

Distribution and Maturity of Medial Collagen Fibers in Thoracoabdominal Post-Dissection Aortic Aneurysms: A Comparative Study of Marfan and Non-Marfan Patients

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Results
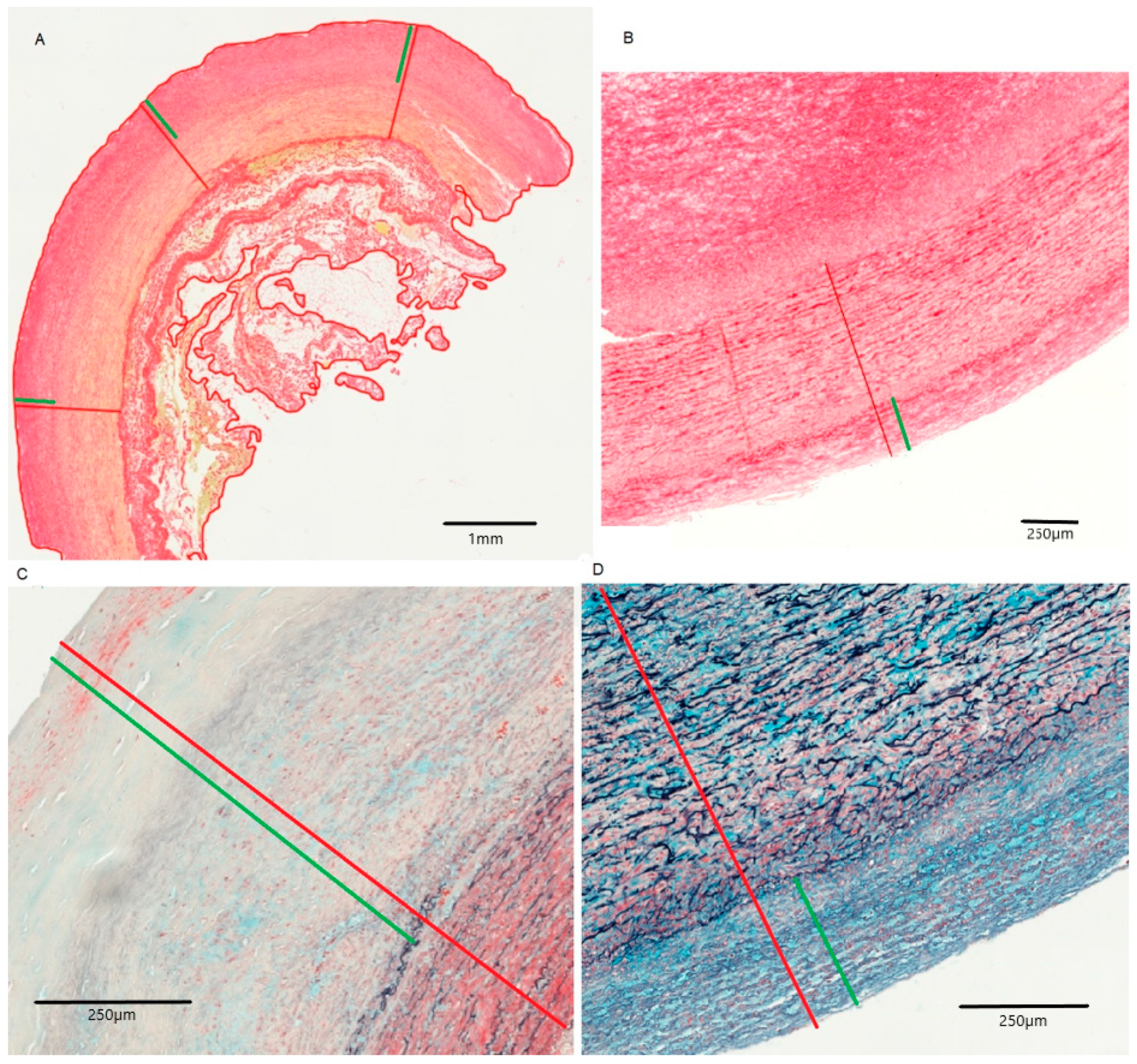
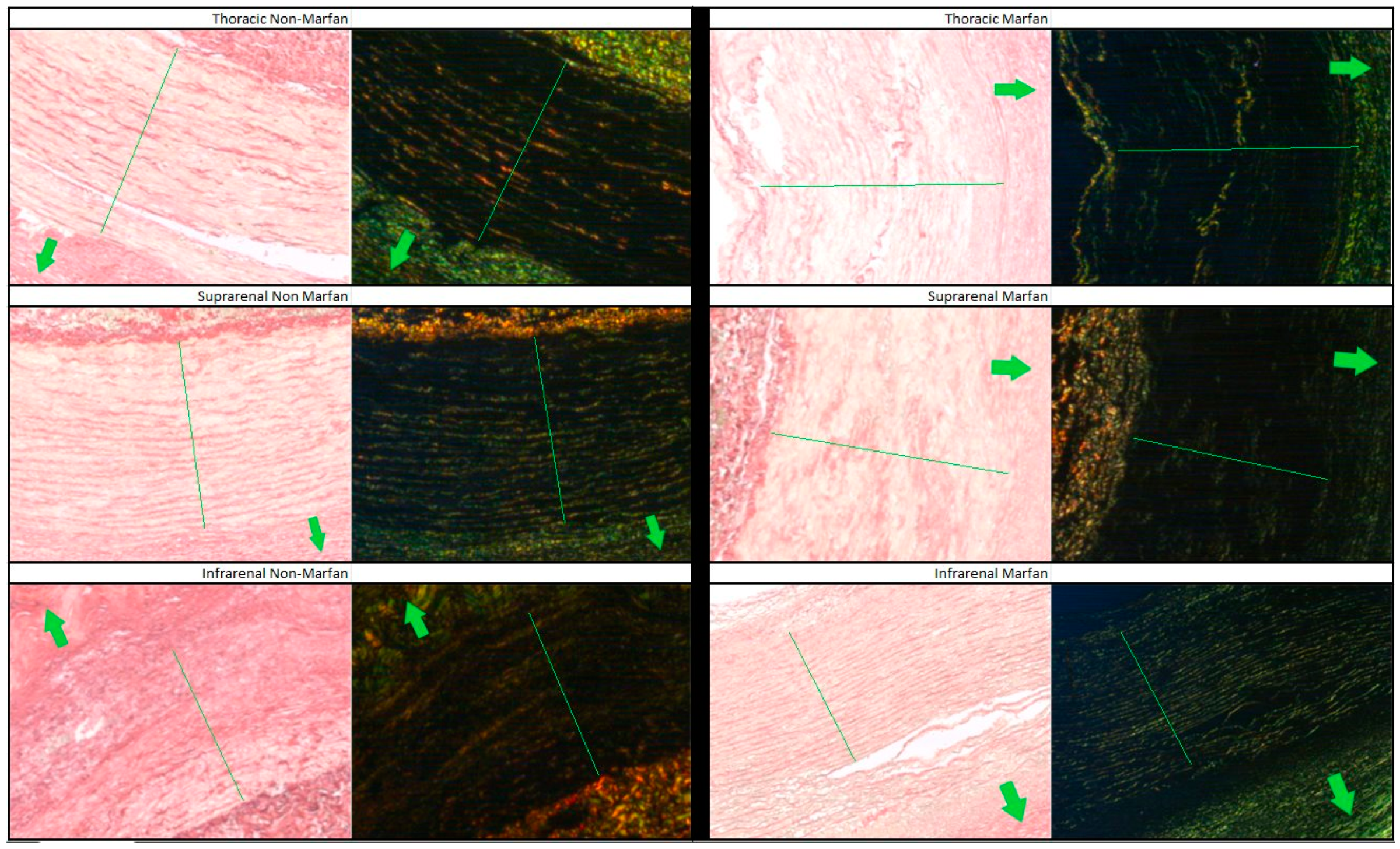
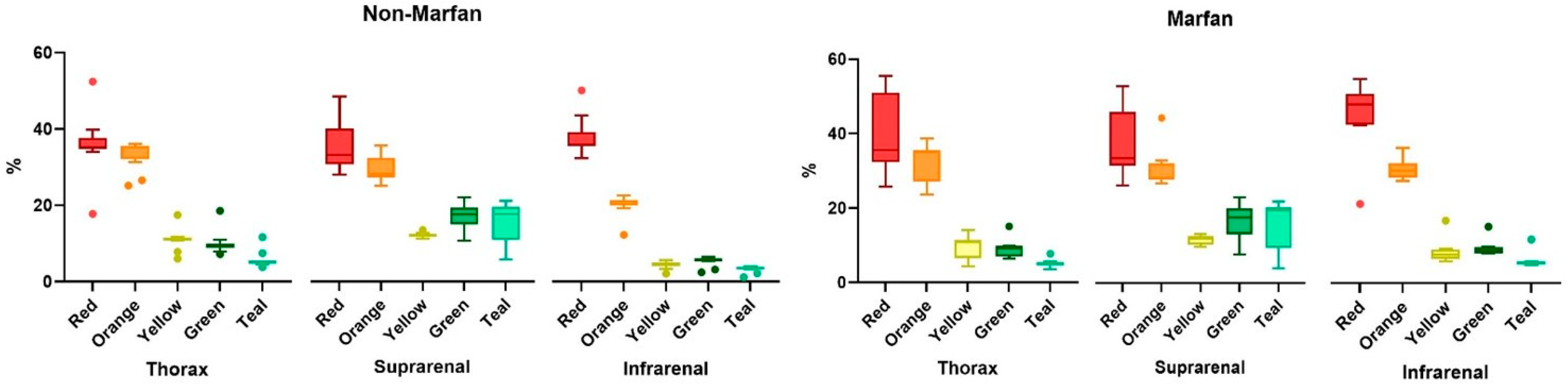
2.1. Collagen Fiber Analysis
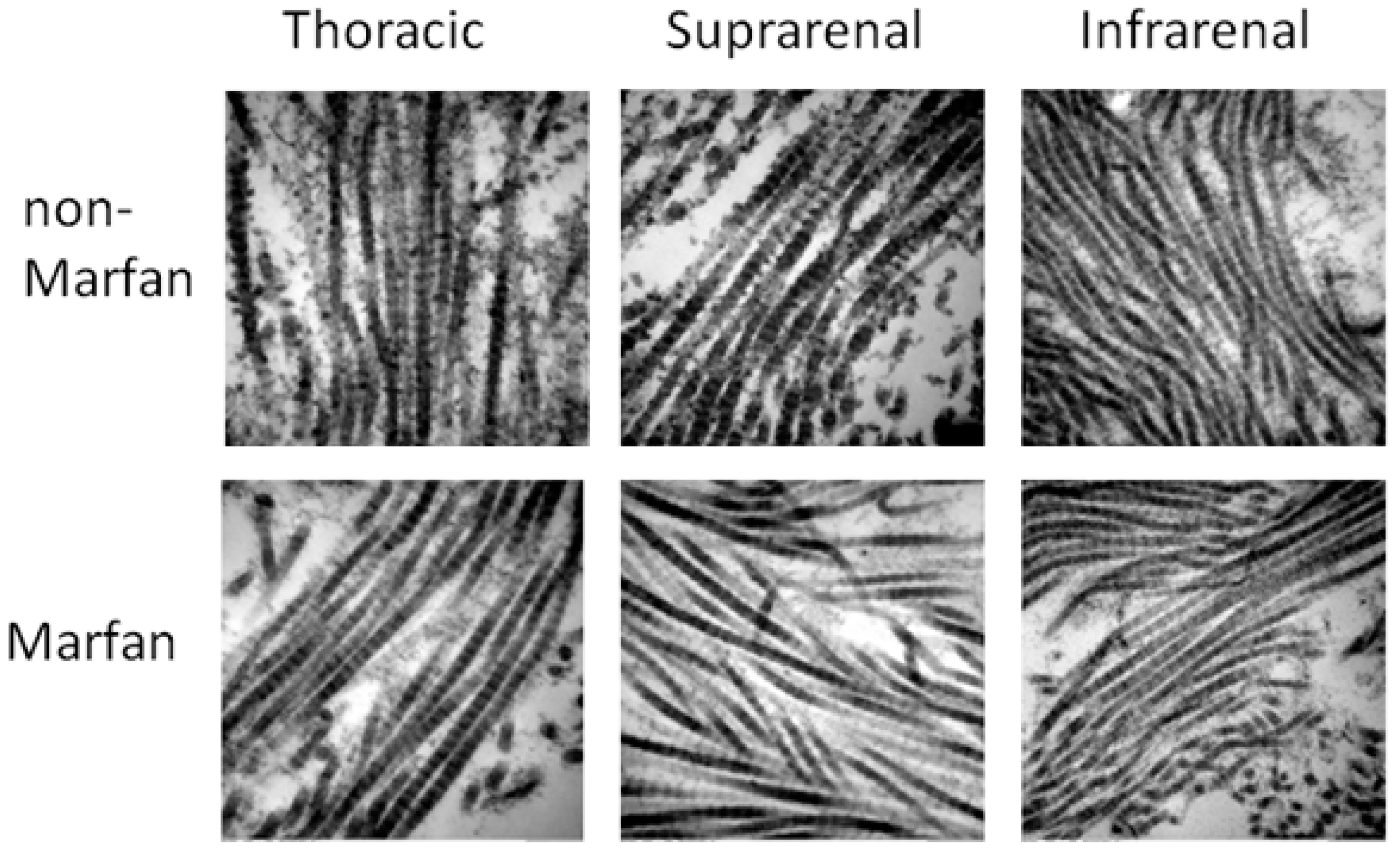
2.2. Electron Microscopy
3. Discussion
4. Materials and Methods
4.1. Study Design and Patient Selection
4.2. Tissue Sample Preparation and Histology
4.3. Electron Microscopy
4.4. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stoecker, J.B.; Wang, G.J. Epidemiology of thoracoabdominal aortic aneurysms. Semin. Vasc. Surg. 2021, 34, 18–28. [Google Scholar] [CrossRef]
- Haque, K.; Bhargava, P. Abdominal Aortic Aneurysm. Am. Fam. Physician 2022, 106, 165–172. [Google Scholar] [PubMed]
- Riambau, V.; Böckler, D.; Brunkwall, J.; Cao, P.; Chiesa, R.; Coppi, G.; Czerny, M.; Fraedrich, G.; Haulon, S.; Jacobs, M.J.; et al. Editor’s Choice—Management of Descending Thoracic Aorta Diseases: Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2017, 53, 4–52. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, J.V.; Hughes, G.C.; Appoo, J.J.; Bavaria, J.E.; Beck, A.W.; Cambria, R.P.; Charlton-Ouw, K.; Eslami, M.H.; Kim, K.M.; Leshnower, B.G.; et al. Society for Vascular Surgery (SVS) and Society of Thoracic Surgeons (STS) reporting standards for type B aortic dissections. J. Vasc. Surg. 2020, 71, 723–747. [Google Scholar] [CrossRef] [PubMed]
- Isselbacher, E.M.; Preventza, O.; Black, J.H.; Augoustides, J.G.; Beck, A.W.; Bolen, M.A.; Braverman, A.C.; Bray, B.E.; Brown-Zimmerman, M.M.; Chen, E.P.; et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2022, 146, e334–e482. [Google Scholar] [CrossRef]
- Zeigler, S.M.; Sloan, B.; Jones, J.A. Pathophysiology and Pathogenesis of Marfan Syndrome. Adv. Exp. Med. Biol. 2021, 1348, 185–206. [Google Scholar]
- Jones, B.; Tonniges, J.R.; Debski, A.; Albert, B.; Yeung, D.A.; Gadde, N.; Mahajan, A.; Sharma, N.; Calomeni, E.P.; Go, M.R.; et al. Collagen fibril abnormalities in human and mice abdominal aortic aneurysm. Acta Biomater. 2020, 110, 129–140. [Google Scholar] [CrossRef]
- Niestrawska, J.A.; Regitnig, P.; Viertler, C.; Cohnert, T.U.; Babu, A.R.; Holzapfel, G.A. The role of tissue remodeling in mechanics and pathogenesis of abdominal aortic aneurysms. Acta Biomater. 2019, 88, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Holzapfel, G.A.; Ogden, R.W. Biomechanical relevance of the microstructure in artery walls with a focus on passive and active components. Am. J. Physiol. Circ. Physiol. 2018, 315, H540–H549. [Google Scholar] [CrossRef] [PubMed]
- Niestrawska, J.A.; Pukaluk, A.; Babu, A.R.; A Holzapfel, G. Differences in Collagen Fiber Diameter and Waviness between Healthy and Aneurysmal Abdominal Aortas. Microsc. Microanal. 2022, 28, 1649–1663. [Google Scholar] [CrossRef]
- Tsamis, A.; Krawiec, J.T.; Vorp, D.A. Elastin and collagen fibre microstructure of the human aorta in ageing and disease: A review. J. R. Soc. Interface 2013, 10, 20121004. [Google Scholar] [CrossRef] [PubMed]
- Asano, K.; Cantalupo, A.; Sedes, L.; Ramirez, F. Pathophysiology and Therapeutics of Thoracic Aortic Aneurysm in Marfan Syndrome. Biomolecules 2022, 12, 128. [Google Scholar] [CrossRef]
- Sulejmani, F.; Pokutta-Paskaleva, A.; Ziganshin, B.; Leshnower, B.; Iannucci, G.; Elefteriades, J.; Sun, W. Biomechanical properties of the thoracic aorta in Marfan patients. Ann. Cardiothorac. Surg. 2017, 6, 610–624. [Google Scholar] [CrossRef]
- Lindeman, J.H.; Ashcroft, B.A.; Beenakker, J.W.; Van Es, M.; Koekkoek, N.B.; Prins, F.A.; Tielemans, J.F.; Abdul-Hussien, H.; Bank, R.A.; Oosterkamp, T.H. Distinct defects in collagen microarchitecture underlie vessel-wall failure in advanced abdominal aneurysms and aneurysms in Marfan syndrome. Proc. Natl. Acad. Sci. USA 2010, 107, 862–865. [Google Scholar] [CrossRef] [PubMed]
- Amabili, M.; Asgari, M.; Breslavsky, I.D.; Franchini, G.; Giovanniello, F.; Holzapfel, G.A. Microstructural and mechanical characterization of the layers of human descending thoracic aortas. Acta Biomater. 2021, 134, 401–421. [Google Scholar] [CrossRef]
- Rombouts, K.B.; van Merrienboer, T.A.R.; Ket, J.C.F.; Bogunovic, N.; van der Velden, J.; Yeung, K.K. The role of vascular smooth muscle cells in the development of aortic aneurysms and dissections. Eur. J. Clin. Investig. 2021, 52, e13697. [Google Scholar] [CrossRef]
- Menashi, S.; Campa, J.S.; Greenhalgh, R.M.; Powell, J.T. Collagen in abdominal aortic aneurysm: Typing, content, and degradation. J. Vasc. Surg. 1987, 6, 578–582. [Google Scholar] [CrossRef]
- Halloran, B.G.; Davis, V.A.; McManus, B.M.; Lynch, T.G.; Baxter, B. Localization of Aortic Disease Is Associated with Intrinsic Differences in Aortic Structure. J. Surg. Res. 1995, 59, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Torres-Fonseca, M.; Galan, M.; Martinez-Lopez, D.; Cañes, L.; Roldan-Montero, R.; Alonso, J.; Reyero-Postigo, T.; Orriols, M.; Mendez-Barbero, N.; Sirvent, M.; et al. Pathophysiology of abdominal aortic aneurysm: Biomarkers and novel therapeutic targets. Clín. E Investig. Arterioscler. (Engl. Ed.) 2019, 31, 166–177. [Google Scholar] [CrossRef]
- Michel, J.-B.; Martin-Ventura, J.-L.; Egido, J.; Sakalihasan, N.; Treska, V.; Lindholt, J.; Allaire, E.; Thorsteinsdottir, U.; Cockerill, G.; Swedenborg, J.; et al. Novel aspects of the pathogenesis of aneurysms of the abdominal aorta in humans. Cardiovasc. Res. 2011, 90, 18–27. [Google Scholar] [CrossRef]
- Kuivaniemi, H.; Ryer, E.J.; Elmore, J.R.; Tromp, G. Understanding the pathogenesis of abdominal aortic aneurysms. Expert. Rev. Cardiovasc. Ther. 2015, 13, 975–987. [Google Scholar] [CrossRef] [PubMed]
- Ruddy, J.M.; Jones, J.A.; Spinale, F.G.; Ikonomidis, J.S. Regional heterogeneity within the aorta: Relevance to aneurysm disease. J. Thorac. Cardiovasc. Surg. 2008, 136, 1123–1130. [Google Scholar] [CrossRef]
- Sweeting, M.J.; Thompson, S.G.; Brown, L.C.; Powell, J.T. Meta-analysis of individual patient data to examine factors affecting growth and rupture of small abdominal aortic aneurysms. Br. J. Surg. 2012, 99, 655–665. [Google Scholar] [CrossRef]
- Tong, J.; Schriefl, A.; Cohnert, T.; Holzapfel, G. Gender Differences in Biomechanical Properties, Thrombus Age, Mass Fraction and Clinical Factors of Abdominal Aortic Aneurysms. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Villard, C.; Eriksson, P.; Hanemaaijer, R.; Lindeman, J.H.; Hultgren, R. The composition of collagen in the aneurysm wall of men and women. J. Vasc. Surg. 2017, 66, 579–585.e1. [Google Scholar] [CrossRef] [PubMed]
- Cattell, M.; Anderson, J.C.; Hasleton, P.S. Age-related changes in amounts and concentrations of collagen and elastin in normotensive human thoracic aorta. Clin. Chim. Acta 1996, 245, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Mattson, J.M.; Zhang, Y. Effect of aging on the biaxial mechanical behavior of human descending thoracic aorta: Experiments and constitutive modeling considering collagen crosslinking. J. Mech. Behav. Biomed. Mater. 2023, 140, 105705. [Google Scholar] [CrossRef]
- Holzapfel, G.A.; Ogden, R.W. An arterial constitutive model accounting for collagen content and cross-linking. J. Mech. Phys. Solids 2019, 136, 103682. [Google Scholar] [CrossRef]
- Shimizu, K.; Mitchell, R.N.; Libby, P. Inflammation and Cellular Immune Responses in Abdominal Aortic Aneurysms. Arter. Thromb. Vasc. Biol. 2006, 26, 987–994. [Google Scholar] [CrossRef]
- Xu, X.; Zhang, F.; Lu, Y.; Yu, S.; Sun, W.; Sun, S.; Cheng, J.; Ma, J.; Zhang, M.; Zhang, C.; et al. Silencing of NONO inhibits abdominal aortic aneurysm in apolipoprotein E-knockout mice via collagen deposition and inflammatory inhibition. J. Cell. Mol. Med. 2019, 23, 7449–7461. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A.J. Molecular mechanisms of ageing in connective tissues. Mech. Ageing Dev. 2001, 122, 735–755. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (n = 25) | Marfan (n = 9) | Non-Marfan (n = 16) | p-Value | |
|---|---|---|---|---|
| Age (years) | 51.1 ± 11 | 42.56 ± 10.06 | 55.88 ± 8.45 | 0.005 * |
| Women | 7 (28) | 4 (44.4) | 3 (18.8) | 0.2 |
| Men | 18 (72) | 5 (55.6) | 13 (81.2) | 0.2 |
| Maximal aortic diameter (mm) | 60.53 ± 14.15 | 58.81 ± 11.45 | 61.49 ± 15.74 | 0.63 |
| Aneurysm extent | 0.56 | |||
| Crawford I | 4 (16) | 1 (11.1) | 3 (18.8) | |
| Crawford II | 10 (40) | 5 (55.6) | 5 (31.3) | |
| Crawford III | 5 (20) | 2 (22.2) | 3 (18.8) | |
| Crawford IV | 6 (24) | 1 (11.1) | 5 (31.3) | |
| Descending Thoracic Aorta | Suprarenal Aorta | Infrarenal Aorta | Friedman p-Value | |
|---|---|---|---|---|
| Marfan | 318.53 [242.4–426.4] | 390.03 [356.3–407.5] | 729.72 [341.6–1032.4] | 0 |
| Non-Marfan | 568.94 [436.9–602.8] | 414.9 [379–421.9] | 1068.30 [1036.8–1147.7] | <0.001 * |
| Mann–Whitney p-value | 0.03 * | 0.14 | 0.02 * |
| Descending Thoracic Aorta | Suprarenal Aorta | Infrarenal Aorta | Friedman ANOVA p-Value | |
|---|---|---|---|---|
| Marfan | 16.8 [13.9–21.7] | 18.1 [16.9–21] | 29.7 [26.9–39] | 0.002 * |
| Non-Marfan | 21.9 [19.5–29.8] | 26.7 [24.8–27.8] | 54.1 [49.5–61.6] | <0.001 * |
| Mann–Whitney p-value | 0.16 | 0.19 | 0.06 |
| Descending Thoracic Aorta | Suprarenal Aorta | Infrarenal Aorta | |
|---|---|---|---|
| Male | 22.15 [18.18–32.16] | 27.76 [20.84–27.76] | 56.19 [40.03–61.63] |
| Female | 15.89 [8.65–20.81] | 18.14 [13.16–18.78] | 28.17 [22.93–31.88] |
| p-value | 0.086 | 0.037 * | 0.014 * |
| Descending Thoracic Aorta | Suprarenal Aorta | Infrarenal Aorta | Friedman p-Value | ||
|---|---|---|---|---|---|
| Red | Marfan | 35.6 [34–41.9] | 28.3 [26.7–35.3] | 46 [41–48.5] | 0.02 |
| Non-Marfan | 35.3 [34.9–36.8] | 28.6 [26.4–34.3] | 48.2 [47.8–50.3] | <0.001 * | |
| p-value | 0.49 | 0.86 | 0.08 | ||
| Orange | Marfan | 35.3 [31.4–35.4] | 23.7 [23.6–25.8] | 28.9 [28.0–30.2] | 0 |
| Non-Marfan | 35.2 [33.9–35.5] | 24.3 [23.6–27.5] | 28.4 [27.4–28.5] | 0.004 * | |
| p-value | 0.749 | 0.799 | 0.151 | ||
| Yellow | Marfan | 10.9 [9.2–11.4] | 10.0 [9.1–10.5] | 7.3 [6.2–7.9] | 0.2 |
| Non-Marfan | 11.3 [11.0–11.4] | 10.6 [10.2–10.7] | 6.3 [5.7–6.4] | <0.001 * | |
| p-value | 0.4 | 0.1 | 0.104 | ||
| Green | Marfan | 9.1 [8.0–9.7] | 14.8 [12.3–16.8] | 8.3 [7.7–8.9] | 0.09 |
| Non-Marfan | 9.6 [9.3–9.8] | 15.2 [13.0–16.7] | 7.9 [7.7–8.0] | <0.001 * | |
| p-value | 0.551 | 0.754 | 0.09 | ||
| Teal | Marfan | 4.9 [4.6–5.2] | 16.4 [10.0–16.9] | 5.3 [4.8–5.5] | 0.09 |
| Non-Marfan | 5.0 [4.9–5.2] | 15.3 [10.5–16.8] | 4.8 [4.6–5.0] | <0.001 * | |
| p-value | 0.47 | 0.96 | 0.13 |
| Descending Thoracic Aorta | Suprarenal Aorta | Infrarenal Aorta | |
|---|---|---|---|
| Marfan | 63.4 ± 8.4 | 50.2 ± 4.4 | 59.8 ± 3.5 |
| Non-Marfan | 64.4 ± 1 | 58.4 ± 14 | 54 ± 8.6 |
| p-value | 0.56 | 0.51 | 0.45 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doukas, P.; Hruschka, B.; Bassett, C.; Buhl, E.M.; Simon, F.; Saraber, P.; Jacobs, M.J.; Uhl, C.; Schurgers, L.J.; Gombert, A. Distribution and Maturity of Medial Collagen Fibers in Thoracoabdominal Post-Dissection Aortic Aneurysms: A Comparative Study of Marfan and Non-Marfan Patients. Int. J. Mol. Sci. 2025, 26, 14. https://doi.org/10.3390/ijms26010014
Doukas P, Hruschka B, Bassett C, Buhl EM, Simon F, Saraber P, Jacobs MJ, Uhl C, Schurgers LJ, Gombert A. Distribution and Maturity of Medial Collagen Fibers in Thoracoabdominal Post-Dissection Aortic Aneurysms: A Comparative Study of Marfan and Non-Marfan Patients. International Journal of Molecular Sciences. 2025; 26(1):14. https://doi.org/10.3390/ijms26010014
Chicago/Turabian StyleDoukas, Panagiotis, Bernhard Hruschka, Cathryn Bassett, Eva Miriam Buhl, Florian Simon, Pepijn Saraber, Michael Johan Jacobs, Christian Uhl, Leon J. Schurgers, and Alexander Gombert. 2025. "Distribution and Maturity of Medial Collagen Fibers in Thoracoabdominal Post-Dissection Aortic Aneurysms: A Comparative Study of Marfan and Non-Marfan Patients" International Journal of Molecular Sciences 26, no. 1: 14. https://doi.org/10.3390/ijms26010014
APA StyleDoukas, P., Hruschka, B., Bassett, C., Buhl, E. M., Simon, F., Saraber, P., Jacobs, M. J., Uhl, C., Schurgers, L. J., & Gombert, A. (2025). Distribution and Maturity of Medial Collagen Fibers in Thoracoabdominal Post-Dissection Aortic Aneurysms: A Comparative Study of Marfan and Non-Marfan Patients. International Journal of Molecular Sciences, 26(1), 14. https://doi.org/10.3390/ijms26010014