
Prognostic Impact of Visceral Adipose Tissue Imaging Parameters in Patients with Cholangiocarcinoma after Surgical Resection

 , , and
, , and
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Correlation Analysis
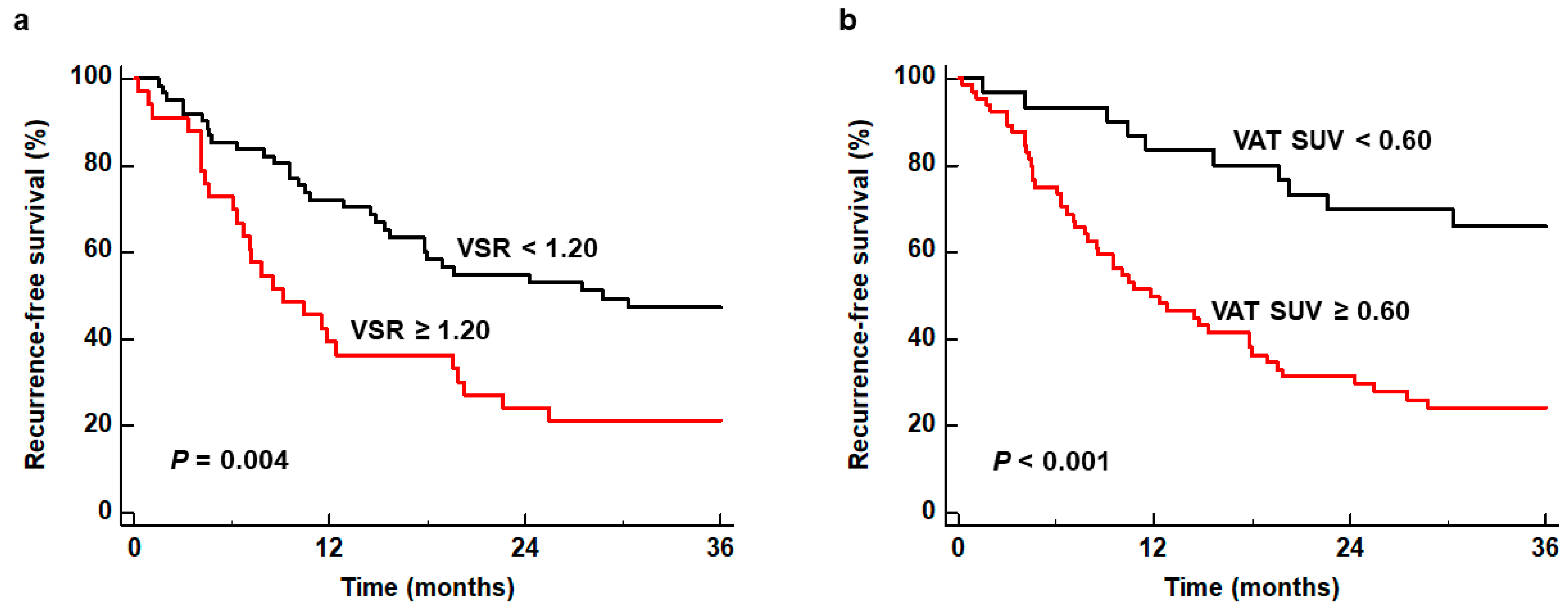
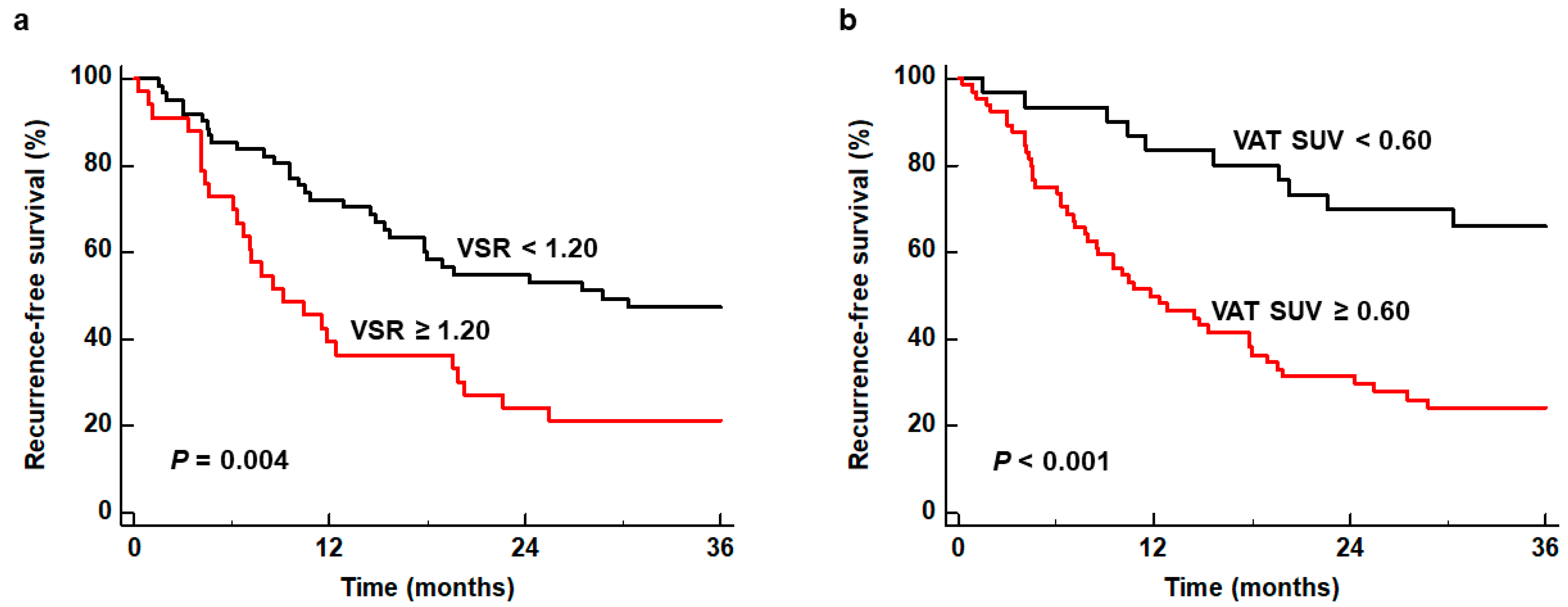
2.3. Survival Analysis for RFS and OS
3. Discussion
4. Materials and Methods
4.1. Study Participants
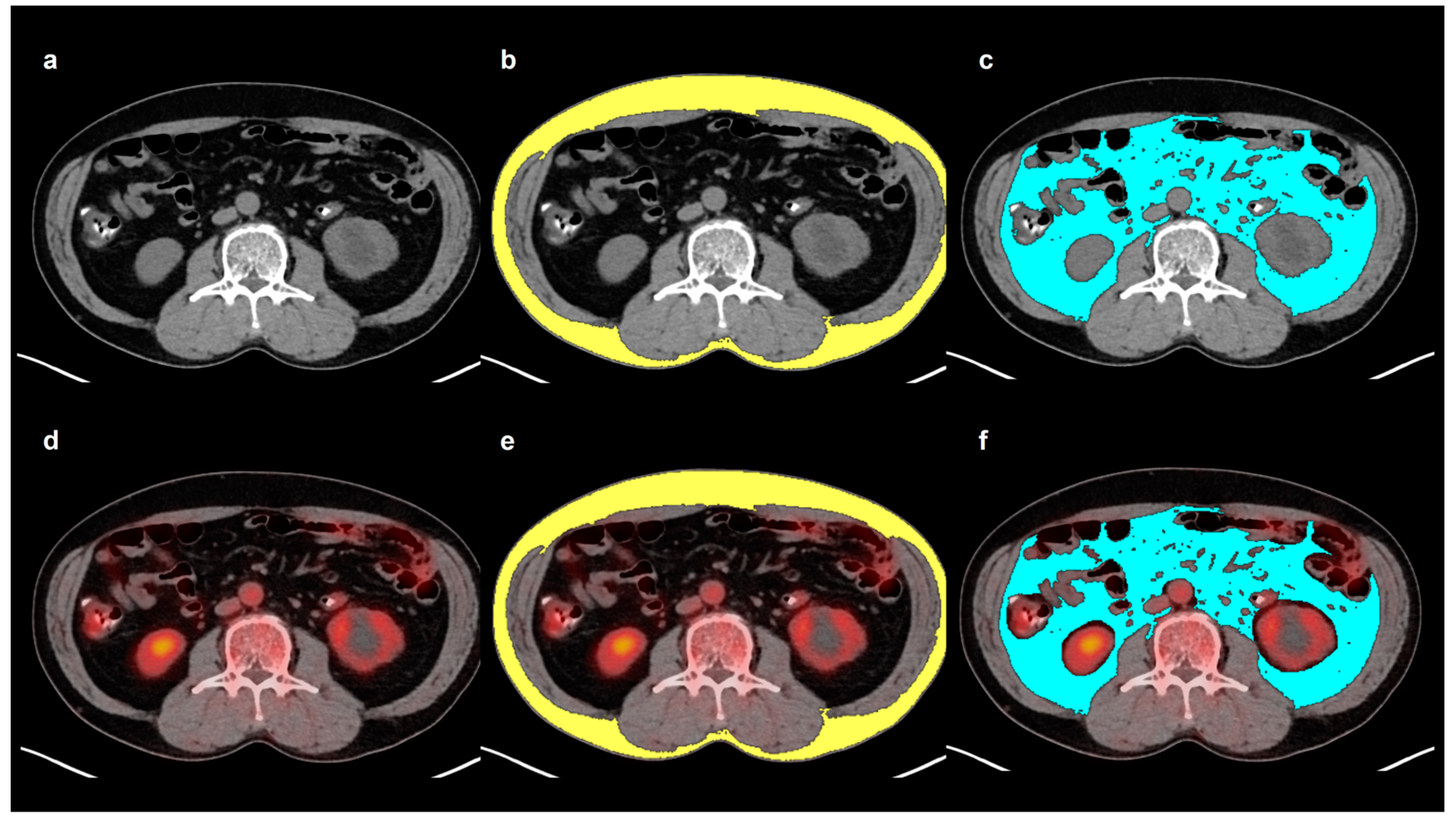
4.2. Adipose Tissue Imaging Parameter Measurements
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kendall, T.; Verheij, J.; Gaudio, E.; Evert, M.; Guido, M.; Goeppert, B.; Carpino, G. Anatomical, histomorphological and molecular classification of cholangiocarcinoma. Liver Int. 2019, 39 (Suppl. 1), 7–18. [Google Scholar] [CrossRef] [PubMed]
- Qurashi, M.; Vithayathil, M.; Khan, S.A. Epidemiology of cholangiocarcinoma. Eur. J. Surg. Oncol. 2023, 107064. [Google Scholar] [CrossRef] [PubMed]
- Hau, H.M.; Devantier, M.; Jahn, N.; Sucher, E.; Rademacher, S.; Seehofer, D.; Sucher, R. Impact of body mass index on tumor recurrence in patients undergoing liver resection for perihilar cholangiocarcinoma (pCCA). Cancers 2021, 13, 4772. [Google Scholar] [CrossRef]
- Merath, K.; Mehta, R.; Hyer, J.M.; Bagante, F.; Sahara, K.; Alexandrescu, S.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; et al. Impact of body mass index on tumor recurrence among patients undergoing curative-intent resection of intrahepatic cholangiocarcinoma- a multi-institutional international analysis. Eur. J. Surg. Oncol. 2019, 45, 1084–1091. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.J.; Williams, P.J.; Claasen, M.; Ivanics, T.; Englesakis, M.; Gallinger, S.; Hansen, B.; Sapisochin, G. Systematic review and meta-analysis of prognostic factors for early recurrence in intrahepatic cholangiocarcinoma after curative-intent resection. Ann. Surg. Oncol. 2022, 29, 4337–4353. [Google Scholar] [CrossRef] [PubMed]
- Pascale, A.; Rosmorduc, O.; Duclos-Vallée, J.C. New epidemiologic trends in cholangiocarcinoma. Clin. Res. Hepatol. Gastroenterol. 2023, 47, 102223. [Google Scholar] [CrossRef] [PubMed]
- Okumura, S.; Kaido, T.; Hamaguchi, Y.; Kobayashi, A.; Shirai, H.; Fujimoto, Y.; Iida, T.; Yagi, S.; Taura, K.; Hatano, E.; et al. Impact of skeletal muscle mass, muscle quality, and visceral adiposity on outcomes following resection of intrahepatic cholangiocarcinoma. Ann. Surg. Oncol. 2017, 24, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Lacaze, L.; Bergeat, D.; Rousseau, C.; Sulpice, L.; Val-Laillet, D.; Thibault, R.; Boudjema, K. High Visceral fat is associated with a worse survival after liver resection for intrahepatic cholangiocarcinoma. Nutr. Cancer 2023, 75, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Lurje, I.; Uluk, D.; Pavicevic, S.; Phan, M.D.; Eurich, D.; Fehrenbach, U.; Geisel, D.; Auer, T.A.; Pelzer, U.; Modest, D.P.; et al. Body composition is associated with disease aetiology and prognosis in patients undergoing resection of intrahepatic cholangiocarcinoma. Cancer Med. 2023, 12, 17569–17580. [Google Scholar] [CrossRef]
- Iyengar, N.M.; Gucalp, A.; Dannenberg, A.J.; Hudis, C.A. Obesity and cancer mechanisms: Tumor microenvironment and inflammation. J. Clin. Oncol. 2016, 34, 4270–4276. [Google Scholar] [CrossRef]
- Chang, M.L.; Yang, Z.; Yang, S.S. Roles of adipokines in digestive diseases: Markers of inflammation, metabolic alteration and disease progression. Int. J. Mol. Sci. 2020, 21, 8308. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Son, M.W.; Chung, I.K.; Cho, Y.S.; Lee, M.S.; Lee, S.M. Significance of CT attenuation and F-18 fluorodeoxyglucose uptake of visceral adipose tissue for predicting survival in gastric cancer patients after curative surgical resection. Gastric Cancer 2020, 23, 273–284. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, D.; Bae, S.J.; Ahn, S.G.; Jeong, J.; Park, W.C.; Ryu, Y.H.; Jeon, T.J.; Lee, Y.; Cha, Y.J.; et al. 18F-FDG uptake of visceral adipose tissue on preoperative PET/CT as a predictive marker for breast cancer recurrence. Sci. Rep. 2022, 12, 21109. [Google Scholar] [CrossRef] [PubMed]
- Ebadi, M.; Moctezuma-Velazquez, C.; Meza-Junco, J.; Baracos, V.E.; DunichandHoedl, A.R.; Ghosh, S.; Sarlieve, P.; Owen, R.J.; Kneteman, N.; Montano-Loza, A.J. Visceral adipose tissue radiodensity is linked to prognosis in hepatocellular carcinoma patients treated with selective internal radiation therapy. Cancers 2020, 12, 356. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.; Lee, J.W.; Jang, S.H.; Lee, H.J.; Lee, J.H.; Oh, M.H.; Lee, S.M. Prognostic significance of imaging features of peritumoral adipose tissue in FDG PET/CT of patients with colorectal cancer. Eur. J. Radiol. 2021, 145, 110047. [Google Scholar] [CrossRef]
- Ahn, H.; Song, G.J.; Jang, S.H.; Son, M.W.; Lee, H.J.; Lee, M.S.; Lee, J.H.; Oh, M.H.; Jeong, G.C.; Yun, J.H.; et al. Predicting the recurrence of gastric cancer using the textural features of perigastric adipose tissue on [18F]FDG PET/CT. Int. J. Mol. Sci. 2022, 23, 11985. [Google Scholar] [CrossRef]
- Sun, D.; Yin, H.; Liu, X.; Ding, Z.; Shen, L.; Sah, S.; Han, J.; Wu, G. Elevated 18F-FDG uptake in subcutaneous adipose tissue correlates negatively with nutritional status and prognostic survival in cachexia patients with gastric cancer. Clin. Nutr. 2024, 43, 567–574. [Google Scholar] [CrossRef]
- Sanhueza, S.; Simón, L.; Cifuentes, M.; Quest, A.F.G. The adipocyte-macrophage relationship in cancer: A potential target for antioxidant therapy. Antioxidants 2023, 12, 126. [Google Scholar] [CrossRef]
- Yun, H.; Jeong, H.R.; Kim, D.Y.; You, J.E.; Lee, J.U.; Kang, D.H.; Koh, D.I.; Ryu, Y.S.; Bae, S.; Jin, D.H. Degradation of AZGP1 suppresses apoptosis and facilitates cholangiocarcinoma tumorigenesis via TRIM25. J. Cell. Mol. Med. 2024, 28, e18104. [Google Scholar] [CrossRef]
- Kalezic, A.; Udicki, M.; Srdic Galic, B.; Aleksic, M.; Korac, A.; Jankovic, A.; Korac, B. Tissue-specific warburg effect in breast cancer and cancer-associated adipose tissue-relationship between AMPK and glycolysis. Cancers 2021, 13, 2731. [Google Scholar] [CrossRef]
- Grigoraș, A.; Amalinei, C. Multi-faceted role of cancer-associated adipocytes in colorectal cancer. Biomedicines 2023, 11, 2401. [Google Scholar] [CrossRef] [PubMed]
- Murphy, R.A.; Register, T.C.; Shively, C.A.; Carr, J.J.; Ge, Y.; Heilbrun, M.E.; Cummings, S.R.; Koster, A.; Nevitt, M.C.; Satterfield, S.; et al. Adipose tissue density, a novel biomarker predicting mortality risk in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Lee, S.M.; Chung, Y.A. Prognostic value of CT attenuation and FDG uptake of adipose tissue in patients with pancreatic adenocarcinoma. Clin. Radiol. 2018, 73, 1056.e1–1056.e10. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wei, Y.; Hu, X.; Pan, J.; Wu, J.; Wang, B.; Zhang, H.; Shi, G.; Liu, X.; Zhao, J.; et al. Fat Attenuation index of renal cell carcinoma reveals biological characteristics and survival outcome. Front. Oncol. 2022, 12, 786981. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Sun, Z.; Li, O.; Guo, C.; Yi, W.; Tan, Z.; Jiang, B. Leptin stimulates the epithelial-mesenchymal transition and pro-angiogenic capability of cholangiocarcinoma cells through the miR-122/PKM2 axis. Int. J. Oncol. 2019, 55, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Xia, T.; Li, K.; Niu, N.; Shao, Y.; Ding, D.; Thomas, D.L.; Jing, H.; Fujiwara, K.; Hu, H.; Osipov, A.; et al. Immune cell atlas of cholangiocarcinomas reveals distinct tumor microenvironments and associated prognoses. J. Hematol. Oncol. 2022, 15, 37. [Google Scholar] [CrossRef]
- Park, H.S.; Kim, H.S.; Beom, S.H.; Rha, S.Y.; Chung, H.C.; Kim, J.H.; Chun, Y.J.; Lee, S.W.; Choe, E.A.; Heo, S.J.; et al. Marked loss of muscle, visceral fat, or subcutaneous fat after gastrectomy predicts poor survival in advanced gastric cancer: Single-center study from the CLASSIC trial. Ann. Surg. Oncol. 2018, 25, 3222–3230. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Factors | Number of Patients (%) | |
|---|---|---|
| Age (years) | 68 (36–81) * | |
| Sex | Men | 66 (70.2%) |
| Women | 28 (29.8%) | |
| Body mass index (kg/m2) | 24.1 (18.0–32.3) * | |
| Obesity | Obese | 38 (40.4%) |
| Underweight/normal | 56 (59.6%) | |
| Blood tests | CA19-9 (U/mL) | 103.0 (0.8–13,328.0) * |
| CRP (mg/dL) | 4.03 (0.12–1005.10) * | |
| Tumor classification | Intrahepatic | 11 (11.7%) |
| Perihilar | 37 (39.4%) | |
| Distal | 46 (48.9%) | |
| T stage | T1 | 16 (17.0%) |
| T2 | 26 (27.7%) | |
| T3 | 29 (30.9%) | |
| T4 | 23 (24.5%) | |
| Lymph node metastasis | Absence | 69 (73.4%) |
| Presence | 25 (26.6%) | |
| TNM stage | Stages I–II | 43 (45.7%) |
| Stages III–IV | 51 (54.3%) | |
| Tumor size (cm) | 3.0 (1.1–12.0) * | |
| Histological grade | Well | 14 (14.9%) |
| Moderately | 62 (66.0%) | |
| Poorly | 18 (19.1%) | |
| Perineural invasion | Absence | 30 (31.9%) |
| Presence | 64 (68.1%) | |
| Lymphovascular invasion | Absence | 61 (64.9%) |
| Presence | 33 (35.1%) | |
| Extent of resection | R0 | 48 (51.1%) |
| R1 | 33 (35.1%) | |
| R2 | 13 (13.8%) | |
| Adjuvant treatment | No | 35 (37.2%) |
| Yes | 59 (62.8%) | |
| Factors | SAI | VAI | VSR | SAT HU | SAT SUV | VAT HU | VAT SUV | |
|---|---|---|---|---|---|---|---|---|
| Tumor classification * | Intrahepatic | 32.9 (25.5–47.5) | 49.1 (30.2–69.9) | 1.22 (0.93–2.13) | −91.8 (−98.7–−86.8) | 0.38 (0.34–0.41) | −85.1 (−98.0–−80.1) | 0.69 (0.54–0.78) |
| Perihilar | 45.9 (33.3–81.8) | 46.5 (31.1–59.8) | 0.87 (0.53–1.30) | −97.7 (−107.0–−91.8) | 0.39 (0.34–0.46) | −89.7 (−97.6–−80.9) | 0.76 (0.61–0.84) | |
| Distal | 44.8 (35.0–61.2) | 46.8 (34.6–61.8) | 1.04 (0.70–1.42) | −97.1 (−101.8–−91.3) | 0.38 (0.33–0.46) | −89.5 (−95.6–−81.6) | 0.63 (0.54–0.86) | |
| p-value | 0.165 | 0.896 | 0.163 | 0.226 | 0.781 | 0.944 | 0.475 | |
| TNM stage * | Stages I–II | 44.9 (35.2–61.2) | 43.4 (31.7–55.6) | 0.90 (0.57–1.26) | −97.5 (−104.4–−94.6) | 0.36 (0.32–0.45) | −91.4 (−99.3–−81.7) | 0.62 (0.54–0.79) |
| Stages III–IV | 44.9 (33.0–64.0) | 49.6 (34.2–68.5) | 1.16 (0.81–1.48) | −96.1 (−102.1–−89.5) | 0.39 (0.34–0.46) | −88.0 (−94.0–−81.6) | 0.71 (0.59–0.84) | |
| p-value | 0.832 | 0.105 | 0.084 | 0.263 | 0.191 | 0.196 | 0.061 | |
| Histological grade * | Well | 47.1 (31.7–80.2) | 55.2 (36.1–70.7) | 1.07 (0.70–1.43) | −104.2 (−107.4–−99.7) | 0.37 (0.29–0.43) | −96.5 (−101.7–−85.9) | 0.55 (0.52–0.76) |
| Moderately | 44.6 (33.4–57.8) | 46.4 (31.5–61.1) | 1.02 (0.62–1.29) | −96.5 (−101.8–−89.5) | 0.38 (0.34–0.46) | −88.6 (−94.2–−81.6) | 0.68 (0.58–0.83) | |
| Poorly | 48.9 (28.3–70.2) | 47.2 (34.3–72.0) | 1.03 (0.68–1.53) | −95.1 (−102.1–−90.5) | 0.39 (0.33–0.48) | −87.2 (−95.3–−77.2) | 0.82 (0.66–0.86) | |
| p-value | 0.642 | 0.404 | 0.825 | 0.017 | 0.424 | 0.042 | 0.008 | |
| Perineural invasion * | Absence | 44.9 (33.0–57.7) | 49.2 (34.6–63.8) | 1.11 (0.61–1.43) | −97.3 (−102.0–−92.3) | 0.39 (0.35–0.47) | −91.6 (−97.4–−85.2) | 0.60 (0.54–0.82) |
| Presence | 45.0 (34.0–66.9) | 46.5 (31.8–62.3) | 0.97 (0.69–1.35) | −97.1 (−103.5–−90.3) | 0.38 (0.33–0.44) | −88.2 (−95.5–−81.3) | 0.70 (0.59–0.85) | |
| p-value | 0.519 | 0.733 | 0.615 | 0.990 | 0.226 | 0.326 | 0.174 | |
| Lymphovascular invasion * | Absence | 46.0 (35.4–66.5) | 47.3 (34.0–63.0) | 0.97 (0.61–1.36) | −99.1 (−104.9–−93.2) | 0.38 (0.34–0.45) | −89.8 (−98.2–−83.2) | 0.65 (0.55–0.82) |
| Presence | 37.7 (25.6–54.6) | 46.4 (31.9–62.8) | 1.16 (0.81–1.52) | −93.6 (−97.7–−86.8) | 0.38 (0.33–0.46) | −85.8 (−94.1–−78.8) | 0.71 (0.63–0.85) | |
| p-value | 0.114 | 0.666 | 0.209 | 0.013 | 0.612 | 0.104 | 0.230 | |
| Extent of resection * | R0 | 45.2 (36.7–58.4) | 48.8 (34.8–66.3) | 1.14 (0.57–1.37) | −99.4 (−103.9–−92.9) | 0.37 (0.33–0.46) | −91.2 (−100.1–−83.6) | 0.65 (0.56–0.83) |
| R1 | 38.9 (24.6–68.3) | 43.4 (31.4–62.0) | 0.97 (0.79–1.41) | −95.6 (−100.8–−86.8) | 0.39 (0.35–0.44) | −89.7 (−93.6–−81.4) | 0.69 (0.59–0.81) | |
| R2 | 41.9 (34.5–73.2) | 49.1 (35.4–61.5) | 0.97 (0.77–1.50) | −96.1 (−103.8–−89.6) | 0.38 (0.34–0.42) | −82.1 (−94.1–−77.1) | 0.81 (0.67–0.88) | |
| p-value | 0.520 | 0.737 | 0.951 | 0.222 | 0.735 | 0.102 | 0.103 | |
| Recur event * | No recurrence | 45.1 (34.9–65.3) | 37.1 (29.6–55.4) | 0.91 (0.61–1.19) | −98.3 (−103.9–−95.0) | 0.36 (0.32–0.41) | −91.8 (−99.7–−83.6) | 0.59 (0.52–0.72) |
| Recurrence | 44.6 (30.6–60.1) | 49.4 (34.9–63.2) | 1.16 (0.73–1.52) | −95.5 (−101.9–−89.5) | 0.39 (0.34–0.46) | −87.2 (−94.1–−80.9) | 0.77 (0.61–0.87) | |
| p-value | 0.744 | 0.097 | 0.057 | 0.119 | 0.093 | 0.052 | 0.011 | |
| Tumor size | Correlation coefficient | 0.125 | 0.198 | 0.152 | −0.066 | 0.013 | −0.098 | 0.040 |
| p-value | 0.231 | 0.057 | 0.147 | 0.529 | 0.904 | 0.351 | 0.701 | |
| Serum CA19−9 | Correlation coefficient | −0.015 | −0.038 | −0.015 | 0.099 | −0.080 | 0.136 | 0.122 |
| p-value | 0.885 | 0.714 | 0.886 | 0.342 | 0.445 | 0.191 | 0.242 | |
| Serum CRP | Correlation coefficient | −0.085 | 0.176 | 0.265 | 0.219 | 0.030 | 0.140 | 0.037 |
| p-value | 0.417 | 0.090 | 0.010 | 0.033 | 0.771 | 0.179 | 0.726 | |
| Variables | Recurrence-Free Survival | Overall Survival | |||
|---|---|---|---|---|---|
| p-Value | Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | ||
| Age | 1-year increase | 0.940 | 0.999 (0.971–1.027) | 0.093 | 1.035 (0.994–1.077) |
| Sex | Women | 1.000 | 1.000 | ||
| Men | 0.324 | 0.762 (0.444–1.308) | 0.442 | 0.769 (0.393–1.503) | |
| Obesity | Underweight/normal | 1.000 | 1.000 | ||
| Obese | 0.507 | 1.239 (0.499–1.609) | 0.053 | 1.499 (0.989–2.750) | |
| Tumor classification | Intrahepatic | 1.000 | 1.000 | ||
| Perihilar | 0.216 | 1.832 (0.703–4.778) | 0.060 | 6.911 (0.923–51.751) | |
| Distal | 0.541 | 1.346 (0.520–3.488) | 0.135 | 4.645 (0.621–34.748) | |
| TNM stage | Stages I–II | 1.000 | 1.000 | ||
| Stages III–IV | 0.001 | 2.417 (1.410–4.143) | 0.025 | 2.143 (1.100–4.176) | |
| Tumor size | 1.0 cm increase | 0.098 | 1.100 (0.980–1.231) | 0.125 | 1.115 (0.970–1.282) |
| Histological grade | Well | 1.000 | 1.000 | ||
| Moderately | 0.125 | 1.965 (0.830–4.653) | 0.645 | 1.256 (0.476–3.311) | |
| Poorly | 0.002 | 4.551 (1.740–11.904) | 0.023 | 3.459 (1.184–10.108) | |
| Perineural invasion | Absence | 1.000 | 1.000 | ||
| Presence | 0.007 | 2.355 (1.265–4.382) | 0.008 | 5.970 (2.107–6.913) | |
| Lymphovascular invasion | Absence | 1.000 | 1.000 | ||
| Presence | 0.033 | 1.748 (1.047–2.918) | 0.006 | 2.442 (1.300–4.589) | |
| Extent of resection | R0 | 1.000 | 1.000 | ||
| R1 | 0.047 | 1.777 (1.008–3.134) | 0.006 | 2.765 (1.339–5.710) | |
| R2 | <0.001 | 3.383 (1.666–6.870) | 0.003 | 4.007 (1.615–9.945) | |
| Serum CA19-9 | 1.0 U/mL increase | 0.790 | 1.000 (0.999–1.000) | 0.438 | 1.000 (0.999–1.000) |
| Serum CRP | <5.00 mg/dL | 1.000 | 1.000 | ||
| ≥5.00 mg/dL | 0.045 | 1.683 (1.011–2.802) | 0.044 | 1.934 (1.019–3.670) | |
| SAI | 1.0 increase | 0.756 | 1.002 (0.991–1.012) | 0.835 | 1.001 (0.988–1.015) |
| VAI | 1.0 increase | 0.067 | 1.010 (0.999–1.021) | 0.239 | 1.008 (0.995–1.021) |
| VSR | 1.00 increase | 0.023 | 1.502 (1.114–2.225) | 0.047 | 1.855 (1.029–3.501) |
| SAT HU | 1.0 HU increase | 0.094 | 1.020 (0.997–1.044) | 0.322 | 1.014 (0.986–1.044) |
| SAT SUV | 1.00 increase | 0.059 | 11.354 (0.980–64.065) | 0.398 | 3.468 (0.194–62.099) |
| VAT HU | 1.0 HU increase | 0.031 | 1.027 (1.002–1.053) | 0.093 | 1.026 (0.996–1.058) |
| VAT SUV | 1.00 increase | 0.001 | 18.747 (4.871–72.160) | 0.003 | 10.334 (2.181–48.959) |
| Variables | Recurrence-Free Survival | Overall Survival | ||
|---|---|---|---|---|
| p-Values | Hazard Ratio (95% Confidence Interval) | p-Values | Hazard Ratio (95% Confidence Interval) | |
| VSR (1.00 increase) | 0.024 | 1.718 (1.073–2.752) | 0.124 | 1.250 (0.823–2.161) |
| VAT HU (1.0 HU increase) | 0.151 | 1.023 (0.992–1.054) | 0.733 | 1.006 (0.972–1.042) |
| VAT SUV (1.00 increase) | 0.033 | 9.781 (2.137–44.769) | 0.126 | 3.479 (0.705–17.180) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.W.; Yoo, I.D.; Hong, S.-p.; Kang, B.; Kim, J.S.; Kim, Y.K.; Bae, S.H.; Jang, S.J.; Lee, S.M. Prognostic Impact of Visceral Adipose Tissue Imaging Parameters in Patients with Cholangiocarcinoma after Surgical Resection. Int. J. Mol. Sci. 2024, 25, 3939. https://doi.org/10.3390/ijms25073939
Lee JW, Yoo ID, Hong S-p, Kang B, Kim JS, Kim YK, Bae SH, Jang SJ, Lee SM. Prognostic Impact of Visceral Adipose Tissue Imaging Parameters in Patients with Cholangiocarcinoma after Surgical Resection. International Journal of Molecular Sciences. 2024; 25(7):3939. https://doi.org/10.3390/ijms25073939
Chicago/Turabian StyleLee, Jeong Won, Ik Dong Yoo, Sun-pyo Hong, Beodeul Kang, Jung Sun Kim, Yung Kil Kim, Sang Ho Bae, Su Jin Jang, and Sang Mi Lee. 2024. "Prognostic Impact of Visceral Adipose Tissue Imaging Parameters in Patients with Cholangiocarcinoma after Surgical Resection" International Journal of Molecular Sciences 25, no. 7: 3939. https://doi.org/10.3390/ijms25073939
APA StyleLee, J. W., Yoo, I. D., Hong, S.-p., Kang, B., Kim, J. S., Kim, Y. K., Bae, S. H., Jang, S. J., & Lee, S. M. (2024). Prognostic Impact of Visceral Adipose Tissue Imaging Parameters in Patients with Cholangiocarcinoma after Surgical Resection. International Journal of Molecular Sciences, 25(7), 3939. https://doi.org/10.3390/ijms25073939