
Biochemical Identification and Clinical Description of Medetomidine Exposure in People Who Use Fentanyl in Philadelphia, PA

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Results
2.1. Study Cohort Description
2.2. Toxicology and Analytical Findings
2.3. Clinical Outcomes
3. Discussion
3.1. Detecting the Shift from Xylazine to Medetomidine
3.2. Toxicology Testing
3.3. Intoxication Phenotype
3.4. Withdrawal Phenotype
3.5. Clinical Outcomes of Withdrawal
3.6. Limitations
3.7. Summative Thoughts and Future Directions
4. Materials and Methods
4.1. Study Design and Setting
4.2. Study Population
4.3. Electronic Health Record Data Collection and Abstraction
4.4. Specimen Collection
4.5. Toxicology Background and Analysis
4.6. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LC-MS/MS | Liquid Chromatography–Tandem Mass Spectroscopy |
| ED | Emergency Department |
| COWS | Clinical Opiate Withdrawal Scale |
| MDM | Multiple Reaction Monitoring |
| PDD | Patient-Directed Discharge |
| 3-OH-M | 3-hydroxy-medetomidine |
| ICU | Intensive Care Unit |
| OUD | Opioid Use Disorder |
| NSTEMI | Non-ST Segment Elevation Myocardial Infarction |
| hsTnT | High-Sensitivity Troponin T |
| PRES | Posterior Reversible Encephalopathy Syndrome |
| MOUD | Medication for Opioid Use Disorder |
Appendix A. Additional Figures
Appendix A.1
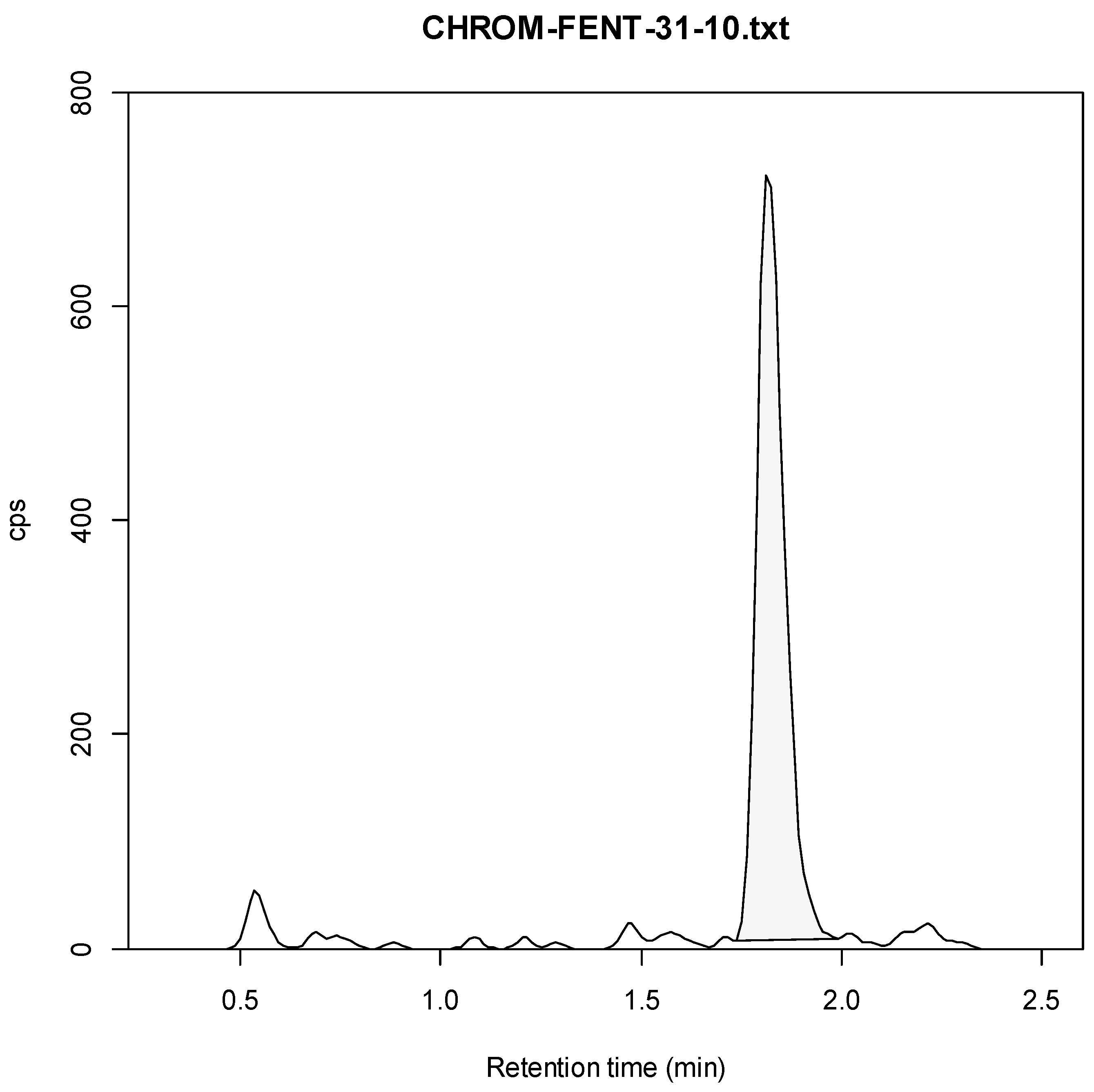
- 1:
- Fentanyl
- Standard Curve
- Example Chromatogram
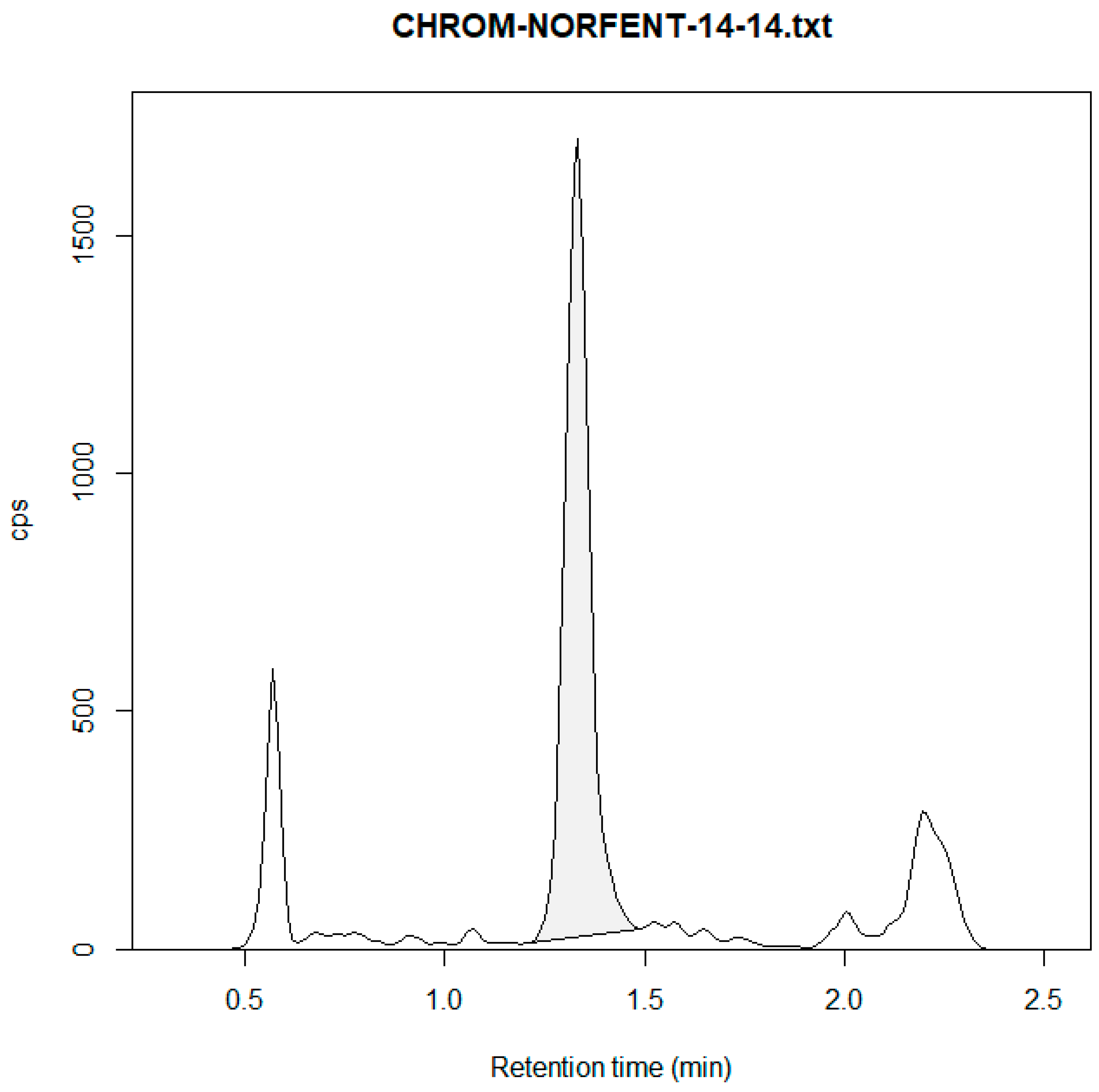
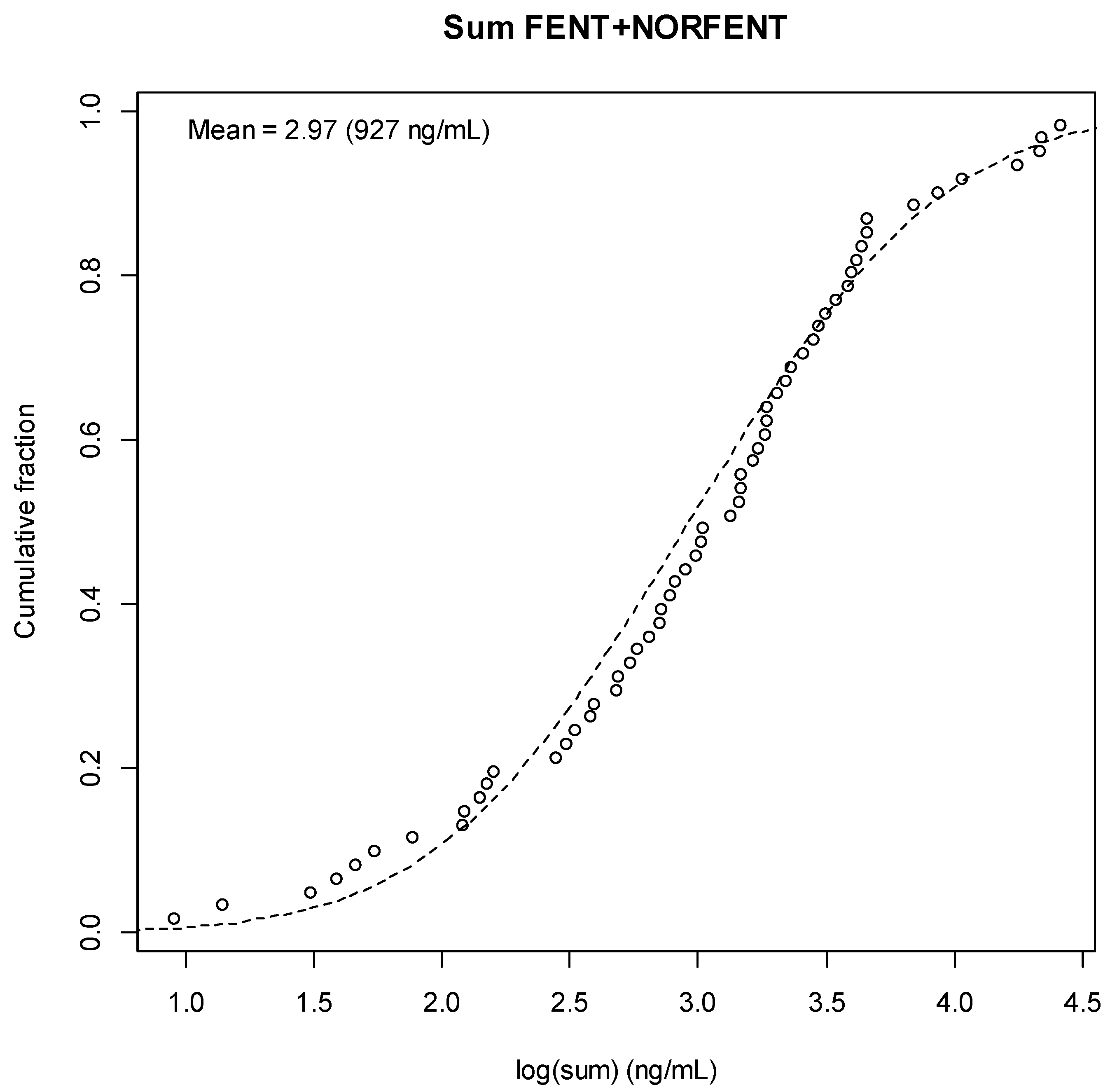
- 2:
- Norfentanyl
- Standard Curve
- Example Chromatogram
- Combined Fentanyl-Norfentanyl Result Distribution
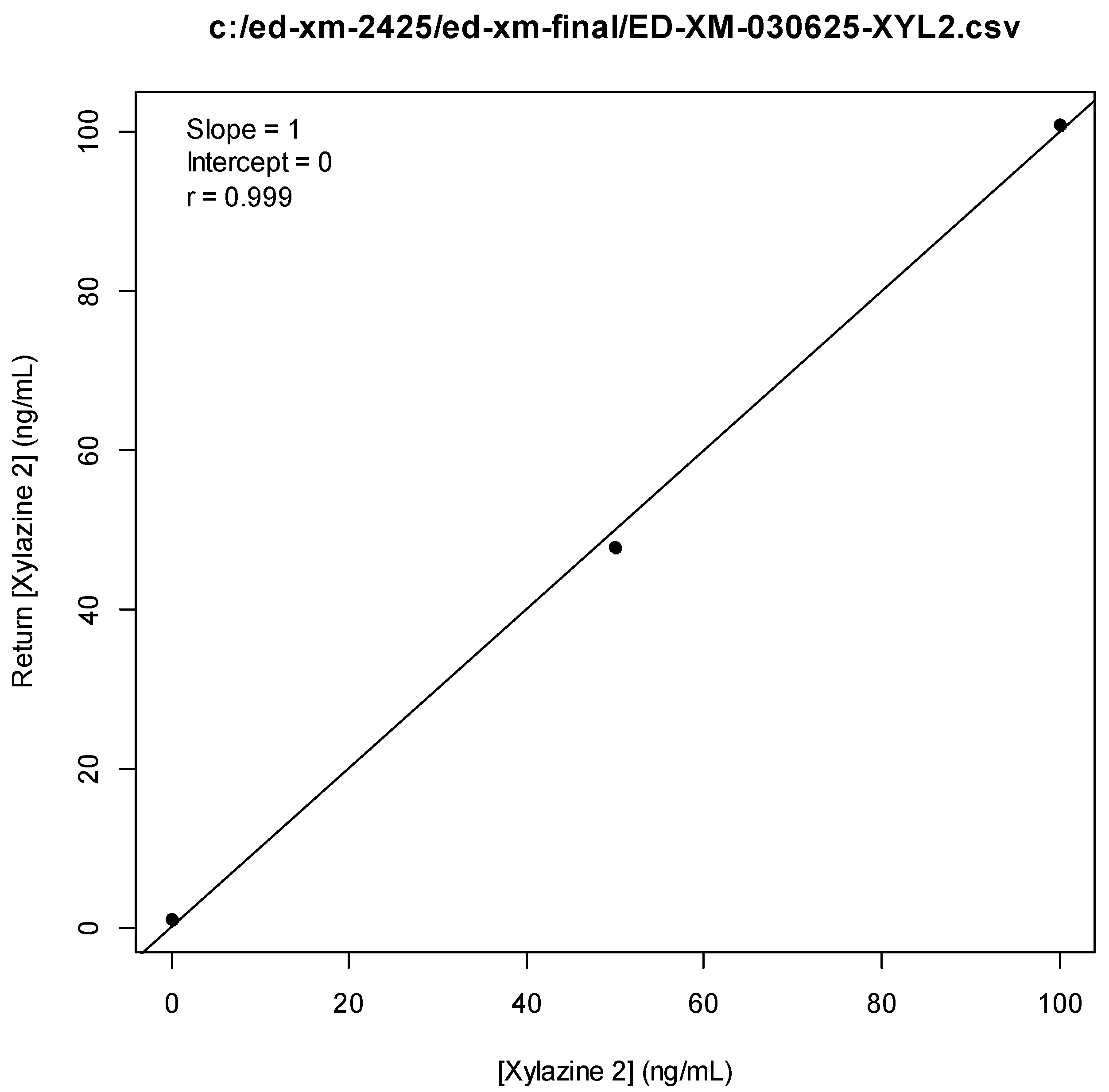
- 3:
- Xylazine
- Standard Curve
- Example Chromatogram
- Result Distribution
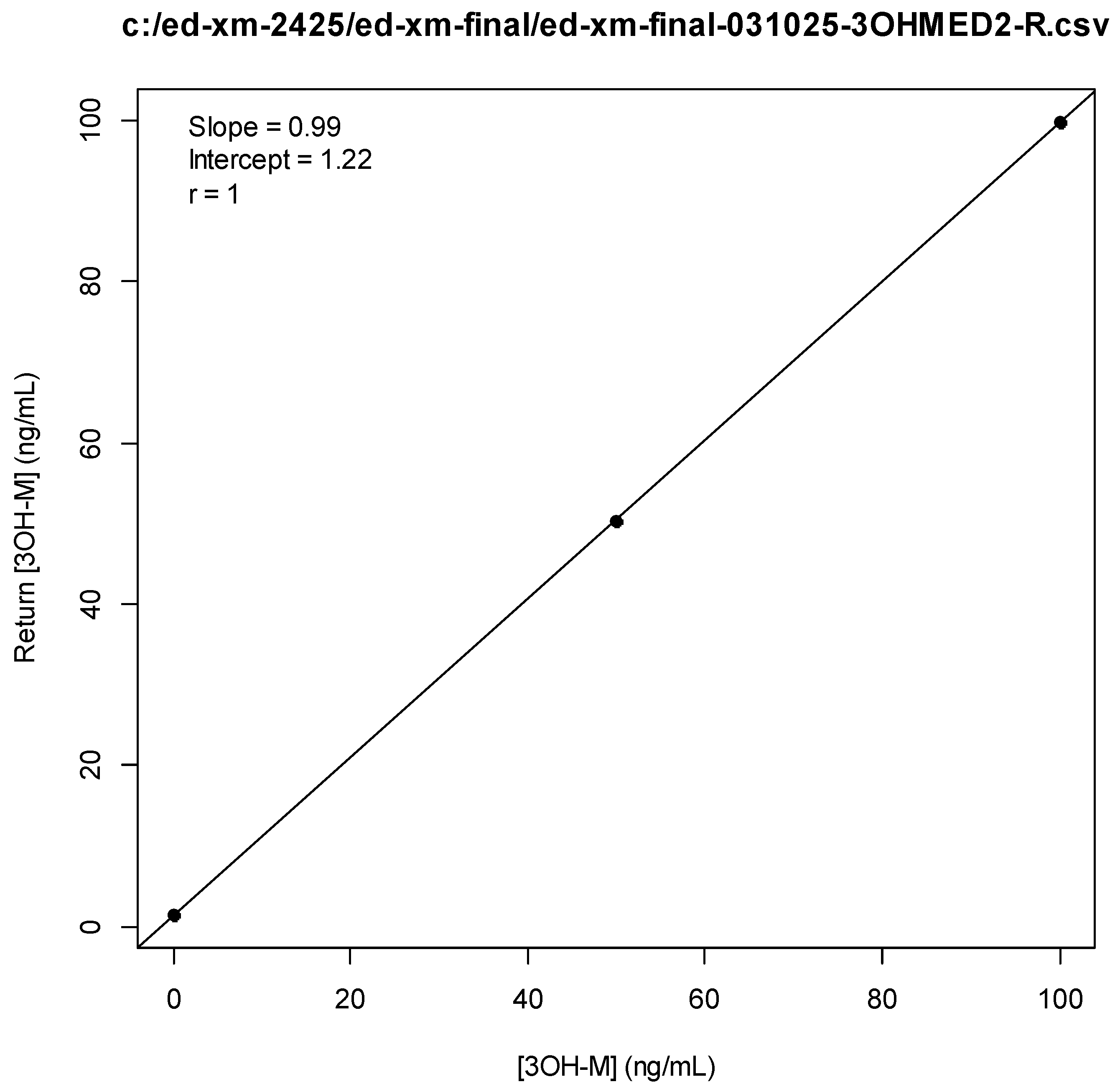
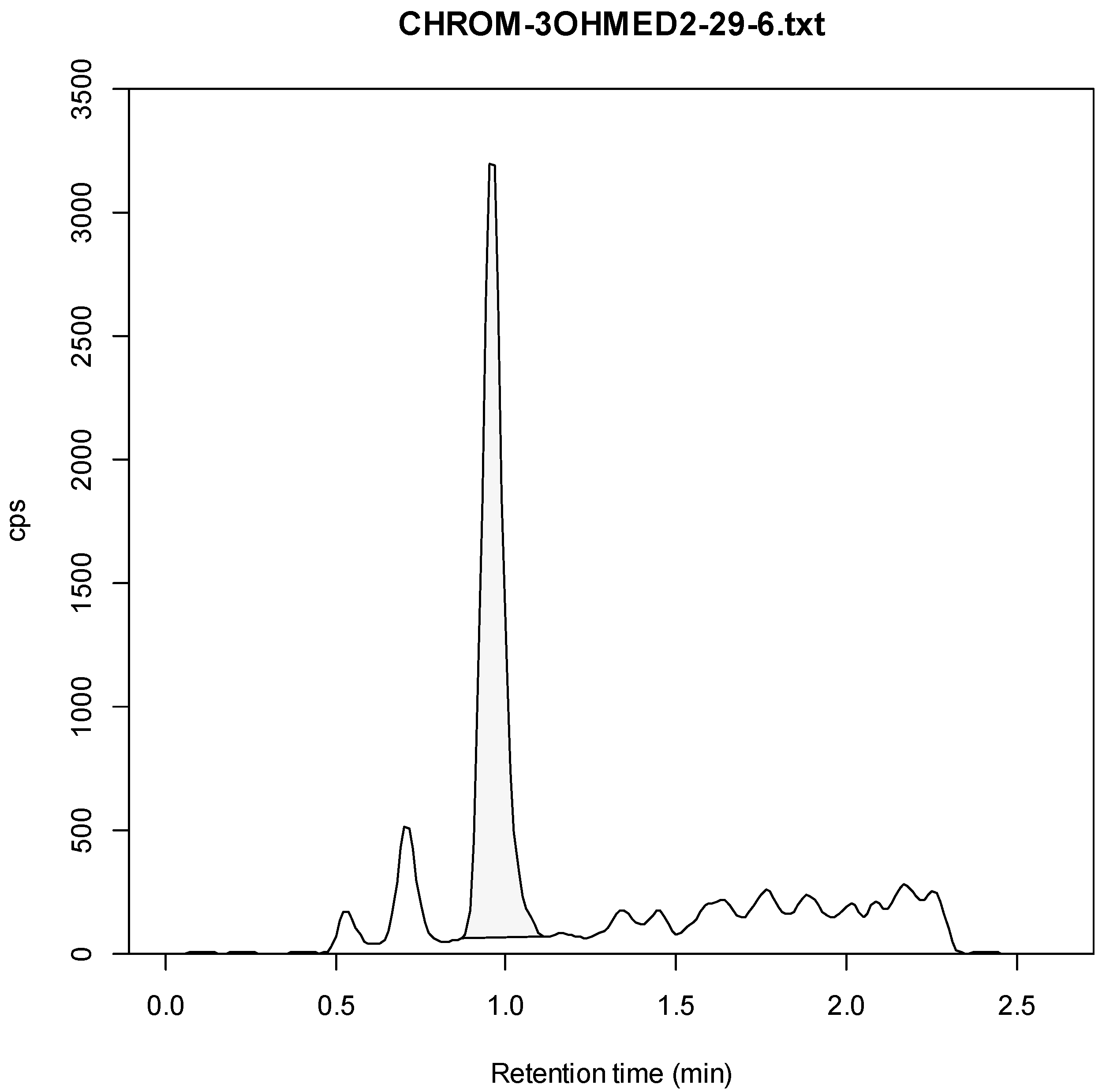
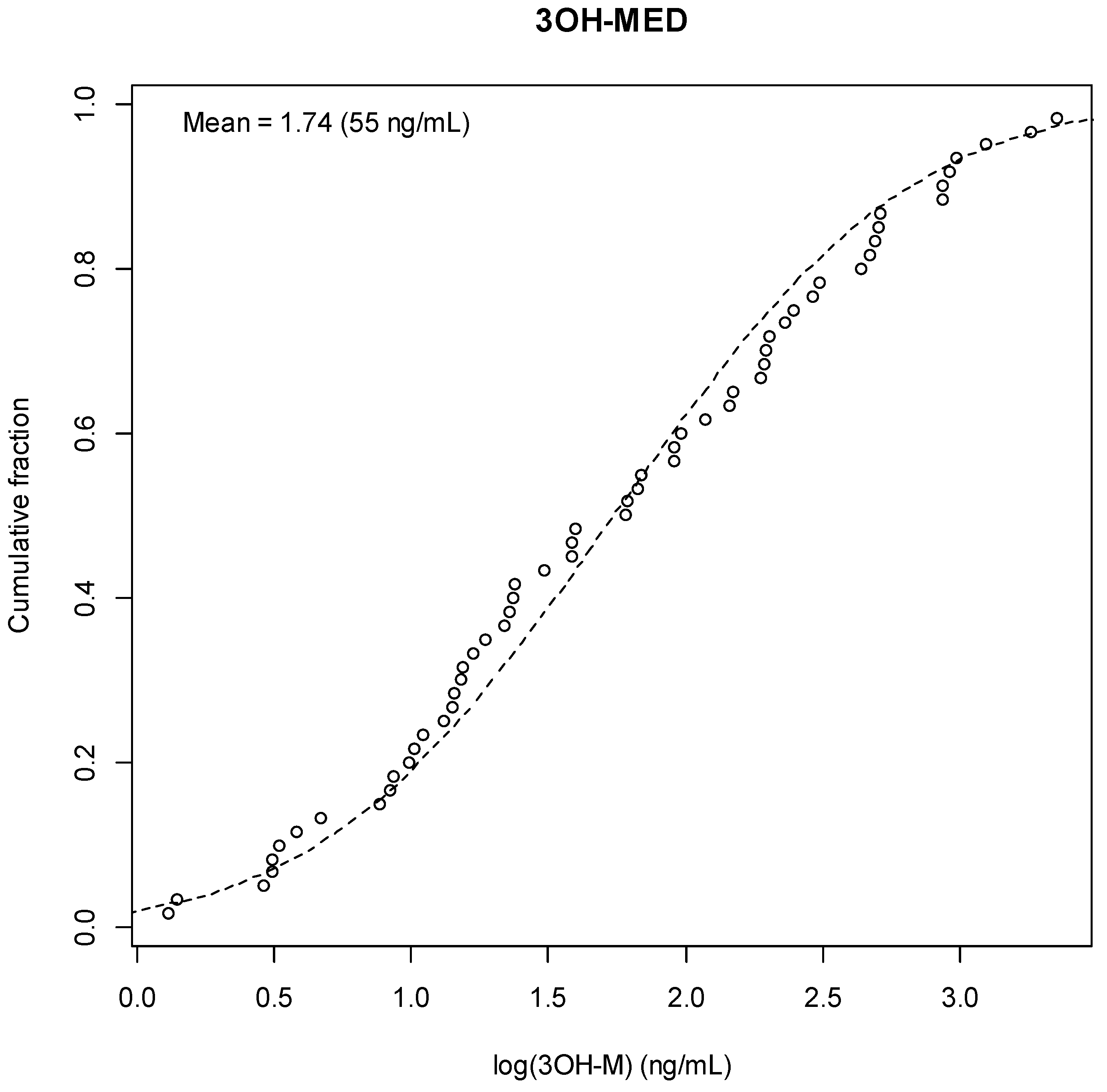
- 4:
- 3-Hydroxy-Medetomidine
- Standard Curve
- Example Chromatogram
- Result Distribution




References
- Philadelphia Department of Public Health. Health Alert: Medetomidine as an Emerging Adulterant in the Illicit Drug Supply; Philadelphia Department of Public Health: Philadelphia, PA, USA, 2024. Available online: https://hip.phila.gov/document/4874/PDPH-HAN-00444A-12-10-2024.pdf (accessed on 9 June 2025).
- Zhu, D.T.; Palamar, J.J. Responding to medetomidine: Clinical and public health needs. Lancet Reg. Health 2025, 44, 101053. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, E.S.; Buchanan, J.; Aldy, K.; Shulman, J.; Krotulski, A.; Walton, S.; Logan, B.; Wax, P.; Campleman, S.; Brent, J.; et al. Notes from the Field: Detection of Medetomidine Among Patients Evaluated in Emergency Departments for Suspected Opioid Overdoses—Missouri, Colorado, and Pennsylvania, September 2020–December 2023. Morb. Mortal. Wkly. Rep. 2024, 73, 672–674. [Google Scholar] [CrossRef]
- PAGroundhogs. PAG Releases New Adulterant Report; PAGroundhogs: Philadelphia, PA, USA, 2025; Available online: https://pagroundhogs.org/news/f/pag-releases-new-adulterant-report (accessed on 9 June 2025).
- Sisco, E.; Appley, M. Identification of the veterinary sedative medetomidine in combination with opioids and xylazine in Maryland. J. Forensic Sci. 2023, 68, 1708–1712. [Google Scholar] [CrossRef] [PubMed]
- Kallio, A.; Salonen, M.; Forssell, H.; Scheinin, H.; Scheinin, M.; Tuominen, J. Medetomidine premedication in dental surgery: A double-blind cross-over study with a new alpha 2-adrenoceptor agonist. Acta Anaesthesiol. Scand. 1990, 34, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Haenecour, A.; Goodwin, A.; Seto, W.; Urbain, C.; Laussen, P.; Balit, C. Prolonged dexmedetomidine infusion and drug withdrawal in critically ill children. Crit. Care 2015, 19, 484. [Google Scholar] [CrossRef]
- Bouajram, R.H.; Bhatt, K.; Croci, R.; Baumgartner, L.; Puntillo, K.; Ramsay, J.; Thompson, A. Incidence of dexmedetomidine withdrawal in adult critically ill patients: A pilot study. Crit. Care Explor. 2019, 1, e0035. [Google Scholar] [CrossRef]
- Huo, S.; London, K.; Murphy, L.; Casey, E.; Durney, P.; Arora, M.; McKeever, R.; Tasillo, A.; Goodstein, D.; Hart, B.; et al. Notes from the Field: Suspected Medetomidine Withdrawal Syndrome Among Fentanyl-Exposed Patients—Philadelphia, Pennsylvania, September 2024–January 2025. Morb. Mortal. Wkly. Rep. 2025, 74, 266–268. [Google Scholar] [CrossRef]
- Philadelphia Department of Public Health. Health Alert: Risks of Xylazine Use and Withdrawal in People Who Use Drugs in Philadelphia; Philadelphia Department of Public Health: Philadelphia, PA, USA, 2022. Available online: https://hip.phila.gov/document/2524/PDPH-HAN_Alert_1_Xylazine_03.16.2022.pdf (accessed on 9 June 2025).
- Reid, J.L.; Campbell, B.C.; Hamilton, C.A. Withdrawal reactions following cessation of central alpha-adrenergic receptor agonists. Hypertension 1984, 6, II71–II75. [Google Scholar] [CrossRef]
- London, K.; Li, Y.; Kahoud, J.L.; Cho, D.; Mulholland, J.; Roque, S.; Stugart, L.; Gillingham, J.; Borne, E.; Slovis, B. Tranq Dope: Characterization of an ED cohort treated with a novel opioid withdrawal protocol in the era of fentanyl/xylazine. Am. J. Emerg. Med. 2024, 85, 130–139. [Google Scholar] [CrossRef]
- Srivastava, A.B.; Mariani, J.J.; Levin, F.R. New directions in the treatment of opioid withdrawal. Lancet 2020, 395, 1938–1948. [Google Scholar] [CrossRef]
- Rudolf, G.; Walsh, J.; Plawman, A.; Gianutsos, P.; Alto, W.; Mancl, L.; Rudolf, V. A novel non-opioid protocol for medically supervised opioid withdrawal and transition to antagonist treatment. Am. J. Drug Alcohol Abus. 2018, 44, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Ehrman-Dupre, R.; Kaigh, C.; Salzman, M.; Haroz, R.; Peterson, L.K.; Schmidt, R. Management of xylazine withdrawal in a hospitalized patient: A case report. J. Addict. Med. 2022, 16, 595–598. [Google Scholar] [CrossRef] [PubMed]
- London, K.S.; Durney, P.; Warrick-Stone, T.; Alexander, K.; Kahoud, J.L. Decreased effectiveness of a novel opioid withdrawal protocol following the emergence of medetomidine as a fentanyl adulterant. Biomed 2025, 5, 13. [Google Scholar] [CrossRef]
- Stobbe, M. Animal Sedative Medetomidine is Showing up in the US Illegal Drug Supply, CDC Says; The Associated Press: New York, NY, USA, 2025; Available online: https://apnews.com/article/medetomidine-cdc-drug-supply-fentanyl-xylazine-8e1acb5a09f5d343e2537dfb0d49d928 (accessed on 9 June 2025).
- Weerink, M.A.S.; Struys, M.M.R.F.; Hannivoort, L.N.; Barends, C.R.M.; Absalom, A.R.; Colin, P. Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine. Clin. Pharmacokinet. 2017, 56, 893–913. [Google Scholar] [CrossRef]
- Karol, M.D.; Maze, M. Pharmacokinetics and interaction pharmacodynamics of dexmedetomidine in humans. Best Pract. Res. Clin. Anaesthesiol. 2000, 14, 261–269. [Google Scholar] [CrossRef]
- Salonen, J.S.; Eloranta, M. Biotransformation of medetomidine in the rat. Xenobiotica 1990, 20, 471–480. [Google Scholar] [CrossRef]
- Fernandes, N.S.; Passos, Y.D.; Arcoverde, K.N.; Mouta, A.N.; Paiva, T.C.; Oliveira, K.D.; Araujo-Silva, G.; de Paula, V.V. Clinical effects and pharmacokinetic profile of intramuscular dexmedetomidine (10 μg/kg) in cats. Animals 2024, 14, 2274. [Google Scholar] [CrossRef] [PubMed]
- Kaivosaari, S.; Toivonen, P.; Aitio, O.; Sipilä, J.; Koskinen, M.; Salonen, J.S.; Finel, M. Regio- and stereospecific N-glucuronidation of medetomidine: The differences between UDP glucuronosyltransferase (UGT) 1A4 and UGT2B10 account for the complex kinetics of human liver microsomes. Drug Metab. Dispos. 2008, 36, 1529–1537. [Google Scholar] [CrossRef]
- Kuusela, E.; Raekallio, M.; Anttila, M.; Falck, I.; Mölsä, S.; Vainio, O. Clinical effects and pharmacokinetics of medetomidine and its enantiomers in dogs. J. Vet. Pharmacol. Ther. 2000, 23, 15–20. [Google Scholar] [CrossRef]
- Salonen, M.; Reid, K.; Maze, M. Synergistic interaction between alpha 2-adrenergic agonists and benzodiazepines in rats. Anesthesiology 1992, 76, 1004–1011. [Google Scholar] [CrossRef]
- Kint, L.T.; Seewoo, B.J.; Hyndman, T.H.; Clarke, M.W.; Edwards, S.H.; Rodger, J.; Musk, G.C. The pharmacokinetics of medetomidine administered subcutaneously during isoflurane anaesthesia in Sprague-Dawley rats. Animals 2020, 10, 1050. [Google Scholar] [CrossRef] [PubMed]
- Sood, N.; Dhillon, G. Illicit Medetomidine Use with Fentanyl. The Hospitalist 2025. Available online: https://www.the-hospitalist.org/hospitalist/article/38385/addiction-medicine/illicit-medetomidine-use-with-fentanyl/ (accessed on 9 June 2025).
- Murphy, L.; Krotulski, A.; Hart, B.; Wong, M.; Overton, R.; McKeever, R. Clinical characteristics of patients exposed to medetomidine in the illicit opioid drug supply in Philadelphia: A case series. Clin. Toxicol. 2025, 63, 438–441. [Google Scholar] [CrossRef]
- Philadelphia Department of Public Health. Health Alert: Medetomidine Identified in the Illicit Drug Supply; Philadelphia Department of Public Health: Philadelphia, PA, USA, 2024. Available online: https://hip.phila.gov/document/4421/PDPH-HAN-0441A-05-13-24.pdf (accessed on 9 June 2025).
- Nham, A.; Le, J.N.; Thomas, S.A.; Gressick, K.; Ussery, E.N.; Ko, J.Y.; Gladden, R.M.; Mikosz, C.A.; Schier, J.G.; Vivolo-Kantor, A.; et al. Overdoses involving medetomidine mixed with opioids—Chicago, Illinois, May 2024. Morb. Mortal. Wkly. Rep. 2025, 74, 258–265. [Google Scholar] [CrossRef]
- Palamar, J.J.; Krotulski, A.J. Medetomidine infiltrates the US illicit opioid market. JAMA 2024, 332, 1425–1426. [Google Scholar] [CrossRef]
- Norman, K.; Nappe, T.M. Alpha receptor agonist toxicity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK500023 (accessed on 9 June 2025).
- Ruiz-Colón, K.; Chavez-Arias, C.; Díaz-Alcalá, J.E.; Martínez, M.A. Xylazine intoxication in humans and its importance as an emerging adulterant in abused drugs: A comprehensive review of the literature. Forensic Sci. Int. 2014, 240, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rimawi, M.; Hamlin, D. Xylazine: A review of intoxication, overdose, and withdrawal symptoms. Am. J. Psychiatry Resid. J. 2025, 20, 11–13. [Google Scholar] [CrossRef]
- Sood, N. Rise of illicit medetomidine use: A worrisome trend. Am. J. Addict. 2025; advance online publication. [Google Scholar] [CrossRef]
- Bharati, S.; Pal, A.; Biswas, C.; Biswas, R. Incidence of cardiac arrest increases with the indiscriminate use of dexmedetomidine: A case series and review of published case reports. Acta Anaesthesiol. Taiwanica 2011, 49, 165–167. [Google Scholar] [CrossRef]
- Bryant, C.E.; England, G.C.W.; Clarke, K.W. A comparison of the sedative effects of medetomidine and xylazine in the horse. J. Vet. Anaesth. 1991, 18, 55–57. [Google Scholar] [CrossRef]
- Tyner, C.L.; Woody, B.J.; Reid, J.S.; Chafetz, E.P.; Lederer, H.A.; Norton, J.F.; Jöchle, W. Multicenter clinical comparison of sedative and analgesic effects of medetomidine and xylazine in dogs. J. Am. Vet. Med. Assoc. 1997, 211, 1413–1417. [Google Scholar] [CrossRef]
- Alexander, R.; Agwuncha, C.; Wilson, C.; Schrecker, J.; Holt, A.; Heltsley, R. Withdrawal signs and symptoms among patients positive for fentanyl with and without xylazine. J. Addict. Med. 2025, 19, 202–207. [Google Scholar] [CrossRef]
- Thakrar, A.P.; Zwiebel, S.J.; Christine, P.; Spadaro, A.; Davis, M.H.; Bhatia, R.; Lowenstein, M. Manifestations of potential xylazine withdrawal: A retrospective cohort study with nested case series. Drug Alcohol Depend. 2025, 265, 110151. [Google Scholar] [CrossRef] [PubMed]
- London, K.; Sholes, R.; Ream, C.; Portnoy, A.; Walsh, C.; Spritzer, K.; Nichols, Z.; Reed, M. A qualitative evaluation of a hospital-based peer recovery support program. J. Subst. Use 2025, 1–7. [Google Scholar] [CrossRef]
- Wesson, D.R.; Ling, W. The clinical opiate withdrawal scale (COWS). J. Psychoact. Drugs 2003, 35, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Chrysostomou, C.; Schmitt, C.G. Dexmedetomidine: Sedation, analgesia and beyond. Expert Opin. Drug Metab. Toxicol. 2008, 4, 619–627. [Google Scholar] [CrossRef]
- Hoy, S.M.; Keating, G.M. Dexmedetomidine: A review of its use for sedation in mechanically ventilated patients in an intensive care setting and for procedural sedation. Drugs 2011, 71, 1481–1501. [Google Scholar] [CrossRef] [PubMed]
- Meyer, R.E.; Fish, R.E. Pharmacology of Injectable Anesthetics, Sedatives, and Tranquilizers. In Anesthesia and Analgesia in Laboratory Animals, 2nd ed.; Fish, R.E., Brown, M.J., Danneman, P.J., Karas, A.Z., Eds.; Academic Press: San Diego, CA, USA, 2008; pp. 27–82. [Google Scholar] [CrossRef]
- Korn, W.R.; Stone, M.D.; Haviland, K.L.; Toohey, J.M.; Stickle, D.F. High prevalence of xylazine among fentanyl screen-positive urines from hospitalized patients, Philadelphia, 2021. Clin. Chim. Acta 2021, 521, 151–154. [Google Scholar] [CrossRef]
- Kyle, P.B.; Mattiello, C.J.; Hua, A.; Toohey, J.M.; Korn, W.R.; Saldana-Reed, A.; Stickle, D.F. Evaluation of the ARK Diagnostics immunoassay for qualitative detection of xylazine in urine. J. Anal. Toxicol. 2024, 48, 468–471. [Google Scholar] [CrossRef]
- Kura Biotech. B-One Quick Start Guide. Available online: https://www.kurabiotech.com/finden-b-one (accessed on 9 June 2025).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Intoxication Phenotype (n = 11) | Withdrawal Phenotype (n = 88) | Paired Samples (n = 2) |
|---|---|---|---|
| Age, median (mean for paired) years (IQR or range) | 39 (36–53) | 39 (35–44) | 61.5 (59.0–64.0) |
| Male sex, n (%) | 4 (36.4%) | 71 (80.7%) | 1 (50%) |
| Female sex, n (%) | 7 (63.6%) | 17 (19.3%) | 1 (50%) |
| Reported Daily Use Volume, bags/day (IQR) | 15 (5–25) | 15 (8–29) | 4.5 (1–8) |
| Route: Injection, n (%) | 11 (85%) | 47 (52%) | 1 (50%) |
| Route: Insufflation, n (%) | 3 (23%) | 32 (36%) | 2 (100%) |
| Route: Smoke, n (%) | 2 (15%) | 8 (9%) | 0 (0%) |
| Route: Not recorded, n (%) | 0 (0%) | 7 (8%) | 0 (0%) |
| Median Max/Min Heart Rate, bpm (IQR) | 54 (50–58) | 132 (112–147) | * |
| Median Max/Min Systolic BP, mmHg (IQR) | 99 (79–102) | 190 (168–210) | ** |
| Median Max/Min Diastolic BP, mmHg (IQR) | 54 (38–58) | 110 (99–127) | *** |
| ED Disposition: Discharged, n (%) | 1 (8%) | 1 (1%) | 0 (0%) |
| ED Disposition: Admitted, n (%) | 12 (92%) | 87 (98.9%) | 2 (100%) |
| Hospital Disposition: Discharged, n (%) | 8 (62%) | 24 (27.2%) | 1 (50%) |
| Hospital Disposition: PDD, n (%) | 4 (31%) | 32 (36.4%) | 1 (50%) |
| Hospital Disposition: Rehab/Detox, n (%) | 1 (8%) | 21 (23.9%) | 0 (0%) |
| Hospital Disposition: Law Enforcement, n (%) | 0 (0%) | 13 (14.8%) | 0 (0%) |
| Hospital LOS, mean days (IQR) | 13 (5–15) | 7 (3 –11) | 10 (7–13) |
| ICU admission, n (%) | 3 (23.1%) | 56 (63.6%) | 1 (50%) |
| Required intubation, n (%) | 2 (15.4%) | 12 (13.6%) | 1 (50%) |
| Xylazine-positive, n (%) | 7 (53.7%) | 31 (62%) | 1 (50%) |
| Benzodiazepine-positive, n (%) | 4 (30.8%) | 36 (36%) | 2 (100%) |
| Urine Drug Test | Positive, n (%) |
|---|---|
| Fentanyl | 100 (100.0%) |
| Cocaine | 60 (60%) |
| Opiates | 40 (40%) |
| Benzodiazepine | 37 (37%) |
| Amphetamine | 35 (35%) |
| Methadone | 24 (24%) |
| Cannabinoid | 14 (14%) |
| Barbiturates | 8 (8%) |
| Analyte | Intoxication (n = 8) | Withdrawal (n = 50) | p-Value (Fisher) | p-Value (Mann–Whitney) |
|---|---|---|---|---|
| Fentanyl, n (%) | 8 (100%) | 34 (68%) | 0.092 | |
| Median Fentanyl, ng/mL (IQR) | 1107 (406–1858) | 39 (0–255) | 0.001 | |
| Norfentanyl, n (%) | 8 (100%) | 50 (100%) | 1.000 | |
| Median Norfentanyl, ng/mL (IQR) | 9666 (2302–18,929) | 741 (312–1769) | 0.001 | |
| 3-OH-M, n (%) | 8 (100%) | 34 (68%) | 0.092 | |
| Median 3-OH-M, ng/mL (IQR) | 561 (233–753) | 13 (0–80) | <0.001 | |
| 3-OH-M post-Glucuronidase, n (%) | 8 (100%) | 50 (100%) | 1.000 | |
| Median 3-OH-M post-Glucuronidase, ng/mL (IQR) | 8423 (375–1311) | 34 (10–166) | <0.001 | |
| Xylazine, n (%) | 4 (50%) | 25 (50%) | 1.000 | |
| Median Xylazine, ng/mL (IQR) | 4 (0–11.2) | 3 (0–43) | 0.691 | |
| Xylazine post-Glucuronidase, n (%) | 8 (100%) | 32 (64%) | 0.048 | |
| Median Xylazine post-Glucuronidase, ng/mL (IQR) | 24 (11–73) | 11 (0–75) | 0.272 |
| Intoxication vs. Withdrawal | Time Between Samples (h) | Fentanyl (ng/mL) | Norfentanyl (ng/mL) | 3-OH-M (ng/mL) | 3-OH-M Post-Glucuronidase (ng/mL) | Xylazine (ng/mL) | Xylazine Post-Glucuronidase (ng/mL) | |
|---|---|---|---|---|---|---|---|---|
| Patient 1 | ||||||||
| Intoxication | -- | 197 | 1131 | 144 | 154 | 7 | 8.0 | |
| Withdrawal | 48.0 | 0 | 330 | 7 | 10 | 0 | 0.0 | |
| Patient 2 | ||||||||
| Intoxication | -- | 1446 | 20,029 | 1070 | 1241 | 0 | 69.0 | |
| Withdrawal | 13.1 | 425 | 3514 | 106 | 502 | 0 | 21.0 |
| Outcome | All Patients (n = 100) |
|---|---|
| Dexmedetomidine Infusion | 63 (63%) |
| Clonidine PO use | 89 (89%) |
| Clonidine Transdermal Patch use | 78 (78%) |
| NSTEMI/hsTnT Elevation > 53 ng/L | 20 (20%) |
| Encephalopathy as diagnosis or PRES | 31 (31%) |
| Seizure During Visit | 5 (5%) |
| Highest COWS Score | 23 (19–28) |
| ID | Analyte | Q1 (m/z) | Q3 (m/z) |
|---|---|---|---|
| 1 | Fentanyl | 337.1 | 117.2 |
| 2 | Norfentanyl | 233.2 | 84.2 |
| 3 | Xylazine | 221.0 | 90.1 |
| 4 | 3-OH-M | 217.1 | 68.2 |
| 5 | Norfentanyl-d5 | 238.2 | 84.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durney, P.; Kahoud, J.L.; Warrick-Stone, T.; Montesi, M.; Carter, M.; Butt, S.; Mencia, A.M.; Omoregie, L.; Shah, M.; Bloomfield, M.; et al. Biochemical Identification and Clinical Description of Medetomidine Exposure in People Who Use Fentanyl in Philadelphia, PA. Int. J. Mol. Sci. 2025, 26, 6715. https://doi.org/10.3390/ijms26146715
Durney P, Kahoud JL, Warrick-Stone T, Montesi M, Carter M, Butt S, Mencia AM, Omoregie L, Shah M, Bloomfield M, et al. Biochemical Identification and Clinical Description of Medetomidine Exposure in People Who Use Fentanyl in Philadelphia, PA. International Journal of Molecular Sciences. 2025; 26(14):6715. https://doi.org/10.3390/ijms26146715
Chicago/Turabian StyleDurney, Phil, Jennifer L. Kahoud, TaReva Warrick-Stone, Maeve Montesi, Meg Carter, Sabrina Butt, Alberto Martinez Mencia, Louisa Omoregie, Monali Shah, Mariah Bloomfield, and et al. 2025. "Biochemical Identification and Clinical Description of Medetomidine Exposure in People Who Use Fentanyl in Philadelphia, PA" International Journal of Molecular Sciences 26, no. 14: 6715. https://doi.org/10.3390/ijms26146715
APA StyleDurney, P., Kahoud, J. L., Warrick-Stone, T., Montesi, M., Carter, M., Butt, S., Mencia, A. M., Omoregie, L., Shah, M., Bloomfield, M., Tomasko, N., Jaffe, R., Herens, A., Korn, W. R., Alexander, K., Stickle, D., Goodstein, D., Weinstein, L. C., & London, K. S. (2025). Biochemical Identification and Clinical Description of Medetomidine Exposure in People Who Use Fentanyl in Philadelphia, PA. International Journal of Molecular Sciences, 26(14), 6715. https://doi.org/10.3390/ijms26146715