
Single-Nucleotide Polymorphisms in the Thioredoxin Antioxidant System and Their Association with Diabetic Nephropathy in Slovenian Patients with Type 2 Diabetes—A Preliminary Study


Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
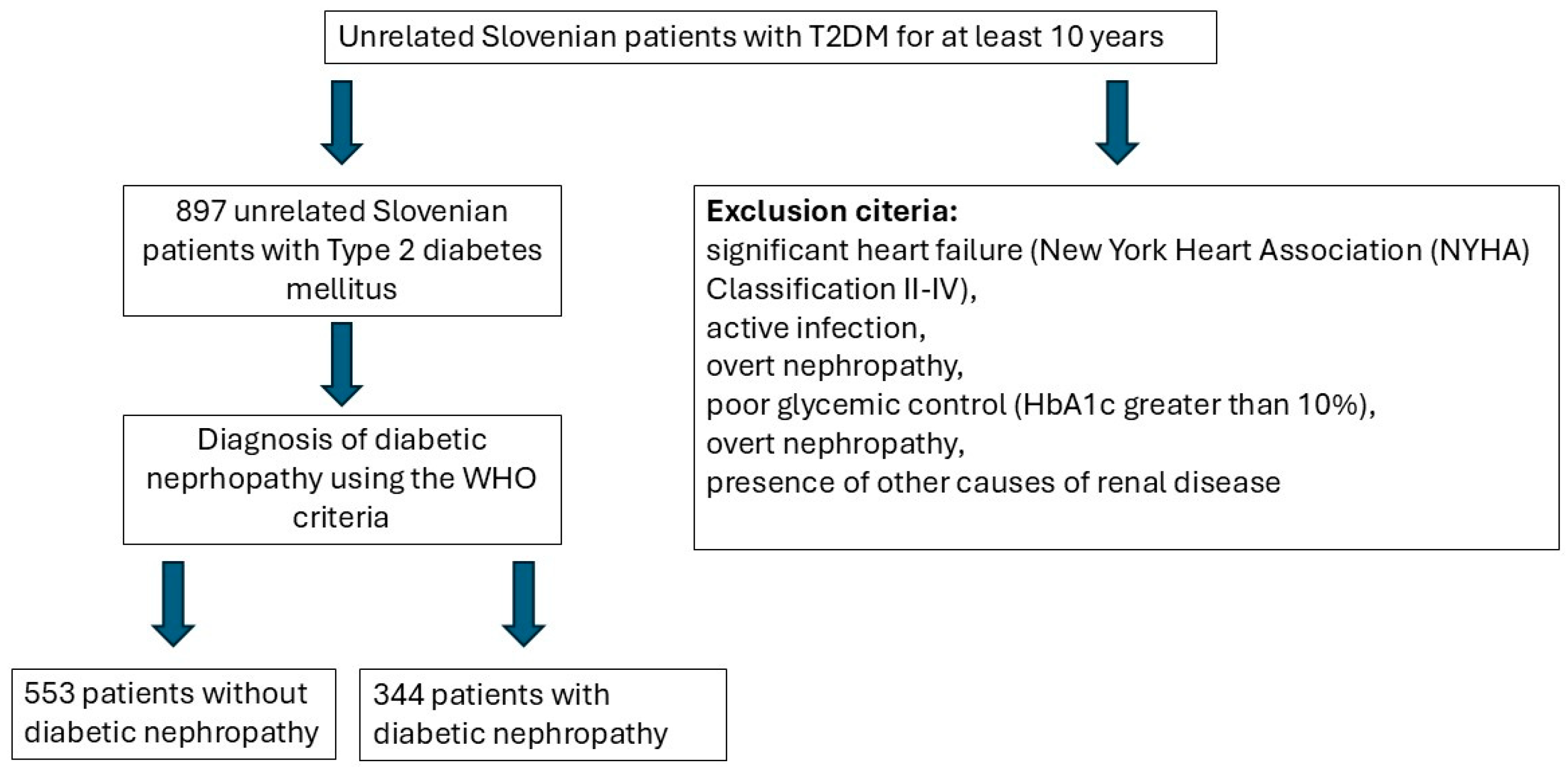
4.1. Patients
4.2. Biochemical Analysis
4.3. Genotyping
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| T2DM | type 2 diabetes mellitus |
| SBP | systolic blood pressure |
| DBP | diastolic blood pressure |
| BMI | body mass index |
| CVD | cardiovascular disease |
| DR | diabetic retinopathy |
| Hb | hemoglobin |
| eGFR | estimated glomerular filtration rate |
| HDL | high-density lipoprotein cholesterol |
| LDL | low-density lipoprotein cholesterol |
| TGS | triglycerides |
| DN | diabetic nephropathy |
| ROS | reactive oxygen species |
| CKD | chronic kidney disease |
| ESKD | end-stage kidney disease |
| TXN | thioredoxin |
| TXNIP | thioredoxin-interacting protein |
| TXNRD | thioredoxin reductase |
| OR | odds ratio |
| CI | confidence interval |
| ASK1 | apoptosis signal-regulating kinase 1 |
| NYHA | New York Heart Association |
| WHO | World Health Organization |
| IL-1β | interleukin 1 β |
| IL-18 | interleukin 18 |
| MAF | minor allele frequency |
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Cole, J.B.; Florez, J.C. Genetics of diabetes mellitus and diabetes complications. Nat. Rev. Nephrol. 2020, 16, 377–390. [Google Scholar] [CrossRef] [PubMed]
- Faselis, C.; Katsimardou, A.; Imprialos, K.; Deligkaris, P.; Kallistratos, M.; Dimitriadis, K. Microvascular Complications of Type 2 Diabetes Mellitus. Curr. Vasc. Pharmacol. 2020, 18, 117–124. [Google Scholar] [CrossRef]
- Selby, N.M.; Taal, M.W. An updated overview of diabetic nephropathy: Diagnosis, prognosis, treatment goals and latest guidelines. Diabetes Obes. Metab. 2020, 22 (Suppl. 1), 3–15. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.; Liu, T.; Qiao, Y.; Liu, D.; Yang, L.; Mao, H.; Ma, F.; Wang, Y.; Peng, L.; Zhan, Y. Oxidative stress and inflammation in diabetic nephropathy: Role of polyphenols. Front. Immunol. 2023, 14, 1185317. [Google Scholar] [CrossRef] [PubMed]
- Palma, F.R.; Gantner, B.N.; Sakiyama, M.J.; Kayzuka, C.; Shukla, S.; Lacchini, R.; Cunniff, B.; Bonini, M.G. ROS production by mitochondria: Function or dysfunction? Oncogene 2024, 43, 295–303. [Google Scholar] [CrossRef]
- Lu, J.; Holmgren, A. The thioredoxin antioxidant system. Free Radic. Biol. Med. 2014, 66, 75–87. [Google Scholar] [CrossRef]
- Bjørklund, G.; Zou, L.; Wang, J.; Chasapis, C.T.; Peana, M. Thioredoxin reductase as a pharmacological target. Pharmacol. Res. 2021, 174, 105854. [Google Scholar] [CrossRef] [PubMed]
- Pan, M.; Zhang, F.; Qu, K.; Liu, C.; Zhang, J. TXNIP: A Double-Edged Sword in Disease and Therapeutic Outlook. Oxid. Med. Cell. Longev. 2022, 2022, 7805115. [Google Scholar] [CrossRef] [PubMed]
- Ji, L.; Wang, Q.; Huang, F.; An, T.; Guo, F.; Zhao, Y.; Liu, Y.; He, Y.; Song, Y.; Qin, G. FOXO1 Overexpression Attenuates Tubulointerstitial Fibrosis and Apoptosis in Diabetic Kidneys by Ameliorating Oxidative Injury via TXNIP-TRX. Oxid. Med. Cell. Longev. 2019, 2019, 3286928. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Sun, R.; Hua, Y.; Lu, Q.; Shao, X. An update on the role of thioredoxin-interacting protein in diabetic kidney disease: A mini review. Front. Med. 2023, 10, 1153805. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.N.C.; Loomis, S.J.; Kang, J.H.; Allingham, R.R.; Gharahkhani, P.; Khor, C.C.; Burdon, K.P.; Aschard, H.; Chasman, D.I.; Igo, R.P., Jr.; et al. Genome-wide association analysis identifies TXNRD2, ATXN2 and FOXC1 as susceptibility loci for primary open-angle glaucoma. Nat. Genet. 2016, 48, 189–194. [Google Scholar] [CrossRef]
- Vithana, E.N.; Khor, C.-C.; Qiao, C.; Nongpiur, M.E.; George, R.; Chen, L.-J.; Do, T.; Abu-Amero, K.; Huang, C.K.; Low, S.; et al. Genome-wide association analyses identify three new susceptibility loci for primary angle closure glaucoma. Nat. Genet. 2012, 44, 1142–1146. [Google Scholar] [CrossRef] [PubMed]
- Koutros, S.; Andreotti, G.; Berndt, S.I.; Barry, K.H.; Lubin, J.H.; Hoppin, J.A.; Kamel, F.; Sandler, D.P.; Burdette, L.A.; Yuenger, J.; et al. Xenobiotic-metabolizing gene variants, pesticide use, and the risk of prostate cancer. Pharmacogenetics Genom. 2011, 21, 615. [Google Scholar] [CrossRef] [PubMed]
- Sibbing, D.; Pfeufer, A.; Perisic, T.; Mannes, A.M.; Fritz-Wolf, K.; Unwin, S.; Sinner, M.F.; Gieger, C.; Gloeckner, C.J.; Wichmann, H.E.; et al. Mutations in the mitochondrial thioredoxin reductase gene TXNRD2 cause dilated cardiomyopathy. Eur. Heart J. 2011, 32, 1121–1133. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, A.; Maudhoo, A.; Chan, L.F.; Novoselova, T.; Prasad, R.; Metherell, L.A.; Guasti, L. Isolated glucocorticoid deficiency: Genetic causes and animal models. J. Steroid Biochem. Mol. Biol. 2019, 189, 73–80. [Google Scholar] [CrossRef]
- Homo_Sapiens—Ensembl Genome Browser 113. Available online: https://www.ensembl.org/Homo_sapiens/Info/Index (accessed on 27 December 2024).
- Alicic, R.Z.; Rooney, M.T.; Tuttle, K.R. Diabetic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2017, 12, 2032–2045. [Google Scholar] [CrossRef]
- Kariž, S.; Mankoč, S.; Petrovič, D. Association of thioredoxin reductase 2 (TXNRD2) gene polymorphisms with myocardial infarction in Slovene patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2015, 108, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Ramus, S.M.; Cilensek, I.; Petrovic, M.G.; Soucek, M.; Kruzliak, P.; Petrovic, D. Single nucleotide polymorphisms in the Trx2/TXNIP and TrxR2 genes of the mitochondrial thioredoxin antioxidant system and the risk of diabetic retinopathy in patients with Type 2 diabetes mellitus. J. Diabetes Complicat. 2016, 30, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Roumeliotis, A.; Roumeliotis, S.; Tsetsos, F.; Georgitsi, M.; Georgianos, P.I.; Stamou, A.; Vasilakou, A.; Kotsa, K.; Tsekmekidou, X.; Paschou, P.; et al. Oxidative Stress Genes in Diabetes Mellitus Type 2: Association with Diabetic Kidney Disease. Oxidative Med. Cell. Longev. 2021, 2021, 2531062. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, N.E.; Omae, S.; Pereira, A.; Rodrigues, M.V.; Miyakawa, A.A.; Campos, L.C.G.; Santos, P.C.; Dallan, L.A.; Martinez, T.L.; Santos, R.D.; et al. Thioredoxin interacting protein genetic variation is associated with diabetes and hypertension in the Brazilian general population. Atherosclerosis 2012, 221, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Alvim, R.O.; Santos, P.C.; Ferreira, N.E.; Mill, J.G.; Krieger, J.E.; Pereira, A.C. Thioredoxin interacting protein (TXNIP) rs7212 polymorphism is associated with arterial stiffness in the Brazilian general population. J. Hum. Hypertens. 2012, 26, 340–342. [Google Scholar] [CrossRef]
- Liang, T.; Wu, Z.; Du, S.; Hu, L. TXNIP Gene Single Nucleotide Polymorphisms Associated with the Risk of Type 2 Diabetes Mellitus in a Chinese Han Population. DNA Cell Biol. 2020, 39, 1513–1520. [Google Scholar] [CrossRef]
- Advani, A.; Gilbert, R.E.; Thai, K.; Gow, R.M.; Langham, R.G.; Cox, A.J.; Connelly, K.A.; Zhang, Y.; Herzenberg, A.M.; Christensen, P.K.; et al. Expression, Localization, and Function of the Thioredoxin System in Diabetic Nephropathy. J. Am. Soc. Nephrol. 2009, 20, 730–741. [Google Scholar] [CrossRef]
- Shah, A.; Xia, L.; Masson, E.A.Y.; Gui, C.; Momen, A.; Shikatani, E.A.; Husain, M.; Quaggin, S.; John, R.; Fantus, I.G. Thioredoxin-Interacting Protein Deficiency Protects against Diabetic Nephropathy. J. Am. Soc. Nephrol. 2015, 26, 2963–2977. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Xu, X.; Tang, C.; Gao, P.; Chen, X.; Xiong, X.; Yang, M.; Yang, S.; Zhu, X.; Yuan, S.; et al. Reactive oxygen species promote tubular injury in diabetic nephropathy: The role of the mitochondrial ros-txnip-nlrp3 biological axis. Redox Biol. 2018, 16, 32. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Case (N = 344) | Control (N = 553) | p Value | |
|---|---|---|---|
| Sex [M] | 201 (58.4%) | 318 (57.5%) | 0.78 |
| Age [years] a | 65.3 ± 9.4 | 65.4 ± 8.6 | 0.90 |
| Duration of T2DM [years] b | 16.0 [13.0–20.0] | 15.0 [12.0–19.0] | <0.001 |
| Duration of hypertension [years] b | 12.0 [7.0–18.0] | 11.0 [5.0–16.0] | 0.0058 |
| SBP [mmHg] b | 155.0 [142.7–167.0] | 145.0 [135.0–160.0] | <0.001 |
| DBP [mmHg] b | 85.0 [77.0–90.0] | 80.0 [75.0–90.0] | 0.0759 |
| BMI a | 30.39 ± 3.56 | 29.94 ± 3.91 | 0.08 |
| Waist circumference a | 108.56 ± 10.41 | 104.59 ± 11.78 | <0.001 |
| Active smokers | 32 (9.3%) | 70 (12.7%) | 0.12 |
| CVD | 89 (25.9%) | 165 (29.8%) | 0.20 |
| DR | 149 (43.3%) | 115 (20.8%) | <0.001 |
| Duration of DR [years] b | 5.0 [5.0–6.0] | 6.0 [4.0–8.0] | <0.001 |
| Diabetic neuropathy | 69 (20.1%) | 39 (7.1%) | <0.001 |
| S-HbA1c [%] b | 7.70 [6.90–8.72] | 7.50 [6.90–8.20] | <0.001 |
| S-fasting glucose [mmol/L] b | 8.70 [7.18–10.33] | 8.10 [6.80–9.50] | <0.001 |
| S-Hb [g/L] a | 138.87 ± 13.26 | 139.65 ± 11.84 | 0.36 |
| S-urea [mmol/L] b | 6.20 [5.20–7.70] | 5.90 [4.80–7.40] | 0.0049 |
| S-creatinine [μmol/L] b | 80.0 [68.0–102.0] | 77.0 [65.0–90.0] | 0.0025 |
| Male sex b | 89.0 [73.0–106.0] | 84.0 [71.0–98.0] | 0.0025 |
| Female sex b | 72.0 [58.0–88.0] | 70.0 [61.0–80.0] | 0.097 |
| eGFR [MDRDequation, mL/min] b | 60.0 [58.0–64.0] | 77.0 [60.0–88.0] | <0.001 |
| Male sex b | 60.0 [60.0–60.0] | 79.0 [68.0–87.0] | <0.001 |
| Female sex b | 62.0 [59.0–66.0] | 60.0 [60.0–60.0] | <0.001 |
| S-cystatin C [mg/L] b | 0.82 [0.69–1.03] | 0.74 [0.65–0.86] | <0.001 |
| S-Total cholesterol [mmol/L] b | 4.35 [3.80–5.20] | 4.40 [3.90–5.10] | 0.82 |
| S-HDL [mmol/L] b | 1.20 [1.00–1.40] | 1.20 [1.00–1.40] | 0.86 |
| S-LDL [mmol/L] b | 2.40 [2.00–3.00] | 2.40 [2.00–3.00] | 0.66 |
| S-TGS [mmol/L] b | 1.60 [1.10–2.32] | 1.40 [1.00–2.10] | 0.0123 |
| U-albumin–creatinine ratio [g/mol], sample no. 1 b | 7.92 [3.51–22.67] | 1.00 [0.60–1.58] | <0.001 |
| U-albumin–creatinine ratio [g/mol], sample no. 2 b | 7.97 [3.58–24.51] | 1.03 [0.68–1.70] | <0.001 |
| U-albumin–creatinine ratio [g/mol], sample no. 3 b | 8.18 [3.52–22.82] | 1.02 [0.68–1.70] | <0.001 |
| Statin use | 275 (79.9%) | 423 (76.5%) | 0.18 |
| Metformin use | 111 (32.3%) | 208 (37.6%) | 0.10 |
| TXN2_rs8140110 | Case (N = 344) | Control (N = 553) | p Value | Adjusted OR (95% CI) |
|---|---|---|---|---|
| TT | 2 (0.6%) | 12 (2.2%) | 0.0322 | 0.21 (0.03–0.84) [p value: 0.0498] |
| TC | 51 (14.8%) | 107 (19.3%) | 0.54 (0.36–0.81) [p value: 0.0034] | |
| CC | 291 (84.6%) | 434 (78.5%) | ref. | |
| ALLELES | ||||
| T (MAF) | 55 (8.0%) | 131 (11.8%) | 0.0093 | 0.52 (0.36–0.74) [p value: <0.001] |
| C | 633 (92.0%) | 975 (88.2%) | ref. | |
| HWE (p value) | 0.88 | 0.0841 | ||
| DOMINANT | ||||
| TT + TC | 53 (15.4%) | 119 (21.5%) | 0.0238 | 0.51 (0.34–0.75) [p value: <0.001] |
| CC | 291 (84.6%) | 434 (78.5%) | ref. | |
| RECESSIVE | ||||
| TT | 2 (0.6%) | 12 (2.2%) | 0.0620 | 0.23 (0.03–0.92) [p value: 0.0661] |
| TC + CC | 342 (99.4%) | 541 (97.8%) | ref. |
| TXNRD2_rs1548357 | Case (N = 344) | Control (N = 553) | p Value | Adj OR (95% CI) |
|---|---|---|---|---|
| CC | 31 (9.0%) | 53 (9.6%) | 0.90 | 0.85 (0.5–1.44) [p value: 0.56] |
| CT | 147 (42.7%) | 241 (43.6%) | 0.85 (0.62–1.17) [p value: 0.32] | |
| TT | 166 (48.3%) | 259 (46.8%) | ref. | |
| ALLELES | ||||
| C (MAF) | 209 (30.4%) | 347 (31.4%) | 0.66 | 0.9 (0.72–1.13) [p value: 0.35] |
| T | 479 (69.6%) | 759 (68.6%) | ref. | |
| HWE (p value) | 0.85 | 0.78 | ||
| DOMINANT | ||||
| CC + CT | 178 (51.7%) | 294 (53.2%) | 0.68 | 0.85 (0.63–1.15) [p value: 0.30] |
| TT | 166 (48.3%) | 259 (46.8%) | ref. | |
| RECESSIVE | ||||
| CC | 31 (9.0%) | 53 (9.6%) | 0.77 | 0.92 (0.55–1.52) [p value: 0.75] |
| CT + TT | 313 (91.0%) | 500 (90.4%) | ref. |
| TXNIP_rs7212 | Case (N = 344) | Control (N = 553) | p Value | Adj OR (95% CI) |
|---|---|---|---|---|
| CC | 1 (0.3%) | 1 (0.2%) | 0.69 | 0.96 (0.04–25.1) [p value: 0.98] |
| CG | 23 (6.7%) | 30 (5.4%) | 1.1 (0.59–1.99) [p value: 0.77] | |
| GG | 320 (93.0%) | 522 (94.4%) | ref. | |
| ALLELES | ||||
| C (MAF) | 25 (3.6%) | 32 (2.9%) | 0.38 | 1.08 (0.61–1.9) [p value: 0.79] |
| G | 663 (96.4%) | 1074 (97.1%) | ref. | |
| HWE (p value) | 0.40 | 0.42 | ||
| DOMINANT | ||||
| CC + CG | 24 (7.0%) | 31 (5.6%) | 0.41 | 1.09 (0.6–1.96) [p value: 0.78] |
| GG | 320 (93.0%) | 522 (94.4%) | ref. | |
| RECESSIVE | ||||
| CC | 1 (0.3%) | 1 (0.2%) | 0.73 | 0.95 (0.04–24.98) [p value: 0.97] |
| CG + GG | 343 (99.7%) | 552 (99.8%) | ref. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Letonja, J.; Nussdorfer, P.; Petrovič, D. Single-Nucleotide Polymorphisms in the Thioredoxin Antioxidant System and Their Association with Diabetic Nephropathy in Slovenian Patients with Type 2 Diabetes—A Preliminary Study. Int. J. Mol. Sci. 2025, 26, 1832. https://doi.org/10.3390/ijms26051832
Letonja J, Nussdorfer P, Petrovič D. Single-Nucleotide Polymorphisms in the Thioredoxin Antioxidant System and Their Association with Diabetic Nephropathy in Slovenian Patients with Type 2 Diabetes—A Preliminary Study. International Journal of Molecular Sciences. 2025; 26(5):1832. https://doi.org/10.3390/ijms26051832
Chicago/Turabian StyleLetonja, Jernej, Petra Nussdorfer, and Danijel Petrovič. 2025. "Single-Nucleotide Polymorphisms in the Thioredoxin Antioxidant System and Their Association with Diabetic Nephropathy in Slovenian Patients with Type 2 Diabetes—A Preliminary Study" International Journal of Molecular Sciences 26, no. 5: 1832. https://doi.org/10.3390/ijms26051832
APA StyleLetonja, J., Nussdorfer, P., & Petrovič, D. (2025). Single-Nucleotide Polymorphisms in the Thioredoxin Antioxidant System and Their Association with Diabetic Nephropathy in Slovenian Patients with Type 2 Diabetes—A Preliminary Study. International Journal of Molecular Sciences, 26(5), 1832. https://doi.org/10.3390/ijms26051832