
Next-Generation Sequencing in Oncology—A Guiding Compass for Targeted Therapy and Emerging Applications

 , ,
, ,  , and
, and
Abstract
1. Introduction
2. The Current Role of NGS in Solid Tumor Oncology
2.1. Challenging Established Classifications and Redefining Diagnostics with Precision Oncology
2.2. Guiding Compass for Tumor-Agnostic Tumors
2.2.1. Neurotrophic Tyrosine Receptor Kinase (NTRK) Fusion-Positive
2.2.2. Rearranged During Transfection (RET) Fusion-Positive Cancers
2.2.3. Von Hippel–Lindau Disease
2.2.4. Human Epidermal Growth Factor Receptor 2-Positive (Her2-Positive) Tumors
2.2.5. BRAF V600E-Mutated Cancers
2.2.6. High Mutational Burden Tumors
2.2.7. Mismatch Repair Deficient (dMMR)/High Microsatellite Instability (MSI-H) Cancers
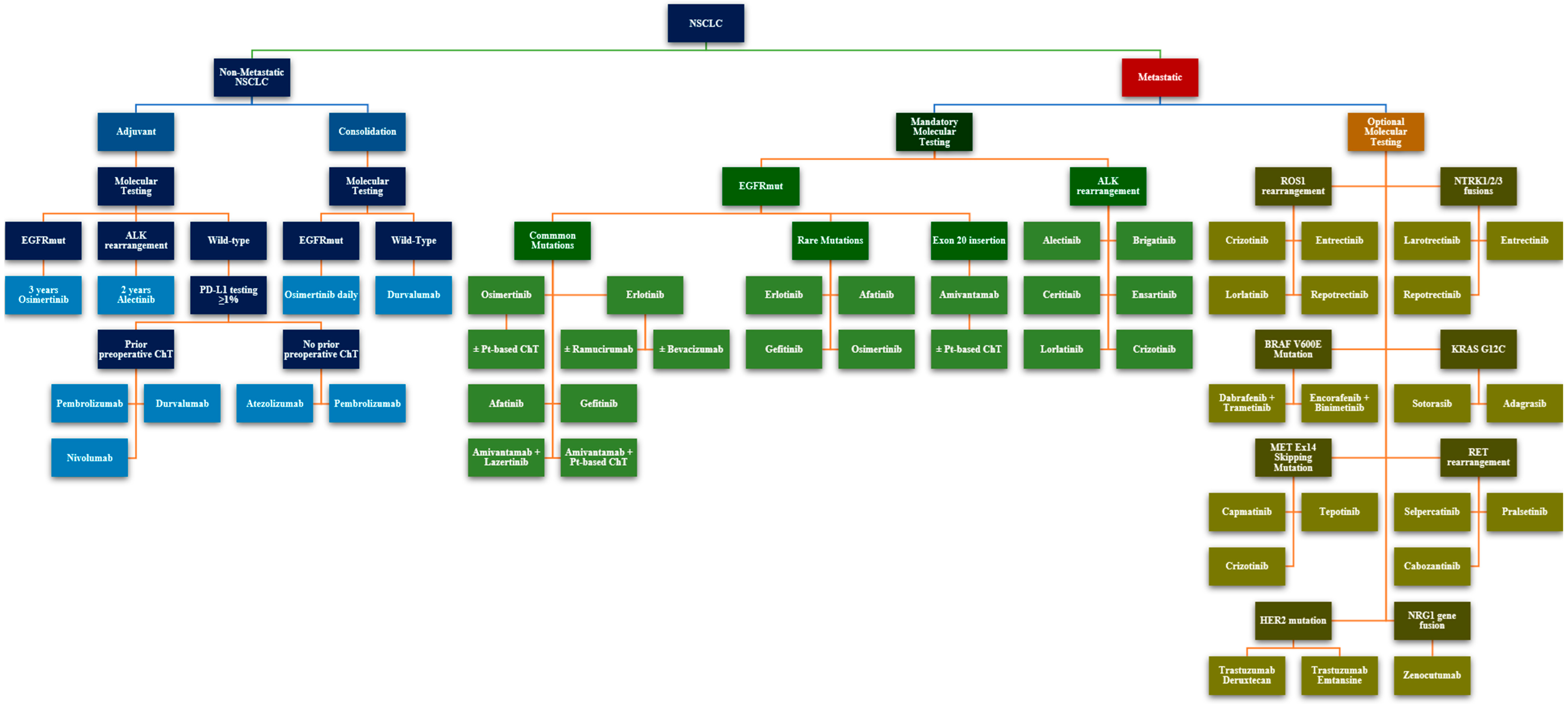
2.3. The Oncogenic Driver Landscape in NSCLC
2.4. Investigating Homologous Repair Deficiencies—Treatment Avenues and Hereditary Cancer Risk Evaluation
2.5. Bridging the Hormone–Chemotherapy Gap in HR-Positive Advanced Breast Cancer
3. Discussion
4. Conclusions
5. Future Directions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AE | Adverse Events |
| ALK | Anaplastic Lymphoma Kinase |
| BRAF | B-Raf Proto-Oncogene |
| BRCA1/2 | Breast Cancer Gene 1/2 |
| CDK4/CDK6 | Cyclin-Dependent Kinases 4 and 6 |
| cfDNA | Circulating Free DNA |
| ChT | Chemotherapy |
| CI | Confidence Interval |
| CNS | Central Nervous System |
| CRC | Colorectal Cancer |
| DFS | Disease-Free Survival |
| dMMR | Deficient Mismatch Repair |
| DoR | Duration of Response |
| EGFR | Epidermal Growth Factor Receptor |
| ER | Estrogen Receptor |
| ERBB2 (HER2) | Erb-B2 Receptor Tyrosine Kinase 2 (also known as HER2) |
| ERBB3 | Erb-B2 Receptor Tyrosine Kinase 3 |
| ESCAT | European Society for Medical Oncology Scale for Clinical Actionability of Molecular Targets |
| ESR1 | Estrogen Receptor 1 |
| FFPE | Formalin-Fixed, Paraffin-Embedded |
| FISH | Fluorescence In Situ Hybridization |
| FGFR1/2/3 | Fibroblast Growth Factor Receptor 1, 2, and 3 |
| HER2 | Human Epidermal Growth Factor Receptor 2 |
| HR | Hazard Ratio |
| HR+ | Hormone Receptor-Positive |
| HRD | Homologous Recombination Deficiency |
| HRR | Homologous Recombination Repair |
| IHC | Immunohistochemistry |
| KIT | KIT Proto-Oncogene, Receptor Tyrosine Kinase |
| KRAS | Kirsten Rat Sarcoma Viral Oncogene |
| mDoR | Median Duration of Response |
| mDoT | Median Duration of Therapy |
| MET | MET Proto-Oncogene |
| MLH1 | MutL Homolog 1 |
| mOS | Median Overall Survival |
| mPFS | Median Progression-Free Survival |
| MPR | Major Pathological Response |
| MSI | Microsatellite Instability |
| MSI-H | Microsatellite Instability-High |
| MTC | Medullary Thyroid Carcinoma |
| mut/Mb | Mutations per Megabase |
| NCCN | National Comprehensive Cancer Network |
| NGS | Next-Generation Sequencing |
| NR | Not Reached |
| NTRK | Neurotrophic Tyrosine Receptor Kinase |
| NSCLC | Non-Small Cell Lung Cancer |
| ORR | Objective Response Rate |
| OS | Overall Survival |
| PARPi | Poly (ADP-ribose) Polymerase Inhibitor |
| PD | Progressive Disease |
| PD-1 | Programmed Death-1 |
| PDGFRA | Platelet-Derived Growth Factor Receptor Alpha |
| PFS | Progression-Free Survival |
| PIK3CA | Phosphatidylinositol-4,5-Bisphosphate 3-Kinase Catalytic Subunit Alpha |
| PTC | Papillary Thyroid Carcinoma |
| PTEN | Phosphatase and Tensin Homolog |
| q3w | Every 3 Weeks |
| RET | Rearranged During Transfection |
| ROS1 | ROS Proto-Oncogene 1 |
| RT | Radiotherapy |
| SCLC | Small Cell Lung Cancer |
| SoC | Standard of Care |
| TMB | Tumour Mutational Burden |
| TKI | Tyrosine Kinase Inhibitor |
| TME | Total Mesorectal Excision |
| TRKA/B/C | Tropomyosin Receptor Kinase A/B/C |
| TSC1/2 | Tuberous Sclerosis Complex 1 and 2 |
| VHL | Von Hippel–Lindau |
References
- Targeted Therapy Drug List by Cancer Type—NCI. Available online: https://www.cancer.gov/about-cancer/treatment/types/targeted-therapies/approved-drug-list (accessed on 14 December 2024).
- Schwartzberg, L.; Kim, E.S.; Liu, D.; Schrag, D. Precision Oncology: Who, How, What, When, and When Not? In American Society of Clinical Oncology Educational Book; American Society of Clinical Oncology: Alexandria, VA, USA, 2024. [Google Scholar]
- Satam, H.; Joshi, K.; Mangrolia, U.; Waghoo, S.; Zaidi, G.; Rawool, S.; Thakare, R.P.; Banday, S.; Mishra, A.K.; Das, G.; et al. Next-Generation Sequencing Technology: Current Trends and Advancements. Biology 2023, 12, 997. [Google Scholar] [CrossRef] [PubMed]
- Galeș, L.N.; Păun, M.-A.; Anghel, R.M.; Trifănescu, O.G. Cancer Screening: Present Recommendations, the Development of Multi-Cancer Early Development Tests, and the Prospect of Universal Cancer Screening. Cancers 2024, 16, 1191. [Google Scholar] [CrossRef]
- Milbury, C.A.; Creeden, J.; Yip, W.-K.; Smith, D.L.; Pattani, V.; Maxwell, K.; Sawchyn, B.; Gjoerup, O.; Meng, W.; Skoletsky, J.; et al. Clinical and Analytical Validation of FoundationOne®CDx, a Comprehensive Genomic Profiling Assay for Solid Tumors. PLoS ONE 2022, 17, e0264138. [Google Scholar] [CrossRef]
- Takeda, M.; Takahama, T.; Sakai, K.; Shimizu, S.; Watanabe, S.; Kawakami, H.; Tanaka, K.; Sato, C.; Hayashi, H.; Nonagase, Y.; et al. Clinical Application of the FoundationOne CDx Assay to Therapeutic Decision-Making for Patients with Advanced Solid Tumors. Oncologist 2021, 26, e588–e596. [Google Scholar] [CrossRef]
- Woodhouse, R.; Li, M.; Hughes, J.; Delfosse, D.; Skoletsky, J.; Ma, P.; Meng, W.; Dewal, N.; Milbury, C.; Clark, T.; et al. Clinical and Analytical Validation of FoundationOne Liquid CDx, a Novel 324-Gene cfDNA-Based Comprehensive Genomic Profiling Assay for Cancers of Solid Tumor Origin. PLoS ONE 2020, 15, e0237802. [Google Scholar] [CrossRef]
- Bauml, J.M.; Li, B.T.; Velcheti, V.; Govindan, R.; Curioni-Fontecedro, A.; Dooms, C.; Takahashi, T.; Duda, A.W.; Odegaard, J.I.; Cruz-Guilloty, F.; et al. Clinical Validation of Guardant360 CDx as a Blood-Based Companion Diagnostic for Sotorasib. Lung Cancer Amst. Neth. 2022, 166, 270–278. [Google Scholar] [CrossRef]
- Cheng, D.T.; Prasad, M.; Chekaluk, Y.; Benayed, R.; Sadowska, J.; Zehir, A.; Syed, A.; Wang, Y.E.; Somar, J.; Li, Y.; et al. Comprehensive Detection of Germline Variants by MSK-IMPACT, a Clinical Diagnostic Platform for Solid Tumor Molecular Oncology and Concurrent Cancer Predisposition Testing. BMC Med. Genom. 2017, 10, 33. [Google Scholar] [CrossRef]
- Saito, A.; Terai, H.; Kim, T.; Emoto, K.; Kawano, R.; Nakamura, K.; Hayashi, H.; Takaoka, H.; Ogata, A.; Kinoshita, K.; et al. Clinical Utility of the Oncomine Dx Target Test multi-CDx System and the Possibility of Utilizing Those Original Sequence Data. Cancer Med. 2024, 13, e7077. [Google Scholar] [CrossRef]
- Dumur, C.I.; Krishnan, R.; Almenara, J.A.; Brown, K.E.; Dugan, K.R.; Farni, C.; Ibrahim, F.Z.; Sanchez, N.A.; Rathore, S.; Pradhan, D.; et al. Analytical Validation and Clinical Utilization of the Oncomine Comprehensive Assay Plus Panel for Comprehensive Genomic Profiling in Solid Tumors. J. Mol. Pathol. 2023, 4, 109–127. [Google Scholar] [CrossRef]
- Beaubier, N.; Tell, R.; Lau, D.; Parsons, J.R.; Bush, S.; Perera, J.; Sorrells, S.; Baker, T.; Chang, A.; Michuda, J.; et al. Clinical Validation of the Tempus xT Next-Generation Targeted Oncology Sequencing Assay. Oncotarget 2019, 10, 2384–2396. [Google Scholar] [CrossRef]
- Carter, P.; Alifrangis, C.; Cereser, B.; Chandrasinghe, P.; Del Bel Belluz, L.; Moderau, N.; Poyia, F.; Schwartzberg, L.S.; Tabassum, N.; Wen, J.; et al. Molecular Profiling of Advanced Breast Cancer Tumors Is Beneficial in Assisting Clinical Treatment Plans. Oncotarget 2018, 9, 17589–17596. [Google Scholar] [CrossRef] [PubMed]
- Mosele, M.F.; Westphalen, C.B.; Stenzinger, A.; Barlesi, F.; Bayle, A.; Bièche, I.; Bonastre, J.; Castro, E.; Dienstmann, R.; Krämer, A.; et al. Recommendations for the Use of Next-Generation Sequencing (NGS) for Patients with Advanced Cancer in 2024: A Report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2024, 35, 588–606. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, D.; Johnson, A.; Sklar, J.; Lindeman, N.I.; Moore, K.; Ganesan, S.; Lovly, C.M.; Perlmutter, J.; Gray, S.W.; Hwang, J.; et al. Somatic Genomic Testing in Patients with Metastatic or Advanced Cancer: ASCO Provisional Clinical Opinion. J. Clin. Oncol. 2022, 40, 1231–1258. [Google Scholar] [CrossRef] [PubMed]
- Trifănescu, O.G.; Trifănescu, R.A.; Mitrică, R.; Mitrea, D.; Ciornei, A.; Georgescu, M.; Butnariu, I.; Galeș, L.N.; Șerbănescu, L.; Anghel, R.M.; et al. Upstaging and Downstaging in Gliomas-Clinical Implications for the Fifth Edition of the World Health Organization Classification of Tumors of the Central Nervous System. Diagnostics 2023, 13, 197. [Google Scholar] [CrossRef]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO Guidelines on the Diagnosis and Treatment of Diffuse Gliomas of Adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186. [Google Scholar] [CrossRef]
- Nannini, M.; Rizzo, A.; Indio, V.; Schipani, A.; Astolfi, A.; Pantaleo, M.A. Targeted Therapy in SDH-Deficient GIST. Ther. Adv. Med. Oncol. 2021, 13, 17588359211023278. [Google Scholar] [CrossRef] [PubMed]
- Radu, P.; Zurzu, M.; Paic, V.; Bratucu, M.; Garofil, D.; Tigora, A.; Georgescu, V.; Prunoiu, V.; Popa, F.; Surlin, V.; et al. Interstitial Cells of Cajal—Origin, Distribution and Relationship with Gastrointestinal Tumors. Medicina 2023, 59, 63. [Google Scholar] [CrossRef]
- Sun, Y.; Yue, L.; Xu, P.; Hu, W. An Overview of Agents and Treatments for PDGFRA-Mutated Gastrointestinal Stromal Tumors. Front. Oncol. 2022, 12, 927587. [Google Scholar] [CrossRef]
- Flaherty, K.T.; Le, D.T.; Lemery, S. Tissue-Agnostic Drug Development. In American Society of Clinical Oncology Educational Book; American Society of Clinical Oncology: Alexandria, VA, USA, 2025. [Google Scholar]
- Subbiah, V.; Gouda, M.A.; Ryll, B.; Burris, H.A.; Kurzrock, R. The Evolving Landscape of Tissue-agnostic Therapies in Precision Oncology. CA. Cancer J. Clin. 2024, 74, 433–452. [Google Scholar] [CrossRef]
- Coquerelle, S.; Darlington, M.; Michel, M.; Durand, M.; Borget, I.; Baffert, S.; Marino, P.; Perrier, L.; Durand-Zaleski, I. Impact of Next Generation Sequencing on Clinical Practice in Oncology in France: Better Genetic Profiles for Patients Improve Access to Experimental Treatments. Value Health 2020, 23, 898–906. [Google Scholar] [CrossRef]
- Park, J.J.H.; Hsu, G.; Siden, E.G.; Thorlund, K.; Mills, E.J. An Overview of Precision Oncology Basket and Umbrella Trials for Clinicians. CA Cancer J. Clin. 2020, 70, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Popat, S.; Ramagopalan, S.V.; Ray, J.; Roze, S.; Subbiah, V. Assessment of Tumour-Agnostic Therapies in Basket Trials. Lancet Oncol. 2022, 23, e7. [Google Scholar] [CrossRef]
- Lengliné, E.; Peron, J.; Vanier, A.; Gueyffier, F.; Kouzan, S.; Dufour, P.; Guillot, B.; Blondon, H.; Clanet, M.; Cochat, P.; et al. Basket Clinical Trial Design for Targeted Therapies for Cancer: A French National Authority for Health Statement for Health Technology Assessment. Lancet Oncol. 2021, 22, e430–e434. [Google Scholar] [CrossRef]
- Gouda, M.A.; Nelson, B.E.; Buschhorn, L.; Wahida, A.; Subbiah, V. Tumor-Agnostic Precision Medicine from the AACR GENIE Database: Clinical Implications. Clin. Cancer Res. 2023, 29, 2753–2760. [Google Scholar] [CrossRef] [PubMed]
- Drilon, A.; Laetsch, T.W.; Kummar, S.; DuBois, S.G.; Lassen, U.N.; Demetri, G.D.; Nathenson, M.; Doebele, R.C.; Farago, A.F.; Pappo, A.S.; et al. Efficacy of Larotrectinib in TRK Fusion–Positive Cancers in Adults and Children. N. Engl. J. Med. 2018, 378, 731–739. [Google Scholar] [CrossRef] [PubMed]
- Laetsch, T.W.; DuBois, S.G.; Mascarenhas, L.; Turpin, B.; Federman, N.; Albert, C.M.; Nagasubramanian, R.; Davis, J.L.; Rudzinski, E.; Feraco, A.M.; et al. Larotrectinib for Paediatric Solid Tumours Harbouring NTRK Gene Fusions: A Multicentre, Open-Label, Phase 1 Study. Lancet Oncol. 2018, 19, 705–714. [Google Scholar] [CrossRef]
- Brose, M.S.; Westphalen, C.B.; Kehl, K.L.; Pan, X.; Bernard-Gauthier, V.; Kurtinecz, M.; Guo, H.; Aris, V.; Brett, N.R.; Majdi, A.; et al. Outcomes of Larotrectinib Compared with Real-World Data from Non-TRK Inhibitor Therapies in Patients with TRK Fusion Cancer: VICTORIA Study. J. Clin. Oncol. 2024, 42, 3105. [Google Scholar] [CrossRef]
- Drilon, A.; Siena, S.; Ou, S.-H.I.; Patel, M.; Ahn, M.J.; Lee, J.; Bauer, T.M.; Farago, A.F.; Wheler, J.J.; Liu, S.V.; et al. Safety and Antitumor Activity of the Multi-Targeted Pan-TRK, ROS1, and ALK Inhibitor Entrectinib (RXDX-101): Combined Results from Two Phase 1 Trials (ALKA-372-001 and STARTRK-1). Cancer Discov. 2017, 7, 400–409. [Google Scholar] [CrossRef]
- Doebele, R.C.; Drilon, A.; Paz-Ares, L.; Siena, S.; Shaw, A.T.; Farago, A.F.; Blakely, C.M.; Seto, T.; Cho, B.C.; Tosi, D.; et al. Entrectinib in Patients with Advanced or Metastatic NTRK Fusion-Positive Solid Tumours: Integrated Analysis of Three Phase 1–2 Trials. Lancet Oncol. 2020, 21, 271–282. [Google Scholar] [CrossRef]
- Desai, A.V.; Robinson, G.W.; Gauvain, K.; Basu, E.M.; Macy, M.E.; Maese, L.; Whipple, N.S.; Sabnis, A.J.; Foster, J.H.; Shusterman, S.; et al. Entrectinib in Children and Young Adults with Solid or Primary CNS Tumors Harboring NTRK, ROS1, or ALK Aberrations (STARTRK-NG). Neuro-Oncology 2022, 24, 1776–1789. [Google Scholar] [CrossRef]
- Drilon, A.; Camidge, D.R.; Lin, J.J.; Kim, S.-W.; Solomon, B.J.; Dziadziuszko, R.; Besse, B.; Goto, K.; De Langen, A.J.; Wolf, J.; et al. Repotrectinib in ROS1 Fusion–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2024, 390, 118–131. [Google Scholar] [CrossRef]
- Subbiah, V.; Wolf, J.; Konda, B.; Kang, H.; Spira, A.; Weiss, J.; Takeda, M.; Ohe, Y.; Khan, S.; Ohashi, K.; et al. Tumour-Agnostic Efficacy and Safety of Selpercatinib in Patients with RET Fusion-Positive Solid Tumours Other than Lung or Thyroid Tumours (LIBRETTO-001): A Phase 1/2, Open-Label, Basket Trial. Lancet Oncol. 2022, 23, 1261–1273. [Google Scholar] [CrossRef] [PubMed]
- Wirth, L.J.; Brose, M.S.; Subbiah, V.; Worden, F.; Solomon, B.; Robinson, B.; Hadoux, J.; Tomasini, P.; Weiler, D.; Deschler-Baier, B.; et al. Durability of Response with Selpercatinib in Patients with RET-Activated Thyroid Cancer: Long-Term Safety and Efficacy From LIBRETTO-001. J. Clin. Oncol. 2024, 42, 3187–3195. [Google Scholar] [CrossRef] [PubMed]
- Drilon, A.; Subbiah, V.; Gautschi, O.; Tomasini, P.; de Braud, F.; Solomon, B.J.; Shao-Weng Tan, D.; Alonso, G.; Wolf, J.; Park, K.; et al. Selpercatinib in Patients with RET Fusion–Positive Non–Small-Cell Lung Cancer: Updated Safety and Efficacy from the Registrational LIBRETTO-001 Phase I/II Trial. J. Clin. Oncol. 2023, 41, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Subbiah, V.; Cassier, P.A.; Siena, S.; Garralda, E.; Paz-Ares, L.; Garrido, P.; Nadal, E.; Vuky, J.; Lopes, G.; Kalemkerian, G.P.; et al. Pan-Cancer Efficacy of Pralsetinib in Patients with RET Fusion–Positive Solid Tumors from the Phase 1/2 ARROW Trial. Nat. Med. 2022, 28, 1640–1645. [Google Scholar] [CrossRef]
- Griesinger, F.; Curigliano, G.; Thomas, M.; Subbiah, V.; Baik, C.S.; Tan, D.S.W.; Lee, D.H.; Misch, D.; Garralda, E.; Kim, D.-W.; et al. Safety and Efficacy of Pralsetinib in RET Fusion–Positive Non-Small-Cell Lung Cancer Including as First-Line Therapy: Update from the ARROW Trial. Ann. Oncol. 2022, 33, 1168–1178. [Google Scholar] [CrossRef]
- Gainor, J.F.; Curigliano, G.; Kim, D.-W.; Lee, D.H.; Besse, B.; Baik, C.S.; Doebele, R.C.; Cassier, P.A.; Lopes, G.; Tan, D.S.W.; et al. Pralsetinib for RET Fusion-Positive Non-Small-Cell Lung Cancer (ARROW): A Multi-Cohort, Open-Label, Phase 1/2 Study. Lancet Oncol. 2021, 22, 959–969. [Google Scholar] [CrossRef]
- Subbiah, V.; Hu, M.I.; Wirth, L.J.; Schuler, M.; Mansfield, A.S.; Curigliano, G.; Brose, M.S.; Zhu, V.W.; Leboulleux, S.; Bowles, D.W.; et al. Pralsetinib for Patients with Advanced or Metastatic RET-Altered Thyroid Cancer (ARROW): A Multi-Cohort, Open-Label, Registrational, Phase 1/2 Study. Lancet Diabetes Endocrinol. 2021, 9, 491–501. [Google Scholar] [CrossRef]
- Lannon, C.L.; Sorensen, P.H.B. ETV6–NTRK3: A Chimeric Protein Tyrosine Kinase with Transformation Activity in Multiple Cell Lineages. Semin. Cancer Biol. 2005, 15, 215–223. [Google Scholar] [CrossRef]
- Pulciani, S.; Santos, E.; Lauver, A.V.; Long, L.K.; Aaronson, S.A.; Barbacid, M. Oncogenes in Solid Human Tumours. Nature 1982, 300, 539–542. [Google Scholar] [CrossRef]
- Ruiz-Cordero, R.; Ng, D.L. Neurotrophic Receptor Tyrosine Kinase (NTRK) Fusions and Their Role in Cancer. Cancer Cytopathol. 2020, 128, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Doebele, R.C.; Davis, L.E.; Vaishnavi, A.; Le, A.T.; Estrada-Bernal, A.; Keysar, S.; Jimeno, A.; Varella-Garcia, M.; Aisner, D.L.; Li, Y.; et al. An Oncogenic NTRK Fusion in a Soft Tissue Sarcoma Patient with Response to the Tropomyosin-Related Kinase (TRK) Inhibitor LOXO-101. Cancer Discov. 2015, 5, 1049–1057. [Google Scholar] [CrossRef]
- Menichincheri, M.; Ardini, E.; Magnaghi, P.; Avanzi, N.; Banfi, P.; Bossi, R.; Buffa, L.; Canevari, G.; Ceriani, L.; Colombo, M.; et al. Correction to Discovery of Entrectinib: A New 3-Aminoindazole as a Potent Anaplastic Lymphoma Kinase (ALK), c-Ros Oncogene 1 Kinase (ROS1), and Pan-Tropomyosin Receptor Kinases (Pan-TRKs) Inhibitor. J. Med. Chem. 2019, 62, 8364. [Google Scholar] [CrossRef]
- Demetri, G.D.; De Braud, F.; Drilon, A.; Siena, S.; Patel, M.R.; Cho, B.C.; Liu, S.V.; Ahn, M.-J.; Chiu, C.-H.; Lin, J.J.; et al. Updated Integrated Analysis of the Efficacy and Safety of Entrectinib in Patients with NTRK Fusion-Positive Solid Tumors. Clin. Cancer Res. 2022, 28, 1302–1312. [Google Scholar] [CrossRef] [PubMed]
- Chi, X.; Michos, O.; Shakya, R.; Riccio, P.; Enomoto, H.; Licht, J.D.; Asai, N.; Takahashi, M.; Ohgami, N.; Kato, M.; et al. Ret-Dependent Cell Rearrangements in the Wolffian Duct Epithelium Initiate Ureteric Bud Morphogenesis. Dev. Cell 2009, 17, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Enomoto, H.; Crawford, P.A.; Gorodinsky, A.; Heuckeroth, R.O.; Johnson, E.M.; Milbrandt, J. RET Signaling Is Essential for Migration, Axonal Growth and Axon Guidance of Developing Sympathetic Neurons. Dev. Camb. Engl. 2001, 128, 3963–3974. [Google Scholar] [CrossRef]
- Enomoto, H.; Heuckeroth, R.O.; Golden, J.P.; Johnson, E.M.; Milbrandt, J. Development of Cranial Parasympathetic Ganglia Requires Sequential Actions of GDNF and Neurturin. Dev. Camb. Engl. 2000, 127, 4877–4889. [Google Scholar] [CrossRef]
- Pachnis, V.; Mankoo, B.; Costantini, F. Expression of the C-Ret Proto-Oncogene during Mouse Embryogenesis. Development 1993, 119, 1005–1017. [Google Scholar] [CrossRef]
- Trupp, M.; Rydén, M.; Jörnvall, H.; Funakoshi, H.; Timmusk, T.; Arenas, E.; Ibáñez, C.F. Peripheral Expression and Biological Activities of GDNF, a New Neurotrophic Factor for Avian and Mammalian Peripheral Neurons. J. Cell Biol. 1995, 130, 137–148. [Google Scholar]
- Regua, A.T.; Najjar, M.; Lo, H.-W. RET Signaling Pathway and RET Inhibitors in Human Cancer. Front. Oncol. 2022, 12, 932353. [Google Scholar] [CrossRef]
- Grieco, M.; Santoro, M.; Berlingieri, M.T.; Melillo, R.M.; Donghi, R.; Bongarzone, I.; Pierotti, M.A.; Della Ports, G.; Fusco, A.; Vecchiot, G. PTC Is a Novel Rearranged Form of the Ret Proto-Oncogene and Is Frequently Detected in Vivo in Human Thyroid Papillary Carcinomas. Cell 1990, 60, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Ou, S.-H.I.; Zhu, V.W. Catalog of 5′ Fusion Partners in RET+ NSCLC Circa 2020. JTO Clin. Res. Rep. 2020, 1, 100037. [Google Scholar] [CrossRef]
- Subbiah, V.; Velcheti, V.; Tuch, B.B.; Ebata, K.; Busaidy, N.L.; Cabanillas, M.E.; Wirth, L.J.; Stock, S.; Smith, S.; Lauriault, V.; et al. Selective RET Kinase Inhibition for Patients with RET-Altered Cancers. Ann. Oncol. 2018, 29, 1869–1876. [Google Scholar] [CrossRef] [PubMed]
- Jonasch, E.; Iliopoulos, O.; Rathmell, W.K.; Narayan, V.; Maughan, B.L.; Oudard, S.; Else, T.; Maranchie, J.K.; Welsh, S.J.; Iversen, A.B.B.; et al. LITESPARK-004 (MK-6482-004) Phase 2 Study of Belzutifan, an Oral Hypoxia-Inducible Factor 2α Inhibitor (HIF-2α), for von Hippel-Lindau (VHL) Disease: Update with More than Two Years of Follow-up Data. J. Clin. Oncol. 2022, 40, 4546–4546. [Google Scholar] [CrossRef]
- Else, T.; Jonasch, E.; Iliopoulos, O.; Beckermann, K.E.; Narayan, V.; Maughan, B.L.; Oudard, S.; Maranchie, J.K.; Iversen, A.B.; Goldberg, C.M.; et al. Belzutifan for von Hippel–Lindau Disease: Pancreatic Lesion Population of the Phase 2 LITESPARK-004 Study. Clin. Cancer Res. 2024, 30, 1750–1757. [Google Scholar] [CrossRef]
- Iliopoulos, O.; Iversen, A.B.; Narayan, V.; Maughan, B.L.; Beckermann, K.E.; Oudard, S.; Else, T.; Maranchie, J.K.; Goldberg, C.M.; Fu, W.; et al. Belzutifan for Patients with von Hippel-Lindau Disease-Associated CNS Haemangioblastomas (LITESPARK-004): A Multicentre, Single-Arm, Phase 2 Study. Lancet Oncol. 2024, 25, 1325–1336. [Google Scholar] [CrossRef]
- Jonasch, E.; Donskov, F.; Iliopoulos, O.; Rathmell, W.K.; Narayan, V.K.; Maughan, B.L.; Oudard, S.; Else, T.; Maranchie, J.K.; Welsh, S.J.; et al. Belzutifan for Renal Cell Carcinoma in von Hippel–Lindau Disease. N. Engl. J. Med. 2021, 385, 2036–2046. [Google Scholar] [CrossRef]
- Curry, L.; Soleimani, M. Belzutifan: A Novel Therapeutic for the Management of von Hippel–Lindau Disease and Beyond. Future Oncol. 2024, 20, 1251–1266. [Google Scholar] [CrossRef]
- Rubin, I.; Yarden, Y. The Basic Biology of HER2. Ann. Oncol. 2001, 12, S3–S8. [Google Scholar] [CrossRef]
- Cho, H.-S.; Mason, K.; Ramyar, K.X.; Stanley, A.M.; Gabelli, S.B.; Denney, D.W.; Leahy, D.J. Structure of the Extracellular Region of HER2 Alone and in Complex with the Herceptin Fab. Nature 2003, 421, 756–760. [Google Scholar] [CrossRef]
- Xia, X.; Gong, C.; Zhang, Y.; Xiong, H. The History and Development of HER2 Inhibitors. Pharmaceuticals 2023, 16, 1450. [Google Scholar] [CrossRef]
- Kallioniemi, O.P.; Kallioniemi, A.; Kurisu, W.; Thor, A.; Chen, L.C.; Smith, H.S.; Waldman, F.M.; Pinkel, D.; Gray, J.W. ERBB2 Amplification in Breast Cancer Analyzed by Fluorescence in Situ Hybridization. Proc. Natl. Acad. Sci. USA 1992, 89, 5321–5325. [Google Scholar] [PubMed]
- Citri, A.; Yarden, Y. EGF–ERBB Signalling: Towards the Systems Level. Nat. Rev. Mol. Cell Biol. 2006, 7, 505–516. [Google Scholar] [CrossRef]
- Yarden, Y. Biology of HER2 and Its Importance in Breast Cancer. Oncology 2001, 61, 1–13. [Google Scholar] [CrossRef]
- Yarden, Y.; Sliwkowski, M.X. Untangling the ErbB Signalling Network. Nat. Rev. Mol. Cell Biol. 2001, 2, 127–137. [Google Scholar] [CrossRef]
- Bazley, L.A.; Gullick, W.J. The Epidermal Growth Factor Receptor Family. Endocr. Relat. Cancer 2005, 12, S17–S27. [Google Scholar] [CrossRef] [PubMed]
- Moasser, M.M. The Oncogene HER2: Its Signaling and Transforming Functions and Its Role in Human Cancer Pathogenesis. Oncogene 2007, 26, 6469–6487. [Google Scholar] [CrossRef] [PubMed]
- Graus-Porta, D.; Beerli, R.R.; Daly, J.M.; Hynes, N.E. ErbB-2, the Preferred Heterodimerization Partner of All ErbB Receptors, Is a Mediator of Lateral Signaling. EMBO J. 1997, 16, 1647–1655. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Makker, V.; Oaknin, A.; Oh, D.-Y.; Banerjee, S.; González-Martín, A.; Jung, K.H.; Ługowska, I.; Manso, L.; Manzano, A.; et al. Efficacy and Safety of Trastuzumab Deruxtecan in Patients with HER2-Expressing Solid Tumors: Primary Results From the DESTINY-PanTumor02 Phase II Trial. J. Clin. Oncol. 2024, 42, 47–58. [Google Scholar] [CrossRef]
- Sweeney, C.J.; Hainsworth, J.D.; Bose, R.; Burris, H.A.; Kurzrock, R.; Swanton, C.; Friedman, C.F.; Spigel, D.R.; Szado, T.; Schulze, K.; et al. MyPathway Human Epidermal Growth Factor Receptor 2 Basket Study: Pertuzumab + Trastuzumab Treatment of a Tissue-Agnostic Cohort of Patients with Human Epidermal Growth Factor Receptor 2–Altered Advanced Solid Tumors. J. Clin. Oncol. 2024, 42, 258–265. [Google Scholar] [CrossRef]
- Gouda, M.A.; Subbiah, V. Precision Oncology for BRAF-Mutant Cancers with BRAF and MEK Inhibitors: From Melanoma to Tissue-Agnostic Therapy. ESMO Open 2023, 8, 100788. [Google Scholar] [CrossRef] [PubMed]
- Wellbrock, C.; Karasarides, M.; Marais, R. The RAF Proteins Take Centre Stage. Nat. Rev. Mol. Cell Biol. 2004, 5, 875–885. [Google Scholar] [CrossRef]
- Pearson, G.; Robinson, F.; Beers Gibson, T.; Xu, B.; Karandikar, M.; Berman, K.; Cobb, M.H. Mitogen-Activated Protein (MAP) Kinase Pathways: Regulation and Physiological Functions. Endocr. Rev. 2001, 22, 153–183. [Google Scholar] [CrossRef] [PubMed]
- Dankner, M.; Rose, A.A.N.; Rajkumar, S.; Siegel, P.M.; Watson, I.R. Classifying BRAF Alterations in Cancer: New Rational Therapeutic Strategies for Actionable Mutations. Oncogene 2018, 37, 3183–3199. [Google Scholar] [CrossRef] [PubMed]
- Yaeger, R.; Corcoran, R.B. Targeting Alterations in the RAF–MEK Pathway. Cancer Discov. 2019, 9, 329–341. [Google Scholar] [CrossRef]
- Zhao, J.; Liu, P.; Yu, Y.; Zhi, J.; Zheng, X.; Yu, J.; Gao, M. Comparison of Diagnostic Methods for the Detection of a BRAF Mutation in Papillary Thyroid Cancer. Oncol. Lett. 2019, 17, 4661–4666. [Google Scholar] [CrossRef]
- Cheng, L.; Lopez-Beltran, A.; Massari, F.; MacLennan, G.T.; Montironi, R. Molecular Testing for BRAF Mutations to Inform Melanoma Treatment Decisions: A Move toward Precision Medicine. Mod. Pathol. 2018, 31, 24–38. [Google Scholar] [CrossRef]
- Szymonek, M.; Kowalik, A.; Kopczyński, J.; Gąsior-Perczak, D.; Pałyga, I.; Walczyk, A.; Gadawska-Juszczyk, K.; Płusa, A.; Mężyk, R.; Chrapek, M.; et al. Immunohistochemistry Cannot Replace DNA Analysis for Evaluation of BRAF V600E Mutations in Papillary Thyroid Carcinoma. Oncotarget 2017, 8, 74897–74909. [Google Scholar] [CrossRef]
- Kwon, J.-H.; Jeong, B.-K.; Yoon, Y.S.; Yu, C.S.; Kim, J. Utility of BRAF VE1 Immunohistochemistry as a Screening Tool for Colorectal Cancer Harboring BRAF V600E Mutation. J. Pathol. Transl. Med. 2018, 52, 157–163. [Google Scholar] [CrossRef]
- Chakravarty, D.; Gao, J.; Phillips, S.; Kundra, R.; Zhang, H.; Wang, J.; Rudolph, J.E.; Yaeger, R.; Soumerai, T.; Nissan, M.H.; et al. OncoKB: A Precision Oncology Knowledge Base. JCO Precis. Oncol. 2017, 1, 1–16. [Google Scholar] [CrossRef]
- Subbiah, V.; Kreitman, R.J.; Wainberg, Z.A.; Cho, J.Y.; Schellens, J.H.M.; Soria, J.C.; Wen, P.Y.; Zielinski, C.; Cabanillas, M.E.; Urbanowitz, G.; et al. Dabrafenib and Trametinib Treatment in Patients with Locally Advanced or Metastatic BRAF V600–Mutant Anaplastic Thyroid Cancer. J. Clin. Oncol. 2018, 36, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Subbiah, V.; Kreitman, R.J.; Wainberg, Z.A.; Cho, J.Y.; Schellens, J.H.M.; Soria, J.C.; Wen, P.Y.; Zielinski, C.C.; Cabanillas, M.E.; Boran, A.; et al. Dabrafenib plus Trametinib in Patients with BRAF V600E-Mutant Anaplastic Thyroid Cancer: Updated Analysis from the Phase II ROAR Basket Study. Ann. Oncol. 2022, 33, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Subbiah, V.; Lassen, U.; Élez, E.; Italiano, A.; Curigliano, G.; Javle, M.; De Braud, F.; Prager, G.W.; Greil, R.; Stein, A.; et al. Dabrafenib plus Trametinib in Patients with BRAFV600E-Mutated Biliary Tract Cancer (ROAR): A Phase 2, Open-Label, Single-Arm, Multicentre Basket Trial. Lancet Oncol. 2020, 21, 1234–1243. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Stein, A.; Van Den Bent, M.; De Greve, J.; Wick, A.; De Vos, F.Y.F.L.; Von Bubnoff, N.; Van Linde, M.E.; Lai, A.; Prager, G.W.; et al. Dabrafenib plus Trametinib in Patients with BRAFV600E-Mutant Low-Grade and High-Grade Glioma (ROAR): A Multicentre, Open-Label, Single-Arm, Phase 2, Basket Trial. Lancet Oncol. 2022, 23, 53–64. [Google Scholar] [CrossRef]
- Kreitman, R.J.; Moreau, P.; Ravandi, F.; Hutchings, M.; Gazzah, A.; Michallet, A.-S.; Wainberg, Z.A.; Stein, A.; Dietrich, S.; de Jonge, M.J.A.; et al. Dabrafenib plus Trametinib in Patients with Relapsed/Refractory BRAF V600E Mutation–Positive Hairy Cell Leukemia. Blood 2023, 141, 996–1006. [Google Scholar] [CrossRef]
- Fusco, M.J.; West, H.; Walko, C.M. Tumor Mutation Burden and Cancer Treatment. JAMA Oncol. 2021, 7, 316. [Google Scholar] [CrossRef]
- Galuppini, F.; Dal Pozzo, C.A.; Deckert, J.; Loupakis, F.; Fassan, M.; Baffa, R. Tumor Mutation Burden: From Comprehensive Mutational Screening to the Clinic. Cancer Cell Int. 2019, 19, 209. [Google Scholar] [CrossRef] [PubMed]
- Subbiah, V.; Solit, D.B.; Chan, T.A.; Kurzrock, R. The FDA Approval of Pembrolizumab for Adult and Pediatric Patients with Tumor Mutational Burden (TMB) ≥10: A Decision Centered on Empowering Patients and Their Physicians. Ann. Oncol. 2020, 31, 1115–1118. [Google Scholar] [CrossRef]
- Chan, T.A.; Yarchoan, M.; Jaffee, E.; Swanton, C.; Quezada, S.A.; Stenzinger, A.; Peters, S. Development of Tumor Mutation Burden as an Immunotherapy Biomarker: Utility for the Oncology Clinic. Ann. Oncol. 2019, 30, 44–56. [Google Scholar] [CrossRef]
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H.; et al. Association of Tumour Mutational Burden with Outcomes in Patients with Advanced Solid Tumours Treated with Pembrolizumab: Prospective Biomarker Analysis of the Multicohort, Open-Label, Phase 2 KEYNOTE-158 Study. Lancet Oncol. 2020, 21, 1353–1365. [Google Scholar] [CrossRef]
- Kang, Y.-J.; O’Haire, S.; Franchini, F.; IJzerman, M.; Zalcberg, J.; Macrae, F.; Canfell, K.; Steinberg, J. A Scoping Review and Meta-Analysis on the Prevalence of Pan-Tumour Biomarkers (dMMR, MSI, High TMB) in Different Solid Tumours. Sci. Rep. 2022, 12, 20495. [Google Scholar] [CrossRef]
- Mirza, M.R.; Chase, D.M.; Slomovitz, B.M.; dePont Christensen, R.; Novák, Z.; Black, D.; Gilbert, L.; Sharma, S.; Valabrega, G.; Landrum, L.M.; et al. Dostarlimab for Primary Advanced or Recurrent Endometrial Cancer. N. Engl. J. Med. 2023, 388, 2145–2158. [Google Scholar] [CrossRef]
- André, T.; Berton, D.; Curigliano, G.; Sabatier, R.; Tinker, A.V.; Oaknin, A.; Ellard, S.; de Braud, F.; Arkenau, H.-T.; Trigo, J.; et al. Antitumor Activity and Safety of Dostarlimab Monotherapy in Patients with Mismatch Repair Deficient Solid Tumors: A Nonrandomized Controlled Trial. JAMA Netw. Open 2023, 6, e2341165. [Google Scholar] [CrossRef]
- Frenel, J.-S.; Le Tourneau, C.; O’Neil, B.; Ott, P.A.; Piha-Paul, S.A.; Gomez-Roca, C.; van Brummelen, E.M.J.; Rugo, H.S.; Thomas, S.; Saraf, S.; et al. Safety and Efficacy of Pembrolizumab in Advanced, Programmed Death Ligand 1-Positive Cervical Cancer: Results From the Phase Ib KEYNOTE-028 Trial. J. Clin. Oncol. 2017, 35, 4035–4041. [Google Scholar] [CrossRef] [PubMed]
- Muro, K.; Chung, H.C.; Shankaran, V.; Geva, R.; Catenacci, D.; Gupta, S.; Eder, J.P.; Golan, T.; Le, D.T.; Burtness, B.; et al. Pembrolizumab for Patients with PD-L1-Positive Advanced Gastric Cancer (KEYNOTE-012): A Multicentre, Open-Label, Phase 1b Trial. Lancet Oncol. 2016, 17, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Kim, T.W.; Van Cutsem, E.; Geva, R.; Jäger, D.; Hara, H.; Burge, M.; O’Neil, B.; Kavan, P.; Yoshino, T.; et al. Phase II Open-Label Study of Pembrolizumab in Treatment-Refractory, Microsatellite Instability–High/Mismatch Repair–Deficient Metastatic Colorectal Cancer: KEYNOTE-164. J. Clin. Oncol. 2020, 38, 11–19. [Google Scholar] [CrossRef]
- Cercek, A.; Lumish, M.; Sinopoli, J.; Weiss, J.; Shia, J.; Lamendola-Essel, M.; El Dika, I.H.; Segal, N.; Shcherba, M.; Sugarman, R.; et al. PD-1 Blockade in Mismatch Repair–Deficient, Locally Advanced Rectal Cancer. N. Engl. J. Med. 2022, 386, 2363–2376. [Google Scholar] [CrossRef]
- Georgescu, M.-T.; Patrascu, T.; Serbanescu, L.G.; Anghel, R.M.; Gales, L.N.; Georgescu, F.T.; Mitrica, R.I.; Georgescu, D.E. When Should We Expect Curative Results of Neoadjuvant Treatment in Locally Advanced Rectal Cancer Patients? Chirurgia 2021, 116, 16. [Google Scholar] [CrossRef]
- André, T.; Tougeron, D.; Piessen, G.; de la Fouchardière, C.; Louvet, C.; Adenis, A.; Jary, M.; Tournigand, C.; Aparicio, T.; Desrame, J.; et al. Neoadjuvant Nivolumab Plus Ipilimumab and Adjuvant Nivolumab in Localized Deficient Mismatch Repair/Microsatellite Instability–High Gastric or Esophagogastric Junction Adenocarcinoma: The GERCOR NEONIPIGA Phase II Study. J. Clin. Oncol. 2023, 41, 255–265. [Google Scholar] [CrossRef]
- Chalabi, M.; Fanchi, L.F.; Dijkstra, K.K.; Van den Berg, J.G.; Aalbers, A.G.; Sikorska, K.; Lopez-Yurda, M.; Grootscholten, C.; Beets, G.L.; Snaebjornsson, P.; et al. Neoadjuvant Immunotherapy Leads to Pathological Responses in MMR-Proficient and MMR-Deficient Early-Stage Colon Cancers. Nat. Med. 2020, 26, 566–576. [Google Scholar] [CrossRef]
- Chalabi, M.; Verschoor, Y.L.; Tan, P.B.; Balduzzi, S.; Lent, A.U.V.; Grootscholten, C.; Dokter, S.; Büller, N.V.; Grotenhuis, B.A.; Kuhlmann, K.; et al. Neoadjuvant Immunotherapy in Locally Advanced Mismatch Repair–Deficient Colon Cancer. N. Engl. J. Med. 2024, 390, 1949–1958. [Google Scholar] [CrossRef]
- Ludford, K.; Ho, W.J.; Thomas, J.V.; Raghav, K.P.S.; Murphy, M.B.; Fleming, N.D.; Lee, M.S.; Smaglo, B.G.; You, Y.N.; Tillman, M.M.; et al. Neoadjuvant Pembrolizumab in Localized Microsatellite Instability High/Deficient Mismatch Repair Solid Tumors. J. Clin. Oncol. 2023, 41, 2181–2190. [Google Scholar] [CrossRef]
- Addeo, A.; Passaro, A.; Malapelle, U.; Banna, G.L.; Subbiah, V.; Friedlaender, A. Immunotherapy in Non-Small Cell Lung Cancer Harbouring Driver Mutations. Cancer Treat. Rev. 2021, 96, 102179. [Google Scholar] [CrossRef] [PubMed]
- Friedlaender, A.; Perol, M.; Banna, G.L.; Parikh, K.; Addeo, A. Oncogenic Alterations in Advanced NSCLC: A Molecular Super-Highway. Biomark. Res. 2024, 12, 24. [Google Scholar] [CrossRef] [PubMed]
- Foffano, L.; Bertoli, E.; Bortolot, M.; Torresan, S.; De Carlo, E.; Stanzione, B.; Del Conte, A.; Puglisi, F.; Spina, M.; Bearz, A. Immunotherapy in Oncogene-Addicted NSCLC: Evidence and Therapeutic Approaches. Int. J. Mol. Sci. 2025, 26, 583. [Google Scholar] [CrossRef]
- Corvaja, C.; Passaro, A.; Attili, I.; Aliaga, P.T.; Spitaleri, G.; Signore, E.D.; Marinis, F. de Advancements in Fourth-Generation EGFR TKIs in EGFR-Mutant NSCLC: Bridging Biological Insights and Therapeutic Development. Cancer Treat. Rev. 2024, 130, 102824. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, M.G.; Di Noia, V.; D’Argento, E.; Vita, E.; Damiano, P.; Cannella, A.; Ribelli, M.; Pilotto, S.; Milella, M.; Tortora, G.; et al. Oncogene-Addicted Non-Small-Cell Lung Cancer: Treatment Opportunities and Future Perspectives. Cancers 2020, 12, 1196. [Google Scholar] [CrossRef]
- Suda, K.; Onozato, R.; Yatabe, Y.; Mitsudomi, T. EGFR T790M Mutation: A Double Role in Lung Cancer Cell Survival? J. Thorac. Oncol. 2009, 4, 1–4. [Google Scholar] [CrossRef]
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef]
- Planchard, D.; Jänne, P.A.; Cheng, Y.; Yang, J.C.-H.; Yanagitani, N.; Kim, S.-W.; Sugawara, S.; Yu, Y.; Fan, Y.; Geater, S.L.; et al. Osimertinib with or without Chemotherapy in EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2023, 389, 1935–1948. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.-W.; Kato, T.; et al. Osimertinib in Resected EGFR -Mutated Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Kato, T.; Dong, X.; Ahn, M.-J.; Quang, L.-V.; Soparattanapaisarn, N.; Inoue, T.; Wang, C.-L.; Huang, M.; Yang, J.C.-H.; et al. Osimertinib after Chemoradiotherapy in Stage III EGFR-Mutated NSCLC. N. Engl. J. Med. 2024, 391, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Yeap, B.Y.; Mino-Kenudson, M.; Digumarthy, S.R.; Costa, D.B.; Heist, R.S.; Solomon, B.; Stubbs, H.; Admane, S.; McDermott, U.; et al. Clinical Features and Outcome of Patients with Non–Small-Cell Lung Cancer Who Harbor EML4-ALK. J. Clin. Oncol. 2009, 27, 4247–4253. [Google Scholar] [CrossRef]
- Soda, M.; Choi, Y.L.; Enomoto, M.; Takada, S.; Yamashita, Y.; Ishikawa, S.; Fujiwara, S.; Watanabe, H.; Kurashina, K.; Hatanaka, H.; et al. Identification of the Transforming EML4-ALK Fusion Gene in Non-Small-Cell Lung Cancer. Nature 2007, 448, 561–566. [Google Scholar] [CrossRef]
- Solomon, B.J.; Bauer, T.M.; Mok, T.S.K.; Liu, G.; Mazieres, J.; de Marinis, F.; Goto, Y.; Kim, D.-W.; Wu, Y.-L.; Jassem, J.; et al. Efficacy and Safety of First-Line Lorlatinib versus Crizotinib in Patients with Advanced, ALK-Positive Non-Small-Cell Lung Cancer: Updated Analysis of Data from the Phase 3, Randomised, Open-Label CROWN Study. Lancet Respir. Med. 2023, 11, 354–366. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Dziadziuszko, R.; Ahn, J.S.; Barlesi, F.; Nishio, M.; Lee, D.H.; Lee, J.-S.; Zhong, W.; Horinouchi, H.; Mao, W.; et al. Alectinib in Resected ALK -Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2024, 390, 1265–1276. [Google Scholar] [CrossRef]
- Vingiani, A.; Agnelli, L.; Duca, M.; Lorenzini, D.; Damian, S.; Proto, C.; Niger, M.; Nichetti, F.; Tamborini, E.; Perrone, F.; et al. Molecular Tumor Board as a Clinical Tool for Converting Molecular Data Into Real-World Patient Care. JCO Precis. Oncol. 2023, 7, e2300067. [Google Scholar] [CrossRef]
- Yang, J.C.-H.; Wu, Y.-L.; Schuler, M.; Sebastian, M.; Popat, S.; Yamamoto, N.; Zhou, C.; Hu, C.-P.; O’Byrne, K.; Feng, J.; et al. Afatinib versus Cisplatin-Based Chemotherapy for EGFR Mutation-Positive Lung Adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): Analysis of Overall Survival Data from Two Randomised, Phase 3 Trials. Lancet Oncol. 2015, 16, 141–151. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Zhou, C.; Hu, C.-P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Shi, J.H.; Lee, K.Y.; et al. Afatinib versus Cisplatin plus Gemcitabine for First-Line Treatment of Asian Patients with Advanced Non-Small-Cell Lung Cancer Harbouring EGFR Mutations (LUX-Lung 6): An Open-Label, Randomised Phase 3 Trial. Lancet Oncol. 2014, 15, 213–222. [Google Scholar] [CrossRef]
- Sequist, L.V.; Yang, J.C.-H.; Yamamoto, N.; O’Byrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.-M.; Boyer, M.; et al. Phase III Study of Afatinib or Cisplatin plus Pemetrexed in Patients with Metastatic Lung Adenocarcinoma with EGFR Mutations. J. Clin. Oncol. 2013, 31, 3327–3334. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.-H.; Shih, J.-Y.; Su, W.-C.; Hsia, T.-C.; Tsai, C.-M.; Ou, S.-H.I.; Yu, C.-J.; Chang, G.-C.; Ho, C.-L.; Sequist, L.V.; et al. Afatinib for Patients with Lung Adenocarcinoma and Epidermal Growth Factor Receptor Mutations (LUX-Lung 2): A Phase 2 Trial. Lancet Oncol. 2012, 13, 539–548. [Google Scholar] [CrossRef]
- Yang, J.C.-H.; Sequist, L.V.; Geater, S.L.; Tsai, C.-M.; Mok, T.S.K.; Schuler, M.; Yamamoto, N.; Yu, C.-J.; Ou, S.-H.I.; Zhou, C.; et al. Clinical Activity of Afatinib in Patients with Advanced Non-Small-Cell Lung Cancer Harbouring Uncommon EGFR Mutations: A Combined Post-Hoc Analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6. Lancet Oncol. 2015, 16, 830–838. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus Standard Chemotherapy as First-Line Treatment for European Patients with Advanced EGFR Mutation-Positive Non-Small-Cell Lung Cancer (EURTAC): A Multicentre, Open-Label, Randomised Phase 3 Trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Shepherd, F.A.; Hirsh, V.; Smylie, M.; Findlay, B.; Santabárbara, P. Erlotinib in Previously Treated Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2005, 353, 123–132. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Tsuji, F.; Linke, R.; Rosell, R.; Corral, J.; et al. Dacomitinib versus Gefitinib as First-Line Treatment for Patients with EGFR-Mutation-Positive Non-Small-Cell Lung Cancer (ARCHER 1050): A Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2017, 18, 1454–1466. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Chawla, A.; Rosell, R.; Corral, J.; Migliorino, M.R.; et al. Updated Overall Survival in a Randomized Study Comparing Dacomitinib with Gefitinib as First-Line Treatment in Patients with Advanced Non-Small-Cell Lung Cancer and EGFR-Activating Mutations. Drugs 2021, 81, 257–266. [Google Scholar] [CrossRef]
- Inoue, A.; Kobayashi, K.; Maemondo, M.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Updated Overall Survival Results from a Randomized Phase III Trial Comparing Gefitinib with Carboplatin–Paclitaxel for Chemo-Naïve Non-Small Cell Lung Cancer with Sensitive EGFR Gene Mutations (NEJ002). Ann. Oncol. 2013, 24, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or Chemotherapy for Non–Small-Cell Lung Cancer with Mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef]
- Tsuboi, M.; Herbst, R.S.; John, T.; Kato, T.; Majem, M.; Grohé, C.; Wang, J.; Goldman, J.W.; Lu, S.; Su, W.-C.; et al. Overall Survival with Osimertinib in Resected EGFR-Mutated NSCLC. N. Engl. J. Med. 2023, 389, 137–147. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Papadimitrakopoulou, V.A.; Mok, T.S.; Han, J.-Y.; Ahn, M.-J.; Delmonte, A.; Ramalingam, S.S.; Kim, S.W.; Shepherd, F.A.; Laskin, J.; He, Y.; et al. Osimertinib versus Platinum-Pemetrexed for Patients with EGFR T790M Advanced NSCLC and Progression on a Prior EGFR-Tyrosine Kinase Inhibitor: AURA3 Overall Survival Analysis. Ann. Oncol. 2020, 31, 1536–1544. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.-L.; Ahn, M.-J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.S.M.E.; et al. Osimertinib or Platinum–Pemetrexed in EGFR T790M–Positive Lung Cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef]
- Zhou, C.; Tang, K.-J.; Cho, B.C.; Liu, B.; Paz-Ares, L.; Cheng, S.; Kitazono, S.; Thiagarajan, M.; Goldman, J.W.; Sabari, J.K.; et al. Amivantamab plus Chemotherapy in NSCLC with EGFR Exon 20 Insertions. N. Engl. J. Med. 2023, 389, 2039–2051. [Google Scholar] [CrossRef]
- Cho, B.C.; Lu, S.; Felip, E.; Spira, A.I.; Girard, N.; Lee, J.-S.; Lee, S.-H.; Ostapenko, Y.; Danchaivijitr, P.; Liu, B.; et al. Amivantamab plus Lazertinib in Previously Untreated EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2024, 391, 1486–1498. [Google Scholar] [CrossRef] [PubMed]
- Goto, K.; Goto, Y.; Kubo, T.; Ninomiya, K.; Kim, S.-W.; Planchard, D.; Ahn, M.-J.; Smit, E.F.; de Langen, A.J.; Pérol, M.; et al. Trastuzumab Deruxtecan in Patients with HER2-Mutant Metastatic Non–Small-Cell Lung Cancer: Primary Results From the Randomized, Phase II DESTINY-Lung02 Trial. J. Clin. Oncol. 2023, 41, 4852–4863. [Google Scholar] [CrossRef]
- de Langen, A.J.; Johnson, M.L.; Mazieres, J.; Dingemans, A.-M.C.; Mountzios, G.; Pless, M.; Wolf, J.; Schuler, M.; Lena, H.; Skoulidis, F.; et al. Sotorasib versus Docetaxel for Previously Treated Non-Small-Cell Lung Cancer with KRASG12C Mutation: A Randomised, Open-Label, Phase 3 Trial. Lancet 2023, 401, 733–746. [Google Scholar] [CrossRef]
- Jänne, P.A.; Riely, G.J.; Gadgeel, S.M.; Heist, R.S.; Ou, S.-H.I.; Pacheco, J.M.; Johnson, M.L.; Sabari, J.K.; Leventakos, K.; Yau, E.; et al. Adagrasib in Non–Small-Cell Lung Cancer Harboring a KRASG12C Mutation. N. Engl. J. Med. 2022, 387, 120–131. [Google Scholar] [CrossRef]
- Drilon, A.; Rekhtman, N.; Arcila, M.; Wang, L.; Ni, A.; Albano, M.; Van Voorthuysen, M.; Somwar, R.; Smith, R.S.; Montecalvo, J.; et al. A Phase 2 Single Arm Trial of Cabozantinib in Patients with Advanced RET-Rearranged Lung Cancers. Lancet Oncol. 2016, 17, 1653–1660. [Google Scholar] [CrossRef]
- Solomon, B.J.; Mok, T.; Kim, D.-W.; Wu, Y.-L.; Nakagawa, K.; Mekhail, T.; Felip, E.; Cappuzzo, F.; Paolini, J.; Usari, T.; et al. First-Line Crizotinib versus Chemotherapy in ALK-Positive Lung Cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef]
- Shaw, A.T.; Kim, D.-W.; Nakagawa, K.; Seto, T.; Crinó, L.; Ahn, M.-J.; Pas, T.D.; Besse, B.; Solomon, B.J.; Blackhall, F.; et al. Crizotinib versus Chemotherapy in Advanced ALK-Positive Lung Cancer. N. Engl. J. Med. 2013, 368, 2385–2394. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.-C.; Tan, D.S.W.; Chiari, R.; Wu, Y.-L.; Paz-Ares, L.; Wolf, J.; Geater, S.L.; Orlov, S.; Cortinovis, D.; Yu, C.-J.; et al. First-Line Ceritinib versus Platinum-Based Chemotherapy in Advanced ALK-Rearranged Non-Small-Cell Lung Cancer (ASCEND-4): A Randomised, Open-Label, Phase 3 Study. Lancet 2017, 389, 917–929. [Google Scholar] [CrossRef]
- Tan, D.S.W.; Geater, S.; Yu, C.-J.; Tsai, C.-M.; Hsia, T.-C.; Chen, J.; Lin, M.-C.; Lu, Y.; Sriuranpong, V.; Yang, C.-T.; et al. Ceritinib Efficacy and Safety in Treatment-Naive Asian Patients with Advanced ALK-Rearranged NSCLC: An ASCEND-4 Subgroup Analysis. JTO Clin. Res. Rep. 2021, 2, 100131. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Kim, T.M.; Crinò, L.; Gridelli, C.; Kiura, K.; Liu, G.; Novello, S.; Bearz, A.; Gautschi, O.; Mok, T.; et al. Ceritinib versus Chemotherapy in Patients with ALK-Rearranged Non-Small-Cell Lung Cancer Previously given Chemotherapy and Crizotinib (ASCEND-5): A Randomised, Controlled, Open-Label, Phase 3 Trial. Lancet Oncol. 2017, 18, 874–886. [Google Scholar] [CrossRef]
- Ahn, M.J.; Kim, H.R.; Yang, J.C.H.; Han, J.-Y.; Li, J.Y.-C.; Hochmair, M.J.; Chang, G.-C.; Delmonte, A.; Lee, K.H.; Campelo, R.G.; et al. Efficacy and Safety of Brigatinib Compared with Crizotinib in Asian vs. Non-Asian Patients with Locally Advanced or Metastatic ALK-Inhibitor-Naive ALK+ Non-Small Cell Lung Cancer: Final Results From the Phase III ALTA-1L Study. Clin. Lung Cancer 2022, 23, 720–730. [Google Scholar] [CrossRef] [PubMed]
- Camidge, D.R.; Kim, H.R.; Ahn, M.-J.; Yang, J.C.-H.; Han, J.-Y.; Lee, J.-S.; Hochmair, M.J.; Li, J.Y.-C.; Chang, G.-C.; Lee, K.H.; et al. Brigatinib versus Crizotinib in ALK -Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2027–2039. [Google Scholar] [CrossRef]
- Camidge, D.R.; Kim, H.R.; Ahn, M.-J.; Yang, J.C.H.; Han, J.-Y.; Hochmair, M.J.; Lee, K.H.; Delmonte, A.; Garcia Campelo, M.R.; Kim, D.-W.; et al. Brigatinib Versus Crizotinib in ALK Inhibitor-Naive Advanced ALK-Positive NSCLC: Final Results of Phase 3 ALTA-1L Trial. J. Thorac. Oncol. 2021, 16, 2091–2108. [Google Scholar] [CrossRef]
- Hochmair, M.J.; Tiseo, M.; Reckamp, K.L.; West, H.L.; Groen, H.J.; Langer, C.J.; Reichmann, W.; Kerstein, D.; Kim, D.-W.; Camidge, D.R. Brigatinib in Crizotinib-Refractory ALK+ NSCLC: Updates from the Pivotal Randomized Phase 2 Trial (ALTA). Ann. Oncol. 2017, 28, ii35–ii36. [Google Scholar] [CrossRef]
- Huber, R.M.; Hansen, K.H.; Rodríguez, L.P.-A.; West, H.L.; Reckamp, K.L.; Leighl, N.B.; Tiseo, M.; Smit, E.F.; Kim, D.-W.; Gettinger, S.N.; et al. Brigatinib in Crizotinib-Refractory ALK+ NSCLC: 2-Year Follow-up on Systemic and Intracranial Outcomes in the Phase 2 ALTA Trial. J. Thorac. Oncol. 2020, 15, 404–415. [Google Scholar] [CrossRef]
- Peters, S.; Camidge, D.R.; Shaw, A.T.; Gadgeel, S.; Ahn, J.S.; Kim, D.-W.; Ou, S.-H.I.; Pérol, M.; Dziadziuszko, R.; Rosell, R.; et al. Alectinib versus Crizotinib in Untreated ALK -Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 829–838. [Google Scholar] [CrossRef]
- Mok, T.; Camidge, D.R.; Gadgeel, S.M.; Rosell, R.; Dziadziuszko, R.; Kim, D.-W.; Pérol, M.; Ou, S.-H.I.; Ahn, J.S.; Shaw, A.T.; et al. Updated Overall Survival and Final Progression-Free Survival Data for Patients with Treatment-Naive Advanced ALK-Positive Non-Small-Cell Lung Cancer in the ALEX Study. Ann. Oncol. 2020, 31, 1056–1064. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.; Wang, Z.; Wu, G.; Poddubskaya, E.; Mok, T.; Reck, M.; Wakelee, H.; Chiappori, A.A.; Lee, D.H.; Breder, V.; et al. Ensartinib vs Crizotinib for Patients with Anaplastic Lymphoma Kinase−Positive Non–Small Cell Lung Cancer: A Randomized Clinical Trial. JAMA Oncol. 2021, 7, 1617–1625. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Bauer, T.M.; De Marinis, F.; Felip, E.; Goto, Y.; Liu, G.; Mazieres, J.; Kim, D.-W.; Mok, T.; Polli, A.; et al. First-Line Lorlatinib or Crizotinib in Advanced ALK -Positive Lung Cancer. N. Engl. J. Med. 2020, 383, 2018–2029. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.J.; Liu, G.; Felip, E.; Mok, T.S.K.; Soo, R.A.; Mazieres, J.; Shaw, A.T.; de Marinis, F.; Goto, Y.; Wu, Y.-L.; et al. Lorlatinib Versus Crizotinib in Patients with Advanced ALK-Positive Non–Small Cell Lung Cancer: 5-Year Outcomes From the Phase III CROWN Study. J. Clin. Oncol. 2024, 42, 3400–3409. [Google Scholar] [CrossRef]
- Shaw, A.T.; Ou, S.-H.I.; Bang, Y.-J.; Camidge, D.R.; Solomon, B.J.; Salgia, R.; Riely, G.J.; Varella-Garcia, M.; Shapiro, G.I.; Costa, D.B.; et al. Crizotinib in ROS1-Rearranged Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2014, 371, 1963–1971. [Google Scholar] [CrossRef]
- Shaw, A.T.; Riely, G.J.; Bang, Y.-J.; Kim, D.-W.; Camidge, D.R.; Solomon, B.J.; Varella-Garcia, M.; Iafrate, A.J.; Shapiro, G.I.; Usari, T.; et al. Crizotinib in ROS1-Rearranged Advanced Non-Small-Cell Lung Cancer (NSCLC): Updated Results, Including Overall Survival, from PROFILE 1001. Ann. Oncol. 2019, 30, 1121–1126. [Google Scholar] [CrossRef]
- Dziadziuszko, R.; Krebs, M.G.; De Braud, F.; Siena, S.; Drilon, A.; Doebele, R.C.; Patel, M.R.; Cho, B.C.; Liu, S.V.; Ahn, M.-J.; et al. Updated Integrated Analysis of the Efficacy and Safety of Entrectinib in Locally Advanced or Metastatic ROS1 Fusion–Positive Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2021, 39, 1253–1263. [Google Scholar] [CrossRef]
- Drilon, A.; Chiu, C.-H.; Fan, Y.; Cho, B.C.; Lu, S.; Ahn, M.-J.; Krebs, M.G.; Liu, S.V.; John, T.; Otterson, G.A.; et al. Long-Term Efficacy and Safety of Entrectinib in ROS1 Fusion–Positive NSCLC. JTO Clin. Res. Rep. 2022, 3, 100332. [Google Scholar] [CrossRef]
- Shaw, A.T.; Solomon, B.J.; Chiari, R.; Riely, G.J.; Besse, B.; Soo, R.A.; Kao, S.; Lin, C.-C.; Bauer, T.M.; Clancy, J.S.; et al. Lorlatinib in Advanced ROS1-Positive Non-Small-Cell Lung Cancer: A Multicentre, Open-Label, Single-Arm, Phase 1–2 Trial. Lancet Oncol. 2019, 20, 1691–1701. [Google Scholar] [CrossRef]
- Wolf, J.; Seto, T.; Han, J.-Y.; Reguart, N.; Garon, E.B.; Groen, H.J.M.; Tan, D.S.W.; Hida, T.; De Jonge, M.; Orlov, S.V.; et al. Capmatinib in MET Exon 14–Mutated or MET -Amplified Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 944–957. [Google Scholar] [CrossRef]
- Wolf, J.; Hochmair, M.; Han, J.-Y.; Reguart, N.; Souquet, P.-J.; Smit, E.F.; Orlov, S.V.; Vansteenkiste, J.; Nishio, M.; Jonge, M. de; et al. Capmatinib in MET Exon 14-Mutated Non-Small-Cell Lung Cancer: Final Results from the Open-Label, Phase 2 GEOMETRY Mono-1 Trial. Lancet Oncol. 2024, 25, 1357–1370. [Google Scholar] [CrossRef] [PubMed]
- Mazieres, J.; Paik, P.K.; Garassino, M.C.; Le, X.; Sakai, H.; Veillon, R.; Smit, E.F.; Cortot, A.B.; Raskin, J.; Viteri, S.; et al. Tepotinib Treatment in Patients with MET Exon 14–Skipping Non–Small Cell Lung Cancer: Long-Term Follow-up of the VISION Phase 2 Nonrandomized Clinical Trial. JAMA Oncol. 2023, 9, 1260. [Google Scholar] [CrossRef] [PubMed]
- Paik, P.K.; Felip, E.; Veillon, R.; Sakai, H.; Cortot, A.B.; Garassino, M.C.; Mazieres, J.; Viteri, S.; Senellart, H.; Van Meerbeeck, J.; et al. Tepotinib in Non–Small-Cell Lung Cancer with MET Exon 14 Skipping Mutations. N. Engl. J. Med. 2020, 383, 931–943. [Google Scholar] [CrossRef]
- Drilon, A.; Clark, J.W.; Weiss, J.; Ou, S.-H.I.; Camidge, D.R.; Solomon, B.J.; Otterson, G.A.; Villaruz, L.C.; Riely, G.J.; Heist, R.S.; et al. Antitumor Activity of Crizotinib in Lung Cancers Harboring a MET Exon 14 Alteration. Nat. Med. 2020, 26, 47–51. [Google Scholar] [CrossRef]
- Planchard, D.; Besse, B.; Groen, H.J.M.; Hashemi, S.M.S.; Mazieres, J.; Kim, T.M.; Quoix, E.; Souquet, P.-J.; Barlesi, F.; Baik, C.; et al. Phase 2 Study of Dabrafenib Plus Trametinib in Patients with BRAF V600E-Mutant Metastatic NSCLC: Updated 5-Year Survival Rates and Genomic Analysis. J. Thorac. Oncol. 2022, 17, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Smit, E.F.; Groen, H.J.M.; Mazieres, J.; Besse, B.; Helland, Å.; Giannone, V.; D’Amelio, A.M.; Zhang, P.; Mookerjee, B.; et al. Dabrafenib plus Trametinib in Patients with Previously Untreated BRAFV600E-Mutant Metastatic Non-Small-Cell Lung Cancer: An Open-Label, Phase 2 Trial. Lancet Oncol. 2017, 18, 1307–1316. [Google Scholar] [CrossRef]
- Riely, G.J.; Smit, E.F.; Ahn, M.-J.; Felip, E.; Ramalingam, S.S.; Tsao, A.; Johnson, M.; Gelsomino, F.; Esper, R.; Nadal, E.; et al. Phase II, Open-Label Study of Encorafenib Plus Binimetinib in Patients with BRAFV600-Mutant Metastatic Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2023, 41, 3700–3711. [Google Scholar] [CrossRef]
- Drilon, A.; Tan, D.S.W.; Lassen, U.N.; Leyvraz, S.; Liu, Y.; Patel, J.D.; Rosen, L.; Solomon, B.; Norenberg, R.; Dima, L.; et al. Efficacy and Safety of Larotrectinib in Patients with Tropomyosin Receptor Kinase Fusion-Positive Lung Cancers. JCO Precis. Oncol. 2022, 6, e2100418. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Doebele, R.C.; Farago, A.F.; Liu, S.V.; Chawla, S.P.; Tosi, D.; Blakely, C.M.; Krauss, J.C.; Sigal, D.; Bazhenova, L.; et al. Entrectinib in NTRK Fusion-Positive Non-Small Cell Lung Cancer (NSCLC): Integrated Analysis of Patients (Pts) Enrolled in STARTRK-2, STARTRK-1 and ALKA-372-001. Ann. Oncol. 2019, 30, ii48–ii49. [Google Scholar] [CrossRef]
- Cho, B.C.; Chiu, C.-H.; Massarelli, E.; Buchschacher, G.L.; Goto, K.; Overbeck, T.R.; Loong, H.H.F.; Chee, C.E.; Garrido, P.; Dong, X.; et al. Updated Efficacy and Safety of Entrectinib in NTRK Fusion-Positive Non-Small Cell Lung Cancer. Lung Cancer 2024, 188, 107442. [Google Scholar] [CrossRef]
- Kim, D.-W.; Schram, A.M.; Hollebecque, A.; Nishino, K.; Macarulla, T.; Rha, S.Y.; Duruisseaux, M.; Liu, S.V.; Al Hallak, M.N.; Umemoto, K.; et al. The Phase I/II eNRGy Trial: Zenocutuzumab in Patients with Cancers Harboring NRG1 Gene Fusions. Future Oncol. Lond. Engl. 2024, 20, 1057–1067. [Google Scholar] [CrossRef]
- Simion, L.; Chitoran, E.; Cirimbei, C.; Stefan, D.-C.; Neicu, A.; Tanase, B.; Ionescu, S.O.; Luca, D.C.; Gales, L.; Gheorghe, A.S.; et al. A Decade of Therapeutic Challenges in Synchronous Gynecological Cancers from the Bucharest Oncological Institute. Diagnostics 2023, 13, 2069. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Silvestri, V.; Leslie, G.; Rebbeck, T.R.; Neuhausen, S.L.; Hopper, J.L.; Nielsen, H.R.; Lee, A.; Yang, X.; McGuffog, L.; et al. Cancer Risks Associated with BRCA1 and BRCA2 Pathogenic Variants. J. Clin. Oncol. 2022, 40, 1529–1541. [Google Scholar] [CrossRef] [PubMed]
- Tasca, G.; Dieci, M.V.; Baretta, Z.; Faggioni, G.; Montagna, M.; Nicoletto, M.O.; Peccatori, F.A.; Guarneri, V.; Colombo, N. Synchronous and Metachronous Breast and Ovarian Cancer: Experience From Two Large Cancer Center. Front. Oncol. 2020, 10, 608783. [Google Scholar] [CrossRef]
- Concolino, P.; Gelli, G.; Rizza, R.; Costella, A.; Scambia, G.; Capoluongo, E. BRCA1 and BRCA2 Testing through Next Generation Sequencing in a Small Cohort of Italian Breast/Ovarian Cancer Patients: Novel Pathogenic and Unknown Clinical Significance Variants. Int. J. Mol. Sci. 2019, 20, 3442. [Google Scholar] [CrossRef]
- den Brok, W.D.; Schrader, K.A.; Sun, S.; Tinker, A.V.; Zhao, E.Y.; Aparicio, S.; Gelmon, K.A. Homologous Recombination Deficiency in Breast Cancer: A Clinical Review. JCO Precis. Oncol. 2017, 1, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Haupts, A.; Kloth, M.; Roth, W.; Hartmann, N. A Novel Targeted NGS Panel Identifies Numerous Homologous Recombination Deficiency (HRD)-Associated Gene Mutations in Addition to Known BRCA Mutations. Diagn. Pathol. 2024, 19, 9. [Google Scholar] [CrossRef]
- Tsantikidi, A.; Papadopoulou, E.; Metaxa-Mariatou, V.; Kapetsis, G.; Tsaousis, G.; Meintani, A.; Florou-Chatzigiannidou, C.; Gazouli, M.; Papadimitriou, C.; Timotheadou, E.; et al. The Utility of NGS Analysis in Homologous Recombination Deficiency Tracking. Diagnostics 2023, 13, 2962. [Google Scholar] [CrossRef]
- Prophylactic Interventions for Hereditary Breast and Ovarian Cancer Risks and Mortality in BRCA1/2 Carriers. Available online: https://www.mdpi.com/2072-6694/16/1/103 (accessed on 30 January 2025).
- Bono, M.; Fanale, D.; Incorvaia, L.; Cancelliere, D.; Fiorino, A.; Calò, V.; Dimino, A.; Filorizzo, C.; Corsini, L.R.; Brando, C.; et al. Impact of Deleterious Variants in Other Genes beyond BRCA1/2 Detected in Breast/Ovarian and Pancreatic Cancer Patients by NGS-Based Multi-Gene Panel Testing: Looking over the Hedge. ESMO Open 2021, 6, 100235. [Google Scholar] [CrossRef]
- Kurian, A.W.; Hughes, E.; Handorf, E.A.; Gutin, A.; Allen, B.; Hartman, A.-R.; Hall, M.J. Breast and Ovarian Cancer Penetrance Estimates Derived From Germline Multiple-Gene Sequencing Results in Women. JCO Precis. Oncol. 2017, 1, 1–12. [Google Scholar] [CrossRef]
- Akbari, M.R.; Wallis, C.J.D.; Toi, A.; Trachtenberg, J.; Sun, P.; Narod, S.A.; Nam, R.K. The Impact of a BRCA2 Mutation on Mortality from Screen-Detected Prostate Cancer. Br. J. Cancer 2014, 111, 1238–1240. [Google Scholar] [CrossRef] [PubMed]
- Bolton, K.L.; Chenevix-Trench, G.; Goh, C.; Sadetzki, S.; Ramus, S.J.; Karlan, B.Y.; Lambrechts, D.; Despierre, E.; Barrowdale, D.; McGuffog, L.; et al. Association Between BRCA1 and BRCA2 Mutations and Survival in Women with Invasive Epithelial Ovarian Cancer. JAMA J. Am. Med. Assoc. 2012, 307, 382–390. [Google Scholar] [CrossRef]
- Zhu, Y.; Wu, J.; Zhang, C.; Sun, S.; Zhang, J.; Liu, W.; Huang, J.; Zhang, Z. BRCA Mutations and Survival in Breast Cancer: An Updated Systematic Review and Meta-Analysis. Oncotarget 2016, 7, 70113–70127. [Google Scholar] [CrossRef]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef]
- DiSilvestro, P.; Banerjee, S.; Colombo, N.; Scambia, G.; Kim, B.-G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; et al. Overall Survival with Maintenance Olaparib at a 7-Year Follow-Up in Patients with Newly Diagnosed Advanced Ovarian Cancer and a BRCA Mutation: The SOLO1/GOG 3004 Trial. J. Clin. Oncol. 2023, 41, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Ray-Coquard, I.; Pautier, P.; Pignata, S.; Pérol, D.; González-Martín, A.; Berger, R.; Fujiwara, K.; Vergote, I.; Colombo, N.; Mäenpää, J.; et al. Olaparib plus Bevacizumab as First-Line Maintenance in Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2416–2428. [Google Scholar] [CrossRef]
- Ray-Coquard, I.; Leary, A.; Pignata, S.; Cropet, C.; González-Martín, A.; Marth, C.; Nagao, S.; Vergote, I.; Colombo, N.; Mäenpää, J.; et al. Olaparib plus Bevacizumab First-Line Maintenance in Ovarian Cancer: Final Overall Survival Results from the PAOLA-1/ENGOT-Ov25 Trial. Ann. Oncol. 2023, 34, 681–692. [Google Scholar] [CrossRef] [PubMed]
- Tutt, A.N.J.; Garber, J.E.; Kaufman, B.; Viale, G.; Fumagalli, D.; Rastogi, P.; Gelber, R.D.; de Azambuja, E.; Fielding, A.; Balmaña, J.; et al. Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer. N. Engl. J. Med. 2021, 384, 2394–2405. [Google Scholar] [CrossRef]
- Geyer, C.E.; Garber, J.E.; Gelber, R.D.; Yothers, G.; Taboada, M.; Ross, L.; Rastogi, P.; Cui, K.; Arahmani, A.; Aktan, G.; et al. Overall Survival in the OlympiA Phase III Trial of Adjuvant Olaparib in Patients with Germline Pathogenic Variants in BRCA1/2 and High-Risk, Early Breast Cancer. Ann. Oncol. 2022, 33, 1250–1268. [Google Scholar] [CrossRef]
- Robson, M.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef]
- Robson, M.E.; Tung, N.; Conte, P.; Im, S.-A.; Senkus, E.; Xu, B.; Masuda, N.; Delaloge, S.; Li, W.; Armstrong, A.; et al. OlympiAD Final Overall Survival and Tolerability Results: Olaparib versus Chemotherapy Treatment of Physician’s Choice in Patients with a Germline BRCA Mutation and HER2-Negative Metastatic Breast Cancer. Ann. Oncol. 2019, 30, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Robson, M.E.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Tung, N.; Armstrong, A.; Dymond, M.; et al. OlympiAD Extended Follow-up for Overall Survival and Safety: Olaparib versus Chemotherapy Treatment of Physician’s Choice in Patients with a Germline BRCA Mutation and HER2-Negative Metastatic Breast Cancer. Eur. J. Cancer 2023, 184, 39–47. [Google Scholar] [CrossRef] [PubMed]
- de Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef]
- Clarke, N.W.; Armstrong, A.J.; Thiery-Vuillemin, A.; Oya, M.; Shore, N.; Loredo, E.; Procopio, G.; de Menezes, J.; Girotto, G.; Arslan, C.; et al. Abiraterone and Olaparib for Metastatic Castration-Resistant Prostate Cancer. NEJM Evid. 2022, 1, EVIDoa2200043. [Google Scholar] [CrossRef] [PubMed]
- Saad, F.; Clarke, N.W.; Oya, M.; Shore, N.; Procopio, G.; Guedes, J.D.; Arslan, C.; Mehra, N.; Parnis, F.; Brown, E.; et al. Olaparib plus Abiraterone versus Placebo plus Abiraterone in Metastatic Castration-Resistant Prostate Cancer (PROpel): Final Prespecified Overall Survival Results of a Randomised, Double-Blind, Phase 3 Trial. Lancet Oncol. 2023, 24, 1094–1108. [Google Scholar] [CrossRef]
- Golan, T.; Hammel, P.; Reni, M.; Cutsem, E.V.; Macarulla, T.; Hall, M.J.; Park, J.-O.; Hochhauser, D.; Arnold, D.; Oh, D.-Y.; et al. Maintenance Olaparib for Germline BRCA-Mutated Metastatic Pancreatic Cancer. N. Engl. J. Med. 2019, 381, 317–327. [Google Scholar] [CrossRef]
- Kindler, H.L.; Hammel, P.; Reni, M.; Van Cutsem, E.; Macarulla, T.; Hall, M.J.; Park, J.O.; Hochhauser, D.; Arnold, D.; Oh, D.-Y.; et al. Overall Survival Results From the POLO Trial: A Phase III Study of Active Maintenance Olaparib Versus Placebo for Germline BRCA-Mutated Metastatic Pancreatic Cancer. J. Clin. Oncol. 2022, 40, 3929–3939. [Google Scholar] [CrossRef]
- Westin, S.N.; Moore, K.; Chon, H.S.; Lee, J.-Y.; Pepin, J.T.; Sundborg, M.; Shai, A.; de la Garza, J.; Nishio, S.; Gold, M.A.; et al. Durvalumab Plus Carboplatin/Paclitaxel Followed by Maintenance Durvalumab with or without Olaparib as First-Line Treatment for Advanced Endometrial Cancer: The Phase III DUO-E Trial. J. Clin. Oncol. 2024, 42, 283–299. [Google Scholar] [CrossRef]
- González-Martín, A.; Pothuri, B.; Vergote, I.; Christensen, R.D.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef]
- Monk, B.J.; Barretina-Ginesta, M.P.; Pothuri, B.; Vergote, I.; Graybill, W.; Mirza, M.R.; McCormick, C.C.; Lorusso, D.; Moore, R.G.; Freyer, G.; et al. Niraparib First-Line Maintenance Therapy in Patients with Newly Diagnosed Advanced Ovarian Cancer: Final Overall Survival Results from the PRIMA/ENGOT-OV26/GOG-3012 Trial. Ann. Oncol. 2024, 35, 981–992. [Google Scholar] [CrossRef]
- Chi, K.N.; Rathkopf, D.; Smith, M.R.; Efstathiou, E.; Attard, G.; Olmos, D.; Lee, J.Y.; Small, E.J.; Pereira de Santana Gomes, A.J.; Roubaud, G.; et al. Niraparib and Abiraterone Acetate for Metastatic Castration-Resistant Prostate Cancer. J. Clin. Oncol. 2023, 41, 3339–3351. [Google Scholar] [CrossRef]
- Coleman, R.L.; Oza, A.M.; Lorusso, D.; Aghajanian, C.; Oaknin, A.; Dean, A.; Colombo, N.; Weberpals, J.I.; Clamp, A.; Scambia, G.; et al. Rucaparib Maintenance Treatment for Recurrent Ovarian Carcinoma after Response to Platinum Therapy (ARIEL3): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet 2017, 390, 1949–1961. [Google Scholar] [CrossRef]
- Ledermann, J.A.; Oza, A.M.; Lorusso, D.; Aghajanian, C.; Oaknin, A.; Dean, A.; Colombo, N.; Weberpals, J.I.; Clamp, A.R.; Scambia, G.; et al. Rucaparib for Patients with Platinum-Sensitive, Recurrent Ovarian Carcinoma (ARIEL3): Post-Progression Outcomes and Updated Safety Results from a Randomised, Placebo-Controlled, Phase 3 Trial. Lancet Oncol. 2020, 21, 710–722. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Piulats, J.M.; Reaume, M.N.; Ostler, P.; McDermott, R.; Gingerich, J.R.; Pintus, E.; Sridhar, S.S.; Bambury, R.M.; Emmenegger, U.; et al. Rucaparib or Physician’s Choice in Metastatic Prostate Cancer. N. Engl. J. Med. 2023, 388, 719–732. [Google Scholar] [CrossRef] [PubMed]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.-H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N. Engl. J. Med. 2018, 379, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Litton, J.K.; Hurvitz, S.A.; Mina, L.A.; Rugo, H.S.; Lee, K.-H.; Gonçalves, A.; Diab, S.; Woodward, N.; Goodwin, A.; Yerushalmi, R.; et al. Talazoparib versus Chemotherapy in Patients with Germline BRCA1/2-Mutated HER2-Negative Advanced Breast Cancer: Final Overall Survival Results from the EMBRACA Trial. Ann. Oncol. 2020, 31, 1526–1535. [Google Scholar] [CrossRef]
- Agarwal, N.; Azad, A.A.; Carles, J.; Fay, A.P.; Matsubara, N.; Heinrich, D.; Szczylik, C.; Giorgi, U.D.; Joung, J.Y.; Fong, P.C.C.; et al. Talazoparib plus Enzalutamide in Men with First-Line Metastatic Castration-Resistant Prostate Cancer (TALAPRO-2): A Randomised, Placebo-Controlled, Phase 3 Trial. Lancet 2023, 402, 291–303. [Google Scholar] [CrossRef]
- Fizazi, K.; Azad, A.A.; Matsubara, N.; Carles, J.; Fay, A.P.; De Giorgi, U.; Joung, J.Y.; Fong, P.C.C.; Voog, E.; Jones, R.J.; et al. First-Line Talazoparib with Enzalutamide in HRR-Deficient Metastatic Castration-Resistant Prostate Cancer: The Phase 3 TALAPRO-2 Trial. Nat. Med. 2024, 30, 257–264. [Google Scholar] [CrossRef]
- Zgura, A.; Gales, L.; Bratila, E.; Mehedintu, C.; Haineala, B.; Barac, R.I.; Popa, A.R.; Buhas, C.; Berceanu, C.; Andreescu, C.V.; et al. Variation of the T Lymphocytes According to Treatment in Breast Cancer. Rev. Chim. 2019, 70, 1649–1654. [Google Scholar] [CrossRef]
- Cardoso, F.; Hirshfield, K.M.; Kraynyak, K.A.; Tryfonidis, K.; Bardia, A. Immunotherapy for Hormone Receptor‒positive HER2-Negative Breast Cancer. Npj Breast Cancer 2024, 10, 104. [Google Scholar] [CrossRef]
- Stemke-Hale, K.; Gonzalez-Angulo, A.M.; Lluch, A.; Neve, R.M.; Kuo, W.-L.; Davies, M.; Carey, M.; Hu, Z.; Guan, Y.; Sahin, A.; et al. An Integrative Genomic and Proteomic Analysis of PIK3CA, PTEN, and AKT Mutations in Breast Cancer. Cancer Res. 2008, 68, 6084–6091. [Google Scholar] [CrossRef] [PubMed]
- Raei, M.; Heydari, K.; Tabarestani, M.; Razavi, A.; Mirshafiei, F.; Esmaeily, F.; Taheri, M.; Hoseini, A.; Nazari, H.; Shamshirian, D.; et al. Diagnostic Accuracy of ESR1 Mutation Detection by Cell-Free DNA in Breast Cancer: A Systematic Review and Meta-Analysis of Diagnostic Test Accuracy. BMC Cancer 2024, 24, 908. [Google Scholar] [CrossRef]
- Turner, N.C.; Im, S.-A.; Saura, C.; Juric, D.; Loibl, S.; Kalinsky, K.; Schmid, P.; Loi, S.; Sunpaweravong, P.; Musolino, A.; et al. Inavolisib-Based Therapy in PIK3CA-Mutated Advanced Breast Cancer. N. Engl. J. Med. 2024, 391, 1584–1596. [Google Scholar] [CrossRef]
- André, F.; Ciruelos, E.; Rubovszky, G.; Campone, M.; Loibl, S.; Rugo, H.S.; Iwata, H.; Conte, P.; Mayer, I.A.; Kaufman, B.; et al. Alpelisib for PIK3CA-Mutated, Hormone Receptor–Positive Advanced Breast Cancer. N. Engl. J. Med. 2019, 380, 1929–1940. [Google Scholar] [CrossRef] [PubMed]
- André, F.; Ciruelos, E.M.; Juric, D.; Loibl, S.; Campone, M.; Mayer, I.A.; Rubovszky, G.; Yamashita, T.; Kaufman, B.; Lu, Y.-S.; et al. Alpelisib plus Fulvestrant for PIK3CA-Mutated, Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor-2-Negative Advanced Breast Cancer: Final Overall Survival Results from SOLAR-1. Ann. Oncol. 2021, 32, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.C.; Oliveira, M.; Howell, S.J.; Dalenc, F.; Cortes, J.; Moreno, H.L.G.; Hu, X.; Jhaveri, K.; Krivorotko, P.; Loibl, S.; et al. Capivasertib in Hormone Receptor–Positive Advanced Breast Cancer. N. Engl. J. Med. 2023, 388, 2058–2070. [Google Scholar] [CrossRef]
- Bidard, F.-C.; Kaklamani, V.G.; Neven, P.; Streich, G.; Montero, A.J.; Forget, F.; Mouret-Reynier, M.-A.; Sohn, J.H.; Taylor, D.; Harnden, K.K.; et al. Elacestrant (Oral Selective Estrogen Receptor Degrader) Versus Standard Endocrine Therapy for Estrogen Receptor–Positive, Human Epidermal Growth Factor Receptor 2–Negative Advanced Breast Cancer: Results from the Randomized Phase III EMERALD Trial. J. Clin. Oncol. 2022, 40, 3246–3256. [Google Scholar] [CrossRef]
- Sebastião, M.M.; Ho, R.S.; de Carvalho, J.P.V.; Nussbaum, M. Diagnostic Accuracy of Next Generation Sequencing Panel Using Circulating Tumor DNA in Patients with Advanced Non-Small Cell Lung Cancer: A Systematic Review and Meta-Analysis. J. Health Econ. Outcomes Res. 2020, 7, 158–163. [Google Scholar] [CrossRef]
- Gašperšič, J.; Videtič Paska, A. Potential of Modern Circulating Cell-Free DNA Diagnostic Tools for Detection of Specific Tumour Cells in Clinical Practice. Biochem. Medica 2020, 30, 030504. [Google Scholar] [CrossRef]
- Gu, W.; Zhuang, W.; Zhuang, M.; He, M.; Li, Z. DNA Damage Response and Repair Gene Mutations Are Associated with Tumor Mutational Burden and Outcomes to Platinum-Based Chemotherapy/Immunotherapy in Advanced NSCLC Patients. Diagn. Pathol. 2023, 18, 119. [Google Scholar] [CrossRef]
- Wang, H.; Sun, L.; Sang, Y.; Yang, X.; Tian, G.; Wang, Z.; Fang, J.; Sun, W.; Zhou, L.; Jia, L.; et al. A Study of ALK-Positive Pulmonary Squamous-Cell Carcinoma: From Diagnostic Methodologies to Clinical Efficacy. Lung Cancer Amst. Neth. 2019, 130, 135–142. [Google Scholar] [CrossRef]
- Byron, S.A.; Van Keuren-Jensen, K.R.; Engelthaler, D.M.; Carpten, J.D.; Craig, D.W. Translating RNA Sequencing into Clinical Diagnostics: Opportunities and Challenges. Nat. Rev. Genet. 2016, 17, 257–271. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, S.N.; Peneva, D.; Cuyun Carter, G.; Palomares, M.R.; Thakkar, S.; Hall, D.W.; Dalglish, H.; Campos, C.; Yermilov, I. Comprehensive Review on the Clinical Impact of Next-Generation Sequencing Tests for the Management of Advanced Cancer. JCO Precis. Oncol. 2023, 7, e2200715. [Google Scholar] [CrossRef]
- Mirza, M.; Goerke, L.; Anderson, A.; Wilsdon, T. Assessing the Cost-Effectiveness of Next-Generation Sequencing as a Biomarker Testing Approach in Oncology and Policy Implications: A Literature Review. Value Health 2024, 27, 1300–1309. [Google Scholar] [CrossRef] [PubMed]
- Trifanescu, O.G.; Gales, L.; Bacinschi, X.; Serbanescu, L.; Georgescu, M.; Sandu, A.; Michire, A.; Anghel, R. Impact of the COVID-19 Pandemic on Treatment and Oncologic Outcomes for Cancer Patients in Romania. Vivo 2022, 36, 934–941. [Google Scholar] [CrossRef]
- Schluckebier, L.; Caetano, R.; Garay, O.U.; Montenegro, G.T.; Custodio, M.; Aran, V.; Gil Ferreira, C. Cost-Effectiveness Analysis Comparing Companion Diagnostic Tests for EGFR, ALK, and ROS1 versus next-Generation Sequencing (NGS) in Advanced Adenocarcinoma Lung Cancer Patients. BMC Cancer 2020, 20, 875. [Google Scholar] [CrossRef]
- Ferreira-Gonzalez, A.; Ko, G.; Fusco, N.; Stewart, F.; Kistler, K.; Appukkuttan, S.; Hocum, B.; Allen, S.M.; Babajanyan, S. Barriers and Facilitators to Next-Generation Sequencing Use in United States Oncology Settings: A Systematic Review. Future Oncol. 2024, 20, 2765–2777. [Google Scholar] [CrossRef]
- Rehm, H.L.; Page, A.J.H.; Smith, L.; Adams, J.B.; Alterovitz, G.; Babb, L.J.; Barkley, M.P.; Baudis, M.; Beauvais, M.J.S.; Beck, T.; et al. GA4GH: International Policies and Standards for Data Sharing across Genomic Research and Healthcare. Cell Genom. 2021, 1, 100029. [Google Scholar] [CrossRef]
- Mulder, N.; Abimiku, A.; Adebamowo, S.N.; de Vries, J.; Matimba, A.; Olowoyo, P.; Ramsay, M.; Skelton, M.; Stein, D.J. H3Africa: Current Perspectives. Pharmacogenom. Pers. Med. 2018, 11, 59–66. [Google Scholar] [CrossRef]
- D’Angelo, S.P.; Araujo, D.M.; Razak, A.R.A.; Agulnik, M.; Attia, S.; Blay, J.-Y.; Garcia, I.C.; Charlson, J.A.; Choy, E.; Demetri, G.D.; et al. Afamitresgene Autoleucel for Advanced Synovial Sarcoma and Myxoid Round Cell Liposarcoma (SPEARHEAD-1): An International, Open-Label, Phase 2 Trial. Lancet 2024, 403, 1460–1471. [Google Scholar] [CrossRef]
- Gulilat, M.; Lamb, T.; Teft, W.A.; Wang, J.; Dron, J.S.; Robinson, J.F.; Tirona, R.G.; Hegele, R.A.; Kim, R.B.; Schwarz, U.I. Targeted next Generation Sequencing as a Tool for Precision Medicine. BMC Med. Genom. 2019, 12, 81. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| NGS Test | Technology Used | Sample Type | Key Notes | Time | Molecular Alterations | Relevant Literature |
|---|---|---|---|---|---|---|
| FoundationOne CDx | Hybrid Capture NGS | Tumor Tissue | Comprehensive solid tumor profiling includes >300 genes and detects fusions and amplifications. | 14 days | EGFR, ALK, BRAF, BRCA1/2, MET, NTRK, ROS1, PIK3CA, RET, ERBB2 (HER2), KRAS, IDH1, FGFR1/2/3, CDK4, CDK6, KIT, PDGFRA, TSC1/2, ERBB3 | [5,6] |
| FoundationOne Liquid CDx | cfDNA Sequencing | Blood (Liquid Biopsy) | Liquid biopsy test; sensitivity decreases for variants with allele frequency <0.1%. | 10–14 days | EGFR, ALK, BRAF, BRCA1/2, MET, NTRK, ROS1, PIK3CA, RET, ERBB2 (HER2), KRAS, IDH1, FGFR2/3 | [7] |
| Guardant360 CDx | cfDNA Sequencing | Blood (Liquid Biopsy) | High sensitivity for detecting rare cfDNA variants; optimized for minimal input samples. | 7 days | EGFR, ALK, BRAF, BRCA1/2, MET, RET, ERBB2 (HER2), PIK3CA, KRAS, IDH1 | [8] |
| MSK-IMPACT | Hybrid Capture NGS | Tumor Tissue | Highly validated for solid tumors; includes 468 cancer-relevant genes. | 21 days | EGFR, ALK, BRAF, BRCA1/2, MET, NTRK, ROS1, PIK3CA, RET, ERBB2 (HER2), KRAS, IDH1, FGFR1/2/3, CDK4, CDK6, KIT, PDGFRA, TSC1/2, ERBB3 | [9] |
| Oncomine Dx Target Test | AmpliSeq NGS | Tumor Tissue | Focused on NSCLC; detects EGFR, ALK, ROS1, BRAF, and other actionable mutations. | 7–10 days | EGFR, ALK, BRAF, ROS1, RET, MET, KRAS | [10] |
| Oncomine Comprehensive Assay | AmpliSeq NGS | Tumor Tissue | Comprehensive tumor profiling with >500 genes, including fusion detection. | 7–14 days | EGFR, ALK, BRAF, ROS1, RET, MET, KRAS | [11] |
| Tempus xT | Hybrid Capture NGS | Tumor Tissue | The broad panel covering >600 genes; includes TMB and MSI analysis. | 10–14 days | EGFR, ALK, BRAF, BRCA1/2, MET, NTRK, ROS1, PIK3CA, RET, ERBB2 (HER2), KRAS, IDH1, FGFR1/2/3, CDK4, CDK6, KIT, PDGFRA, TSC1/2, ERBB3 | [12] |
| Caris Molecular Intelligence | Multiple NGS Platforms | Tumor Tissue | Uses multiple platforms; integrates NGS, IHC, and other molecular tests for a holistic profile. | 10–14 days | EGFR, ALK, BRAF, BRCA1/2, MET, NTRK, ROS1, PIK3CA, RET, ERBB2 (HER2), KRAS, IDH1, FGFR1/2/3, CDK4, CDK6, KIT, PDGFRA, TSC1/2, ERBB3 | [13] |
| Com.Pl.it DX Colon | Hybrid Capture NGS | Tumor Tissue | Focused on colorectal cancer profiling; including MSI detection and fusion analysis. | 10–14 days | EGFR, ALK, BRAF, KRAS, MET, RET, PIK3CA, ERBB2 (HER2), MSI detection | |
| Com.Pl.it DX Liquid Biopsy | cfDNA Sequencing | Blood (Liquid Biopsy) | Designed for liquid biopsy; slightly lower sensitivity than tissue-based assays for rare variants. | 10–14 days | EGFR, ALK, BRAF, KRAS, MET, RET, PIK3CA, ERBB2 (HER2), FGFR1/2/3, MSI |
| Molecular Marker | Biological Function of Affected Genes | Diagnostic Role | Therapeutic Value |
|---|---|---|---|
| IDH1 (R132) or IDH2 (R172) mutation | Gain-of-function mutation | Distinguishes diffuse gliomas with IDH mutation from IDH-wild-type glioblastomas or other gliomas | Predictive biomarker for treatment with Vorasidenib in IDH-1 or IDH-2-mutant low-grade gliomas |
| 1p/19q codeletion | Inactivation of putative tumor suppressor genes on 1p (such as FUBP1) and 19q (such as CIC) | Distinguishes IDH-mutant oligodendroglioma and 1p/19q-codeleted from IDH-mutant astrocytoma | Different therapeutic management |
| Loss of nuclear ATRX | Cell proliferation and longevity promoter with telomere lengthening activity | Characteristic of tumors of astrocytic lineage | Specific therapeutic management of astrocytic tumors |
| Histone H3 K27M | Missense mutations affect the epigenetic regulation of gene expression | Characteristic of the particular diffuse midline glioma, H3 K27M-mutant | Specific therapeutic management, radiotherapy alone as adjuvant treatment permitted |
| Histone H3.3 G34R/V mutation | Mutation that affects the epigenetic regulation of gene expression | Characteristic of the particular diffuse hemispheric glioma, H3.3 G34-mutant | Specific adjuvant management with Temozolomide chemoradiotherapy as standard |
| MGMT promoter methylation | DNA repair | None | Predictive biomarker for the benefit of alkylating ChT agents in IDH-wt glioblastoma (very important in frail or elderly patients) |
| Homozygous deletion of CDKN2A/CDKN2B | Encode kinase inhibitors and tumor suppressors functioning as regulators of Rb1 and p53-dependent signaling | Marker of poor outcome and WHO Grade 4 disease in IDH-mutant astrocytoma. | Specific adjuvant management with Temozolomide chemoradiotherapy |
| EGFR amplification | Impact on cellular proliferation, invasion, and resistance to induction of apoptosis | Molecular marker characteristic of glioblastoma, IDH wild type, WHO Grade 4 | Specific therapeutic management–Stupp protocol, with adjuvant Temozolomide for 6 months following Temozolomide chemoradiotherapy |
| TERT promotor alteration | Cell proliferation marker, which promotes cellular longevity via increased TERT expression | Molecular marker of glioblastoma, IDH wild type, WHO Grade 4 | Specific therapeutic management–Stupp protocol, with adjuvant Temozolomide for 6 months following Temozolomide chemoradiotherapy |
| +7/−10 cytogenetic signature | Gain of chromosome 7 combined with loss of chromosome 10, meaning gain of genes such as PDGFA and EGFR simultaneous with the loss of PTEN and MGMT | Molecular marker of glioblastoma, IDH wild type, WHO Grade 4 | Specific therapeutic management–Stupp protocol, with adjuvant Temozolomide for 6 months following Temozolomide chemoradiotherapy |
| BRAF V600E mutation | Oncogenic driver mutation that leads to the activation of the MAPK pathway | Rare in adult diffuse gliomas | Amenable to pharmacological intervention with BRAF inhibitors (Dabrafenib ± Trametinib, Vemurafenib ± Cobimetinib) |
| Therapy | Targeted Molecular Alteration(s) | ESCAT | Key Clinical Trial(s) and Relevant Literature | Molecular Tests Performed | Tumors Included | Trial Design | Trial Outcomes | Toxicity and AEs From |
|---|---|---|---|---|---|---|---|---|
| Larotrectinib (First-Generation NTRKi) | TRKA/B/C | IC | NAVIGATE [28] (NCT02576431 NCT02122913) | NGS, FISH | Soft tissue sarcomas, salivary gland tumors, thyroid, lung, colorectal, melanoma, breast, pancreatic, and primary CNS tumors. | Phase 2 basket trial that enrolled 55 patients, both adults and children, with TRK fusion-positive tumors. | The most common are fatigue, dizziness, and nausea. Serious (Grade ≥ 3): 13% of patients, primarily elevated liver enzymes. No treatment-related deaths. | |
| SCOUT [29] (NCT02637687) | NGS, FISH | Infantile fibrosarcoma, thyroid, CNS tumors, and other solid tumors in children. | Phase 1/2 trial enrolled 24 pediatric patients with locally advanced or metastatic solid or CNS tumors, 17 of which had NTRK fusion-positive tumors. Larotrectinib was administered orally, twice daily, on a continuous 28 day cycle in increasing dose levels. | Demonstrated antitumor activity for all patients with TRK fusion-positive tumors at a dose of 100 mg/m2 (cap of 100 mg), ORR 93%. | ||||
| VICTORIA [30] | NA | Protocol-driven, an exact-matching analysis comparing 82 patients with TRK fusion-positive cancers treated with Larotrectinib in clinical trials with TRK fusion-positive treated with other non-TRK inhibitor therapies in a real-world setting. | Improved OS (NR vs. 37.2 months, HR 0.44, 95% CI 0.23–0.83), longer time to next therapy, duration of therapy, and PFS (36.8 vs. 5.2 months, HR 0.29, 95% CI 0.18–0.46). | |||||
| Entrectinib (First-Generation NTRKi) | TRKA/B/C, ROS1, ALK | IC | ALKA-372-001 (EudraCT 2012-000148-88) and STARTRK-1 (NCT02097810) [31] | NGS, FISH | NSCLC, colorectal, breast, pancreatic, thyroid, and salivary gland tumors. | Two Phase I trials assessed the safety, tolerability, and preliminary efficacy in 119 adults with advanced or metastatic tumors harboring fusions in the NTRK1/2/3, ROS1, or ALK genes. | Demonstrated a favorable safety profile with preliminary antitumor activity and established the recommended dose of 600 mg of Entrectinib daily. | Most common: fatigue, dysgeusia, dizziness. Serious (Grade ≥ 3): eosinophilic myocarditis, cognitive disturbance, fatigue—resolved with dose interruption. No treatment-related deaths. |
| STARTRK-2 [32] (NCT02568267) | NGS, FISH | NSCLC, colorectal, breast, pancreatic, thyroid, soft tissue sarcomas, and salivary gland tumors. | Phase II, basket trial, evaluating the efficacy and safety of Entrectinib 600 mg daily in patients with tumors with NTRK1/2/3, ROS1, and ALK gene functions. | ORR for NTRK fusion-positive tumors: 57.4% (95% CI 43.2–70.8); mDoR 10.4 months; mPFS 11.2 months; mOS 20.9 months. | Most common: Grade 1–2 dysgeusia (47.1%), constipation (27.9%), fatigue (27.9%). Serious (Grade ≥ 3): anemia (11.8%), weight increase (10.3%). No treatment-related deaths. | |||
| STARTRK-NG [33] (NCT02650401) | NGS, FISH | Neuroblastoma, infantile fibrosarcoma, glioblastoma, high-grade gliomas, medulloblastoma, soft tissue sarcomas, Ewing sarcoma, rhabdomyosarcoma. | Phase I/II, open-label, dose-escalation, and expansion study in 47 pediatric and young adult patients with solid tumors or primary CNS tumors harboring NTRK1/2/3, ROS1, or ALK gene fusions. | Established the recommended phase II dose for pediatric patients; observed objective responses in NTRK fusion-positive tumors (ORR 57.7%, 95% CI 36.9–76.7, mDoR NR, mDoT 10.6 months, 4.2–18.4 months), indicating potential efficacy in the pediatric population. | Safety profile consistent with adult studies; common AEs included fatigue, gastrointestinal symptoms, and increased liver enzymes; no new safety signals were identified in the pediatric population. | |||
| Repotrectinib (Second-Generation NTRKi) | TRKA/B/C, ROS1, ALK | IC | (ongoing) TRIDENT-1 [34] (NCT03093116) | NGS | NSCLC, colorectal, breast, pancreatic, thyroid, soft tissue sarcomas, and salivary gland tumors. | Phase I/II, open-label, multicenter study in patients with advanced solid tumors harboring specific gene fusions. Includes both treatment-naïve and pretreated patients. | Current data are available only for ROS1 fusion-positive advanced NSCLC [34]. The trial determined a recommended dose of 160 mg daily Repotrectinib for 14 days, followed by 160 mg twice daily. For treatment-naïve tumors: ORR 79% (95% CI, 68–88%), mDoR 34.1 months, mPFS 35.7 months. For ROS1 TKI-pretreated patients: ORR 38% (95% CI, 25–52%), mDoR 14.8 months, mPFS 9 months. Data are immature for NTRK-positive tumor agnostics. | Most common: dizziness (58%), dysgeusia (50%), paresthesia (30%). Serious (Grade ≥ 3): reported in 29% of patients—anemia, increased blood creatine kinase levels, dizziness. No treatment-related deaths. |
| Selpercatinib | RET gene fusions and mutations | IC | LIBRETTO-001 [35,36,37] (NCT03157128) | NGS, FISH | NSCLC, MTC, and PTC thyroid cancer, pancreatic cancer, and colorectal cancer. | Ongoing Phase I/II, open-label trial in patients with RET fusion-positive or RET-mutant cancers. | NSCLC (n = 105): ORR 85%; mDoR: 18.4 months. Thyroid (MTC, n = 143; PTC, n = 19): MTC: ORR 69%; mPFS: 23.6 months. PTC: ORR 79%. Agnostic non-thyroid, non-NSCLC, n = 45: ORR 57%; mDoR: 13.0 months. | Most common: dry mouth, diarrhea, hypertension, fatigue. Serious (Grade ≥ 3): hypertension, increased liver enzymes. No treatment-related deaths. |
| Pralsetinib | RET gene fusions and mutations | IC | ARROW [38,39,40,41] (NCT03037385) | NGS, FISH | NSCLC, MTC, PTC, pancreatic cancer, cholangiocarcinoma, neuroendocrine, SCLC, unknown primary, thymic, ovarian, head and neck, colorectal. | Phase I/II, open-label study evaluating RET fusion-positive or RET-mutant cancers. | NSCLC (n = 216): ORR 70% (95% CI: 62–77); mPFS: 17.1 months. Thyroid (RET-mutant MTC and RET fusion-positive thyroid cancer, n = 29): ORR 60%; mPFS: not reached. Agnostic (non-thyroid, non-NSCLC, n = 38): ORR 57% (95% CI: 42–71). | Most common: constipation (30%), dry mouth (26%), hypertension (24%), fatigue (23%). Serious (Grade ≥ 3): hypertension (15%), neutropenia (10%), anemia (8%). No treatment-related deaths. |
| Trial Name | Immunotherapy | Indication | Neoadjuvant Regimen | Design | MSI-H (No. of Patients) | Clinical Outcome |
|---|---|---|---|---|---|---|
| NEONIPIGA [103] (NCT04006262) | Nivolumab plus Ipilimumab | Localized esophageal and gastric adenocarcinoma | Nivolumab 240 mg once every 2 weeks ×6 and ipilimumab 1 mg/kg once every 6 weeks ×2, followed by surgery and adjuvant nivolumab 480 mg once every 4 weeks (nine injections). | Phase II, prospective-single-arm, open-label | 32 | 29/32 patients underwent surgery, 17/29 had pCR. |
| NICHE-1 [104] (NCT03026140) | Nivolumab plus Ipilimumab | Colon cancer | 1 mg/kg Ipilimumab (1 dose) and 3 mg/kg Nivolumab (2 doses), followed by surgery. | Phase II, prospective-single-arm, open-label | 20 | All patients responded, with 19/20 having an MPR and 12/20 achieving pCR. |
| NICHE-2 [105] (NCT03026140) | Nivolumab plus Ipilimumab | Colon cancer | 1 mg/kg Ipilimumab (1 dose) and 3 mg/kg Nivolumab (2 doses), followed by surgery. | Phase II, prospective-single-arm, open-label | 115 | 113/115 had surgery, 109/111 had a response, 105 had MPR, and 75 achieved pCR. |
| Cercek et al. [101] (NCT04165772) | Dostarlimab | Rectal cancer | 500 mg q3w for 6 months (9 cycles), followed by RT (50.4 Gy/28 fractions with concurrent Capecitabine at standard doses) and then TME if no cCR. | Phase II, prospective-single-arm | 12 | 100% cCR |
| Ludford et al. [106] (NCT04082572) | Pembrolizumab | Colorectal cancer | 200 mg q3w for 6 months, followed by surgical resection, with an option to continue therapy for 1 year. | Phase II, open-label, single-center trial | 35 (27 CRC, 8 non-CRC) | 17/35 underwent surgery. Of these, 14 had CRC, and 11/14 had pCR. |
| Targetable Oncogenic Alteration | Drug | Setting | Trial | Design | ORR | mPFS/DFS in mo. (HR) | mOS in mo. (HR) |
|---|---|---|---|---|---|---|---|
| EGFR typical and atypical mutations | Afatinib * | First line | LUX-Lung 3/6 [122,123,124] (NCT00949650; NCT01121393) | Phase 3 open-label trial comparing Afatinib to platinum-based ChT in Asian and Western patients. | 66% | 11.0 vs. 6.9 (HR: 0.58) | 27.3 vs. 24.3 (HR: 0.81) |
| Subsequent post-ChT | LUX-Lung 2 [125,126] (NCT00525148) | Phase 2 single-arm trial | 58% | 4.4 | 24.8 | ||
| Erlotinib * | First line | EURTAC [127] (NCT00446225) | Phase 3 open-label trial comparing Erlotinib to ChT | 58% | 9.7 vs. 5.2 (HR: 0.37) | 19.3 (NR for chemo) | |
| Subsequent post-ChT | NCIC-CTG [128] | Phase 3 open-label trial comparing Erlotinib to ChT | 8.9% | 2.2 vs. 1.8 (HR: 0.61) | 6.7 vs. 4.7 (HR: 0.70) | ||
| Dacomitinib * | First line | ARCHER1050 [129,130] (NCT01774721) | Phase 3 double-blind trial comparing Dacomitinib to Gefitinib | 74.9% | 14.7 vs. 9.2 (HR: 0.59) | 34.1 vs. 26.8 (HR: 0.76) | |
| Gefitinib * | First line | NEJ002 [131,132] (UMIN-CTR, C000000376) | Phase 3 open-label trial comparing Gefitinib to ChT | 73.7% | 10.8 vs. 5.4 (HR: 0.30) | 30.5 vs. 23.6 (HR: 0.72) | |
| Osimertinib * | Adjuvant | ADAURA [115,133] (NCT02511106) | Phase 3 double-blind trial comparing Osimertinib to placebo as adjuvant 3 year-treatment after surgical resection of Stage IB-IIIA NSCLC | NA | NR vs. 27.5 months (HR: 0.20) | 5-yr OS: 88% vs. 78% (HR: 0.49) | |
| Post-RT consolidation | LAURA [116] (NCT03521154) | Phase 3 double-blind trial comparing Osimertinib to placebo as consolidation treatment | NA | 39.1 vs. 5.6 (HR: 0.16) | Data not yet mature | ||
| First line | FLAURA [113,134] (NCT02296125) | Phase 3 double-blind trial comparing Osimertinib to first-generation EGFR TKI in first-line metastatic EGFR-positive (exon 19 deletion or L858R) NSCLC | 80% | 18.9 vs. 10.2 (HR: 0.46) | 38.6 vs. 31.8 (HR: 0.80) | ||
| First line + ChT | FLAURA2 [114] (NCT04035486) | Ongoing Phase 3 trial investigating the addition of chemotherapy to first-line Osimertinib | 83% | 29.4 vs. 19.9 (HR 0.62) | Data not yet mature | ||
| Subsequent post-ChT | AURA3 [135,136] (NCT02151981) | Phase 3 double-blind trial comparing Osimertinib to platinum-pemetrexed chemotherapy for treatment of T790M EGFR-mutant metastatic NSCLC. | 71% | 10.1 vs. 4.4 (HR: 0.30) | 26.8 vs. 22.5 (HR: 0.87) | ||
| Amivantamab | First line + ChT | PAPILLON [137] (NCT04538664) | Ongoing Phase 3 trial investigating the addition of Amivantamab to platinum ChT in EGFR exon 20 insertion mutations | 73% | 11.4 vs. 6.7 (HR: 0.40) | Data not yet mature | |
| First line + Lazertinib | MARIPOSA [138] (NCT04487080) | Ongoing Phase 3 trial investigating the addition of Amivantamab to Lazertinib, in comparison with Osimertinib | 86% | 23.7 vs. 16.6 (HR: 0.70) | Data not yet mature | ||
| HER2 mutation (IHC3+) | T-DXd | Subsequent lines | DESTINY-Lung02 [139] (NCT04644237) | Phase 2 single-arm trial investigating T-DXd for previously treated (platinum-ChT) patients with Her2 mutation-positive patients | 49% | 9.9 | 19.5 |
| KRAS G12C | Sotorasib | Subsequent lines | CodeBreak200 [140] (NCT04303780) | Phase 3 double-blind trial comparing Sotorasib to Docetaxel in patients with previously treated metastatic NSCLC with KRAS G12C mutation | 28% | 5.6 vs. 4.5 (HR: 0.66) | 10.6 vs. 11.3 months (HR: 1.01) |
| Adagrasib | Subsequent lines | KRYSTAL-1 [141] (NCT03785249) | Phase 2 single-arm trial | 42.9% | 6.5 | 12.6 | |
| RET rearrangement | Selpercatinib | First line | LIBRETTO-001 [37] (NCT03157128) | Phase 1/2 basket trial | 84% | 20.3 | Not available |
| Pralsetinib | First line | ARROW [40] (NCT03037385) | Phase 1/2 basket trial | 70% | 16.5 | Not available | |
| Cabozantinib | Subsequent lines | Drilon et al, 2016 [142] NCT01639508 | Phase 2, single-center, open-label, Simon two-stage trial investigating the effectiveness of Cabozantinib in RET rearranged metastatic NSCLC | 31% | 5.5 | 9.9 | |
| ALK rearrangement | Crizotinib | First line | PROFILE 1014 [143] (NCT01154140) | Phase 3 double-blind trial comparing Crizotinib to ChT in the first line setting for ALK fusion-positive metastatic NSCLC | 74% | 10.9 vs. 7 (HR 0.45) | 47.5 vs. 47.7 (HR 1.00) |
| Subsequent post-ChT | Shaw et al, 2013 [144] (NCT00932893) | Phase 3 open-label trial comparing Crizotinib to ChT in previously ChT-treated ALK fusion-positive metastatic NSCLC patients | 65% | 7.7 vs. 3.0 (HR 0.49) | 20.3 vs. 22.8 (HR 1.02) | ||
| Ceritinib | First line | ASCEND-4 [145,146] (NCT01828099) | Phase 3 open-label trial comparing Ceritinib to ChT | 72.5% | 16.6 vs. 8.1 (HR: 0.55) | NR vs. 26.2 (HR 0.73) | |
| Subsequent post-ChT | ASCEND-5 [147] (NCT01828112) | Phase 3 double-blind trial comparing Ceritinib to ChT | 39.1% | 5.4 vs. 1.6 (HR: 0.49) | NR vs. 20.0 | ||
| Brigatinib | First line | ALTA-1L [148,149,150] (NCT02737501) | Phase 3 open-label trial comparing Brigatinib to Crizotinib | 74% | 24.0 vs. 11.0 (HR: 0.49) | NR vs. 52.2 | |
| Subsequent lines | ALTA [151,152] (NCT02094573) | Phase 2 single-arm trial investigating Brigatinib in Crizotinib-refractory ALK fusion-positive metastatic NSCLC | 53% | 15.6 | 34.1 | ||
| Alectinib | First/subsequent lines | ALEX [153,154] (NCT02075840) | Phase 3 open-label trial, compared with Crizotinib | 82.9% | 25.8 vs. 12.7 (HR: 0.51) | 5-yr OS: 62.5% vs. 45.5% (HR 0.67) | |
| Ensartinib | First line | eXalt3 [155] (NCT02767804) | Phase 3 open-label trial, compared with Crizotinib | 75% | 25.8 vs. 12.7 (HR: 0.51) | 5-yr OS: 78% vs. 78% | |
| Lorlatinib | First/subsequent lines | CROWN [119,156,157] (NCT03052608) | Phase 3 double-blind trial, compared with Crizotinib | 81% | NR vs. 9.1 (HR: 0.19) | Data not yet mature | |
| ROS1 rearrangement | Crizotinib | First line | PROFILE 1001 [158,159] (NCT00585195) | Phase 1/2 single-arm trial | 72% | 19.2 | 51.4 |
| Entrectinib | First line | STARTRK-1, -2 and ALKA-001 [160,161] (NCT02097810; NCT02568267; EudraCT, 2012–000148–88 | Integrated analysis of three Phase 1/2 trials investigating the efficiency of Entrectinib in ROS1 rearrangement-positive tumors | 77% | 19 | 47.8 | |
| Repotrectinib | First/subsequent lines | TRIDENT-1 [34] (NCT03093116) | Phase 1/2 basket trial, investigating first line or subsequent line Repotrectinib in tumors harboring ROS1, NTRK1-3, ALK gene fusions, including metastatic NSCLC. | 79% in the first line | 35.7 in the first line | Not estimable in the first line | |
| 38% post-TKI | 9 post-TKI | 25.1 post-TKI | |||||
| Lorlatinib | First/subsequent lines | Shaw et al, 2019 [162] (NCT01970865) | Open-label, single-arm Phase 1/2 trial investigating Lorlatinib in ROS1-positive NSCLC | 62% in the first line | 21.0 in the first line | Not available | |
| 35% post-TKI | 8.5 post-TKI | Not available | |||||
| MET exon 14 skipping mutation | Capmatinib | First/subsequent lines | GEOMETRY mono-1 [163,164] (NCT02414139) | Phase 2 single-arm trial | 41% in first line | 12.5 in first line | 21.4 in first line |
| 44% post-TKI | 5.5 post-TKI | 16.8 in first line | |||||
| Tepotinib | First/subsequent lines | VISION [165,166] (NCT02864992) | Phase 2 single-arm trial | 57.3% in first line | 12.6 in first line | 21.3 in first line | |
| 45.0% in pretreated | 11 in pretreated | 19.3 in pretreated | |||||
| Crizotinib | First/subsequent lines | Drilon et al., 2021 [167] (NCT00585195) | Phase 2 single-arm trial | 32% | 7.3 | 20.5 | |
| BRAF V600E | Dabrafenib + Trametinib | First/subsequent lines | Planchard et al, 2017 [168,169] (NCT01336634) | Phase 2 single-arm | 63.9% in first line | 10.8 in first line | 17.3 in first line |
| 68.4% in pretreated | 10.2 in pretreated | 18.2 in pretreated | |||||
| Encorafenib + Binimetinib | First/subsequent lines | Riely et al, 2023 [170] (NCT03915951) | Phase 2 single-arm | 75% in first line | NE in first line | Not available | |
| 46% in pretreated | 9.3 in pretreated | ||||||
| NTRK1/2/3 gene fusion | Larotrectinib | First/subsequent lines | Drilon et al, 2018 [171] (NCT02576431 NCT02122913) | Retrospective analysis of multiple Phase 1/2 single-arm trials | 73% | 35.4 | 40.7 |
| Entrectinib | First/subsequent lines | Paz-Ares et al, 2019 [172,173] ALKA (EudraCT 2012-000148-88), STARTRK-1, -2 (NCT02097810; NCT02568267) | Integrated analysis of multiple Phase 1/2 single-arm trials enrolling patients treated with Entrectinib for NTRK fusion-positive tumors, including metastatic NSCLC | 62.7% | 27.3 | 41.5 | |
| Repotrectinib | First/subsequent lines | TRIDENT-1 (NCT03093116) | Ongoing Phase 1/2 basket trial, results published for patients with ROS1 fusion (see above). | Not Available | Not Available | Not Available | |
| NRG1 gene fusion | Zenocutuzumab | Subsequent lines | eNRGy [174] (NCT02912949) | Ongoing Phase 2 single-arm trial | Not Available | Not Available | Not Available |
| PARP inhibitor | Cancer Treated | Clinical Setting | Clinical Trial | Trial Design | mPFS/DFS in mo. (HR) | mOS in mo. (HR) |
|---|---|---|---|---|---|---|
| Olaparib | Ovarian | Maintenance post-ChT | SOLO-1 [188,189] (NCT01844986) | Phase 3 double-blind trial vs. placebo, which included 391 patients with gBRCA1/2m, treated until PD/unacceptable toxicity or no evidence of disease after 2 years of treatment with Olaparib 300 mg bid. | 56.0 vs. 13.8 (0.33) | NR vs. 75.2 (0.55) |
| Maintenance post-ChT (with Bevacizumab) | PAOLA-1 [190,191] (NCT02477644) | Phase 3 double-blind trial vs. placebo, which included 806 patients with HRD-positive tumors, treated with Bevacizumab 15 mg/kg IV q3w until PD/unacceptable toxicity, or up to 15 months of treatment (including the period when Bevacizumab was offered as primary treatment), and Olaparib 300 mg bid as maintenance until PD/unacceptable toxicity or up to 2 years. | 22.1 vs. 16.6 (0.59) | 75.2 vs. 57.3 (0.62) | ||
| Breast | Adjuvant | OlympiA [192,193] (NCT02032823) | Phase 3 double-blind trial vs. placebo, which included 1836 patients with gBRCA1/2m high-risk, HER2-negative early breast cancer for 1 year of treatment with adjuvant 300 mg bid Olaparib. | NR (Δ4yr-iDFS = 7.3%, HR: 0.63) | NR (Δ4yr-OS = 3.4%, HR: 0.68) | |
| Metastatic | OlympiAD [194,195,196] (NCT02000622) | Phase 3 open-label trial vs. chemotherapy (physician’s choice), which included 302 patients with gBRCA1/2m and HER2-negative advanced breast cancer who received Olaparib 300 mg bid until PD/unacceptable toxicities. | 7.0 vs. 4.2 (0.58) | 22.6 vs. 14.7 (0.55) | ||
| Prostate | Second line mCRPC (monotherapy) | PROfound [197] (NCT02987543) | In a Phase 3 open-label trial, Cohort A included 245 patients with alterations in BRCA1, BRCA2, or ATM, previously treated with Enzalutamide or Abiraterone. Patients were randomized 2:1 to receive Olaparib 300 mg bid or a novel hormonal agent (physician’s choice between Enzalutamide or Abiraterone). | 7.4 vs. 3.6 (0.34) | 18.5 vs. 15.1 (0.64) | |
| First line mCRPC (with Abiraterone) | PROpel [198,199] (NCT03732820) | Phase 3 double-blind trial vs. placebo, which included 796 patients with mCRPC who received Olaparib 300 mg bid plus Abiraterone 1000 mg daily vs. placebo plus Abiraterone as first-line treatment, regardless of HRD status. | 24.8 vs. 16.6 (HR: 0.66) | 42.1 vs. 34.7 (HR: 0.81) | ||
| Pancreatic | Maintenance | POLO [200,201] (NCT02184195) | Phase 3 double-blind trial vs. placebo. Patients with gBRCA1/2m pancreatic adenocarcinoma who did not progress after 16 weeks of first-line platinum-based ChT received maintenance Olaparib 300 mg bid until PD/unacceptable toxicity. | 7.4 vs. 3.8 (HR: 0.53) | 19.0 vs. 19.2 (HR: 0.83; not significant) | |
| Endometrial | Advance/Recurrent | DUO-E/GOG-3041/ENGOT-EN10 [202] (NCT04269200) | Phase 3 double-blind trial evaluating Olaparib in combination with Durvalumab as maintenance therapy after primary ChT plus Durvalumab for 718 patients with advanced endometrial cancer. | 15.1 vs. 9.6 (HR: 0.55) | NR vs. 25.9 (HR: 0.59) | |
| Niraparib | Ovarian | Maintenance post-ChT | PRIMA [203,204] (NCT02655016) | Phase 3 double-blind trial vs. placebo, investigating maintenance Niraparib 300 mg daily for up to 36 months in patients who responded to primary platinum-based ChT, regardless of HRD status. | 13.8 vs. 8.2 (HR: 0.62 in the overall population) 21.9 vs. 10.4 (HR: 0.43 in patients with HRD-positive) | No significant difference in OS in the overall population. |
| Prostate | mCRPC (with Abiraterone) | MAGNITUDE [205] (NCT03748641) | Phase 3 double-blind trial vs. placebo, investigating the efficiency of Niraparib added to Abiraterone in 423 patients with HRD-positive and 247 with no HRD alterations. | 16.5 vs. 13.7 (HR: 0.73 in the HRD-positive group, while HRD-negative was closed for futility) | NA | |
| Rucaparib | Ovarian | Maintenance post-ChT | ARIEL3 [206,207] (NCT01968213) | Phase 3 open-label trial vs. physician’s choice, which investigated the efficiency of Rucaparib 600mg bid for up to 24 months as maintenance in 564 patients who responded to primary platinum-based ChT. | 10.8 vs. 5.4 (HR: 0.36 in the overall population, regardless of BRCA1/2m or HRD status) | No significant difference in OS in the overall population. |
| Prostate | mCRPC monotherapy | TRITON3 [208] (NCT02975934) | Phase 3 open-label trial vs. physician’s choice in patients with mCRPC who progressed after first-line treatment (novel hormonal agent or docetaxel). Patients (405) with BRCA1/2m or ATM alteration were randomized 2:1. | 10.2 vs. 6.4 (HR: 0.61 in the overall population) 11.2 vs. 6.4 (HR: 0.50 in the BRCA1/2m population) | NA | |
| Talazoparib | Breast | Metastatic | EMBRACA [209,210] (NCT01945775) | Phase 3 open-label trial, which enrolled 431 patients with gBRCA1/2m advanced breast cancer to compare Talazoparib 1 mg/day to physician’s choice single-agent ChT. | 8.6 vs. 5.6 (HR: 0.55) | No significant difference in mOS. |
| Prostate | mCRPC (with Enzalutamide) | TALAPRO-2 [211,212] (NCT03395197) | Phase 3 open-label trial, enrolling 805 patients to investigate the efficiency of Talazoparib and Enzalutamide in first-line treatment of mCRPC, regardless of HRD status. Another analysis presented data for the HRD-positive cohort, 399 patients, investigating the efficiency of Talazoparib 1mg/day added to Enzalutamide as first-line therapy of mCRPC. | rPFS: NR vs. 13.8 (HR: 0.45 for HRD-positive) rPFS: NR vs. 21.9 (HR: 0.63 for all participants) | Data are immature. |
| Biomarker | FDA Approved Therapies | Clinical Trial | Trial Design | Trial Outcomes |
|---|---|---|---|---|
| PIK3CA activating mutation | Inavolisib + Palbociclib + Fulvestrant | INAVO120 [217] (NCT04191499) | The 325 patients with ER-positive, HER2-negative ABC, who progressed within 12 months after the completion of adjuvant endocrine therapy, were randomized to receive Inavolisib 9mg daily or placebo, with Fulvestrant and Palbociclib. | In the ongoing study, mPFS was improved (15 months vs. 7.3 months, HR 0.43, 95% CI 0.32–0.59 p < 0.001), but with higher toxicities associated. Data for OS are still immature. |
| Alpelisib + Fulvestrant | SOLAR-1 [218,219] (NCT02437318) | A randomized, Phase 3 trial enrolled 572 patients with ER-positive, HER2-negative ABC, who progressed on previous endocrine therapy. | Improved PFS (11.0 vs. 5.7 months; HR = 0.65, p < 0.001) in PIK3CA-mutated tumors. There is no PFS/OS benefit for patients without PIK3CA mutation. | |
| Capivasertib + Fulvestrant (active on PIK3CA or AKT1 activating mutations, as well as PTEN alterations) | CAPItello-291 [220] (NCT04305496) | The 708 patients with HER2-negative, ER-positive, and ABC who progressed on first-line CDK4/6 inhibitor were enrolled in a Phase 3, randomized, double-blind trial comparing the addition of Capivasertib to Fulvestrant with placebo. | Significant improvement in PFS (7.2 vs. 3.6 months; HR = 0.60, p < 0.001); OS data pending. | |
| ESR1 mutation | Elacestrant | EMERALD [221] (NCT03778931) | The 477 patients with ER-positive/HER2-negative ABC, who had 1–2 line(s) of endocrine therapy (CDK4/6 inhibitor, and ≤1 ChT) were randomized in an open-label, Phase III trial to receive Elacestrant 400 mg/day or SoC endocrine monotherapy. | PFS benefit both for ESR1-positive (3.8 vs. 1.9 months; HR = 0.55, p < 0.001) and for the general population (2.8 vs. 1.9 months; HR = 0.70); OS trend favoring Elacestrant only for ESR1-positive. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galeș, L.N.; Păun, M.-A.; Butnariu, I.; Simion, L.; Manolescu, L.S.C.; Trifănescu, O.G.; Anghel, R.M. Next-Generation Sequencing in Oncology—A Guiding Compass for Targeted Therapy and Emerging Applications. Int. J. Mol. Sci. 2025, 26, 3123. https://doi.org/10.3390/ijms26073123
Galeș LN, Păun M-A, Butnariu I, Simion L, Manolescu LSC, Trifănescu OG, Anghel RM. Next-Generation Sequencing in Oncology—A Guiding Compass for Targeted Therapy and Emerging Applications. International Journal of Molecular Sciences. 2025; 26(7):3123. https://doi.org/10.3390/ijms26073123
Chicago/Turabian StyleGaleș, Laurenția Nicoleta, Mihai-Andrei Păun, Ioana Butnariu, Laurentiu Simion, Loredana Sabina Cornelia Manolescu, Oana Gabriela Trifănescu, and Rodica Maricela Anghel. 2025. "Next-Generation Sequencing in Oncology—A Guiding Compass for Targeted Therapy and Emerging Applications" International Journal of Molecular Sciences 26, no. 7: 3123. https://doi.org/10.3390/ijms26073123
APA StyleGaleș, L. N., Păun, M.-A., Butnariu, I., Simion, L., Manolescu, L. S. C., Trifănescu, O. G., & Anghel, R. M. (2025). Next-Generation Sequencing in Oncology—A Guiding Compass for Targeted Therapy and Emerging Applications. International Journal of Molecular Sciences, 26(7), 3123. https://doi.org/10.3390/ijms26073123