Abstract
Cyclophosphamide (CPX) is an alkylating agent commonly used for various hematological and solid malignancies. In addition to its use as a cytotoxic agent to directly kill tumor cells, numerous immunomodulatory properties of CPX in the tumor microenvironment (TME) of several cancer types have also been documented. These properties include the selective depletion of immune-suppressive regulatory T cells (Tregs), triggering of immunogenic cell death (ICD) and enhanced antigen presentation, and release of type I interferons (IFNs). Moreover, preclinical models as well as human clinical trials have investigated the efficacy of the low-dose “metronomic” scheduling of CPX in combination with immunotherapies such as immune checkpoint inhibitors, dendritic cell tumor vaccines, and tumor antigen peptide vaccines. The metronomic dosing schedule involves administering a continuous (or frequent, such as daily) low dose of chemotherapy rather than using the canonical approach of administering the maximum tolerated dose. Despite the approval of immune checkpoint inhibitors for clinical usage against an increasing number of cancers, many malignancies simply do not respond to checkpoint inhibition, in part due to the heterogeneous intratumoral network of immune-suppressive cell populations. The immunomodulatory effects of cyclophosphamide have strong translational applicability and could serve to enhance and bolster anti-tumor immunity, potentially synergizing with immune checkpoint inhibitors and other existing immunotherapy agents.
1. Introduction
Chemotherapeutic agents have historically been a part of the standard treatment modalities for many malignancies, and they serve to directly destroy actively dividing tumor cells. Despite the use of chemotherapies as the backbone of anti-cancer treatment regimens, many patients eventually develop therapeutic resistance and tumor relapse. While the development of immune checkpoint inhibitors and other novel immunotherapies for use as second-line therapies has been a significant advancement in the treatment of cancer, unfortunately many patients do not achieve complete remission and therefore still succumb to their disease.
There are several tumor types (so-called “cold” tumors) that tend to lack an inflammatory phenotype and the presence of anti-tumor infiltrating immune cells [1], which is partially attributable to the highly immune-suppressive tumor microenvironment (TME) in these cancers. Tumors can contain myriad immune-suppressive cell populations such as M2 macrophages, regulatory T cells (Tregs), and myeloid-derived suppressor cells (MDSCs) that release cytokines and growth factors which lead to impaired anti-tumor immunity. Moreover, these cell populations have been well known to express high levels of cell-surface immune-inhibitory molecules such as cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), programmed cell death protein 1 (PD-1), and programmed death-ligand 1 (PD-L1).
Cyclophosphamide (CPX) has been routinely utilized as a chemotherapeutic for a variety of malignancies, including lymphoma, leukemia, and neuroblastoma. In vivo, CPX is metabolized by the liver via the cytochrome P450 pathway, resulting in multiple metabolites (Figure 1). The primary CPX metabolite that initiates the cytotoxic effect of this drug is phosphoramide mustard. Phosphoramide mustard forms irreversible cross-linkages in and between deoxyribonucleic acid (DNA) of actively dividing tumor cells at the N-7 guanosine position, leading to cell death [2].
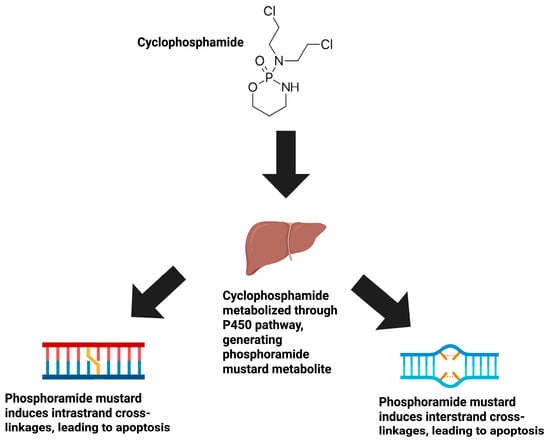
Figure 1.
The mechanism of action of CPX. CPX exists as a prodrug compound, requiring subsequent biochemical metabolism via the P450 pathway in the liver. This biochemical pathway converts the CPX prodrug into its active metabolite, phosphoramide mustard. Phosphoramide mustard then proceeds to induce intrastrand and interstrand cross-linkages at the N7 position of DNA in actively dividing tumor cells, leading to apoptosis.
In recent years, there has been considerable interest in the immunomodulatory properties of chemotherapeutic agents, including the immunomodulatory effects of CPX. In this review, the immunomodulatory properties of CPX will be outlined, specifically its abilities to selectively target immune-suppressive Tregs, promote the induction of immunogenic cell death (ICD), improve antigen presentation, affect immune checkpoint and major histocompatibility complex (MHC) class I expression on tumor cells, and induce type I interferons (IFNs) (Figure 2). Due to the discovery of these effects, CPX has been identified as a means to induce an immunologically “hot” tumor phenotype in immunologically “cold” tumor types. This review will also present the potential advantages of using a metronomic dosing schedule of CPX concurrently to bolster the impact of immunotherapies such as immune checkpoint inhibitors, tumor antigen vaccines, and dendritic cell vaccines.
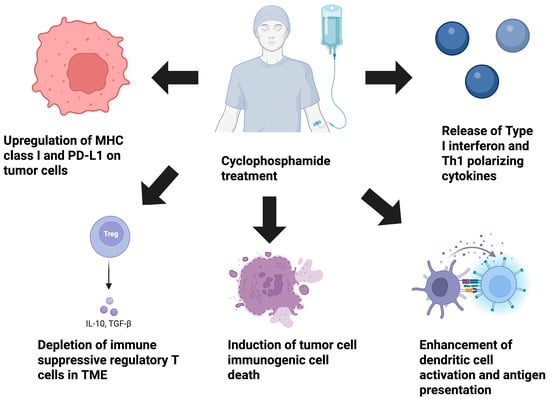
Figure 2.
The immunomodulatory properties of CPX. The schematic image articulates the immune-modulating properties of the alkylating agent CPX. Preclinical studies of CPX have demonstrated that it is capable of restructuring the TME and bolstering anti-tumor immunity. CPX can deplete immune-suppressive regulatory T cells, trigger ICD through damage-associated molecular pattern release, augment dendritic cell antigen presentation, and modify the cytokine milieu within the TME through promoting the release of type I IFN and Th1 polarizing cytokines such as IFN-γ and IL-12. Lastly, CPX can enhance the immunogenicity of tumor cells directly by up-regulating MHC class I expression (enhancing the ability of cytotoxic T cells to eliminate tumor cells), and the immune checkpoint molecule PD-L1 (increasing susceptibility to PD-L1 checkpoint blockade). CPX, cyclophosphamide; ICD, immunogenic cell death; IFN, interferon; TME, tumor microenvironment; MHC, major histocompatibility complex class I; PD-L1, programmed death-ligand 1.
2. Selective Depletion of Immune-Suppressive Cell Populations Within the TME
Studies have documented the capability of CPX to selectively target and deplete immune-suppressive cell populations such as Tregs. Under normal physiological conditions, Tregs serve to maintain peripheral tolerance and restrain autoimmunity [3]. In the context of the TME, Tregs are highly effective at dampening anti-tumor immunity through several mechanisms, including the following: the expression of constitutively high levels of the immune checkpoint molecules CTLA-4 and PD-1, release of immune suppressive cytokines such as interleukin (IL)-10 and transforming growth factor (TGF)-β, metabolic consumption of IL-2 through expression of the high affinity chain of the IL-2R (CD25), and direct killing of effector CD8+ T cells [4].
Multiple studies have highlighted the ability of CPX to selectively deplete immune-suppressive Tregs in the TME. While the exact mechanism by which CPX selectively targets Tregs is still not fully understood, in vitro studies have suggested that Tregs express low levels of the adenosine triphosphate (ATP) influx and efflux receptors CD39 and CD73. Both CD39 and CD73 are important mediators of intracellular ATP levels. ATP, while commonly known as an energy source, is also integral for the generation of the antioxidant glutathione. Glutathione has been shown to reverse the DNA damage associated with CPX metabolites. The low expression of Treg CD39/73 reduces Tregs’ ability to correct and repair CPX-mediated DNA damage, leading to cell death [5]. A study published by Leong et al. in 2019 demonstrated that low-dose CPX (at 40 mg/kg) significantly reduced the frequency of intratumoral Tregs in a syngeneic CT26 murine model of colon carcinoma [6]. The investigators further reported that low-dose CPX synergized with a novel in situ vaccination with a CpG-class Toll-like receptor (TLR9) agonist, generating superior induction of CD8+ T cell responses and polarization of macrophages towards an M1 phenotype. Moreover, a report published by Zhong et al. demonstrated that treatment of a murine model of Lewis lung carcinoma with 150 mg/kg CPX reduced CD4+CD25+FoxP3+ Tregs (in both the spleen and TME) and increased the proportion of CD4+ and CD8+ T cells [7]. Huang et al. published data further demonstrating that low-dose metronomic CPX administration significantly reduced levels of intratumoral Tregs and reduced the levels of IL-10 and TGF-β in a metastatic murine model of CT26 colon adenocarcinoma [8]. In short, several preclinical models of cancer have shown the potency of CPX in selectively depleting Tregs in the TME, which serves to shift the ratio of effector CD8+ T cells to Tregs toward a greater proportion of effector CD8+ T cells in the TME. This ratio of CD8+ T cells to Tregs has been well characterized as a crucial positive prognostic indicator in multiple cancer types. Thus, shifting the balance of T cell populations to favor greater quantities of CD8+ T cells by selectively depleting Tregs with chemotherapeutic agents such as CPX is a strategic tactic that warrants significant interest.
3. Influence of CPX on ICD in Cancer
ICD is an inflammatory and immunogenic form of apoptosis whereby damaged tumor cells release damage-associated molecular patterns that can be taken up by antigen-presenting cells such as dendritic cells and lead to the induction of anti-tumor immunity. These damage-associated molecular patterns include high-mobility group box protein 1 (HMGB1), ecto-calreticulin (ecto-CRT), and extracellular ATP [9,10]. HMGB1 is a chromatin-binding protein that plays a role in regulating transcription by interacting with chromatin, nucleosomes, and histones. CRT is a chaperone protein that is normally expressed on the endoplasmic reticulum and sarcoplasmic reticulum of eukaryotic cells. During states of cellular stress, both HMGB1 and CRT are translocated to the cell surface. HMGB1 is released into the extracellular space while CRT is directly expressed on the cell surface. Several in vivo and in vitro studies have indicated that CPX is able to induce ICD. A study published by Webb et al. in 2022 showed that low-dose CPX induced HMGB1 release, using both in vitro and in vivo models of neuroblastoma [11]. The induction of ICD has been shown to increase dendritic cell activation and lead to more robust T helper 1 (Th1) immunity and superior priming of CD8+ T cell responses. The release of HMGB1 has been demonstrated to increase dendritic cell activation and antigen presentation capability through the activation of TLR2 and TLR4 on dendritic cells [12]. CRT expression of damaged tumor cells has been shown to also enhance dendritic cell antigen presentation and IL-12 secretion through the activation of the TLR4/MyD88 signaling pathway.
4. CPX’s Impact on Myeloid Cell Activation
Myeloid cells, such as macrophages and dendritic cells, are antigen-presenting cells that are key mediators of robust anti-tumor immunity [13]. Macrophages can also phagocytose and directly kill tumor cells through the release of lytic enzymes and reactive oxygen species. Dendritic cells are professional antigen-presenting cells that are regarded as potent activators of CD4+ and CD8+ T cell responses. Investigators have shown that low-dose CPX can trigger ICD, which has been shown to enhance antigen presentation and lead to T cell responses in various in vivo models of cancer [14,15]. Low-dose CPX has been shown to restructure the TME, polarizing macrophages to an M1 anti-tumoral phenotype and increasing the production of IL-6 and IL-12 [16]. Moreover, such M1 macrophages generated reduced levels of IL-10 and TGF-β. The triggering of ICD due to low-dose CPX treatment has been shown to produce abundant damage-associated molecular patterns that are potent ligands of dendritic cell TLRs, and their binding to these TLRs induces dendritic cell maturation and antigen presentation. Specifically, low-dose CPX has been shown to release damage-associated molecular patterns such as extracellular ATP and Annexin A1 in multiple in vitro studies, leading to the increased dendritic cell activation of T cell responses [17].
Using a model of colon carcinoma, Radojcic et al. published in 2010 a report that showed low- to moderate-dose CPX was capable of triggering increased production of IL-12 and tumor necrosis factor (TNF)-α, key indicators of Th1 immunity [18]. Shurin et al. (2009) further articulated the effects of low-dose CPX on dendritic cell activation, showing significant up-regulation of the co-stimulatory molecules and antigen-presenting molecules CD40, CD80, CD86, and MHC class II [19]. One of the key bottlenecks in effective cancer immunotherapy responses is proper antigen presentation. The immune suppressive nature of the cancer TME can often render antigen-presenting cells such as dendritic cells unable to properly activate effector immune cell populations. Consequently, these studies highlight a novel application of low-dose CPX to improve defective antigen presentation.
5. Direct Effects of CPX on Tumor Cells
Previous studies in preclinical models of cancer have indicated that chemotherapeutic agents such as CPX can often have direct effects on tumor cells that are relevant to immune responses, including up-regulating the expression of immune checkpoint molecules such as PD-L1 and of MHC class I molecules [6,20,21,22,23]. The tumor cell up-regulation of immune checkpoint molecules is a critical immune escape mechanism, and this provides the scientific basis for the use of immune checkpoint inhibitors for multiple tumor types. MHC class I is a critical antigen-presenting molecule that is required for direct, antigen-specific tumor cell killing by CD8+ T cells. As an additional immune escape mechanism, tumor cells will often down-regulate MHC class I expression to evade detection and lysis by CD8+ T cells. In a study published by Peng et al. in 2015, low doses of CPX were shown to up-regulate surface PD-L1 and MHC class I expression in various in vitro experiments using ID8 ovarian cancer cells [24]. Low-dose CPX further sensitized ID8 tumor-bearing mice to anti-PD-L1 blockade and increased the proportion of effector tumor-infiltrating leukocytes in vivo. Moreover, in a study published by Khan et al. in 2020, low-dose CPX was once again shown to potentiate up-regulation of PD-L1, sensitizing 4T1 triple-negative breast cancer tumor-bearing mice to anti-PD-L1 blockade in vivo [20]. These studies highlight a novel treatment paradigm in which low-dose chemotherapy can be used strategically to up-regulate key immune checkpoint molecules to enhance the clinical efficacy of immune checkpoint blockade in immunologically cold tumor types.
6. CPX Stimulation of Type I IFN Release
Type I IFNs comprise a subset of cytokines that modulate and control inflammation and the activity of various immune cell types such as T cells, B cells, and dendritic cells. Type I IFN has been shown to play a role in both anti-viral and anti-tumor immunity. The activation of the receptors for IFN-a and -b induces downstream signaling via Janus kinase/signal transducers and activators of transcription (JAK/STAT), mitogen-activated protein kinase (MAPK), nuclear factor kappa B (NF-κB), and phosphoinositide 3-kinase/Akt (PI3K/Akt) signaling for the downstream activation of IFN and pro-inflammatory cytokine-mediating genes. In vitro assays have demonstrated that CPX can trigger the release of type I IFN, enhancing the immunogenicity of tumor cells directly as well as improving anti-tumor immunity mediated by key immune cell types such as dendritic cells, CD4+ and CD8+ T cells, macrophages, and natural killer (NK) cells [25,26,27,28,29,30,31,32].
Type I IFN release has been shown to enhance dendritic cell activation and antigen presentation through the up-regulation of co-stimulatory molecules CD80/86 and CD40, as well as MHC class II expression in vivo. Type I IFN-stimulated dendritic cells display an improved capacity to prime both CD4+ and CD8+ T cell responses in multiple preclinical models of solid tumors. In a report published by Schiavoni et al. in 2011, low-dose CPX was shown to release significant amounts of type I IFN, leading to the superior induction of CD8α+ dendritic cells and priming of IFN-γ+ CD8+ T cells in an EG7 thymoma mouse model [33]. In a model of murine glioma, Du et al. (2020) demonstrated that low-dose CPX generated type I IFN release from GL261 and CT-2A murine glioma cells in vitro [34]. These results were then followed by in vivo studies in GL261 tumor-bearing mice, showing that tumor peptide vaccine synergizes with type I IFN release induced by CPX in vivo. These studies highlight the therapeutic potential of low-dose CPX to bolster the clinical efficacy of other novel immunotherapies against multiple tumor types.
7. CPX’s Influence on Th1 Immunity
Durable anti-tumor immunity is contingent on a multitude of concurrent immunological signaling cascades and activation of long-term effector immune cell activity. Broadly speaking, Th1 immune responses often take place in response to intracellular pathogens but are also crucial for anti-tumor immunity. Th1 immune responses are of a cell-mediated phenotype and are orchestrated by dendritic cells, CD8+ T cells, NK cells, M1 macrophages, and CD4+ T cells. Extensive study into how low-dose CPX can shift the immune phenotype post-treatment has indicated that low-dose CPX can restructure the TME to produce Th1 immunity. A study published by Malvicini et al. in 2009 showed that low-dose CPX in conjunction with IL-12 synergized to induce superior levels of CD4+ Th1 cells producing IFN-γ in an in vivo model of CT26 colon adenocarcinoma [35]. Likewise, a publication by Matar and colleagues in 2002 indicated that a single low-dose injection of CPX into lymphoma-bearing rats shifted splenic immune cell phenotypes from predominantly Th2 skewed to Th1 skewed, once again leading to superior production of IFN-γ and TNF-α-producing T cells [36]. The levels of immune suppressive cytokines IL-10, TGF-β, and nitric oxide were also highly reduced, further showing low-dose CPX’s ability to shift the immune response phenotype to an anti-tumor, cell-mediated Th1 phenotype.
8. Metronomic Low-Dose Administration of Chemotherapy
Canonically, chemotherapy is typically administered to cancer patients for the purpose of killing as many actively dividing and proliferating tumor cells as possible to maximize the patients’ chances of survival. Moreover, chemotherapy is generally given at or near the maximum tolerated dose, and therefore it often leads to severe toxicity and the potential for long-term complications in patients who are long-term survivors. In addition, while conventional high-dose CPX administration can directly kill tumor cells for tumor debulking, this high-dose administration often depletes key immune cell populations such as T cells, NK cells, and dendritic cells, which are crucial for robust anti-tumor immunity. High-dose administration of CPX is often associated with significant toxicities and side effects, including anemia, neutropenia, nausea, vomiting, cognitive fog, and infertility [37,38]. More severe side effects such as cardiac toxicities and hemorrhagic cystitis have also been documented during high-dose CPX treatment. These side effects often have significant adverse effects on the overall quality of life during and potentially after treatment. Over the past several years, the notion of low-dose metronomic chemotherapy administration has garnered more attention in preclinical cancer models as well as human clinical trials of various cancer types to reduce severe toxicities [39,40]. This treatment approach involves administering continuous, regularly scheduled, low doses of chemotherapy as a supplemental treatment to standard of care cancer immunotherapies. The advantages of low-dose metronomic chemotherapy are numerous, including unique immunomodulatory properties of chemotherapy on the TME as well as tumor cells individually, the decreased angiogenesis of solid tumors, and significantly less severe toxicity [37,38,39,40,41,42]. Evidence for CPX’s anti-angiogenic effects was published by Peyrl et al. (2023), who demonstrated that a dual treatment of low-dose oral tablet CPX plus etoposide in conjunction with bevacizumab exhibited potent anti-angiogenic properties in patients with recurrent medulloblastoma [41]. The median overall survival was 25.5 months with a progression-free survival (PFS) of 8.5 months. It was also noted that of the patients who exhibited a positive clinical response, the 5-year PFS was 66.7%, highlighting the potential anti-angiogenic properties of low-dose CPX and etoposide.
9. Metronomic Low-Dose Administration of CPX to Enhance Existing Cancer Immunotherapy in Preclinical Cancer Models
Due to the growing body of data highlighting the immunomodulatory effects of metronomic CPX, researchers have begun evaluating the efficacy of combining metronomic chemotherapy with current immunotherapies in both preclinical models and human clinical trials [11,42,43,44,45,46,47,48,49,50]. In this section, we will provide an overview of the increasing evidence for the therapeutic efficacy of metronomic CPX treatment in conjunction with existing cancer immunotherapies. Through testing with in vivo preclinical models of cancer, metronomic CPX has been shown to enhance the effectiveness of immune checkpoint inhibitors, tumor peptide vaccines, and other immunomodulatory anti-cancer agents [11,51,52,53,54]. For example, in a report published by Weir and colleagues in 2014, metronomic low-dose CPX was demonstrated to enhance anti-tumor immunity in conjunction with a novel tumor peptide vaccine that was tested in C3 tumor-bearing mice [52]. ELISpot and flow cytometry assays showed significant increases in IFN-γ-secreting CD8+ T cells. Adoptive transfer experiments indicated durable immunological memory that was transferable from mice treated with low-dose CPX and peptide vaccine to naïve mice. Park et al. published in 2011 that low-dose CPX plus dendritic cell vaccine derived from irradiated tumor cells improved the control of tumor growth kinetics, reduced intratumoral regulatory cells, and reduced levels of immune suppressive IL-10 and TGF-β in a model of mammary carcinoma [53]. Pfirschke et al. (2016) showed that metronomic low-dose CPX and oxaliplatin combined with either anti-CTLA4 or anti-PD-1 blockade generated superior induction of CD8+ T cells in a TLR-4 dependent manner in a model of pancreatic ductal adenocarcinoma [54].
10. Metronomic Low-Dose Administration of CPX to Enhance Existing Cancer Immunotherapy in Clinical Trials
The metronomic administration of chemotherapeutic agents such as CPX has become increasingly prevalent in clinical trials for solid tumor treatment [42,43,44,45,46,47,48,49,50]. Several examples of clinical investigations combining metronomic CPX treatment with immunotherapies are shown in Table 1. A Phase II clinical trial published by Mo and colleagues in 2024 showed superior clinical efficacy in patients with metastatic HER-2+ breast cancer treated with a dual treatment of low-dose CPX and toripalimab anti-PD-1 checkpoint blockade [42]. In a study published by Zsiros and colleagues in 2021, a Phase II clinical trial of recurrent ovarian cancer also showed that low-dose CPX and anti-PD-1 checkpoint blockade was well tolerated and 95% of patients experienced clinical benefit [43]. Interestingly, 25% of patients who participated in the trial observed a long-term treatment response of greater than 12 months, suggesting that metronomic chemotherapy and immune checkpoint blockade synergized positively in a manner that resembles the effects in preclinical studies.

Table 1.
Clinical trials of metronomic (MN) CPX and immunotherapy combinations (from 2016 to 2025).
11. Discussion
Chemotherapeutic agents such as CPX have been widely adopted in the standard of care treatment regimens for many solid and hematological malignancies. Despite their ability to directly kill cancer cells for tumor debulking, chemotherapies also often exhibit unacceptable toxicity. Given these clinical limitations, both clinicians and researchers have explored administering chemotherapies such as CPX in a metronomic dosing schedule, showing highly reduced toxicities and an objective clinical response, even in relapsed and refractory disease [55,56,57,58,59,60]. Although there are very limited human clinical data directly comparing metronomic CPX to conventional dose CPX, multiple human studies clearly show favorable toxicity and safety profiles using metronomic dosing. Studies directly comparing a metronomic or conventional dosage scheduling of CPX in preclinical models indicated that metronomic CPX was superior in reducing intratumoral Tregs in conjunction with increasing CD8+ T cell and NK cell activity [61,62,63,64,65]. Preclinical studies have also reported increased dendritic cell activation and antigen presentation through the induction of ICD post-metronomic CPX treatment, and multiple effects on the cytokine milieu and composition of the TME have also been documented in both preclinical and clinical studies of metronomic CPX [66,67,68,69]. This suggests that the use of metronomic CPX in conjunction with other immunotherapies such as immune checkpoint inhibitors could be used to achieve stable disease and objective clinical responses with substantial reductions in significant adverse events, facilitating a better quality of life during and after cancer treatment. Additional studies will be needed to completely elucidate the clinical efficacy of metronomic CPX as opposed to conventional dose CPX in the treatment of solid and hematological malignancies. Currently, there is a dearth of studies in the scientific literature that clearly delineate the circumstances and patient populations in which metronomic CPX treatment would be clinically optimal. This is compounded by the fact that the interrelated mechanisms of metronomic CPX’s effects on immune cells and tumor cells is still not fully elucidated. Further characterizing the effects of metronomic CPX in restructuring the immunopeptidome and activation of innate immune sensors of tumor cells is of considerable interest for future studies. This mechanistic insight could drive further development of tumor peptide vaccines and/or pairing of innate immune sensor agonist therapies with metronomic CPX. Additional studies will need to be conducted to stipulate clearly what dose of CPX is best suited for specific tumor and molecular subtypes on the metronomic dosing schedule, as well as to identify better therapeutic biomarkers for potential responses to metronomic CPX. Characterizing the importance of the frequency and dosage of metronomic CPX is also urgently needed to enhance the efficacy and tolerability of metronomic CPX. These novel avenues have the potential to enhance the immunogenicity of canonically cold tumor types and provide further optimized cancer treatment.
In addition to further characterizing the immunological mechanism of metronomic CPX, the usage of metronomic CPX in the context of palliative care is an emerging field of interest, particularly in geriatric and pediatric populations. While there is a paucity of research investigating the therapeutic efficacy of metronomic CPX in the context of palliative care, the limited literature on this topic has shown promise at slowing disease progression, while simultaneously increasing the quality of life during palliative care [70,71,72,73,74,75]. This approach of metronomic CPX would be highly attractive in patients who have limited ability to tolerate conventional therapeutic doses of chemotherapy due to pre-existing health conditions. Larger and more diverse tumor type clinical studies will need to be performed to elucidate these gaps in mechanism and identify optimal patient populations in both palliative and non-palliative settings.
12. Conclusions/Perspectives
In summary, the alkylating agent CPX has a well-documented set of novel immunomodulatory properties that have a strong translational application to the treatment of many solid and hematological malignancies. Moreover, the well-established direct impact of CPX on tumor cells complements the numerous effects of CPX on the TME that can serve to significantly alter the immune landscape of solid tumors that are often immunologically cold and unresponsive to immunotherapies (such as immune checkpoint blockade). This review also presents the applicability of the metronomic dosing schedule of CPX to synergize with other anti-cancer therapeutics while limiting overall toxicity and complications that are commonly seen in the canonical administration of chemotherapy agents. Further preclinical testing and human clinical studies are required to characterize the effects of CPX on the cancer TME when combined with other immunotherapies, to optimize the delivery strategies by which CPX can be administered, and to determine how it alters the immune suppressive nature of stromal cells and immune cell populations.
Author Contributions
Conceptualization, B.D.G.; investigation, B.D.G.; resources, D.W.C. and J.C.S.; writing—original draft preparation, B.D.G.; writing—review and editing, B.D.G., D.W.C. and J.C.S.; visualization, B.D.G. and J.C.S.; supervision, D.W.C. and J.C.S.; project administration, J.C.S.; funding acquisition, D.W.C. and J.C.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Pediatric Cancer Research Group, part of the Child Health Research Institute; the National Cancer Institute (NCI)-supported Cancer Biology Training Program T32 CA009476; and the Fred & Pamela Buffett Cancer Center NCI Cancer Center Support Grant P30 CA036727 and its supplements P30 CA036727-37S4 and P30 CA036727-38S3.
Acknowledgments
The figures in this review were created with BioRender.com.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ATP | adenosine triphosphate |
| CR | complete response |
| CRT | calreticulin |
| CPX | cyclophosphamide |
| DNA | deoxyribonucleic acid |
| HMGB1 | high-mobility group box protein 1 |
| ICD | immunogenic cell death |
| IFN | interferon |
| IL | interleukin |
| JAK/STAT | Janus kinase/signal transducers and activators of transcription |
| MAPK | mitogen-activated protein kinase |
| MDSC | myeloid-derived suppressor cell |
| MHC class I | major histocompatibility complex class I |
| MHC class II | major histocompatibility complex class II |
| NF-κB | nuclear factor kappa B |
| NK cell | natural killer cell |
| ORR | overall response rate |
| OS | overall survival |
| PFS | progression-free survival |
| PD-1 | programmed cell death protein 1 |
| PD-L1 | programmed death-ligand 1 |
| PI3K/Akt | phosphoinositide 3-kinase/Akt |
| TGF-β | transforming growth factor beta |
| Th1 | T helper 1 |
| TME | tumor microenvironment |
| TNF-α | tumor necrosis factor alpha |
| Treg | regulatory T cell |
| VEGF | vascular endothelial growth factor |
| VEX | treatment regimen of metronomic cyclophosphamide, vinorelbine, and capecitabine |
References
- Zhu, S.; Zhang, T.; Zheng, L.; Liu, H.; Song, W.; Liu, D.; Li, Z.; Pan, C.X. Combination strategies to maximize the benefits of cancer immunotherapy. J. Hematol. Oncol. 2021, 14, 156. [Google Scholar] [CrossRef] [PubMed]
- Ahlmann, M.; Hempel, G. The effect of cyclophosphamide on the immune system: Implications for clinical cancer therapy. Cancer Chemother. Pharmacol. 2016, 78, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Zhulai, G.; Oleinik, E. Targeting regulatory T cells in anti-PD-1/PD-L1 cancer immunotherapy. Scand. J. Immunol. 2022, 95, e13129. [Google Scholar] [CrossRef] [PubMed]
- Shan, F.; Somasundaram, A.; Bruno, T.C.; Workman, C.J.; Vignali, D.A.A. Therapeutic targeting of regulatory T cells in cancer. Trends Cancer 2022, 8, 944–961. [Google Scholar] [CrossRef]
- Buccione, C.; Fragale, A.; Polverino, F.; Ziccheddu, G.; Aricò, E.; Belardelli, F.; Proietti, E.; Battistini, A.; Moschella, F. Role of interferon regulatory factor 1 in governing Treg depletion, Th1 polarization, inflammasome activation and antitumor efficacy of cyclophosphamide. Int. J. Cancer 2018, 142, 976–987. [Google Scholar] [CrossRef]
- Leong, W.I.; Ames, R.Y.; Haverkamp, J.M.; Torres, L.; Kline, J.; Bans, A.; Rocha, L.; Gallotta, M.; Guiducci, C.; Coffman, R.L.; et al. Low-dose metronomic cyclophosphamide complements the actions of an intratumoral C-class CpG TLR9 agonist to potentiate innate immunity and drive potent T cell-mediated anti-tumor responses. Oncotarget 2019, 10, 7220–7237. [Google Scholar] [CrossRef]
- Zhong, H.; Lai, Y.; Zhang, R.; Daoud, A.; Feng, Q.; Zhou, J.; Shang, J. Low dose cyclophosphamide modulates tumor microenvironment by TGF-beta signaling pathway. Int. J. Mol. Sci. 2020, 21, 957. [Google Scholar] [CrossRef]
- Huang, X.M.; Zhang, N.R.; Lin, X.T.; Zhu, C.Y.; Zou, Y.F.; Wu, X.J.; He, X.S.; He, X.W.; Wan, Y.L.; Lan, P. Antitumor immunity of low-dose cyclophosphamide: Changes in T cells and cytokines TGF-beta and IL-10 in mice with colon-cancer liver metastasis. Gastroenterol. Rep. 2019, 8, 56–65. [Google Scholar] [CrossRef]
- Fucikova, J.; Kepp, O.; Kasikova, L.; Petroni, G.; Yamazaki, T.; Liu, P.; Zhao, L.; Spisek, R.; Kroemer, G.; Galluzzi, L. Detection of immunogenic cell death and its relevance for cancer therapy. Cell Death Dis. 2020, 11, 1013. [Google Scholar] [CrossRef]
- Jin, M.Z.; Wang, X.P. Immunogenic cell death-based cancer vaccines. Front. Immunol. 2021, 12, 697964. [Google Scholar] [CrossRef]
- Webb, E.R.; Moreno-Vicente, J.; Easton, A.; Penfold, C.; Beers, S.A.; Gray, J.C. Cyclophosphamide depletes tumor infiltrating T regulatory cells and combined with anti-PD1 therapy improves survival in murine neuroblastoma. iScience 2022, 25, 104995. [Google Scholar] [CrossRef] [PubMed]
- Dumitriu, I.E.; Baruah, P.; Valentinis, B.; Voll, R.E.; Herrmann, M.; Nawroth, P.P.; Arnold, B.; Bianchi, M.E.; Manfredi, A.A.; Rovere-Querini, P. Release of high mobility group box 1 by dendritic cells controls T cell activation via the receptor for advanced glycation end products. J. Immunol. 2005, 174, 7506–7515. [Google Scholar] [CrossRef] [PubMed]
- Van Vlerken-Ysla, L.; Tyurina, Y.Y.; Kagan, V.E.; Gabrilovich, D.I. Functional states of myeloid cells in cancer. Cancer Cell 2023, 41, 490–504. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, T.; Uchi, H.; Lesokhin, A.M.; Avogadri, F.; Rizzuto, G.; Hirschhorn-Cymerman, D.; Panageas, K.S.; Merghoub, T.; Wolchok, J.D.; Houghton, A.N. Cyclophosphamide enhances immunity by modulating the balance of dendritic cell subsets in lymphoid organs. Blood 2010, 115, 4384–4392. [Google Scholar] [CrossRef]
- Kroemer, G.; Galassi, C.; Zitvogel, L.; Galluzi, L. Immunogenic cell stress and death. Nat. Immunol. 2022, 23, 487–500. [Google Scholar] [CrossRef]
- Bryniarski, K.; Szczepanik, M.; Ptak, M.; Zemelka, M.; Ptak, W. Influence of cyclophosphamide and its metabolic products on the activity of peritoneal macrophages in mice. Pharmacol. Rep. 2009, 61, 550–557. [Google Scholar] [CrossRef]
- Zhai, J.; Gu, X.; Liu, Y.; Hu, Y.; Jiang, Y.; Zhang, Z. Chemotherapeutic and targeted drugs-induced immunogenic cell death in cancer models and antitumor therapy: An update review. Front. Pharmacol. 2023, 14, 1152934. [Google Scholar] [CrossRef]
- Radojcic, V.; Bezak, K.B.; Skarica, M.; Pletneva, M.A.; Yoshimura, K.; Schulick, R.D.; Luznik, L. Cyclophosphamide resets dendritic cell homeostasis and enhances antitumor immunity through effects that extend beyond regulatory T cell elimination. Cancer Immunol. Immunother. 2010, 59, 137–148. [Google Scholar] [CrossRef]
- Shurin, G.V.; Tourkova, I.L.; Kaneno, R.; Shurin, M.R. Chemotherapeutic agents in noncytotoxic concentrations increase antigen presentation by dendritic cells via an IL-12-dependent mechanism. J. Immunol. 2009, 183, 137–144. [Google Scholar] [CrossRef]
- Khan, K.A.; Ponce de Léon, J.L.; Benguigui, M.; Xu, P.; Chow, A.; Cruz-Munoz, W.; Man, S.; Shaked, Y.; Kerbel, R.S. Immunostimulatory and anti-tumor metronomic cyclophosphamide regimens assessed in primary orthotopic and metastatic murine breast cancer. npj Breast Cancer 2020, 6, 29. [Google Scholar] [CrossRef]
- Desterke, C.; Xiang, Y.; Elhage, R.; Duruel, C.; Chang, Y.; Hamaï, A. Ferroptosis inducers upregulate PD-L1 in recurrent triple-negative breast cancer. Cancers 2023, 16, 155. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Li, T.; Jiang, R.; Yang, X.; Guo, H.; Yang, R. Targeting MHC-I molecules for cancer: Function, mechanism, and therapeutic prospects. Mol. Cancer 2023, 22, 194. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.M.; Fowler, D.W.; Smith, P.; Dalgleish, A.G. Pre-treatment with chemotherapy can enhance the antigenicity and immunogenicity of tumours by promoting adaptive immune responses. Br. J. Cancer 2010, 102, 115–123. [Google Scholar] [CrossRef]
- Peng, J.; Hamanishi, J.; Matsumura, N.; Abiko, K.; Murat, K.; Baba, T.; Yamaguchi, K.; Horikawa, N.; Hosoe, Y.; Murphy, S.K.; et al. Chemotherapy induces programmed cell death-ligand 1 overexpression via the nuclear factor-κB to foster an immunosuppressive tumor microenvironment in ovarian cancer. Cancer Res. 2015, 75, 5034–5045. [Google Scholar] [CrossRef]
- Yu, R.; Zhu, B.; Chen, D. Type I interferon-mediated tumor immunity and its role in immunotherapy. Cell. Mol. Life Sci. 2022, 79, 191. [Google Scholar] [CrossRef]
- Meyer, S.P.; Bauer, R.; Brüne, B.; Schmid, T. The role of type I interferon signaling in myeloid anti-tumor immunity. Front. Immunol. 2025, 16, 1547466. [Google Scholar] [CrossRef]
- Zannikou, M.; Fish, E.N.; Platanias, L.C. Signaling by Type I interferons in immune cells: Disease consequences. Cancers 2024, 16, 1600. [Google Scholar] [CrossRef]
- Swann, J.B.; Hayakawa, Y.; Zerafa, N.; Sheehan, K.C.F.; Scott, B.; Schreiber, R.D.; Hertzog, P.; Smyth, M.J. Type I IFN contributes to NK cell homeostasis, activation, and antitumor function. J. Immunol. 2007, 178, 7540–7549. [Google Scholar] [CrossRef]
- Cauwels, A.; Van Lint, S.; Paul, F.; Garcin, G.; De Koker, S.; Van Parys, A.; Wueest, T.; Gerlo, S.; Van der Heyden, J.; Bordat, Y.; et al. Delivering Type I interferon to dendritic cells empowers tumor eradication and immune combination treatments. Cancer Res. 2018, 78, 463–474. [Google Scholar] [CrossRef]
- Del Prete, A.; Salvi, V.; Soriani, A.; Laffranchi, M.; Sozio, F.; Bosisio, D.; Sozzani, S. Dendritic cell subsets in cancer immunity and tumor antigen sensing. Cell. Mol. Immunol. 2023, 20, 432–447. [Google Scholar] [CrossRef]
- Montoya, M.; Schiavoni, G.; Mattei, F.; Gresser, I.; Belardelli, F.; Borrow, P.; Tough, D.F. Type I interferons produced by dendritic cells promote their phenotypic and functional activation. Blood 2002, 99, 3263–3271. [Google Scholar] [CrossRef]
- Luft, T.; Pang, K.C.; Thomas, E.; Hertzog, P.; Hart, D.N.; Trapani, J.; Cebon, J. Type I IFNs enhance the terminal differentiation of dendritic cells. J. Immunol. 1998, 161, 1947–1953. [Google Scholar] [CrossRef]
- Schiavoni, G.; Sistigu, A.; Valentini, M.; Mattei, F.; Sestili, P.; Spadaro, F.; Sanchez, M.; Lorenzi, S.; D’Urso, M.T.; Belardelli, F.; et al. Cyclophosphamide synergizes with type I interferons through systemic dendritic cell reactivation and induction of immunogenic tumor apoptosis. Cancer Res. 2011, 71, 768–778. [Google Scholar] [CrossRef]
- Du, B.; Waxman, D.J. Medium dose intermittent cyclophosphamide induces immunogenic cell death and cancer cell autonomous type I interferon production in glioma models. Cancer Lett. 2020, 470, 170–180. [Google Scholar] [CrossRef]
- Malvicini, M.; Rizzo, M.; Alaniz, L.; Piñero, F.; García, M.; Atorrasagasti, C.; Aquino, J.B.; Rozados, V.; Scharovsky, O.G.; Matar, P.; et al. A novel synergistic combination of cyclophosphamide and gene transfer of interleukin-12 eradicates colorectal carcinoma in mice. Clin. Cancer Res. 2009, 15, 7256–7265. [Google Scholar] [CrossRef]
- Matar, P.; Rozados, V.R.; Gervasoni, S.I.; Scharovsky, G.O. Th2/Th1 switch induced by a single low dose of cyclophosphamide in a rat metastatic lymphoma model. Cancer Immunol. Immunother. 2002, 50, 588–596. [Google Scholar] [CrossRef]
- Gottdiener, J.S.; Appelbaum, F.R.; Ferrans, V.J.; Deisseroth, A.; Ziegler, J. Cardiotoxicity associated with high-dose cyclophosphamide therapy. Arch. Int. Med. 1981, 141, 758–763. [Google Scholar] [CrossRef]
- Campagne, O.; Zhong, B.; Nair, S.; Lin, T.; Huang, J.; Onar-Thomas, A.; Robinson, G.; Gajjar, A.; Stewart, C.F. Exposure-toxicity association of cyclophosphamide and its metabolites in infants and young children with primary brain tumors: Implications for dosing. Clin. Cancer Res. 2020, 26, 1563–1573. [Google Scholar] [CrossRef]
- Simsek, C.; Esin, E.; Yalcin, S. Metronomic chemotherapy: A systematic review of the literature and clinical experience. J. Oncol. 2019, 2019, 543791. [Google Scholar] [CrossRef]
- Cazzaniga, M.E.; Cordani, N.; Capici, S.; Cogliati, V.; Riva, F.; Cerrito, M.G. Metronomic chemotherapy. Cancers 2021, 13, 2236. [Google Scholar] [CrossRef]
- Peyrl, A.; Chocholous, M.; Sabel, M.; Lassaletta, A.; Sterba, J.; Leblond, P.; Nysom, K.; Torsvik, I.; Chi, S.N.; Perwein, T.; et al. Sustained survival benefit in recurrent medulloblastoma by a metronomic antiangiogenic regimen: A nonrandomized controlled trial. JAMA Oncol. 2023, 9, 1688–1695. [Google Scholar] [CrossRef]
- Mo, H.; Yu, Y.; Sun, X.; Ge, H.; Yu, L.; Guan, X.; Zhai, J.; Zhu, A.; Wei, Y.; Wang, J.; et al. Metronomic chemotherapy plus anti-PD-1 in metastatic breast cancer: A Bayesian adaptive randomized phase 2 trial. Nat. Med. 2024, 30, 2528–2539. [Google Scholar] [CrossRef]
- Zsiros, E.; Lynam, S.; Attwood, K.M.; Wang, C.; Chilakapati, S.; Gomez, E.C.; Liu, S.; Akers, S.; Lele, S.; Frederick, P.J.; et al. Efficacy and safety of pembrolizumab in combination with bevacizumab and oral metronomic cyclophosphamide in the treatment of recurrent ovarian cancer: A Phase 2 nonrandomized clinical trial. JAMA Oncol. 2021, 7, 78–85. [Google Scholar] [CrossRef]
- Muraro, E.; Vinante, L.; Fratta, E.; Bearz, A.; Höfler, D.; Steffan, A.; Baboci, L. Metronomic chemotherapy: Anti-tumor pathways and combination with immune checkpoint inhibitors. Cancers 2023, 15, 2471. [Google Scholar] [CrossRef]
- Noguchi, M.; Moriya, F.; Koga, N.; Matsueda, S.; Sasada, T.; Yamada, A.; Kakuma, T.; Itoh, K. A randomized phase II clinical trial of personalized peptide vaccination with metronomic low-dose cyclophosphamide in patients with metastatic castration-resistant prostate cancer. Cancer Immunol. Immunother. 2016, 65, 151–160. [Google Scholar] [CrossRef]
- Borch, T.H.; Engell-Noerregaard, L.; Zeeberg Iversen, T.; Ellebaek, E.; Met, Ö.; Hansen, M.; Andersen, M.H.; Thor Straten, P.; Svane, I.M. mRNA-transfected dendritic cell vaccine in combination with metronomic cyclophosphamide as treatment for patients with advanced malignant melanoma. Oncoimmunology 2016, 5, e1207842. [Google Scholar] [CrossRef]
- Pasqualini, C.; Rubino, J.; Brard, C.; Cassard, L.; André, N.; Rondof, W.; Scoazec, J.Y.; Marchais, A.; Nebchi, S.; Boselli, L.; et al. Phase II and biomarker study of programmed cell death protein 1 inhibitor nivolumab and metronomic cyclophosphamide in paediatric relapsed/refractory solid tumours: Arm G of AcSé-ESMART, a trial of the European Innovative Therapies for Children With Cancer Consortium. Eur. J. Cancer 2021, 150, 53–62. [Google Scholar] [CrossRef]
- André, N.; Le Deley, M.C.; Léguillette, C.; Probst, A.; Willems, L.; Travers, R.; Aerts, I.; Faure-Conter, C.; Revond-Riviere, G.; Min, V.; et al. METRO-PD1: Phase 1 study of nivolumab in combination with metronomic chemotherapy in children and adolescents with relapsing/refractory solid tumors. Eur. J. Cancer 2024, 198, 113525. [Google Scholar] [CrossRef]
- Merlano, M.C.; Merlotti, A.M.; Licitra, L.; Denaro, N.; Fea, E.; Galizia, D.; Di Maio, M.; Fruttero, C.; Curcio, P.; Vecchio, S.; et al. Activation of immune responses in patients with relapsed-metastatic head and neck cancer (CONFRONT phase I-II trial): Multimodality immunotherapy with avelumab, short-course radiotherapy, and cyclophosphamide. Clin. Transl. Radiat. Oncol. 2018, 12, 47–52. [Google Scholar] [CrossRef]
- Toulmonde, M.; Cousin, S.; Kind, M.; Guegan, J.P.; Bessede, A.; Le Loarer, F.; Perret, R.; Cantarel, C.; Bellera, C.; Italiano, A. Randomized phase 2 trial of intravenous oncolytic virus JX-594 combined with low-dose cyclophosphamide in patients with advanced soft-tissue sarcoma. J. Hematol. Oncol. 2022, 15, 149. [Google Scholar] [CrossRef]
- Wu, J.; Waxman, D.J. Immunogenic chemotherapy: Dose and schedule dependence and combination with immunotherapy. Cancer Lett. 2018, 419, 210–221. [Google Scholar] [CrossRef]
- Weir, G.; Hrytsenko, O.; Stanford, M.; Berinstein, N.; Liwski, R.; Karkada, M.; Mansour, M. Multi-modal treatment with peptide vaccine, metronomic cyclophosphamide and anti-PD1 monoclonal antibody provides effective control of tumors in multiple models. J. Immunother. Cancer 2014, 2 (Suppl. 3), P130. [Google Scholar] [CrossRef]
- Park, Y.S.; Bae, J.H.; Son, C.H.; Lee, K.S.; Kim, W.; Jung, M.H.; Yang, K.; Kim, S.H.; Kang, C.D. Cyclophosphamide potentiates the antitumor effect of immunization with injection of immature dendritic cells into irradiated tumor. Immunol. Investig. 2011, 40, 383–399. [Google Scholar] [CrossRef]
- Pfirschke, C.; Engblom, C.; Rickelt, S.; Cortez-Retamozo, V.; Garris, C.; Pucci, F.; Yamazaki, T.; Poirier-Colame, V.; Newton, A.; Redouane, Y.; et al. Immunogenic chemotherapy sensitizes tumors to checkpoint blockade therapy. Immunity 2016, 44, 343–354. [Google Scholar] [CrossRef]
- Spiliopoulou, P.; Hinsley, S.; McNeish, I.A.; Roxburgh, P.; Glasspool, R. Metronomic oral cyclophosphamide in relapsed ovarian cancer. Int. J. Gynecol. Cancer 2021, 31, 1037–1044. [Google Scholar] [CrossRef]
- Le, D.T.; Jaffee, E.M. Regulatory T-cell modulation using cyclophosphamide in vaccine approaches: A current perspective. Cancer Res. 2012, 72, 3439–3444. [Google Scholar] [CrossRef]
- Delahousse, J.; Molina, L.; Paci, A. Cyclophosphamide and analogues; a matter of dose and schedule for dual anticancer activities. Cancer Lett. 2024, 598, 217119. [Google Scholar] [CrossRef]
- Peres, T.; Aeppli, S.; Fischer, S.; Gysel, K.; Rothermundt, C. Metronomic cyclophosphamide for bone marrow carcinomatosis in metastatic castration-resistant prostate cancer. J. Cancer Res. Clin. Oncol. 2024, 150, 84. [Google Scholar] [CrossRef]
- de Boo, L.W.; Vulink, A.J.E.; Bos, M.E.M.M. Metronomic cyclophosphamide-induced long-term remission after recurrent high-grade serous ovarian cancer: A case study. Mol. Clin. Oncol. 2017, 7, 1130–1134. [Google Scholar] [CrossRef][Green Version]
- Peristeri, D.V.; Tepelenis, K.; Karampa, A.; Kapodistrias, N.; Goussia, A.C.; Pappas-Gogos, G.; Glantzounis, G.K. Metronomic chemotherapy with cyclophosphamide for the treatment of advanced hepatocellular cancer: A case report. Ann. Med. Surg. 2021, 72, 103043. [Google Scholar] [CrossRef]
- Tomar, M.S.; Singh, R.K.; Ulasov, I.V.; Kaushalendra; Acharya, A. Refurbishment of NK cell effector functions through their receptors by depleting the activity of nTreg cells in Dalton’s Lymphoma-induced tumor microenvironment: An in vitro and in vivo study. Cancer Immunol. Immunother. 2023, 72, 1429–1444. [Google Scholar] [CrossRef]
- Noordam, L.; Kaijen, M.E.H.; Bezemer, K.; Cornelissen, R.; Maat, L.A.P.W.M.; Hoogsteden, H.C.; Aerts, J.G.J.V.; Hendriks, R.W.; Hegmans, J.P.J.J.; Vroman, H. Low-dose cyclophosphamide depletes circulating naïve and activated regulatory T cells in malignant pleural mesothelioma patients synergistically treated with dendritic cell-based immunotherapy. Oncoimmunology 2018, 7, e1474318. [Google Scholar] [CrossRef]
- Berinstein, N.L.; Karkada, M.; Oza, A.M.; Odunsi, K.; Villella, J.A.; Nemunaitis, J.J.; Morse, M.A.; Pejovic, T.; Bentley, J.; Buyse, M.; et al. Survivin-targeted immunotherapy drives robust polyfunctional T cell generation and differentiation in advanced ovarian cancer patients. Oncoimmunology 2015, 4, e1026529. [Google Scholar] [CrossRef]
- Huijts, C.M.; Lougheed, S.M.; Bodalal, Z.; van Herpen, C.M.; Hamberg, P.; Tascilar, M.; Haanen, J.B.; Verheul, H.M.; de Gruijl, T.D.; van der Vliet, H.J.; et al. The effect of everolimus and low-dose cyclophosphamide on immune cell subsets in patients with metastatic renal cell carcinoma: Results from a phase I clinical trial. Cancer Immun. Immunother. 2019, 68, 503–515. [Google Scholar] [CrossRef]
- Doloff, J.C.; Waxman, D.J. VEGF receptor inhibitors block the ability of metronomically dosed cyclophosphamide to activate innate immunity-induced tumor regression. Cancer Res. 2012, 72, 1103–1115. [Google Scholar] [CrossRef]
- Merlano, M.C.; Abbona, A.; Paccagnella, M.; Falletta, A.; Granetto, C.; Ricci, V.; Fea, E.; Denaro, N.; Ruatta, F.; Merlotti, A.; et al. Cytokine profiling of end stage cancer patients treated with immunotherapy. Vaccines 2021, 9, 235. [Google Scholar] [CrossRef]
- Rozados, V.R.; Mainetti, L.E.; Rico, M.J.; Zacarías Fluck, M.F.; Matar, P.; Scharovsky, O.G. The immune response and the therapeutic effect of metronomic chemotherapy with cyclophosphamide. Oncol. Res. 2010, 18, 601–605. [Google Scholar] [CrossRef]
- Chen, C.S.; Doloff, J.C.; Waxman, D.J. Intermittent metronomic drug schedule is essential for activating antitumor innate immunity and tumor xenograft regression. Neoplasia 2014, 16, 84–96. [Google Scholar] [CrossRef]
- Son, C.H.; Shin, D.Y.; Kim, S.D.; Park, H.S.; Jung, M.H.; Bae, J.H.; Kang, C.D.; Yang, K.; Park, Y.S. Improvement of antitumor effect of intratumoral injection of immature dendritic cells into irradiated tumor by cyclophosphamide in mouse colon cancer model. J. Immunother. 2012, 35, 607–614. [Google Scholar] [CrossRef]
- Revannasiddaiah, S.; Joshi, S.C.; Pandey, K.C.; Rastogi, M.; Sharma, M.; Gupta, M. The results with the addition of metronomic cyclophosphamide to palliative radiotherapy for the treatment of non-small cell lung carcinoma. Ann. Transl. Med. 2015, 3, 305. [Google Scholar] [CrossRef]
- Devi, R.N.; Menon, A.; Shenoy, P.K.; Avaronnan, M.; Shahana, S.; George, A. Oral metronomic therapy: An effective palliative treatment option for epithelial ovarian cancer. Cureus 2024, 16, e73171. [Google Scholar] [CrossRef] [PubMed]
- Gebbia, V.; Boussen, H.; Valerio, M.R. Oral metronomic cyclophosphamide with and without methotrexate as palliative treatment for patients with metastatic breast carcinoma. Anticancer Res. 2012, 32, 529–536. [Google Scholar] [PubMed]
- Ladoire, S.; Eymard, J.C.; Zanetta, S.; Mignot, G.; Martin, E.; Kermarrec, I.; Mourey, E.; Michel, F.; Cormier, L.; Ghiringhelli, F. Metronomic oral cyclophosphamide prednisolone chemotherapy is an effective treatment for metastatic hormone-refractory prostate cancer after docetaxel failure. Anticancer Res. 2010, 30, 4317–4323. [Google Scholar] [PubMed]
- Vogt, T.; Hafner, C.; Bross, K.; Bataille, F.; Jauch, K.W.; Berand, A.; Landthaler, M.; Andreesen, R.; Reichle, A. Antiangiogenetic therapy with pioglitazone, rofecoxib, and metronomic trofosfamide in patients with advanced malignant vascular tumors. Cancer 2003, 98, 2251–2256. [Google Scholar] [CrossRef]
- Revannasiddaiah, S.; Madabhavi, I.; Bodh, A.; Thakur, P.; Sharma, M. Metronomic chemotherapy in anaplastic thyroid carcinoma: A potentially feasible alternative to therapeutic nihilism. Indian J. Palliat. Care 2015, 21, 245–249. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).