
Exploring Molecular Signatures Associated with Inflammation and Angiogenesis in the Aqueous Humor of Patients with Non-Proliferative Diabetic Retinopathy
 , , , ,
, , , ,
Abstract
1. Introduction
2. Results
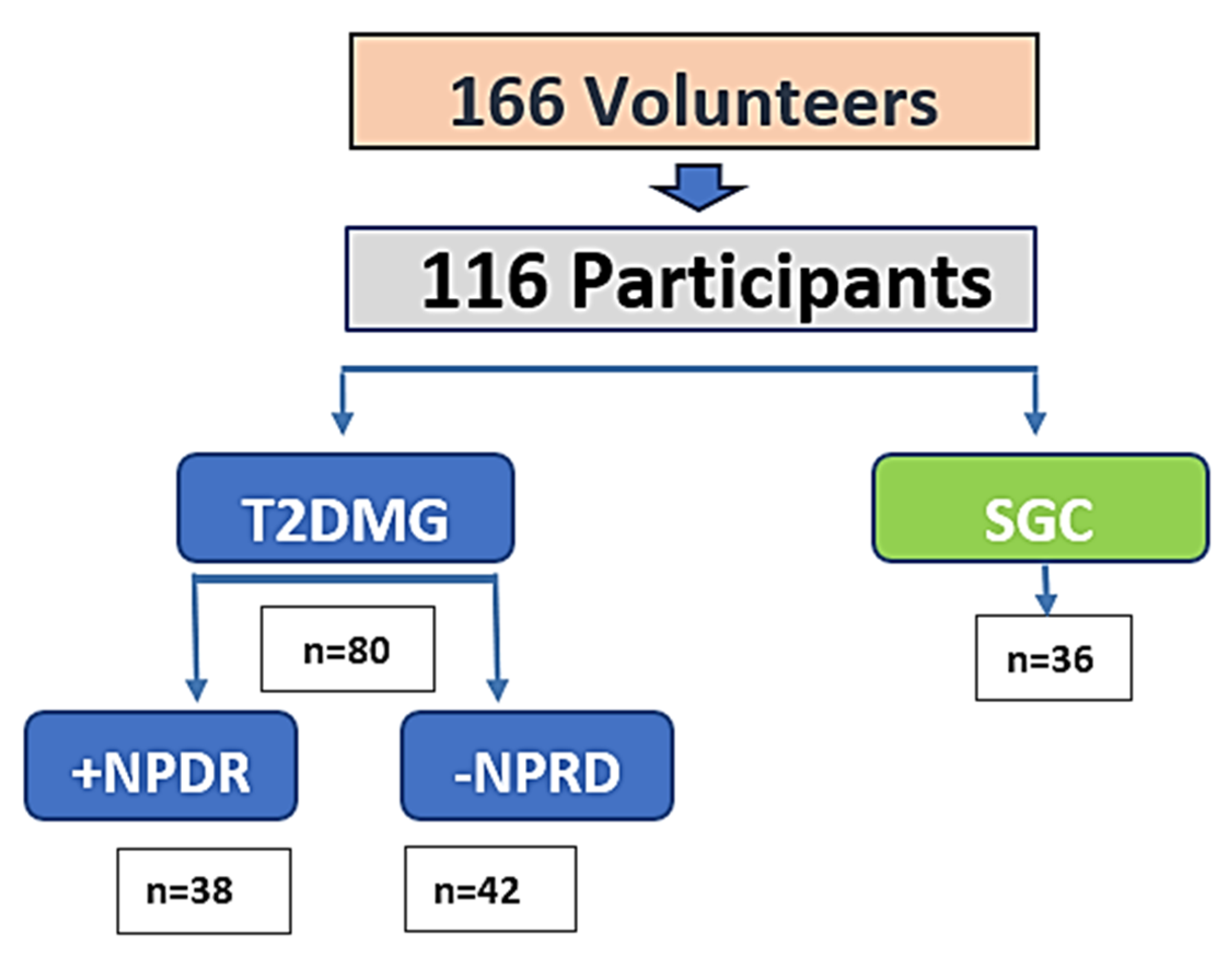
2.1. Study Cohort and Group Assignment
2.2. Sociodemographic and Clinical Characteristics
2.3. Ophthalmological Evaluation
2.4. Biochemical Profile
2.5. Molecular Profiling of Aqueous Humor
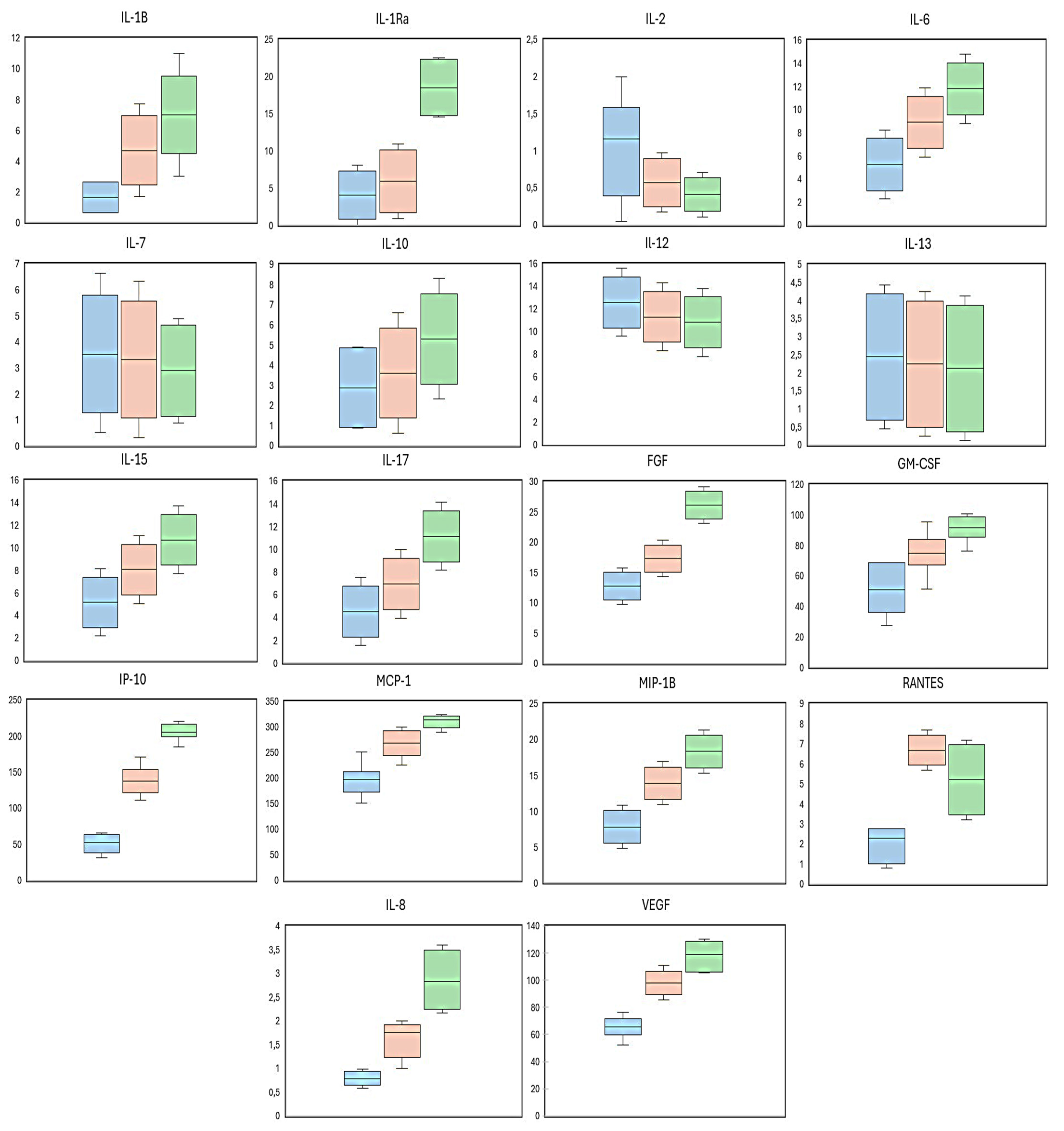
2.6. Expression Patterns and Group Comparisons
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Inclusion and Exclusion Criteria
4.3. Ophthalmological Examination
4.4. Sampling Procedures
4.4.1. Blood Samples and Biochemical Testing
4.4.2. Aqueous Humor Sampling
- Anti-inflammatory ILs: IL-1Ra, IL-4, IL-5, IL-10, IL-13
- Pro-inflammatory cytokines: IL-1β, IL-2, IL-6, IL-12, IL-17, IL-18, IFN-γ, TNF-α
- Chemokines: IP-10, MCP-1, MIP-1α, MIP-1β, RANTES, Eotaxin
- Others: IL-15, MIF, G-CSF, GM-CSF
- Angiogenic and hematopoietic factors: IL-7, bFGF, PDGF, VEGF
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AH | Aqueous humor |
| ANG | Angiogenesis |
| BCVA | Best corrected visual acuity |
| BRB | Blood–retinal barrier |
| CAT | Cube average thickness |
| CFP | Color fundus photography |
| CSFT | Central subfield foveal thickness |
| DM | Diabetes mellitus |
| DR | Diabetic retinopathy |
| DME | Diabetic macular edema |
| HbA1c | Glycated hemoglobin |
| IL | Interleukin |
| INF | Inflammation |
| IOP | Intraocular pressure |
| IP-10 | Interferon gamma-induced protein 10 kDa |
| IRMA | Intraretinal microvascular abnormalities |
| LE | Left eye |
| LogMAR | Logarithm of the minimum angle of resolution |
| MCP-1 | Monocyte chemoattractant protein-1 |
| MDC | Minimal detectable concentration |
| MIF | Macrophage migration inhibitory factor |
| MIP-1α/β | Macrophage inflammatory protein-1 alpha/beta |
| NPDR | Non-proliferative diabetic retinopathy |
| OCT | Optical coherence tomography |
| PDGF | Platelet-derived growth factor |
| RA | Receptor antagonist |
| RE | Right eye |
| RANTES | Regulated on activation, normal T cell-expressed and -secreted |
| SCG | Surrogate control group |
| SD | Standard deviation |
| SD-OCT | Spectral domain optical coherence tomography |
| T2DM | Type 2 diabetes mellitus |
| T Chol | Total cholesterol |
| TNF-α | Tumor necrosis factor alpha |
| TRG | Triglycerides |
| VEGF | Vascular endothelial growth factor |
References
- Teo, Z.L.; Tham, Y.C.; Yu, M.; Chee, M.L.; Rim, T.H.; Cheung, N.; Bikbov, M.M.; Wang, Y.X.; Tang, Y.; Lu, Y.; et al. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045: Systematic Review and Meta-analysis. Ophthalmology 2021, 128, 1580–1591. [Google Scholar] [CrossRef] [PubMed]
- Yau, J.W.Y.; Rogers, S.L.; Kawasaki, R.; Lamoureux, E.L.; Kowalski, J.W.; Bek, T.; Chen, S.J.; Dekker, J.M.; Fletcher, A.; Grauslund, J.; et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 2012, 35, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Knudtson, M.D.; Lee, K.E.; Gagnon, R.; Klein, B.E.K. The Wisconsin Epidemiologic Study of Diabetic Retinopathy XXIII: The twenty-five-year incidence of macular edema in persons with type 1 diabetes. Ophthalmology 2009, 116, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Antonetti, D.A.; Silva, P.S.; Stitt, A.W. Current understanding of the molecular and cellular pathology of diabetic retinopathy. Nat. Rev. Endocrinol. 2021, 17, 195–206. [Google Scholar] [CrossRef]
- Wilkinson, C.P.; Ferris, F.L.; Klein, R.E.; Lee, P.P.; Agardh, C.D.; Davis, M.; Dills, D.; Kampik, A.; Pararajasegaram, R.; Verdaguer, J.T.; et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology 2003, 110, 1677–1682. [Google Scholar] [CrossRef]
- Early Treatment Diabetic Retinopathy Study Research Group. Grading diabetic retinopathy from stereoscopic color fundus photographs—An extension of the modified Airlie House classification. Ophthalmology 1991, 98, 786–806. [Google Scholar] [CrossRef]
- Brownlee, M. The pathobiology of diabetic complications: A unifying mechanism. Diabetes 2005, 54, 1615–1625. [Google Scholar] [CrossRef]
- Pinazo-Durán, M.D.; Gallego-Pinazo, R.; García-Medina, J.J.; Zanón-Moreno, V.; Nucci, C.; Dolz-Marco, R.; Martínez-Castillo, S.; Galbis-Estrada, C.; Marco-Ramírez, C.; López-Gálvez, M.I.; et al. Oxidative stress and its downstream signaling in aging eyes. Clin. Interv. Aging 2014, 9, 637–652. [Google Scholar] [CrossRef]
- Hammes, H.-P. Diabetic retinopathy: Hyperglycaemia, oxidative stress and beyond. Diabetologia 2018, 61, 29–38. [Google Scholar] [CrossRef]
- Andrés-Blasco, I.; Gallego-Martínez, A.; Machado, X.; Cruz-Espinosa, J.; Di Lauro, S.; Casaroli-Marano, R.; Alegre-Ituarte, V.; Arévalo, J.F.; Pinazo-Durán, M.D. Oxidative Stress, Inflammatory, Angiogenic, and Apoptotic Molecules in Proliferative Diabetic Retinopathy and Diabetic Macular Edema Patients. Int. J. Mol. Sci. 2023, 24, 8227. [Google Scholar] [CrossRef]
- Zhou, J.; Chen, B. Retinal Cell Damage in Diabetic Retinopathy. Cells 2023, 12, 1342. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, X.; Zou, Y.; Han, F. CPSF1 mediates retinal vascular dysfunction in diabetes mellitus via the MAPK/ERK pathway. Arch. Physiol. Biochem. 2022, 128, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Khashaba, N.A.M.; Abdel Hafez, S.M.N.; Abdelzaher, W.Y.; Farid, A.S.; Omran, A.S. Therapeutic effects of selenium nanoparticles versus selenium on experimentally induced diabetic retinopathy via modulation of TLR4/NF-κB/VEGF/connexin 43 signaling. Tissue Barriers 2025, 13, 2491911. [Google Scholar] [CrossRef] [PubMed]
- Yuan, D.; Xu, Y.; Xue, L.; Zhang, W.; Gu, L.; Liu, Q. Resveratrol protects against diabetic retinal ganglion cell damage by activating the Nrf2 signaling pathway. Heliyon 2024, 10, e30786. [Google Scholar] [CrossRef] [PubMed]
- Noma, H.; Yasuda, K.; Shimura, M. Involvement of Cytokines in the Pathogenesis of Diabetic Macular Edema. Int. J. Mol. Sci. 2021, 22, 3427. [Google Scholar] [CrossRef]
- Porter, A.G.; Jänicke, R.U. Emerging roles of caspase-3 in apoptosis. Cell Death Differ. 1999, 6, 99–104. [Google Scholar] [CrossRef]
- Sankaramoorthy, A.; Roy, S. High Glucose-Induced Apoptosis Is Linked to Mitochondrial Connexin 43 Level in RRECs: Implications for Diabetic Retinopathy. Cells 2021, 10, 3102. [Google Scholar] [CrossRef]
- Andrés-Blasco, I.; Gallego-Martínez, A.; Casaroli-Marano, R.P.; López-Murillo, D.; Pinazo-Durán, M.D. Molecular-Genetic Biomarkers of Diabetic Macular Edema. J. Clin. Med. 2024, 13, 7426. [Google Scholar] [CrossRef]
- Maghbooli, Z.; Hossein-nezhad, A.; Larijani, B.; Amini, M.; Keshtkar, A. Global DNA methylation as a possible biomarker for diabetic retinopathy. Diabetes Metab. Res. Rev. 2015, 31, 183–189. [Google Scholar] [CrossRef]
- Karam-Palos, S.; Andrés-Blasco, I.; Campos-Borges, C.; Zanón-Moreno, V.; Gallego-Martínez, A.; Alegre-Ituarte, V.; García-Medina, J.J.; Pastor-Idoate, S.; Sellés-Navarro, I.; Vila-Arteaga, J.; et al. miR-15b-5p targets TP53 and modulates apoptosis and angiogenesis in diabetic retinopathy. J. Transl. Med. 2023, 21, 237. [Google Scholar]
- Sun, H.; Cheng, Y.; Yan, Z.; Liu, X.; Zhang, J. Mining the proliferative diabetic retinopathy-associated genes and pathways by integrated bioinformatic analysis. Int. Ophthalmol. 2020, 40, 269–279. [Google Scholar] [CrossRef]
- Vujosevic, S.; Toma, C.; Di Bisceglie, M.; Villani, E.; Nucci, P.; Brambilla, M.; De Cillà, S.; Midena, E. The role of inflammatory and angiogenic biomarkers in diabetic retinopathy progression. J. Clin. Med. 2020, 9, 2516. [Google Scholar] [CrossRef]
- Yamakawa, N.; Komatsu, H.; Usui, Y.; Tsubota, K.; Wakabayashi, Y.; Goto, H. Immune Mediators Profiles in the Aqueous Humor of Patients with Simple Diabetic Retinopathy. J. Clin. Med. 2023, 12, 6931. [Google Scholar] [CrossRef] [PubMed]
- Maier, R.; Weger, M.; Haller-Schober, E.M.; El-Shabrawi, Y.; Wedrich, A.; Theisl, A.; Aigner, R.; Barth, A.; Haas, A. Multiplex bead analysis of vitreous and serum concentrations of inflammatory and proangiogenic factors in diabetic patients. Mol. Vis. 2008, 14, 637–643. [Google Scholar]
- Kuwabara, T.; Hasegawa, H.; Asano, S.; Yamamoto, M.; Saito, K.; Fujita, T.; Nakamura, Y.; Suzuki, A.; Tanaka, H.; Matsumoto, K. Interleukin-17 contributes to neovascularization and BRB breakdown in diabetic retinopathy. Am. J. Pathol. 2021, 191, 1046–1060. [Google Scholar]
- Zhang, X.; Zhao, L.; Xu, Y.; Li, M.; Chen, H.; Wang, J.; Liu, S.; Wu, Q.; Yang, Z.; Liu, Y. Interleukin-17 promotes angiogenesis by stimulating VEGF production of cancer cells via ERK1/2 pathway. J. Interferon Cytokine Res. 2011, 31, 661–668. [Google Scholar]
- Karin, N. The multiple faces of CXCL10 in autoimmune diseases. J. Immunol. Res. 2010, 184, 2647–2653. [Google Scholar]
- Dong, N.; Xu, B.; Chu, L. Role of inflammation in the pathogenesis of diabetic retinopathy. Int. J. Ophthalmol. 2012, 5, 697–703. [Google Scholar]
- Li, W.; Liu, Y.; Li, X.; Zhang, H.; Chen, J.; Wang, S.; Xu, L.; Yang, Q.; Zhao, R.; Huang, T. Chemokine receptor CXCR3: Role in ocular inflammatory diseases. Mediat. Inflamm. 2020, 2020, 1060921. [Google Scholar]
- Gao, C.; Liu, Y.; Fu, Q.; Zhang, H.; Chen, J.; Wang, S.; Xu, L.; Li, M.; Yang, Q.; Zhao, R. MIP-1β promotes diabetic retinopathy by inducing retinal capillary endothelial cell migration and proliferation. Front. Med. 2023, 10, 1141747. [Google Scholar]
- Seghezzi, G.; Patel, S.; Ren, C.J.; Gualandris, A.; Pintucci, G.; Robbins, E.S.; Shapiro, R.L.; Galloway, A.C.; Rifkin, D.B.; Mignatti, P. Fibroblast growth factor-2 (FGF-2) induces vascular endothelial growth factor (VEGF) expression in endothelial cells. J. Biol. Chem. 1998, 273, 21291–21298. [Google Scholar]
- Farooq, M.; Iqbal, M.; Islam, N.U.; Khan, H.; Ahmad, S.; Shahid, M.; Rehman, A.U.; Ali, Z.; Raza, W.; Tariq, M. Role of basic fibroblast growth factor in diabetic retinopathy: A systematic review. Biomed. Pharmacother. 2023, 162, 114630. [Google Scholar]
- Zhang, C.Y.; Duan, H.X.; Hu, C.X.; Li, J.; Wang, Y.P.; Xu, Q.; Chen, L.; Zhao, M.; Liu, S.; Yang, X. Basic fibroblast growth factor prevents diabetic retinopathy via suppressing the oxidative stress and inflammatory response through the PI3K/AKT pathway. Clin. Exp. Ophthalmol. 2022, 50, 482–494. [Google Scholar]
- Shah, S.; Feher, M.; McGovern, A.; Sherlock, J.; Whyte, M.B.; Munro, N.; Hinton, W.; Gatenby, P.; de Lusignan, S. Diabetic retinopathy in newly diagnosed Type 2 diabetes mellitus: Prevalence and predictors of progression. Diabetes Res. Clin. Pract. 2021, 175, 108776. [Google Scholar] [CrossRef] [PubMed]
- Kropp, M.; Golubnitschaja, O.; Mazurakova, A.; Koklesova, L.; Sargheini, N.; Vo, T.K.S.; de Clerck, E.; Polivka JJr Potuznik, P.; Polivka, J.; Stetkarova, I.; et al. Diabetic retinopathy as the leading cause of blindness and early predictor of cascading complications-risks and mitigation. EPMA J. 2023, 14, 21–42. [Google Scholar] [CrossRef]
- Roig-Revert, M.J.; Lleó-Pérez, A.; Zanón-Moreno, V.; Vivar-Llopis, B.; Marín-Montiel, J.; Dolz-Marco, R.; Alonso-Muñoz, L.; Albert-Fort, M.; López-Gálvez, M.I.; Galarreta-Mira, D.; et al. Enhanced Oxidative Stress and Other Potential Biomarkers for Retinopathy in Type 2 Diabetics: Beneficial Effects of the Nutraceutic Supplements. Biomed Res. Int. 2015, 2015, 408180. [Google Scholar] [CrossRef]
- Rheinberger, M.; Jung, B.; Segiet, T.; Nusser, J.; Kreisel, G.; Andreae, A.; Manz, J.; Haas, G.; Banas, B.; Stark, K.; et al. Poor risk factor control in outpatients with diabetes mellitus type 2 in Germany: The DIAbetes COhoRtE (DIACORE) study. PLoS ONE 2019, 14, e0213157. [Google Scholar] [CrossRef]
- Sanz-González, S.M.; García-Medina, J.J.; Zanón-Moreno, V.; López-Gálvez, M.I.; Galarreta-Mira, D.; Duarte, L.; Valero-Velló, M.; Ramírez, A.I.; Arévalo, J.F.; Pinazo-Durán, M.D. On Behalf of The Valencia Study Group on Diabetic Retinopathy Vsdr Report Number. Clinical and Molecular-Genetic Insights into the Role of Oxidative Stress in Diabetic Retinopathy: Antioxidant Strategies and Future Avenues. Antioxidants 2020, 9, 1101. [Google Scholar] [CrossRef]
- Cuevas Fernández, F.J.; Pérez de Armas, A.; Cerdeña Rodríguez, E.; Hernández Andreu, M.; Iglesias Girón, M.J.; García Marrero, M.R.; Cabrera de León, A.; García Bello, M.Á. Uncontrolled type 2 diabetes in primary care health center: Modifiable factors and target population. Aten. Primaria 2021, 53, 102066. [Google Scholar] [CrossRef]
- Gadde, S.G.K.; Kshirsagar, A.; Anegondi, N.; Mochi, T.B.; Heymans, S.; Ghosh, A.; Roy, A.S. Correlation of Volume of Macular Edema with Retinal Tomography Features in Diabetic Retinopathy Eyes. J. Pers. Med. 2021, 11, 1337. [Google Scholar] [CrossRef]
- Aitchison, R.T.; Kennedy, G.J.; Shu, X.; Mansfield, D.C.; Shahani, U. Sub-clinical thickening of the fovea in diabetes and its relationship to glycaemic control: A study using swept-source optical coherence tomography. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 633–641. [Google Scholar] [CrossRef]
- Oh, J.W.; Ahn, S.J.; Jung, J.H.; Kim, T.W.; Kim, K.P. Proteomic Analysis of Aqueous Humor Identified Clinically Relevant Molecular Targets for Neovascular Complications in Diabetic Retinopathy. Mol. Cell Proteom. 2025, 24, 100953. [Google Scholar] [CrossRef] [PubMed]
- Gomel, N.; Barequet, I.; Lipsky, L.; Bourla, N.; Einan-Lifshitz, A. The effect of the glycemic control on the aqueous humor glucose levels in diabetic patients undergoing elective cataract surgery. Eur. J. Ophthalmol. 2020, 31, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Parsi, S.; Zhu, C.; Motlagh, N.J.; Kim, D.; Küllenberg, E.G.; Kim, H.H.; Gillani, R.L.; Chen, J.W. Basic science of neuroinflammation and involvement of the inflammatory response in disorders of the nervous system. Magn. Reson. Imaging Clin. N. Am. 2024, 32, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Zlotnik, A.; Yoshie, O. The chemokine superfamily revisited. Immunity 2012, 36, 705–716. [Google Scholar] [CrossRef]
- Naveed, M.; Zhou, Q.G.; Han, F. Cerebrovascular inflammation: A critical trigger for neurovascular injury? Neurochem. Int. 2019, 126, 165–177. [Google Scholar] [CrossRef]
- Fahey, E.; Doyle, S.L. IL-1 Family Cytokine Regulation of Vascular Permeability and Angiogenesis. Front Immunol. 2019, 10, 1426. [Google Scholar] [CrossRef]
- Taghavi, Y.; Hassanshahi, G.; Kounis, N.G.; Koniari, I.; Khorramdelazad, H. Monocyte chemoattractant protein-1 (MCP-1/CCL2) in diabetic retinopathy: Latest evidence and clinical considerations. J. Cell Commun. Signal. 2019, 13, 451–454. [Google Scholar] [CrossRef]
- Jiang, P.; Zhang, Y.; Ru, B.; Yang, Y.; Vu, T.; Paul, R.; Mirza, A.; Altan-Bonnet, G.; Liu, L.; Ruppin, E.; et al. Systematic investigation of cytokine signaling activity at the tissue and single-cell levels. Nat. Methods 2021, 18, 1181–1191. [Google Scholar] [CrossRef]
- Obadă, O.; Pantalon, A.D.; Rusu-Zota, G.; Hăisan, A.; Lupuşoru, S.I.; Constantinescu, D.; Chiseliţă, D. Aqueous Humor Cytokines in Non-Proliferative Diabetic Retinopathy. Medicina 2022, 58, 909. [Google Scholar] [CrossRef]
- Zegeye, M.M.; Andersson, B.; Sirsjö, A.; Ljungberg, L.U. IL-6 trans-Signaling Impairs Sprouting Angiogenesis by Inhibiting Migration, Proliferation and Tube Formation of Human Endothelial Cells. Cells 2020, 9, 1414. [Google Scholar] [CrossRef]
- Canataroglu, H.; Varinli, I.; Ozcan, A.A.; Canataroglu, A.; Doran, F.; Varinli, S. Interleukin (IL)-6, Interleukin (IL)-8 Levels and Cellular Composition of the Vitreous Humor in Proliferative Diabetic Retinopathy, Proliferative Vitreoretinopathy, and Traumatic Proliferative Vitreoretinopathy. Ocul. Immunol. Inflamm. 2005, 13, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Loporchio, D.F.; Tam, E.K.; Cho, J.; Chung, J.; Jun, G.R.; Xia, W.; Fiorello, M.G.; Siegel, N.H.; Ness, S.; Stein, T.D.; et al. Cytokine Levels in Human Vitreous in Proliferative Diabetic Retinopathy. Cells 2021, 10, 1069. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhao, T.; Sun, Y. Interleukin-17A in diabetic retinopathy: The crosstalk of inflammation and angiogenesis. Biochem. Pharmacol. 2024, 225, 116311. [Google Scholar] [CrossRef]
- Chibber, R.; Ben-Mahmud, B.M.; Chibber, S.; Kohner, E.M. Leukocytes in diabetic retinopathy. Curr. Diabetes Rev. 2007, 3, 3–14. [Google Scholar] [CrossRef]
- Stanley, E.R.; Biundo, F.; Gökhan, Ş.; Chitu, V. Differential regulation of microglial states by colony stimulating factors. Front Cell Neurosci. 2023, 17, 1275935. [Google Scholar] [CrossRef]
- Sajadi, S.M.; Khoramdelazad, H.; Hassanshahi, G.; Rafatpanah, H.; Hosseini, J.; Mahmoodi, M.; Arababadi, M.K.; Derakhshan, R.; Hasheminasabzavareh, R.; Hosseini-Zijoud, S.M.; et al. Plasma levels of CXCL1 (GRO-alpha) and CXCL10 (IP-10) are elevated in type 2 diabetic patients: Evidence for the involvement of inflammation and angiogenesis/angiostasis in this disease state. Clin. Lab. 2013, 59, 133–137. [Google Scholar] [CrossRef]
- Gupta, N.; Mansoor, S.; Sharma, A.; Sapkal, A.; Sheth, J.; Falatoonzadeh, P.; Kuppermann, B.; Kenney, M. Diabetic retinopathy and VEGF. Open Ophthalmol. J. 2013, 7, 4–10. [Google Scholar] [CrossRef]
- Bahr, T.A.; Bakri, S.J. Update on the Management of Diabetic Retinopathy: Anti-VEGF Agents for the Prevention of Complications and Progression of Nonproliferative and Proliferative Retinopathy. Life 2023, 13, 1098. [Google Scholar] [CrossRef]
- Wu, H.; Wang, M.; Li, X.; Shao, Y. The Metaflammatory and Immunometabolic Role of Macrophages and Microglia in Diabetic Retinopathy. Hum. Cell 2021, 34, 1617–1628. [Google Scholar] [CrossRef]
- Saxena, S.; Lai, T.Y.; Koizumi, H.; Farah, M.E.; Ferrara, D.; Pelayes, D.; Sato, T.; Meyer, C.H.; Murray, T.; International Pharmacokinetic Collaboration. Anterior chamber paracentesis during intravitreal injections in observational trials: Effectiveness and safety and effects. Int. J. Retin. Vitr. 2019, 5, 8. [Google Scholar] [CrossRef]
- Wilson, S.; Siebourg-Polster, J.; Titz, B.; Jiang, Z.; Bartolo, F.; Lavergne, V.; Gayán, J.; Garweg, J.G.; Fauser, S.; Dieckmann, A. Correlation of aqueous, vitreous, and serum protein levels in patients with retinal diseases. Transl. Vis. Sci. Technol. 2023, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Pinazo-Durán, M.D.; Zanón-Moreno, V.; García-Villanueva, C.; Martucci, A.; Peris-Martínez, C.; Vila-Arteaga, J.; García-Medina, J.J.; Andrés-Blasco, I.; Gallego-Martínez, A.; Nucci, C.; et al. Biochemical-molecular-genetic biomarkers in the tear film, aqueous humor, and blood of primary open-angle glaucoma patients. Front. Med. 2023, 10, 1157773. [Google Scholar] [CrossRef] [PubMed]
- Pinazo-Durán, M.D.; García-Medina, J.J.; Bolarín, J.M.; Sanz-González, S.M.; Valero-Vello, M.; Abellán-Abenza, J.; Zanón-Moreno, V.; Moreno-Montañés, J. Computational Analysis of Clinical and Molecular Markers and New Theranostic Possibilities in Primary Open-Angle Glaucoma. J. Clin. Med. 2020, 9, 3032. [Google Scholar] [CrossRef] [PubMed]
- Okuwobi, I.P.; Shen, Y.; Li., M.; Fan, W.; Yuan, S.; Chen, Q. Hyperreflective Foci Enhancement in a Combined Spatial-Transform Domain for SD-OCT Images. Transl. Vis. Sci. Technol. 2020, 9, 19. [Google Scholar] [CrossRef]
- Rodríguez Del Águila, M.; González-Ramírez, A. Sample size calculation. Allergol. Immunopathol. 2014, 42, 485–492. [Google Scholar] [CrossRef]
- International Council of Ophthalmology. ICO Guidelines for Diabetic Eye Care: Initial and Follow-Up Evaluation. Available online: https://www.icoph.org/downloads/ICOGuidelinesforDiabeticEyeCare.pdf (accessed on 1 May 2025).
- Sharma, R.K.; Rogojina, A.T.; Chalam, K.V. Multiplex immunoassay analysis of biomarkers in clinically accessible quantities of human aqueous humor. Mol. Vis. 2009, 15, 60–69. [Google Scholar]
- Muether, P.S.; Droege, K.M.; Fauser, S. Vascular endothelial growth factor suppression times in patients with diabetic macular oedema treated with ranibizumab. Br. J. Ophthalmol. 2014, 98, 179–181. [Google Scholar] [CrossRef]
- Proust-Lima, C.; Liquet, B. Estimation of extended mixed models using latent classes and latent processes: The R package lcmm. J. Stat. Softw. 2017, 78, 1–56. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | SCG (n = 36) | T2DM–DR (n = 42) | T2DM + DR (n = 38) |
|---|---|---|---|
| Age (years) | 59 ± 5 | 62 ± 5 | 65 ± 7 |
| Sex (male/female) | 16/20 | 22/20 | 26/12 |
| T2DM duration (years) | – | 15 ± 6 | 17 ± 8 |
| T2DM familial History (%) | 23% | 58% | 72% |
| Eye Parameters | SCG (n = 36) | T2DM–DR (n = 42) | T2DM + DR (n = 38) |
|---|---|---|---|
| BCVA LogMAR RE | 0.09 | 0.30 | 0.44 |
| BCVA LogMAR LE | 0.08 | 0.35 | 0.52 |
| IOP RE (mm Hg) | 14 ± 3 | 16 ± 3 | 17 ± 2 |
| IOP LE (mm Hg) | 15 ± 2 | 16 ± 2 | 16 ± 2 |
| CSFT RE (µm) | 248 ± 20 | 295 ± 26 | 335 ± 34 |
| CSFT LE (µm) | 257 ± 21 | 275 ± 23 | 282 ± 25 |
| Variables | SCG (n = 36) | T2DM–DR (n = 42) | T2DM + DR (n = 38) |
|---|---|---|---|
| Basal Glycemia (mg/dL) | 87 ± 8 | 124 ± 25 | 134 ± 32 |
| HbA1c (%) | 5.5 ± 0.3 | 6.8 ± 0.7 | 7.2 ± 1.1 |
| Total Chol (mg/dL) | 136 ± 34 | 186 ± 39 | 198 ± 42 |
| Triglycerides (mg/dL) | 76 ± 12 | 122 ± 15 | 130 ± 18 |
| Cytokine | MDC (pg/mL) | AH Sampling According to MDC (%) |
|---|---|---|
| IL-1ra | 2.13 | 80 |
| IL-1β | 1.41 | 90 |
| IL-2 | 0.56 | 78 |
| IL-4 | 0.21 | 0 |
| IL-5 | 2.50 | 0 |
| IL-6 | 4.04 | 100 |
| IL-7 | 1.71 | 76 |
| IL-8 | 0.71 | 55 |
| IL-9 | 0.50 | 0 |
| IL-10 | 1.29 | 92 |
| IL-12 | 7.76 | 100 |
| IL-13 | 1.36 | 58 |
| IL-15 | 3.42 | 95 |
| IL-17 | 2.42 | 95 |
| bFGF | 7.28 | 85 |
| EOTAXIN | 2.10 | 0 |
| G-CSF | 2.05 | 0 |
| GM-CSF | 41.08 | 100 |
| IP10 | 23.08 | 100 |
| IFγ | 1.70 | 0 |
| MIP1α | 1.10 | 0 |
| MIP1β | 5.76 | 100 |
| MCP1 | 139.12 | 100 |
| RANTES | 0.87 | 92 |
| TNFα | 5.10 | 0 |
| PDGF | 1.60 | 0 |
| VEGF | 2.30 | 100 |
| Parameters (pg/mL) | SCG Mean ± SD | T2DMG–DR Mean ± SD | T2DMG + DR Mean ± SD | p-Value SCG vs. –DR | p-Value SCG vs. +DR | p-Value –DR vs. +DR |
|---|---|---|---|---|---|---|
| IL-1β | 1.64 ± 0.23 | 4.7 ± 3.25 | 7 ± 2.09 | 0.0142 | 0.1630 | 0.0014 |
| IL-1Ra | 4.03 ± 1.9 | 5.91 ± 3.67 | 18.54 ± 0.09 | 0.0019 | 0.0002 | 0.4317 |
| IL-2 | 1.05 ± 0.49 | 0.57 ± 0.25 | 0.41 ± 0.12 | 0.1572 | 0.0573 | 0.3669 |
| IL-6 | 5.24 ± 1.20 | 8.88 ± 2.8 | 11.81 ± 3.32 | 0.0237 | 0.0007 | 0.0575 |
| IL-7 | 3.53 ± 1.82 | 3.32 ± 2.03 | 2.89 ± 1.17 | 0.8778 | 0.6605 | 0.7676 |
| IL-8 | 0.79 ± 0.08 | 1.62 ± 0.73 | 2.85 ± 0.95 | 0.0016 | 0.0002 | 0.0050 |
| IL-10 | 2.87 ± 1.58 | 3.60 ± 0.94 | 5.30 ± 2.82 | 0.5703 | 0.0784 | 0.2417 |
| IL-12 | 12.58 ± 4.92 | 11.30 ± 4.5 | 10.81 ± 3.03 | 0.3709 | 0.2242 | 0.7273 |
| IL-13 | 2.44 ± 1.08 | 2.24 ± 1.86 | 2.12 ± 1.85 | 0.8819 | 0.8123 | 0.9289 |
| IL-15 | 5.15 ± 2.08 | 8.05 ± 3.12 | 10.69 ± 2.33 | 0.0821 | 0.0023 | 0.0597 |
| IL-17 | 4.53 ± 2.11 | 6.95 ± 2.5 | 11.14 ± 4.31 | 0.0119 | 0.0006 | 0.1069 |
| bFGF | 12.75 ± 5.47 | 17.3 ± 8.09 | 26.12 ± 10.18 | 0.0076 | 1.94 × 10−6 | 7.30 × 10−5 |
| GM-CSF | 50.58 ± 9.5 | 74.48 ± 8.99 | 91.32 ± 11.16 | 7.91 × 10−9 | 4.21 × 10−11 | 2.27 × 10−7 |
| IP-10 | 51.68 ± 28.6 | 137.33 ± 106.5 | 205.31 ± 92.18 | 2.59 × 10−14 | 4.68 × 10−17 | 1.60 × 10−13 |
| MIP-1β | 7.82 ± 2.06 | 13.89 ± 3.74 | 18.32 ± 5.15 | 0.0012 | 1.67 × 10−5 | 0.0088 |
| MCP-1 | 198.61 ± 59.49 | 267.53 ± 60.12 | 310.41 ± 71.28 | 2.27 × 10−13 | 1.82 × 10−15 | 2.53 × 10−11 |
| RANTES | 2.03 ± 1.16 | 6.68 ± 4.01 | 5.56 ± 7.71 | 0.0003 | 0.0221 | 0.1868 |
| VEGF | 65.26 ± 20.8 | 97.36 ± 22.24 | 118.4 ± 30.16 | 4.42 × 10−10 | 3.01 × 10−12 | 2.71 × 10−8 |
| Inclusion | Exclusion |
|---|---|
| Individuals of both sexes aged 40–80 years | Individuals of both sexes, younger than 40 years or older than 80 years |
| Accurate NPDR diagnosis for the corresponding group of T2DM participants | Other DM or DR type |
| Non-diabetic healthy individuals for the surrogate comparative group of participants (SCG) | Other ocular diseases and/or comorbidities. Patients receiving local or systemic treatment that may interfere with the study. Eye/laser surgery in the previous 12 months |
| Precise and complete data included in the clinical history | Clinical history including any diagnosis that did not fit with the study’s purpose |
| Adequate psycho-physical status for participating in the study | Unfeasibility for having a thorough and complete clinical history. Unable to participate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alegre-Ituarte, V.; Andrés-Blasco, I.; Peña-Ruiz, D.; Di Lauro, S.; Crespo-Millas, S.; Martucci, A.; Vila-Arteaga, J.; Pinazo-Durán, M.D.; Galarreta, D.; García-Feijoo, J. Exploring Molecular Signatures Associated with Inflammation and Angiogenesis in the Aqueous Humor of Patients with Non-Proliferative Diabetic Retinopathy. Int. J. Mol. Sci. 2025, 26, 6461. https://doi.org/10.3390/ijms26136461
Alegre-Ituarte V, Andrés-Blasco I, Peña-Ruiz D, Di Lauro S, Crespo-Millas S, Martucci A, Vila-Arteaga J, Pinazo-Durán MD, Galarreta D, García-Feijoo J. Exploring Molecular Signatures Associated with Inflammation and Angiogenesis in the Aqueous Humor of Patients with Non-Proliferative Diabetic Retinopathy. International Journal of Molecular Sciences. 2025; 26(13):6461. https://doi.org/10.3390/ijms26136461
Chicago/Turabian StyleAlegre-Ituarte, Víctor, Irene Andrés-Blasco, David Peña-Ruiz, Salvatore Di Lauro, Sara Crespo-Millas, Alessio Martucci, Jorge Vila-Arteaga, María Dolores Pinazo-Durán, David Galarreta, and Julián García-Feijoo. 2025. "Exploring Molecular Signatures Associated with Inflammation and Angiogenesis in the Aqueous Humor of Patients with Non-Proliferative Diabetic Retinopathy" International Journal of Molecular Sciences 26, no. 13: 6461. https://doi.org/10.3390/ijms26136461
APA StyleAlegre-Ituarte, V., Andrés-Blasco, I., Peña-Ruiz, D., Di Lauro, S., Crespo-Millas, S., Martucci, A., Vila-Arteaga, J., Pinazo-Durán, M. D., Galarreta, D., & García-Feijoo, J. (2025). Exploring Molecular Signatures Associated with Inflammation and Angiogenesis in the Aqueous Humor of Patients with Non-Proliferative Diabetic Retinopathy. International Journal of Molecular Sciences, 26(13), 6461. https://doi.org/10.3390/ijms26136461