
High PD-L1 Expression in HRS Cells and Macrophages in Tumor Immune Microenvironment Is Associated with Adverse Outcome and EBV Positivity in Classical Hodgkin Lymphoma

 , ,
, ,
Abstract
1. Introduction
2. Results
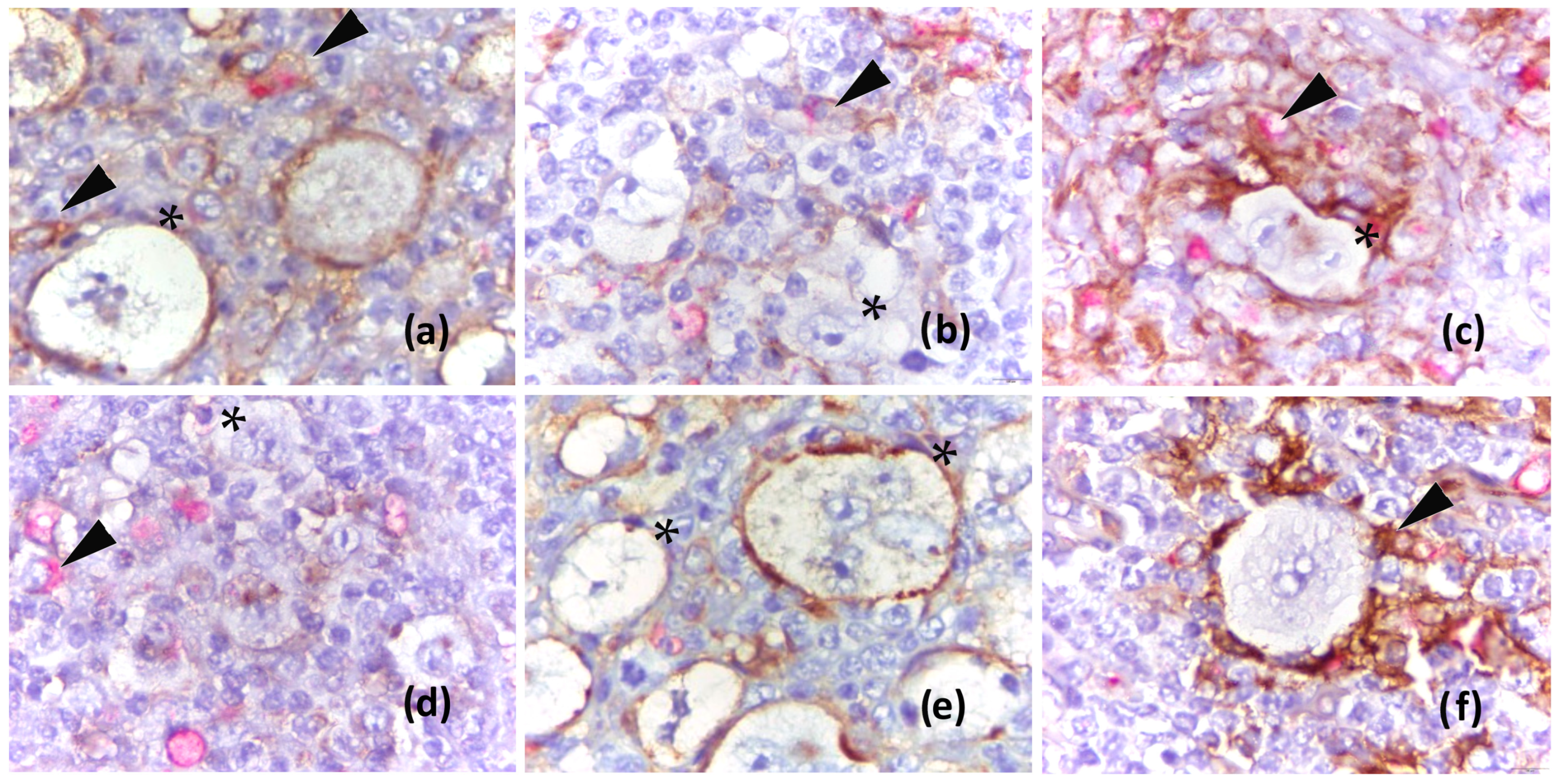
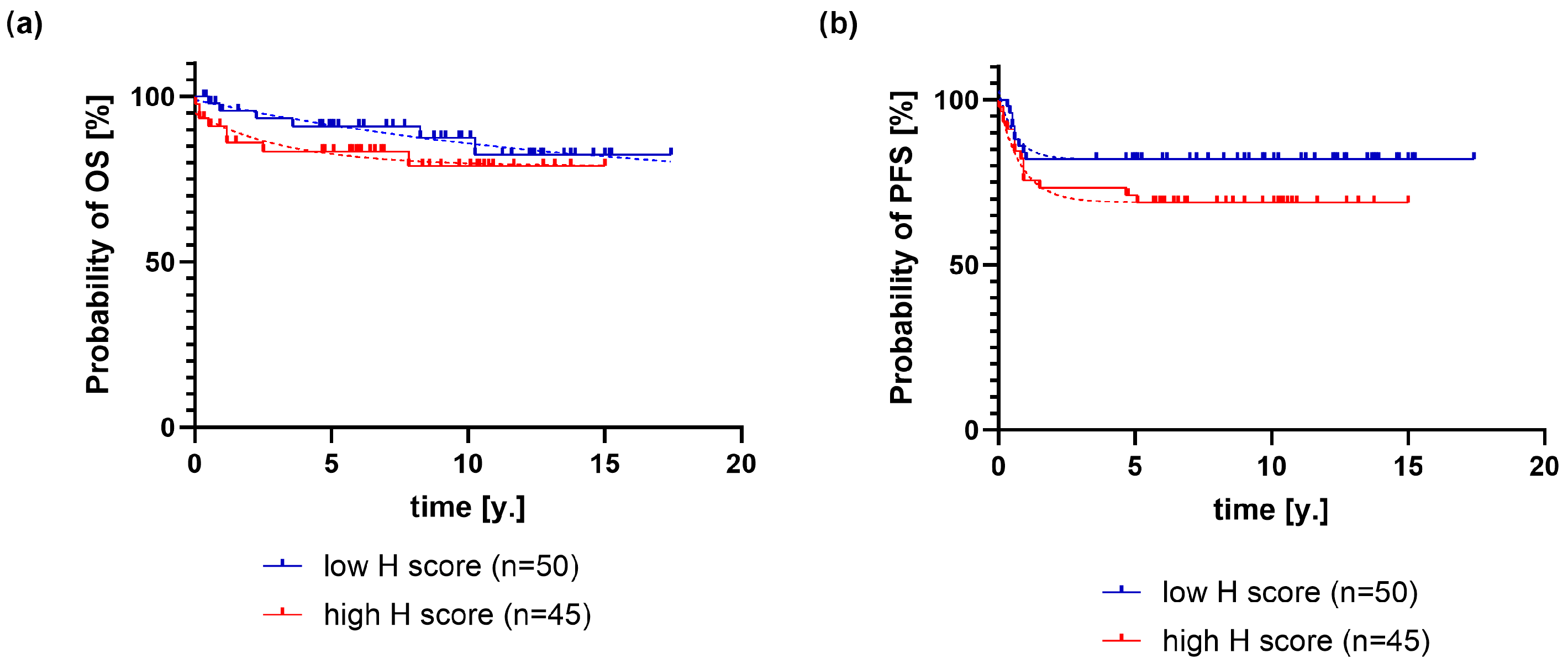
2.1. Association of PD-L1 Expression on HRS Cells with Clinical and Pathological Variables and Outcome of Classical Hodgkin Lymphoma
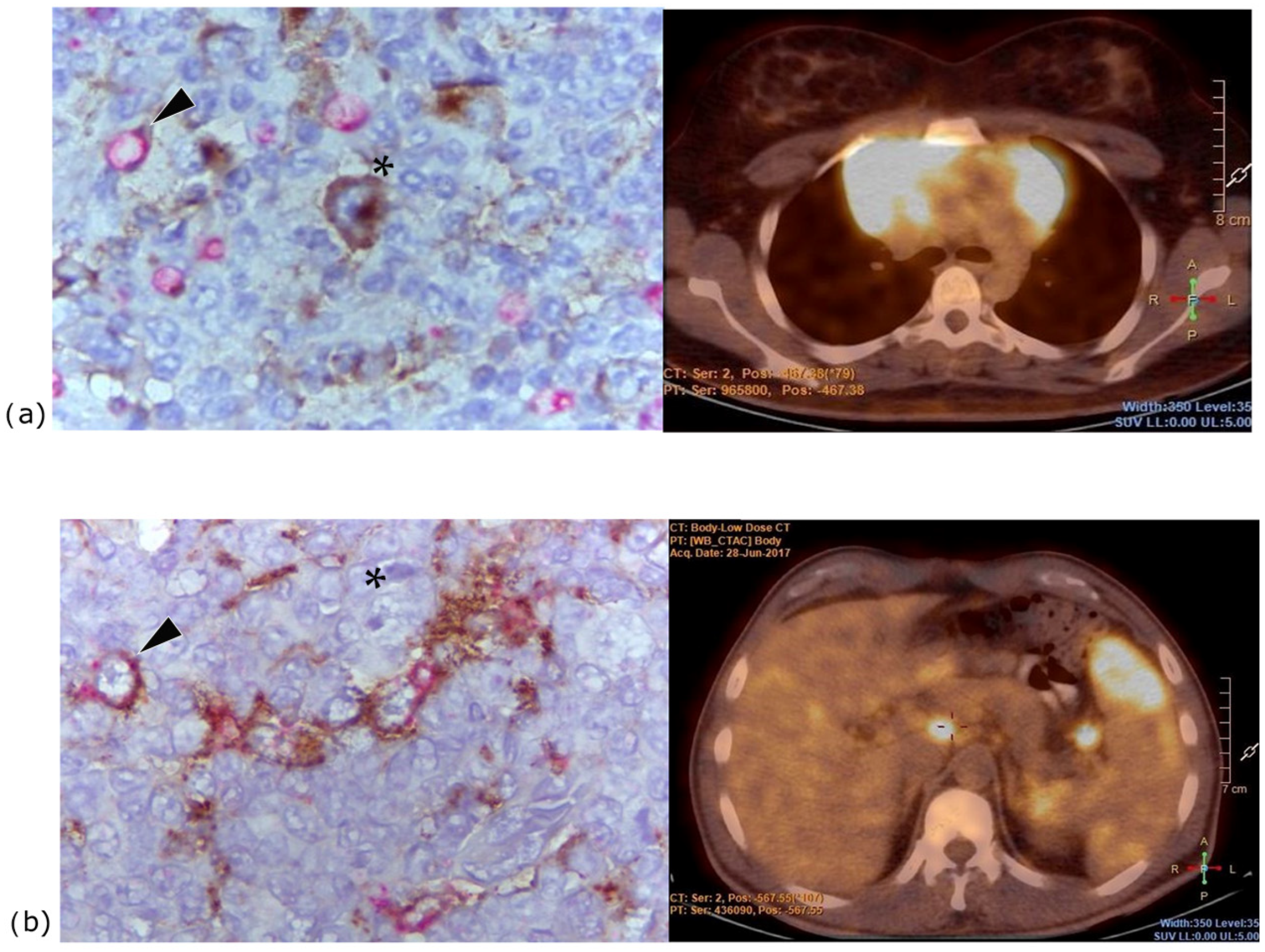
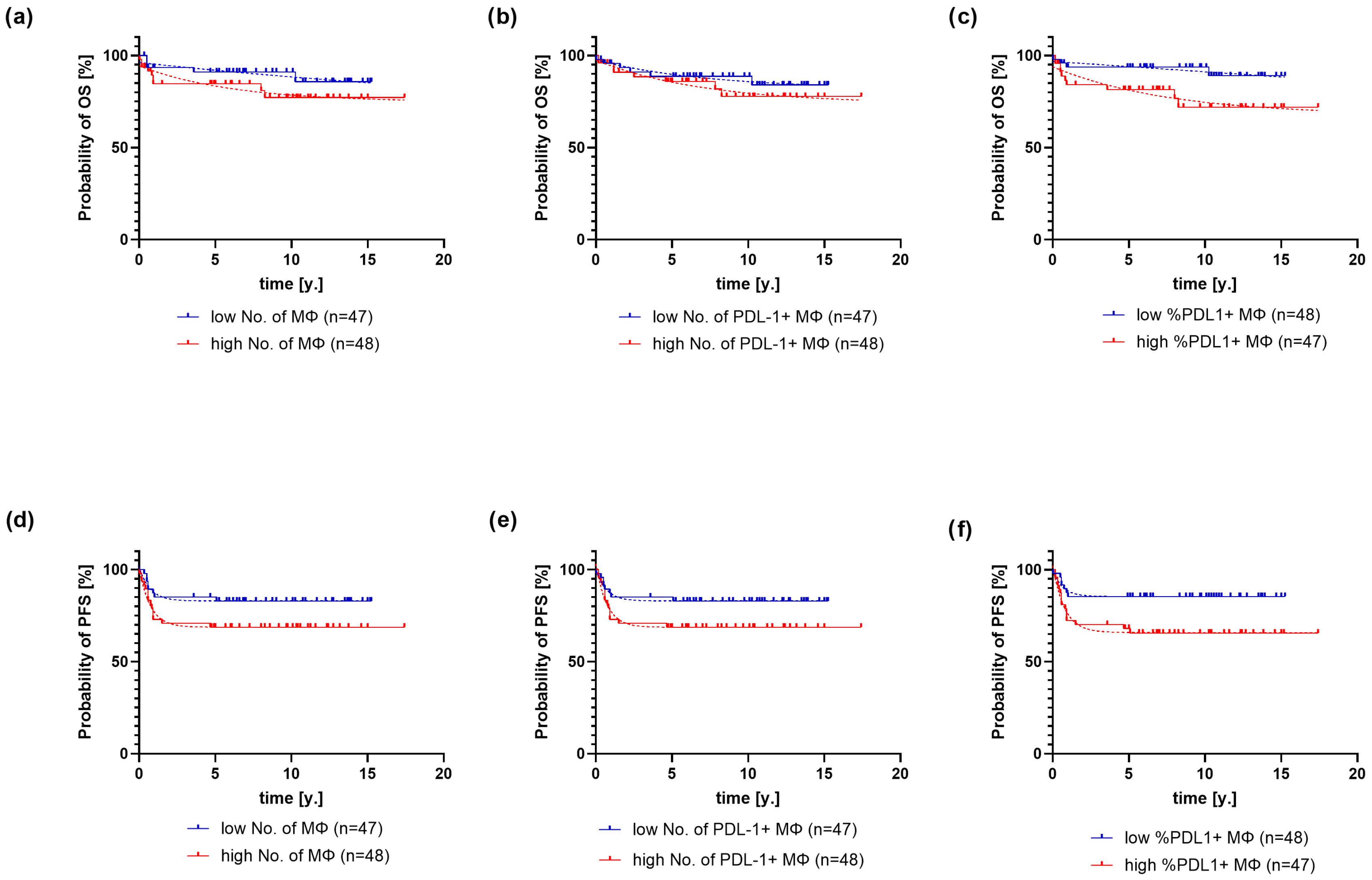
2.2. Association of PD-L1 Expression on Macrophages with Clinical and Pathological Variables and Outcome of Classical Hodgkin Lymphoma
3. Discussion
4. Materials and Methods
4.1. Patient Characteristics
4.2. Methods
4.2.1. Analysis of PD-L1 in HRS Cells
4.2.2. Analysis of PD-L1 in Macrophages
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PD-L1 | Programmed Death-Ligand 1 |
| HRS | Hodgkin and Reed–Sternberg |
| cHL | Classical Hodgkin Lymphoma |
| TME | Tumor Immune Microenvironment |
| OS | Overall Survival |
| PFS | Progression-Free Survival |
| EBV | Epstein–Barr Virus |
| H-score | Histologic Score |
| CR | Complete Remission |
| IFN-γ | Interferon Gamma |
| PD-1 | Programmed Cell Death 1 |
| ICIs | Checkpoint Inhibitors |
| R/R | Relapsed/Refractory |
| IQR | Interquartile Range |
| MΦ | Macrophages |
| EBER | Epstein–Barr Virus-Encoded RNA |
| CI | Confidence Interval |
| ANOVA | Analysis of Variance |
| PET-CT | Positron Emission Tomography–Computed Tomography |
| ER | Evidence Ratio |
| CROHEM | Croatian Cooperative Group for Hematologic Diseases |
| NCCN | National Comprehensive Cancer Network |
| ABVD | Chemotherapy protocol: Doxorubicin, Bleomycin, Vinblastine, and Dacarbazine |
| BEACOPP | Bleomycin, Etoposide, Doxorubicin, Cyclophosphamide, Vincristine, Procarbazine, and Prednisone |
| OEPA | Vincristine, Etoposide, Prednisone, and doxorubicin |
| DHAP | Cisplatin, Cytarabine, and Dexamethasone |
| ICE | Ifosfamide, Carboplatin, and Etoposide |
| ISH | In Situ Hybridization |
| DAB | 3,3’-diaminobenzidine |
| IHC | Immunohistochemistry |
References
- Press, O.W.; Li, H.; Schöder, H.; Straus, D.J.; Moskowitz, C.H.; LeBlanc, M.; Rimsza, L.M.; Bartlett, N.L.; Evens, A.M.; Mittra, E.S.; et al. US Intergroup Trial of Response-Adapted Therapy for Stage III to IV Hodgkin Lymphoma Using Early Interim Fluorodeoxyglucose-Positron Emission Tomography Imaging: Southwest Oncology Group S0816. J. Clin. Oncol. 2016, 34, 2020–2027. [Google Scholar] [CrossRef] [PubMed]
- Epperla, N.; Herrera, A.F. How I Incorporate Novel Agents into the Treatment of Classical Hodgkin Lymphoma. Blood 2021, 138, 520–530. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-J.; Jang, B.-C.; Lee, S.-W.; Yang, Y.-I.; Suh, S.-I.; Park, Y.-M.; Oh, S.; Shin, J.-G.; Yao, S.; Chen, L.; et al. Interferon Regulatory Factor-1 Is Prerequisite to the Constitutive Expression and IFN-γ-Induced Upregulation of B7-H1 (CD274). FEBS Lett. 2006, 580, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Abiko, K.; Matsumura, N.; Hamanishi, J.; Horikawa, N.; Murakami, R.; Yamaguchi, K.; Yoshioka, Y.; Baba, T.; Konishi, I.; Mandai, M. IFN-γ from Lymphocytes Induces PD-L1 Expression and Promotes Progression of Ovarian Cancer. Br. J. Cancer 2015, 112, 1501–1509. [Google Scholar] [CrossRef]
- Green, M.R.; Monti, S.; Rodig, S.J.; Juszczynski, P.; Currie, T.; O’Donnell, E.; Chapuy, B.; Takeyama, K.; Neuberg, D.; Golub, T.R.; et al. Integrative Analysis Reveals Selective 9p24.1 Amplification, Increased PD-1 Ligand Expression, and Further Induction via JAK2 in Nodular Sclerosing Hodgkin Lymphoma and Primary Mediastinal Large B-Cell Lymphoma. Blood 2010, 116, 3268–3277. [Google Scholar] [CrossRef]
- Ansell, S.M.; Bröckelmann, P.J.; von Keudell, G.; Lee, H.J.; Santoro, A.; Zinzani, P.L.; Collins, G.P.; Cohen, J.B.; de Boer, J.P.; Kuruvilla, J. Nivolumab for Relapsed/Refractory Classical Hodgkin Lymphoma: 5-Year Survival from the Pivotal Phase 2 CheckMate 205 Study. Blood Adv. 2023, 7, 6266–6274. [Google Scholar] [CrossRef]
- Younes, A.; Santoro, A.; Shipp, M.; Zinzani, P.L.; Timmerman, J.M.; Ansell, S.; Armand, P.; Fanale, M.; Ratanatharathorn, V.; Kuruvilla, J. Nivolumab for Classical Hodgkin’s Lymphoma after Failure of Both Autologous Stem-Cell Transplantation and Brentuximab Vedotin: A Multi-Centre, Multicohort, Single-Arm Phase 2 Trial. Lancet Oncol. 2016, 17, 1283–1294. [Google Scholar] [CrossRef]
- Chen, R.; Zinzani, P.L.; Lee, H.J.; Armand, P.; Johnson, N.A.; Brice, P.; Radford, J.; Ribrag, V.; Molin, D.; Vassilakopoulos, T.P.; et al. Pembrolizumab in Relapsed or Refractory Hodgkin Lymphoma: 2-Year Follow-Up of KEYNOTE-087. Blood 2019, 134, 1144–1153. [Google Scholar] [CrossRef]
- De Re, V.; Caggiari, L.; Repetto, O.; Mussolin, L.; Mascarin, M. Classical Hodgkin’s Lymphoma in the Era of Immune Checkpoint Inhibition. J. Clin. Med. 2019, 8, 1596. [Google Scholar] [CrossRef]
- Pavlović, A.; Miljak, A.; Brzica, K.; Glavina Durdov, M. The Abundance of FOXP3, FOXP3/CD4 and CD8 Cells in the Microenvironment of Nodular Sclerosis and Mixed Cellularity Subtypes Is Associated with the Epstein–Barr Virus Status of Classic Hodgkin Lymphoma. Biomedicines 2024, 12, 1680. [Google Scholar] [CrossRef]
- Paydas, S.; Bağır, E.; Seydaoglu, G.; Ercolak, V.; Ergin, M. Programmed Death-1 (PD-1), Programmed Death-Ligand 1 (PD-L1), and EBV-Encoded RNA (EBER) Expression in Hodgkin Lymphoma. Ann. Hematol. 2015, 94, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Antel, K.; Chetty, D.; Oosthuizen, J.; Mohamed, Z.; Van der Vyver, L.; Verburgh, E. CD68-Positive Tumour Associated Macrophages, PD-L1 Expression, and EBV Latent Infection in a High HIV-Prevalent South African Cohort of Hodgkin Lymphoma Patients. Pathology 2021, 53, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, O.; Colli, S.; Garcia Lombardi, M.; Preciado, M.V.; De Matteo, E.; Chabay, P. Epstein–Barr Virus Recruits PDL1-Positive Cells at the Microenvironment in Pediatric Hodgkin Lymphoma. Cancer Immunol. Immunother. 2021, 70, 1519–1526. [Google Scholar] [CrossRef]
- Hollander, P.; Kamper, P.; Smedby, K.E.; Enblad, G.; Ludvigsen, M.; Mortensen, J.; Amini, R.M.; Hamilton-Dutoit, S.; d’Amore, F.; Molin, D.; et al. High Proportions of PD-1+ and PD-L1+ Leukocytes in Classical Hodgkin Lymphoma Microenvironment Are Associated with Inferior Outcome. Blood Adv. 2017, 1, 1427–1439. [Google Scholar] [CrossRef] [PubMed]
- Roemer, M.G.M.; Advani, R.H.; Ligon, A.H.; Natkunam, Y.; Redd, R.A.; Homer, H.; Connelly, C.F.; Sun, H.H.; Daadi, S.E.; Freeman, G.J.; et al. PD-L1 and PD-L2 Genetic Alterations Define Classical Hodgkin Lymphoma and Predict Outcome. J. Clin. Oncol. 2016, 34, 2690–2697. [Google Scholar] [CrossRef]
- Koh, Y.W.; Jeon, Y.K.; Yoon, D.H.; Suh, C.; Huh, J. Programmed Death 1 Expression in the Peritumoral Microenvironment Is Associated with a Poorer Prognosis in Classical Hodgkin Lymphoma. Tumour Biol. 2016, 37, 7507–7514. [Google Scholar] [CrossRef]
- Steidl, C.; Lee, T.; Shah, S.P.; Farinha, P.; Han, G.; Nayar, T.; Delaney, A.; Jones, S.J.; Iqbal, J.; Weisenburger, D.D.; et al. Tumor-Associated Macrophages and Survival in Classic Hodgkin’s Lymphoma. N. Engl. J. Med. 2010, 362, 875–885. [Google Scholar] [CrossRef]
- Guo, B.; Cen, H.; Tan, X.; Ke, Q. Meta-Analysis of the Prognostic and Clinical Value of Tumor-Associated Macrophages in Adult Classical Hodgkin Lymphoma. BMC Med. 2016, 14, 159. [Google Scholar] [CrossRef]
- Karihtala, K.; Leivonen, S.-K.; Brück, O.; Karjalainen-Lindsberg, M.-L.; Mustjoki, S.; Pellinen, T.; Leppä, S. Prognostic Impact of Tumor-Associated Macrophages on Survival Is Checkpoint Dependent in Classical Hodgkin Lymphoma. Cancers 2020, 12, 877. [Google Scholar] [CrossRef]
- Carey, C.D.; Gusenleitner, D.; Lipschitz, M.; Roemer, M.G.M.; Stack, E.C.; Gjini, E.; Hu, X.; Redd, R.; Freeman, G.J.; Neuberg, D.; et al. Topological Analysis Reveals a PD-L1-Associated Microenvironmental Niche for Reed-Sternberg Cells in Hodgkin Lymphoma. Blood 2017, 130, 2420–2430. [Google Scholar] [CrossRef]
- Kawashima, M.; Carreras, J.; Higuchi, H.; Kotaki, R.; Hoshina, T.; Okuyama, K.; Suzuki, N.; Kakizaki, M.; Miyatake, Y.; Ando, K.; et al. PD-L1/L2 Protein Levels Rapidly Increase in Monocytes via Trogocytosis from Tumor Cells in Classical Hodgkin Lymphoma. Leukemia 2020, 34, 2405–2417. [Google Scholar] [CrossRef] [PubMed]
- Bettadapur, A.; Miller, H.W.; Ralston, K.S. Biting Off What Can Be Chewed: Trogocytosis in Health, Infection, and Disease. Infect. Immun. 2020, 88, e00930-19. [Google Scholar] [CrossRef]
- Zeng, Q.; Schwarz, H. The Role of Trogocytosis in Immune Surveillance of Hodgkin Lymphoma. OncoImmunology 2020, 9, 1781334. [Google Scholar] [CrossRef] [PubMed]
- Stewart, B.J.; Fergie, M.; Young, M.D.; Jones, C.; Sachdeva, A.; Blain, A.; Bacon, C.M.; Rand, V.; Ferdinand, J.R.; James, K.R.; et al. Spatial and Molecular Profiling of the Mononuclear Phagocyte Network in Classic Hodgkin Lymphoma. Blood 2023, 141, 2343–2358. [Google Scholar] [CrossRef]
- Jarrett, A.F.; Armstrong, A.A.; Alexander, E. Epidemiology of EBV and Hodgkin’s Lymphoma. Ann. Oncol. 1996, 7 (Suppl. S4), S5–S10. [Google Scholar] [CrossRef]
- Moyano, A.; Ferressini, N.; De Matteo, E.; Preciado, M.V.; Chabay, P. PD-L1 Is Upregulated in CD163+ Tonsillar Macrophages from Children Undergoing EBV Primary Infection. Front. Immunol. 2022, 13, 940910. [Google Scholar] [CrossRef]
- Yu, J.; Jin, S.; Yin, X.; Du, H. Expression of the Immune Checkpoint Molecules PDL1 and PD1 in EBV Associated Lymphoproliferative Disorders: A Meta-Analysis. Exp. Ther. Med. 2023, 7, 12294. [Google Scholar] [CrossRef]
- Green, M.R.; Rodig, S.; Juszczynski, P.; Ouyang, J.; Sinha, P.; O’Donnell, E.; Neuberg, D.; Shipp, M.A. Constitutive AP-1 Activity and EBV Infection Induce PD-L1 in Hodgkin Lymphomas and Post-Transplant Lymphoproliferative Disorders: Implications for Targeted Therapy. Clin. Cancer Res. 2012, 18, 1611–1618. [Google Scholar] [CrossRef]
- Moskowitz, A.J.; Perales, M.-A.; Kewalramani, T.; Yahalom, J.; Castro-Malaspina, H.; Zhang, Z.; Vanak, J.; Zelenetz, A.D.; Moskowitz, C.H. Outcomes for Patients Who Fail High-Dose Chemoradiotherapy and Autologous Stem Cell Rescue for Relapsed and Primary Refractory Hodgkin Lymphoma. Br. J. Haematol. 2009, 146, 158–163. [Google Scholar] [CrossRef]
- Roemer, M.G.M.; Redd, R.A.; Cader, F.Z.; Pak, C.J.; Abdelrahman, S.; Ouyang, J.; Sasse, S.; Younes, A.; Fanale, M.; Santoro, A.; et al. Major Histocompatibility Complex Class II and Programmed Death Ligand 1 Expression Predict Outcome After Programmed Death 1 Blockade in Classic Hodgkin Lymphoma. J. Clin. Oncol. 2018, 36, 942–950. [Google Scholar] [CrossRef]
- Bröckelmann, P.J.; Goergen, H.; Keller, U.; Meissner, J.; Ordemann, R.; Halbsguth, T.V.; Sasse, S.; Sökler, M.; Kerkhoff, A.; Mathas, S.; et al. Efficacy of Nivolumab and AVD in Early-Stage Unfavorable Classic Hodgkin Lymphoma: The Randomized Phase 2 German Hodgkin Study Group NIVAHL Trial. JAMA Oncol. 2020, 6, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.N.; Nahar, A.; Kim, E.; Marinello, P. Sequential Pembrolizumab (Pembro) and Chemotherapy (Chemo) in Newly Diagnosed, Early Unfavorable, or Advanced-Stage Classical Hodgkin Lymphoma (cHL): The Phase 2 KEYNOTE-C11 Study. J. Clin. Oncol. 2022, 40 (Suppl. S16), TPS7584. [Google Scholar] [CrossRef]
- Reinke, S.; Bröckelmann, P.J.; Iaccarino, I.; Garcia-Marquez, M.; Borchmann, S.; Jochims, F.; Kotrova, M.; Pal, K.; Brüggemann, M.; Hartmann, E. Tumor and Microenvironment Response but No Cytotoxic T-Cell Activation in Classic Hodgkin Lymphoma Treated with Anti-PD1. Blood 2020, 136, 2851–2863. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Median, IQR |
|---|---|
| PD-L1+ HRS H-score | 80 (36.5–142.8) |
| Macrophages | 6.8 (5.3–8.9) |
| PD-L1+ macrophages | 5.4 (3.6–7.1) |
| Proportion of PD-L1+ macrophages (%) | 85.9 (65.4–91.9) |
| Variable | PD-L1 H-Score | IQR of H-Score | p |
|---|---|---|---|
| Histological subtype | 0.10 | ||
| Nodular sclerosis (n = 73) | 83 | 40–50 | |
| Mixed cellularity (n = 21) | 75 | 31–121 | |
| Lymphocyte-rich (n = 3) | 20 | 3–80 | |
| Lymphocyte-depleted (n = 1) | 216 | 216–216 | |
| Clinical stage | 0.28 | ||
| Early favorable (n = 23) | 81 | 25–145 | |
| Early unfavorable (n = 29) | 67 | 35–118 | |
| Advanced (n = 45) | 85 | 40–190 | |
| Extranodal disease | 0.35 | ||
| no (n = 66) | 84 | 40–154 | |
| yes (n = 30) | 77 | 33–142 | |
| Bulky disease | 0.69 | ||
| no (n = 72) | 82 | 28–133 | |
| yes (n = 26) | 80 | 38–145 | |
| B symptoms | 0.42 | ||
| no | 75 | 36–143.5 | |
| yes | 85 | 37.5–143.5 | |
| EBV status | 0.005 | ||
| no (n = 75) | 70 | 34–104 | |
| yes (n = 22) | 136 | 82.5–182.3 |
| Variable | Macrophages | PD-L1+ Macrophages | Proportion of PD-L1+ Macrophages | |||||
|---|---|---|---|---|---|---|---|---|
| Subtype | N | IQR | N | IQR | % | IQR | ||
| Nodular sclerosis | 6.3 | 4.65–7.73 | 4.9 | 3.21–6.65 | 85.3 | 63.3–91.2 | ||
| Mixed cellularity | 9.6 | 7.62–10.65 | 8.0 | 6.4–10.31 | 89.8 | 83.9–93.9 | ||
| Lymphocyte-rich | 5.2 | 4.3–6.7 | 4.2 | 1.4–4.6 | 68.7 | 32.6–80.8 | ||
| Lymphocyte-depleted | 8.7 | 8.7–8.7 | 4.6 | 4.6–4.6 | 52.9 | 52.9–52.9 | ||
| p | 0.0002 | <0.0001 | 0.02 | |||||
| Extranodal | ||||||||
| no | 6.65 | 4.92–7.92 | 5.0 | 3.21–6.8 | 85.1 | 63.1–90.2 | ||
| yes | 7.48 | 5.3–9.8 | 6.3 | 4.0–8.42 | 88.7 | 76.7–94.9 | ||
| p | 0.18 | 0.05 | 0.06 | |||||
| Bulky | ||||||||
| no | 7.35 | 5.3–9.2 | 5.75 | 4.0–8.0 | 87.1 | 74.4–92.0 | ||
| yes | 6.2 | 4.1–7.78 | 3.9 | 2.87–6.4 | 82.3 | 56.2–91.7 | ||
| p | 0.07 | 0.04 | 0.04 | |||||
| EBV status | ||||||||
| negative | 6.3 | 4.6–7.8 | 4.8 | 3.3–6.8 | 84 | 64.1–90.9 | ||
| positive | 8.3 | 6.9–9.8 | 6.8 | 5.6–8.9 | 90.7 | 82.2 –94.6 | ||
| p | 0.008 | 0.005 | 0.11 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miljak, A.; Pavlović, A.; Benzon, B.; Čutura, L.V.; Galušić, D.; Vujčić, M.; Blaslov, V.; Durdov, M.G. High PD-L1 Expression in HRS Cells and Macrophages in Tumor Immune Microenvironment Is Associated with Adverse Outcome and EBV Positivity in Classical Hodgkin Lymphoma. Int. J. Mol. Sci. 2025, 26, 5592. https://doi.org/10.3390/ijms26125592
Miljak A, Pavlović A, Benzon B, Čutura LV, Galušić D, Vujčić M, Blaslov V, Durdov MG. High PD-L1 Expression in HRS Cells and Macrophages in Tumor Immune Microenvironment Is Associated with Adverse Outcome and EBV Positivity in Classical Hodgkin Lymphoma. International Journal of Molecular Sciences. 2025; 26(12):5592. https://doi.org/10.3390/ijms26125592
Chicago/Turabian StyleMiljak, Antonija, Antonia Pavlović, Benjamin Benzon, Lučana Vicelić Čutura, Davor Galušić, Milan Vujčić, Viktor Blaslov, and Merica Glavina Durdov. 2025. "High PD-L1 Expression in HRS Cells and Macrophages in Tumor Immune Microenvironment Is Associated with Adverse Outcome and EBV Positivity in Classical Hodgkin Lymphoma" International Journal of Molecular Sciences 26, no. 12: 5592. https://doi.org/10.3390/ijms26125592
APA StyleMiljak, A., Pavlović, A., Benzon, B., Čutura, L. V., Galušić, D., Vujčić, M., Blaslov, V., & Durdov, M. G. (2025). High PD-L1 Expression in HRS Cells and Macrophages in Tumor Immune Microenvironment Is Associated with Adverse Outcome and EBV Positivity in Classical Hodgkin Lymphoma. International Journal of Molecular Sciences, 26(12), 5592. https://doi.org/10.3390/ijms26125592