
Association between PD-L1 Expression and the Prognosis and Clinicopathologic Features of Non-Clear Cell Renal Cell Carcinoma

 ,
,
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
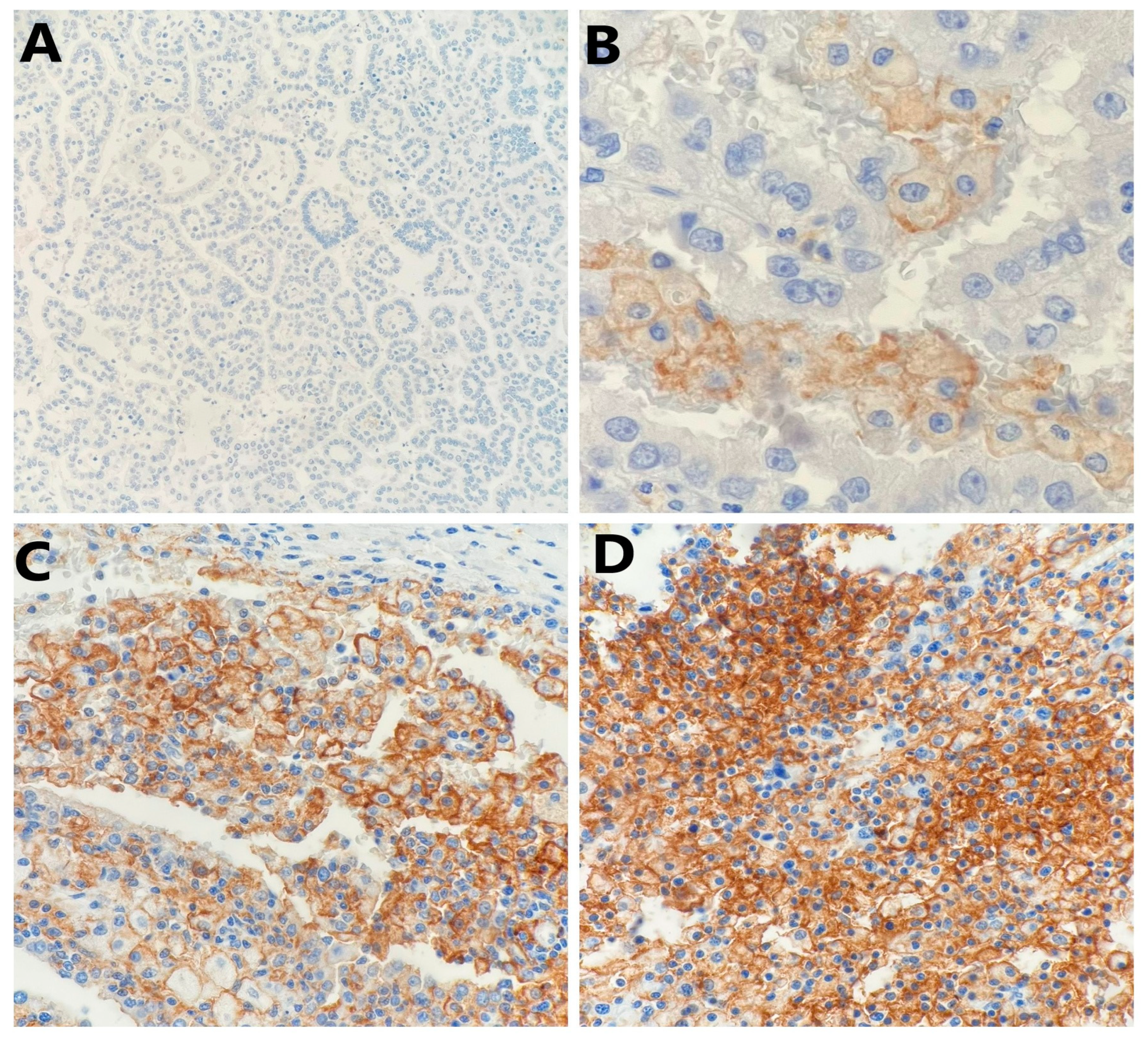
2.2. PD-L1 Expression in Tumor Cells and Clinicopathological Features
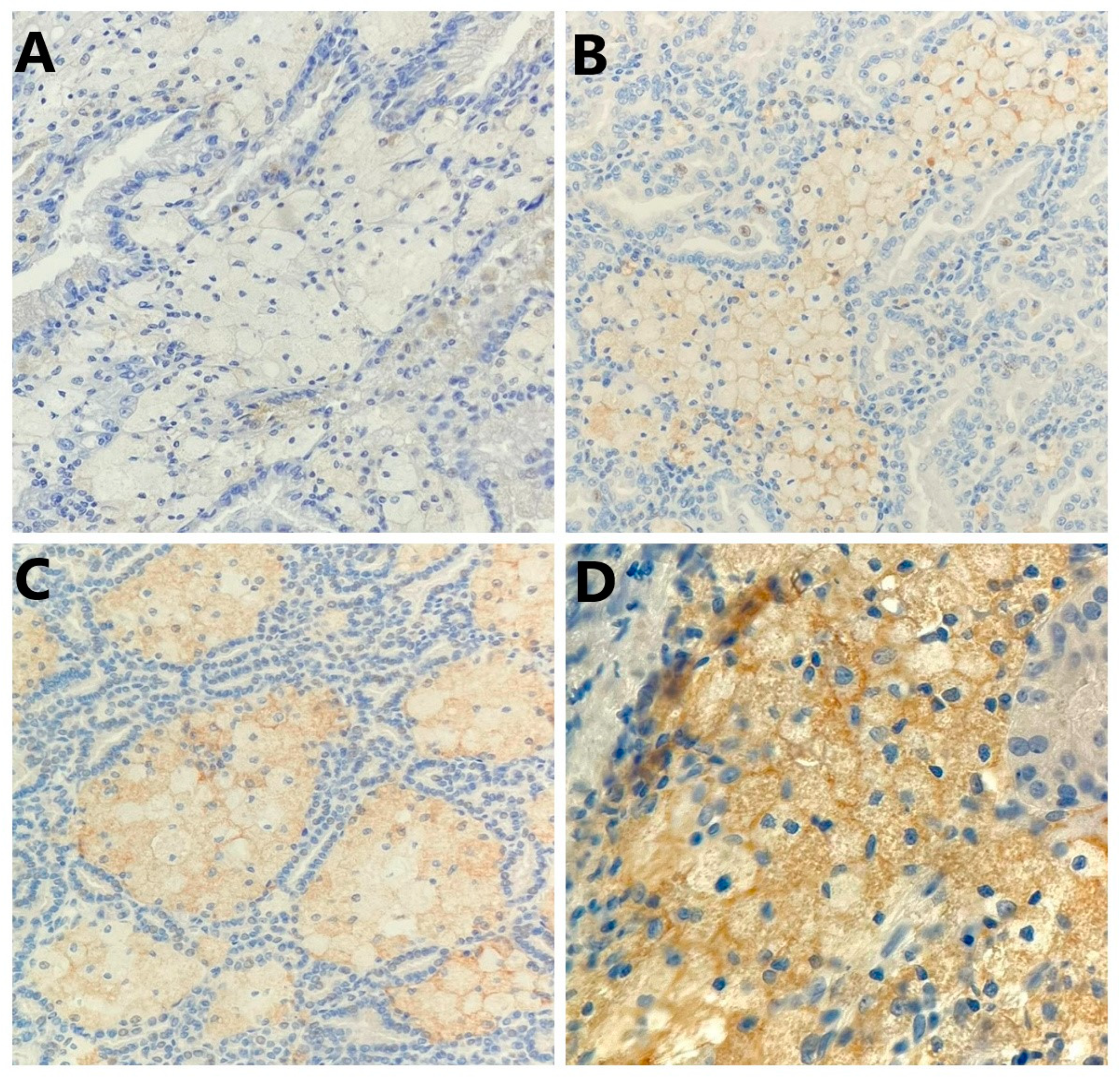
2.3. PD-L1 Expression in Tumor-Infiltrating Mononuclear Cells (TIMCs) and Clinicopathological Features
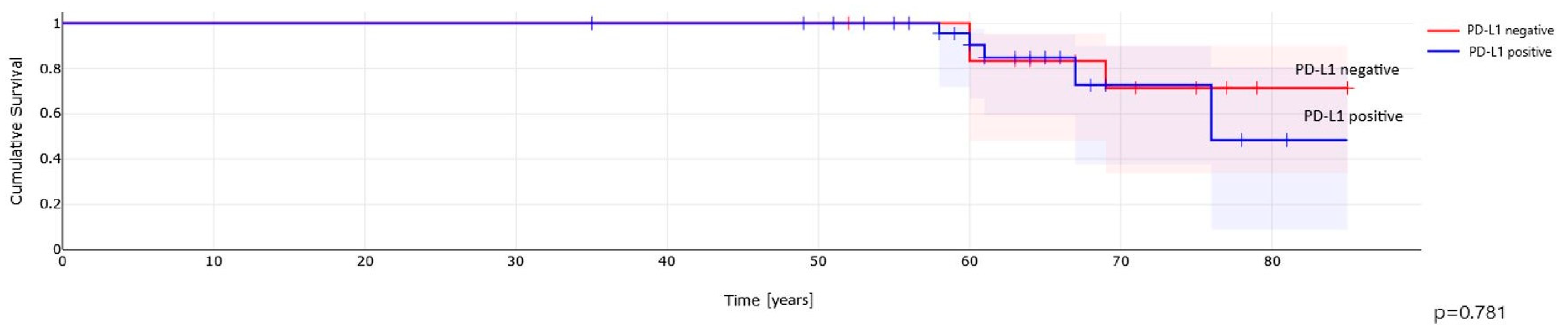
2.4. PD-L1 Expression and Clinical Outcome in Non-ccRCC Patients
3. Discussion
4. Materials and Methods
4.1. Patients and Tumor Characteristics
4.2. Immunohistochemical Staining
4.3. Interpretation of IHC Staining
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shen, M.; Chen, G.; Xie, Q.; Li, X.; Xu, H.; Wang, H.; Zhao, S. Association between PD-L1 Expression and the Prognosis and Clinicopathologic Features of Renal Cell Carcinoma: A Systematic Review and Meta-Analysis. Urol. Int. 2020, 104, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Moch, H.; Humphrey, P.A.; Ulbright, T.M.; Reuter, V. WHO Classification of Tumours of the Urinary System and Male Genital Organs; International Agency for Research on Cancer: Lyon, France, 2016.
- Möller, K.; Fraune, C.; Blessin, N.C.; Lennartz, M.; Kluth, M.; Hube-Magg, C.; Lindhorst, L.; Dahlem, R.; Fisch, M.; Eichenauer, T.; et al. Tumor cell PD-L1 expression is a strong predictor of unfavorable prognosis in immune checkpoint therapy-naive clear cell renal cell cancer. Int. Urol. Nephrol. 2021, 53, 2493–2503. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Fay, A.P.; Gray, K.P.; Callea, M.; Ho, T.H.; Albiges, L.; Bellmunt, J.; Song, J.; Carvo, I.; Lampron, M.; et al. PD-L1 expression in nonclear-cell renal cell carcinoma. Ann. Oncol. 2014, 25, 2178–2184. [Google Scholar] [CrossRef]
- Heng, D.Y.; Choueiri, T.K. Non-clear cell renal cancer: Features and medical management. J. Natl. Compr. Cancer Netw. 2009, 7, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Bacik, J.; Mariani, T.; Russo, P.; Mazumdar, M.; Reuter, V. Treatment outcome and survival associated with metastatic renal cell carcinoma of non-clear-cell histology. J. Clin. Oncol. 2002, 20, 2376–2381. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; Choueiri, T.K.; Fougeray, R.; Schutz, F.A.; Salhi, Y.; Winquist, E.; Culine, S.; von der Maase, H.; Vaughn, D.J.; Rosenberg, J.E. Prognostic factors in patients with advanced transitional cell carcinoma of the urothelial tract experiencing treatment failure with platinum-containing regimens. J. Clin. Oncol. 2010, 28, 1850–1855. [Google Scholar] [CrossRef]
- Shin, S.J.; Jeon, Y.K.; Kim, P.J.; Cho, Y.M.; Koh, J.; Chung, D.H.; Go, H. Clinicopathologic Analysis of PD-L1 and PD-L2 Expression in Renal Cell Carcinoma: Association with Oncogenic Proteins Status. Ann. Surg. Oncol. 2016, 23, 694–702. [Google Scholar] [CrossRef]
- Abbas, M.; Steffens, S.; Bellut, M.; Becker, J.U.; Großhennig, A.; Eggers, H.; Wegener, G.; Kuczyk, M.A.; Kreipe, H.H.; Grünwald, V.; et al. Do programmed death 1 (PD-1) and its ligand (PD-L1) play a role in patients with non-clear cell renal cell carcinoma? Med. Oncol. 2016, 33, 59. [Google Scholar] [CrossRef]
- Han, Y.; Liu, D.; Li, L. PD-1/PD-L1 pathway: Current researches in cancer. Am. J. Cancer Res. 2020, 10, 727–742. [Google Scholar]
- Ahmadzadeh, M.; Johnson, L.A.; Heemskerk, B.; Wunderlich, J.R.; Dudley, M.E.; White, D.E.; Rosenberg, S.A. Tumor antigen-specific CD8 T cells infiltrating the tumor express high levels of PD-1 and are functionally impaired. Blood 2009, 114, 1537–1544. [Google Scholar] [CrossRef]
- Sharpe, A.H.; Wherry, E.J.; Ahmed, R.; Freeman, G.J. The function of programmed cell death 1 and its ligands in regulating autoimmunity and infection. Nat. Immunol. 2007, 8, 239–245. [Google Scholar] [CrossRef]
- Ohaegbulam, K.C.; Assal, A.; Lazar-Molnar, E.; Yao, Y.; Zang, X. Human cancer immunotherapy with antibodies to the PD-1 and PD-L1 pathway. Trends Mol. Med. 2015, 21, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Diaz, A.; Shin, D.S.; Moreno, B.H.; Saco, J.; Escuin-Ordinas, H.; Rodriguez, G.A.; Zaretsky, J.M.; Sun, L.; Hugo, W.; Wang, X.; et al. Interferon receptor signaling pathways regulating PD-L1 and PD-L2 expression. Cell Rep. 2017, 19, 1189–1201. [Google Scholar] [CrossRef] [PubMed]
- Dong, P.; Xiong, Y.; Yue, J.; Hanley, S.J.B.; Watari, H. Tumor-intrinsic PD-L1 signaling in cancer initiation, development and treatment: Beyond immune evasion. Front. Oncol. 2018, 8, 386. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Strome, S.E.; Salomao, D.R.; Tamura, H.; Hirano, F.; Flies, D.B.; Roche, P.C.; Lu, J.; Zhu, G.; Tamada, K.; et al. Tumor-associated B7-H1 promotes T-cell apoptosis: A potential mechanism of immune evasion. Nat. Med. 2002, 8, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Zou, W.; Chen, L. Inhibitory B7-family molecules in the tumour microenvironment. Nat. Rev. Immunol. 2008, 8, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.; Hwu, W.J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef]
- Chipollini, J.; Azizi, M.; Peyton, C.C.; Tang, D.H.; Dhillon, J.; Spiess, P.E. Implications of Programmed Death Ligand-1 Positivity in Non-Clear Cell Renal Cell Carcinoma. J. Kidney Cancer VHL 2018, 5, 6–13. [Google Scholar] [CrossRef]
- Chandrasekaran, D.; Sundaram, S.; Kadhiresan, N.; Padmavathi, R. Programmed Death Ligand 1; An Immunotarget for Renal Cell Carcinoma. Asian Pac. J. Cancer Prev. 2019, 20, 2951–2957. [Google Scholar] [CrossRef] [PubMed]
- Walter, B.; Gil, S.; Naizhen, X.; Kruhlak, M.J.; Linehan, W.M.; Srinivasan, R.; Merino, M.J. Determination of the Expression of PD-L1 in the Morphologic Spectrum of Renal Cell Carcinoma. J. Cancer 2020, 11, 3596–3603. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Chen, M.; Nie, H.; Yuan, Y. PD-1 and PD-L1 in cancer immunotherapy: Clinical implications and future considerations. Hum. Vaccin. Immunother. 2019, 15, 1111–1122. [Google Scholar] [CrossRef]
- Sanmamed, M.F.; Chen, L. A paradigm shift in cancer immunotherapy: From enhancement to normalization. Cell 2018, 175, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Schrader, A.J.; Varga, Z.; Hegele, A.; Pfoertner, S.; Olbert, P.; Hofmann, R. Second-line strategies for metastatic renal cell carcinoma: Classics and novel approaches. J. Cancer Res. Clin. Oncol. 2006, 132, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Vera-Badillo, F.E.; Templeton, A.J.; Duran, I.; Ocana, A.; de Gouveia, P.; Aneja, P.; Knox, J.J.; Tannock, I.F.; Escudier, B.; Amir, E. Systemic therapy for non-clear cell renal cell carcinomas: A systematic review and meta-analysis. Eur. Urol. 2015, 67, 740–749. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Sullivan, D.C.; Brookland, R.K. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2016. [Google Scholar]
- Thompson, R.H.; Gillett, M.D.; Cheville, J.C.; Lohse, C.M.; Dong, H.; Webster, W.S.; Krejci, K.G.; Lobo, J.R.; Sengupta, S.; Chen, L.; et al. Costimulatory B7-H1 in renal cell carcinoma patients: Indicator of tumor aggressiveness and potential therapeutic target. Proc. Natl. Acad. Sci. USA 2004, 101, 17174–17179. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.H.; Kuntz, S.M.; Leibovich, B.C.; Dong, H.; Lohse, C.M.; Webster, W.S.; Sengupta, S.; Frank, I.; Parker, A.S.; Zincke, H.; et al. Tumor B7-H1 is associated with poor prognosis in renal cell carcinoma patients with long-term follow-up. Cancer Res. 2006, 66, 3381–3385. [Google Scholar] [CrossRef] [PubMed]
- Festino, L.; Botti, G.; Lorigan, P.; Masucci, G.V.; Hipp, J.D.; Horak, C.E.; Melero, I.; Ascierto, P.A. Cancer Treatment with Anti-PD-1/PD-L1 Agents: Is PD-L1 Expression a Biomarker for Patient Selection? Drugs 2016, 76, 925–945. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Papillary RCC | Chromophobe RCC | Total Non-ccRCC |
|---|---|---|---|
| Number of tumor samples [n (%)] | 41 (67.2%) | 20 (32.8%) | 61 (100.0%) |
| Age at diagnosis, years [mean ± SD] | 64 ± 8 | 60 ± 9 | 62 ± 9 |
| Gender [n (%)] | |||
| Female | 9 (21.9%) | 7 (35.0%) | 16 (26.2%) |
| Male | 32 (78.1%) | 13 (65.0%) | 45 (73.8%) |
| Type of operation [n (%)] | |||
| Radical nephrectomy | 14 (34.1%) | 5 (25.0%) | 19 (31.1%) |
| Partial nephrectomy | 27 (65.9%) | 15 (75.0%) | 42 (68.9%) |
| Tumor location [n (%)] | |||
| Right kidney | 24 (41.5%) | 11 (55.0%) | 35 (57.4%) |
| Left kidney | 17 (58.5%) | 9 (45.0%) | 26 (42.6%) |
| Tumor size, cm (mean ± SD) | 4.9 ± 3.3 | 3.8 ± 2.1 | 4.5 ± 1.9 |
| Tumor stage [n (%)] | |||
| pT1 | 26 (63.4%) | 13 (65.0%) | 39 (63.9%) |
| pT2 | 7 (17.1%) | 2 (10.0%) | 9 (14.8%) |
| pT3 | 8 (19.5%) | 5 (25.0%) | 13 (21.3%) |
| pT4 | 0 | 0 | 0 |
| WHO/ISUP grading | |||
| G1 | 11 (26.8%) | - | - |
| G2 | 24 (58.5%) | - | - |
| G3 | 2 (4.9%) | - | - |
| G4 | 4 (9.8%) | - | - |
| Tumor necrosis area % (mean ± SD) | 14.5 ± 26.8 | 2.5 ± 7.8 | 10.6 ± 2.6 |
| Sarcomatoid area % (mean ± SD) | 2.5 ± 12.6 | - | - |
| Rhabdoid area % (mean ± SD) | 0 | - | - |
| Lymphatic invasion present [n (%)] | 4 (9.8%) | 0 | 4 (6.3%) |
| Angioinvasion present [n (%)] | 5 (12.2%) | 0 | 5 (7.9%) |
| Neuroinvasion present [n (%)] | 2 (4.9%) | 0 | 2 (3.2%) |
| Renal fibrous capsule invasion present [n (%)] | 21 (51.2%) | 8 (40.0%) | 29 (47.5%) |
| Perinephric fat invasion present [n (%)] | 7 (17.1%) | 4 (20.0%) | 11 (18.0%) |
| Renal sinus fat invasion present [n (%)] | 4 (9.8%) | 1 (5.0%) | 5 (8.2%) |
| Renal sinus vascular invasion present [n (%)] | 3 (7.3%) | 0 | 3 (4.9%) |
| Deaths [n (%)] | 6 (14.6%) | 0 | 6 (9.8%) |
| Feature | PD-L1 in Cancer Cells | PD-L1 in TIMCs | ||||
|---|---|---|---|---|---|---|
| PD-L1 + n (%) | PD-L1 – n (%) | p-Value | PD-L1 + n (%) | PD-L1 – n (%) | p-Value | |
| Age at surgery | 0.74 | 0.02 | ||||
| 35–45 | 1 (2.43%) | 0 | 1 (2.43%) | 0 | ||
| 46–55 | 1 (2.43%) | 4 (9.76%) | 4 (9.76%) | 1 (2.43%) | ||
| 56–65 | 6 (14.30%) | 12 (29.27%) | 15 (36.58%) | 3 (7.32%) | ||
| 66–75 | 4 (9.76%) | 7 (17.07%) | 7 (17.07%) | 4 (9.76%) | ||
| 76–85 | 3 (7.32%) | 3 (7.32%) | 3 (7.32%) | 3 (7.32%) | ||
| Sex | 0.89 | 0.47 | ||||
| Male | 10 (24.39%) | 22 (53.66%) | 26 (63.41%) | 6 (14.30%) | ||
| Female | 5 (12.19%) | 4 (9.76%) | 4 (9.76%) | 5 (12.19%) | ||
| Tumor stage | 0.25 | 0.51 | ||||
| pT1 | 9 (21.95%) | 11 (26.83%) | 14 (34.50%) | 6 (14.30%) | ||
| pT2 | 4 (9.76%) | 8 (19.51%) | 10 (24.39%) | 2 (4.88%) | ||
| pT3/4 | 2 (4.88%) | 7 (17.07%) | 6 (14.30%) | 3 (7.32%) | ||
| WHO/ISUP grade | 0.81 | 0.61 | ||||
| G1 | 3 (7.32%) | 8 (19.51%) | 8 (19.51%) | 3 (7.32%) | ||
| G2 | 11 (26.83%) | 13 (31.70%) | 18 (43.90%) | 6 (14.30%) | ||
| G3 | 0 | 2 (4.88%) | 2 (4.88%) | 0 | ||
| G4 | 1 (2.43%) | 3 (7.32%) | 2 (4.88%) | 2 (4.88%) | ||
| Tumor necrosis | 0.27 | 0.65 | ||||
| Present | 4 (9.76%) | 12 (29.27%) | 10 (24.39%) | 6 (14.30%) | ||
| Absent | 11 (26.83%) | 14 (34.50%) | 20 (48.78%) | 5 (12.19%) | ||
| Angioinvasion | 0.27 | 0.28 | ||||
| Present | 3 (7.32%) | 2 (4.88%) | 5 (12.19%) | 0 | ||
| Absent | 12 (29.27%) | 24 (58.54%) | 25 (60.97%) | 11 (26.83%) | ||
| Neuroinvasion | 0.25 | 0.15 | ||||
| Present | 1 (2.43%) | 1 (2.43%) | 2 (4.88%) | 0 | ||
| Absent | 14 (34.50%) | 25 (60.97%) | 28 (68.29%) | 11 (26.83%) | ||
| Renal fibrous capsule invasion | 0.69 | 0.39 | ||||
| Present | 9 (21.95%) | 10 (24.39%) | 14 (34.50%) | 5 (12.19%) | ||
| Absent | 6 (14.30%) | 16 (39.02%) | 15 (36.58%) | 6 (14.30%) | ||
| Perinephric fat invasion | 0.80 | 0.15 | ||||
| Present | 2 (4.88%) | 4 (9.76%) | 6 (14.30%) | 0 | ||
| Absent | 13 (31.70%) | 22 (53.66%) | 24 (58.54%) | 11 (26.83%) | ||
| Overall survival | 0.80 | 0.15 | ||||
| Death | 2 (4.88%) | 4 (9.76%) | 6 (14.30%) | 0 | ||
| Survival | 13 (31.70%) | 22 (53.66%) | 24 (58.54%) | 11 (26.83%) | ||
| Feature | PD-L1 in Cancer Cells | PD-L1 in TIMCs | ||||
|---|---|---|---|---|---|---|
| PD-L1 + n (%) | PD-L1 – n (%) | p-Value | PD-L1 + n (%) | PD-L1 – n (%) | p-Value | |
| Age at diagnosis | 0.35 | 0.28 | ||||
| 35–45 | 1 (5%) | 0 | 1 (5%) | 0 | ||
| 46–55 | 3 (15%) | 2 (10%) | 2 (10%) | 3 (15%) | ||
| 56–65 | 7 (35%) | 0 | 5 (25%) | 2 (10%) | ||
| 66–75 | 6 (30%) | 1 (5%) | 2 (10%) | 5 (25%) | ||
| Sex | 0.14 | 0.35 | ||||
| Male | 12 (60%) | 1 (5%) | 7 (35%) | 6 (30%) | ||
| Female | 5 (25%) | 2 (10%) | 3 (15%) | 4 (20%) | ||
| Tumor stage | 0.33 | 0.71 | ||||
| pT1 | 9 (45%) | 2 (10%) | 6 (30%) | 5 (25%) | ||
| pT2 | 6 (30%) | 1 (5%) | 3 (15%) | 4 (20%) | ||
| pT3/4 | 2 (10%) | 0 | 1 (5%) | 1 (5%) | ||
| Tumor necrosis | 0.97 | 0.32 | ||||
| Present | 3 (15%) | 0 | 1 (5%) | 2 (10%) | ||
| Absent | 15 (75%) | 2 (10%) | 9 (45%) | 8 (40%) | ||
| Angioinvasion | 0.052 | 0.056 | ||||
| Present | 0 | 0 | 0 | 0 | ||
| Absent | 17 (85%) | 3 (15%) | 10 (50%) | 10 (50%) | ||
| Neuroinvasion | 0.050 | 0.054 | ||||
| Present | 0 | 0 | 0 | 0 | ||
| Absent | 17 (85%) | 3 (15%) | 10 (50%) | 10 (50%) | ||
| Renal fibrous capsule invasion | 0.81 | 0.39 | ||||
| Present | 7 (35%) | 1 (5%) | 5 (25%) | 3 (15%) | ||
| Absent | 10 (50%) | 2 (10%) | 5 (25%) | 7 (35%) | ||
| Perinephric fat invasion | 0.73 | 0.13 | ||||
| Present | 3 (15%) | 1 (5%) | 1 (5%) | 3 (15%) | ||
| Absent | 14 (70%) | 2 (10%) | 9 (45%) | 7 (35%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chrabańska, M.; Szweda-Gandor, N.; Rynkiewicz, M.; Hraboš, D.; Drozdzowska, B. Association between PD-L1 Expression and the Prognosis and Clinicopathologic Features of Non-Clear Cell Renal Cell Carcinoma. Int. J. Mol. Sci. 2024, 25, 3916. https://doi.org/10.3390/ijms25073916
Chrabańska M, Szweda-Gandor N, Rynkiewicz M, Hraboš D, Drozdzowska B. Association between PD-L1 Expression and the Prognosis and Clinicopathologic Features of Non-Clear Cell Renal Cell Carcinoma. International Journal of Molecular Sciences. 2024; 25(7):3916. https://doi.org/10.3390/ijms25073916
Chicago/Turabian StyleChrabańska, Magdalena, Nikola Szweda-Gandor, Magdalena Rynkiewicz, Dominik Hraboš, and Bogna Drozdzowska. 2024. "Association between PD-L1 Expression and the Prognosis and Clinicopathologic Features of Non-Clear Cell Renal Cell Carcinoma" International Journal of Molecular Sciences 25, no. 7: 3916. https://doi.org/10.3390/ijms25073916
APA StyleChrabańska, M., Szweda-Gandor, N., Rynkiewicz, M., Hraboš, D., & Drozdzowska, B. (2024). Association between PD-L1 Expression and the Prognosis and Clinicopathologic Features of Non-Clear Cell Renal Cell Carcinoma. International Journal of Molecular Sciences, 25(7), 3916. https://doi.org/10.3390/ijms25073916