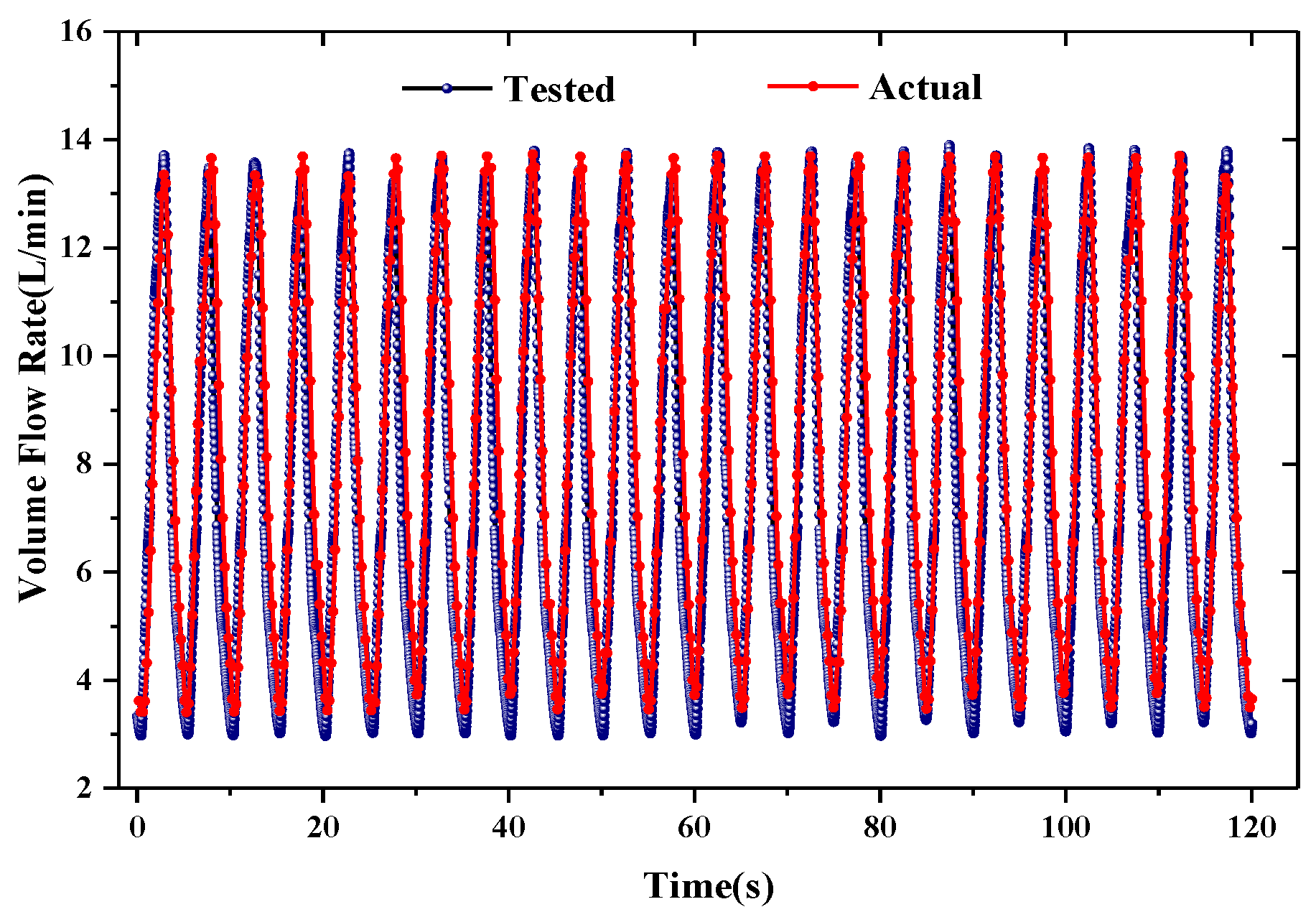
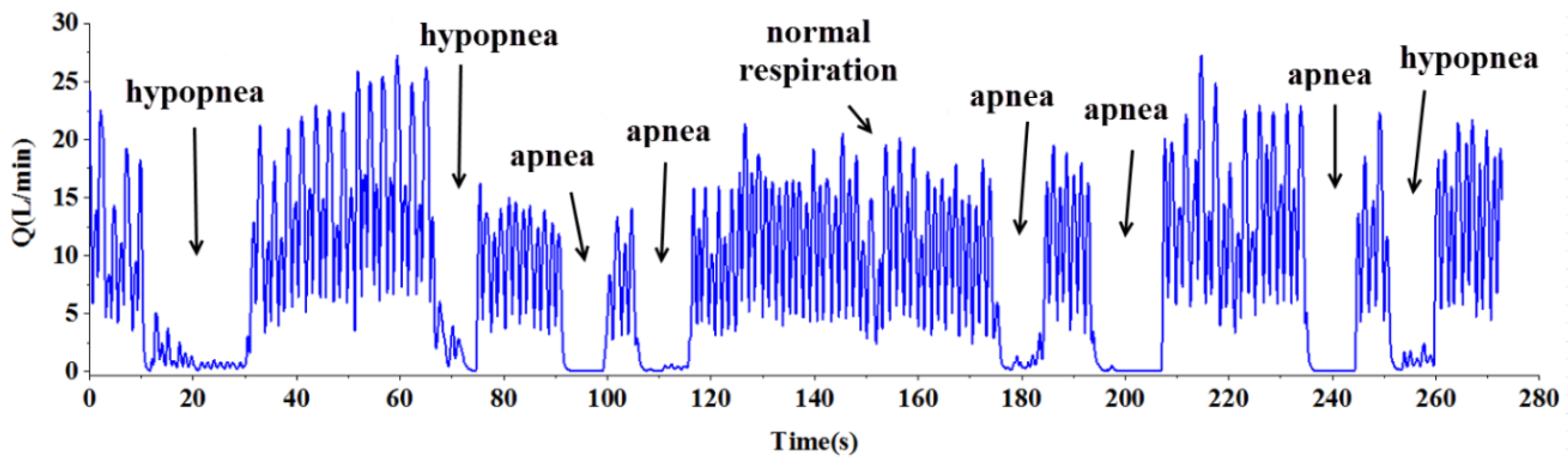
3.3. Monitoring of Respiration
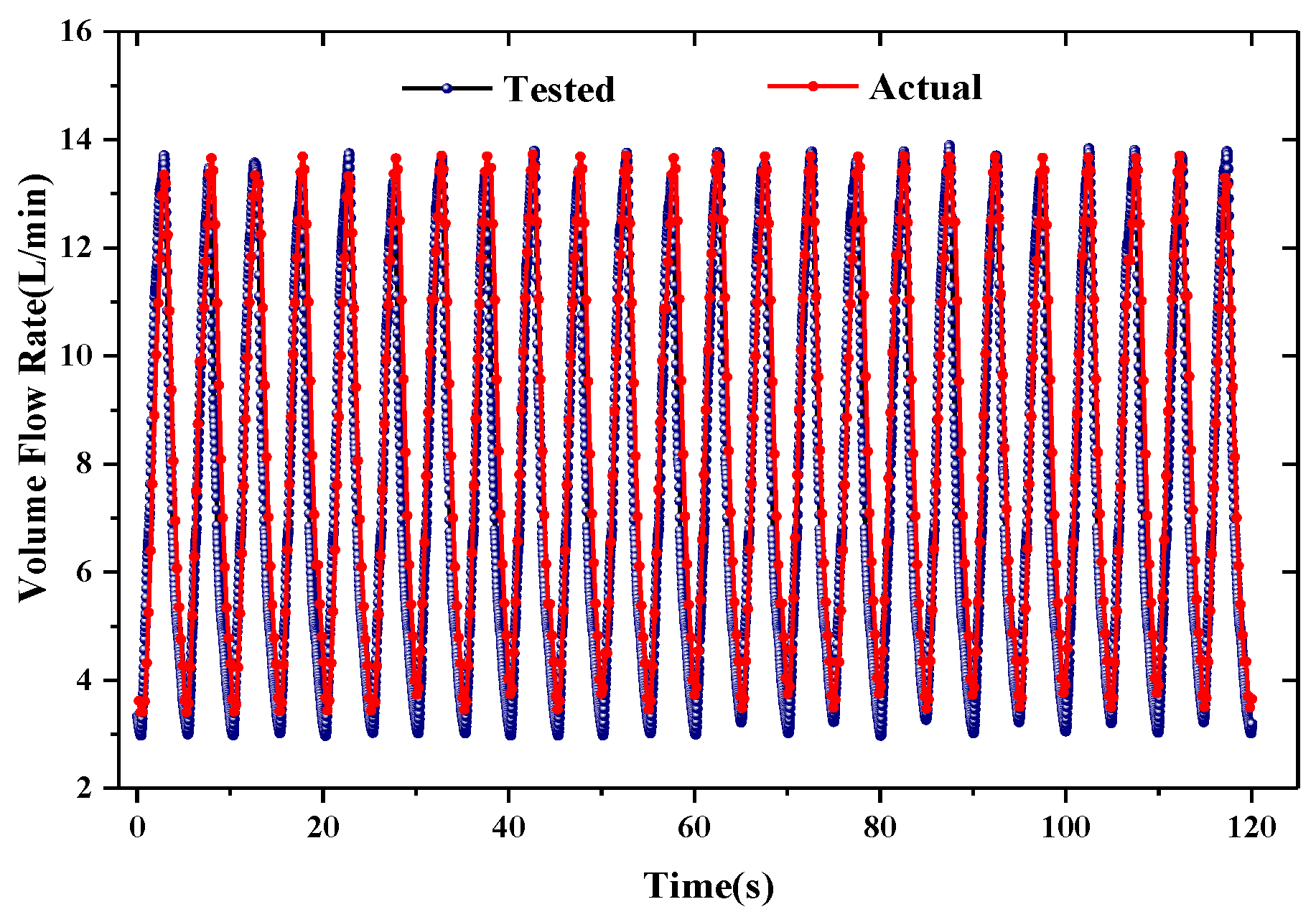
| Parameters | MV (L) | TV (L) | PIF (L/min) | RR (min−1) |
|---|---|---|---|---|
| Tested value | 8.0 | 0.67 | 14.2 | 12 |
| Actual value | 8.3 | 0.69 | 13.9 | 12 |
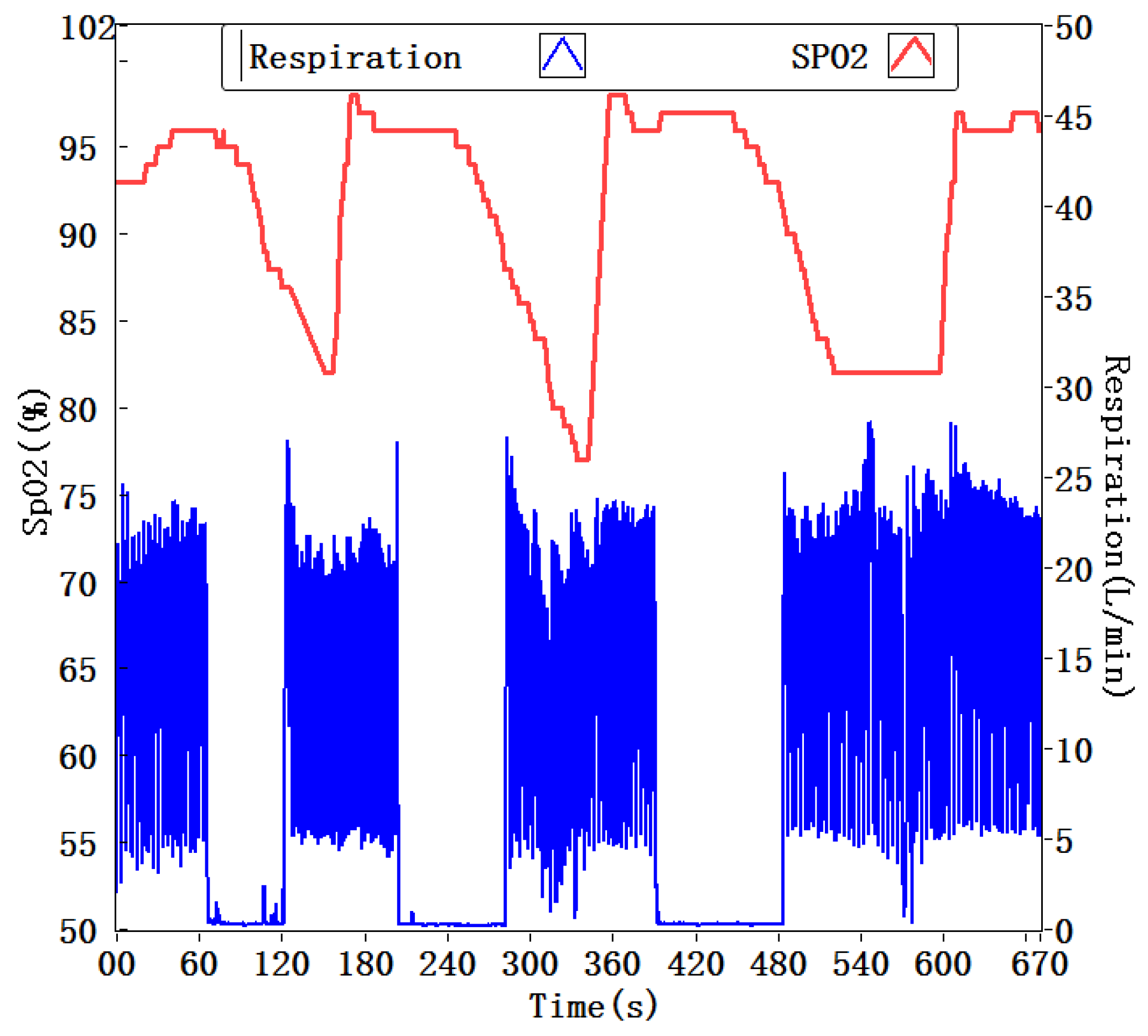
3.4. Monitoring of Oxygen Saturation and Respiration
3.5. Monitoring of Sleep Posture, Oxygen Saturation, and Respiration

4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. The 10 Leading Causes of Death in the World, 2000 and 2012; World Health Organization: Geneva, Switzerland, 2014. Available online: http://www.who.int/mediacentre/factsheets/fs310/en/ (accessed on 15 May 2014).
- Jain, C.D.; Bhaskar, D.J.; Kalra, M.; Gandhi, R.; Bohra, P. Recent Improvements in the Management of Obstructive Sleep Apnea: The Dental Perception. Int. J. Adv. Health Sci. 2015, 1, 7–10. [Google Scholar]
- Vaessen, T.J.; Overeem, S.; Sitskoorn, M.M. Cognitive complaints in obstructive sleep apnea. Sleep Med. Rev. 2015, 19, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Yaggi, H.K.; Araujo, A.B.; McKinlay, J.B. Sleep duration as a risk factor for the development of type 2 diabetes. Diabetes Care 2006, 29, 657–661. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. National Heart, Lung and Blood Institute (NHLBI). Guidelines for the Diagnosis and Management of Asthma (EPR-3); NHLBI: Bethesda, MD, USA. Available online: http://www.nhlbi.nih.gov/guidelines/asthma (accessed on 10 Feburary 2011).
- Kushida, C.A.; Littner, M.R.; Morgenthaler, T.; Alessi, C.A.; Bailey, D.; Coleman, J., Jr.; Friedman, L.; Hirshkowitz, M.; Kapen, S.; Kramer, M. Practice parameters for the indications for polysomnography and related procedures: An update for 2005. Sleep 2005, 28, 499–521. [Google Scholar] [PubMed]
- Oliveira, M.G.; Nery, L.E.; Santos-Silva, R.; Sartori, D.E.; Alonso, F.F.; Togeiro, S.M.; Tufik, S.; Bittencourt, L. Is portable monitoring accurate in the diagnosis of obstructive sleep apnea syndrome in chronic pulmonary obstructive disease? Sleep Med. 2012, 13, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Lowe, A.A.; Bai, Y.; Hamilton, P.; Fleetham, J.A.; Almeida, F.R. Evaluation of a portable recording device (apnealink™) for case selection of obstructive sleep apnea. Sleep Breath. 2009, 13, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Collop, N.A.; Anderson, W.M.; Boehlecke, B.; Claman, D.; Goldberg, R.; Gottlieb, D.; Hudgel, D.; Sateia, M.; Schwab, R. Clinical guidelines for the use of unattended portable monitors in the diagnosis of obstructive sleep apnea in adult patients. J. Clin. Sleep Med. 2007, 3, 737–747. [Google Scholar] [PubMed]
- Petrović, M.; Petrovic, J.; Daničić, A.; Vukčević, M.; Bojović, B.; Hadžievski, L.; Allsop, T.; Lloyd, G.; Webb, D. Non-invasive respiratory monitoring using long-period fiber grating sensors. Biomed. Opt. Express. 2014, 5, 1136–1144. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Zhu, R.; Que, R.-Y. A wireless portable system with microsensors for monitoring respiratory diseases. IEEE Trans. Biomed. Eng. 2012, 59, 3110–3116. [Google Scholar] [PubMed]
- Folke, M.; Cernerud, L.; Ekström, M.; Hök, B. Critical review of non-invasive respiratory monitoring in medical care. Med. Biol. Eng. Comput. 2003, 41, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Dziuda, L. Fiber-optic sensors for monitoring patient physiological parameters: A review of applicable technologies and relevance to use during magnetic resonance imaging procedures. J. Biomed. Opt. 2015, 20, 010901. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C.; Yu, X.; Czaplik, M.; Rossaint, R.; Blazek, V.; Leonhardt, S. Remote monitoring of breathing dynamics using infrared thermography. Biomed. Opt. Express 2015, 6, 4378–4394. [Google Scholar] [CrossRef] [PubMed]
- Schena, E.; Massaroni, C.; Saccomandi, P.; Cecchini, S. Flow measurement in mechanical ventilation: A review. Med. Eng. Phys. 2015, 37, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Snepvangers, Y.; de Winter, P.; Burger, H.; Brouwers, H.A.; Bogaard, J.M.; van der Ent, K. Correction factors for oxygen and gas flow-rate effects on neonatal Fleisch and Lilly pneumotachographs. Pediat. Crit. Care Med. 2003, 4, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Tardi, G.; Massaroni, C.; Saccomandi, P.; Schena, E. Experimental Assessment of a Variable Orifice Flowmeter for Respiratory Monitoring. J. Sens. 2015. [Google Scholar] [CrossRef]
- Kuo, J.T.; Yu, L.; Meng, E. Micromachined thermal flow sensors—A review. Micromachines 2012, 3, 550–573. [Google Scholar] [CrossRef]
- Nguyen, N. Micromachined flow sensors—A review. Flow Meas. Instrum. 1997, 8, 7–16. [Google Scholar] [CrossRef]
- Sturm, H.; Lang, W. Membrane-based thermal flow sensors on flexible substrates. Sens. Actuators A Phys. 2013, 195, 113–122. [Google Scholar] [CrossRef]
- Petropoulos, A.; Pagonis, D.N.; Kaltsas, G. Flexible PCB-MEMS flow sensor. Procedia Eng. 2012, 47, 236–239. [Google Scholar] [CrossRef]
- Sturm, H.; Brauns, E.; Froehner, K.; Lang, W.; Buchner, R. Thermoelectric Flow Sensors on Flexible Substrates and Their Integration Proces. In Proceedings of the IEEE Sensors, Kona, HI, USA, 1–4 November 2010; pp. 575–579.
- Bowman, B.; Stasz, P. Method of Making a Respiration Sensor. U.S. Patent 5,832,592, 10 November 1998. [Google Scholar]
- Zhao, S.; Zhu, R. Monolithic integration of a flexible micro thermal flow sensor. In Applied Mechanics and Materials; Trans Tech Publication: Beijing, China, 2015; pp. 89–92. [Google Scholar]
- Bruun, H.H. Hot-Wire Anemometry Principles and Signal Analysis. Meas. Sci. Technol. 1995, 7. [Google Scholar] [CrossRef]
- Gomez, C.; Oller, J.; Paradells, J. Overview and evaluation of bluetooth low energy: An emerging low-power wireless technology. Sensors 2012, 12, 11734–11753. [Google Scholar] [CrossRef]
- Devita, G.; Wong, A.; Dawkins, M.; Glaros, K.; Kiani, U.; Lauria, F.; Madaka, V.; Omeni, O.; Schiff, J.; Vasudevan, A. A 5 mw Multi-Standard Bluetooth Le/Ieee 802.15. 6 Soc for Wban Applications. In Proceedings of the 40th European Solid State Circuits Conference (ESSCIRC), Venice, Italy, 22–26 September 2014; IEEE: New York, NY, USA, 2014; pp. 283–286. [Google Scholar]
- Zuurbier, M.; Hoek, G.; van den Hazel, P.; Brunekreef, B. Minute ventilation of cyclists, car and bus passengers: An experimental study. Environ. Health 2009, 8, 48. [Google Scholar] [CrossRef] [PubMed]
- Harrison, K.L.; Bogard, D.G. Comparison of Rans Turbulence Models for Prediction of Film Cooling Performance. In Proceedings of the ASME Turbo Expo 2008: Power for Land, Sea, and Air, Berlin, Germany, 9–13 June 2008; pp. 1187–1196.
- Grossman, E.; Grossman, A.; Schein, M.; Zimlichman, R.; Gavish, B. Breathing-control lowers blood pressure. J. Hum. Hypertens. 2001, 15, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Collop, N.A.; Tracy, S.L.; Kapur, V.; Mehra, R.; Kuhlmann, D.; Fleishman, S.A.; Ojile, J.M. Obstructive sleep apnea devices for out-of-center (ooc) testing: Technology evaluation. J. Clin. Sleep Med. JCSM 2011, 7, 531–548. [Google Scholar] [CrossRef] [PubMed]
- Ozeke, O.; Erturk, O.; Gungor, M.; Hizel, S.B.; Aydin, D.; Celenk, M.K.; Dincer, H.; Ilicin, G.; Ozgen, F.; Ozer, C. Influence of the right-versus left-sided sleeping position on the apnea-hypopnea index in patients with sleep apnea. Sleep Breath. 2012, 16, 617–620. [Google Scholar] [CrossRef] [PubMed]
- Tamilia, E.; Taffoni, F.; Formica, D.; Ricci, L.; Schena, E.; Keller, F.; Guglielmelli, E. Technological solutions and main indices for the assessment of newborns' Nutritive Sucking: A review. Sensors 2014, 14, 634–658. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, P.; Zhao, S.; Zhu, R. Smart Sensing Strip Using Monolithically Integrated Flexible Flow Sensor for Noninvasively Monitoring Respiratory Flow. Sensors 2015, 15, 31738-31750. https://doi.org/10.3390/s151229881
Jiang P, Zhao S, Zhu R. Smart Sensing Strip Using Monolithically Integrated Flexible Flow Sensor for Noninvasively Monitoring Respiratory Flow. Sensors. 2015; 15(12):31738-31750. https://doi.org/10.3390/s151229881
Chicago/Turabian StyleJiang, Peng, Shuai Zhao, and Rong Zhu. 2015. "Smart Sensing Strip Using Monolithically Integrated Flexible Flow Sensor for Noninvasively Monitoring Respiratory Flow" Sensors 15, no. 12: 31738-31750. https://doi.org/10.3390/s151229881
APA StyleJiang, P., Zhao, S., & Zhu, R. (2015). Smart Sensing Strip Using Monolithically Integrated Flexible Flow Sensor for Noninvasively Monitoring Respiratory Flow. Sensors, 15(12), 31738-31750. https://doi.org/10.3390/s151229881