
Measurement Properties of the Smartphone-Based B-B Score in Current Shoulder Pathologies


Abstract
:1. Introduction
1.1. Measurement Properties in Shoulder Function Evaluation
1.2. Influence of Shoulder Pathologies on Physiological Movement
1.3. Study Aim and Hypotheses
- -
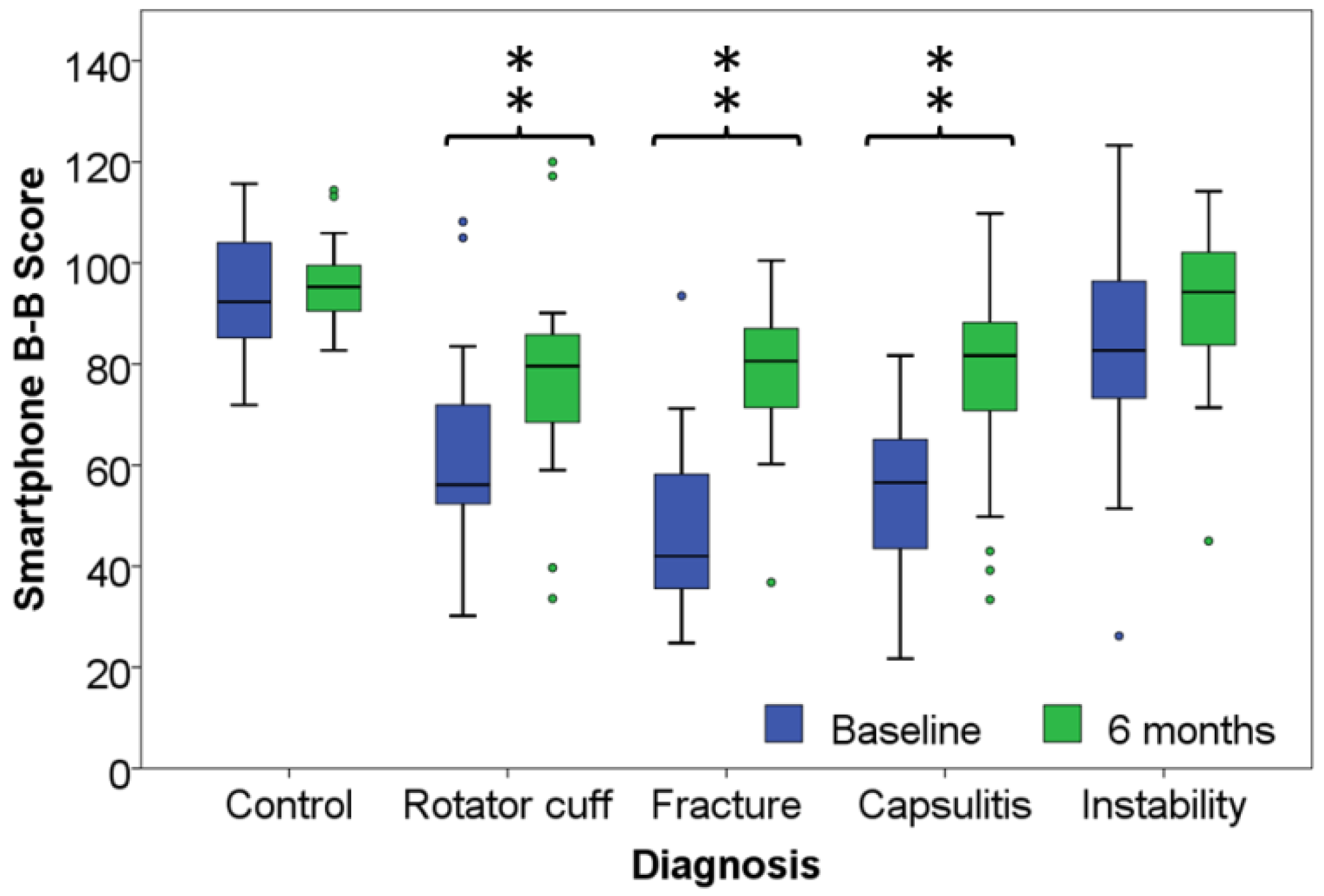
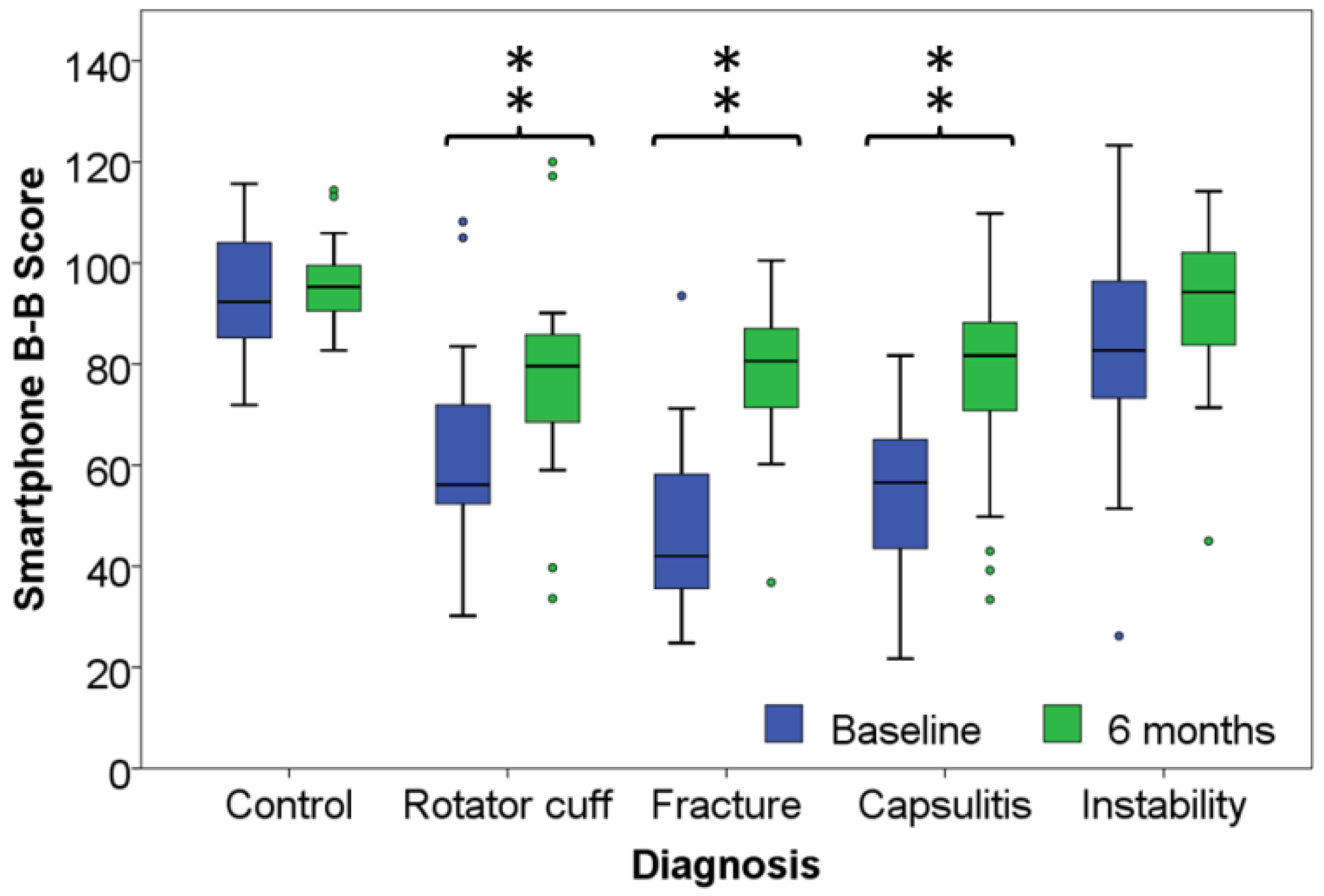
- the score would remain stable in the control group while it would progress significantly (p < 0.05) over time in each pathological group,
- -
- the responsiveness would be comparable to that of validated clinical questionnaires,
- -
- the area under the receiver operating characteristic (ROC) curve indicative of diagnostic power, would be at least adequate (≥0.70),
- -
2. Experimental Section
2.1. Participants
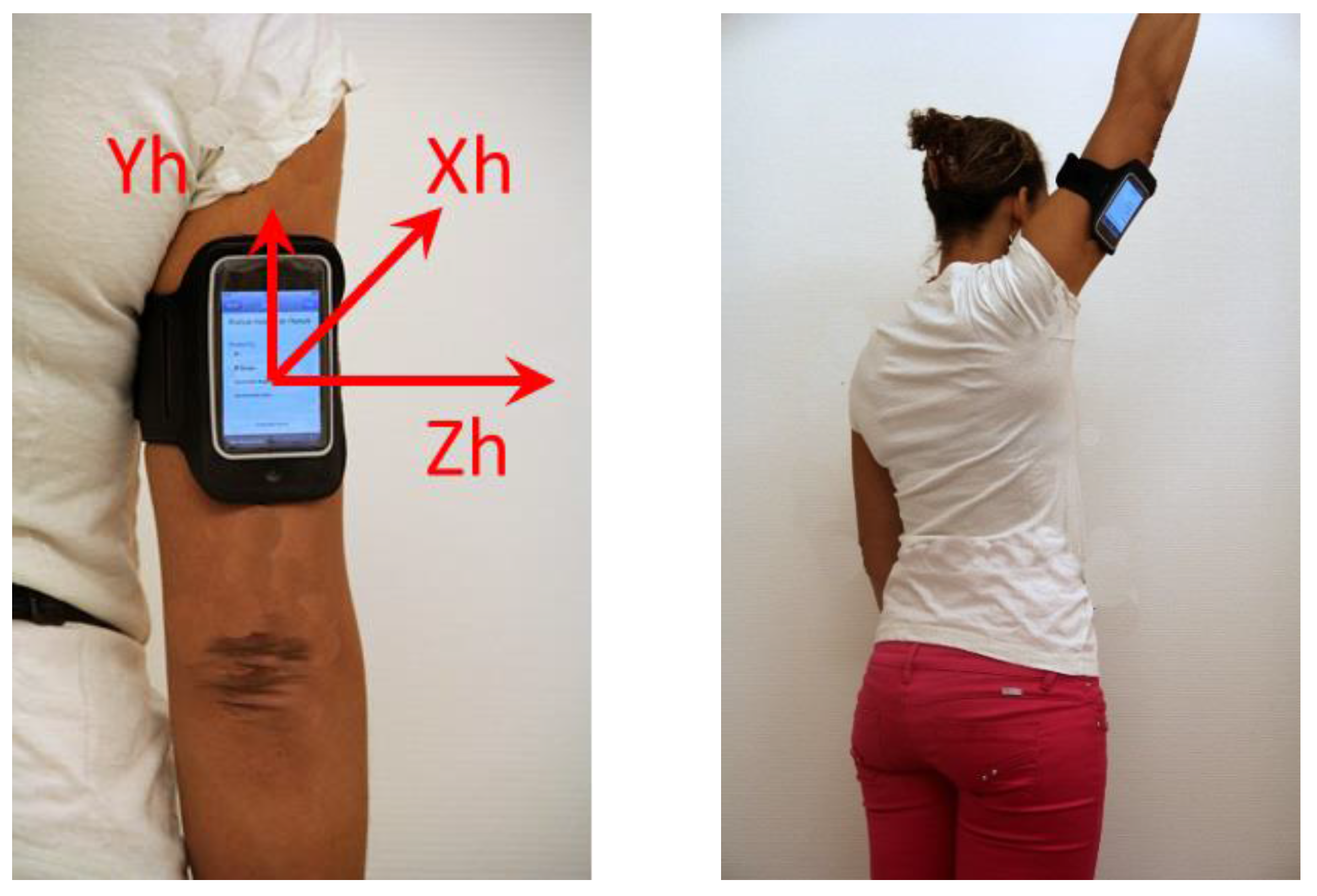
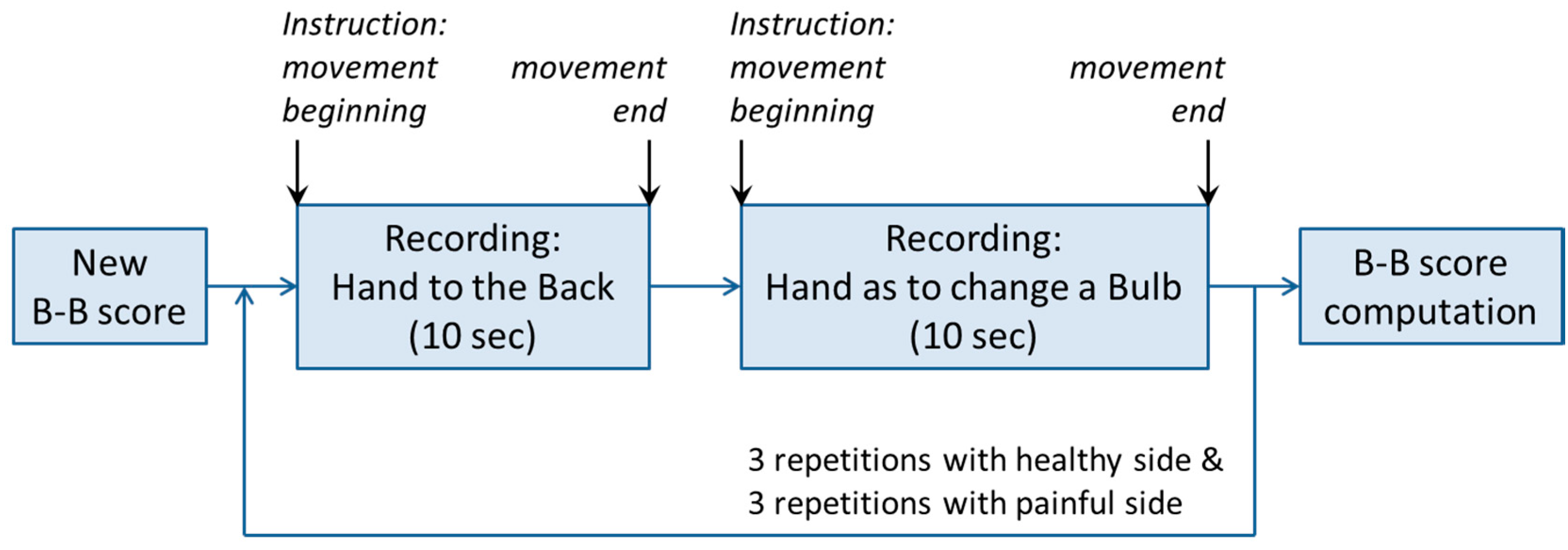
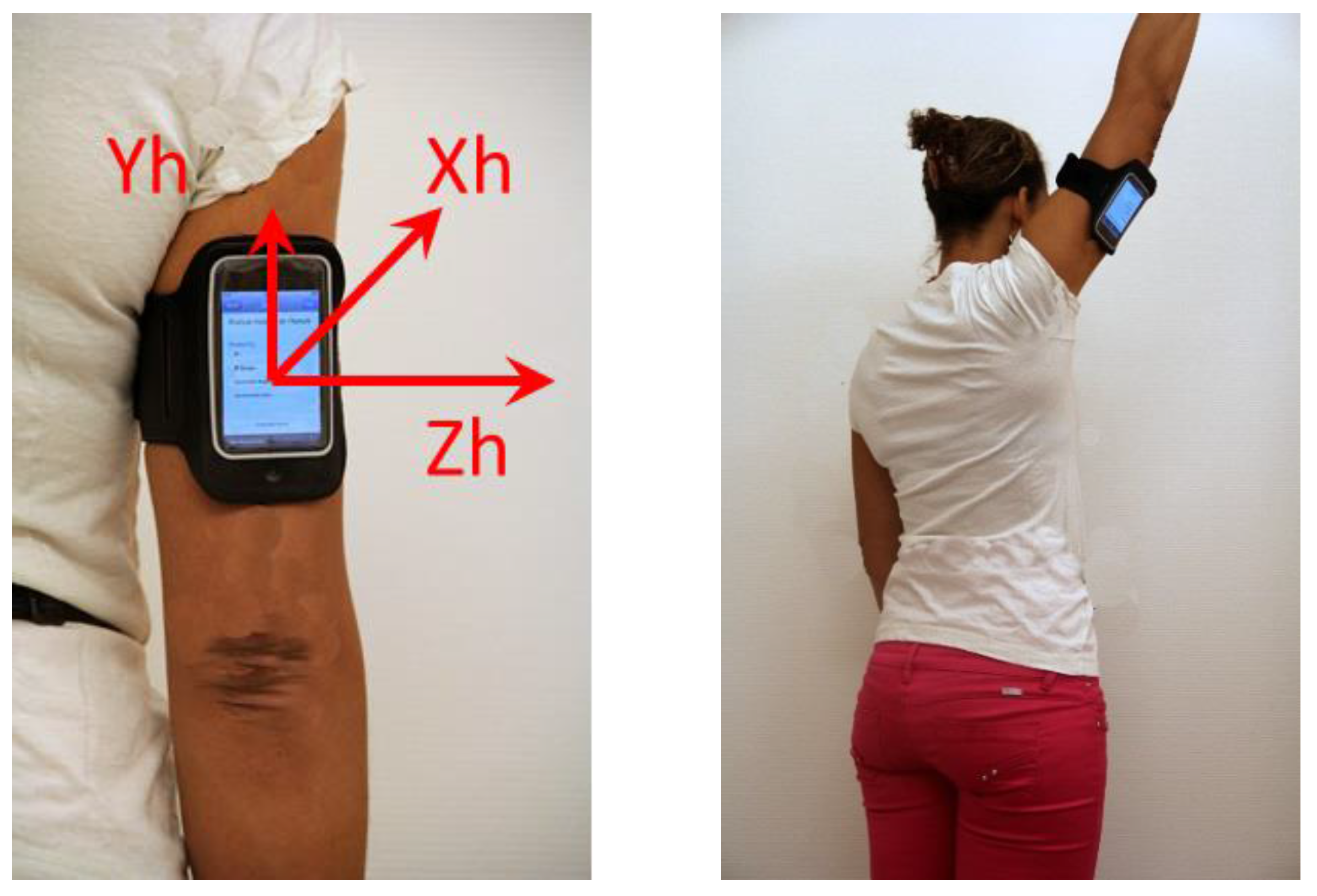
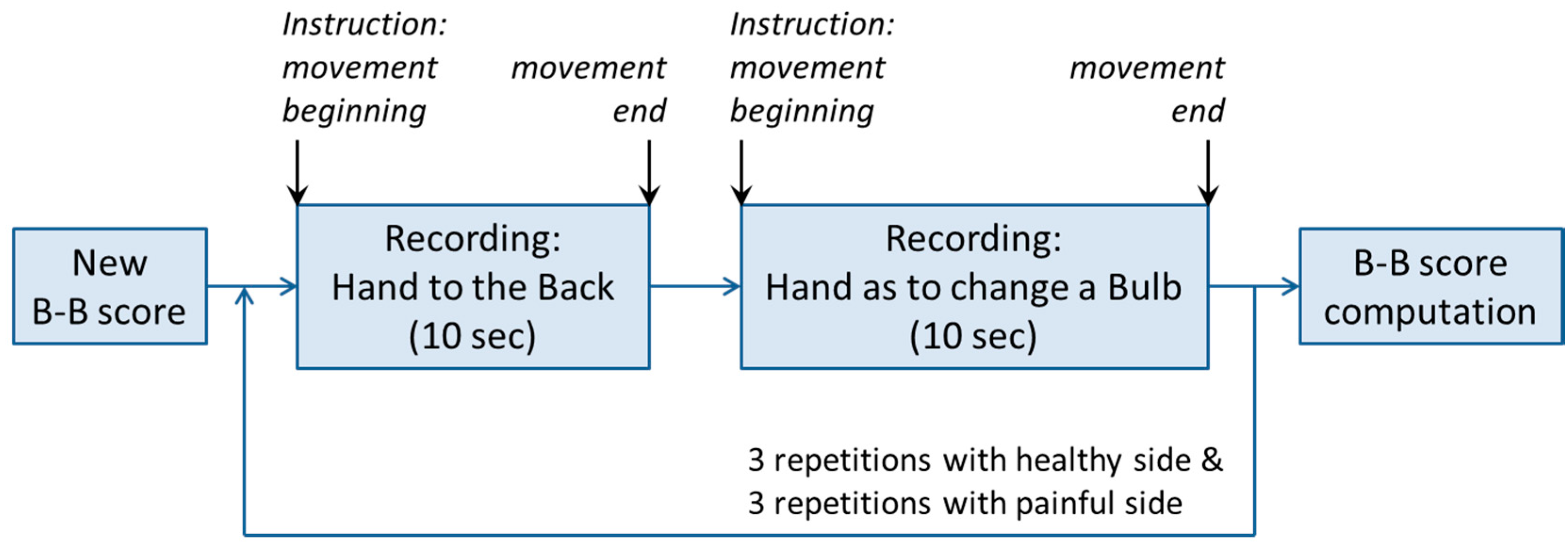
2.2. Measurement Protocol Heading
2.3. Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
| Rotator Cuff (n = 20) | Fracture (n = 23) | Capsulitis (n = 22) | Instability (n = 23) | Control (n = 20) | |
|---|---|---|---|---|---|
| Age mean (SD), Years | 63.5 * (10.6) | 60.1 * (15.6) | 52.5 * (13.8) | 32.1 (14.1) | 28.2 (6.2) |
| Sex, % Women | 50 | 78 | 60 | 43 | 50 |
| Weight Mean (SD), kg | 78.3 (18.2) | 69.6 (15.1) | 78.3 (15.1) | 70.8 (12.9) | 74.7 (17.4) |
| Body Mass Index Mean (SD), kg/m2 | 25.8 (5.4) | 25.8 (5.4) | 25.8 (5.4) | 25.8 (5.4) | 24.2 (3.9) |
| Size Mean (SD), m. | 164.0 * (7.4) | 167.7 (9.7) | 172.4 (10.9) | 172.6 (9.4) | 175.0 (10.3) |
| Hand Dominance, % Right-Handed | 90 | 87 | 100 | 87 | 90 |
| Affected Side, % Dominant Side | 70 | 25 | 45 | 52 | - |
| Pathology | Control | Rotator Cuff | Humerus Fracture | Capsulitis | Shoulder Instability | |
|---|---|---|---|---|---|---|
| Baseline | Mean (SD) | 94.1 (11.1) * | 63.1 (19.7) * | 46.3 (17.5) * | 54.4 (14.6) * | 84.5 (22.6) |
| Sample size | 20 | 20 | 23 | 22 | 23 | |
| 6 months | Mean (SD) | 96.0 (8.3) * | 77.6 (21.1) *,† | 78.9 (15.1) *,† | 75.3 (20.5) *,† | 91.2 (15.6) |
| Sample size | 20 | 19 | 20 | 21 | 20 | |
| Outcome Measure | Rotator Cuff | Fracture | Capsulitis | Instability |
|---|---|---|---|---|
| Effect Size (95% CI) | ||||
| B-B Score | 0.69 (0.02–1.33) | 1.94 (1.14–2.67) | 1.16 (0.49–1.79) | 0.10 (−0.52–0.72) |
| Constant | 0.54 (−0.12–1.18) | 2.09 (1.26–2.83) | 1.05 (0.38–1.67) | 0.21 (−0.42–0.82) |
| Relative Constant | 0.50 (−0.15–1.14) | 2.10 (1.27–2.84) | 1.04 (0.38–1.67) | 0.27 (−0.36–0.89) |
| SST | 0.52 (−0.13–1.16) | 1.65 (0.89–2.35) | 0.86 (0.22–1.48) | 0.10 (−0.53–0.71) |
| QuickDASH | 0.35 (−0.30–0.98) | 1.25 (0.53–1.91) | 0.55 (−0.08–1.16) | 0.01 (−0.61–0.63) |
| WOSI | - | - | - | 0.47 (0.17–1.09) |
| EQ-5D | 0.23 (−0.42–0.86) | 0.76 (0.09–1.40) | 0.34 (−0.27–0.94) | 0.37 (−0.26–0.99) |
| EQ-5D VAS | 0.07 (−0.57–0.70) | 0.37(−0.26–0.99) | 0.06 (−0.55–0.66) | 0.11 (−0.51–0.73) |
| AUC (95% CI) | B-B Score Threshold (%) | Sensitivity (%) | Specificity (%) | |
| Rotator Cuff | 0.90 (0.78–1.00) | 83.6 | 90 | 90 |
| Humerus Fracture | 0.98 (0.94–1.00) | 71.6 | 100 | 96 |
| Capsulitis | 0.99 (0.98–1.00) | 82.1 | 95 | 100 |
| Shoulder Instability | 0.67 (0.50–0.84) | 81.6 | 95 | 48 |
| Rotator Cuff | Humerus Fracture | Capsulitis | Shoulder Instability | |
|---|---|---|---|---|
| Constant | 0.82 ** | 0.70 ** | 0.68 ** | 0.46 * |
| Relative Constant | 0.84 ** | 0.69 ** | 0.69 ** | 0.43 * |
| SST | 0.63 ** | 0.66 ** | 0.76 ** | 0.52 * |
| QuickDASH | −0.55 * | −0.40 | −0.64 ** | −0.57 ** |
| WOSI | - | - | - | 0.58 |
| VAS pain | −0.50 * | −0.07 | −0.39 | −0.19 |
| EQ5D | 0.33 | 0.18 | 0.63 ** | 0.46 * |
| EQ5D-VAS | 0.16 | −0.30 | 0.44 * | 0.47 * |
4. Discussion
4.1. Results Interpretation
4.2. Limitations and Further Developments
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Picavet, H.S.; Schouten, J.S. Musculoskeletal pain in the Netherlands: Prevalences, consequences and risk groups, the DMC(3)-study. Pain 2003, 102, 167–178. [Google Scholar] [CrossRef]
- Huang, H.; Grant, J.A.; Miller, B.S.; Mirza, F.M.; Gagnier, J.J. A systematic review of the psychometric properties of patient-reported outcome instruments for use in patients with rotator cuff disease. Am. J. Sports Med. 2015, 43, 2572–2582. [Google Scholar] [CrossRef] [PubMed]
- Fayad, F.; Mace, Y.; Lefevre-Colau, M.M. Les échelles d’incapacité fonctionnelle de l’épaule: Revue systématique. Ann. Réadaptation Méd. Phys. 2005, 48, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Christie, A.; Hagen, K.B.; Mowinckel, P.; Dagfinrud, H. Methodological properties of six shoulder disability measures in patients with rheumatic diseases referred for shoulder surgery. J. Shoulder Elbow Surg. 2009, 18, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.H.; Jo, K.H.; Kim, W.S.; Gong, H.S.; Han, S.G.; Kim, Y.H. Comparative evaluation of the measurement properties of various shoulder outcome instruments. Am. J. Sports Med. 2009, 37, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Prentice Hall Health: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Lippitt, S.B.; Harryman, D.T.; Matsen, F.A. A practical tool for evaluating function: The simple shoulder test. In The Shoulder: A Balance of Mobility and Stability; Matsen, American Academy of Orthopaedic Surgery: Rosemont, IL, USA, 1993; pp. 501–518. [Google Scholar]
- Coley, B.; Jolles, B.M.; Farron, A.; Bourgeois, A.; Nussbaumer, F.; Pichonnaz, C.; Aminian, K. Outcome evaluation in shoulder surgery using 3D kinematics sensors. Gait Posture 2007, 25, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Pichonnaz, C.; Lecureux, E.; Bassin, J.P.; Duc, C.; Farron, A.; Aminian, K.; Jolles, B.M.; Gleeson, N. Enhancing clinically-relevant shoulder function assessment using only essential movements. Physiol. Meas. 2015, 36, 547–560. [Google Scholar] [CrossRef] [PubMed]
- Pichonnaz, C.; Duc, C.; Jaccard, H.; Ancey, C.; Lécureux, E.; Aminian, K.; Farron, A.; Jolles, B.M.; Gleeson, N. Comparison of a dedicated body-worn inertial system and a smartphone for shoulder function and arm elevation evaluation. Physiotherapy 2015, 101, 1205–1206. [Google Scholar] [CrossRef]
- Tubach, F.; Ravaud, P.; Beaton, D.; Boers, M.; Bombardier, C.; Felson, D.T.; van der Heijde, D.; Wells, G.; Dougados, M. Minimal clinically important improvement and patient acceptable symptom state for subjective outcome measures in rheumatic disorders. J. Rheumatol. 2007, 34, 1188–1193. [Google Scholar] [PubMed]
- Beaton, D.E.; Bombardier, C.; Katz, J.N.; Wright, J.G.; Wells, G.; Boers, M.; Strand, V.; Shea, B. Looking for important change/differences in studies of responsiveness. J. Rheumatol. 2001, 28, 400–405. [Google Scholar] [PubMed]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Colvin, A.C.; Egorova, N.; Harrison, A.K.; Moskowitz, A.; Flatow, E.L. National trends in rotator cuff repair. J. Bone Joint Surg. Am. 2012, 94, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Coley, B. Shoulder Function and Outcome Evaluation after Surgery Using 3D Inertial Sensors; Doctorate ès Sciences, Swiss Institute of Technology: Lausanne, Switzerland, 2007. [Google Scholar]
- Jolles, B.M.; Duc, C.; Coley, B.; Aminian, K.; Pichonnaz, C.; Bassin, J.P.; Farron, A. Objective evaluation of shoulder function using body-fixed sensors: A new way to detect early treatment failures? J. Shoulder Elbow Surg. 2011, 20, 1074–1081. [Google Scholar] [CrossRef] [PubMed]
- Van der Windt, D.A.; Koes, B.W.; Boeke, A.J.; Deville, W.; De Jong, B.A.; Bouter, L.M. Shoulder disorders in general practice: Prognostic indicators of outcome. Br. J. Gen. Pract. 1996, 46, 519–523. [Google Scholar] [PubMed]
- Yamamoto, A.; Takagishi, K.; Osawa, T.; Yanagawa, T.; Nakajima, D.; Shitara, H.; Kobayashi, T. Prevalence and risk factors of a rotator cuff tear in the general population. J. Shoulder Elbow Surg. 2010, 19, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Van der Windt, D.A.; Koes, B.W.; de Jong, B.A.; Bouter, L.M. Shoulder disorders in general practice: Incidence, patient characteristics, and management. Ann. Rheum. Dis. 1995, 54, 959–964. [Google Scholar] [CrossRef] [PubMed]
- Court-Brown, C.M.; Caesar, B. Epidemiology of adult fractures: A review. Injury 2006, 37, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Liavaag, S.; Svenningsen, S.; Reikeras, O.; Enger, M.; Fjalestad, T.; Pripp, A.H.; Brox, J.I. The epidemiology of shoulder dislocations in oslo. Scand. J. Med. Sci. Sports 2011, 21, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Owens, B.D.; Duffey, M.L.; Nelson, B.J.; DeBerardino, T.M.; Taylor, D.C.; Mountcastle, S.B. The incidence and characteristics of shoulder instability at the United States Military Academy. Am. J. Sports Med. 2007, 35, 1168–1173. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.; Adebajo, A.; Hay, E.; Carr, A. Shoulder pain: Diagnosis and management in primary care. BMJ 2005, 331, 1124–1128. [Google Scholar] [CrossRef] [PubMed]
- O’Kane, J.W.; Toresdahl, B.G. The evidenced-based shoulder evaluation. Curr. Sports Med. Rep. 2014, 13, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Moosmayer, S.; Smith, H.J.; Tariq, R.; Larmo, A. Prevalence and characteristics of asymptomatic tears of the rotator cuff: An ultrasonographic and clinical study. J. Bone Joint Surg. Br. 2009, 91, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Kelley, M.J.; Shaffer, M.A.; Kuhn, J.E.; Michener, L.A.; Seitz, A.L.; Uhl, T.L.; Godges, J.J.; McClure, P.W. Shoulder pain and mobility deficits: Adhesive capsulitis. J. Orthop. Sports Phys. Ther. 2013, 43, A1–A31. [Google Scholar] [CrossRef] [PubMed]
- Handoll, H.H.; Ollivere, B.J.; Rollins, K.E. Interventions for treating proximal humeral fractures in adults. Cochrane Database Syst. Rev. 2012, 12. [Google Scholar] [CrossRef]
- Handoll, H.H.; Almaiyah, M.A.; Rangan, A. Surgical versus non-surgical treatment for acute anterior shoulder dislocation. Cochrane Database Syst. Rev. 2004. [Google Scholar] [CrossRef]
- Rouleau, D.M.; Faber, K.; MacDermid, J.C. Systematic review of patient-administered shoulder functional scores on instability. J. Shoulder Elbow Surg. 2010, 19, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- Munro, B.H. Statistical Methods for Health Care Research; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Soper, D.S. Statistics Calculators. Available online: http://www.webcitation.org/6ZEMd2NIS (accessed on 12 May 2015).
- Lenth, R.V. Java Applets for Power and Sample Size. Available online: http://www.webcitation.org/6ZEMrvmpu (accessed on 12 May 2015).
- Mark, D.; Nutting, J.; LaMarche, J. Beginning iOS 5 Development: Exploring the iOS SDK; Apress: New York, NY, USA, 2011. [Google Scholar]
- Oïhénart, L.; Duc, C.; Aminian, K. iShould: Functional evaluation of the shoulder using a Smartphone. Gait Posture 2012, 36, 61–62. [Google Scholar] [CrossRef]
- Smartphone App iShould. Available online: http://lmam.epfl.ch/smartphone/ishould (accessed on 23 October 2015).
- Constant, C.R.; Murley, A.H. A clinical method of functional assessment of the shoulder. Clin. Orthop. Relat. Res. 1987, 214, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Richards, R.R.; An, K.N.; Bigliani, L.U.; Friedman, R.J.; Gartsman, G.M.; Gristina, A.G.; Iannotti, J.P.; Mow, V.C.; Sidles, J.A.; Zuckerman, J.D. A standardized method for the assessment of shoulder function. J. Shoulder Elbow Surg. 1994, 3, 347–352. [Google Scholar] [CrossRef]
- American Academy of Orthopaedic Surgeons. The DASH Outcome Measure. Available online: http://www.webcitation.org/6ZEN143eU (accessed on 12 May 2015).
- EuroQol Group. EQ-5D a Standardised Instrument for Use as a Measure of Health Outcome. Available online: http://www.webcitation.org/6ZEN3QDth (accessed on 12 May 2015).
- Kirkley, A.; Griffin, S.; McLintock, H.; Ng, L. The development and evaluation of a disease-specific quality of life measurement tool for shoulder instability. Am. J. Sports Med. 1998, 26, 764–772. [Google Scholar] [PubMed]
- Constant, C.R.; Gerber, C.; Emery, R.J.H.; Søjbjerg, J.O.; Gohlke, F.; Boileau, P. A review of the Constant score: Modifications and guidelines for its use. J. Shoulder Elbow Surg. 2008, 17, 355–361. [Google Scholar] [CrossRef] [PubMed]
- St-Pierre, C.; Desmeules, F.; Dionne, C.E.; Fremont, P.; MacDermid, J.C.; Roy, J.S. Psychometric properties of self-reported questionnaires for the evaluation of symptoms and functional limitations in individuals with rotator cuff disorders: A systematic review. Disabil. Rehabil. 2015. [Google Scholar] [CrossRef] [PubMed]
- Gartsman, G.M.; Morris, B.J.; Unger, R.Z.; Laughlin, M.S.; Elkousy, H.A.; Edwards, T.B. Characteristics of clinical shoulder research over the last decade: A review of shoulder articles in the Journal of Bone & Joint Surgery from 2004 to 2014. J. Bone Joint Surg. Am. 2015, 97. [Google Scholar] [CrossRef]
- Angst, F.; Schwyzer, H.K.; Aeschlimann, A.; Simmen, B.R.; Goldhahn, J. Measures of adult shoulder function: Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH) and its short version (QuickDASH), Shoulder Pain and Disability Index (SPADI), American Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form, Constant (Murley) Score (CS), Simple Shoulder Test (SST), Oxford Shoulder Score (OSS), Shoulder Disability Questionnaire (SDQ), and Western Ontario Shoulder Instability Index (WOSI). Arthritis Care Res. 2011, 63, 174–188. [Google Scholar]
- McHorney, C.A.; Tarlov, A.R. Individual-patient monitoring in clinical practice: Are available health status surveys adequate? Qual. Life Res. 1995, 4, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Cline, M.G.; Meredith, K.E.; Boyer, J.T.; Burrows, B. Decline of height with age in adults in a general population sample: Estimating maximum height and distinguishing birth cohort effects from actual loss of stature with aging. Hum. Biol. 1989, 61, 415–425. [Google Scholar] [PubMed]
- Torrens, C.; Sanchez, J.F.; Isart, A.; Santana, F. Does fracture of the dominant shoulder have any effect on functional and quality of life outcome compared with the nondominant shoulder? J. Shoulder Elbow Surg. 2015, 25, 677–681. [Google Scholar] [CrossRef] [PubMed]
- Baguley, T. Standardized or simple effect size: What should be reported? Br. J. Psychol. 2009, 100, 603–617. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, J.; Hamman, R.; Lowenstein, S.; Briggs, K.; Kocher, M. Reliability, validity, and responsiveness of the simple shoulder test: Psychometric properties by age and injury type. J. Shoulder Elbow Surg. 2007, 16, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Fitzpatrick, R.; Carr, A. The assessment of shoulder instability. J. Bone Joint Surg. Br. 1999, 81, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Jimerson, S.R.; Burns, M.K.; VanDerHeyden, A. Handbook of Response to Intervention: The Science and Practice of Assessment and Intervention; Springer Science & Business Media: Berlin, Germany, 2007. [Google Scholar]
- Tubach, F.; Ravaud, P.; Baron, G.; Falissard, B.; Logeart, I.; Bellamy, N.; Bombardier, C.; Felson, D.; Hochberg, M.; van der Heijde, D.; et al. Evaluation of clinically relevant changes in patient reported outcomes in knee and hip osteoarthritis: The minimal clinically important improvement. Ann. Rheum. Dis. 2005, 64, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Tubach, F.; Ravaud, P.; Baron, G.; Falissard, B.; Logeart, I.; Bellamy, N.; Bombardier, C.; Felson, D.; Hochberg, M.; van der Heijde, D.; et al. Evaluation of clinically relevant states in patient reported outcomes in knee and hip osteoarthritis: The patient acceptable symptom state. Ann. Rheum. Dis. 2005, 64, 34–37. [Google Scholar] [CrossRef] [PubMed]
- McDowell, I. Measuring Health: A Guide to Rating Scales and Questionnaires; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pichonnaz, C.; Duc, C.; Gleeson, N.; Ancey, C.; Jaccard, H.; Lécureux, E.; Farron, A.; Jolles, B.M.; Aminian, K. Measurement Properties of the Smartphone-Based B-B Score in Current Shoulder Pathologies. Sensors 2015, 15, 26801-26817. https://doi.org/10.3390/s151026801
Pichonnaz C, Duc C, Gleeson N, Ancey C, Jaccard H, Lécureux E, Farron A, Jolles BM, Aminian K. Measurement Properties of the Smartphone-Based B-B Score in Current Shoulder Pathologies. Sensors. 2015; 15(10):26801-26817. https://doi.org/10.3390/s151026801
Chicago/Turabian StylePichonnaz, Claude, Cyntia Duc, Nigel Gleeson, Céline Ancey, Hervé Jaccard, Estelle Lécureux, Alain Farron, Brigitte M. Jolles, and Kamiar Aminian. 2015. "Measurement Properties of the Smartphone-Based B-B Score in Current Shoulder Pathologies" Sensors 15, no. 10: 26801-26817. https://doi.org/10.3390/s151026801
APA StylePichonnaz, C., Duc, C., Gleeson, N., Ancey, C., Jaccard, H., Lécureux, E., Farron, A., Jolles, B. M., & Aminian, K. (2015). Measurement Properties of the Smartphone-Based B-B Score in Current Shoulder Pathologies. Sensors, 15(10), 26801-26817. https://doi.org/10.3390/s151026801